Acce
pted M
anus
cript
1
©TheAuthor2014.PublishedbyOxfordUniversityPressonbehalfoftheInfectiousDiseasesSocietyofAmerica.Allrightsreserved.ForPermissions,pleasee‐mail:[email protected].
Anobservational,laboratory‐basedstudyofoutbreaksofMERS‐Coronavirusin
JeddahandRiyadh,KingdomofSaudiArabia,2014
ChristianDrosten1,2,*,#,DoreenMuth1,*,VictorCorman1,2,*,RaheelaHussain4,7,*,
MalakiAlMasri3,WaleedHajOmar7,OlfertLandt5,AbdullahAssiri3,Isabella
Eckerle1,AliAlShangiti7,JaffarA.Al‐Tawfiq6,AliAlbarrak8,AlimuddinZumla3,9,
AndrewRambaut10,ZiadMemish3,11,+
1InstituteofVirology,UniversityofBonnMedicalCentre,Bonn,Germany
2GermanCentreforInfectionResearch
3GlobalCentreforMassGatheringsMedicine(GCMGM),MinistryofHealth,Riyadh,KingdomofSaudiArabia(KSA)
4JeddahRegionalLaboratory,Jeddah,KingdomofSaudiArabia
5Tib‐Molbiol,Berlin
6JohnsHopkinsAramcoHealthcare,SaudiAramco,Dhahran,KingdomofSaudiArabiaandIndianaUniversitySchoolofMedicine,Indianapolis,IN(USA)
7RegionalLaboratory,MinistryofHealth
8PrinceSultanMilitaryMedicalCity,Riyadh,KSA
9DivisionofInfectionandImmunity,UniversityCollegeLondon,andNIHRBiomedicalResearchCentre,UniversityCollegeLondonHospitalsNHSFoundationTrust,London,UnitedKingdom
10InstituteofEvolutionaryBiology,UniversityofEdinburgh,CentreforInfection,ImmunityandEvolution,UniversityofEdinburgh,UK,andFogartyInternationalCenter,NationalInstitutesforHealth,USA
11AlfaisalUniversity,Riyadh,KingdomofSaudiArabia
+Correspondingauthor:ZiadA.MemishEmail:[email protected]
#Alternatecorrespondingauthor:ChristianDrostenEmail:drosten@virology‐bonn.de
*equalcontribution
Clinical Infectious Diseases Advance Access published October 16, 2014 at W
ashington State University L
ibraries on October 21, 2014
http://cid.oxfordjournals.org/D
ownloaded from

Acce
pted M
anus
cript
2
Summary
Inspring2014,anexplosiveoutbreakofMERS‐CoronavirusinJeddahcaused
conjecturesaboutchangesinviraltransmissibility.Functionalexaminationof
circulatingvirusesaswellasanalysesofdiagnosticlaboratorydatasuggestcausationby
nosocomialtransmissionofabiologicallyunchangedvirus.
Abstract
Background
Inspring2014,asuddenriseinthenumberofnotifiedMERS‐Coronavirusinfections
occurredacrossSaudiArabiawithafocusinJeddah.Hypothesestoexplaintheoutbreak
patternincludeincreasedsurveillance,increasedzoonotictransmission,nosocomial
transmission,changesinviraltransmissibility,aswellasdiagnosticlaboratoryartifacts.
Methods
DiagnosticresultsfromJeddahRegionalLaboratorywereanalyzed.Virusesfromthe
JeddahoutbreakandvirusesoccurringduringthesametimeinRiyadh,Al‐Kharj,and
Madinahwerefullyorpartiallysequenced.Asetoffoursinglenucleotide
polymorphismsdistinctivetotheJeddahoutbreakweredeterminedfromadditional
viruses.VirusesfromRiyadhandJeddahwereisolatedandstudiedincellculture.
Resultsandconclusions
Upto481sampleswerereceivedperdayforRT‐PCRtesting.Alaboratoryproficiency
assessmentsuggestedpositiveandnegativeresultstobereliable.Forty‐ninepercentof
168positive‐testingsamplesduringtheJeddahoutbreakstemmedfromKingFahd
Hospital.AllvirusesfromJeddahweremonophyleticandsimilar,whilevirusesfrom
Riyadhwereparaphyleticanddiverse.Ahospital‐associatedtransmissioncluster,to
whichcasesinIndiana/USAandtheNetherlandsbelonged,wasdiscoveredinRiyadh.
OneJeddah‐typeviruswasfoundinRiyadh,withmatchingtravelhistorytoJeddah.
VirusisolatesrepresentingoutbreaksinJeddahandRiyadhwerenotdifferentfrom
MERS‐CoVEMC/2012inreplication,escapeofinterferonresponse,andserum
neutralization.Detectionratesandaveragevirusconcentrationsdidnotchange
significantlyovertheoutbreakinJeddah.Theseresultssuggesttheoutbreakstohave
beencausedbybiologicallyunchangedvirusesinconnectionwithnosocomial
transmission.
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
3
Introduction
TheMiddleEastrespiratorysyndromecoronavirus(MERS‐CoV)wasdiscoveredin2012
andhassincebeenfoundtocausesporadiccasesandsmallcaseclustersofsevereacute
respiratoryillness[1].AllpatientsoccurredintheArabianpeninsulaorhad
epidemiologicallinkstotheregion.Thetotalnumberofnotifiedcasessince2012was
199asof25March2014[2].FromtheendofMarchthroughApril2014anexponential
increaseofnewcasesoccurredinSaudiArabiawithafocusinJeddah,causing
conjecturesaboutpotentialchangesinfundamentalepidemiologicalparameters[3].
Hypothesestoexplaintheoutbreakpatternincludeincreasedsurveillance,increased
zoonotictransmission,increasingnosocomialtransmission,changesinviral
transmissibility,aswellasfalsepositiveresultsduetolaboratoryerrors.Thelatter
optioncausedconcernaboutthevalidityoftheoverallcasecountnotifiedtoWHO[3].
TofullyappreciatetheextensiveoutbreakinJeddah,itwillbenecessarytoreconstruct
transmissionchainsanddissecttheepidemiologyinsuchawaythatfundamental
epidemiologicalparameterscanbeinferred.Whiletheseanalysesmaytakeconsiderable
time,healthauthoritiesareinurgentneedofinformationtoguidepotentialalterations
ofpreventivemeasuresandtravelrecommendations.Virologicalstudiescanprovide
valuableinsightintovirulenceandtransmissibilityeveninabsenceofdetailedclinicalor
epidemiologicalinformation.Moreover,thetrendinnumbersandnatureofrequests
receivedinthediagnosticlaboratorycanprovidehelpfulinsightintothegeneral
situationatpointofcare.
DuringtheoutbreakinJeddah,allRT‐PCRtestingwascentrallyperformedbyJeddah
RegionalLaboratory(JRL).JRLisareferencefacilitywithinthelaboratorynetworkof
theSaudiMinistryofHealththatservestheJeddahregionandprovidesconfirmatory
MERS‐CoVtestingforallMinistryofHealthlaboratoriesacrosstheKingdom.Herewe
providedirectinsightintolaboratoryresultsfromJRLandperformedathorough
analysisoftheoutbreak‐associatedvirusalongwithfunctionalstudiesofvirulenceand
immuneescapeincellculture.WecompareJeddah‐derivedviruseswithviruses
occurringelsewhereinthecountryduringthesametime.
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
4
MaterialsandMethods
RT‐PCRandsequencing
Allproceduresfollowedprotocolsdescribedpreviously[5‐7].JRLusedLightMixkits
(TIBMolbiol)containingpre‐mixedprimersandprobefortheupEandORF1Aassaysto
minimizetheriskofreagent‐basedcontaminationanddetectionartifacts[5].Primers
forviralgenomesequencingareavailableuponrequest.
Virusisolation
SampleswereinoculatedinVeroB4cellsseededat3x105cells/mLin24wellplates16h
priortoinfection,for1hat37°C.Cellswereincubatedat37°Candcheckeddailyfor
cytopathogeniceffects.Every2days,cellculturesupernatantwassampledandtestedby
real‐timeRT‐PCRforincreaseofMERS‐CoV‐specificviralRNA.PCRpositivewellswere
harvestedandusedfortheproductionofvirusstocks.Virusstockswerequantifiedby
plaquetitrationonVeroB4cellsasdescribedearlier[8].
Virusgrowthkinetics
A549cells(ATCCCCL‐185)wereseededat2x105cells/wellin24wellplates16hprior
toinfection.At1,8,24,48and72hpostinfection,supernatantsweresampledandthe
increaseofMERS‐CoV‐specificviralRNAquantifiedbyreal‐timeRT‐PCR[8].
Plaquetitrationandneutralizationassay
VeroB4cellswereseededat1.5x105cells/wellin24wellplates16hpriortotitration.
Cellswereoverlaidafterinfectionwith500µLAvicel(FCMBioPolymer)atafinal
concentrationof1.2%inDMEM[9].Threedayspostinfection,cellswerefixedin6%
formaldehydeandstainedwithcrystalvioletsolution.Forneutralizationassay[10,11],
25plaqueformingunitsofMERS‐CoVwerepre‐incubatedwithdilutedserumforone
hourat37°C.
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
5
Results
Laboratoryperformanceandoveralldiagnosticresults
CaseidentificationandnotificationduringtheoutbreakinJeddahwasmainlybasedon
laboratorytesting.Toobtaininsightintolaboratorytestingduringtheoutbreak,the
samplereceptionlistinJRLwasanalyzed(Figure1).Therewasastrikingincreaseof
diagnosticrequestsduringAprilwhichwasmainlycausedbysamplesfromJeddah
(Figure1A).FromJanuary1sttoApril28th,JRLreceived6,285samplesforRT‐PCR
testingforMERS‐CoV.5,828ofthesesampleswerereceivedonlysinceMarch26th,the
datewhenthefirstcaseintheJeddahoutbreakwastested.Thissuggestsa36.8‐fold
increaseofthemonthlyworkloadinApril.Themaximalnumberofsamplesreceivedina
singledaywas481.AlmosthalfofallpositivetestingsamplesduringtheJeddah
outbreak(82of168)stemmedfromKingFahdHospital.Therateofsampleswith
positivetestsfromKingFahdHospitalseemedtoincreaseearlierthaninotherhospitals
inthecity(Figure1B).OverthecourseoffourweeksinApril,thefractionofpositive
RT‐PCRresultsinsamplesfromJeddahaswellassamplesfromallcitiesdidnotvary
significantly(SupplementaryTable1).Whilethelaboratoryentrylistdidnotidentify
thesymptomsstatusofpatients,itindicatedbypresenceofapatientidentifiercode
whethercaseswereinhospitalorlikelypartofacontactinvestigation(Table1).There
wasamarkedincreaseofcontactinvestigationsinJeddahversusotherlocations.
Expectedly,theproportionofsampleswithlowviralloads(indicatedbyhighCtvalues)
washighincontactinvestigations(Figures1CandD).
StudiesofreliabilityoflaboratoryproceduresaspresentedinSupplementarydataset
1didnotrevealanyevidenceforgenericbackgroundcontaminationinthelaboratory.
Viralgenomesequenceandphylogeny
SevenvirusesfromtheJeddahoutbreakwereentirelysequencedandcomparedwith
full‐lengthorsubtotalgenomesequencesavailableinApril2014inGenBank
(SupplementaryTable2).Ananalysisofmajorreadingframesacrossthegenome
takingintoaccountadditionalspikegenesequences(KM027263‐KM027276)suggested
nouniqueaminoacidchangesinrelevantproteindomains(SupplementaryDataset2).
AllvirusespertainingtotheJeddahoutbreakclusteredinonephylogeneticclade
(Figure2).Seventeenpartialgenomesequencesweredeterminedfromsamples
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
6
obtainedfromRiyadh,Al‐Kharj,andMadinahduringMarchandApril2014for
comparison.Thesepartialsequencescomprisedtheentirestructuralproteingenesof
theMERS‐CoVgenomes,ca.8.7kBinlength.AsshowninFigure2,virusesfromRiyadh
fellinto6differentpositions,oneofwhich(clade2)mayconstituteahuman‐to‐human
transmissionclustertowhichalsotheexportedcasestoIndiana/USAaswellasthe
Netherlandsbelong(SupplementaryTable3)[12,13].AnothervirusfromRiyadh
clusteredwithJeddah‐typeviruses.ThispatientoriginatedfromJeddahandhadvisited
hissicksoninKingFahdHospitalinJeddahbeforehistriptoRiyadh.
TobetterevaluatethediversityofvirusescirculatinginJeddah,singlenucleotide
polymorphisms(SNP)werestudied(Table2).Allsamplesexceptonehadthesame
combinationofSNPs.TheonedeviatingsamplewastakenonApril22ndandhada
doublepeakinoneSNPthatwasconfirmedtwicebyrepetitionofRT‐PCRand
sequencing.Furtherpartialsequencingofthisvirusdidnotyieldanyotherdouble
peaks,suggestingtheongoingformationofquasispeciesasdescribedbefore[14],rather
thansimultaneousinfectionwithtwoviruses.ThesequencesfromaUScaseandacase
inRiyadhwithknowntravelhistoriestoJeddahhadJeddah‐typicalSNPpatterns(Table
2).Incontrast,virusesdetectedinJeddahonemonthand5monthsbeforetheoutbreak
didnotclusterwiththeJeddah‐typeoutbreakviruses.AvirusdetectedinRiyadh
(SA2014_158)wasrelatedtocamelvirusessharingarecentcommonancestorwith
Jeddah‐typeoutbreakviruses,butwasdistinctinitsSNPpattern.
Virusinfectionstudies
Tostudypotentialalterationsinvirusfunctions,16clinicalsamplesfromJeddahwith
projectedviralloadsof5x106copiespersampleorhigherwereselectedandinoculated
inVeroB4cells.Fiveviralisolateswereobtained.Becausethereplicationphenotypeof
allviruseswashighlysimilarinpreliminaryexperiments,oneisolatetermedMERS‐CoV
Jeddah_10306wasfullysequencedandchosenforfurtherstudy(GenBankNo
KM027260,SupplementaryTable2).Forcomparison,viruswasisolatedfrompatients
inahospital‐associatedclusterinRiyadhandanisolatetermedMERS‐CoVRiyadh_683
waschosenandsequenced(GenBankNoKM027262,SupplementaryTable3).The
originalviralisolateEMC/2012[1]wascomparedaswell.
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
7
SinglestepgrowthcurvesweredoneonVerocellsbyinoculationwithhigh
multiplicitiesofinfection(MOI)of1infectiousdosepercell,whichwillrevealgross
differencessuchasintheviruses´capacitytoentercells.AsshowninFigure3A,there
werenorelevantdifferencesinreplicationbetweenthethreeviralstrains.BecauseVero
cellsderivedfromrhesusmonkeykidneytissuemightnotoptimallyreflectthetarget
tissueofMERS‐CoVinfection,A549cellsderivedfromahumanalveolarepithelial
carcinoma(nonsmallcelllungcancer)wereusedinparallel.Resultsofone‐stepgrowth
curveswerehighlysimilar(Figure3B).
Becausedifferencesintheviruses´adaptationtoreplicateinprimatecellsmaynot
becomeobviousinone‐stepgrowthcurves,replicationtrialswererepeatedinparallel
inbothcelllinesusingareducedMOIof0.01thatcausesaprolongedcourseof
replicationwithmultipleroundsofinfectioninculture.Norelevantdifferencein
replicationwasseenbetweenall3viralisolatesinVeroandA549cells(Figure3Cand
D).
ThetypeIinterferonsystemisamongthemostefficientinnateantiviraldefenses.As
MERS‐CoVEMC/2012wasshowntobehighlysusceptibleagainsttypeIinterferon,
infectiontrialsweredoneinVerocellspre‐treatedwithinterferonalphatoinducean
antiviralstatepriortoinfectionincellsatMOI=0.01.EventhoughVerocellsareknown
toinduceanefficientantiviralstateuponexternalIFNstimulus,nodifferencesbetween
thethreeviralstrainswereseen(Figure3E).
Antibodyfunctionsprovidealaboratorycorrelateofadaptiveimmunity.Asvirusesmay
differintheirrobustnessagainstneutralizingantibodies,allthreeviruseswere
subjectedtoplaquereductionneutralizationassaysusingserumofaMERSpatientwith
knownantibodytiter[7].Norelevantdifferencesinthereductionofviralplaques
dependingonserumdilutionwereseenwithanyvirus(Figure3F).
Viralloads
Viralloaddatareflectclinicalvirusexcretion,whichcannotbemodeledincellculture.Ct
valuesasasurrogateofviralloadswerecomparedbetweensamplesfromJeddahand
othercities(Figure4AandB).MeanCtvaluesinJeddahandelsewherewerenot
significantlydifferent(30.4and31.4,respectively).However,thefrequency
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
8
distributionsandmedianvaluessuggestedapronunciationoflowerviralloadsamples
inJeddah.WithinJeddah,CtvaluesinKFH(n=82)werenotdifferentfromthoseinany
otherhospitals(n=108).AllsamplesfromJeddahtestedduringAprilwerecategorized
byweekofreceptionandplottedasshowninFigure4C.Therewasasubjectivetrend
towardlowerCtvaluesbythethirdweek.However,thesepointswereidentifiedas
outliervaluesandmeanviralloadsdidnotdiffersignificantlyinanyoftheweeksof
AprilaccordingtoANOVAanalysis(F=0.82,p=0.48).Oneofthoseoutliersampleswitha
verylowCtvalueencounteredonApril20th,2014yieldedtheisolateofMERS‐CoV
C10306,whichhasbeenentirelysequencedwithoutanyevidenceforsignificant
mutations,andwhichwasstudiedinabove‐describedcellcultureexperimentswithout
anyevidenceforincreasedvirulence.
Discussion
TheunprecedentedincreaseinnewcasesofMERS‐CoVinfectionsduringspring2014
hascausedconcerninthepublichealthcommunityworldwide.Ourinitialsequence
analysescommunicatedduringtheongoingoutbreakprovidedapreliminaryideaofthe
molecularepidemiologywithoutbreakvirusesformingahomogeneous,monophyletic
clade[4].Paraphylyofconcurrentvirusesisexpectedwheninfectionsare
independentlyacquiredfromadiversifiedsourcepopulationsuchasexpectedinanimal
reservoirs.InRiyadh,concurrentlycirculatingviruseswereindeeddistributedacrossat
leastsixdifferentclades,suggestingtheseinfectionstoresultfromincreasedzoonotic
activityorintroductionofhumanvirusesfromotherregions.Onelargerviruscluster
wasobservedinRiyadh,associatedwithonespecifichospitalsuggestingnosocomial
transmission(clade2).ThecaseexportedtoIndiana/USAhadworkedinthishospital
whilethecasesintheNetherlandswerehospitalizedinMadinahbutnotRiyadh[12,13].
Thissuggestsunnoticedtransmissionlinkssuchasinfectedpatientstransferred
betweenhospitals,oracquisitionfromcommonzoonoticsources.
Interestingly,oneofthevirusesseeninRiyadhresembledcamelvirusesinclose
relationshiptoJeddah‐typestrains.Thesevirusesmayhavebeenwidelydistributedin
camelsbylate2013toearly2014,astheyweredetectedinTaifsouthwestofJeddahand
inQatarontheeasternArabianPeninsula[14,15].VirusesencounteredinJeddah
shortlybeforetheoutbreaksuchasJeddah‐1orJeddah_C6664wereclearlydistinct,
suggestingthattheoutbreakmighthavebeeninitiatedbytheintroductionofJeddah‐
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
9
typevirusesintocamelsintheregion.Themonophylyandsimilarityofoutbreakviruses
favorstheideathatthesubsequenttransmissiontookplaceinhumans.Theregional
restrictionofoutbreakvirusesmatchesourearlierobservationoflowtransmissibility
betweenhumansinnon‐nosocomialsettingssuchashouseholdcontactclusters[16].In
spiteofadocumentedtransmissionfromJeddahtothecapitalRiyadh,therewasno
evidenceoffurtherhuman‐to‐humanspreadinRiyadh.FromtheanalysisofSNP
patternsitwasconcludedthatallJeddah‐typeviruseswerehomogenouswithout
evidenceforconcomitantcirculationofotherstrainsduringtheoutbreak.Nevertheless,
ourpreliminarysequencingstudiesfoundnorelevantgeneticchangessufficientto
explainanalteredepidemicpattern[4].Aswehavenowbeenabletoisolateliveviruses,
wecanprovideafirstside‐by‐sidecomparisonofdifferentviralstrainsofMERS‐CoV.Of
note,thesevirusisolateswererepresentativeoftwolikelynosocomialoutbreaksin
JeddahandRiyadh,bothcausinginternationalspreadofthevirustotheUSA,the
Netherlands,aswellasGreece.Cellcultureexperimentsyieldednoevidenceforchanges
inviralreplicationorimmuneescape.Theabsenceofdifferencesinserum
neutralizationdisfavorsantigenicvariabilityasapromoteroftransmissibility.Asthe
selectedvirusesrepresentmajorbranchesoftheknownMERS‐CoVtree,thesedata
additionallysuggesttheabsenceofserotypesinMERS‐CoV,whichisreassuring
regardingtheprospectstodevelopimmunizationapproaches.
BytheendoftheoutbreaklateinApril2014,theaccumulationoflaboratorydataatJRL
allowedfirstinsightsintosheddingpropertiesofcirculatingvirus,whichcompensates
fortheinabilityofcellculturetoreflectvirustransmissibility.Wehaveobtainedno
evidencesuggestingthatconcentrationsofshedvirusmighthavechanged.Asubjective
trendtowardhigherpeak(butnotaverage)concentrationslaterintotheoutbreakmay
beexplainedbyincreaseddiseaseawarenessinhospitalsleadingtoanearlier
investigationofsuspectedcases.SimilarobservationsweremadeduringtheSARS
epidemicinHongKongwherecasesweredetectedearlieraftersometimeintothe
outbreak[17].Theabsenceofchangesinaveragevirusconcentrationsmakesitunlikely
forthevirustohavechangeditstransmissibilityandvirulenceoverthecourseofthe
outbreak.
ThereasonfortheexplosivenatureoftheepidemicinJeddahmaythusbefound
elsewhere,suchasintherateofhuman‐to‐humancontact.Inthislight,ouranalysisof
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
10
laboratorystatisticsishighlysuggestiveofanoutbreakfuelledbythehealthcaresetting.
Notonlydidabouthalfofallpatientswithapositivediagnosispertaintooneparticular
hospital,butalsothefirstpeakcasecountsinthishospitalpredatedincreases
elsewhere,andnewpeakswerefollowedbypeaksofcasesinotherhospitals.This
patternishighlysuggestiveofanepidemiologicalhotspotwherethevirusisamplified
andfromwherelimitedtransmissionchainsareseeded.Indeed,KingFahdHospitalis
thelargestcommunalhospitalinJeddahservingastheprimarycarecenterforall
patientsattendingtheMOHhealthcaresystem,aswellasforalargefractionof
expatriateworkersinthecity.ItisreassuringthatthenumberofnewcasesinKingFahd
Hospitalcamedowntowardtheendofthestudyperiod.Thistrendstartedevenbefore
changessuchastheclosureofemergencyroomsandthetransferofinfectedpatients
wereimplemented,pointingtothepossibilitythattransmissionmayhavebeenlimited
mainlybyheightenedawarenessofthediseaseamonghealthcareworkersandpatients.
Again,asimilareffecthasbeendocumentedduringtheSARSepidemicinHongKong
[17].
Animportantobservationincasenotificationsduringtheoutbreakwastheincreaseof
casesnotifiedas"asymptomatic"or"mild"intheJeddahcasestatistics.Asshowninour
assessmentofsamplereceptions,thehugeamountoflaboratoryrequestsduringpeak
phasesoftheepidemiccausedanoverloadonlaboratorycapacitieswithoutasignificant
increaseofthefractionofrequeststhatwereconfirmedvirus‐positive.Alowpredictive
valueofclinicalsuspicioniscausedbyaninsufficientcasedefinitionorlackof
adherencetothecasedefinition,suchassuggestedbyahighfractionoftestsincases
withoutproperhospitalregistrationnumber.UnjustifiedRT‐PCRtestingraisesthe
likelihoodofhumanerror.Asfaraspossible,wehaveassessedthetechnicalcapabilities
ofJRLandfoundnogeneralissuesofcross‐contamination.Nevertheless,wecannot
excludeissueselsewhereinthelogisticschain,suchasnearthebedsidewhere
diagnosticsamplesmayhavebeenhandledinbulk.ThehighsimilarityofallJeddah‐type
viruseswillmakeitimpossibletoresolvepotentialcontaminationsources
retrospectivelybysequencingofstoredsamples.Nevertheless,acertainrateofpositive
testresultsinasymptomaticpersonsmightbeconsideredplausibleasunnoticed
replicationhasbeenshownforSARS‐CoVwhoseRNAwasdetectedinexposed
healthcareworkerswithnoormildsymptoms,aswellasinourrecentstudyon
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
11
householdcontactsofMERS‐CoVcases[16,18].Suchreplicationmaybetransient,and
thelowviralloadsseenincontactsmightnotsufficetoestablishinfectionchains.
Inconclusion,ourinvestigationssuggestapredominanceofhuman‐to‐human
transmissionduringtheJeddahoutbreakwithoutevidenceformodificationofviral
shedding,replication,andimmuneescape.AcoincidentincreaseofcasesinRiyadhwas
theresultofmultiple,independent,sourceswithsomephylogeneticevidenceof
nosocomialspread.ContacttracingbyRT‐PCRshouldberestrictedtodefinedgroupsof
patientstoavoidanoverloadonthehealthcaresystem.Retrospectiveserologicaltests
mayprovideavalidalternativetoRT‐PCRtestingofcontacts[16].
ACKNOWLEDGEMENTS:WearegratefultoallstaffoftheMinistryofHealth,Saudi
Arabia.
FINANCIALSUPPORT:ChristianDrostenacknowledgessupportfromtheEuropean
Commission(EMPERIE;www.emperie.eu/emp/;contractno.223498)andANTIGONE
(contractno.278976),infrastructuralsupportfromtheGermanCentreforInfection
Research,theGermanMinistryforResearchandEducation,andtheGermanResearch
Council(grants01KIO701andDR772/3‐1).IsabellaEckerle,DoreenMuth,andVictor
CormanacknowledgegrantsupportfromEuropeanCommission,MinistryofResearch
(Germany),andGermanResearchCouncil(DFG).AlimuddinZumlaacknowledges
supportfromtheUniversityCollegeLondonHospitalsNHSFoundationTrust,the
NationalInstituteofHealthResearch,BiomedicalResearchCentre,UCLHospitals,the
EDCTPandtheEC‐FW7(RiD‐RTI).AndrewRambautacknowledgessupportbythe
EuropeanCommissionundertheprojectPREDEMICS(contractno.278433).
CONFLICTSOFINTEREST:OlfertLandtisCEOofTibMolbiol,acompanyproviding
someoftheRT‐PCRreagentsusedinthisstudy.Heorhiscompanyhadnoinfluencein
thedecisiontousethesereagents.Theworkdoesnotmakeanycomparisonsofthese
reagentswithproductsprovidedbycompetingcommercialornoncommercialentities.
Allotherauthorsdeclarenoconflictsofinterest.
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
12
Table1.Testsinsampleswithandwithouthospitalnumber,byCity
City Testswithhospitalnumber Testswithouthospitalnumbera Ratio
Jeddah 3739(4%positive) 1056 (1.7%positives) 28%
Non‐Jeddah 1072(2.9%positive) 59(0positives) 5.5%
a:Thesecaseswereenlistedwithnohospitalnumberbutcarriedeitherofthefollowing
identifiers:"Contact","HCW",orhadacellphonenumberenteredintheidentifierfieldthatthe
laboratorywasaskedtocallincaseofself‐initiateddiagnostictestsbyphysiciansortheirfamily
members(n=41).
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
13
Table2.SinglenucleotidepolymorphismsinJeddah‐typevirusesandreferenceviruses
SNP position in EMC/2012 genomeSample ID Sample/patient origin Sampling date 737 17836 23953 2877868 samples from JRLa Jeddah, Makkah 26 Mar to 23 Apr 2014 C T G A Human|2014SA_693b Riyadh 22 Apr 2014 C T G A Human|Florida/USA-2/Jeddah Jeddah 10 May 2014 C T G A Human|C10829 Jeddah 22 Apr 2014 C T G A/T Camel|Qatar_2|KJ650098 Qatar 16 Feb 2014 C C A T Human|C6664c Jeddah 18 Feb 2014 T C ? T Human| 2014SA_158d Riyadh 20 Mar 2014 T C A T Camel|Jeddah_1_2013|KJ556336e Jeddah 6 Nov 2013 T C A T Camel|KSA-505|KJ713295 Taif Nov 2013 T C A T Camel|KSA_378|KJ713296 Taif Nov 2013 T C A T Human|2014SA_683 Riyadh 21 Apr 2014 T C A T Camel|KSA-503|KJ713297 Taif Nov 2013 T T A T Camel|KSA-363|KJ713298 Taif Nov 2013 T T A T Human|EMC/2012|JX869059 Bisha Jun 2012 T C A T
a:Mediansamplingdateon14.April.The68samplesrepresented40%ofallpositivesamplesidentifiedatJRLinJeddahpatients
b:ThispatienthadatravelhistorytoKingFahdHospitalinJeddahwithinoneincubationtimebeforeonsetofsymptoms
c:ThiswasthelastpatientdetectedandsequencedinJeddahbeforetheonsetoftheoutbreakendofMarch.TheSNPatposition23953
couldnotbesequencedbecausethediagnosticsamplecontainedonlyminuteamountsofRNAandhadbeenstoredat‐20°Cforprolonged
time.
d:Thispatienthadnotravelhistory.Virus2014_SA158clustersamongstcamelvirusesinancestralrelationshiptoJeddah‐typehuman
viruses,suchasCamel_Qatar2_KJ650098.
e:ThisviruswastransmittedfromacamelinJeddah,October/November2013
at Washington State University Libraries on October 21, 2014 http://cid.oxfordjournals.org/ Downloaded from

Acce
pted M
anus
cript
14
LegendstoFigures
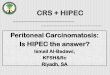
Figure1.SummaryoffeaturesoftheoutbreakasderivedfromJRLlabfiledata.A,
overalldiagnosticrequests;B,positivecases(yscale=casesperday)inKingFahd
Hospitalversusallotherhospitals,recording3‐dayintervalsstartingonMarch26and
endingonApril28.CandD:DistributionofCtvaluesin1056samplespertainingto
investigationsincaseswithouthospitalnumberinJeddah(n=18positivesamples),
versus3799sampleswithhospitalnumber(n=150positivesamples).AverageCtvalues
incasesandcontactswere30and33.1,respectively(2‐tailedt‐test,p<0.009).
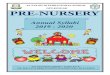
Figure2.PhylogenetictreeinferredusingMrBayes[20]fortheconcatenatedcoding
regionsof105MERS‐CoVgenomesorpartialgenomessampledfromhumansand
camels.Weemployedacodon‐position‐specificGTRsubstitutionmodelwithgamma‐
distributedratesamongstsites.Displayedisthemajority‐consensusof10,000trees
sampledfromtheposteriordistributionwithmeanbranchlengths.Posteriorsupportis
shownfornodeswherelessthan0.90.Sequencessampledfromcamelsaredenoted
withayellowcircle,thosefromhumanswithagreencircle.Sequencesnewtothisstudy
arelabelledinbold.TheclustercomprisingvirusesisolatedfromtheJeddah/Makkah
hospitalsinApril2014arehighlightedwitharedboxandthosefromthePrinceSultan
MilitaryMedicalCity,RiyadhinMarch,April2014arehighlightedinblue.For
comparisontheAl‐Hasa2013hospitaloutbreak[21]ishighlightedinyellowandthe
2013Hafr‐Al‐Batincommunityoutbreak[22]ingreen.
Figure3:GrowthkineticsofMERS‐CoVEMC/2012,Jeddah_10306,andRiyadh_683in
cellculture.VeroB4andA459cellswereinfectedatMOI1(AandB,respectively)orMOI
0.01(CandD,respectively).Samplesfromthesupernatantweretakenatindicatedtime
pointsandvirusgrowthwasmeasuredbyreal‐timeRT‐CPR.VeroB4cellsinfectedat
MOI1(A)showedtotalcytopathogeniceffect48hpostinfection,terminatingthe
experiment.A459cellsdidnotshowanyCPEevenwheninfectedatMOI1at72hp.i.
(B).E,effectofpretreatmentofcellcultureswithtypeIinterferonatloworhighdosage.
D,virusneutralizingeffectofhumanserumwithknownanti‐MERS‐CoVneutralizing
antibodytiteratdifferentdilutions.
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
15
Figure4.Virussheddinginpatients.CtvaluesduringtheoutbreakinJeddah.AandB,
frequencydistributionofCtvaluesinJeddahversusothercities;C,Ctvaluesduringthe
outbreakinJeddahbyweek,startingonMarch26th,2014.
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
16
References
1.ZakiAM,vanBoheemenS,BestebroerTM,OsterhausAD,FouchierRA.IsolationofanovelcoronavirusfromamanwithpneumoniainSaudiArabia.TheNewEnglandjournalofmedicine2012;367:1814‐20.2.Anonymous.MERS‐CoV.ProMedmail2014;20140325.2356854.3.Anonymous.SevererespiratorydiseaseassociatedwithMiddleEastrespiratorysyndromecoronavirus(MERS‐CoV);Ninthupdate,24April2014.EuropeanCentersforDiseaseControl2014;24April.4.DrostenC,CormanV.SequenceinformationandcommentsregardingMERS‐Coronavirus(CoV)inJeddah,KingdomofSaudiArabia.ProMedmail2014;20140426.2432140.5.CormanVM,EckerleI,BleickerT,etal.Detectionofanovelhumancoronavirusbyreal‐timereverse‐transcriptionpolymerasechainreaction.Eurosurveillance:bulletinEuropeensurlesmaladiestransmissibles=Europeancommunicablediseasebulletin2012;17.6.CormanVM,MullerMA,CostabelU,etal.Assaysforlaboratoryconfirmationofnovelhumancoronavirus(hCoV‐EMC)infections.Eurosurveillance:bulletinEuropeensurlesmaladiestransmissibles=Europeancommunicablediseasebulletin2012;17.7.DrostenC,SeilmaierM,CormanVM,etal.ClinicalfeaturesandvirologicalanalysisofacaseofMiddleEastrespiratorysyndromecoronavirusinfection.TheLancetinfectiousdiseases2013;13:745‐51.8.MullerMA,RajVS,MuthD,etal.HumancoronavirusEMCdoesnotrequiretheSARS‐coronavirusreceptorandmaintainsbroadreplicativecapabilityinmammaliancelllines.mBio2012;3.9.HerzogP,DrostenC,MullerMA.PlaqueassayforhumancoronavirusNL63usinghumancoloncarcinomacells.VirolJ2008;5:138.10.MemishZA,CottenM,MeyerB,etal.HumanInfectionwithMERSCoronavirusafterExposuretoInfectedCamels,SaudiArabia,2013.Emerginginfectiousdiseases2014;20:1012‐5.11.MeyerB,MullerMA,CormanVM,etal.AntibodiesagainstMERScoronavirusindromedarycamels,UnitedArabEmirates,2003and2013.Emerginginfectiousdiseases2014;20:552‐9.12.Kraaij‐DirkzwagerM,TimenA,DirksenK,etal.MiddleEastrespiratorysyndromecoronavirus(MERS‐CoV)infectionsintworeturningtravellersintheNetherlands,May2014.Eurosurveillance:bulletinEuropeensurlesmaladiestransmissibles=Europeancommunicablediseasebulletin2014;19.13.BialekSR,AllenD,Alvarado‐RamyF,etal.FirstconfirmedcasesofMiddleEastrespiratorysyndromecoronavirus(MERS‐CoV)infectionintheUnitedStates,updatedinformationontheepidemiologyofMERS‐CoVinfection,andguidanceforthepublic,clinicians,andpublichealthauthorities‐May2014.MMWRMorbidityandmortalityweeklyreport2014;63:431‐6.14.BrieseT,MishraN,JainK,etal.MiddleEastrespiratorysyndromecoronavirusquasispeciesthatincludehomologuesofhumanisolatesrevealedthroughwhole‐genomeanalysisandvirusculturedfromdromedarycamelsinSaudiArabia.mBio2014;5:e01146‐14.15.RajVS,ElmoubasherABAF,ReuskenCBEM,etal.IsolationofMERSCoronavirusfromaDromedaryCamel,Qatar,2014.Emerginginfectiousdiseases2014;earlyonline.16.DrostenC,MeyerB,MüllerMA,etal.TransmissionofMERS‐Coronavirusinhouseholdcontacts.TheNewEnglandjournalofmedicine2014.
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
17
17.LeungGM,HedleyAJ,HoLM,etal.Theepidemiologyofsevereacuterespiratorysyndromeinthe2003HongKongepidemic:ananalysisofall1755patients.Annalsofinternalmedicine2004;141:662‐73.18.HoHT,ChangMS,WeiTY,etal.Colonizationofsevereacuterespiratorysyndrome‐associatedcoronavirusamonghealth‐careworkersscreenedbynasopharyngealswab.Chest2006;129:95‐101.19.AzharEI,El‐KafrawySA,FarrajSA,etal.EvidenceforCamel‐to‐HumanTransmissionofMERSCoronavirus.TheNewEnglandjournalofmedicine2014.20.RonquistF,TeslenkoM,vanderMarkP,etal.MrBayes3.2:efficientBayesianphylogeneticinferenceandmodelchoiceacrossalargemodelspace.Systematicbiology2012;61:539‐42.21.AssiriA,McGeerA,PerlTM,etal.HospitaloutbreakofMiddleEastrespiratorysyndromecoronavirus.TheNewEnglandjournalofmedicine2013;369:407‐16.22.MemishZA,CottenM,WatsonSJ,etal.CommunityCaseClustersofMiddleEastRespiratorySyndromeCoronavirusinHafrAl‐Batin,KingdomofSaudiArabia:ADescriptiveGenomicstudy.Internationaljournalofinfectiousdiseases:IJID:officialpublicationoftheInternationalSocietyforInfectiousDiseases2014;23:63‐8.
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
18
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
19
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
20
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from

Acce
pted M
anus
cript
21
at Washington State U
niversity Libraries on O
ctober 21, 2014http://cid.oxfordjournals.org/
Dow
nloaded from
Recommended