Abdominal Tuberculosis
Dr.Sujith Mathew JosePG in General Surgery
Coimbatore Medical College Coimbatore
Introduction
TB can involve any part of GIT from mouth to
anus, peritoneum &
pancreatobiliary system.
• TB of GIT(peritoneal)- 6th most frequent extrapulmonary site.
• LYMPHATIC ----- 1st
• GENITOURINARY• BONE & JOINTS• MILIARY• MENINGEAL------ 5th
• Most case from reactivation of latent peritonial disease, previously established hematogenously from primary pulmonary focus
Pathogenesis• Mechanisms by which M. tuberculosis reach the
GIT:– Hematogenous spread from primary lung focus
– Ingestion of bacilli in sputum from active pulmonary focus.
– Direct spread from adjacent organs.
– Via lymph channels from infected LN
• In India, organism from all intestinal lesions – M. tuberculosis and not M. bovis.
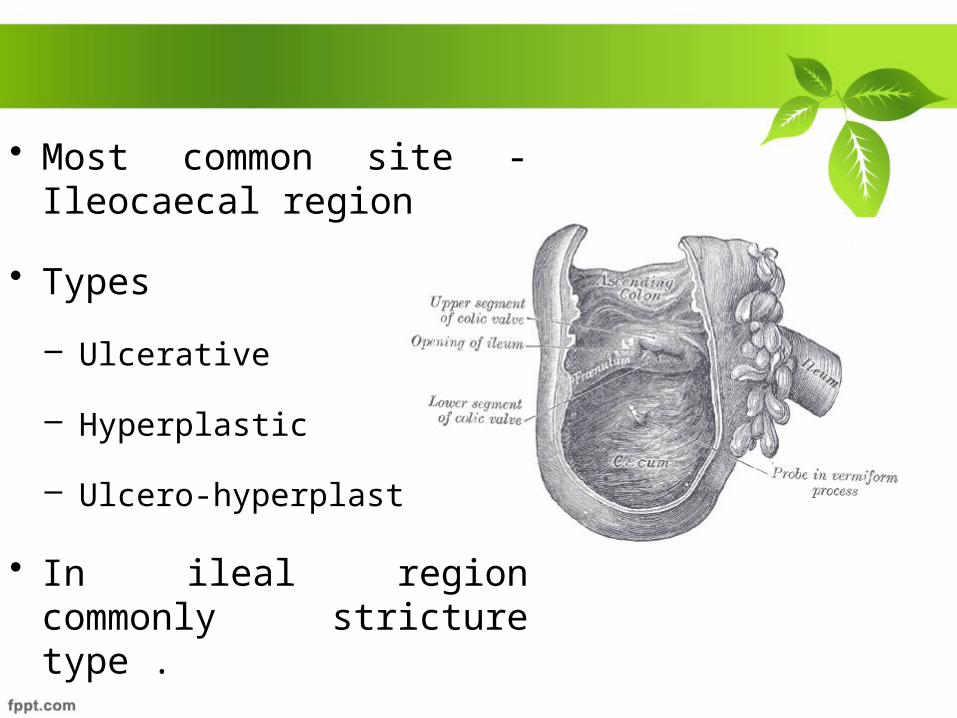
• Most common site - Ileocaecal region
• Types
– Ulcerative
– Hyperplastic
– Ulcero-hyperplastic
• In ileal region commonly stricture type .
• Peritoneal involvement occurs from : – Spread from Lymph node– Intestinal lesions – Tubercular salpingitis
• Abdominal lymph node and peritoneal TB may occur without GIT involvement in ~ 1/3 cases.
Peritoneal tuberculosis occurs in 3 forms.
• Wet type - ascitis.
• Encysted (loculated) type
• Fibrotic type - masses composed of mesenteric &
omental thickening, with matted bowel loops.
Clinical Features• Mainly disease of young adults,
• 2/3 of pts are 21-40 yr with equal sex incidence• Clinical presentation
– Acute – Chronic– Acute on chronic
Abdominal swelling caused by ascitis is the most common symptom
• Constitutional symptoms – Fever (40%-70%)– Weight loss (40%-90%)– Anorexia– Malaise
• Pain abdomen (80%-95%) – Colicky (luminal stenosis) , – Continous ( LN involvement)
• Alternating constipation and diarrhoea
• POSITIVE TUBERCULIN TEST• ASCITIC FLUID SAAG less
than 1.1g/dl• Microscopic examination of
ascitic fluid – ERYTHROCYTES– Increased LEUCOCYTES
(LYMPHOCYTES)
ASCITIC FLUID ADENOSINE DEAMINASE
ACTIVITY IS HIGHLY SENSITIVE AND SPECIFIC FOR
TUBERCULOUS PERITONITIS
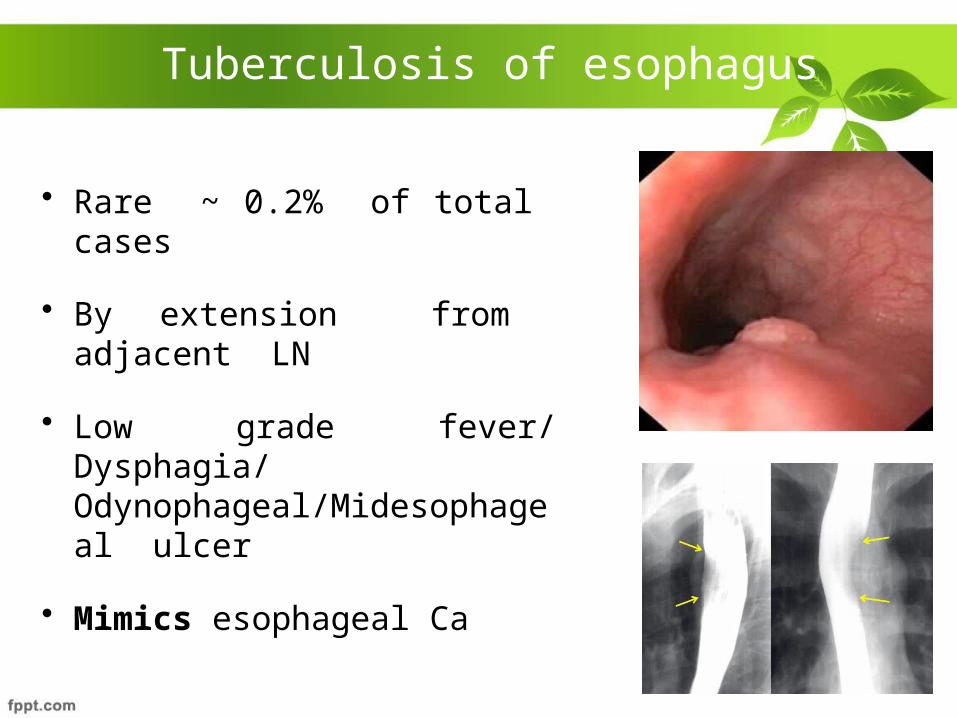
Tuberculosis of esophagus
• Rare ~ 0.2% of total cases
• By extension from adjacent LN
• Low grade fever/ Dysphagia/ Odynophageal/Midesophageal ulcer
• Mimics esophageal Ca
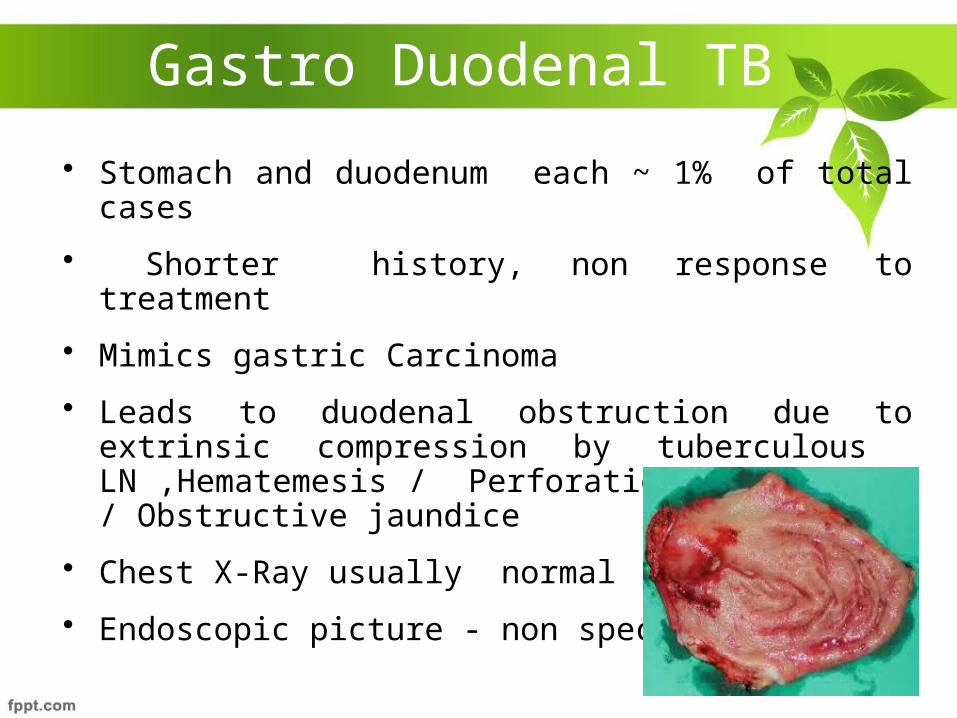
Gastro Duodenal TB
• Stomach and duodenum each ~ 1% of total cases
• Shorter history, non response to treatment
• Mimics gastric Carcinoma
• Leads to duodenal obstruction due to extrinsic compression by tuberculous LN ,Hematemesis / Perforation / Fistulae / Obstructive jaundice
• Chest X-Ray usually normal
• Endoscopic picture - non specific
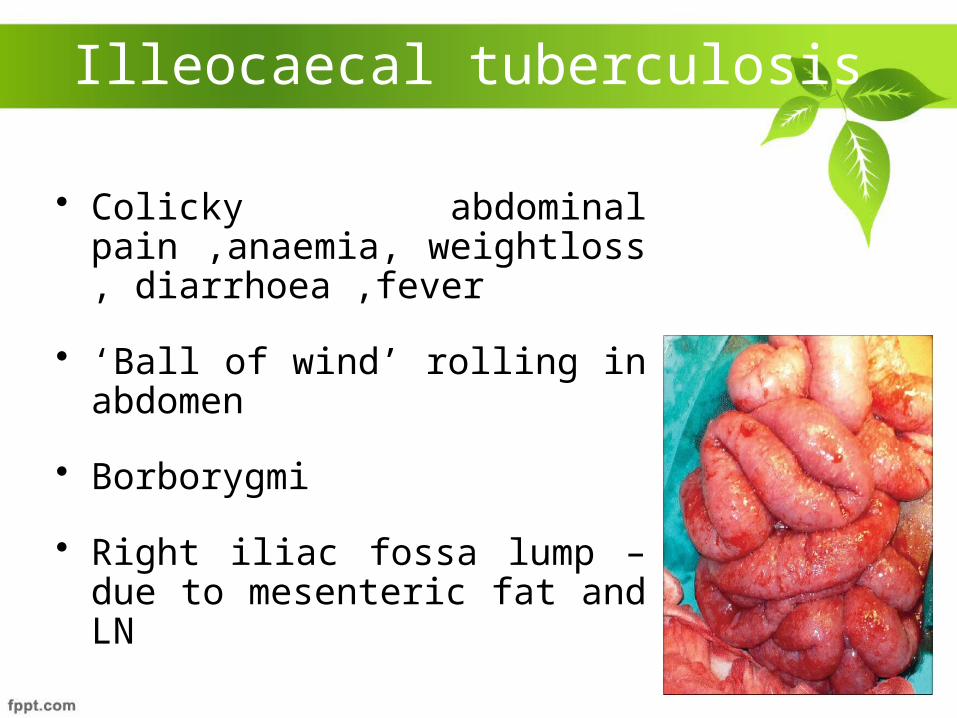
Illeocaecal tuberculosis
• Colicky abdominal pain ,anaemia, weightloss , diarrhoea ,fever
• ‘Ball of wind’ rolling in abdomen
• Borborygmi
• Right iliac fossa lump – due to mesenteric fat and LN
Segmental / Isolated colonic tuberculosis
• Involvement of the colon without involvement of the ileocaecal region
• 9.2% of all cases
• Multifocal involvement in ~ 1/3 of cases (28% to 44%)
• Median symptom duration <1 year
Colonic tuberculosis
• Pain --- predominant symptom ( 78%-90% )• Hematochezia in < 1/3 - usually minor
Overall, TB accounts for ~ 4% of lower GI bleeding
• Other features--- fever / anorexia / weight loss / change in bowel habits
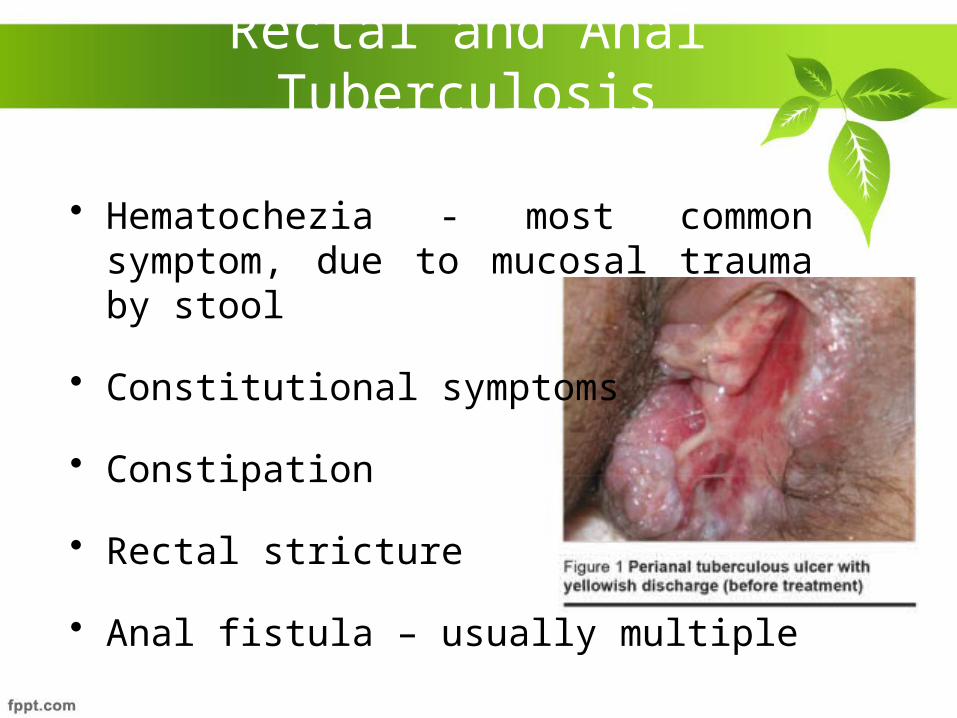
Rectal and Anal Tuberculosis
• Hematochezia - most common symptom, due to mucosal trauma by stool
• Constitutional symptoms
• Constipation
• Rectal stricture
• Anal fistula – usually multiple
Complications
• Obstruction
• Perforation -2nd commonest cause after typhoid ,usually single and proximal to a stricture,Pneumoperitoneum in ~ 50% cases
• Mal-absorption
• Fecal fistula
• Cold abscess
• Haemorrhage
Diagnosis and InvestigationsRaised ESR
Positive Mantoux Test
Chest X Ray Findings
Low Hb ----- anemia
Hypoalbuminemia
ELISA (90%)
SAFA (Soluble Antigen Fluroscent Antibody)
Serum IgG
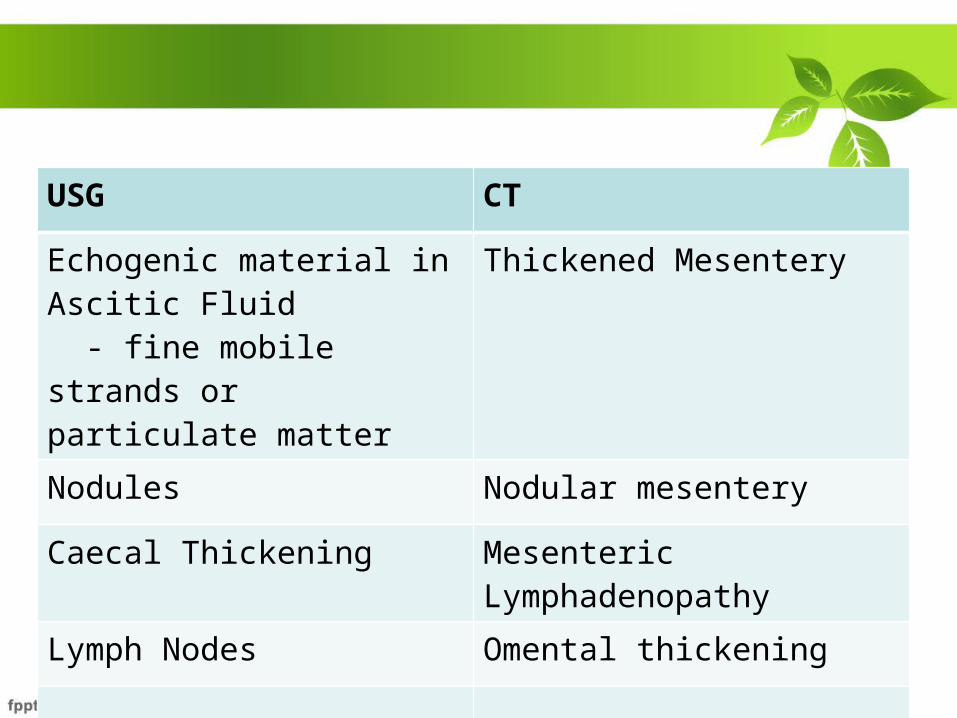
USG CT
Echogenic material in Ascitic Fluid - fine mobile strands or particulate matter
Thickened Mesentery
Nodules Nodular mesentery
Caecal Thickening Mesenteric Lymphadenopathy
Lymph Nodes Omental thickening
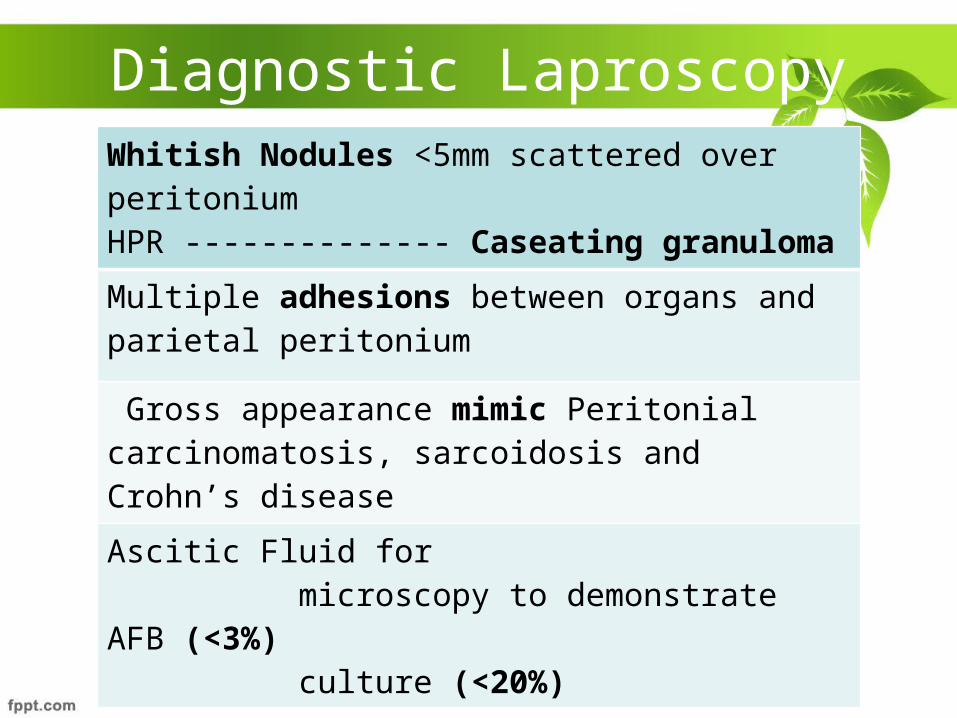
Diagnostic LaproscopyWhitish Nodules <5mm scattered over peritoniumHPR -------------- Caseating granuloma
Multiple adhesions between organs and parietal peritonium
Gross appearance mimic Peritonial carcinomatosis, sarcoidosis and Crohn’s disease
Ascitic Fluid for microscopy to demonstrate AFB (<3%) culture (<20%)
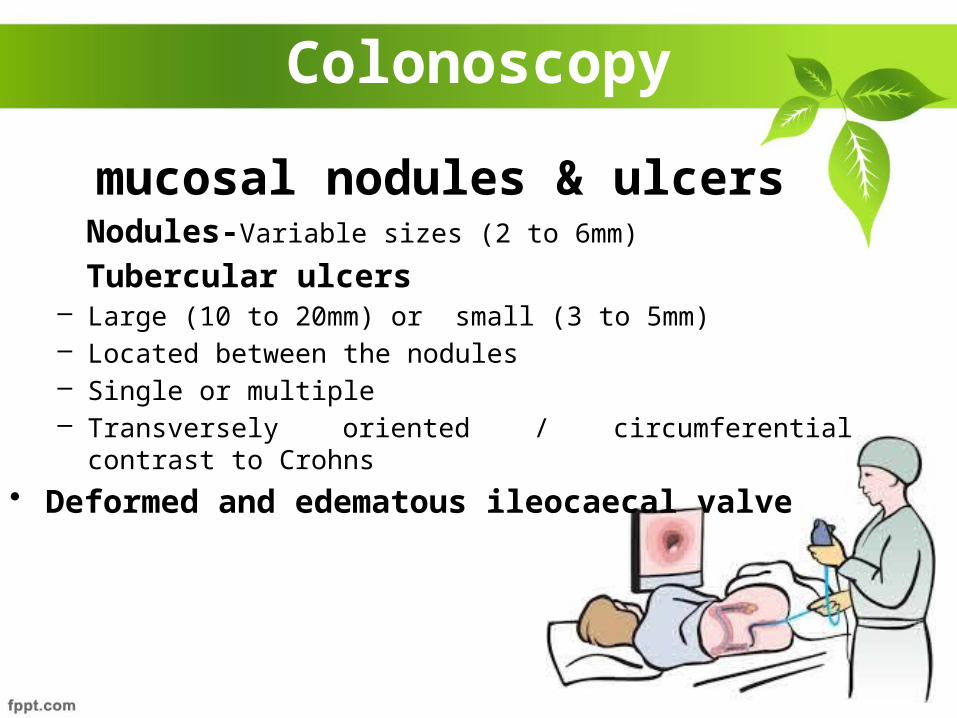
Colonoscopy
mucosal nodules & ulcers Nodules-Variable sizes (2 to 6mm)
Tubercular ulcers– Large (10 to 20mm) or small (3 to 5mm) – Located between the nodules – Single or multiple – Transversely oriented / circumferential contrast to Crohns
• Deformed and edematous ileocaecal valve
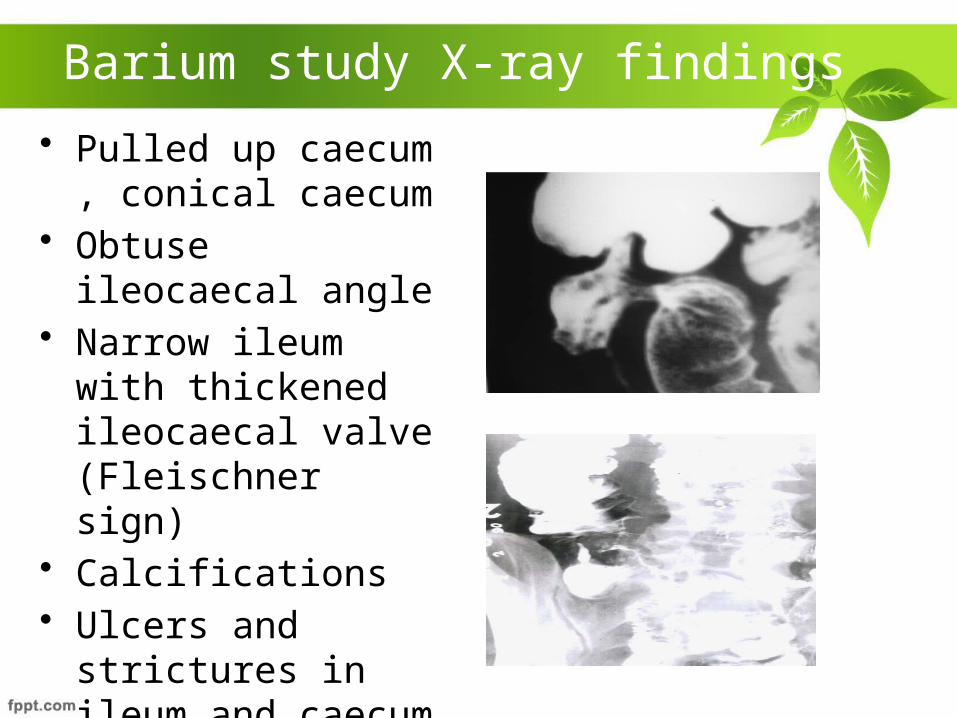
Barium study X-ray findings • Pulled up caecum ,
conical caecum • Obtuse ileocaecal
angle • Narrow ileum with
thickened ileocaecal valve (Fleischner sign)
• Calcifications• Ulcers and strictures
in ileum and caecum –napkin lesions
Ascitic Fluid Study
• Straw coloured Exudate
• Protein >3g/dL
• Total count of 150-4000/µl, Lymphocytes >70%
• SAAG < 1.1 g/dL
• ZN stain positive in < 3% cases
• Positive culture in < 20% cases
• ADA positive
• Glucose <30mg
Treatment
• ATT for at least 6 months -Rifampicin, INH, Pyrazinamide and Ethambutol.
• Surgery –Indications
Intestinal obstruction , severe haemorrhage , perforations , intra-abdominal abscess
• For ileocaecal TB -Limited ileocaecal resection
• Single stricture – stricturoplasty
• In perforation –resection and anastomosis
• In obstruction – ileo-transverse anastomosis
• Drainage of intra-abdominal abscess , perianal abscess
THANK YOU
Recommended

















