-
8/6/2019 9c Cost of Treatment
1/6
98 't l i ' . i i l i-i a a',- a i'. :, '' .: ..
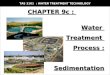
Income group-wise cost of medical treatment of the households:
The cost omedical treatment by income group in the sampied
households in the districts alsshows variation. The poor of Birbhum
district (incomes below Rs. 16,000 annualhspent much more on
medicai treatment than their Dumka counterparts.
The lowest income group households in Birbhum incurred an annuaT
xpenditure of Rs.2,052 on medical treatment alone,which constituted
17.9percent of thei^vet^ge annual income. The same figure was Rs.
1,356 in Dumka, which constitutec12.4 percent of the ^verage annual
income of these households. While the averagexpenditure on medical
treatment was higher for the upper income groups (R.s. ,56in the
caseof Birbhum and Rs. 3,786 for Dumka), the percentageof such
expenditure to total annual expenditure was found to be sharply
different.
While the cost of medical treatmeflt for the lowest income group
in Birbhurrformed alarge share of thefu total annual income (17.9
percent), the figure was muclower - only 6.3 percent, for the
uppermost income group. In the caseof Dumka,the averagecost of
medical treatment for the uppermost income group v/as neadypercent
of annual income, which was much lower than the figure for the
lowesincome group (12.4percenr). t can be seen rom the graph that
the lowest incomgroups - the poorest of all - suffer the most from
health ailments, being more susceptibie to various diseases.The
cost of treatment coflsumes a large share of theimeagre nnual
ncome.cost of hospitalisation: of the 447 persons in the sampled
households inBirbhum and 468 persons in Dumka (who suffered from
any ailment in the year pre-ceding the canvassing of
questionnaires) 88 percent in Bitbhum and 92 percent inDumka were
found to have undergone medical treatment. only a small number
o1hospitalisatioriswere repoted. Again, we found some variation
amongst the two districts concerning hospitalisation of patients.
While 3.8 percent (17 in number) of al
Chart 7 3 Annual health expenditure: by caste
WlJitbla*n S{ l S1 ' (Jthets[:il l]umka
qfrllf r
= A(fiOu - , , . . , .o. -luullXrrlo ^ . . ^ .O.T
IL'L'Uq>.
U
-*'
Chatt 7 4 Annual health expenditure: by income group
c!-? o
9 Gc ' -u ^u^! P
f< Rs 16|{ l i - 25001- 35001- 45001- >6Ci0(x,16000 2-5000
35000 4500{-} {10000' :r ' - Eirbhum -* - Dumka
-
8/6/2019 9c Cost of Treatment
2/6
7L: ' t l i . i ' | i i i t l - ' . i
::rients in Birbhum were reportedly hospitalised, the figure for
Dumka was only 1.5:ercent (seven n number). In some of the cases,
espondents mentioned that despite:ceding hospitalisation many could
not avajl,of the same because of the anticipatedr'rsts involved,
and the difficulties in accessinghospitals.
The averagecost per hospitalisation in Birbhum district was Rs.
9,171, while itras Rs. 2,258 in Dumka. The cost of hospitalisation
included rent for beds, travel-\penses, medicines, charges for
diagnostic tests and other medical expenses.
Of the totaI1.7 hospitalisation cases n Birbhum, only one was
admitted to a pri-";etenursing home, the cost of which was similar
to that obtaining in the public hos-ritals. However, the patient
was suffering from Hepatitis and needed only three
days'iospitalisation. Of the 16 patients admitted to the public
hospitals only two received:ree bed and medicines.The o thers had
to pay for these.
Of the total sevencasesof hospitalisation in Dumka five were
reportedly admit-ied to a public hospital and the rest resorted to
private treatment. !flhile the aver^gecost of hospitalisation n the
pubJic hospitals was Rs. 2,302 - ranging berween Rs.600 and Rs.
5,500, he averagccost in private hospitalswas Rs. 2,150 - in the
rangeRs. 2,000 - Rs. 2,300. As reported, none of the patients
admitted ro the public hos-pitals was given free beds or
'medicines. (SeeAppendix tablesD | 0 and D
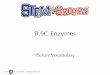
10.a.fordetails.)Service-wise cost of treatment: QLralified private
doctors were found to be themost expensivesource of medical
treatment in both the districts. Obvioush; the socio-economic
differences between the two districts have influenced the
expenditure pat-tern on medical treatment. \\&ile the ^veruge
cost of medical treatment by privatequalifieddoctors per patient n
Birbhum was Rs. 3,155, t was Rs. 1.,490n Dumka.
Public health facilities came as the second most expensive
source of medicaltreatment itr both districts. The averagecost of
treatment per patient (at public healthfacilities) in Birbhum was
Rs 959, rvhile the figure for Durnka u'as higher (R.s. ,115).The
high cost of public health care n both the districts ndicates he
gradual ebbing
l
Barik Shcikh, 70, is a arge farmer o{- a Birbhum village. He
cultivatesmore than ten acresoi double-cropped land,having
assuredirrig:rtion to*.Y., submersible:l*rl"lr He ,,s-esn:-. ": ,
only ro irngatehisown andbur also or h.iring ut and his assrucs
ua)'s - ph)sical lvand f inaric ia[ ] - he nou Lives poor man's
i fe ar his in- laws'rcsidcnce. ,'
him a strhstantial ncome, and reladr,ely arge savings.Tlre
finance accumulatedcame ro his assistancewhen he suffetocl
.a'heart. ;attack. Hc spent Rs. 71,000 on treatment, ve t he ciid
not have to borrow or seek assistance rom oihers. His lan4
submersiblc.t"-T:i;5ffi ;"#,il..t til:':",n.uliag.s
nlrlmltncar:a*.to the fove. esa26 ear-ordonsrrucuonork-e-1 nd
is,thc onl1,earning member of his fanuly.One of his legswas badly
inlured following an accident Aiijul went to the subr and rs thc
onJv carrung member ot Lus amtly. ()ne of hi5 legswas badly injured
following an accident. Aiijul wbnt to rhe subdivisional hospital at
Sian, Bolpur, and despitespendrnga substantialarnount of time and
monel' at the governmeni facriiry' oundno improvpment in his
conditjon. He was subsequenth'admitted to a pri'natenursing home
v'here iris cg was amputarcd. He hadto spund about Rs. 90,000on his
treamrent.Since he had no savingsor other assetshe haci ro sell his
housc. f-landicappcd n"borh ,
-
8/6/2019 9c Cost of Treatment
3/6
9A 1 y f, l io .'.1 ,.;;',114. t :-T- 7. i .:',,t '' t
of a ftee public health delivery system. Of course there is much
greater differenceberween the two districts in the degree of
utilisation of public health services andtheir cost. The difference
in cost between the pubJic sourcesof ffeatment in the twodistricts,
perhaps 'justifies'the high degree of reliance on private services
n Dumk4as the costs of the public health sources was found to be
much higher in DumkaConversely, the relatively large gap between
public and private (qualified) sources oftreatrneflt ensured that
public sourceswere the first choice for a rclaavely higher num-bers
of patients (29 percent) in Birbhum than in Dumka (12 percent).
In the caseof unqualified medical practitioners (tJMPs or
quacks), there was amuch larger difference between the two
districts. While tn Birbhum the averagecostof medical treatment
taken from an UMP was Rs. 480 per case, n Dumka it was Rs.858.
Perhaps the re'latively better accessibility of the public health
services inBirbhum was responsible for a lower percentage of
patients visiting quacks Q9 percent) than in Dumka (62 percent).
Despite the high cost of medical treatment b\UMPs, people continued
to seek their services, as the poor condition of publichealth
facilities and the poor socio-economic condition of the households
combineto create dependence on the services of quacks. The poor
service delivery of thepublic health centres made the UMPs a better
choice than expensive private doctors.The modes of operation of
theSequacks (such as giving treatment on credit,
readvavai-labrJitynd willingness to render service) were reportedly
what attracted villagersin Dumka district to them.
While we found about seven percent of the patients visiting
homoeopaths inBirbhum, in Dumka there was no case at all of
patients visiting homeopaths fortreatment. The avetage cost per
case for homoeopathic treatmeflt was Rs. 383.
As for the other sources of treaulent - mainly herbal medical
ptactitioners(kabirEs or uaids)and witch doctors (Ehas,deysiq
angarus)the average cost involvementper case n Birbhum and Dumka
was Rs. 709 and Rs. 199 respectively.F{owever, veryfew people in
Birbhum were observed seeing such practitioners. On the other hand,
in
Dumka such practitioners were reJiedupon by 14percent of the
patients, which uzs higher than thenumbet visiting public services.
As we have dis-cussed n section 5, such dependencewas rrot
areflection of "superstitious bel-ief", or !'abhor-rence towards
moderfl medicine", but the com-pelling factor of inaccessibility
and consequentinability of people to avail of modern health
care.
Cost involvement, as the responses indicate,is a major factor in
choosing particular health ser-vices - although not the only one.
Many of rherespondents in Birbhum attributed their choiceof going
to UMPs to their experience of theUMPs being iess expensive than
the PHCs orhospitals. Such experierrceswere much more
Chart 7.5 Cost of treatment: by service35003000
o ?5frf lo - - ' 'qd z r . , r j t . rb
1000500
0WRirbham Govt. Pvt Qly Quack Homeo Othershi',]Dumka
-
8/6/2019 9c Cost of Treatment
4/6
common in Dumka. Howeveg the cheaper-of mofe readily available
private soulceswefe not cofisidefed sufficient for all the
different ailments suffered by people whohad to choose expenslve
sources for critical cases. n the following section we shalldiscuss
the cost involvement of different ailrnents in a disaggregated
form'
Ailment-wise cost of tfeatment: As mentionedin the previous
section, the pattern
of ailments in the two distticts was different, yet there wefe
some common diseasesthat people from the sainpled households of
both districts suffeted' These werelarge\ ,io-u.h ailments,
diarrhoea, the cold-cough-fever syndrome, bone
relateddiseases,gynaecological problems, skin diseases,TB, etc'
While for some of the.ailments the averagecost of medical
tfeatment in boththe districts v/as found to be similar, in other
cases he degree of difference v/as quitenotable. For example, in
the caseof cold-cough-feveq the ^vef^ge cost of tfeatmentper
patient in Birbhum and Dumka was Rs. 208 and Rs. 177 respectively,
but thei"rp..ti-r. costs fof the treatment of diarrhoea wefe Rs.
614 and Rs. 981' The mainfeasofrs for such similarities and
differences afe complex and sociologically embed-ded - the delivery
of public health sefvices, pefceptions of people about
differentailments and soufces of treatments, the accessibility to
vadous sefvices, the socio-economic status of the households,
etc'
Let us take the case of the averagecost of tfeatment for
cold-cough-fever' Inboth the districts, people considered the
ailment to be of a non-setious natufe andtook the help of locally
avasTableuMPs. nterestingly, in caseof this parricular ailmentthe
difference in the pattern of medical treatrnent between various
sources (i.e. gov-efnmeflt public health cefrtfe, qualified private
doctors and UMPs) was less signifi-cant. A similar use of medicines
was found on examination of the prescriptions (andmedicine foils
and caftons used) by all three service providers. Perhaps, the
commondegreeof effectivenessof all the t}ree major sourcesof
medical attention made peo-ple depend mofe ofl the relatively
cheaper and mofe easily availablesource of med-ical treatment - the
UMPs. Use of UMP services for this particular ailment was fuf-ther
justified by the saving of time that would accfue through pattonage
of the UMPsas against visits to public and private soufces. Hence,
the cost of medical tfeatmentin real terms made quacks mofe
ecoftomically acceptable for this particular ailment'
In the case of tuberculosis the averagecost for medical
treatrnent in Birbhumwas much lower (Rs. i,2701th^nin Dumka
(Rs,2,003). The main reason behind thiswas rhat the maiority of the
patients (71 percent) availed of the public health ser-vices in
Birbhum, while private qualified doctofs wefe the chief soufce of
such ffeat-ment (52 percent) in Dumka. The relatively high success
rate of the public healthdelivery system has perhaps attfacted the
majority of the patlents in Birbhum' whilethe public sector in
Dumka has appatendy failed to do so'
This process has a class dimension as well. A large maiority of
the TB patientsin both the districts belonged to the poorer
economic classes, or whom the publichealth deJivery system was a
preferred source given the financial implications ofmedical
tfeatment. It was the uttefly deficient and near-defunct public
health system
-
8/6/2019 9c Cost of Treatment
5/6
in Dumka that compelled the poorer patients to seek pivate
health services.A rela-tively better functioning public health
sysrem in Birbhum was able ro make a hugedifference in health
seeking behaviour. This finding has special relevance for
districthealth administation in particulat and for the health
sector of the ccuntry as awhole. When a modicum of public attention
can make a significant difference inhealth seeking behaviour, there
no real reason why the district health a&ninistrationin Dumka
cannot make the services effective and why the Birtrhum
adrninistrationcannot make such services universal. An equitable
public health delivery systemwould be of immense help, particulady
for the poorer sections of society.It is also worth noting here
that, in both districts, peoples' own perceptionsregarding the
seriousnessof the diseaseskept them away from the UMps.
The cost of treatment of other diseaseswas found to be much
higher inBirbhum than in Dumka, specifically heart diseases,ENT
problems, epilepsy, acci-dent iniuries, etc. A high degree of
difference in the perception of the seriousnessof such diseaseswas
found amongst the people of the two districts. \fhile mostpatients
n such cases n Dumka were rreatedby local UMps (and in some
casesbykabirEs), neady all in Birbhum sought adr,-iceand treatment
from qualified prtvatedoctors.
The poot delivery of public health services becomes more visible
in the caseofCh.an 7,6 Cost of treatment: by ailment
-
8/6/2019 9c Cost of Treatment
6/6
malarn. There is r,rry litde scope for making a comparison
between the trvo districtswith regard to the cost of medical
treatment for malaria, since Birbhum had only twopatients. In
Dumka, malatia.was a menace that many a ttme ruined households
dueto the high cost of medical treatmerit. The averagecost of
treatment for malaia inDumka was Rs. 611 per case the lower and
upper limits being Rs. 100 and Rs.4,500).The wide extent of malaria
prevalence (where all members of manv householdsreportedly suffered
from mafarta) exacetbates the situation by forcing the house-holds
to spend a significant portion of their annual household income on
malaiatfeatment.
The cliief source of treatment for malariain Dumka, as seeri n
the previous sec-tion, was the UMPs. The frequencv of maladal
attacks made the quacks indispens-able, for at both public health
points and in the clinics of private qualified doctorspeople need
hard cash for medical treatment, whjle the UMPs ffeated them on
cred-it. The sarnewas the case withkala-azaL diarchoea and othet
stomach ailments. Thisindispensability has given rise to rampant
drug abuse and corrupt practices in per-vasive and exploitative
"health bazaars".
Nfe shail briefly examine the complexities of this market in the
following part ofour discussion.
M L r r t N C T H t c o s l o i t u 4 r D i { . A tf r i A T t u
1[ N T"kog ki sabajinis be, ho1 batemare, noi bhatemare!'("Illness
is not an easy hing - it kills either by hand [i.e.directly] or by
[depriving oneof] rice [the main staplefoodl!").As shown in table
7.1 many households suffer from an adverse pattern of lowincome and
high expenditure. At the same time, poverty, hunger and ignorance
havecreated an environment that results in malnutrition and various
ailments.2 Theabsenceof an effective public health delivery
systemhas made things worse. \7e haveeadier discussedthe abusive
and corrupt practices of private doctors (quacks as wellas
qualified private practitioners). The financial cost of health
care, both at the pri-vate and public facilities made people,
particulady those from the poorer classes,more r,'ulnerable.
Respondents recounted many different stories about their
sufferings particular-ly those concerning the arrangement of money
fot meeting the costs of medicaltreatment. The money reported to
have been spent in the year preceding the studywas arranged, in
most cases, tom man,vdifferent sources including reguiar
incomesources,savings, oans (with or w-ithout interest),
proceedings from selling assetsandproperties, mortgaging of
assetsand propeties, etc. Assets included livestock,
trees,ornaments, utensils, bicycles, wristwatches, etc. while
property inciuded land andbuildings.
In severalcases, he cost of medical treatment in both the
distficts was met fromthe regular income of respondents either in
full or in pan. In a significant number