1
Physician Assisted Suicide and Palliative Care Update
Lesca Hadley MD, FAAFP, AGSF, CMD
Assistant Professor UNTHSC Institute for Healthy Aging: Center for Geriatrics
Geriatric Fellowship Program Director JPS Health Network
Objectives
Discuss the current state of Physician Assisted Suicide in the United States
Review latest recommendations from the National Consensus Guidelines for Palliative Care
Manage a request for Physician Assisted Suicide

2
CASE
Would you be willing to perform Physician Assisted Suicide?

3
DEFINING TERMS
• Suicide• Intentionally killing oneself
• Pulling the Plug • Discontinuing futile medical interventions that prolong
suffering during the dying process
• Refusing Treatment
• Physician Assisted Suicide (PAS) • Doctor prescribes a lethal dose of one or more
medications
EUTHANASIA
Ending the life of an individual suffering from a terminal illness or an incurable condition

4
Euthanasia
• Passive Euthanasia• Withholding or withdrawing medical interventions without
consent with the intent to cause death
• Active Euthanasia• Deliberate action to cause death of “suffering” patient
• Voluntary – Patient Consents
• Non-Voluntary – Patient Can’t Consent
• Involuntary – Patient refuses or can give consent but not asked
Washington v GlucksbergVacco v. Quill
Unanimous Ruling: No constitutional right to assisted suicide States may prohibit it
Supreme Court Ruling
• State Has Interest in• Preserving Life – No Sliding Scale• Preventing Suicide
• Protecting Integrity of Medical Profession
• Protecting Vulnerable from abuse, neglect, mistakes• Avoiding likely slippery slope
• Did not address• Protecting family members and loved ones
• Protecting people with disabilities

5
Supreme Court Ruling
• “Withdrawing treatment does not equal assisted suicide”
• Fundamental legal principle of causation• “When pt. refuses treatment, pt. dies of
underlying disease.”• “When pt. ingests lethal medication, he is
killed by that medication”• The doctrine of double effect does not equal
assisted suicide
Fundamental Legal Principle of Intentgal principle of intent
• Physician withdrawing or not starting treatment intends to respect patient’s wishes.
• Physician giving lethal medication intends to kill the patient.
Opening the door
for debate at the state level

6
States which have PAS Laws

7
Would you support Physician Assisted Suicide for a family member?
WOULD YOU ASK FOR PHYSICIAN ASSISTED SUICIDE OR EUTHANASIA FOR YOURSELF?
DEMOGRAPHICS

8
Patients who Access PAS Laws
• Well educated
• Excellent health care
• Good insurance
• Access to hospice, financial, emotional, and physical support
• Two out of three are aged 65 years or older
• Median age at death is 71 years.
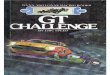
Patients who Access PAS: Oregon
0
10
20
30
40
50
60
70
80
90
100
Cancer ALS At home Hospice
Frequently Mentioned EOL Concerns
• Loss of autonomy 89.7 %
• Decreasing ability to participate in activities that made life enjoyable 91.6 %
• Loss of dignity 78.7 %

9
PROCESS FOR PAS
Physician Determines Residency Requirement
• State-issued ID or driver license
• Lease agreement or property ownership document
• State voter registration
• Recent state tax return
• No length-of-residency requirement

10
Additional Qualifications
• Mentally competent• Terminal illness • Self-administer medication • Two physicians must determine
if meeting criteria • Two oral requests• One written request
• Waiting periods• Can change mind• Confidential report• Not required
• Family notification• Psychiatric exam
Cautions
• Patient continues to receive the best possible palliative care coordinated with an interdisciplinary team
• Reasonable alternatives to PAD have been considered
• Use best available practices that limit avoidable suffering through the end of life
• If the request conflicts with the physician's values, the response should take into account professional obligations of non-abandonment and patient's ongoing clinical needs
Class C misdemeanor if no suicide or bodily injury results; state jail felony if suicide or attempted suicide with serious bodily injury
Texas Code 22.08

11
Do you support a state law allowing physician assistedsuicide??
Do you support a state law permitting euthanasia??

12
"We always listen to the patient. We never tell a patient:'This is what you have to do. You have no choice.' Yet atthe moment when their life is ending — when they say, 'Idon’t want to live in this bed for the next three weekswaiting to die' — it's an odd change in the consentprocedure. Suddenly they become wrong and webecome right. That does not make sense to me. Dyingshould not be completely separate from everything elsewe do in medicine."
Lonny Shavelson, MD, Head of the Bay Area End of Life Options Teams, author, and journalist
PHYSICIAN ASSISTED SUICIDE HAS BEEN PROHIBITED IN MEDICINE
FOR OVER 2000 YEARS
PHYSICIAN ASSISTED SUICIDE HAS BEEN PROHIBITED IN MEDICINE
FOR OVER 2000 YEARS
• History of Hippocratic Oath• The oath says the doctor “will
neither give a deadly drug to anybody if asked for it, nor will I make a suggestion to this effect”
• First “Do no harm”

13
Christian Beliefs Oppose PAS
• Human life is sacred because man is made in God’s image
• - Genesis 1:26
• God alone is sovereign over life and death
• Psalm 139:16
• People’s bodies belong to God - 1 Corinthians 6:19
• The Bible teaches that human dignity is inherent and not based on capabilities
JEWISH BELIEFS ABOUT PAS
We cannot sanction, favor or support the
legalization of physician-assisted
suicide.
Central Conference of American Rabbis
Central Conference of American Rabbis
MUSLIM BELIEFS A Doctor shall not take away life even when motivated by mercy. This is prohibited because this is not one of the legitimate indications for killing. Direct guidance in this respect is given by the Prophet's tradition: "In old times there was a man with an ailment that taxed his endurance. He cut his wrist with a knife and bled to death. God was displeased and said “My subject has hastened his end I deny him paradise.”
The Quran
The Quran

14
• “PAS is fundamentally inconsistent with the physician’s professional role as healer.”
• “The medical profession must redouble its efforts to provide optimal end of life care.”
• “The ANA prohibits nurses’ participation because these acts are in violation of the Code for Nurses and the ethical traditions and goals of the profession.”
• Nurses “have an obligation to provide humane, comprehensive and compassionate care that respects the rights of patients but upholds the standards of the profession in the presence of chronic, debilitating illness at end-of-life.
Studied neutrality on the subject of whether PAD should be legallypermitted or prohibited. However, as a matter of social policy, theAcademy has concerns about a shift to include physician-assisteddying in routine medical practice, including palliative care. Such achange risks unintended long-range consequences that may notyet be discernable, including effects on the relationship betweenmedicine and society, the patient and physician, and the perceivedor actual integrity of the medical profession. Any statuteslegalizing PAD and related regulations must include safeguards toappropriately address these concerns, such as limiting eligibility todecisionally capable individuals with a limited life expectancy.

15
PHYSICIAN ASSISTED SUICIDE
IS
DANGEROUS
Gives Physicians
Too Much Power
“My specialty is death” 60 min May 16, 1996

16
DANGEROUS FOR
PATIENTS
The Right to Die may become
The Duty to Die

17
Elderly in Holland in NH
IT IS DANGEROUS FOR
SOCIETY

18
SAFEGUARDSDON’T WORK
Lives Not Worthy to be Lived?

19
Systematic Approach to Evaluate PAD Requests• Determine the nature of the request
• Thoughts of ending life with no specific intent or plan? • Frustrated with living with illness?
• Clarify the cause(s) of intractable suffering• Loss of functional autonomy? • Severe pain or other unrelieved physical symptoms?
• Evaluate the patient's decision-making capacity• Explore emotional factors• Explore situational factors
• Poor social network? Exploitation or abuse?
COMMIT TO THE PATIENT THEINTENTION OF WORKINGTOWARD A MUTUALLYACCEPTABLE SOLUTION FORTHE PATIENT'S SUFFERING

20
Consider the Benefits and Burdens of other Alternatives
• Discontinuation of potentially life-prolonging treatments such as steroids, insulin, oxygen supplementation, dialysis, or medically assisted hydration and nutrition
• Voluntary cessation of oral intake if ethically acceptable to the patient and treating practitioners
• Palliative sedation, potentially to unconsciousness, if suffering is intractable and severe
Holistic care at the end of life requires pain and symptom control in addition to giving family,
spiritual and other needed support

21
Holistic Care
• Pain Management
• Palliative & Hospice Care
• Dx and Rx Depression
Palliative and Hospice Care
Department of HHS Centers for Medicare & Medicaid Services &the National Quality Forum Palliative Care DefinitionPatient and family-centered care that optimizes quality of life by anticipating, preventing, and treating suffering. Palliative care throughout the continuum of illness involves addressing physical, intellectual, emotional, social, and spiritual needs to facilitate patient autonomy, access to information, and choice
HOSPICEPalliative care for patients in their last year of life

22
NATIONAL CONSENSUS PROJECT CLINICAL PRACTICE GUIDELINES FOR QUALITY PALLIATIVE CARE
Third edition
Interprofessional Teamwork

23
CHOOSING WISELY AAHPMDon’t use topical lorazepam, diphenhydramine, haloperidol (“ABH”) gel for nausea.
CHOOSING WISELY AAHPMDon’t delay palliative care for a patient with serious illness who has physical, psychological, social or spiritual distress because they are pursuing disease-directed treatment.
FDA WarningAugust 31, 2016- Opioid pain and cough medicines combined with benzodiazepines
• Growing combined use of opioid medicines with benzodiazepines or other drugs that depress the CNS has resulted in serious side effects
• Slowed or difficult breathing and deaths
• FDA adding boxed warnings to the drug labeling of benzodiazepines and prescription opioid pain and cough medicines

24
FDA WarningMarch 22, 2016 Opioid pain medicines
• Potentially harmful interactions with numerous other medicines
• Problems with the adrenal glands
• Decreased sex hormone levels
• Required changes in labels to warn about these risks
Additional Resources
• http://www.stoppain.org/palliative_care/content/symptom/pain.asp
• http://www.EPERC.mcw.edu/EPERC/FastFactsandConcepts
• http://www.palliativemed.org

25
NATIONAL CONSENSUS PROJECT CLINICAL PRACTICE GUIDELINES FOR QUALITY PALLIATIVE CARE
Third edition
Consortium Organizations
• American Academy of Hospice and Palliative Medicine
• Center to Advance Palliative Care
• Hospice and Palliative Nurses Association
• National Hospice and Palliative Care Organization
• National Association of Social Workers
• National Palliative Care Research Center

26
Characteristics of Palliative Care Philosophy & Delivery NCP Guidelines
• Care is provided and services are coordinated by an interdisciplinary team
• Patients, families, palliative and non-palliative healthcare workers collaborate & communicate about care needs
• Services are available concurrently with or independent of curative or life-prolonging care
• Patient and family hopes for peace and dignity are supported throughout the course of illness, during the dying process , and after death
Structure and Processes of Care
• Emphasis on interdisciplinary team engagement and collaboration with patients and families
• Interdisciplinary team composition, qualifications, and support
• Emphasis on coordinated assessment and continuity of care across healthcare settings
• Quality assessment process and improvement
Physical Aspects of Care
• Assessment and treatment with appropriate validated tools
• Multidimensional management with pharmacological, interventional, behavioral, and complementary management
• Policies for treatment of pain and symptom management
• Safe prescribing of controlled substances

27
Psychological and Psychiatric Aspects
• Collaborative assessment process of psychological concerns and psychiatric diagnoses
• Patient-family communication on assessment, diagnosis, and treatment
• Options for common conditions in context of respect of goals of care of the patient and family
• Required elements of a bereavement program
Social Aspects of Care
• Interdisciplinary social work engagement and collaboration with patients and families to identify, support, and capitalize on patient and family strengths
Spiritual, Religious, and Existential Aspects of Care• Definition of spirituality, stressing assessment,
access, and staff collaboration in attending to spiritual concerns throughout the illness trajectory
• Interdisciplinary team, inclusive of an appropriately trained chaplain, to explore, assess, and attend to spiritual issues of the patients and family
• Promote spiritual and religious rituals practices for comfort and relief

28
Cultural Aspects of care
• Cultural competence for the interdisciplinary team, underscoring culture as a source of resilience and strength for patient and family
• Linguistic competence including plain language, literacy, and linguistically appropriate service delivery
Care of the Patient at the End of Life
• Communication and documentation of signs and symptoms of the dying process in the circle of care: the patient, the family, and all other involved health providers
• Assessment and management of pain and other symptoms
• Bereavement support beginning with anticipatory grief before the actual death and continuing through the actual death
Ethical and Legal Aspects of Care• Advanced care planning
• Team competencies in the identification and resolution of commonly encountered ethical issues are described, with emphasis on the importance of seeking advice and counsel from ethics committees
• Necessity of and access to expert legal counsel to navigate intricate and sensitive legal and regulatory issues

29
INSTITUTE FOR CLINICAL SYSTEMS IMPROVEMENTPalliative Care for Adults Guideline
50+ medical group and hospital members representing 9,000 physicians in Minnesota and surrounding areas, and is sponsored by five nonprofit health plans. Emphasized interprofessional teams
Recommended