Poster Session II Hypertension, Diabetes, Prematurity, Physiology www.AJOG.org
disorders were defined by: 1) traditional criteria (ACOG, 2002), 2)atypical criteria (proteinuria or hypertension, with �1 additionalfinding - symptoms, plts <100K, LFTs>70, fetal growth delay), or 3)newly proposed criteria (ACOG, 2013). Severe adverse outcomeswere confirmed by chart review.RESULTS: 1,258 women were recruited, and of these 1,223 wereevaluable. Final diagnoses and pregnancy outcomes are shown inTable 1. Hypertension was the most common presenting sign (80%),but less than half of subjects had proteinuria. Of subjects < 35weeks, 61% ultimately met traditional criteria for preeclampsia,compared to only 33% at term. The proportion of atypical pre-eclampsia is roughly the same in each gestational age strata (10-21%). The new ACOG criteria increase the diagnosis of preeclampsiaby 17, 43, and 61%, in the three respective gestational age groups. Ofpatients presenting at less than 37 weeks, 68% were delivered pre-term. While the risk of SGA is significant in each gestational agegroup, fetal/neonatal loss and severe maternal adverse outcomeswere concentrated in women with early presentation and are rare.CONCLUSION: The PETRA study is a large, representative nationalcohort of women evaluated for suspected preeclampsia. The pre-senting signs and symptoms of such women are varied, and clinicalclassification systems do not accurately predict severe adverse out-comes, and may lead to over-intervention. There is an urgent needfor improved risk stratification with appropriate biomarkers.
Characteristics and outcomes of womenpresenting with suspected preeclampsia
Data reported as median (IQR) or n (% of N); PE-preeclampsia, MAO-
maternal adverse outcome (abruption, renal failure, pulmonary edema/
distress, fatty liver, TTP, DIC, stroke, and retinal detachment).
242
The risk of hypertensive disorders of pregnancy withexpectant management at termKelly Gibson1, Thaddeus Waters2, Jennifer Bailit11MetroHealth Medical Center, Case Western Reserve University School ofMedicine, Obstetrics and Gynecology, Cleveland, OH, 2Loyola UniversityMedical Center, Obstetrics and Gynecology, Maywood, ILS130 American Journal of Obstetrics & Gynecology Supplement to JANUARY
OBJECTIVE: Non-medically indicated induction (NMII) prior to 39weeks gestation is discouraged due to concerns for neonatalmorbidity. However, little data exist on the maternal risks of pro-longing term pregnancy. We evaluated the frequency of developinghypertensive disorders of pregnancy in term low risk patients whohad an NMII or were expectantly managed.STUDY DESIGN: This is a retrospective cross-sectional study from 19US hospitals, 2002 to 2008 (Safe Labor Consortium). Women withviable, vertex, singleton pregnancies at 37 to 41 weeks were included.Women with a history of hypertension, diabetes mellitus, cardio-vascular disease, prior uterine surgery, planned cesarean delivery, orfrom centers with incomplete hypertensive data were excluded.Women with NMII in each week were compared to women managedexpectantly without NMII until the next week of gestation orbeyond. The primary outcome was the frequency of developinghypertensive complication (gestational hypertension (GHTN), pre-eclampsia (PE), or eclampsia (EC)). As the risk of hypertensivecomplications was 0% by definition in the NMII group, statisticalcomparisons were not performed.RESULTS: Of 121,466 low risk deliveries, 12,780 (10.5%) had NMII.The cohort was 49.2% nulliparous, 51.0% Caucasian, obese (meanBMI 30.2� 5.7 kg/m2), and a mean gestational age of 39.2�1.1 wks.The risk of developing any hypertension in expectantly managedwomenwas 4.1% at 37 weeks, 3.5% at 38 weeks, 3.2% at 39 weeks, and2.6% at 40 weeks. When evaluating the cases expectantly managed butwho delivered within the same week, the frequency of hypertensivecomplications were: 9.2% in the 37th week (4.5% GHTN, 6.2% PE,0.1% EC); 6.5% in the 38th week (3.2% GHTN, 4.3% PE, 0.03% EC);4.6% in the 39thweek (2.1%GHTN, 3.1%PE, 0.03%EC), and 3.9% inthe 40th week (1.6% GHTN, 2.7% PE, 0.03% EC).CONCLUSION: For women expectantly managed at term, there is amaternal risk of developing hypertensive complications (2.6-9.2%)for each week in a low risk population.
243
Thrombin increases the production of sFlt1 in primarycultured cytotrophoblasts while angiotensin II and TNF-ahave no effectChao Li1, Christie Thomas21University of Iowa, OB/GYN, Iowa City, IA, 2University of Iowa,Nephrology, Iowa City, IAOBJECTIVE: Soluble fms-like tyrosine kinase 1 (sFlt1) plays animportant role in the development of preeclampsia. sFlt1 is made inlarge amounts by the placental cytotrophoblasts (CTB). The produc-tion mechanism of sFlt1 is still unclear. Previous studies had shownthat thrombin and angiotensin II could stimulate the production ofsFlt1. Also there were studies showed a possible link between theproduction of tumor necrosis factor a (TNF- a) and sFlt1. The pre-vious studies have been done in animal model, cell lines and placentavillous explants. None of the studies were done on humanCTB. In thisstudy, we tested the effect of thrombin, angiotensin II and TNF- a onthe production of sFlt1 in primary cultured human CTB.STUDY DESIGN: Human CTB was isolated from placentas of un-complicated pregnancy delivered at 37-40 weeks gestation. The CTBwas preconditioned with 8% oxygen for 24 hours then was treatedwith thrombin (1,5,10 u/ml), angiotensin II (1uM) and TNF- a(10ng/ml) for another 24 hours. Elisa was used to test sFlt1 inconditioned medium. qRT-PCR was used to test sFlt1 mRNA. Theexperiments were repeated at least 3 times. Each sample wasanalyzed in triplicates. Statistics: Student T-test. One way Anova.RESULTS: Thrombin stimulates the production of sFlt1 (Figure 1). Theeffect is significant at 1u/ml (p<0.05) and peaks at 5u/ml (P< 0.01
2014
www.AJOG.org Hypertension, Diabetes, Prematurity, Physiology Poster Session II
comparing to 1u/ml) (Figure 2). There is no different in effect between5u/ml and 10u/ml. The expression of sFlt1 mRNAwas also increased(P<0.05) by thrombin (Figure 3). Angiotensin II and TNF- a have nosignificant effect on the production of sFlt1 (Figure 1).CONCLUSION: Thrombin stimulates the production of sFlt1 in a dosedependent fashion in primary cultured human CTB. Angiotensin IIand TNF- a have no effect on the production of sFlt1 in human CTBeven at a high concentration. The discrepancy between our resultsand previous studies may be secondary to the different study modelsand unadjusted oxygen concentrations in previous studies.
Supplem
244
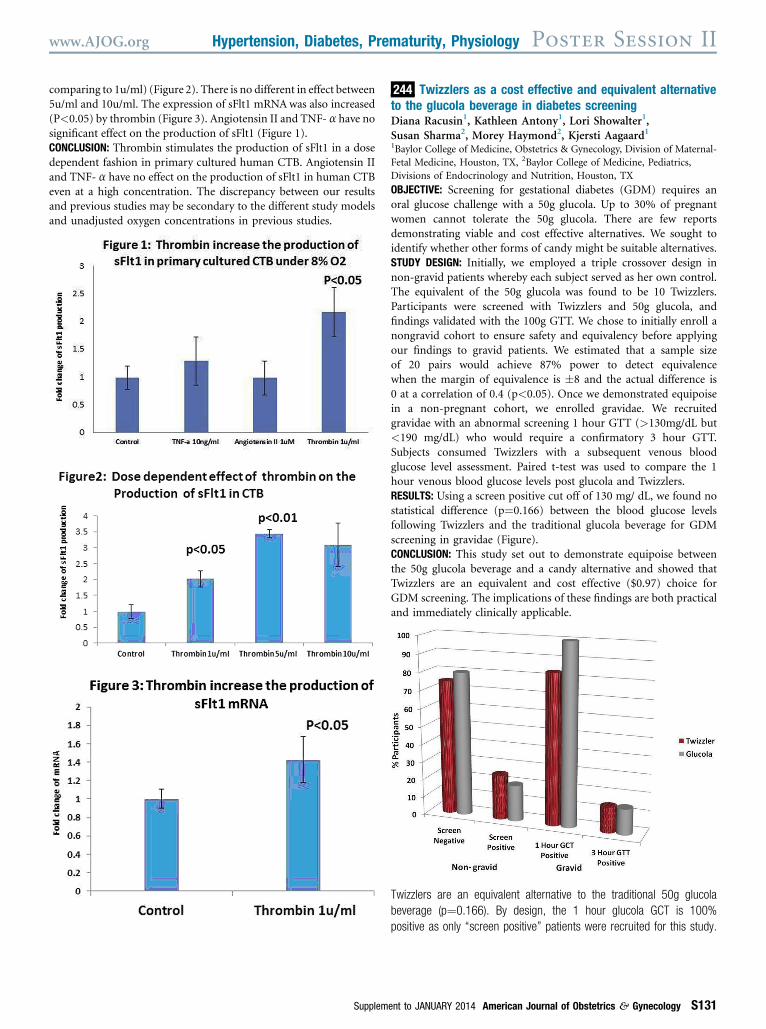
Twizzlers as a cost effective and equivalent alternativeto the glucola beverage in diabetes screeningDiana Racusin1, Kathleen Antony1, Lori Showalter1,Susan Sharma2, Morey Haymond2, Kjersti Aagaard11Baylor College of Medicine, Obstetrics & Gynecology, Division of Maternal-Fetal Medicine, Houston, TX, 2Baylor College of Medicine, Pediatrics,Divisions of Endocrinology and Nutrition, Houston, TXOBJECTIVE: Screening for gestational diabetes (GDM) requires anoral glucose challenge with a 50g glucola. Up to 30% of pregnantwomen cannot tolerate the 50g glucola. There are few reportsdemonstrating viable and cost effective alternatives. We sought toidentify whether other forms of candy might be suitable alternatives.STUDY DESIGN: Initially, we employed a triple crossover design innon-gravid patients whereby each subject served as her own control.The equivalent of the 50g glucola was found to be 10 Twizzlers.Participants were screened with Twizzlers and 50g glucola, andfindings validated with the 100g GTT. We chose to initially enroll anongravid cohort to ensure safety and equivalency before applyingour findings to gravid patients. We estimated that a sample sizeof 20 pairs would achieve 87% power to detect equivalencewhen the margin of equivalence is �8 and the actual difference is0 at a correlation of 0.4 (p<0.05). Once we demonstrated equipoisein a non-pregnant cohort, we enrolled gravidae. We recruitedgravidae with an abnormal screening 1 hour GTT (>130mg/dL but<190 mg/dL) who would require a confirmatory 3 hour GTT.Subjects consumed Twizzlers with a subsequent venous bloodglucose level assessment. Paired t-test was used to compare the 1hour venous blood glucose levels post glucola and Twizzlers.RESULTS: Using a screen positive cut off of 130 mg/ dL, we found nostatistical difference (p¼0.166) between the blood glucose levelsfollowing Twizzlers and the traditional glucola beverage for GDMscreening in gravidae (Figure).CONCLUSION: This study set out to demonstrate equipoise betweenthe 50g glucola beverage and a candy alternative and showed thatTwizzlers are an equivalent and cost effective ($0.97) choice forGDM screening. The implications of these findings are both practicaland immediately clinically applicable.
Twizzlers are an equivalent alternative to the traditional 50g glucola
beverage (p¼0.166). By design, the 1 hour glucola GCT is 100%
positive as only “screen positive” patients were recruited for this study.
ent to JANUARY 2014 American Journal of Obstetrics & Gynecology S131
Recommended