AG
AA
bst
ract
s
808
Safety and Proof of Concept Demonstrated With a Novel Prep-Less X-RayImaging Capsule for Colon Cancer ScreeningMenachem Moshkowitz, Nadir Arber
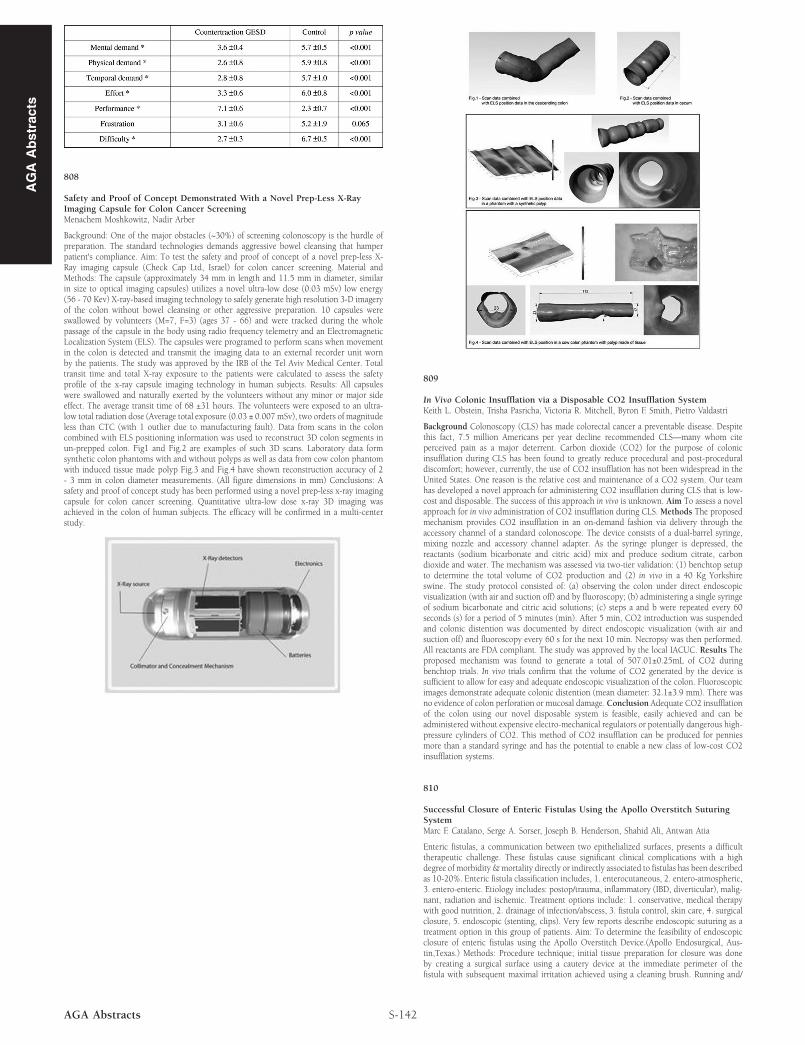
Background: One of the major obstacles (~30%) of screening colonoscopy is the hurdle ofpreparation. The standard technologies demands aggressive bowel cleansing that hamperpatient's compliance. Aim: To test the safety and proof of concept of a novel prep-less X-Ray imaging capsule (Check Cap Ltd, Israel) for colon cancer screening. Material andMethods: The capsule (approximately 34 mm in length and 11.5 mm in diameter, similarin size to optical imaging capsules) utilizes a novel ultra-low dose (0.03 mSv) low energy(56 - 70 Kev) X-ray-based imaging technology to safely generate high resolution 3-D imageryof the colon without bowel cleansing or other aggressive preparation. 10 capsules wereswallowed by volunteers (M=7, F=3) (ages 37 - 66) and were tracked during the wholepassage of the capsule in the body using radio frequency telemetry and an ElectromagneticLocalization System (ELS). The capsules were programed to perform scans when movementin the colon is detected and transmit the imaging data to an external recorder unit wornby the patients. The study was approved by the IRB of the Tel Aviv Medical Center. Totaltransit time and total X-ray exposure to the patients were calculated to assess the safetyprofile of the x-ray capsule imaging technology in human subjects. Results: All capsuleswere swallowed and naturally exerted by the volunteers without any minor or major sideeffect. The average transit time of 68 ±31 hours. The volunteers were exposed to an ultra-low total radiation dose (Average total exposure (0.03 ± 0.007 mSv), two orders of magnitudeless than CTC (with 1 outlier due to manufacturing fault). Data from scans in the coloncombined with ELS positioning information was used to reconstruct 3D colon segments inun-prepped colon. Fig1 and Fig.2 are examples of such 3D scans. Laboratory data formsynthetic colon phantoms with and without polyps as well as data from cow colon phantomwith induced tissue made polyp Fig.3 and Fig.4 have shown reconstruction accuracy of 2- 3 mm in colon diameter measurements. (All figure dimensions in mm) Conclusions: Asafety and proof of concept study has been performed using a novel prep-less x-ray imagingcapsule for colon cancer screening. Quantitative ultra-low dose x-ray 3D imaging wasachieved in the colon of human subjects. The efficacy will be confirmed in a multi-centerstudy.
S-142AGA Abstracts
809
In Vivo Colonic Insufflation via a Disposable CO2 Insufflation SystemKeith L. Obstein, Trisha Pasricha, Victoria R. Mitchell, Byron F. Smith, Pietro Valdastri
Background Colonoscopy (CLS) has made colorectal cancer a preventable disease. Despitethis fact, 7.5 million Americans per year decline recommended CLS—many whom citeperceived pain as a major deterrent. Carbon dioxide (CO2) for the purpose of colonicinsufflation during CLS has been found to greatly reduce procedural and post-proceduraldiscomfort; however, currently, the use of CO2 insufflation has not been widespread in theUnited States. One reason is the relative cost and maintenance of a CO2 system. Our teamhas developed a novel approach for administering CO2 insufflation during CLS that is low-cost and disposable. The success of this approach in vivo is unknown. Aim To assess a novelapproach for in vivo administration of CO2 insufflation during CLS. Methods The proposedmechanism provides CO2 insufflation in an on-demand fashion via delivery through theaccessory channel of a standard colonoscope. The device consists of a dual-barrel syringe,mixing nozzle and accessory channel adapter. As the syringe plunger is depressed, thereactants (sodium bicarbonate and citric acid) mix and produce sodium citrate, carbondioxide and water. The mechanism was assessed via two-tier validation: (1) benchtop setupto determine the total volume of CO2 production and (2) in vivo in a 40 Kg Yorkshireswine. The study protocol consisted of: (a) observing the colon under direct endoscopicvisualization (with air and suction off) and by fluoroscopy; (b) administering a single syringeof sodium bicarbonate and citric acid solutions; (c) steps a and b were repeated every 60seconds (s) for a period of 5 minutes (min). After 5 min, CO2 introduction was suspendedand colonic distention was documented by direct endoscopic visualization (with air andsuction off) and fluoroscopy every 60 s for the next 10 min. Necropsy was then performed.All reactants are FDA compliant. The study was approved by the local IACUC. Results Theproposed mechanism was found to generate a total of 507.01±0.25mL of CO2 duringbenchtop trials. In vivo trials confirm that the volume of CO2 generated by the device issufficient to allow for easy and adequate endoscopic visualization of the colon. Fluoroscopicimages demonstrate adequate colonic distention (mean diameter: 32.1±3.9 mm). There wasno evidence of colon perforation or mucosal damage. Conclusion Adequate CO2 insufflationof the colon using our novel disposable system is feasible, easily achieved and can beadministered without expensive electro-mechanical regulators or potentially dangerous high-pressure cylinders of CO2. This method of CO2 insufflation can be produced for penniesmore than a standard syringe and has the potential to enable a new class of low-cost CO2insufflation systems.
810
Successful Closure of Enteric Fistulas Using the Apollo Overstitch SuturingSystemMarc F. Catalano, Serge A. Sorser, Joseph B. Henderson, Shahid Ali, Antwan Atia
Enteric fistulas, a communication between two epithelialized surfaces, presents a difficulttherapeutic challenge. These fistulas cause significant clinical complications with a highdegree of morbidity & mortality directly or indirectly associated to fistulas has been describedas 10-20%. Enteric fistula classification includes, 1. enterocutaneous, 2. entero-atmospheric,3. entero-enteric. Etiology includes: postop/trauma, inflammatory (IBD, diverticular), malig-nant, radiation and ischemic. Treatment options include: 1. conservative, medical therapywith good nutrition, 2. drainage of infection/abscess, 3. fistula control, skin care, 4. surgicalclosure, 5. endoscopic (stenting, clips). Very few reports describe endoscopic suturing as atreatment option in this group of patients. Aim: To determine the feasibility of endoscopicclosure of enteric fistulas using the Apollo Overstitch Device.(Apollo Endosurgical, Aus-tin,Texas.) Methods: Procedure technique; initial tissue preparation for closure was doneby creating a surgical surface using a cautery device at the immediate perimeter of thefistula with subsequent maximal irritation achieved using a cleaning brush. Running and/
Recommended








![Formulation, Evaluation and Optimization of Osmotically ... · colon delivery capsule, CODESTM, osmotically controlled drug delivery system, pulsincap system, time clock system etc.[9]](https://img.pdfslide.us/doc/110x75/60124578e7baad691103f81b/formulation-evaluation-and-optimization-of-osmotically-colon-delivery-capsule.jpg)