3/24/2014
1
25‐G. Skin Care Considerations in IV Therapy—When the IV Site Becomes a
Wound
Janelle Flaherty, RD, CD, CNSC, Lead Clinical DietitianCoram Specialty Infusion Services, Littleton, CO
Kathleen Iacuone, RN, BSN, Branch Nurse ManagerCoram Specialty Infusion Services, Tampa, FL
Heather Marees, RD, Enteral SpecialistCoram Specialty Infusion Services, Littleton, CO
Debra Thayer, MS, RN, CWOCN, Senior Technical Service Specialist3M Critical and Chronic Care Solutions Division, St. Paul, MN
CE Credit in Five Easy Steps!1. Scan your badge as you enter each session.
2. Carry your Evaluation Packet to every session so you can add session evaluation forms to it.
3. Track your hours on the “Statement of Session Attendance Form” as you go.
4. At your last session, total the hours and sign both pages of your Statement of Session Attendance Form.
Keep the PINK copy for your records.
Put the YELLOW and WHITE copies in your Evaluation Packet.
Make sure a completed Session Evaluation Form is in your Evaluation Packet for each session you attended.
• Missing one? Extras are in a file near Registration.
5. Complete the General Attendance Evaluation Form located in your Evaluation Packet—and place it back in your envelope.
Write your name on the outside of your Evaluation Packet envelope, seal it, and drop it in the box near Registration.
Applying for Pharmacy CPE? If you have not yet registered for an NABP e‐Profile ID, please visit www.MyCPEmonitor.net to do so before submitting your packet.
You must enter your NABP e‐Profile ID in order to receive CE credit this year!
3/24/2014 2
Disclosure Slide
The speakers declares no conflicts of interest or financial interest in any service or product mentioned in this program.
Clinical trials and off‐label/investigational uses will not be discussed during this presentation.
3/24/2014 3
3/24/2014
2
Skin Care Considerations in Intravenous Therapy‐When The IV Site
Becomes A Wound
Debra Thayer, MS, RN, CWOCN, Senior Technical Service Specialist
3M Critical and Chronic Care Solutions Division, St. Paul, MN
How Often Does This Happen?
Why Is This a Problem?
http://creepypasta.wikia.com/wiki/Panic_Disorder
http://scrubsmag.com/letting‐go‐releasing‐nurses‐from‐the‐need‐to‐control/
Increased discomfortProcedure modification needed
Colonization/Increased risk of infection
InfectionCan't maintain a dressingFull thickness wound
3/24/2014
3
When Skin Damage Happens, There is a Tendency to Blame…
MARSI: Consensus Panel Definition
“A medical adhesive‐related skin injury is an occurrence in which erythema and/or other
manifestation of cutaneous abnormality (including, but not limited to, vesicle, bulla, erosion, or tear) persists 30 minutes or more after removal of the adhesive.”
Panel’s Conclusion: Healthcare providers should strive to prevent and reduce the incidence of MARSI, but first must be aware of the problem and its causes.

3/24/2014
4
http://cvcbundle.com/maximum‐barrier‐zone/chloraprep‐applicatorshttp://en.wikipedia.org/wiki/Peripherally_inserted_central_catheterhttp://www.ivteam.com/wp‐content/uploads/2009/09/mmmchg.jpg
For every complex problem there is an answer that is clear, simple, and wrong.
H. L. Mencken
To Understand Skin Integrity, We Must First Understand the Epidermis
Primary Functions
http://greatergood.berkeley.edu/article/item/hands_on_research
ProtectionHomeostasis

3/24/2014
5
http://greatergood.berkeley.edu/article/item/hands_on_research
http://www.cixip.com/index.php/page/content/id/1056
http://www.djc.com/news/co/12000280.html

3/24/2014
6
Epidermis-Five layers from the bottom up:1. Strata Germinativum (SG),2. Strata Spinosum (SS), 3. Strata Granulosum (SGR),4. Strata Lucidum (not pictured) 5. Strata Corneum (SC)
Stratum Corneum
SG
SS
SGR
Cross Section of Epidermis
The Stratum Corneum as a Barrier
• Old thinking– Compared to a brick
wall:• Bricks represent cells (corneocytes)
• Mortar represents intercellular lipids
–Ceramides
–Cholesterol–Fatty acids–and water
• New thinking
– Compared to highly responsive sponge
• Composition is the same but not a rigid structure
• Cells capable of changing shape
Corneocyte
Intercellular lipids and water
Keratin
Rawlings AV. Recent advances in skin ‘barrier’ research. J. Pharmacy and Pharmacology. 2010; 62: 671‐677.
Acid pH
– Protects against microorganisms
– Supports formation and maturation of epidermal lipids
– Supports barrier repair
Fore J.A. Review of Skin and the Effects of Aging on Skin Structure and Function. Ostomy Wound Management. 2006; 52(9): 24‐35.

3/24/2014
7
Permeation
• Affected by:
– Substance/Vehicle• Size of molecule
– Skin structure & characteristics
• Location
• Hydration
• Disease/damage
• Age (extremes)
– Diminished barrier integrity
– Prolonged barrier repair
But!
“Any topically applied chemical substance has the potential to induce an irritant or hypersensitization reaction in any individual at some time.”
Shelanski, Phillips and Potts. Intl J Dermatol 1996 35(2); 138.
Irritant Contact Dermatitis
Image courtesy of R. Huneke‐Rosenberg

3/24/2014
8
Irritant Contact Dermatitis
Image courtesy of R. Huneke‐Rosenberg
Allergic Contact Dermatitis
Allergic Contact Dermatitis

3/24/2014
9
What Happens When Skin Becomes Wet?
Increased permeability of Stratum corneum
Changes in skin PH
Inflammation
+
+
Friction Contributes to Skin Damage
When skin is wet
Moisture‐Associated Skin Damage (aka Maceration)
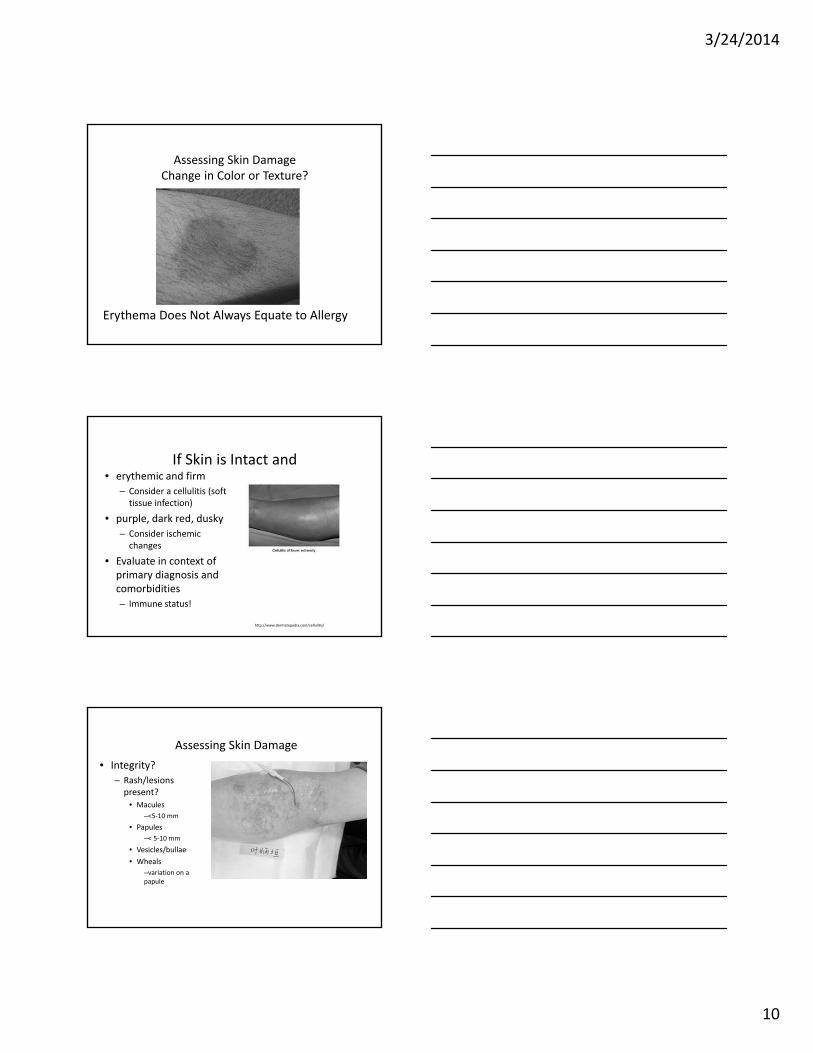
Assessing Skin DamageChange in Color or Texture?
3/24/2014
10
Erythema Does Not Always Equate to Allergy
Assessing Skin DamageChange in Color or Texture?
If Skin is Intact and • erythemic and firm
– Consider a cellulitis (soft tissue infection)
• purple, dark red, dusky
– Consider ischemic changes
• Evaluate in context of primary diagnosis and comorbidities
– Immune status!
http://www.dermatopedia.com/cellulitis/
Assessing Skin Damage
• Integrity?
– Rash/lesions present?
• Macules
–<5‐10 mm
• Papules
–< 5‐10 mm
• Vesicles/bullae
• Wheals
–variation on a papule

3/24/2014
11
Candidiasis
• Maculo‐papular or maculo‐pustular rash
• Central area of erythema
• Satellite lesions
http://www.webmd.boots.com/skin‐problems‐and‐treatments/guide/candidiasis‐yeast
Assessing Skin DamageIs There Tissue Loss?
Skin injury results when the skin to adhesive attachment
is stronger than the skin to skin attachment
skin
adhesivebacking
How Do Mechanical Adhesive Injuries Occur?

3/24/2014
12
• Epidermal-dermal junctionthinning
• Decreased collagen and elastin• Loss of fat
Increased risk of injury
Stripping +Friction + Contact Dermatitis
Mechanism of Damage
Shear force
Skin‐adhesive attachment > skin‐skin attachment
Epidermis pulls away from dermis
Secondary to “strapping” (i.e. stretching) &/or edema
Tension Blisters
3/24/2014
13
So, how do we prevent MARSI?
Selection of adhesive product
8. Select the most appropriate adhesive product based on its intended purpose, the anatomic location the adhesive will be applied to, and the ambient conditions present at the application site.
Medical Adhesive Tape/Dressing/Device Composition

3/24/2014
14
1. Adhesive profile over time
2. Surface tension
3. Skin cell removal
Acrylate adhesive
Silicone adhesive
Silicone adhesive Acrylate adhesives
Differences Between Acrylate and Silicone Adhesives
Skin Preparation is Critical
• Remove excess hair
“Respect the Prep”*
*E. Tardiff
3/24/2014
15
15. Consider application of a skin barrier prior to applying an adhesive product.
Skin Preparation
Is There Really a Difference Between Barrier Films?
Barrier films create protective interface‐not intended to increase adhesion!
Barrier Films• Formulations differ
– Polymer system• CHG compatibility?
– Solvent
• Alcohol vs alcohol‐free
– Fast drying?
– Non‐sticky?
– Presence of a plasticizer
– Sterile vs. non‐sterile
3/24/2014
16
2013 Data Presented at INS Annual Meeting
• “Role of skin protectant in reducing the local complications in PICC lines”– Sr. Mary George; Tata Memorial Hospital Mumbai India
– Looked at incidence of local complications (redness/rash, peeling, maceration, adhesive transfer)
• Incidence of skin peels:– Routine care bundle group‐42%
– Addition of alcohol‐free, terpolymer based film‐ 2%
16.Limit or avoid substances, such as compound tincture of benzoin, which increases the stickiness of adhesives.
Skin Preparation
Application and Removal
17.Use proper application and removal techniques for adhesive‐containing products.
3/24/2014
17
Will help prevent tension blistersRe‐dress site/re‐tape tubing if edema develops/increases
Firm pressure applied to the surface of medical tape will activate adhesive and increase
surface area contact
Medical Adhesives Are Pressure Sensitive
Application and Removal
18.Consider use of medical adhesive removers to minimize discomfort and skin damage associated with removal of adhesive products.
Considerations for IV site care?

3/24/2014
18
Removal Techniques• Remove adhesives slowly, keeping adhesive close to skin, back over itself in the direction of hair growth, while supporting adjacent skin/device
Superficial vs. Full thickness wounds
Injury
Hemostasis
Inflammation
Re-epithelialization Angiogenesis Connectivetissue repair
ContractionRemodeling
Healed wound
Granulation
3/24/2014
19
Wound Healing Impediments
• Intrinsic factors
– Age
– Perfusion
– Immune status
– Nutrition
– Co‐morbidities
• e.g. Diabetes, malignancy
• Wound‐related factors
– Infection
– Necrotic tissue/ foreign body
– Size
– Age
– Complexity
“Moist” Wound Healing?• First described
~1940• Winter’s publication-
Nature-1962 – Superficial wounds – Control group allowed
to dry– Experimental group
covered with thin plastic film-2x faster re-epithelialization
Wound Management Objectives
Manage impediments
Create an environment that supports healing
Prevent infectionPromote comfort
Preserve functionPreserve the vascular access site and function

3/24/2014
20
Interventions• Consult WOCN if you have one• Reevaluate and modify regimen• Suspect ACD? (erythema, vesicles, wheals, itching)‐discontinue
offending agent • For widespread mod. to severe dermatitis/partial thickness
damage consider omitting cytotoxic agents (CHG, PVI, alcohol) to affected area – cleanse with saline, meticulous sterile technique, q 24 hour
dressing change– steroid/antibiotic cream may interfere with transparent dressing
• For isolated area of partial thickness damage: – can prep around wound – modify size of securement dressing if wound at periphery or – consider combination of wound dressing to cover wound and
securement dressing
Dressing Pro Con
*Acrylic absorbent Can observe site Can’t cut
*Foam adhesive (+/‐silver)
Gentle Can’t view site
*Hydrocolloid Can’t view site; some leave residue; some are aggressive
Transparent film Secures catheter; conformable; can observe site
No absorbency
No one recipe for topical care
Plastic Surgery consult: deep/ complex woundDerm. consult: severe, refractory dermatitis, complex pt.
Mechanical Trauma+ Contact Dermatitis‐Resolving
Transparent dressing wear time consis. w INS guidelines (#46) re: freq of drsg change
3/24/2014
21
Skin Damage in Infusion Therapy…
• is a reality, but we lack data on prevalence and incidence
– Systemic and therapy‐related factors contribute
• Its not just about adhesives and allergy
– Contact dermatitis (both ICD and ACD), moisture‐associated skin damage and MARSI likely represent majority of damage
– Prevention is key!
• Several simple interventions can make a difference!
Thank [email protected]
CASE STUDY:Adhesives, Antibiotics, Hormones —
What Next?
Kathleen Iacuone, RN, BSN, Branch Nurse Manager
Coram Specialty Infusion Services, Tampa, FL
3/24/2014
22
Patient Background
• Hyperemesis patient, 34 years old
• 15 weeks’ gestation, second pregnancy
• Developed nausea at 5 weeks, emesis at 6 weeks
• NKA
• Minimal p.o. intake
• Weight loss of 12 pounds
• First pregnancy (currently a two‐year‐old girl)– Normal pregnancy/vaginal delivery w/o complications
– Mild nausea, no skin irritations or rashes
Treatments
– Ondansetron 1 mg/hr IV continuous infusion
– Total Parenteral Nutrition (TPN) with IV lipids
• 2,650 mL daily, 7 days a week
• Initiated at 24 hours, tapered to 12 hours daily
8/24: Site Documentation on Admission Visit
• Discharged from hospital with transparent semipermeable membrane (TSM) dressing in place– Securement device dry and intact from 8/23
– Antibacterial patch in place
– No signs or symptoms of irritation

3/24/2014
23
8/24: Admission Visit
• Initiated TPN and ondansetron infusion
• Conducted patient assessment
• Performed teach/train therapy
• Noted no skin irritations
8/25–9/25: Follow‐Up Weekly Visits
• RN conducted follow‐up teach and train for ondansetron and TPN
– 8/25: Patient complained of “itching on stomach and legs from tape used at hospital”
– Performed routine weekly visits for labs and PICC line dressing changes
– Reinforced teaching and signs/symptoms of infection, when to call RN/RPh for assistance
Adhesive Skin Irritant

3/24/2014
24
9/25: Risk of PICC Infection!
70© 2014 Coram LLC | Proprietary and Confidential |
PICC Infection Confirmed
• 9/25: Patient hospitalized after doctor appointment — temperature of 99.9°F
• 9/27: Increased fever/chills
• 9/28: PICC line culture confirmed for staph infection — PICC removed, vancomycinstarted
• 9/30: PICC replaced, patient discharged home on IV vancomycin, TPN, and ondansetron
PICC Site — Post‐Removal
3/24/2014
25
Changes of Technique
• 10/3–10/7: Patient reports to RN that PICC dressing “itching like crazy”
• Dressing changes bi‐weekly
• RN documents: “(Securement device) moved to allow dressing to be moved away from rash.”
• New rash developed after vancomycin infusion
• MD felt it may be an “adhesive skin reaction”
• Changed to a different TSM dressing
10/7: Documentation of Rash
• Communication train —Patient to Pharmacist to RN
Changes Noted 10/14–11/25
• Rash appears to change every 2 to 3 days without any consistency of improvement
• Spread to cheek/neck/chest
• Irritation seen under the removable edges of TSM dressing; edges removed
• Cortisone cream ordered for rash
• Changed skin antiseptic from chlorhexidine/alcohol to povidoneiodine/alcohol combination

3/24/2014
26
Neck and Chest Rash
PICC Infection #2 and Clot
• 11/27: Patient called — cap at end of PICC line fell off under sweater unnoticed, PICC exposed
• PICC site red in 5 cm diameter; MAC now increased from 28 cm to 29 cm
• MD notified, patient sent to hospital
• PICC removed, identified small clot; documented by hospital that systemic anticoagulation not necessary
• 12/7: New PICC, TPN weaned off
• Antibiotic IV cefazolin started and written for discharge, continued IV ondansetron
PICC Infection with Clot

3/24/2014
27
Change of Therapy
• For next 20 days, patient complained of intensity and spreading of rash to different areas of body, including PICC site
• 12/27: PICC removed due to severe redness around site
• Therapy changed to subcutaneous ondansetron
• MD discussing nasogastric (NG) tube placement for nutrition– Patient tolerating small amounts by mouth and maintaining weight
Angry Skin!
PUPPP Rash?
• Pruritic Urticarial Papules and Plaques of Pregnancy
• Description– Occurs in 1 out of 160 pregnancies
– Less common in African American women
– Cause and pathogenesis not known
– Suggestion of a relationship between skin distention
– Fetal cell DNA found in mother skin, and increased maternal weight gain
– Benign disorder• No known systemic complications
• No fetal mortality risk
– Severe pruritus is the most distressing feature

3/24/2014
28
PUPPP Rash? (cont.)
• Treatment
– No curative treatment for PUPPP (apart from delivery!)
– Palliative care
• Emollients (moisturizers)
• Topical steroids (applied thinly twice daily to red, itchy patches)
• Antihistamines (conventional antihistamine tablets appear safe in late pregnancy)
PUPPP Rash? (cont.)
• Resolution
– Typically resolves within four to six weeks, independent of delivery
– Does not usually recur with subsequent pregnancies
PUPP RASH

3/24/2014
29
January
• Continuation of subcutaneous ondansetron
• Hydration ordered via PIV for positive ketone’s in urine as needed
• Maintaining weight– Patient refused NG feeding
– Moderate by mouth intake
• Induction planned for February
Quinn Marie 2/10/148 pounds, 7 ounces
Thank [email protected]

3/24/2014
30
Enteral Case Studies
Janelle Flaherty, RD, CD, CNSC, Lead Clinical Dietitian and
Heather Marees, RD, Enteral Specialist
Coram Specialty Infusion Services, Littleton, CO
CASE STUDY #1
Gastrostomy Tube Site Infection
Background Information
• Male cancer patient, non‐compliant with tube feeding
• Seen daily at cancer treatment center for radiation
• Radiation RN primary caregiver
• Self‐proclaimed “couch surfer”
• Pain rated 12 on scale of 1‐10
3/24/2014 90
3/24/2014
31
Tube Site Care
• Split gauze around the stoma
• Bolster pulled away from skin surface
• H 2O2 for cleaning
• Checked by RN
3/24/2014 91
Reported Concerns
• Leaking at tube site
• Pain and redness at tube site
• Suspected excessive HCI production
3/24/2014 92
Interventions
• Nystatin BID (topical)
• Barrier cream BID (topical)
• Hydrocortisone 2% BID (topical)
• H2 blockers
• Corrected cleaning protocol
• Set bolster closer to skin
3/24/2014 93

3/24/2014
32
Week 1 Week 3 Week 5
Results
3/24/2014 94
CASE STUDY #2
Low‐Profile Button Site Infection
Background Information
• 25‐year‐old male cystic fibrosis patient on tube feeding for 10 years
• Low‐profile access device
• Changed providers due to insurance issues
• RD‐liaison noticed tube site abnormality
3/24/2014 96

3/24/2014
33
Reported Concerns
• Bright red inflammation
• Button appeared too big
• Reported leaking
3/24/2014 97
Interventions
• Nystatin BID (topical)
• Barrier cream BID (topical)
• Hydrocortisone 2% BID (topical)
• Replaced with correct button size
3/24/2014 98
Stoma Measuring Device
3/24/2014 99
Recommended