A Study of Host-Parasite Relationshipin Loa Loa*A Case Report
WILLIAM R. FELTS, M .D . and EDMUND .1 . TALBOTT, M.D .
Washington, D. C .
P aTHOCENtc filarial infections in man havebeen confined principally to four species of
worms (Wuchereria bancrofti and malayi,Onchocerea volvulus and Loa loa) [1-72] . De-spite considerable knowledge of these parasites,there has been surprisingly little understandingof the exact manner whereby these species exerttheir pathogenic effect .
Hypersensitivity to parasitic antigen has beensuggested as important in the mechanism offilarial infection [13-22]. Coordinated objectivelaboratory and clinical data in support of thisconcept thus far have been inadequate . In thepresent study further data favoring the conceptof hypersensitivity have been made available bythe study of a case of loiasis of twelve years'standing . A detailed study of this case was under-taken in an attempt to (1) determine the hostresponse to prolonged untreated filarial infectionand (2) measure by clinical and laboratorymethods any changes in this response with insti-tution of therapy, with particular reference tostudies of visceral functions and the serologicreflections thereof, and (3) effect a clinical im-provement and possible remission .
CASE REPORT
The patient was a twenty year old white femalecollege student who was admitted to the GeorgeWashington University Hospital on November 3,1952, with a history of first exposure to Loa loa in-fection in 1940 .
The first manifestations were noted approximatelyone year later, while in Gabon, French EquatorialAfrica, a highly endemic area for loiasis [23] . These
re complaints of an intermittent crawling sensationvaried skin areas associated with itching and
occasional low grade fever . Six months to one year
Upland, California
later the patient noticed wormlike forms beneath theskin on the extensor surface of her forearm ; theseforms had continued to be active in different areas ofher body on varied occasions . She described the wormsas having the appearance of a reddish, ire ar,wavy line about ! i to 1 inch in length, and the "sizeof a pin" in diameter, remaining visible from a periodof a few seconds to eight to twelve hours . One episodeof a worm in the subconjunctival tissues had oc-curred, the migration taking three to five minutes .This was associated with itching, burning and in-creased lacrimation . The patient stated that she wasable to localize many of the adult worms by being ableto feel them move in the deep layers of the skin invarious parts of her body, although frequently no ob-jective signs would be visible .
After four years in Gabon, Africa, the patient re-turned to the United States (Florida), apparently infairly good health except for feeling run-down and foroccasional symptoms of subcutaneous activity of adultworms, During the next seven years, with increasingfrequency, she noted intermittent swellings whichappeared in many parts of her body and were accom-panied by malaise . These Calabar swellings were de-scribed as tissue swellings, usually non-painful, occur-ring most often about a joint and lasting for variableperiods of time up to one day . The largest of theseswellings was about 4 inches in diameter .
After seven years in Florida she moved to Indiana(1951) and was exposed for the first time to cold win-ters . From the time of this climatic change until thehospital admission in 1952 she had increased symp-toms, almost to the point of incapacitation, withincreased surface activity of worms, severe malaise,arthralgia, backache, neckaine, vertigo, intolerance tothe extremes of heat and cold, occasional nightsweats, diurnal frontal headaches, diurnal listlessness,severe nocturnal restlessness, occasional sotnnambu-lance, talking in her sleep, and more recently abdomi-nal pain of a variable and indistinct type accompaniedby distention, flatulence, eructations and constipation .
*From the Department of Medicine, The George Washington University Hospital, Washington, D . C. and theLaboratory of Tropical Diseases, National Institutes of Health, Bethesda, Maryland .
IrNE, 1957
995

996The abdominal symptoms persisted after an electiveappendectomy in September, 1952. Premenstrualaggravation of all complaints was noted .
Physical examination at the time of admission re-vealed a well developed, well nourished white womanappearing listless but in no acute distress. Her tem-
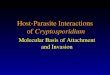
FIG. 1 . Periodicity chart of microfilariae loa in the pa-tient reported herein .
perature was 37° c., pulse 80, respirations 24, bloodpressure 110/60, height 6034 inches and weight 115pounds. No abnormalities of the skin were noted . Sev-eral small, discrete, non-tender lymph nodes werepalpable in the neck. Examination of the chest wasnegative. The abdomen was slightly protuberant withno tenderness and no palpable masses or viscera . Peri-stalsis was slightly hyperactive . Rectal and pelvicexaminations were normal . More complete studieslater revealed bilateral congenital nephroptosis and leftdouble ureter with a double renal pelvis . Generalizedabdominal visceroptosis was also noted but was feltto be asymptomatic. Neurologic examination wasnegative .
Laboratory studies on admission revealed a leuko-cyte count of 12,100 per cu. mm. with 9 per centeosinophilia. The total eosinophil count was 1,729 percu. mm. The hematocrit was 43 per cent and thesedimentation rate 25 mm. in one hour (Wintrobe,corrected) . The gamma globulin was 10.5 unitsmeasured by the zinc sulfate technic [24] . The serumalbumin was 3 .8, serum globulin 3.4 gm. per cent.Liver function tests (including bromsulphalein,thymol turbidity, cephalin-cholesterol flocculationtest, alkaline phosphatase and serum van den Bergh),electrocardiogram, electroencephalogram and chestx-ray were normal. X-rays of the entire gastro-intestinal tract and proctoscopic examination werenegative. Lumbar puncture was performed and thespinal fluid dynamics, chemical tests and cell countswere normal . A search for microfilariae in the spinalfluid was negative. No trypanosomes were demon-strated by direct microscopic, cultural or animalinoculation technics. Multiple stool examination by
Loa Loa-Felts, Talbottdirect, concentration and cultural technics were nega-tive for ova and parasites. Serologic tests for syphiliswere negative. Serologic tests for leishmania, trichinaand endamoeba infections were negative . Notably,the complement-fixation test for filariasis, usingDirofilaria immitis antigen [25], was repeatedlynegative. Microfilariae loa were readily demonstratedin both capillary and venous blood on fresh dropletexamination and by stained preparations. They weredefinitely identified as being L . loa with hematoxylinand eosin preparations, and were described assheathed worms of a length of approximately 275microns, having body nuclei extending to the tip ofthe tail, and an external configuration that was mostoften angular and tortuous .
Periodicity study [26] of microfilariae in this patientwas performed on capillary blood with 20 cu. mm .specimens in triplicate, counted and averaged everyfour hours over a five-day period . The result is illus-trated in Figure 1 .
During the first two weeks of hospitalization emo-tional upsets manifested by agitation were pronouncedand were only partially controlled by barbiturates .These symptoms were worsened during a three-daypremenstrual period .
Because of variable reactions occurring shortlyafter the initial use of hetrazan ® [4,5,13,27-40j, it wasdecided to begin therapy with very low doses of thedrug. Accordingly, the patient was started on hetrazanon November 19, 1952, in doses of 0 .25 mg. per kg .of body weight at six-hour intervals. Serial micro-filarial counts were essentially unchanged during thefollowing week and clinically the patient had no com-plaints or symptoms that were not present prior toinitiation of therapy.
Because of this apparent lack of drug effect thedosage of hetrazan was increased after one week to0.5 mg. per kg . of body weight at six-hour intervals .The response was dramatic . A marked decrease ofmicrofilariae was noted . (Fig . 2 .) Within twelve hoursthe patient became upset emotionally even more thanusual . She complained of sharp right upper quadrantpain, unrelated to respiration, accompanied by ano-rexia, nausea and occasional vomiting . Additionalcomplaints were mild chest pain, myalgia, arthralgiaand pruritus (for the first time) . The patient appearedto be quite ill .
Within twenty-four hours the liver became palpable3 cm. below the right costal margin and was markedlytender. Because of the psychologic state of the patientbiopsies of the liver were not obtained . Liver functiontests now disclosed a 21 per cent bromsulphaleinretention after forty-five minutes ; thymol turbidity,cephalin-cholesterol flocculation test and serumbilirubin remained normal . Gamma globulin was in-creased to 12 .5 units. Blood urea nitrogen was in-creased to 37 mg . per cent with normal urinalysis . Thepatient also noted a marked increase in the activity ofthe adult worms, and for the first time since her
AMERICAN JOURNAL OF MEDICINE

admission to the hospital they actually came to thesurface of the skin . Hetrazan therapy was not stoppedbecause it was anticipated that the hepatitis wouldsubside in spite of continued therapy, as has beenseen by others [3-5,39] . Four days later the liver haddecreased in size and was less tender . Within a week itwas no longer palpable and liver function tests re-verted towards normal . The blood urea nitrogen hadreturned to normal. The total eosinophil count wasnow increased to 2,364 per cu. mm .
At the end of the second week of hetrazan therapythe initial episode of giant urticaria developed, thewheals being distributed primarily over the thighs,lower abdomen and back. The wheals were from 5onus, to 2 cm, in diameter, hyperemic at the onset,fading after a few minutes with blanching at theperiphery and occasional retention of a small spot ofhyperemia in the center of the lesion. Rarely thewheals would start in the shape of a worm, with linearswellings preceding the urticarial spots by a fewseconds or minutes. We were quite impressed by thepatient's distressing complaints which initially wereoften subjective but frequently were followed withinminutes or hours by the appearance of adult wormsand urticariae in the exact skin areas which had been asite of complaint . Antihistamines gave only moderaterelief from the pruritus . (Fig . 3 .)
After the third week of hetrazan therapy the patienthad subjectively recovered from the hepatitis and wasimproved with regard to the adult worm activity . Theremainder of the laboratory work may be seen inFigure 4 where the relation of the various laboratoryfindings to the antiparasitic drugs is shown . It is to benoted that most of the abnormal laboratory findingsreached their peak during the third and fourth weekof hetrazan therapy. For the first time the comple-ment-fixation test for filariasis became strongly posi-JunE, 1957
Loa Loa-Felts, Talbott
i OA LCAEFFECT OF RETRAZAN THERAPY ON CAPTLI ART
BL000 -EVELS OF MICROFILARIAE BLOODSY CIMFNS CRAWK A 200 PM DAILY
Fic . 2 . Effect of hetrazan on daily peak microfilariae levels in this patient .
1
997
Live, then gradually declined during the next threeweeks and again became negative . This occurreddespite the continued presence of small numbers ofcirculating microfilariae . (Fig . 4 .)
We now assumed that the total number of micro-filariae had been so greatly reduced that an increase inhetrazan dosage would no longer have an adverseeffect upon the liver . Thus the hetrazan dosage wasfurther increased gradually (with microfilariac disap-pearing at 4 mg ./kg. per day) until a level of 16 mg .per kg . of body weight per day was reached . The pa-tient received a total of 17 gm. of hetrazan over aperiod of seventy-seven days . Six weeks after initiationof hetrazan therapy two small masses were felt in thedeep subcutaneous tissues near the deltoid muscleinsertion in both arms, and others were found laterelsewhere. These initially appeared as tender, elon-gated masses approximately 3 cm. long which gradu-ally lost their tenderness and decreased in size over anumber of weeks. Permission for biopsy of the masseswas not granted . At this same time an electrocardio-gratn disclosed an inversion of the T wave in leadAVF . This reverted to normal with continuedhetazan therapy one week later .
After five weeks of negative studies for circulatingmicrofilariae and in spite of eleven weeks of hetrazantherapy the patient continued to be troubled occa-sionally, but quite severely, by the adult worm activ-ity and accompanying urticarial reactions . Becausehetrazan is only partially effective against adultfilarial worms [15,41] it was decided to attempteradication of the adult filariae by using a course ofsuramin (naphuride sodium) [42-45] . On February 6,1953, a single intravenous injection of 0 .25 gm. ofsuramin was given . Within ten minutes a solitary2 cm. wheal developed over the left buttock, an areain which the patient had felt an irritation from a

998
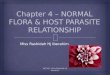
FIG. 3A . Filaria loa beneath skin on thigh in this patient .
Loa Loa-Felts, Talbott
17p , OF 1O< LO INrrCnT : I I ,
,~ ,J
, , I I . 9 L . .
1
l
1.
1' 81111 !'111 'm
FIG. 3B . Urticarial wheal in same site as worm picturedin Figure 3A, which appeared thirty minutes after anintravenous injection of suramin .
FIG . 4. Clinical laboratory studies in this patient with Loa loa as related tochanges in therapy . C. F . = cephalin-cholesterol flocculation. T. T. = thymolturbidity . E. = per cent eosinophils on differential . C. F. T. = complementfixation test for filariasis .
crawling worm shortly before the injection. Five On February 13 a second injection of 1 .0 gm. ofhours later she complained of generalized aching, suramin was given intravenously . Thirty minutes latermalaise and nausea, but noted no additional adult a solitary wheat appeared on the left buttock, startingworm activity. The following week was not remark- in the shape of an adult worm and enlarging to a 13yable. Laboratory findings remained unchanged,
cm. diameter . It faded spontaneously after ten min-AMERICAN JOURNAL OP MEDICINE

Fro . 5 . Electrocardiographic changes illustrated in case of Loa loa during treatment with suramin .
uses . During the following week the only laboratorychange was the development of a 1 to 2 + albuminuria .
On February 20 the patient received the third andlast intravenous injection of 1 .0 gin . of suramin with-out any immediate reaction developing. After approxi-mately twelve hours she noticed a small Calabar swel-ling on the dorsal surface of the left wrist whichsubsided after an hour .
Three days later abdominal distention, crampyabdominal pain, nausea, anorexia, belching and com-plaints of flatus developed . This was followed by vom-iting . There was marked increase in the complaintsof worm activity but the worms were never seen afterthe second suramin injection . The cephalin-cholesterolflocculation test and the thymol turbidity againbecame transiently elevated. For the next two weeksshe was quite ill, and symptoms became so severe thatintravenous fluids had to be given daily . On March 2additional hives on the back, arms, thighs andpopliteal areas, a swollen and hot right elbow jointand severe edema of the right lower eyelid developed,Antihistaminics gave no relief, During this periodelectrocardiographic changes were again noted, butwere more marked than with hetra2an, with inversionof all T waves (leads f, IF, III, AVR, AVL, AVF, andV, to V s) . Serum electrolyte studies (potassium,sodium, calcium, phosphorus, chlorides and CO,combining power) were within normal limits . A thera-peutic trial with oral potassium chloride failed to affectthese changes. A Thorn test, performed with 100 mg .of cortisone, was normal . (Fig . 5 .)
it was our interpretation that the observed ab-normalities were nut due to drug toxicity but to hyper-sensitivity to the filarial antigen . It was decided,therefore, during the fifteenth week of therapy to ad-minister cortisone in order to affect the presumedantigen-antibody reaction . The initial dose of corti-
,luxV, 1957
Loa Loa-Felts . Talbott 999
sane was 100 mg. per day. Dosage was graduallyreduced during the following week and then dis-continued. The clinical response was dramatic .Within twenty-four hours the patient was feeling bet-ter and took food for the first time in four days .Although she continued to have occasional urticariaewhile receiving cortisone, the accompanying subjec-tive reactions became less severe and less frequent . Theelectrocardiogram was unaffected by cortisone butreverted to normal three weeks later. After dischargethe patient was followed for an additional three yearswithout medications . She no longer complains ofmalaise, lethargy, arthralgia or myalgia, and hermental attitude and alertness have improved greatlyin contrast to her previous listless state . She feels betterthan at any time during the twelve years of infectionand realizes, in retrospect, the severity acrd incapacita-tion of her chronic illness . All laboratory tests haveremained normal .
COMMENTS
In this patient with chronic loiasis andmarked parasitemia physical examination priorto treatment did not reveal any objective evi-dence of organic disorder . Except for the posi-tive blood smears, the laboratory studies showedonly slight and non-specific abnormalities . Thescarcity of objective abnormal findings was incontrast to the patient's severe subjective com-plaints. It is of interest that diving the earls*phase of the antiparasitic therapy objective evi-dence of severe multiple system involvementbecame manifest. This treatment eventuallyachieved elimination of circulating microfilariac,control of adult worm activity and marked sub-jective improvement .

1000
Loa Loa-Felts, TalbottA review of the twelve-year history of this case
together with the course of events during threemonths of therapy make it evident that thechanges of physical and laboratory findings dur-ing treatment were related to the therapy em-ployed. In interpretation of these findings twoquestions present themselves . Was the transientclinical worsening of the patient due to drugtoxicity? Or was it related to the specific anti-parasitic action of these drugs in a patient withchronic loiasis, a condition in which patho-genesis is related to hypersensitivity of the hostas well as to parasitic invasion?
The clinical abnormalities observed were asfollows: severe emotional disturbance, abdomi-nal symptomatology, enlargement of the liver,Layalgia, arthralgia and joint swelling, angio-neurotic edema, electrocardiographic evidence ofcarditis, increased surface activity of adultworms, recurrence of Calabar swellings anddevelopment of pruritus and giant urticaria forthe first time in the patient's illness .
A survey of the abnormal laboratory findingsrevealed an increase in the leukocyte count,eosinophils, sedimentation rate, gamma globulinand blood urea nitrogen, also abnormal liverfunction tests and albuminuria . A markedlypositive complement-fixation test for filariasisdeveloped for the first time .
Some of the changes observed, such as theIeukocytosis, elevated sedimentation rate andvague abdominal symptomatology were so non-specific that their interpretation would be con-jectural . They served mainly to emphasize thepresence of organic disease in this patient inwhom the original subjective complaints out-weighed objective findings. Severe emotional dis-turbance and central nervous system involve-ment are known features in filariasis [46,47] . Theclinical and laboratory findings consistent withan acute anicteric hepatitis during hetrazantherapy are noteworthy. Pharmacologic studiesin dogs [14] gave no indication that hetrazanaffects liver function, renal function, the hemato-poetic system or the electrocardiogram . Clinicalstudies likewise have not suggested toxic effectson these organs. In the patient herein described,although elevation of blood urea nitrogen andacute hepatitis developed during the first week oftherapy when small doses of the drug wereadministered, later on during the regimen aneightfold dose of hetrazan was tolerated withoutanv observable undue reaction .
The mechanism of action of hetrazan in loiasis
is not completely understood [48-52] . This drugis not microfilaricidal in vitro. It may affect themicrofilariae as an opsonin, thereby facilitatingtheir phagocytosis [3,36] . As thenumberofmicro-filariae in the blood stream begins to decrease,rapid accumulation of dead and dying micro-filariae occurs in the liver with coincidental liverengorgement [3,5] . This may conceivably lead tothe development of abnormal liver functions. Itis of interest that, in the case presented, doses ofD.25 mg. of hetrazan per kg. of body weighteffected no discernible change . An increasedsingle dose of 0.5 mg./kg. apparently consti-tuted a minimally effective or "critical" level forthis patient, as it brought about a sharp drop incirculating microfilariae . This was rapidly fol-lowed by an exacerbation of all previous sub-jective complaints and the development of theacute objective illness described in the case re-port. Laboratory abnormalities reached theirpeak only two or three weeks after this exacerba-tion. This sequence of events, particularlywith the notable development of a positivecomplement-fixation test with accompanyingmarked eosinophilia, indicates that, in additionto the mechanical effect of accumulation ofmicrofilariae in the liver, antigen-antibodyreactions also contributed to the pathogenesis ofthe observed illness . This interpretation is inaccordance with the concept of other workers,namely that the clinical and laboratory changesduring hetrazan therapy are due in large part toreactions of a hypersensitized host to newlyliberated allergens [53,55] . In this case thestrongly positive complement-fixation test, whichslowly became negative with clinical improve-ment, is good evidence of the specificity of theallergic reaction, as this test is considered reliablewhen positive [25] .
The critical or minimally effective dose ofhetrazan for this patient did not suffice toeliminate the microfilariae. Capillary bloodstudies continued to be positive until the dosageof drug was increased about five weeks later to1 mg./kg. every six hours. The need for largedoses has been noted by others [13,27] . Once themicrofilariae disappeared from the blood streamthey never again became demonstrable by directsmear or by concentration technics during fol-low-up observation of three years . It can beassumed that some of the adult worms also wereaffected by hetrazan as their activity increasedat the critical dosage level with prompt andactive appearance in the cutaneous areas and
AMERICAN JOURNAL OF MEDICINE

local allergic reaction . But activity of adult loapersisted despite the relatively large doseseventually employed, consistent with previousreports [3,4,13,39] . Unfortunately no methods areavailable to allow quantitative estimation of theeffect of drugs on adult worms .
Suramin was administered in an attempt toachieve adult loa eradication . The most promi-nent events during suramin therapy weredevelopment of albuminuria, urticaria andmarked electrocardiographic abnormality. Tox-icity studies on suramin show primarily achronic, cumulative renal irritation [44,45] .In view of the marked hypersensitivity aspect inloiasis and in this particular patient one mayalso postulate that the albuminuria is, at least inpart, the result of host renal reaction to liberatedantigen, or possibly to altered parasite protein .The angioneurotic edema and joint swelling ob-served during suramin therapy also may beinterpreted as hypersensitivity reactions . Thedelayed host reaction to the drug correlates wellwith its slow action on adult loa [56] . In con-trast, the cutaneous reactions of this patientoccurred very soon after administration of thedrug. This early allergic manifestation wouldsuggest that the drug also has some immediateeffect on the parasite .
The electrocardiographic abnormalities notedduring hetrazan and more prominently duringand after suramin therapy were of particularinterest . These changes during hetrazan therapywere slight and resolved while hetrazan was stillbeing administered . In view of this it would bedifficult to attribute them to drug toxicity .There are also no reports in the literature thatelectrocardiographic changes are caused bysuramin which has been used extensively inAfrican trypanosomiasis . Therefore it seemsquite unlikely that the cardiac involvementnoted in this case was related to drug toxicity .Electrolyte shift was considered as a possiblecause of the electrocardiographic changes notedin this patient, but was not demonstrable .
Localization of adult loa in the heart hasbeen reported [6] . Electrocardiographic changesmight therefore result from the presence of adultworms in the myocardium. Such changes werenot present before therapy . They occurred inthis patient simultaneously with increased adultworm activity with associated visible allergicphenomena. They were more pronounced andprotracted during suramin therapy . This is feltto be significant as suramin has more effect onJUNE, 1957
Loa Loa-Felts, Talbott 1001
adult loa than hetrazan . It is conceivable thatincreased activity of adult worms and dead anddisintegrating loa localized in the myocardiumcould incite a local allergic reaction and that theassociated inflammation could persist for severalweeks [57] . It is postulated that in this case ofloiasis the electrocardiographic changes were areflection of an allergic carditis, brought aboutby destruction of the parasite by the drugs em-ployed . It has been reported by Mikulichick [58]that in rabbits exposed to antigen-antibodyreactions almost 100 per cent of the hearts exam-ined showed anaphylactic "cell injury." Theoccurrence of an allergic carditis has been con-sidered in another parasitic disease, trichinosis,where local parasitization of the heart as well asabnormal electrocardiograms without apparentparasitization have been noted [5.9-S1] . To ourknowledge allergic carditis as an expression of anantigen-antibody reaction in loiasis has not beenpreviously reported . In this patient the in-tensity of the cardiac reaction was not severeenough to cause clinical signs of cardiac em-barrassment . Follow-up studies have shown thatelectrocardiographic changes were reversible inthis case .
It has been stated in the case report that thispatient was initially treated with relatively smalldoses of hetrazan and that increase in dosage wasaccomplished only gradually. Such gradual andcautious medication appears advisable in infec-tious diseases in which the host may have be-come markedly hypersensitive to the infectiousagent or its products . Frequently a certainequilibrium appears to develop between host andparasite . Disturbance of this balance may occurduring specific therapy directed against theinciting antigen. Initial large doses of the specifictherapeutic agent may then call forth a markedantigen-antibody reaction which manifests itselfas severe clinical illness . In spite of the initialsmall doses employed, this patient experienced amoderately severe exacerbation of her illnessduring therapy . With clinical improvementlarger doses of hetrazan were eventually welltolerated . It is impossible to state whether or notthis patient would have tolerated larger doses onprotracted therapy with suramin . However therisk of possibly prolonging or worsening thecourse of the allergic, therapeutically inducedcarditis did not appear justified .
This patient has shown no evidence of a returnof subjective symptoms or of objective evidenceof parasite activity during the three years since

1002
Loa Loa--Felts, Talbolltermination of therapy. We feel justified inregarding her as being in a state of therapeuticremission which, it is to he hoped, will prove tobe permanent .
SUMMARY
1 . A case report is presented of a patientheavily infected with L . loa. The infection wasknown to have exceeded twelve years in duration .
2 . The patient was treated with hetrazan andsuramin . A therapeutic remission was obtained .
3 . The host reactions to destruction of micro-filariae by hetrazan and to destruction of adultloa by suramin are described . These consisted ofthe development of a positive complement-fixa-tion test for filariasis and frank allergic cutaneous
manifestations . In addition there were gastro-intestinal and central nervous system manifesta-tions. Acute anicteric hepatitis and myocarditisalso occurred .
4. The possible mechanism of these reactionsis discussed in terms of an altered host-parasiterelationship .
REFERENCES
1 . BELDING, D . L. Textbook of Clinical Parasitology,2nd ed. New York, 1952. Appleton-Century .Crofts, Inc .
2. LANE, C. Bancroftian filariasis . Tr . Roy . Soc. Trap .Med. & Hyg., 41 : 717, 1948 .
3 . HAWKING, F . Some recent work on filariasis . Tr. Roy .Soc . Trop . Med. & Hyg ., 44 : 153, 1950 .
4. SCHNEIDER, J . Etat actuel de la therapeutique de lafilariose a F. loa par le 1-diethyl-carbamyl-4-inethylpipcrazine . Acta Trap ., 8 : 345, 1951 .
5 . WOODRUFF, A. W. Destruction of microlilariae of Loaloa in the liver in loiasis treated with banoside .Tr. Roy. Soc. Trop. Med. & Hyg ., 44: 4, 1951 .
6. STRONG, R. P. Stitt's Diagnosis, Prevention andTreatment of Tropical Diseases, 6th ed . chap . 46 .Philadelphia, 1942 . Blakiston Co .
7. MACKIE, T. T . et al . A Manual of Tropical Medicine,2nd ed . Philadelphia, 1954. W. B. Saunders Co .
S. MANSoN-BANK, P . H . Tropical Diseases, 13th ed .London, 1953. Cassell & Co ., Ltd .
9. NEVEU-LEMARIE, M. Traite d'Helminthologie Medi-cale et V€t6rinaire . Paris, 1936 . Vigor Fr6res.
10. BRUMPT, L. D. Precis de Parasitologie. Paris, 1949 .11 . CRAIG, C . F. and FAUST, E . C . Clinical Parasitology .
Philadelphia, 1951 . Lea & Febiger .12. SHATTUCK, G . C . Diseases of the Tropics . New York,
1951. Appleton-Century-Crofts, Inc.13. WILSON, T. Hetrazan in the treatment of filariasis
due to Wuehereria malayi . Tr . Roy. Soc . Trop .Med. & Hyg ., 44: 49, 1950 .
14. HARNEn, B. K . et al. Studies on chemotherapy offilariasis . J. Lab. & Clin . Med ., 33: 216, 1948 .
15 . BURCH, T . A . Experimental therapy of onchocerciasiswith suramin and hetrazan . Rol. Ofic. son . panam,,2B : 233, 1949 .
16. RIFKIN, H . and EBERIIARD, T. P . Pulmonary filaria-sis. Ann . Int . Med., 25: 324, 1946 .
17. BROWN, '1'. MCP., STIFLER, W. C. and BETHEA,W. R . Early filariasis . Bull, Johns Hopkins Hasp ., 78 :126, 1946 .
18. HUNTINGTON, R . W., ,JR ., EIouoLn, S . and SCOTT,O. K. Allergic filarial lymphangitis (mumu) inAmerican troops in the Samoan area in World WarH . Am. J. Trap . Med., 30: 873, 1950 .
19. FAIRLEY, N . H. Serological and intradermal tests infilariasis. Tr. Roy . .Soc . Trop . Med. & Hyg ., 24 : 635,1931 ; 25 : 220, 1932 .
20. Dusols, A. and VAN DEN BERGHE, L . Diseases of theWarm Climates. New York, 1948 . Grune & Strat-ton .
21 . JORDAN, P. Observations on W . bancrofti and A.perstans in Tanganyika. Tr . Roy . Soc . Trop . Med. &Hyg ., 49: 460, 1955 .
22. RODIIAIN, J . Pathogenesis of filariasis . Ada. Trop., 10 ;194, 1953.
23. GORDON, R . M., KERSHAW, W . E ., CREWE, W. andOLDRovD, H. The problem of Loiasis in WestAfrica. Tr. Roy. .Soc . Trap. Med. & Hyg ., 44: 11,1950 .
24. KUNKEL, H. C. Estimation of alterations of serumgamma globulin by a turbidimetric technique.Broc . Soc. Exper . Biol. & Med ., 66 : 217, 1947 .
25. Bozteevten, J. and HOTTER, A. M. Intradermal andserological tests with Dirofilaria immitis antigen incases of human filariasis . Am . J. Trop . Med ., 24 :203, 1944 .
26. KUATT, J . Method for making microfilarial surveyson days blood . Tr . Roy. Sot . Trap . Med. & Hyg., 33 :191, 1939 .
27. BEYE, H . K . et al. Preliminary observations on theprevalence, clinical manifestations, and controlof filariasis in the Society Islands . Am . .1. Trop.Med., 1 : 637, 1952 .
28. KENNEY, M. and HEWITT, R. The treatment ofbancroftian filariasis with hetrazan in BritishGuiana . Am . J. Trap . Med ., 29: 89, 1949 .
29. SANTIAGO-STEvENSON, D ., OLIVER-GONzAuEz, J. andHEWITT, R . I . The treatment of filariasis bancroftiwith hetrazan . Ann. New York Acad . Sc ., 50 : 161,1948 .
30. SHOOKOFF, H . G. and Dw0RK, K. G. Treatment ofLoa Ina infections with hetrazan . Am. J. Trap .Med., 29: 589, 1949 .
31 . STEFANOPOULO, G. J. and SCHNEIDER, J. Essais detraitement de la filariose it F . loa par la 1-di€thyl-carbamyl 4-methylpiperazine . Comet . rend . Soc . debiol ., 142 : 930, 1948 .
32. HEWITT, R. Mass therapy with hetrazan as a controlmeasure for bancroftian filariasis on St . Croix .Nature, London, 164: 1135, 1949.
33. MCGRECOR, I., HAWKING, F . and SMITH, D . Con-trol of filariasis with hetrazan, Brit M. J ., 4790 :908, 1952-
34 . VON SCHOWINCEN, R . S. Further experiences in thetreatment of filariasis with hetrazan . Acta . Trap .,9 : 270, 1952 .
35. STONES, P. B. Successful treatment of Loiasis withhetrazan in low dosage. West Africa M. J., 1 : 4,1952 .
36. HEWITT, R. Experimental chemotherapy of filariasisin . J . Lab . & Clin . Med., 32: 1314, 1947 .
AMERICAN JOURNAL OF MEDICINE

37 . WANSON, M. L'hetrazan dans la p6riode d'invasionde I'onchocercosc . Sac . beige de Med. Trop ., 29 : 85,1949 .
38. WANSON, M . Essai de traitcment curatif de la filariosea Loa-loa et de la filariose aperiodique par letderives de la piperazine. Soc . beige de rued- trop .,29 : 73, 1949 .
39 . OTTO, G. F., JACHOWSKI, L . A ., JR. and WHARTON,J . D. Studies on chemotherapy against nonperiodicform of W. bancrofti. Am. J. Trop . Mrd., 2 : 495,1953 .
40. WANSON, M ., Contribution a l'etude de I'oochocer-cose africaine humaine_ Soc. beige de med . trop ., 30 :667, 1950 .
41 . MADELL, S. H. and SPRINCARN, C . L . Filariasis due toLoa Ina . Am. J. Med., 15 : 272, 1953 .
42. AsIIBURN, L . L., BURGH, T. A. and BRADY, F . J . Path-ologic effects of suramin, hetrazan, and arsenamideon adult O . volvulus . Biel . Ofic . San . panarm, 28 :1107, 1949 .
43. BuRc's, T . A. and ASHBURN, L . L. Experimentaltherapy of onchocerciasis with suramin andhetrazan . Am . .1. Trap . Med ., 31 : 617, 1951 .
44. FINDLAY, G . M. Recent Advances in Chemotherapy,3rd cd ., p . 404 . London, 1950 . Churchill.
45. Swans, A. The persistence in the blood stream ofsome compounds related to suramin . Biaehem . J.,42 : 109, 1948 .
46. JANSSENS, P. G. R6marques au sujet de la possibilitede manifestations nerveuses on psychiques causeespar Les filarioses . Soc . beige de med . trop ., 32 : 229,1952 .
47. KIVTs, M . Quatre cas d'encCphalite mortelle aver in-vasion du liquide chphalo-rachidien par micro-filaria loa . Soc . beige de med . trap ., 32 : 235, 1952 .
48 . LA GRANGE . E. Essais de traitcment des filari~ a
JUNE, 1957
Loa Loa-Fells, Talbott 1003
Loa-loa ct O . volvulus par le diethylcarhamazinechloride . Sac . beige de Med . Trap ., 29 : 19, 1949 .
49. HECKENROTH, F., BECUWE, R., MAYAN, L. andLEROUX, G. Filarioses (Loa et perstans) et derivesde la piperazine . Bull. Soc, de path . exot ., 43 : 354,1950 .
50. BONNIN, H . and MORETTS, C . F . Preuves clinique etbiopsique de Faction lethale d'un derive de lapiperazine sin' la filaire Loa Loa adulte . Bull . Sum .de path . exot ., 43 : 279, 1950 .
51 . GARIN, C . and GARIS, J . P . Sur le traitcment de lafilariosc a F. loo par lc notezinc. .1 . de m id . de Lyon,32 : 13, 1951 .
52. MURGATROYD, F. and WOODRUFF, A. W. Loiasistreated with hetrazan . Lancet, 2 : 147, 1949 .
53 . TALIAFERRO, W. H. Inhibition of reproduction ofparasites by immune factors . Bart . Rec ., 12 : 1, 1948 .
54. CHANDLER, A . C . Production of typical calabar swell-ings in Loa patient by injection of dirolilariaantigen . Am . J. Trap . aped ., 10 : 345, 1930 .
55 . FULLEBORN, F, fiber die Lage von Mikrofilaria Ion(diurna) im Trokkcnpraparat. Arch . f. Sckiffs . u .Trap. Hyg ., 18 : 232, 1914 .
56 . CUI.BERTSON, J. T. Experimental chemotherapy offilariasis hancrofti . Tr . Roy . Sac. Trap . Med. & Hyg .,41 : 18, 1947 .
57 . LAWRENCE, H. S. Delayed type of allergic inflam-matory response . Am . .1. Med., 20 : 428, 1956 .
58 . MIKULscmec, G. EKG changes in experimentalanaphylactic reactions . .1. Allergy, 22 : 249, 1951 .
59 . BELCHER, C . H. EKG findings in 44 cases of mildtrichinosis . Am. heart J ., 16 : 219, 1938 .
60 . GOULD, S . E. Trichinosis . Springfield, Ill ., 1945 .Charles C Thomas .
61 . REICH, N . E. Uncommon Diseases of the Heart .Springfield, III ., 1954 . Charles C Thomas .
Recommended