1
Inherited Oral DiseasesInherited Oral DiseasesDisorders Affecting Periodontium/Gingiva• Papillon-LeFèvre Syndrome• Cyclic Neutropenia
Disorders affecting Jaw bones and Facies
• Cherubism• Cleidocranial dysplasia• Gardner syndrome• Mandibulofacial dysostosis
(Treacher-Collins syndrome)• Nevoid basal cell carcinoma
syndrome• Osteogenesis Imperfecta• Aperts Syndrome• Crouzon Syndrome
Disorders affecting Oral Mucosa• Hereditary Hemorrhagic Telangiectasia• Multiple Endocrine Neoplasia
Syndrome IIB• Neurofibromatosis• Peutz-Jeghers Syndrome• White Sponge Nevus
Disorders of Teeth• Amelogenesis Imperfecta• Dentinogenesis Imperfecta• Dentin Dysplasia• Hypohidrotic ectodermal dysplasia• Hypophophatasia• Vitamin D deficient rickets
Papillon-LeFèvre Syndrome
• Autosomal Recessive• Cathepsin C gene mutation which affects the immune
response to infection
• Hyperkeratosis of the palms and feet• Sometimes elbows and knees• Dramatic periodontitis (periodontoclasia) of both
dentitions – Floating teeth– DD: Langerhans’ cell disease
Teeth erupt in normal sequence, position and time
1.5 to 2 years, a severe gingivo-periodontal inflammatory process develops
Edema, bleeding, alveolar bone resorption, and mobility of teeth withconsequent exfoliation
Teeth are lost in the sequence they are erupted. After loss of last teeth,gingiva regains a normal appearance
Permanent teeth are lost before 14 years
Peripheral blood neutrophil is depressed in all patients with Papillon-Lefèvresuggesting that neutrophils are important factor in pathogenesis of severeperiodontal disease
Papillon-LeFèvre Syndrome
Retinoid therapy: Improves the skin condition but not the periodontal therapy
Periodontal condition: No effective treatment
Treatment

2
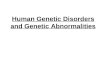
Cherubism
• Autosomal dominant• Facial appearance similar to “cherub”-like• 2 – 5 yrs of age• The clinical alterations typically progress until puberty,
stabilize and slowly regress• Bilateral involvement of the posterior mandible – most
common appearance – “cherub”-like (all 4 quadrants)• “Eyes upturned to heaven” appearance – due to involvement
of the infraorbital rim and orbital floor• Painless bilateral expansion of the post. mand.• Marked widening and distortion of alveolar ridges• Tooth displacement and eruption failure
Radiographic features• Multilocular radiolucency with massive expansion• Both erupted and unerupted teeth are randomly distributed• After stabilization, lesions exhibit a “ground glass” appearanceHistopathology• Similar to giant cell granuloma• But clinical and radiographic correlation necessary• Vascular fibrous tissue and giant cells (smaller and
more focal)• Eosinophilic cuffing around blood vesselsTreatment• Prognosis is unpredictable• Delayed till after puberty (curettage)
Cherubism

3
CleidocranialCleidocranial DysplasiaDysplasia
Caused by a defect in Cbfa1/Runx2 geneCaused by a defect in Cbfa1/Runx2 gene
Autosomal dominant and sporadic patternAutosomal dominant and sporadic pattern
Bone defects involve the clavicle and skullBone defects involve the clavicle and skullClavicles are absent (unilateral or bilateral) Clavicles are absent (unilateral or bilateral) –– 10% of cases10% of cases
Short stature with large heads; ocular Short stature with large heads; ocular hypertelorismhypertelorism; broad; broadbase of nose and depressed nasal bridgebase of nose and depressed nasal bridge
Large heads and parietal bossingLarge heads and parietal bossing
Skull sutures show delayed closure and may remain openSkull sutures show delayed closure and may remain open
Dental manifestations include narrow, highDental manifestations include narrow, high--arched palatearched palatewith increased prevalence of cleft palate with increased prevalence of cleft palate

4
Presence of numerous unerupted permanent andPresence of numerous unerupted permanent andsupernumery teeth with many distorted crown and root shapessupernumery teeth with many distorted crown and root shapes
Prolonged retention of deciduous teeth and delay or completeProlonged retention of deciduous teeth and delay or completefailure of eruption of permanent teethfailure of eruption of permanent teeth
Histology:Histology:Unerupted permanent teeth lack secondary cementum Unerupted permanent teeth lack secondary cementum
Treatment:Treatment:No treatment; fullNo treatment; full--mouth extractions with denture construction;mouth extractions with denture construction;removal of primary and supernumery teeth followed byremoval of primary and supernumery teeth followed byexposure and orthodontic treatment of permanent teethexposure and orthodontic treatment of permanent teeth
CleidocranialCleidocranial DysplasiaDysplasia
CrouzonCrouzon Syndrome (Craniofacial Syndrome (Craniofacial DysostosisDysostosis))
CraniosynostosisCraniosynostosis: Premature closure of sutures: Premature closure of sutures
Mutation in FGFR2; 1 in 65,000 births; ADMutation in FGFR2; 1 in 65,000 births; AD
Wide variation in clinical presentation: Wide variation in clinical presentation: BrachycephalyBrachycephaly;;scaphocephalyscaphocephaly; ; trigonocephalytrigonocephaly; ; ““cloverleafcloverleaf”” skull (skull (kleeblattschkleeblattschäädeldel))
Ocular Ocular proptosisproptosis: blindness and hearing deficit: blindness and hearing deficit
Headaches; normal intelligenceHeadaches; normal intelligence
Underdeveloped maxilla: Underdeveloped maxilla: MidfaceMidface hypoplasia; crowding ofhypoplasia; crowding ofmaxillary teeth; bifid uvulamaxillary teeth; bifid uvula
““Beaten metalBeaten metal”” skull in radiographsskull in radiographs
Surgical treatmentSurgical treatment

5
ApertsAperts Syndrome (Syndrome (AcrocephalosyndactylyAcrocephalosyndactyly))
CraniosynostosisCraniosynostosis syndromesyndrome
Mutation in FGFR2; 1 in 65,000 to 160,000 births, ADMutation in FGFR2; 1 in 65,000 to 160,000 births, AD
AcrobrachycephalyAcrobrachycephaly (tower skull); (tower skull); kleeblattschkleeblattschäädeldel (severe cases)(severe cases)
Ocular Ocular proptosisproptosis; ; hypertelorismhypertelorism; vision loss; ; vision loss; ““beaten metalbeaten metal””radiographsradiographs
MidfaceMidface hypoplasia; hypoplasia; ‘‘VV””--shaped arch shaped arch ““openopen--mouthmouth”” feature;feature;hearing losshearing loss
SYNDACTYLY of the 2SYNDACTYLY of the 2ndnd, 3, 3rdrd and 4and 4thth digits; MENTAL RETARDATIONdigits; MENTAL RETARDATION
Pseudo cleft palate due to swellings (accumulation of Pseudo cleft palate due to swellings (accumulation of glycosglycos--aminoglycansaminoglycans) of the lateral hard palate and crowding of) of the lateral hard palate and crowding ofmaxillary teeth; bifid uvulamaxillary teeth; bifid uvula
Surgery Surgery

6
TreacherTreacher--Collins Syndrome (Collins Syndrome (MandibulofacialMandibulofacial DysostosisDysostosis))
Defects of 1Defects of 1stst and 2and 2ndnd BABA
AD; 1 in 25,000 to 50,000 births; 60% new mutationsAD; 1 in 25,000 to 50,000 births; 60% new mutations
Mutations in the TCOF1 geneMutations in the TCOF1 gene
Characteristic face: Characteristic face: HypoplasticHypoplastic zygomazygoma causing narrow face withcausing narrow face withdepressed cheeks and downward slanting depressed cheeks and downward slanting palpebralpalpebral fissuresfissures
ColobomaColoboma (notch) at the outer portion of lower eyelid(notch) at the outer portion of lower eyelid
Ears anomalies: Deformed Ears anomalies: Deformed pinnaepinnae, extra ear tags, middle ear, extra ear tags, middle earossicle defects cause hearing lossossicle defects cause hearing loss
Underdeveloped mandible; Underdeveloped mandible; condylecondyle and and coronoidcoronoid hypoplasiahypoplasia
Lateral facial Lateral facial cleftingclefting and cleft palateand cleft palate
No treatment required in most cases; Cosmetic surgery inNo treatment required in most cases; Cosmetic surgery insevere casessevere cases

7
Multiple Nevoid Basal Cell Carcinoma Syndrome (Gorlin
Syndrome)• A.D.; high penetrance, variable expressivity• patched mutation, chr. 9• Chief characteristics: multiple basal cell
carcinomas, odontogenic keratocysts, epidermal cysts, palmar/plantar pits, calcified falx cerebri, rib anomalies, hypertelorism
• Less common: strabismus, kyphoscoliosis, CNS tumors
Multiple Nevoid Basal Cell Carcinoma Syndrome (Gorlin
Syndrome)• Face: Frontal and temporoparietal bossing
(big head), hypertelorism, mild mandibular prognathism
• Skin: Basal cell carcinomas even in children and adolescence, often on non-sun exposed skin, few to hundreds; plantar and palmarpits (retardation of the epithelial growth)
• Skeletal: bifid ribs, kyphoscoliosis• More than one odontogenic keratocysts

8

9
Neurofibromatosis(von Recklinghausen disease of
the skin)
• A.D.; 50% of cases are new mutations; 1:3,000 births
• Many forms• NF1 most common; chr. 17• Malignant transformation
Neurofibromatosis(von Recklinghausen disease of the skin)
• Diagnostic criteria (2 or more needed)– Six or more café au lait macules over 5mm in
prepubertal and 15mm in postpubertal– Two NFs or one plexiform NF– Axillary freckles (Crowe’s sign)– Optic glioma– Lisch nodules (brown pigmented spots of the iris)– Distinct osseous lesions (thinning of long bone cortex)– 1st degree relative with 2 or more of these findings
Neurofibromatosis(von Recklinghausen disease of
the skin)
• Oral lesions– NFs anywhere– Enlargement of fungiform papillae– Enlargement of mandibular foramen– Enlargement of the mandibular canal

10

11
Multiple Endocrine Neoplasia, Type IIB
• MEN I: tumors of pancreatic islets, adrenal cortex, parathyroid glands and pituitary gland
• MEN IIA: Sipple syndrome, pheochromocytomas and medullary thyroid carcinoma
• MEN IIB: MEN IIA and mucosal neuromas
Multiple Endocrine Neoplasia, Type IIB
• A.D.; 50% new mutations• Mutation of ret proto-oncogene, chr.10• Marfanoid phenotype• Narrow face, thick lips, everted upper eyelid• Neuromas on conjuctiva, eyelid margin or cornea• Oral lesions may be the first sign
– Lips, anterior tongue, buccal mucosa, gingiva, palate, bilateral commissural neuromas
Multiple Endocrine Neoplasia, Type IIB
• Pheochromocytoma– Secretion of catecholamines– Sweating, diarrhea, headaches, flushing,
heart palpitations and hypertension• Medullary carcinoma of the thyroid
– Calcitonin production– Highly metastatic

12

13
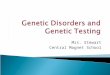
PeutzPeutz--JeghersJeghers SyndromeSyndrome
Autosomal DominantAutosomal Dominant
Multiple perioral and oral Multiple perioral and oral ephelidesephelides or or melanoticmelanotic maculesmacules
Intestinal Intestinal polyposispolyposisConsidered Considered hamartomashamartomas but have minimal neoplasticbut have minimal neoplasticpotential (2 to 3% potential (2 to 3% adenocarcinomaadenocarcinoma))Small intestine (jejunum)Small intestine (jejunum)Abdominal pain, rectal bleeding and diarrhea Abdominal pain, rectal bleeding and diarrhea
Peutz-Jeghers syndrome

14
Amelogenesis Imperfecta
General Information
• Classification is impractical for clinicians• Problems arise in one or more of the
three stages of enamel formation– Elaboration of enamel matrix; hypoplastic– Mineralization; hypocalcified– Maturation; hypomaturation
General Information
• Absence of systemic disorder • Can be part of a syndrome• Many types • Different modes of inheritance• Understanding of molecular events• 1:800 – 1:15,000 (clustering)• Both dentitions

15
Hypoplastic type
• Inadequate deposition of organic matrix• Normal mineralization• Radiographic contrast• Seven types
Hypoplastic typeGeneralized Pitted
• A.D.• Pinpoint/head pits in rows or columns• In-between enamel normal• Across the surface• Buccal surface more severely affected• Does not correlate with pattern of
environmental damage
Hypoplastic typeGeneralized Pitted
Hypoplastic typeGeneralized Pitted
Hypoplastic typeDiffuse Smooth A.D.
• Thin, hard, glossy• Like crown preparations, open bite• Opaque white to brown• X-ray: peripheral thin enamel outline• Unerupted exhibit resorption

16
Hypoplastic typeDiffuse Smooth A.D.
Hypoplastic typeDiffuse Smooth A.D.
Hypomaturation Type
• Defect in the maturation of enamel crystals
• Normal shape• Mottled appearance• White, yellow or brown• Enamel is soft• Radiodensity similar to dentin
Hypomaturation TypeDiffuse Pigmented A.D.
• Mottled brown• Chipping from dentin with an explorer• Very uncommon anterior open bite• Soft similar to hypocalcified• Calculus
Hypomaturation TypeDiffuse Pigmented A.D.
Hypomaturation TypeDiffuse Pigmented A.D.

17
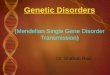
Hypomaturation TypeSnow-capped Teeth
• X-linked, A.D.?• Zone of white opaque enamel on incisal and
occlusal surface (1/4 to 1/3 of the surface)• Looks like fluorosis• Anteriors, anteriors/bicuspids,
premolars/molars• Both dentitions
Hypomaturation TypeSnow-capped Teeth
Hypomaturation TypeSnow-capped Teeth Hypocalcified Type
• A.D. or A.R. (more severe)• No significant mineralization• Normally shaped teeth at eruption• Enamel very thin and easily lost• Yellow or brown color• Calculus• Open bite
Hypocalcified Type Amelogenesis ImperfectaTreatment
• Restorations as soon as possible• Dentures (overdentures)• Veneers in mild cases• Glassionomers for better adhesion to
dentin

18
Osteogenesis ImperfectaOsteogenesis Imperfecta
Heterogeneous group of disorders characterized by impairmentHeterogeneous group of disorders characterized by impairmentof collagen maturationof collagen maturation
Mutations in type I collagen gene Mutations in type I collagen gene
Most common type of inherited bone diseaseMost common type of inherited bone disease
Collagen forms a major portion of bone, dentin, Collagen forms a major portion of bone, dentin, scleraesclerae,,ligaments, and skinligaments, and skin
Autosomal dominant, autosomal recessive hereditary; sporadicAutosomal dominant, autosomal recessive hereditary; sporadic
Severity variesSeverity varies
Weak bones, blue sclera, altered teeth, hearing loss,Weak bones, blue sclera, altered teeth, hearing loss,long bone and spine deformity and joint hyperextensionlong bone and spine deformity and joint hyperextension
Radiographic features include osteopenia, bowing,Radiographic features include osteopenia, bowing,deformity of long bones and multiple fracturesdeformity of long bones and multiple fractures
Oral manifestations are clinically similar to Oral manifestations are clinically similar to dentinogenesisdentinogenesisimperfecta imperfecta –– premature pulpal obliterationpremature pulpal obliteration
Shell teeth can also be notedShell teeth can also be noted
However the two are different processes caused by differentHowever the two are different processes caused by differentmutationsmutations
Opalescent teeth if associated with OIOpalescent teeth if associated with OI
Maxillary hypoplasiaMaxillary hypoplasia
Osteogenesis ImperfectaOsteogenesis Imperfecta
Four major types of OIFour major types of OI
Type I: Most common and mildest formType I: Most common and mildest formType II: Most severe; patients die before 4 weeks of ageType II: Most severe; patients die before 4 weeks of ageType III: Most severe form beyond the perinatal ageType III: Most severe form beyond the perinatal ageType IV: Mild to moderate formType IV: Mild to moderate form
Treatment:Treatment: No treatment of OINo treatment of OIVaried prognosisVaried prognosis
Osteogenesis ImperfectaOsteogenesis Imperfecta

19
Shell Teeth
Hypophosphatasia
• Autosomal recessive trait• Decreased alkaline phosphatase• Increased blood and urinary phosphoethanolamine• Bone defects similar to rickets
• Premature loss of primary teeth without evidence of inflammatory response– No cementum on teeth
Perinatal: most severeInfantile: normal till 6 months; failure to grow after that (severe)Childhood: usually detected at later age; teeth defects with enlarged pulpchambers; open fontanelles with premature fusion of cranial suturesAdult: mild

20
Vitamin D-Resistant Rickets(Hereditary Hypophosphatemic Rickets)
Rickets resistant to vitamin DInherited as X-linked dominant traitMales affected more severely than femalesMutations in PHEX gene
Rickets, hypophosphatemia due to decreaed capacity to reabsorb phosphate
Teeth with large pulp chambers with pulp horns that extend almostto the DE junction leading to very small pulp exposures leading to multiplePeriapical lesions and gingival sinus tracts
It will as though periapical lesions on otherwise normal teeth as theexposures are so tiny
Recommended