American Journal of Medical Genetics 29:95-106 (1988)
A New Acro-Cranio-Facial Dysostosis Syndrome in Sisters Paige Kaplan, Henri Plauchu, Naomi Fitch, and Sigrid Jequier
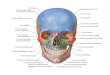
Division of Medical Genetics and Research Instifute, Montreal Children’s Hospital (P.K., H. P.); Lady Davis Institute, Sir Mortimer B. Davis Jewish General Hospital, (N, F.): and Department of Radiology, Montreal Children’s Hospital (S. J.), Montreal, Quebec, Canada
Two sisters born to consanguineous parents had a syndrome of short stature, acrocephaly, hypertelorism, proptosis, ptosis, down-slanting palpebral fissures, high nose bridge and anteverted nares, short philtrum, cleft palate, micrognathia, abnormal external ears, preauricular pits, sensorineural and conductive deafness, proximally placed first toes and digitalized thumbs, bulbous digits, metatarsus adductus, and pectus excavatum.
Radiological abnormalities included craniosynostosis, increased mandibular angle and antegonial notching of mandible; hypoplastic first metacarpals and metatarsals; hypoplastic distal phalanges; partial duplication of the distal phalanx of the thumb; malformed malleus and incus; tall lumbar vertebrae, increased interpedicular distance, and posterior scalloping; flared iliac wings, narrow supraacetabular regions, acetabular “dysplasia,” and coxa valga.
Autosomal recessive inheritance is suggested.
Key words acro-cranio-facial syndrome, oto-palato-digital syndrome, autosomal recessive inheritance, ptosis, proptosis, craniosynostosis, cleft palate, deafness, digit abnormalities
INTRODUCTION
Two oto-palato-digital syndromes, OPD I, [Dudding et al, 1967; Langer, 1967; Taybi, 19621 and OPD I1 [Andre et al, 1981; Fitch et al, 1976, 1983; Kozlowski et al, 1977; Brewster et al, 19851 and several autosomal recessive, autosomal dominant, and sporadic acro-facial-dysostosis syndromes [Lewin and Opitz, 1986; Reynolds et al, 19861 have been delineated. These syndromes are characterized by deafness (sometimes
Received for publication February 13, 1987; revision received June 11, 1987
Paige Kaplan’s current address is Children’s Hospital of Philadelphia, 34th and Civic Center Blvd., Philadelphia, PA 19104.
This is publication 87013 from the McGill University-Montreal Children’s Hospital Research Institute.
Address reprint requests to Dr. Paige Kaplan, Montreal Children’s Hospital, 2300 Tupper Street, Montreal, Quebec, Canada H3H IP3.
0 1988 Alan R. Liss, Inc.

96 Kaplan et al.
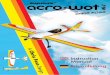
Fig. 1 . proptosis, severe ptosis, micrognathia, abnormal auricle, and pre-auricular pit.
Facial profiles: a) patient 1 , 25 wk gestation; b) patient 2, birth. Note flat forehead, beaked nose,
associated with bony abnormalities of the middle ear), cleft palate, micrognathia, telecanthus, variable abnormalities of limbs, and occasionally, short stature and mental retardation. However, there appears to be phenotypic and radiologic variability within these syndromes.
We describe two sisters with cranio-facial and distal limb abnormalities whose condition resembles the acro-facial dysostosis and OPD syndromes in some respects but is sufficiently different to be considered unique. Autosomal recessive inheritance is suggested in this family because the parents are consanguineous and unaffected.
CLINICAL REPORTS Patient 1 (see Fig. la)
A girl was born to a primigravid 22-yr-old mother and 30-yr-old father, who were first cousins, of Sephardic Jewish origin and of normal intelligence. The pregnancy terminated after 25 wk gestation because of abruptio placenta. Weight was 670 gm and length 32 cm. She had hypertelorism (inner canthal distance 1.2 cm: outer canthal distance 4.5 cm), broad nose with high bridge and small nares, cleft palate, three maxillary teeth, micrognathia, low-set ears, a preauricular pit, slightly webbed neck, proximally placed moderately rotated halluces, relatively long 2nd toe (see Fig. 4a), short broad tips of thumbs and fingers with small nails (but no obvious syndactyly), atrial and ventricular septa1 defect, and transposition of the great vessels. She died 26 hr after birth.
Radiologic Findings
The infant had hypertelorism, 11 pairs of ribs, wide interpedicular distance of lumbar spine, and small iliac wings, The thumbs, index, and fifth fingers had short metacarpals and distal phalanges (see Fig. 6a); the fingers showed ulnar deviation. The large toes had very short first metatarsals and distal phalanges; the other toes had immature middle and distal phalanges.

Acro-Cranio-Facial Dysostosis Syndrome 97
Fig. 2. Face, patient 2: a) birth, b) 3% yr.
Patient 2 J.D. (M.C.H. 736984)
A girl was born 2 yr later, after a 40-wk gestation. An obstetrical ultrasound examination in midtrimester appeared normal. Delivery was done by Cesarean section because of persistent breech position. The Apgar ratings were 7 at 1 and 5 min. Multiple cranio-facio-digital abnormalities were noted at birth (Figs. lb, 2a, and see 4b): large anterior fontanel, wide sagittal sutures; low-set ears with prominent crus of antihelix and preauricular pits; beaked nose; telecanthus and proptosis; hirsute forehead; cleft palate, micrognathia; broad distal phalanges of the thumbs; fourth fingers as long as the third; rocker-bottom heels and proximally placed, rotated halluces.
Birth weight was 2,540 gm (3rd centile); length was 48 cm (3rd centile) and occipitofrontal head circumference (OFC) was 33 cm (25th centile). By age 2 mo all three growth parameters were below the 3rd centile and have remained below it; at age 3 yr the height age was 21 mo (83 cm), OFC was average for 11 mo (45 cm), and weight was average for 12 mo. The posterior fontanel closed after 8 mo and the large anterior fontanel after 2 yr.
Shortly after birth, J.D. developed upper respiratory obstruction and cor pulmonale which were thought to be due to glossoptosis (as a consequence of the micrognathia and cleft palate) and choanal stenosis. Her respiratory status improved after the insertion of nasal tubes. After the removal of these, there were several periods of upper respiratory tract obstruction. At 18 mo she developed chronic nocturnal respiratory obstruction. With direct laryngoscopy and bronchoscopy examinations no anatomical lesions were found and the obstruction was attributed to neuromuscular incoordination and inability to clear nasopharyngeal secretions adequately. A tracheostomy was done and has remained in place. The nasolacrimal duct was found to have bony obstruction.
In the neonatal period there was a grade II/VI heart murmur, but echocardiography and electrocardiogram were normal at that time.
A congenital paraesophageal hernia was repaired surgically at 6 mo. Gastro- esophageal reflux, demonstrated radiologically, caused recurrent vomiting and possible

98 Kaplanet al.
Fig. 3. Hands: patient 2, showing rotated position and bulbous tip of thumb.
pulmonary aspiration. This necessitated a feeding gastrostomy; episodic vomiting con- tinued in spite of the gastrostomy. Oral feeding was reintroduced at age 3 yr.
Nonprogressive sensorineural and conductive deafness was demonstrated by age 8 mo.
J.D. had global developmental delay particularly in motor function and language. Independent walking was achieved at 3 yr at which time she had begun to say a few words.
Examination
At 3 yr (Fig 2b) she was an alert girl with curly brown hair, a flat and high forehead with a horizontal groove above the eyebrows, telecanthus (inner canthal distance 3.4 cm, outer canthal distance 6.8 cm.) with downslanting palpebral fissures, and marked proptosis and ptosis bilaterally. The left optic disc was slightly pale and there was myopia. The nose bridge was moderately high and the nares anteverted, giving the nose a beaked appearance. The philtrum was short, lips thick, and tongue and gums normal. The palate had a narrow midline cleft and the remainder of the palate appeared furrowed. The chin was small and the neck short. The right ear was low set, the superior helices of the pinnae were overturned and thick, the external canals narrow, and there was a bilateral preauricular pit. There was pectus excavatum and small inverted nipples.
The thumbs appeared long with two skin creases but only one interphalangeal joint (Fig. 3). All the digits had bulbous tips. The fingernails were flat and wide. There was bilateral metatarsus adductus and both large toes were proximally placed, thin and curved (Fig. 4c). The toes were curved towards the hallux with deep skin creases, especially distally. There were six arch patterns (on the lst, 3rd, and 4th fingertips).
Chromosomes (G banding, 300 bands) were normal (46, XX).

Acro-Cranio-Facial Dysostosis Syndrome 99
Fig. 4. Feet: a) patient 1, b) patient 2, birth, c) patient 2,31/2 yr.
Radiologic Findings
Skull (Fig. 5). At 3'/2 yr, there was acrocephaly due to coronal synostosis. All other sutures of the cranial vault were narrow but open. There were prominent brain markings in the posterior parietal and occipital areas. There was a steep anterior fossa, mild hypertelorism, opacified paranasal sinuses and mastoids, a prominent galea, and the mandibular angle was increased, with a notch in the body of the mandible underlying the tooth bud of the first molar (antegonial notching). The sphenoid sinuses were normal, and the ethmoid and maxillary sinuses opacified due to chronic nasal congestion.
Axial skeleton. Cervical and upper thoracic spine were normal. The lumbar spine showed widening of the interpedicular distance, increased height of the vertebral bodies, posterior scalloping, as well as spina bifida occulta of LA-5 and the sacrum.
Pelvis. There was flaring of the iliac wings, narrow supra-acetabular regions, small and steep acetabulae, and bilateral coxa valga.
Limbs. There was mild genu valgum. The long tubular bones showed no major abnormality. There was marked shortness of the distal phalanges of the hands (Figs. 6b, c), and to a lesser degree, of the metacarpals. The distal phalanx of the thumb was short

100 Kaplan et al.
Fig. 5. suture, steep and high anterior fossa, and increased antegonial notch of the mandible.
a) Skull AP and b) lateral: patient 2, 3% yr, showing mild hypertelorism, craniosynostosis of the coronal

Acro-Cranio-Facial Dysostosis Syndrome 101
Fig. 6. Hand: a) patient 1, b) patient 2, birth, c) patient 2, 3% yr.

102 Kaplan et al.
4 r
L 0 z
- 2 E 2 c
-8L- - - IIlil 1 2 3 4 5 1 2 3 4 5 2 3 4 5 1 2 3 4 5 Metacarpal Proximal Middle Distal
Fig. 7. different ages.
Hand pattern profile: patient 2 at birth (---) and 3 yr (-) showing unusual patterns and variation at
and deformed, with partial duplication of the distal phalanx. Carpal bones were normal. Bone age corresponded to chronological age. The metacarpophalangeal profile (Fig. 7) was abnormal: it had changed in configuration since birth due to reduced growth of the metacarpals and some proximal phalanges.
Feet (Figs. 8a, b). Both feet showed severe hypoplasia of the first ray with a very small abnormally shaped triangular first metatarsal bilaterally. The first cuneiforms were more distally located than usual, lateral to the base of the second metatarsals. There was metatarsus adductus and severe hypoplasia of the distal phalanges.
Special Investigation
Ultrasound studies of the brain in early infancy and a CT scan of the brain were normal.
Tomography of the middle and inner ears at 2"/12 yr, showed a normal cochlea bilaterally but a malformed malleus and incus on the right with poor visualization of the incus and stapes on the left, probably because of underdevelopment.
Auditory evoked responses have shown moderately severe nonprogressive bilateral hearing loss since age 8 mo. Normal interwave latencies suggested normal brain stem conduction.
Renal ultrasonography showed mild parenchymal scarring in the right kidney. Voiding cystourethrography demonstrated bilateral grade I1 vesico-ureteric reflux.
Family History
The mother has had two pregnancies. She had a slightly high palate, slight pseudo-ptosis but normal elevation of the left upper lid, subtle facial asymmetry due to flattening of the left supraorbital ridge, and preauricular pits. Her height was 162.5 cm, OFC was 56.5 cm (75th centile), and her cephalic index was normal. There were no palpable cranial defects. Hands and feet were normal. (One of the mother's brothers was reported to have some facial asymmetry; her sister and three brothers had preauricular pits). The father's OFC was 57.3 cm (75th centile) and his cephalic index was normal. The physical examination of both parents were otherwise normal. In both parents, the skull, hand and foot roentgenograms, including metacarpophalangeal profiles, were normal.

Acro-Cranio-Facial Dysostosis Syndrome 103
Fig. 8. Feet, patient 2: a) birth, b) 3% yr.
DISCUSSION
The two sisters described here have a syndrome easily recognizable by 25 wk gestation. It has many similarities to the autosomal dominant acrofacial dysostosis reported by Reynolds et a1 [1986]: affected individuals in three generations had craniofacial abnormalities that included prominent forehead, ptosis, downslanting palpe- bra1 fissures, malar and zygomatic-arch hypoplasia, micrognathia, mild congenital mixed hearing loss, duplication of the thumb in one child, and radiologic evidence of metacarpal “hypoplasia.” One major difference in our patient was the Occurence of craniosynostosis. In addition the patients of Reynolds et a1 [ 19861 did not have limb abnormalities as severe as our patient’s; their proximal phalanges were hypoplastic whereas in our patients the shortening affected the distal phalanges. Furthermore, although our proposita’s mother had slight apparent ptosis and asymmetry of the supraorbital ridge there was no other physical nor any radiological signs to suggest that she had partial manifestation of an acro-cranio-facial syndrome.
In the autosomal recessive acro-facial dysostosis syndrome of GenCe- Wiedemann [Lewin and Opitz, 19861 there may be similar craniofacial anomalies with hypoplastic supraorbital ridges, prominent eyes, micrognathia, small ears, cleft palate, congenital heart disease, and many arches on the fingertips (Table 1). However, the limb anomalies in our patients are different because they do not have postaxial hypoplasia or polydactyly; furthermore, they do not have abnormalities of the middle phalanges but of distal phalanges and metacarpals. Our patients do not have abnormalities of vertebral segmenta- tion, extra nipples, or upslanting eyes.
The syndrome affecting our patients has many similarities to the oto-palato-digital I and I1 syndromes: external and bony ear anomalies, hypertelorism or telecanthus, antimongoloid slant of palpebral fissures, cleft palate and micrognathia, pectus excava- tum, proximally placed and abnormally shaped first digits on hands and feet, with short

104 Kaplan et al.
TABLE I. Clinical and Radiological Changes: Comparison of Patients in This Report with OPD I and U Syndromes, and AFD Syndrome*
Patient I Patient 2 OPD I OPD I1 AFD
Clinical OFC <3rd centile Anterior fontanelle large Forehead:
flat prominent
Telecanthus Antimongoloid slant of fissures Proptosis and ptasis Nasolacrimal duct stenosis Choanal stenosis External ears malformed Preauricular pits Nose bridge:
high flat
Cleft palate Micrognathia Deafness: sensorineural 0 Thumbs:
long short broad tip
Fingers: broad tips First toe:
long proximally placed rotated
Second toe: long All toes: broad tips Nails: short, broad Pectus excavatum Cardiac malformations Congenital Para-esophageal hernia Developmental delay
Craniosynostosis Carpals-Tarsals
Radiological
absent/abnormal fused
short fused
Phalanges proximal short middle short distal short
Metacarpals-Metatarsals
+ + ?+
+ + + - + +
+ - + + + + + + + + + -
- -
+t -
- - -
+ +
+ + + - + + + + + + + + -
+ + + + - + + + + + + + + + - + +
coronal + - -
++ - - - -
++
-
+ + + + + - + (ptosis) -
-
++ +a: - +
+ +ae + += + + w 4 ) + +(1/4)
*AFD, acrofacial dysostosis [Reynolds et al, 19861; [ + I , present; [-I, absent; [ 1, no data; [a:], thumbs only; [ O ] , * conductive.

Acro-Cranio-Facial Dysostosis Syndrome 105
distal phalanges, clinodactyly of many digits with broad termini, and (in the living child) conductive and neural hearing loss, short stature, and psychomotor retardation.
However, there are several differences phenotypically, radiologically, and in mode of inheritance. The condition reported here differs from the OPD I and I1 syndromes (Table I) with respect to microcephaly, acrocephaly with flat and high forehead and coronal craniosynostosis, marked proptosis and ptosis, high nose bridge, choanal stenosis, naso- lacrimal duct stenosis, and hiatus hernia. The first metatarsals and metacarpals are short and there is partial duplication of distal phalanges of the thumbs. Neuromuscular incoordination has been implicated in one girl as an additional factor causing severe respiratory obstructive disease.
The metacarphophalangeal profile of patient 2 (Fig. 7) differed from that seen in OPD I (except for the first distal phalanx) [Gall et al, 19721, OPD I1 [Fitch et al, 19831, and Saethre-Chotzen and Pfeiffer syndromes [Escobar and Bixler, 19771.
In the classical OPD (type I) males are affected in most cases, resulting in the hypothesis of X-linked recessive transmission. Autosomal dominant inheritance has been considered, although male-to-male transmission has been suggested in one family only [Salinas et al, 19791. However, it is not certain whether the patients in that family had OPD I syndrome. Female heterozygotes have not manifested the complete syndrome [Gall et al, 19721. Affected males differ from our patients in having frontal and occipital prominence, flat and broad nasal bridge, fusions of tarsal and metatarsal bones especially cuneiforms, abnormally shaped carpals, and extra ossification centers.
The OPD I1 syndrome appears to be X-linked recessive [AndrC et al, 198 1; Fitch et al, 1976, 1983; Kozlowski et al, 1977; Brewster et al, 19851. Affected patients have several anomalies not seen in our patients, such as prominent forehead, broad nose, flat nasal bridge, midfacial hypoplasia, and small downturned mouths: camptomelia and campto- dactyly seem to be distinctive anomalies of OPD 11. The fibulae may be absent. The fourth metatarsal is hypoplastic and the fifth nonossified. The middle phalanges of the 2nd and 4th fingers are hypoplastic.
OPD syndromes affecting girls have been reported several times [Gall et al, 1972; Plenier et al, 1983; Salinas et al, 1979; Sirvent Gomez et al, 19841. Some are heterozygotes for OPD I. None of them are identical to or as severely affected as the subjects of this report; although the mother and daughter (cases 1 and 2) and another unrelated girl (case 6 ) reported by Salinas et a1 [ 19791 have many similar clinical anomalies, the “gestalt” is different. An important difference is the distal placement of thumbs in the patients of Salinas et al [ 19791. Radiologically there are also differences: the patients of Salinas et a1 [ 19791 have fusion or hypoplasia of carpal bones, normal distal phalanges, curved tibias, and delayed bone age. They do not have craniosynostosis, ptosis, proptosis, or microgna- thia.
The condition of the sisters in this report also show some similarities to the acrocephalosyndactyly syndromes of Saethre-Chotzen (acrocephaly, ptosis, absence of 1 st metatarsus, cleft palate) Pfeiffer (short thumbs and great toes), and Noack (partial duplication of distal phalanges of great toes, acrocephaly). All of these syndromes are autosomal dominant traits. However, in our patients there was no polydactyly or syndactyly; radiologically the metacarpophalangeal pattern profile in the proposita was very different to that in Saethre-Chotzen and Pfeiffer [Escobar and Bixler, 19771. The metacarpals were shorter, only the 3rd proximal phalanges were short, the middle phalanges normal, and the distal phalanges very short.

106 Kaplan et al.
The most likely cause of the syndrome in this consanguineous family is homozygos- ity for an autosomal recessive gene.
ACKNOWLEDGMENTS
We thank the family for their cooperation, Dr. John M. Graham Jr. and Dr. K. Kozlowski for advice, Dr. John M. Opitz and the reviewers for valuable criticism, and Mme. Lise Vertefeuille, and Ms. Marie-France Williams for preparing the manuscript.
REFERENCES
AndrC M, Vigneron J, Didier F (1981): Abnormal facies, cleft palate, and generalized dysostosis: A lethal
Brewster TG, Lachman RS, Kushner DC, Holmes LB, Isler RJ, Rimoin DL (1985): Oto-palato-digital
Dudding B, Gorlin RL, Langer LO (1967): The otc-palato-digital syndrome. Am J Dis Child I13:21&221. Embar V, Bixler D (1977): The acrocephalosyndactyly syndromes: A metacarpophalangeal pattern profile
analysis. Clin Genet 11:295-305. Fitch N, JQuier S, Papageorgiou A (1976): A familial syndrome of cranial, facial, oral and limb anomalies. Clin
Genet 10:226-231. Fitch N, JQuier S, Gorlin R (1983): The otepalato-digital syndrome, proposed Type 11. Am J Med Genet
15:655-664. Gall JC Jr, Stern AM, Poznanski AK, Garn SM, Weinstein ED, Hayward JR (1972): Oto-palato-digital
syndrome: Comparison of clinical and radiographic manifestations in males and females. Am J Hum Genet 24:2&36.
Kozlowski K, Turner G, Scougall J, Harrington J (1977): Oto-palato-digital syndrome with severe X-ray changes in two half brothers. Pediatr Radio1 6:97-102.
Langer L (1967): The roentgenographic features of the otc-palato-digital (OPD) syndrome. Am J Roentgen
Lewin SO, Opitz JM (1986): Fibular a/hypoplasia: Review and documentation of the fibular developmental field. Am J Med Genet Suppl2:215-238.
Plenier V, Delaire J, David A, Cohen JY (1983): Le syndrome otc-palatedigital. A propos de trois cas fhinins. Rev Stomatol Chir Maxillofac 84322-329.
Reynolds JF, Webb MJ, Opitz JM (1986): A new autosomal dominant acrofacial dysostosis syndrome. Am J Med Genet Suppl2143-150.
Salinas CF, Jorgenson RJ, Lorenzo RL (1979): Variable expression in otopalatodigital syndrome; cleft palate in female. In ODonnell JJ, Hall BD (eds): “Penetrance and Variability in Malformation Syndromes.” New York: Alan R. Liss, Inc., for the National Foundation-March of Dimes. BD:OAS XV (5B):329-345.
Sirvent Gomez J, Rodriguez Valcarcel G, Alfayate Miguelez S, Pombo Felipe F (1984): Sindrome otc- palato-digital. Aportacion de un caso en el sex0 femenino. Ann ESP Pediatr 20905-910.
Taybi H (1962): Generalized skeletal dysplasia with multiple anomalies. Am J Roentgen 88:450-457.
X-linked syndrome. J Pediatr 98:747-752.
syndrome, Type 11: An X-linked skeletal dysplasia. Am J Med Genet 20249-254.
100:63-70.
Edited by John M. Opitz and James F. Reynolds
Recommended