Norovirus 3rd WHO Product Development for Vaccines
Advisory Committee Meeting (PDVAC) 8 June 2016
Ben Lopman, PhD
Division of Viral Diseases
Global Burden of Norovirus
• WHO Foodborne Disease Burden Epidemiology Reference Group (FERG)
• Global and regional age-stratified estimates of illnesses, deaths, and DALYs
• Total norovirus burden annually: – 685 million cases; 200 million in children <5 – 212,489 deaths; 54,214 in children <5 – 85% of illnesses and 99% of deaths occur in developing countries – $60 billion in direct health system costs and productivity loses
• Norovirus ranking as foodborne hazard: – #1 cause of foodborne illness – #4 cause of foodborne deaths – #5 cause of foodborne DALYs
Pires 2015 PLoS One; Kirk 2015 PLoS Med; Bartsch 2016 PLoS One
Key features: clinical
• Short incubation period
– 24-48 hours
• Acute-onset vomiting and/or diarrhea – Watery, non-bloody stools – Abdominal cramps, nausea, low-grade fever
• Most recover after 12-72 hours – ~10% seek medical attention; some require
hospitalization and fluid therapy – Severe illness and death in elderly and those
with underlying conditions
• 30% of infections are asymptomatic
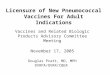
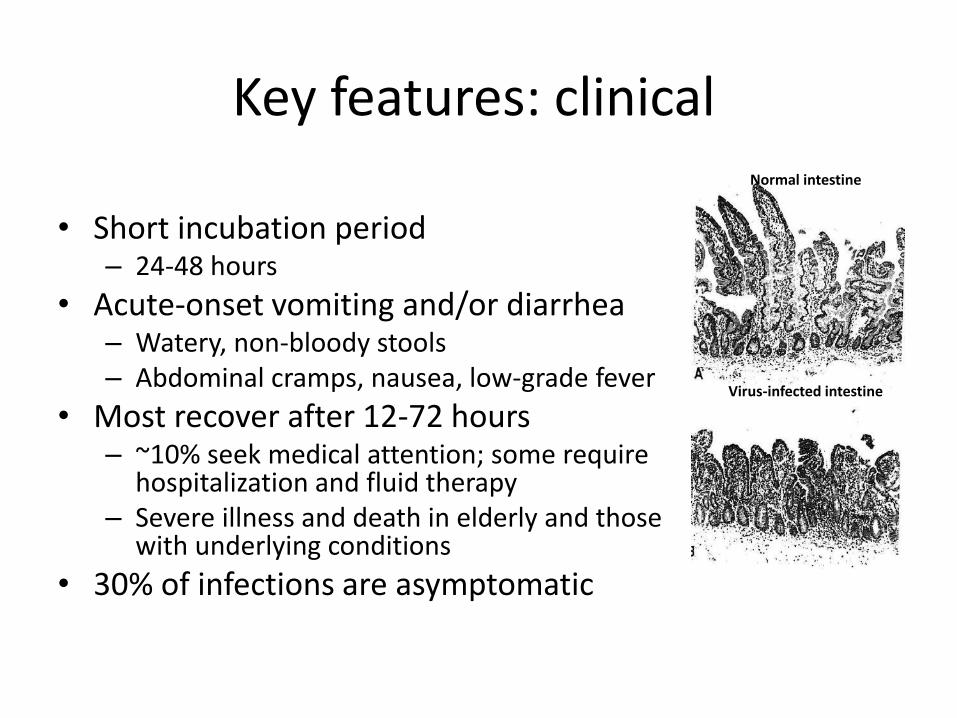
Normal intestine
Virus-infected intestine
Key features: virological
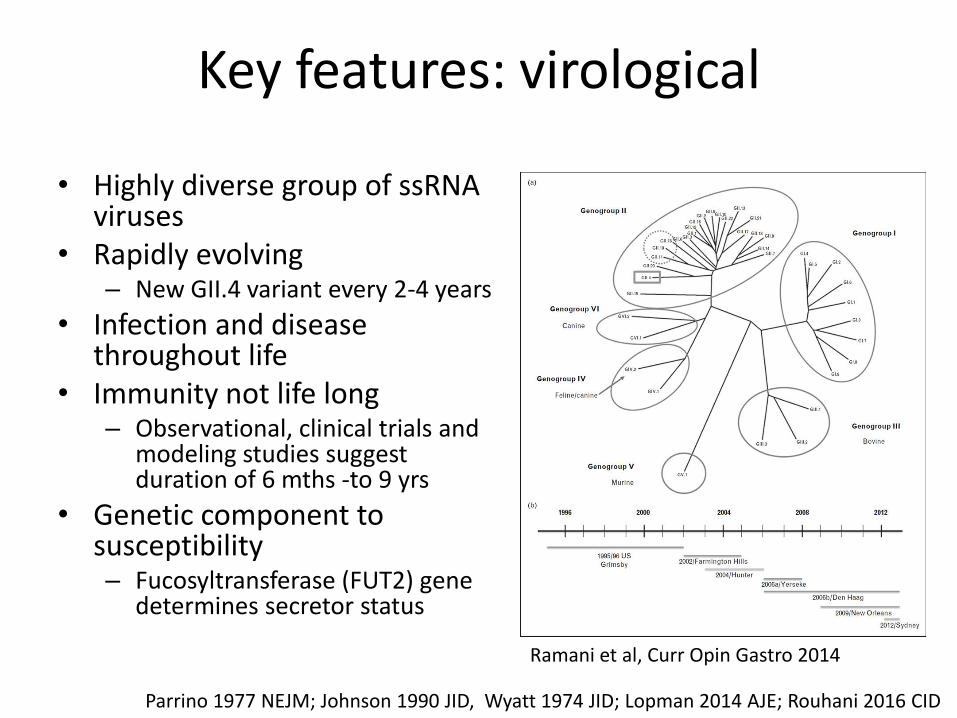
• Highly diverse group of ssRNA viruses
• Rapidly evolving – New GII.4 variant every 2-4 years
• Infection and disease throughout life
• Immunity not life long – Observational, clinical trials and
modeling studies suggest duration of 6 mths -to 9 yrs
• Genetic component to susceptibility – Fucosyltransferase (FUT2) gene
determines secretor status
Parrino 1977 NEJM; Johnson 1990 JID, Wyatt 1974 JID; Lopman 2014 AJE; Rouhani 2016 CID
Ramani et al, Curr Opin Gastro 2014
Progress in cell culture
• No small animal model – chimpanzees, swine, humanized mice
• Cell culture – Human B cells
• Jones et al., 2014 Science
– Human Intestinal Enteroids
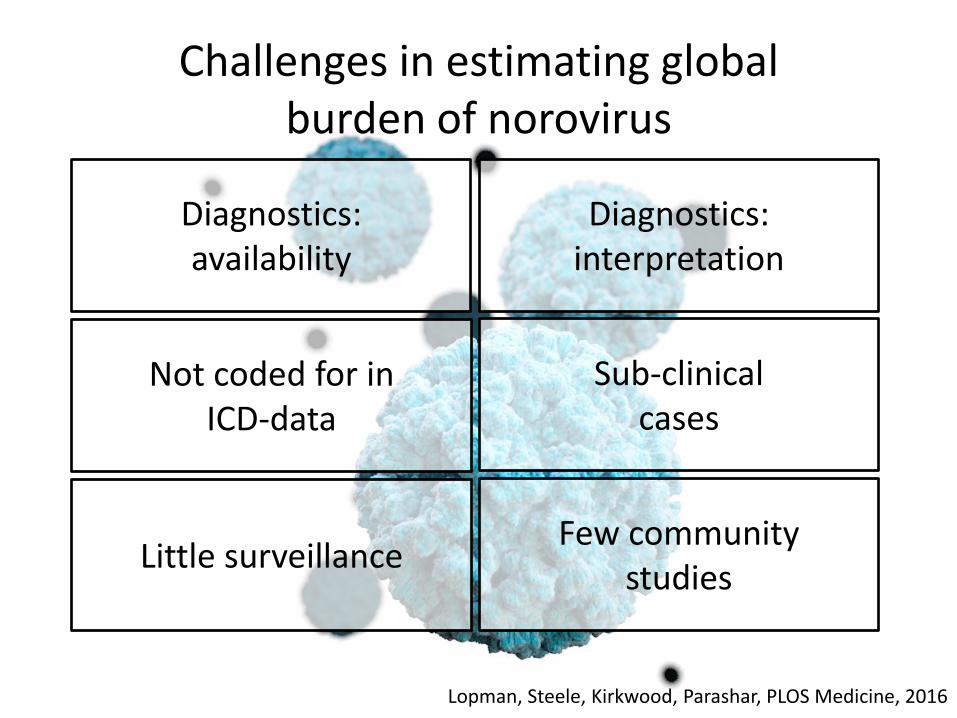
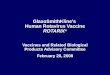
Challenges in estimating global burden of norovirus
Lopman, Steele, Kirkwood, Parashar, PLOS Medicine, 2016
Diagnostics: availability
Not coded for in ICD-data
Diagnostics: interpretation
Sub-clinical cases
Little surveillance Few community
studies
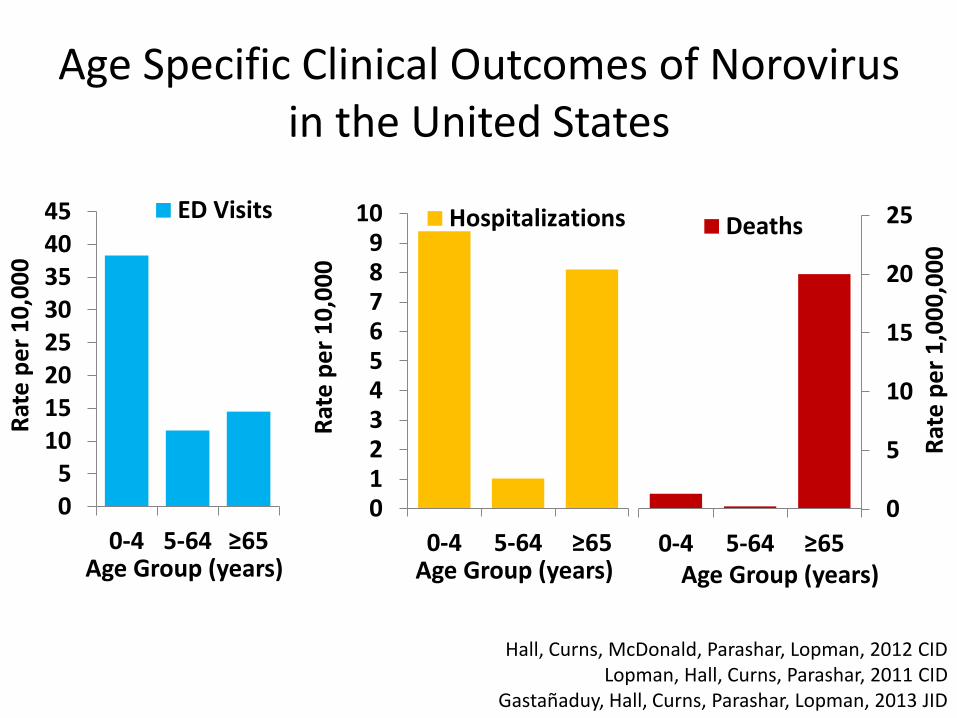
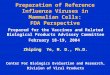
Age Specific Clinical Outcomes of Norovirus in the United States
05
1015202530354045
0-4 5-64 ≥65
Rat
e p
er
10
,00
0
Age Group (years)
ED Visits
0
5
10
15
20
25
0-4 5-64 ≥65
Rat
e p
er
1,0
00
,00
0
Age Group (years)
Deaths
Hall, Curns, McDonald, Parashar, Lopman, 2012 CID Lopman, Hall, Curns, Parashar, 2011 CID
Gastañaduy, Hall, Curns, Parashar, Lopman, 2013 JID
0123456789
10
0-4 5-64 ≥65
Rat
e p
er
10
,00
0
Age Group (years)
Hospitalizations
Potential strategies for norovirus vaccination
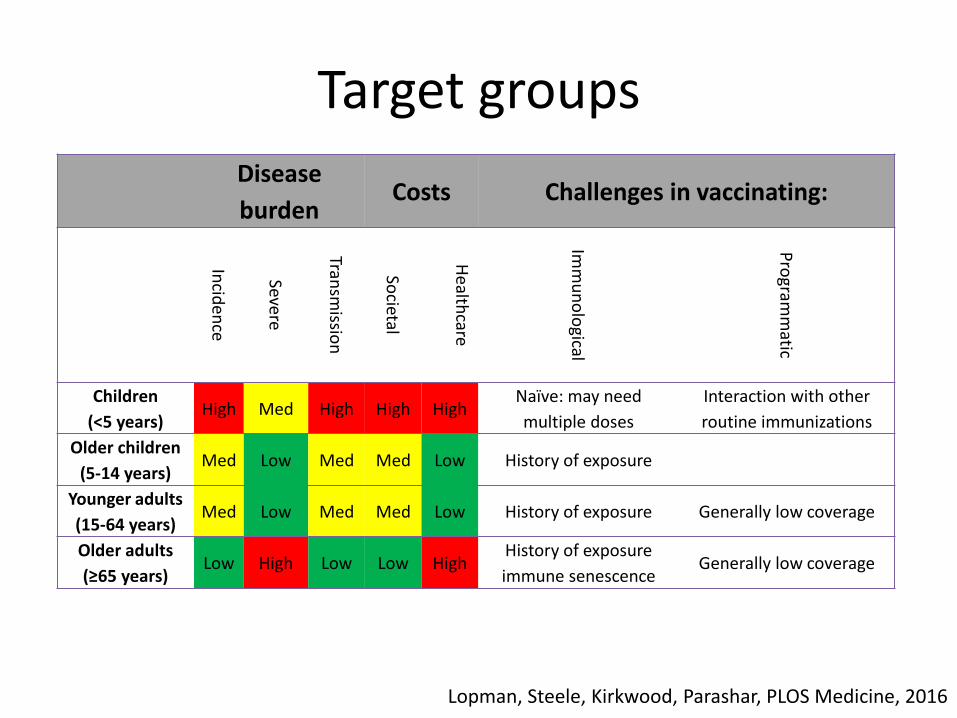
Target groups
Disease
burden Costs Challenges in vaccinating:
Incid
ence
Severe
Transm
ission
Societal
Health
care
Imm
un
olo
gical
Pro
gramm
atic
Children
(<5 years) High Med High High High
Naïve: may need
multiple doses
Interaction with other
routine immunizations
Older children
(5-14 years) Med Low Med Med Low History of exposure
Younger adults
(15-64 years) Med Low Med Med Low History of exposure Generally low coverage
Older adults
(≥65 years) Low High Low Low High
History of exposure
immune senescence Generally low coverage
Lopman, Steele, Kirkwood, Parashar, PLOS Medicine, 2016
Specific sub-population target groups for vaccination
• Healthcare workers
• Travelers
• Military personnel
• Immunocompromised
• Food service workers
Each group has unique epidemiological, economic and programmatic considerations
Norovirus vaccines
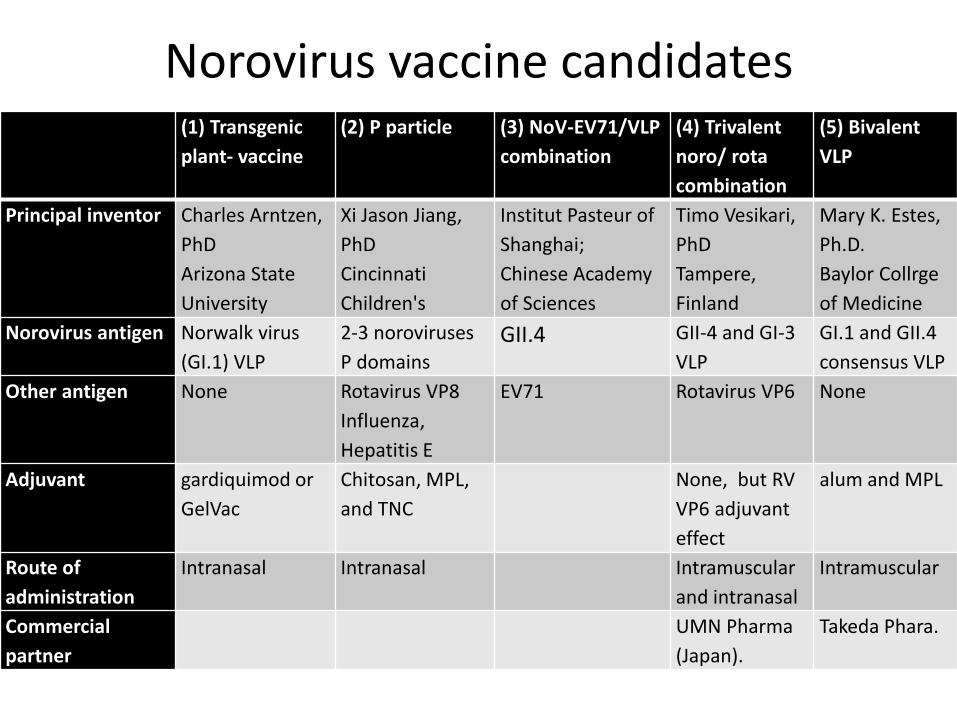
(1) Transgenic
plant- vaccine
(2) P particle (3) NoV-EV71/VLP
combination
(4) Trivalent
noro/ rota
combination
(5) Bivalent
VLP
Principal inventor Charles Arntzen,
PhD
Arizona State
University
Xi Jason Jiang,
PhD
Cincinnati
Children's
Institut Pasteur of
Shanghai;
Chinese Academy
of Sciences
Timo Vesikari,
PhD
Tampere,
Finland
Mary K. Estes,
Ph.D.
Baylor Collrge
of Medicine
Norovirus antigen Norwalk virus
(GI.1) VLP
2-3 noroviruses
P domains
GII.4 GII-4 and GI-3
VLP
GI.1 and GII.4
consensus VLP
Other antigen None Rotavirus VP8
Influenza,
Hepatitis E
EV71 Rotavirus VP6 None
Adjuvant gardiquimod or
GelVac
Chitosan, MPL,
and TNC
None, but RV
VP6 adjuvant
effect
alum and MPL
Route of
administration
Intranasal Intranasal Intramuscular
and intranasal
Intramuscular
Commercial
partner
UMN Pharma
(Japan).
Takeda Phara.
Norovirus vaccine candidates
Vesikari et al Trivalent norovirus/rotavirus
combination vaccine • Rationale: 2 most important causes of AGE in young children • Inactivated rotavirus vaccine could overcome safety and efficacy
challenges • Components:
– Norovirus: GII-4 and GI-3 VLP – Rotavirus: VP6 nanotubes
• Only animal studies – Suggest broad anti-norovirus and rotavirus response – Rotavirus VP6 may have adjuvant effect for norovirus
• Clinical development plan for – Phase I in adults – Phase I/II in older children – Phase II/III in young children
Blazevic et al, Hum Vaccin Immunother. 2016 Lappalainen et al, Arch Virol 2015
Malm et al, Clin Vaccine Immunol. 2015
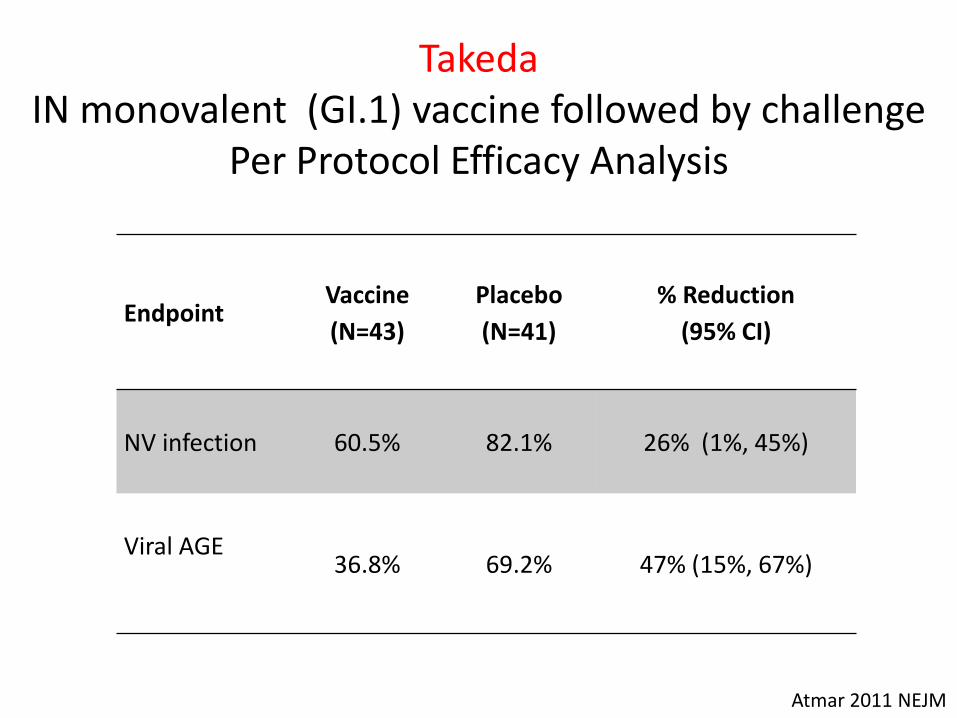
Takeda IN monovalent (GI.1) vaccine followed by challenge
Per Protocol Efficacy Analysis
Endpoint Vaccine
(N=43)
Placebo
(N=41)
% Reduction
(95% CI)
NV infection 60.5% 82.1% 26% (1%, 45%)
Viral AGE
36.8% 69.2% 47% (15%, 67%)
Atmar 2011 NEJM
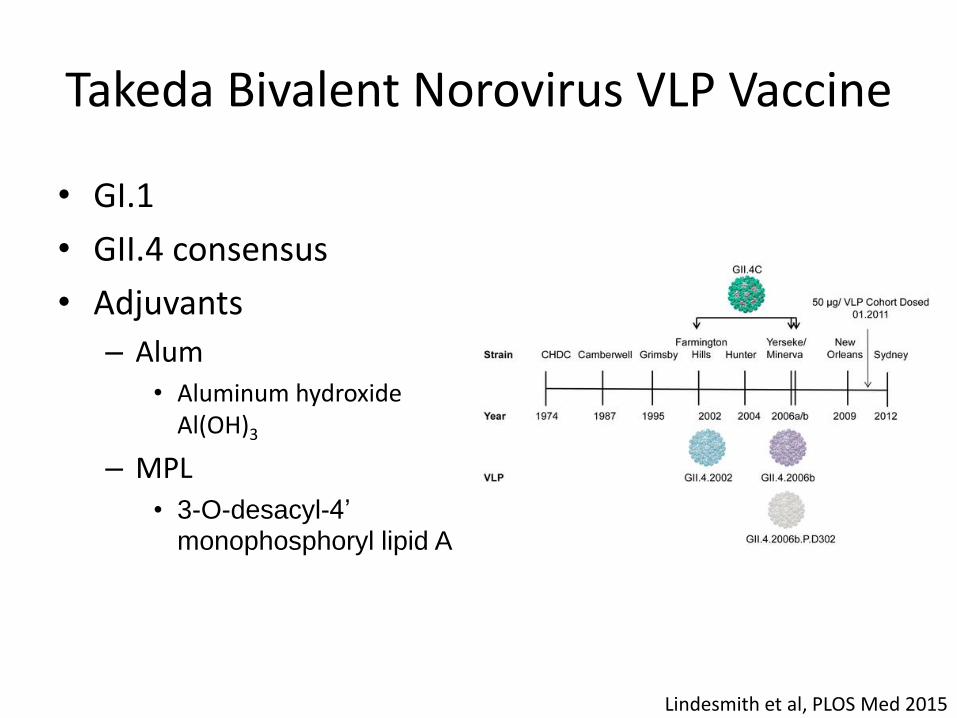
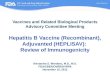
Takeda Bivalent Norovirus VLP Vaccine
• GI.1
• GII.4 consensus
• Adjuvants
– Alum • Aluminum hydroxide
Al(OH)3
– MPL
• 3-O-desacyl-4’ monophosphoryl lipid A
Lindesmith et al, PLOS Med 2015
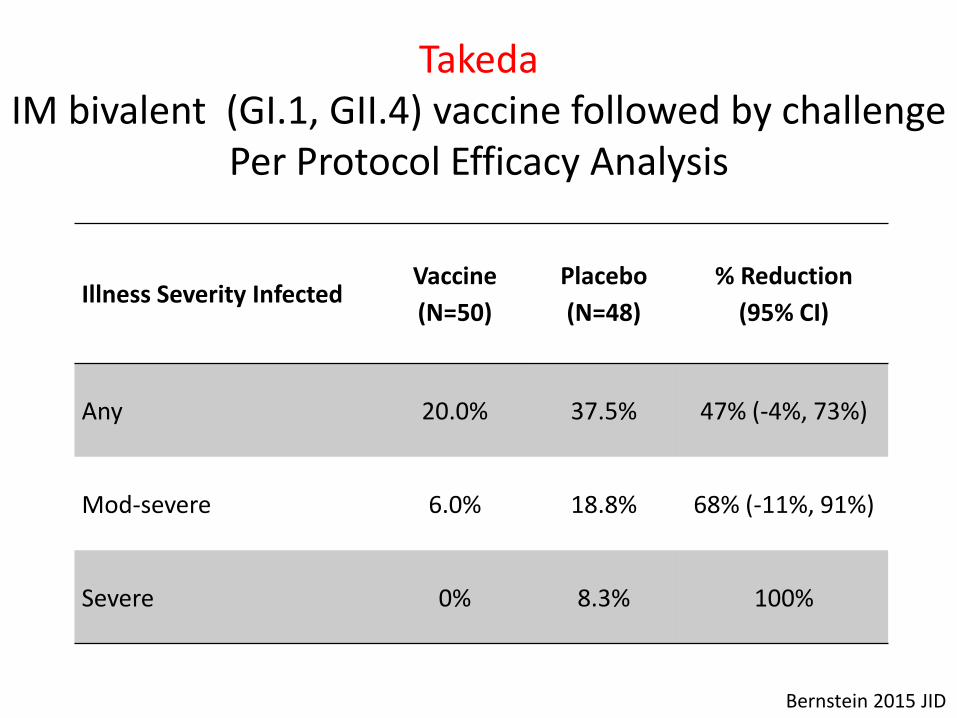
Takeda IM bivalent (GI.1, GII.4) vaccine followed by challenge
Per Protocol Efficacy Analysis
Illness Severity Infected Vaccine
(N=50)
Placebo
(N=48)
% Reduction
(95% CI)
Any 20.0% 37.5% 47% (-4%, 73%)
Mod-severe 6.0% 18.8% 68% (-11%, 91%)
Severe 0% 8.3% 100%
Bernstein 2015 JID
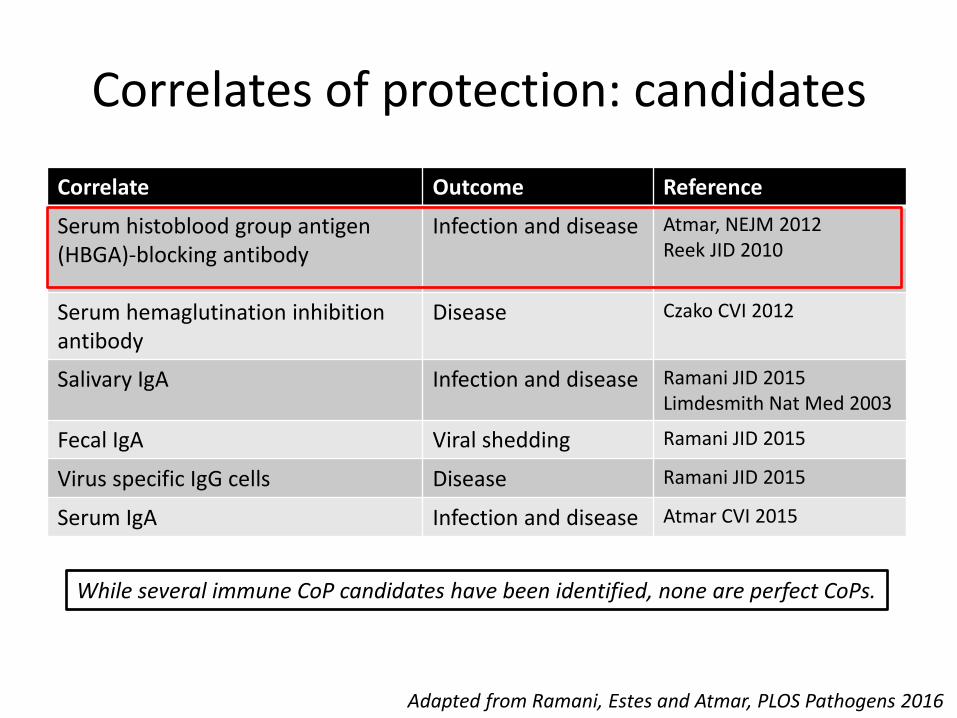
Correlates of protection: candidates
Correlate Outcome Reference
Serum histoblood group antigen (HBGA)-blocking antibody
Infection and disease Atmar, NEJM 2012 Reek JID 2010
Serum hemaglutination inhibition antibody
Disease Czako CVI 2012
Salivary IgA Infection and disease Ramani JID 2015 Limdesmith Nat Med 2003
Fecal IgA Viral shedding Ramani JID 2015
Virus specific IgG cells Disease Ramani JID 2015
Serum IgA Infection and disease Atmar CVI 2015
Adapted from Ramani, Estes and Atmar, PLOS Pathogens 2016
While several immune CoP candidates have been identified, none are perfect CoPs.
Challenges for a norovirus vaccine 1. Role of prior infection history?
2. Duration of protection?
3. Protection against multiple genotypes?
4. Need to be updated to keep up with viral evolution?
5. Need for different vaccine formulation for certain groups?
6. Variation in human genetic susceptibility?
http://www.cdc.gov/norovirus/downloads/global-burden-report.pdf
Weaknesses of current pipeline
• Only one product with any human efficacy data
• All data from generally healthy adults
• Under appreciated burden of disease
• Multiple potential target populations complicates clinical development plans
Remaining questions A role for WHO?
• Current data suggests noroviruses cause a large disease burden globally – Need for better data from many regions
• Leverage Global Rotavirus Surveillance Network
• Norovirus are diverse and rapidly evolving – Need for ongoing global norovirus surveillance to monitor trends and
emergence of new strains and their epidemiologic impacts
• Leverage Global Rotavirus Laboratory Network
• Initial trials of candidate vaccines show promise though several key issues require further study to develop effective norovirus vaccine program – Need for consensus of target groups for vaccination
Thank you
For more information please contact Centers for Disease Control and Prevention
1600 Clifton Road NE, Atlanta, GA 30333
Telephone: 1-800-CDC-INFO (232-4636)/TTY: 1-888-232-6348
Visit: www.cdc.gov | Contact CDC at: 1-800-CDC-INFO or www.cdc.gov/info
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Recommended