1
Surgical Intensive CareJUNYI LI, MD
Board certified in AnesthesiologyBoard certified in Critical Care MedicineBoard certified in Transesophageal Echocardiography
March 31, 2009

2
Subspecialty ICU
• Medical Intensive Care Unit (MICU)• Coronary Care Unit (CCU)• Surgical Intensive Care Unit (SICU)• Neurological Intensive Care Unit (NICU)• Cardiovascular Intensive Care Unit (CVICU)• Pediatric Intensive Care Unit (PICU)• Neonatal Intensive Care Unit (NICU)

3
SICU Admission Criteria• Preoperative status Major trauma Surgical Procedure Pt’s preexisting disease• Intraoperative event Large volume shift Unexpected surgical complication Unexpected anesthesia complication• Postoperative status Unexpected postop complication Pt’s status

4
Who need to be admitted to SICU ?• 18 y/o health male presented for right inguinal hernia repair
under spinal anesthesia and uneventful intraop and postop.• 50 y/o female with controlled HTN and DM for lumbar
laminectomy under general anesthesia with EBL 500 ml.• 75 y/o male with stable angina, COPD required home oxygen
for TURP under spinal anesthesia• 60 y/o male presented for AAA repair• 54 y/o female with esophageal cancer presented for
esophagectomy • 95 y/o female presented for right hip arthroplasty

5
SICU Management• Respiratory care • Hemodynamic monitoring and management Noninvasive Invasive• Infection in SICU• Acid-base disorders• Fluid and electrolyte disorders• Blood component therapy• Nutrition support

6
Respiratory care – basic monitor
• Respiratory rate• Chest movement• Breath sound• Color

7
Respiratory care – lung volume
• Tidal volume (VT)• Minute ventilation (Vm)• Functional residual capacity (FRC)• Vital capacity (VC)

8
Respiratory care - ventilation
• Ventilation-perfusion (V/Q) ratio: normal V/Q=4L/5L=0.8
• Dead space ventilation: V/Q>1 anatomic dead space & physiologic dead space
• Intrapulmonary shunt: V/Q<0.8 true shunt (V/Q=0) and venous admixture

9
V/Q relationship and associated blood gas

10
Effect of shunt fraction on PAO2

11
Effect of shunt fraction on PAO2 and PACO2

12
Ventilation-perfusionQuantitative determinations
• Dead space (Vd/Vt) = (PACO2 – PECO2)/PACO2
• Shunt fraction (Qs/Qt) = (CCO2 – CAO2)/(CCO2 –CVO2)
• A-a gradient (PAO2 – PaO2) PAO2 = PIO2 – (Paco2/RQ) PAO2 = FIO2(PB –PH2O) – (PaCO2/RQ) PAO2 = 0.21(760 – 47) – (40 /0.8) = 100 mmHg
• PAO2/FIO2<200, Qs/Qt>20% PAO2/FIO2>200, Qs/Qt<20%

13
Hypoxemia
Disorder A-a PO2 PVO2
Hypoventilation Normal Normal Pulmonary disorder Increased Normal DO2/VO2 imbalance Increased Decreased
DO2/VO2 – oxygen deliver and uptake ratio A-a PO2 – PO2 difference between alveolar gas and arterial blood PVO2 – Mixed venous PO2

14
Evaluation of hypoxemia

15
Hypercapnia
• Hypercapnia is PACO2>45 mm Hg, due to • Increased CO2 production• Hypoventilation• Increased dead space ventilation

16
Evaluation of hypercapnia
High

17
Oximetry
• Oximetry detects arterial blood HbO2 and Hb ratio
• Ear oximetry• Pulse oximetry• Co-Oximeters can detect Met Hb and CO Hb• Mixed venous oximetry measured O2 sat in PA
blood

18
CO2 detector and capnometry• CO2 detector is a method for determining the
success or failure of ET intubation.• Clinical application of capnometry in ICU: - Cardiac output monitor - Ventilator-related mishap detection - Early detection of nosocomial disorders - Ventilator weaning - Controlled hyperventilation

19
Acute respiratory distress syndrome (ARDS)
• A leading cause of acute respiratory failure with high mortality
• A diffuse inflammatory injury in the lung• Not an accumulation of watery edema fluid• Not a primary disease, but a complication

20
Common conditions that predispose to ARDS

21
ARDS microscopic changes and CXR

22
Diagnostic criteria for ALI and ARDS
• Acute onset• Presence of predisposing condition• PaO2/FiO2 < 200 mm Hg for ARDS,
< 300 mm Hg for ALI• CXR – bilateral infiltrates• PAOP < 18 mm Hg or no clinical evidence of
high LA pressure

23
Management of ARDS
• No real treatment for ARDS, only supportive• Mechanical ventilation:
low-volume ventilation permissive hypercapnia positive end-expiratory pressure
• Fluid management – reducing extravascular lung water
• Pharmacotherapy – uncertain effect

24
Respiratory therapy
• Oxygen inhalation therapy• Chest physical therapy• Respiratory pharmacotherapy• Mechanical ventilation

25
Oxygen inhalation therapy
• Arterial hypoxemia: PaO2 < 60 mm Hg (SaO2 < 90 %)
• Tissue hypoxia: blood lactate > 4 mmHg
• Endpoint of O2 therapy is tissue oxygenation• Tissue hypoxia may not consistent with
arterial hypoxemia

26
Effect of Oxygen on blood flow
• Oxygen tends to reduce systemic blood flow due to: 1. vasoconstrction in all vascular bed except
the pulmonary circulation 2. decrease in cardiac output 3. negative inotropic effect

27
Method of oxygen inhalation
• Low-flow oxygen delivery system with variable FiO2
• High-flow oxygen delivery system with constant FiO2

28
Device Reservoir Oxygen flow FiO2 capacity (L/min) Nasal cannula 50 ml 1 0.21-0.24 2 0.24-0.28 3 0.28-0.34 4 0.34-0.38 5 0.38-0.42 6 0.42-0.46Oxygen face mask 150-250 ml 5-10 0.40-0.60Mask-reservoir bag 750-1250 ml Partial rebreather 5-7 0.35-0.75 Nonrebreather 5-10 0.40-1.0
Low-flow oxygen delivery systems
FiO2 = 20 + 4 X oxygen flow (L/ml)

29
Respiratory pharmacotherapy
• Bronchodilators
• Corticosteroids
• Mucokinetic therapy

30
Mechanical Ventilation

31
Mechanical ventilation
• Mechanical ventilation is positive pressure ventilation
• Indications of mechanical ventilation Rate ABG: hypoxia and hypercapnia Mechanical parameter: MV, VC and NIP Dead space and shunt
• Contraindication of mechanical ventilation

32
Normal lung Noncompliant lung
Effect of positive pressure ventilation

33
Effect of positive pressure ventilation

34
Respiratory parameter
• Rate: 10 – 20/min• VT: 6 – 10/kg• FiO2: 40 – 100%• PEEP: 5 – 10 cm H2O• PS: 5 – 10 cm H2O• I:E ratio: 1:2

35
Patterns of mechanical ventilation
• Control mode ventilation
• Assist-control ventilation

36
Pattern of mechanical ventilation
• Volume-controlled ventilation ACV (assist control ventilation) IMV (intermittent mandatory ventilation) SIMV (synchronized IMV)
• Pressure-controlled ventilation• Pressure support ventilation• Special pattern:

37
Functional mode of ventilator
• PEEP (positive end expiratory pressure)
• PS (pressure support)
• I:E reversal ratio

38
Ventilatory mode of mechanical ventilation

39
Volume-controlled ventilation

40
Pressure-controlled & Pressure support

41
PEEP and CPAP

42
Effect of PEEP on arterial oxygenation and CI

43
Discontinuing mechanical ventilation
• Ventilator required for brainstem respiratory depression (e.g.,GA in OR or drug overdose) is easy to discontinue
• Ventilator required for cardiopulmonary insufficiency is weaning in gradual process

44
Discontinuing mechanical ventilation
Clinical evaluation: Awake Spontaneous breathing Ability of airway protection Stable hemodynamics

45
Discontinuing mechanical ventilation
Sequence of weaning: FiO2 to 50% or less PEEP to 5 cm H2O or less PS to 10 cm H2O or less

46
Discontinuing mechanical ventilation Bedside weaning parameters:Parameter Normal range Threshold for weaningPaO2/FiO2 >400 200 VT 5-7 ml/kg 5 ml/kg Rate 10-20/min <40/min VC 65-75 ml/kg 10 ml/kg VE 5-7 L/min <10 L/min
Pi max >-90 cm H2O (F) -24 cm H2O >-120 cm H2O (M) Rate/VT <50/min/L <100/min/L

47
Predictive value of selected weaning parameters

48
Discontinuing mechanical ventilation
Methods of weaning: T-piece weaning IMV weaning CPAP weaning

49
Diagram of T-shaped circuit

50
Hemodynamic monitoring Noninvasive
• ECG: heart rate, rhythm, ischemia (ST-T)• Noninvasive BP• Echocardiography: TTE, TEE, color-doppler Contractility Volume status EF Ischemia (RWMA) • Noninvasive cardiac output (through A-line)

51
Hemodynamic monitoringInvasive
• Arterial blood pressure• Central venous pressure• Pulmonary artery catheter and wedge pressure• Cardiac output

52
Invasive arterial blood pressure
• Major CV surgery• Surgery with great hemodynamic change• Surgery with large volume shift and bleeding• Shock and other critical ill patients• Surgery requiring hemodilution and control
hypotension• Frequent ABG
Indication

53
Invasive arterial blood pressure
• Contraindication: only relative contraindication except for puncture site infection

54
Invasive arterial blood pressureSelection of artery for cannulation
• Radial artery• Ulnar artery• Brachial artery• Femoral artery• Dorsalis pedis and posterior tibial arteries• Axillary artery• Carotid artery – do not use

55
Invasive arterial blood pressureComplication
• Bleeding and hematoma• Vasospam• Thrombosis and thrombi• Aneurysm• Infection• Nerve damage• Necrosis of skin overlying the catheter

56
Invasive arterial blood pressureWaveform
SBP gradually increasesMBP remains unchanged

57
Invasive arterial blood pressure Waveform distortion
Normal test
underdamped
overdamped

58
Central venous pressureIndication
• Fluid administration for severe hypovolemia and shock
• Infusion of cardiac drugs• Aspiration of air emboli in craniotomy• Insertion of transcutaneous pacing leads• Total parenteral nutrition (TPN)• Venous access for patients with poor
peripheral veins

59
Central venous pressureContraindication
• Renal cell Ca extension into RA, RA myxoma, or fungating tricuspid valve vegetations
• Skin infection at cannulation site• Severe coagulopathy • Ipsilateral carotid endarterectomy (IJ),
pneumothorax and hemothorax are relative contraindication

60
Central venous pressureSelective sites of cannulation
• Internal jugular veins• Subclavian veins• Femoral veins• External veins• Basilic veins

61
Central venous pressureMeasurement
• Catheter’s tip lies above or the junction of SVC and RA
• CVP is measured with cm H2O• CVP should be measured during end expiration

62
Central venous pressureWaveform
• a wave – atrial contraction, absent in A fib and exaggearted in JR (cannon wave)
• c wave – TV elevation@early ventricular contraction• v wave – venous return against to closed TV• x descent – downward displacement of TV (systole)• y descent – TV opening during diastole

63
Central venous pressureComplication
• Bleeding and hemotoma• Pneumothorax and hemothorax• Pleural effusion and chylothorax• Line-related infection• Air thrombi

64
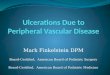
Pulmonary artery catheterization
Length 110 cmOD 2.3 mmDistal portProximal portBalloon at tipThemistor

65
“It Is Time To Pull The PAC”
PAC dose not improve outcome in critically ill patients

66
Background• Pulmonary artery catheter(PAC) has been used in
critical care practice for three decades• Majority of PAC are inserted to aid in
management of critically ill pts in ICU and high risk surgical pts in OR
• Observational studies & small randomized controlled trials (RCT) showed variable results:
Worse outcome No difference in outcome Some benefit

67
Summary
• PAC-directed management in high risk surgical, severe sepsis, shock and RADS pts is a safe procedure
• PAC use dose not improve outcome• PAC use may not increase cost of care

68
Pulmonary artery catheterizationIndication
• Cardiac disease: CAD with LV dysfunction, valvular heart disease, heart failure
• Pulmonary disease: ARDS, severe COPD, Pulmonary hypertension
• Complex fluid management: shock, acute burn ARF, MOF
• Specific surgical procedure: aortic cross clamp pheochromocytoma, liver transplants,
• Hemodynamic unstability required cardiovascular drug therapy
• High-risk obstetrics: severe toxemia

69
Pulmonary artery catheterizationContraindication
• Severe TV or PV stenosis• RA or RV tumor• Endocarditis with vegetation on TV or PV• Other contraindication related to central
venous cannulation

70
Pulmonary artery catheter

71
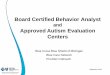
Pulmonary artery catheterization Insertion of catheter

72
PCWP and CVP

73
Pulmonary artery catheter in chest x-ray

74
Pulmonary artery catheterizationComplication
• Complication associated with CV cannulation• Bacteremia and endocarditis• Thrombogenesis and pulmonary infarction• Pulmonary artery rupture and hemorrhage• Arrhythmias and conduction abnormalities• Pulmonary valve damage

75
Pulmonary capillary wedge pressure
CVP = RAP = RVEDPPCWP = LAP = LVEDP

76
Hemodynamic parameter
• BSA = (Ht + Wt – 60)/100, nl 1.6 to 1.9 m2• CO = HR x SV• CI = CO/BSA• DO2 = CI x 13.4 x Hb x SaO2
• VO2 = CI x 13.4 x Hb x (SaO2 – SvO2) * SvO2 obtained from PAC distal port

77
Hemodynamic Profiles
• Heart failure: Right heart failure Left heart failure High RAP High PCWP Low CI Low CI High PVRI High SVRI

78
Hemodynamic profiles
• Hypotension: Hypovolemic Cardiogenic Vasogenic Low CVP High CVP Low CVP Low CI Low CI High CI High SVRI High SVRI Low SVRI

79
Cardiac output monitoring
• Thermodilution methods Pulmonary artery catheter Peripheral artery catheter (Picco)
• Dye dilution methods• Echocardiography• Thoracic bioimpedance

80
Cardiac output monitoring Fick principle
CO = Oxygen consumptiona – v O2 content difference
= VO2
CaO2 – CvO2
Fick principle is the basis of all indicatordilution methods of determining cardiac output

81
Thermodilution method

82
Hemodynamic management
• Preload• Afterload• Cardiac contractility

83
Hemodynamic managementPreload
• Monitoring via CVP or PCWP• Increased preload by giving volume• Decreased preload by giving diuretics and/or
vasodilators (nitroglycerin)

84
Hemodynamic managementAfterload
• Vascular resistance• Balance between cardiac work and organ perfusion • Vasodilators: Systemic vasodilators: nitroprusside, calcium channel blockers, a1-blockers Pulmonary vasodilators: PGE1, PGI, NO• Vasocontrictors: levophed, epinephrine, vasopresin

85
Hemodynamic managementInotropic agents
• Positive inotropic agents: epinephrine, dopamine, dobutamine, PDEI (milrinone)
• Negative inotropic agents: beta blocker and calcium channel blockers

86
Hemodynamic managementMechanical support (IABP)

87
Hemodynamic effect of IABP
• Decrease afterload and promote SV• Increased diastolic pressure and coronary
blood flow in hypotensive patients• Indication: AMI, cardiac shock, unstable
angina, acute MR• Contraindication: AI, aortic dissection and
aortic graft in thoracic aorta• Complication: leg ischemia, septicemia

88
Acute renal failure (ARF)• The hallmark of ARF is azotemia and oliguria• Lab: blood urea nitrogen(BUN), criatinine(Cr), blood
electrolytes, glumerular filtration rate• Etiology: prerenal, renal and postrenal Renal ischemia (50%), Nephrotoxines (35%), Intrinsic renal disease (15%) 50% of ARF in SICU due to major trauma or surgery

89
Etiology of ARF

90
Treatment of ARF
• Supportive management• Diuretics and mannitol to maintain urine
output in nonoliguric patients• Renal dose dopamine?• Glucocorticoids for ARF due to vasculitis or
glomerulonephritis• Other: restrict fluid, sodium, potassium, posph• Renal replacement therapy (dialysis)

91
Renal Replacement Therapy

92
Infection in SICU
• Infections are leading cause of death in ICUs• Community acquired and hospital acquired infection • Strains of bacteria resistant to commonly used
antibiotics are common• Advanced age, prolonged use of invasive devices,
respiratory failure, renal failure and head trauma are established risk factors for hospital acquired infection
• Multiple antibiotics and broad spectrum antibiotics are commonly used in SICU

93
Nutrition support in SICU
• Maintaining adequate nutrition in critically ill patients improves wound healing. Restore immune competence and reduces morbidity and mortality
• Critically ill patients generally required 1.0-1.5g/kg/day instead of 0.5g/kg/day for nonstressed patients
• Enteral nutrition and parenteral nutrition

94
Enteral Nutrition in SICU
• GI tract is the route of choice for nutrition support when its functional integrity is intact
• Enteral nutrition is simpler, cheaper, less complicated, and fewer complication
• Enteral nutrition can better preserve GI structure and function
• Diarrhea is most common problem related to hyperosmolarity of the solution or lactose intolerance

95
Parenteral Nutrition in SICU
• Total parenteral nutrition (TPN) is indicated if the GI tract cannot be used of if absorption is inadequate
• Complications of TPN are catheter-related and metabolic
• The most common problem in TPN is hyperglycermia
Recommended