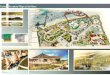
Tropical waters of Caribbean regions including Grenada are popular, used for recreational activities, and resources from the waters serve as a major source of livelihood for the community (Figure 1) [1]. Therefore, monitoring of coastal water quality is important for the public health.
Microbial pollution may result in economic loss due to closure of recreational beaches and sea food harvesting areas [2]. Several pathogens, for example cholera bacterium, survive in the marine water. Others are carried into coastal waters following e.g. sewage effluent from ships/yachts, urination of recreating population, agriculture, septic tanks near the shore and stormwater runoffs, industrial processes, wildlife, and urban development [3].
Coastal water quality have been monitored by the Environmental Testing Unit (ETU) of St. George’s University (SGU) since 2003 using fecal-indicator bacteria such as fecal coliforms and enterococci to evaluate potential health risks [4].
Lack of traceability is a major problem in finding the source of pollution of the coastal water [5]. There is a serious need for the development of methods for the identification of the sources of the pollution to facilitate the remediation of the polluted waters.
The antibiotic susceptibility profiles of dominant marine bacterial indicators were utilized to determine whether bathing in the coastal waters may expose to antibiotic-resistant bacterial indicators [6]. Our previous studies have shown the presence of antibiotic-resistant bacterial indicators and other opportunistic pathogens in the coastal waters of Grenada [5, 6, 7], however it is not known if coastal waters may harbor bacteria with resistance patterns similar to the human pathogens and if there is a potential of exposure. This is a first report documenting the antibiogram of Escherichia coli isolated from patient urine in Grenada and comparison of resistance patterns among clinical and marine isolates.
Aims of the study To compare the antibiotic resistance patterns of culture collection of E. coli strains isolated from
human urine at the St. George’s University Diagnostic Unit to the resistance patterns of collection of E. coli isolated from the coastal waters of Southern Grenada.
Predict probability of exposure to resistant bacteria in result of contact with coastal water.
Conclusions
Tropical Beach Waters Harbor Resistant Bacterial Indicators: Escherichia coli Presented Similar Antibiotic
Resistance Patterns To Uropathogenic IsolatesBy V. A. Amadi1, G. Dolphin2, R. Gue3, S. Graff3, S. V. Giesler-Kotelnikova4
1Pathobiology Academic Program, School of Veterinary Medicine, St. George’s University, St. George’s, Grenada; 2St. George’s University Diagnostic Unit; 3School of Medicine, St. George’s University; 4Environmental Testing Unit, St. Georges
University
Bibliography
Methods The marine coliforms (116) were isolated from 255 water samples, which were collected from four
coastal sites including Grand Anse Beach (GAB), in Grand Anse; Prickly Bay (PB), in L’Anse Aux Epine; Black Sand Beach (BSB); and True Blue Bay (TBB) in Grenada, West Indies (Figure 1) on a weekly basis between November 2008 and November 2010. Pure cultures of the marine species were isolated from the confirmed positives MPN tubes and identified using phenotypic characteristics (Figure 2) [6]. The prevalent bacterial indicators (Figure 3) were tested for antibiotic resistance using Kirby-Bauer method [5] using 12 and 6 antibiotics for fecal coliforms, and fecal enterococci respectively (Table 1, Figure 6)[6].
Twenty nine clinical isolates from urine were identified as E. coli using the following bacteriological analysis (Figure 2) [6], standardized using the McFarland assay and analyzed using the Kirby-Bauer assay and reference pure cultures against 11 antibiotics (Figure 5).
The antibiotic resistance patterns of marine and clinical E. coli were analyzed and compared using five antibiotics (Figure 4). The difference in the resistance patterns observed was tested using the Chi-Square (Contingency table or McNemar) and T-test analyses available in Microsoft Excel program 2007 (Table 2).
The likelihoods of exposure to dominant antibiotic-resistant bacterial indicators including E. coli , Klebsiella pneumonia, Enterobacter cloacae and Enterococcus faecalis were predicted based on MPN, compliance, and Kirby-Bauer analyses performed for four tropical beaches during a period of two years [5].
1. Fujioka, R. S. (2002). Microbial Indicators of Marine Recreational Water Quality. In C. J. Hurst, R. L. Crawford, G. R. Knudsen, M. J. McInerney and L. D. Stetzenbach (Eds.), Manual of Environmental Microbiology (2nd ed., pp. 234-243). Washington, D.C.: ASM Press.
2. Bartram, J., and Rees, G. (2000). Introduction. In J. Bartram and G. Rees (Eds.), Monitoring bathing waters - A practical guide to the design and implementation of assessments and monitoring programmes (pp. 1-15). New York: E and FN Spon.
3. Lepesteur, M., and Rooney, G. (2012). Marine pathogens. Retrieved. from http://www.ozcoasts.gov.au/indicators/marine_pathogens.jsp.4. Patel, R. H., Pedersen, K. and Kotelnikova, S. (2010). The bacteriological analysis and health risk in the urban estuary of St. George’s Bay, Grenada, West Indies. Journal of Environmental Health, (cover story), 73, 22-28.5. Amadi, V. A. (2012). Occurrence of antibiotic-resistant fecal indicators in coastal waters of Southern Grenada. Thesis .St. George's University., pp. 1-181.6. Kotelnikova, S., Bahadoor –Yetman, A. A.T. and Amadi, V. A., (2010). Occurrence of antibiotic-resistant fecal indicators in coastal waters of Southern Grenada. [Electronic Version]. WINDREF Research Institute Annual
Report. pp 19-21. Retrieved 23/3/11 from http://etalk.sgu.edu/windref/pdf/AnnualReport2010.pdf 7. Amadi, V. A., Lennon, D. E., Qureshi, A. A., Jungkind, D. L., and Kotelnikova, S. V. (2011). Occurrence of antibiotic-resistant indicators in paradise coastal water of Grenada, West Indies. . Paper presented at the 4th
Congress of European Microbiologist, Federation of European Microbiological Societies (FEMS), Geneva, Switzerland.8. Farmer, J. J., 3rd, Davis, B. R., Hickman-Brenner, F. W., McWhorter, A., Huntley-Carter, G. P., Asbury, M. A., et al. (1985). Biochemical identification of new species and biogroups of Enterobacteriaceae isolated from
clinical specimens. J Clin Microbiol, 21(1), 46-76.9. Gross, K. C., Houghton, M. P., and Senterfit, L. B. (1975). Presumptive speciation of Streptococcus bovis and other group D streptococci from human sources by using arginine and pyruvate tests (Vol. 1, pp. 54-60).
Of the 113 coliforms isolated from the 4 tested sites between November 2008 and November 2010, the E. coli comprised 50%, K. pneumoniae 34%, and E. cloacae, 5%. Figure 3 presents the percentages of different species that comprised fecal coliforms isolated and identified during our study.
Figure 4 compares the percentages of resistant strains of E. coli isolated from urine (out of 29) compared to those from the 4 marine sites tested (30 to 79 per site).
Our results showed that 11% to 25% of clinical E. coli strains were resistant to multiple antibiotics while 7% of the marine E. coli were multiresistant, and 14% to a single antibiotic. Figure 5 represents the strains of marine and clinical E. coli that showed multiple resistance and the types of antibiotics they were resistant to.
In accordance with the McNemar, and T-tests analyses, resistance patterns of strains of marine E. coli against ciprofloxacin, cephalothin, and gentamicin were not statistically different from the patterns observed in the clinical strains of E. coli isolated from patient’s urine samples between November 2008 and November 2010 (Table 2).
The likelihoods of exposure to dominant antibiotic-resistant bacterial indicators including E. coli , K. pneumonia, and E. faecalis predicted is shown on Figure 6.
Marine E. coli presented similar susceptibility patterns to uropathogenic clinical isolates against gentamicin, cephalothin, and ciprofloxacin in all tested sites. Resistance to ampicillin were similar to clinical strains only in isolates from BSB and GAB
Marine E. coli presented different resistance patterns against amoxicillin/clavulonic acid when compared to the clinical strains except in BSB.
Our model predicted highest likelihood of exposure for BSB for ampicillin and tetracycline-resistant E. coli (9%); for PB, GAB, and TBB for ampicillin-resistant K. pneumoniae (11-20%); for GAB for penicillin for E. faecalis (4%) (Figure 6).
Introduction Results
St. George’s University
Amoxicillin/Clavulanic acid = AmC-30µg
Cephalothin = CF-30µg
Ampicillin = AM-10µg
Ciprofloxacin = CIP-5µg
Gentamicin = GM-10µg
Penicillin = P-10µg
Ertapenem = ETP-10µg
Chloramphenicol = C-30µg
Cefoxitin= FOX-30µg
Cefotaxime = CTX-30µg
Cefepime = FEP-30µg
Meropenem = MEM-10µg
Tetracycline = Te-30µg
Nitrofurantoin = F/M-300µg
Trimethoprim/Sulfamethoxazole = SXT-25µg
Carbenicillin = CB-100µg
Cefixime = CFM-5µg
Streptomycin= S-10µg
Ceftriaxone= CRO-30µg
Vancomycin = Va-30µg
Nalidixic Acid= NA-30µg
Table1: List of antibiotics tested against marine and clinical isolates and their concentration
Red = Antibiotics used for comparison of the resistance patterns in populations of marine and clinical E. coli
Marine/Clinic Analysis
Antibiotic
P-value
McNemar Test Paired T-Test
Clinic vs GAB
AmC
0.066 0.013
Clinic vs PB 0.038 0.037
Clinic vs TBB 0.061 0.007
Clinic vs BSB 0.121 0.208
Clinic vs GAB
GM
0.119 0.060
Clinic vs PB 0.195 0.096
Clinic vs TBB 0.245 0.096
Clinic vs BSB 0.882 0.400
Clinic vs GAB
CF
0.463 0.222
Clinic vs PB 0.694 0.315
Clinic vs TBB 0.245 0.090
Clinic vs BSB 0.340 0.189
Clinic vs GAB
CIP
0.226 0.120
Clinic vs PB 0.107 0.05
Clinic vs TBB 0.148 0.051
Clinic vs BSB 0.826 0.464
Clinic vs GAB
AM
0.070 0.059
Clinic vs PB 0.075 0.032
Clinic vs TBB 0.030 0.006
Clinic vs BSB 0.766 0.406
Table 2: Comparison of antibiotic resistance patterns among strains of E. coli isolated from marine and clinical samples using McNemar and paired T-tests. Values in red show statistically significant difference.
AcknowledgementsThe authors are thankful to the Board of Trustees of SGU, the Chancellor Dr. C. Modica for providing funds for the research GSP-SGRI-10004-SGUIRB10008, and for the trip and the ETU team.
Figure 2: Bacteriological analysis used to determine the occurrence of antibiotic-resistant bacterial indicators
250 ml of H2O
Figure 1: Map of Grenada showing the SGU-ETU sampling sites
Grand Anse Beach Grenada
Figure 3: Species representing the isolated coliforms found in waters in the 4 coastal sites of Southern Grenada between November 2008 and November 2010
Figure 4: Percentage of resistant strains of E. coli isolated from urine compared to those isolated from the 4 coastal sites of Southern Grenada between November 2008 and November 2010
Figure 5: Marine and clinical strains of E. coli that showed multiple resistance and the types of antibiotics they were resistant to.The full names of the antibiotics tested are shown in Table 1. For marine isolates: PE, GE and BE represents sites of isolation that is Prickly-Bay, Grand-Anse-Beach and Black-Sand-Beach respectively. For clinical isolates: S1 – S7 represents individual strains.
Figure 6: Probability of exposure to antibiotic-resistant bacterial indicators in the coastal waters to southern Grenada during a period of two years.
Recommended