Jessica Anderson2nd Year OVCMT Student
A Case Study:
The Effectiveness of Massage Therapy in reducing the symptoms of Thoracic Outlet Syndrome in a person presenting with Military
Posture.
�1
Table of Contents:
Introduction………………………………………………3
Case History……………………………………………..7
Assessment……………………………………………...8
Treatment Plan………………………………………….9
Outcomes……………………………………………….12
Discussion/Conclusion………………………………..16
References……………………………………………..17
Table 1…………………………………………………..18
Table 2/ Graph 1……………………………………….19
Table 3…………………………………………………..20
�2
Introduction
Thoracic Outlet Syndrome (TOS) is a common condition known to have an effect on many peoples
lives. TOS is a blanket term to describe a few conditions occurring at the thoracic outlet, which is
located at the lateral neck between the clavicle and first rib. Passing through this space is the
Brachial Plexus composed of nerve roots C5-T1 , which gives sensory and motor function to the entire
upper limb. Also to pass is the subclavian artery, and subclavian vein. These structures travel
together as the "neurovascular bundle," and can be compressed between the anterior and middle
scalene muscles, between the coracoid and pectorals minor muscle, or between the clavicle and first
rib. Systemic or metabolic disorders such as diabetes and rheumatoid arthritis can also compromise
the space of the thoracic outlet with varying degrees of inflammation and swelling. Any type of trauma
to the neck or shoulder girdle, for example, whiplash, can leave subsequent scarring and inflammation
in the area causing compression. Use of crutches is a good example of how the neuromuscular
bundle may be compressed externally rather than internally. Also, TOS can been seen in pregnancy
due to increased fluid retention and postural changes. (Rattray, 2000) Another common cause of TOS
is seen in individuals who maintain a prolonged or repetitive position. 30% of the population with TOS
have a history of repetitive activity with arm overhead. (Hertling and Kessler, 2006) It is frequently
seen in people who play sports such as racquet ball, baseball, swimming, and occupations such as
trades. (Hertling and Kessler, 2006) It is common for the neurovascular bundle to be compressed in
more than one location, often referred to as a "double crush syndrome. " (Rattray, 2000) Onset of
symptoms is most often insidious, and most of the time there is not definite event in which the patient
can recall an onset of symptoms. Treatment includes physical therapy, analgesics, and in severe
cases, surgery. (Merk Manual , 2011)
�3

In TOS there is either a neuronal compression of the Brachial Plexus, or a vascular compression of
the Subclavian Artery and/or vein, or a combination of the two. Patients experiencing a neuronal
compression will first feel numbness and tingling, referred to as paresthesia, down the forearm and
usually the ulnar border of the hand in the C8, T1 dermatomal distribution. (Rattray, 2000) Later on,
throbbing pain can be felt in the upper limb, as well as trigger point referral from the affected and
compensatory muscles. If left untreated, the compression may cause irreversible nerve damage,
muscle atrophy and weakness of fine motor skills. Next, with a vascular compression the individual is
likely to experience cold and possibly painful arms, and hands that appear to be cyanotic. Rare
complications include Raynaud's syndrome and distal gangrene. (Merk Manual, 2011)
The cause of TOS is quite often multifactorial, rather than having a single source and is a
product of combined anomalies of soft tissue and bony dysfunction. (Hertling and Kessler, 2006)
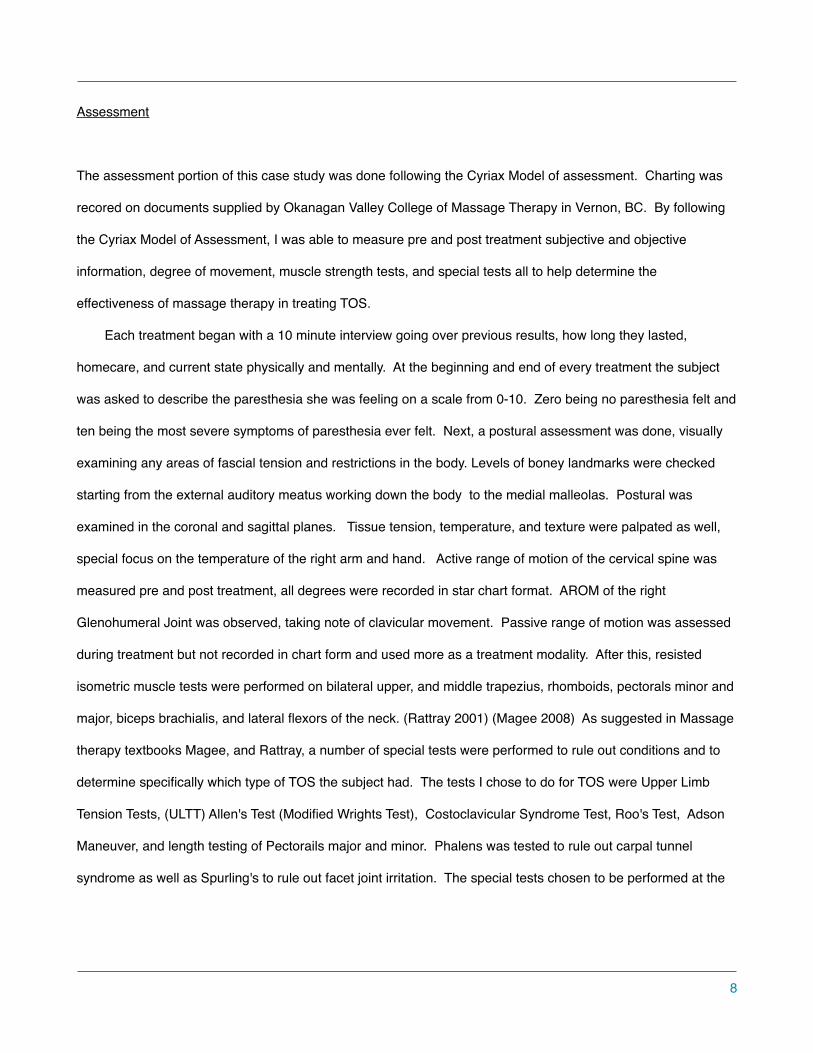
More than half of the people with TOS presents with a congenital presence of a cervical rib at C7.
(Rattray, 2000) The transverse process of C7 extends outwards sometimes as far as the first rib.
This projection will cause narrowing at the interscalene triangle. This triangle is composed of the
anterior and middle scalenes and the first fib. Only the brachial plexus and subclavian artery pass
here, the subclavian vein passes anteriorly to the anterior scalene. Most often surgical removal of the
cervical rib C7 is recommended.
Anterior Scalene Syndrome is a type of TOS where the anterior triangle space becomes
narrowed due to several factors such a hypertonicity of anterior and middle sclalenes, position of the
1st rib, or some type of space occupying lesion. This usually only affects the brachial plexus and
subclavian artery. Patients will experience paresthesia and weakness in the fourth and fifth digits.
(Rattray, 2000)
�4
Costoclavicular Syndrome is generally a vascular compression more than nerve. (Rattray,2000) The
space between the clavicle and 1st rib is compromised due to postural dysfunctions, such as military
type posture, as well as hypertonicty and trigger points in the subclavius muscle restricting clavicular
movement. Symptoms are similar to anterior scalene syndrome as well as chronic edema distally due
to venous congestion.
Lastly, Pectoralis Minor Syndrome occurs when the brachial plexus, and now named Axillary
artery and vein are compressed in the subpectoral space between the clavicle and pectorals minor
muscle at the coracoid process. Also named "Hyperabduction Syndrome" because symptoms are
elicited when the arm is hyperabducted and externaly rotated. This condition can be brought upon by
prolonged positional postures such as painting the ceiling. (Rattray, 2000)
In relation to massage therapy, TOS is a treatable condition where many people are able to find
some relief. With massage treatments, manual manipulation to the surrounding musculature and
fascial covering can help to create functional space within the thoracic outlet and along the nerve
pathways. A study published to Pubmed in 2014, by Marie Lillias Wakefield, demonstrates the
effectives of massage therapy in treating TOS, in particular a compression of the subclavian artery
and lower branch of the brachial plexus. Techniques such as myofascial release, NMT, and MLD
were used to help decrease the hypertonicity in compressive muscles and decrease any vascular
congestion. After six, 50 min treatments the subject no longer suffered with symptoms of paresthesia
and this lasted a year following. (Wakefield, 2014)
The objective of this case report is to outline the treatment and results of massage therapy
techniques, assessments, and home care applied to a 57 year old female presenting with TOS
symptoms. The primary outcome for this case study is for the subject to have eliminated or reduced
paresthesia symptoms in her right arm and hand. The secondary outcome is an improvement of
cervical spine range of motion and an increased awareness of proper breathing and postural habits.
�5
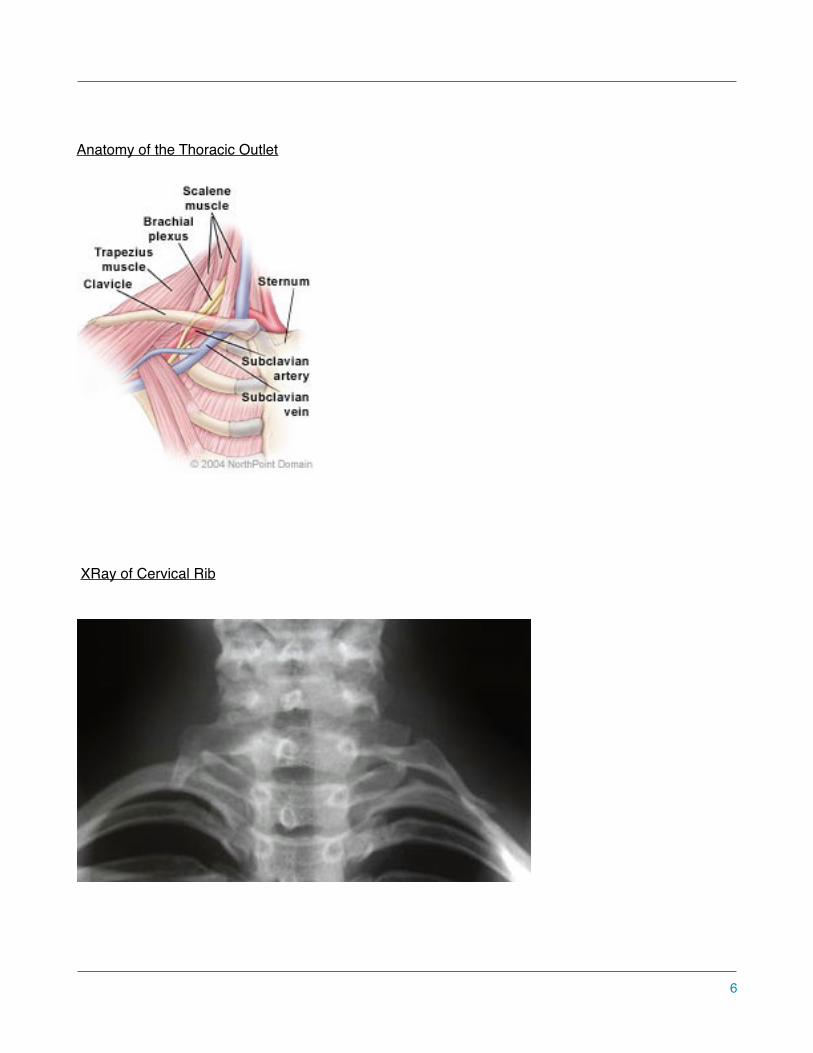
Anatomy of the Thoracic Outlet
�
XRay of Cervical Rib
�
�6

Case History
The subject of this case is a 57 old female who works regular 12 hour shifts at a metal fabricating and
processing facility, in which she is the owner. Her job is in the shipping and receiving department which involves
repetitive bending, lifting heavy objects over head, and working with arms pronated and in front of her body.
She is on her feet most of the day, and occasionally will do paper and computer work in the office. Pastimes
include gardening, hiking, and skiing. Having such an active lifestyle, the subject is in good physical condition.
Over the past few years she has been experiencing TOS symptoms in her right arm. This arm is cooler than her
left, and she experiences paresthesia down the ulnar side of her forearm, into the palmar surface of her hand
and medial three digits. She describes the sensations as numbness and tingling, but no pain. She will wake up
in the morning with these symptoms especially after a long day of gardening and doing dextrous activities.
However, these symptoms done wake her up during the night. The frequency is more related to how hard she
has been working; the more she does the more TOS symptoms she will experience. The paresthesia will often
last a couple days, and is especially prevalent when she feel "stiffness" and tender musculature around C7-T1.
Symptoms will often carry on throughout he day, or during certain above head activities such a brushing her hair
or operating hand held power tools. Relieving factors include, rest, massage, and chiropractic adjustments of
her cervical and thoracic spine. Patient has never received massage therapy treatments for her TOS
symptoms. The subject was willing and looking foreword to treatments and curious to see the comparison
between chiropractic and massage therapy. The subject has sustained a few concussions and whip lash type
trauma to her neck while in her childhood years. She is taking medication for hypothyroidism and anemia. She
has an abnormally wide left carotid artery which was diagnosed by a physician, as well as an extra branch of her
tibial artery which pools into her right foot creating pain, heat, and lack of medial arch. This has also been
diagnosed by a doctor. During the course of our case study, she wasn't receiving any other physical therapy.
�7
Assessment
The assessment portion of this case study was done following the Cyriax Model of assessment. Charting was
recored on documents supplied by Okanagan Valley College of Massage Therapy in Vernon, BC. By following
the Cyriax Model of Assessment, I was able to measure pre and post treatment subjective and objective
information, degree of movement, muscle strength tests, and special tests all to help determine the
effectiveness of massage therapy in treating TOS.
Each treatment began with a 10 minute interview going over previous results, how long they lasted,
homecare, and current state physically and mentally. At the beginning and end of every treatment the subject
was asked to describe the paresthesia she was feeling on a scale from 0-10. Zero being no paresthesia felt and
ten being the most severe symptoms of paresthesia ever felt. Next, a postural assessment was done, visually
examining any areas of fascial tension and restrictions in the body. Levels of boney landmarks were checked
starting from the external auditory meatus working down the body to the medial malleolas. Postural was
examined in the coronal and sagittal planes. Tissue tension, temperature, and texture were palpated as well,
special focus on the temperature of the right arm and hand. Active range of motion of the cervical spine was
measured pre and post treatment, all degrees were recorded in star chart format. AROM of the right
Glenohumeral Joint was observed, taking note of clavicular movement. Passive range of motion was assessed
during treatment but not recorded in chart form and used more as a treatment modality. After this, resisted
isometric muscle tests were performed on bilateral upper, and middle trapezius, rhomboids, pectorals minor and
major, biceps brachialis, and lateral flexors of the neck. (Rattray 2001) (Magee 2008) As suggested in Massage
therapy textbooks Magee, and Rattray, a number of special tests were performed to rule out conditions and to
determine specifically which type of TOS the subject had. The tests I chose to do for TOS were Upper Limb
Tension Tests, (ULTT) Allen's Test (Modified Wrights Test), Costoclavicular Syndrome Test, Roo's Test, Adson
Maneuver, and length testing of Pectorails major and minor. Phalens was tested to rule out carpal tunnel
syndrome as well as Spurling's to rule out facet joint irritation. The special tests chosen to be performed at the
�8

beginning of the case study and at the end were Allens, Costoclavicular, ULTT, and Spurlings. All of the testing
was performed bilaterally to set a base line "normal" for the subject. (Magee, 2008)
Treatment
The treatment goals developed for this case study were designed to decrease the compression
of the brachial plexus and subclavian artery and vein at the costoclavicular space, and in return
decrease the symptoms of TOS felt in the right arm and hand. The first goal is to decrease fascial
restrictions to the upper cervical fascia, bilateral SCM's, upper and mid trapezius, scalenes,
subclavius, pecs, deltoid, biceps, and flexors of the wrist to increase muscle pliability. Next, decrease
hypertonicity and trigger points to bilateral trapezius, scalenes, suboccipitals, subclavius, pecs,
rhomboids, deltoid, biceps, flexors, and extensors of the wrist to decrease paresthesia and
compression of the brachial plexus, and subclavian artery and vein. Also, increase the functional
movement of the right clavicle to allow a more smooth superior roll during glenohumeral flexion. Next,
increase the length of bilateral subclavius and rhomboids to balance out military posture and increase
the anterior rotation of the shoulders. Lastly, encourage subject to allow softening and relaxation of
the shoulders to bring them foreword to create more space between the clavicle and first rib for the
neurovascular bundle to pass.
The case study occurred over a five week period with biweekly treatments of approximately 90
minutes each, total of 9 treatments. Approximately 10 minutes was allotted for the interview, 20
minutes assessment (pre and post), and 60 minutes treatment time. After two weeks, there was a
one week period where there were no treatments due to scheduling availability of subject. Because
the subject presented with more of a unique presentation of TOS with Military posture, the treatment
wasn't as traditional as it would be with someone with a different posture. The Clinical Massage
�9
Therapy textbook by Fiona Rattray, published in 2001, has similar techniques and treatment goals
that can be used as a guideline for all types of TOS.
Treatments began in the prone position with deep diaphragmatic breathing exercises. General
full body rocking progressing to segmental vertebra lateral rocking was performed to entrain the body
and introduce touch. Next, compression to the full back muscles, and then myofascial techniques
were applied. Skin rolling, cross hands, separating trapezius from latissimus dorsi, and
thoracolumbar fascia. Lavender infused oil was applied to full back and swedish and circulatory
techniques were used to warm up the tissue. Starting superficially, and then working deeper into the
rhomboids and erectors with deep stripping and ischemic compression applied to trigger points.
Trigger points were treated three times each. Time spent in prone was approximately 25 minutes
each treatment.
Now with patient in supine, gentle rhythmic compressions were applied to bilateral shoulder
complex to assess movement of tissue and bones. Passive range of motion was applied to the
Cervical spine, taking note of effected ranges and tissue tension. Next, intermuscular myofascial
techniques were applied to the deep investing layer of Cervical fascia. This included the nuchal line
attachment, spine attachment, mastoid tip to the clavicle, chin to the sternal notch, anterior border of
traps and posterior border of SCM, and anterior border of SCM and trachea. All myofascial
techniques were shown by Natale Rao in the Myofascial Integration Course held at OVCMT during
the first year of the program. Passive and active intramuscular release of pectorals major, minor, and
subclavius is performed within patients pain tolerance. After this, oil is applied to shoulder, chest and
neck. The area is warmed up with circulatory techniques such as effleurage, fingertip kneading and
picking up. Next, deep stroking and trigger point release of scalenes, upper trapezius, SCM,
subclavius, and levator scapulae is performed. Origin and insertion, golgi- tendon organ technique
and "S bowing" is applied to bilateral SCM, being cautious not to over treat and cause a headache
�10
flare up. After this, the whole neck area was thoroughly flushed out with swedish techniques. A
suboccipital release is then followed by cervical spine traction, held for 2 minutes. Next, a facilitated
contract relax/Agonist contraction stretch is done to the bilateral neck flexors. Each stretch held for
6-8 seconds 3 times, after the stretch Passive ROM of cervical spine is performed. The clavicles are
then assessed, and grade 1 sustained and grade 2 oscillations are performed to the sternoclavicular
and acromioclavicular joints in the direction of inferior, superior,anterior, posterior, and traction glides.
Working down the arm, intermuscular facial separation is applied to the deltoid, biceps, brachialis,
flexors and extensors of the wrist. The goal here is to ensure functional space for the ulnar nerve as it
travels down its pathway to the medial wrist. Flushing and deep stroking with oil, treating any trigger
points is followed. Lastly, PROM of the Glenohumeral, Humeroulnar, Proximal Radioulnar, distal
Radioulnar and Radiocarpal joint is applied, 3 times each range. The subject was then asked to
slowly get off the table when she was ready and move around to see how she felt, symptoms of
paresthesia and temperature of the right arm and hand were analyzed using the scale from 0-10 and
palpation. Time spent in the supine position was approximately 45 minutes each treatment. After
several treatments, I spent less time trying to increase the length of the pecs, after realizing that with
the Military type posture they were actually not shortened, as they would be in a more traditional
presentation of TOS.
After each treatment, home care was written down for subject in a journal in which they took
home with them. Deep diaphragmatic breathing was given to practice twice a day in the evenings
before falling asleep and during the day at work. Also, postural awareness throughout the day,
working on letting the shoulders be more relaxed and slightly anteriorly rotated. For stretches, the
subject was given the doorway pec stretch at three levels, which now in hindsight wasn't the most
beneficial choice because the pecs were already lengthened. A scalene and levator scapuale stretch
�11
was given to the subject to do twice a day, three times each side, holding for 30 seconds. Subject
complied and was very willing to participate in homecare exercises throughout the five weeks.
Outcomes
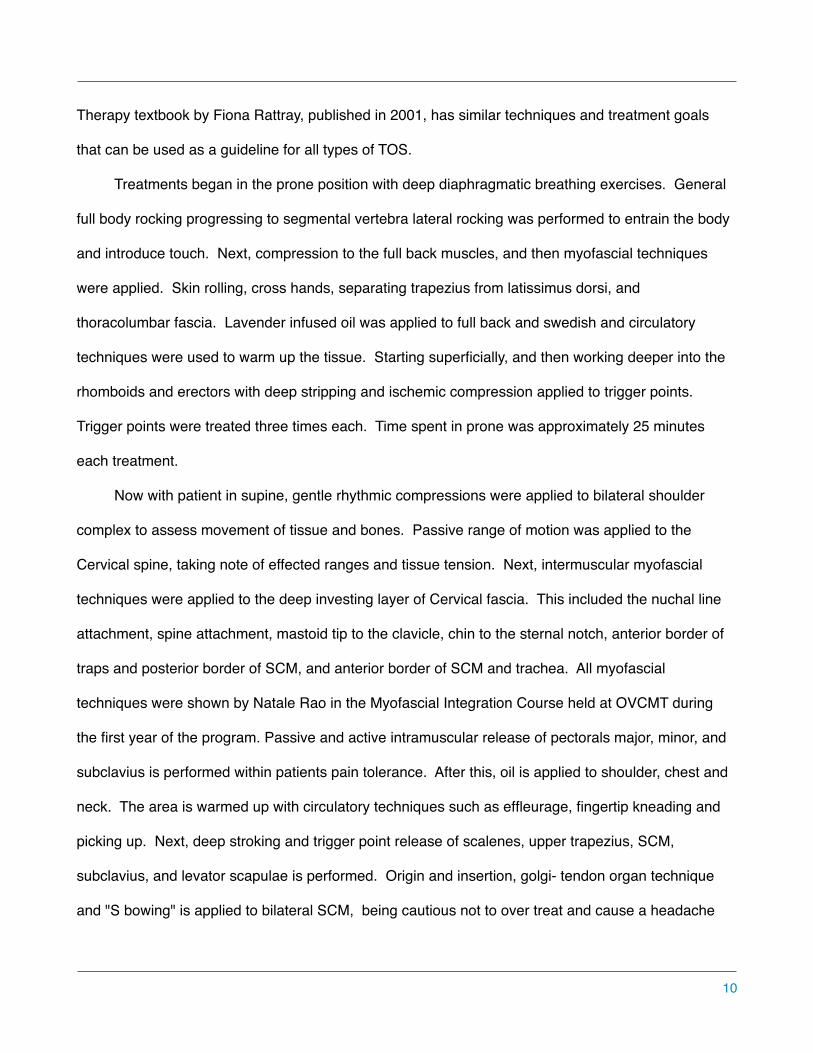
Postural assessment was an important aspect of this research project. One of the first things
observed was the presentation of the "Military Type Posture". The humeral heads sat posterior in the
glenoid fossa, almost more posterior than the external auditory meatus. The sternum and ribs were
slightly protruded anteriorly in a Pectus Carinatum type of appearance. Clavicles blended back into
acromion in an elevated posterior direction. The Cervical spine had good curvature but the transition
to the thoracic spine at C7-T1 created an axis that protruded slightly posterior. There was a lack of
Thoracic kyphosis, with scapular winging, and a hyperlordosis of the Lumbar spine. The hips were
rotated anteriorly, 18 degrees on the right and 16 degrees on the left. Breathing at rest was observed
as apical.
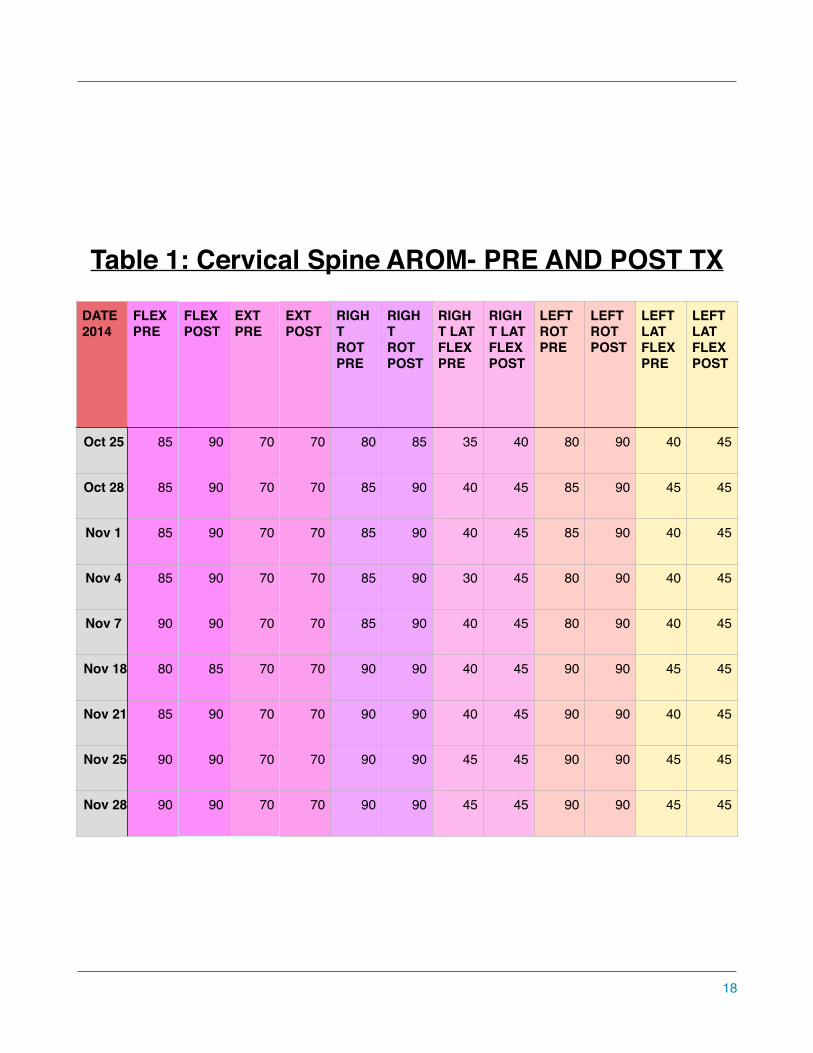
Each treatment, cervical spine active range of motion was evaluated pre and post massage.
Please refer to Table #1: Cervical Spine AROM- Pre and post treatment, page 18. All ranges were
done with minimal to no discomfort, except for right and left lateral flexion, subject felt muscle
tightness on opposite side of neck. Left rotation was also slightly restricted in comparison to right
rotation, subject feeling muscle tightness and stretch on the right side of neck. During the first
treatment on October 25th, 2014, left rotation pre massage was 80 degrees, but post massage
subject gained 10 degrees of movement. During the last treatment on November 28th, 2014, left
rotation pre and post massage was 90 degrees. All ranges performed in post assessment were done
more smoothly, and each range gained 5-10 degrees each time. New ranges were lost in-between
the first 5 treatments, but after that the subject was able to keep the new ranges, perhaps due to
treatment and application of homecare stretches maintaining the new ranges.
�12
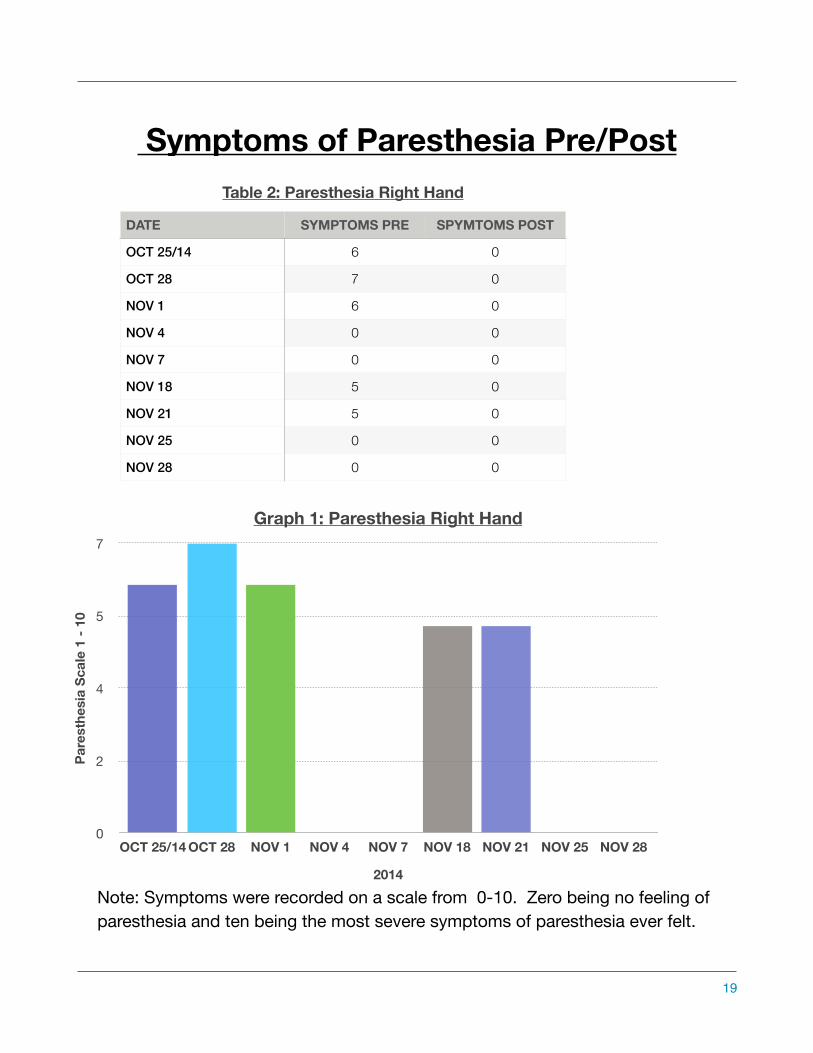
Subjective information was gathered from patient pre and post massage regarding the levels of
paresthsia felt in the right arm and hand. As mentioned above, a scale from 0-10 was used to rate
what the subject was feeling. Please refer to Table #2 and Graph #1- Paresthesia Right hand, on
Page #19. The first few treatments the subject felt about 6-7/10 pre treatment, but the 5th and 6th
treatments the subject felt no paresthesia at all before the treatment. After taking a week off of
treatments however, the paresthesia come back at 5/10. During the last few treatments of the study,
the subject felt no symptoms of paresthesia at all. All post assessment symptoms were 0/10.
Temperature of right hand was also monitored. Pre treatment palpation of the hand and arm was
quite cold and post treatment was flushed and warm.
All muscle testing was referred to from the Muscle Testing and Function textbook. There were
no significant muscle weaknesses or pain during any of the muscle strength tests. The muscles
evaluated were upper and middle trapezius, rhomboids, pectorals minor and major, biceps, and the
lateral cervical spine flexors. All muscles were tested unaffected side first, isometrically, bilaterally,
and three times each side. All muscles were graded a strong 5/5.
Special Tests were an important part of the assessment to help determine the type of TOS,
where the compression was at, and to rule out other pathologies. The positive tests were tested the
first treatment, and then retested again at the last treatment. Please refer to Chart #3- Special Tests,
on Page #20. Pectoralis minor and major length tests were negative ruling out compression at the
coracoid process under pectorals minor. A negative Phalen's and Tinel's tests ruled out the possibility
of Carpal Tunnel Syndrome as a secondary condition, as well as no report of being awaken during the
night from symptoms which is common for CTS and not so prevalent in TOS. Allen's maneuver
(modified version of Wrights Hyperabducton Test), and the Costoclavicular Syndrome Test (Military
�13

Brace Test) were both positive on the right. This concluded that the compression was occurring at
the costoclavicular space between the clavicle and first rib. There was neuronal compression of the
brachial plexus, as well as vascular compression of the Subclavian Artery and possibly vein, hence
the cold right hand. These findings complemented the postural presentation of the subject with the
Military posture, the subject stood very erect, with the shoulders back decreasing the costcoclavicular
space. The Upper Limb Tension Tests revealed bilateral positives for # 1, 2, and 4. This showed
stress to the Median, Musculocutaneus, and Ulnar Nerves. Allen's test and Costoclavicular Syndrome
Test were retested on the 8th, and 9th treatments. Findings were positive on the 8th treatment, and
negative on the 9th treatment. Between those 2 treatments, the subject was doing yoga regularly
which may have effected the test results. Yoga was a new activity for the subject.
I followed up with the subject about a month after the last treatments for an interview. She
noted that the Massage Treatments definitely helped with her TOS symptoms the weeks that followed
her last treatment. Her paresthesia did not return and she noted the movement of her neck was more
smooth without crepitus. She also had a comment from her Chiropractor that he could tell a
difference in the tissue health around her cervical and thoracic spine.
I feel as though most of the treatment goals were met during the 9 treatments. Facial
restrictions and hypertonicity of the upper cervical fascial and musculature was reduced as well as the
trigger points found in subclavius and rhomboids. During Glenohumeral flexion, the clavicle's superior
roll was more noticeably functional in comparison to how it had moved before. With homecare and
practice during treatments, the subjects breathing style was more diaphragmatic than apical. More
focus and time on reducing the military type posture would have be beneficial for the subject. More in
depth patient education and guidance could have been implemented for postural alignment and
homecare techniques.
�14

Patient compliance, and interest to better her health, played a significant role in the treatment
outcomes. Home care exercises were followed willingly and with enthusiasm. Subject always
showed up to scheduled appointments. For the purposes of this case study, there was no money
exchanged for treatments. The subject willingly volunteered to participate and comply to receiving
treatments offered for educational purposes. In the event of a massage therapist charging a fee for
the same amount of treatments as the case study, I believe it would be realistically affordable.
However, fitting in two treatments a week may be challenging for individuals with busy schedules.
Outcomes found in this case report are supported by previous research on the topic. For
instance, an article published to Pubmed in 2013 by Robin Streit, outlines the effectiveness of 8
massage therapy treatments on a patient with Neurogenic TOS. Techniques used were similar to the
ones in my case study: myofascial release, trigger point therapy, cross fiber friction, muscle stripping,
and gentle passive stretching. Findings showed improvement of Glenohumeral range of motion,
reduction of muscle weakness, pain, and paresthesia. The author suggests that massage may be
useful as a broad approach to maintaining TOS symptoms and improving mobility.
�15

Military Type Posture
�
Discussion/Conclusion
This case study was able to prove the hypothesis true. " The primary outcome for this case study
is for the subject to have eliminated or reduced paresthesia symptoms in her right arm and hand. The
secondary outcome is an improvement of cervical spine range of motion and an increased awareness
of proper breathing and postural habits." Following each treatment, and a month afterwards,
symptoms were reduced and and subject noted smoother movement in cervical spine. As mentioned
above, the Military Posture, perhaps a confounding factor, didn't have much of a change since the
beginning of treatment, it stayed the same throughout the whole case study. The treatment plan was
appropriate for this condition, and there weren't any unexpected reactions to the treatment. In regards
�16
to the special tests that were positive, I think it would have been more appropriate to retest them after
each treatment , instead of once at the beginning and at the end of the case study. By testing more
regularly, it would have shown a better indication of the progression of the treatments. Myotomal,
dermatomal, and reflex testing would have been beneficial to do as well. Also, more literacy research
could have been done on TOS presenting with the Military Type posture, there is a lot of knowledge
on the traditional presentations of head forward postures, but little on Military Type.
References
1) Fiona Rattray, 2000, Clinical Massage Therapy, Talus Incorporated, Elora, Ontario.
2) David J. Magee, 2008, Orthopedic Physical Assessment, (5th Edition), Saunders Elsevier, St.Louis, Missouri.
3) Florence Kendall, 2005, Muscles-Testing and Function with Posture and Pain , (5th Edition), Lippincott Williams and Wilkins, Baltimore, MD.
4) Dr. Nikita Vizniak, Muscle Manual, 2012, Professional Health Systems Inc, Canada.
5) Darlene Hertling and Randolph Kessler, 2006, Management of Common Musculoskeletal Disorders, (4th Edition), Lippincott Williams and Wilkins, Philadelphia.
6) Mary Wakefield, 2014, Case Report: The Effects of Massage Therapy on a Woman with TOS, PubMed, 11.
7) Robin Streit, 2013, NTOS symptoms and mobility: a case study on neurogenic thoracic outlet syndrome involving massage therapy, PubMed.
8) Physiopedia, http://www.physio-pedia.com/File:Tos.jpg, April 16,1015, Chelsey Walker.
Images:
9)http://www.massagetherapycanada.com/content/view/1532/132/
10)https://embodypilates.wordpress.com/2014/05/29/what-posture-type-are-you/
11)http://www.nhs.uk/conditions/cervical-rib/Pages/Introduction.aspx
�17
�18
Table 1: Cervical Spine AROM- PRE AND POST TX
DATE 2014
FLEX PRE
FLEX POST
EXT PRE
EXT POST
RIGHT ROT PRE
RIGHT ROT POST
RIGHT LAT FLEX PRE
RIGHT LAT FLEX POST
LEFT ROT PRE
LEFT ROT POST
LEFT LAT FLEX PRE
LEFT LAT FLEX POST
Oct 25 85 90 70 70 80 85 35 40 80 90 40 45
Oct 28 85 90 70 70 85 90 40 45 85 90 45 45
Nov 1 85 90 70 70 85 90 40 45 85 90 40 45
Nov 4 85 90 70 70 85 90 30 45 80 90 40 45
Nov 7 90 90 70 70 85 90 40 45 80 90 40 45
Nov 18 80 85 70 70 90 90 40 45 90 90 45 45
Nov 21 85 90 70 70 90 90 40 45 90 90 40 45
Nov 25 90 90 70 70 90 90 45 45 90 90 45 45
Nov 28 90 90 70 70 90 90 45 45 90 90 45 45
�19
Table 2: Paresthesia Right Hand
DATE SYMPTOMS PRE SPYMTOMS POST
OCT 25/14 6 0
OCT 28 7 0
NOV 1 6 0
NOV 4 0 0
NOV 7 0 0
NOV 18 5 0
NOV 21 5 0
NOV 25 0 0
NOV 28 0 0
Graph 1: Paresthesia Right Hand
2014
Pare
sthe
sia
Scal
e 1
- 10
0
2
4
5
7
OCT 25/14 OCT 28 NOV 1 NOV 4 NOV 7 NOV 18 NOV 21 NOV 25 NOV 28
Symptoms of Paresthesia Pre/Post
Note: Symptoms were recorded on a scale from 0-10. Zero being no feeling of paresthesia and ten being the most severe symptoms of paresthesia ever felt.
Graph 1

�20
Table 3: Special Tests First and Last Treatments
Date Special Test Positive Negative
Oct. 25/14 Allens Maneuver Right
Costoclavicular Test Right
ULTT 1,2,4 Right 3
Adson Manuever Right
Spurlings Test ✔
Nov.28/14 Allens Maneuver Right
Costoclavicular Test Right
ULTT 1,2,3,4 Right
Adson Manuever Right
Spurlings Test ✔

�21

�22
Recommended