Embed Size (px)
Citation preview

ZS21 day old ♀
‘Chicken pox in the neonate’

Content
1. Case presentation
2. Varicella - clinical features- differential diagnosis- treatment- complications- vaccination

D1 assessment
Call to A&E resus from A&E SpR requesting Paed support
21/7 old with chicken pox in respiratory distressS
B 4/7 hx of varicella, with recent infection of sibling. Unremarkable birth history.
A
R
Oxygen via NRBM, preparing to obtain iv access and take blds
Immediate attendance of Paeds consultant

Assessment in A&E resus
Self maintained, no added sounds. A
B Self ventilating in air. Sats 92% A. Oxygen applied via NRBM at 10L, sats 100%. Increased effort of breathing. Tachypnoic >70 RR/min. Tracheal tug, recession ++. AE reduced throughout, no wheeze/crackles.
C
D
Crt 2-3 sec. Tachycardic 170 bpm. Mild-moderate dehydration.Pale.
BM 4.5. Alert & responsive. Not encephalopathic. Tone, power and reflexes normal. Fontanelle normotensive. Temp 36.8
E Abdomen soft, no organomegally, slightly full.Widespread varicella skin lesions.

Immediate management in A&E resus
Oxygen to maintain O2 sats >95%iv accessBlood cultures, FBC, CRP, U&E, VBGiv cefotaxime & flucloxacilliniv aciclovirCXRFluid bolus 0.9% normal saline 10ml/kgMaintenance ivf 10% dextrose + 0.18 NaCl
Admit Paeds, for incubator care in HDU, continuous sats monitoring
VBG in A&E :pH 7.31, pCO2 7.45, pO2 5.64, HCO3 24.2, BE -2.0, Lactate 2.7, Glu 4.5

A&E Resus0209102153

4/7 varicella, 1/7 reduced feeds, 4 hours of respiratory distress.PMC
HPC Born AGH 38/40, NVD. Normal preg, scans & birth. ?IUGR in later stages of pregnancy. No SCBU. BW 2.64 kg.Consanguineous parents (1st cousins).
Whilst 8 months pregnant, baby’s nephew had chicken pox. Mother therefore given immunoglobulin (see hadn’t had chicken pox before).
Baby’s one year old sister has recently had chickenpox which resolved 5/7 ago.
Up until this evening, baby has been well. Was feeding by breast 3 hourly, alert, no fever, wet nappies x3/d, BO x2/d

HPC Parents have been in touch with GP three times over the phone in the last 5/7. Told “providing feeding well and skin lesions improving then no concerns.”
At 1700hrs on day of admission, increased breathing rate and not feeding. Parents phones GP. Told to take to A&E.
PMH/ FH Consanguineous parents. Baby’s nephew has a VSD.Had BCG vacc at birth, nil else.

Blds from A&E
Hb 15.9WCC 27.3 Neu 14.7Plt 246
CRP 24Na 135K 6.0Urea 3.0Cl 95
CBGAfter 6 hrs
pH 7.32pO2 5.8pCO2 7.6
HCO3- 28.8BE 1.4
Na 140K 4.3Ca 1.02
Cl 102Glu 4.9
Results

Summary of WR review D2
O2 requirement overnight upto 50%, currently 28% O2 sats 99%RR70, HR 150-200, temp 38.3 despite antipyretic and reduced incubator Temp, ivf 19ml/hr 10% dex + 0.18%NaCl. PU good amounts. BO normal. NBM
CBG pH 7.3, pCO2 8.2, HCO3 29.5, BE +1.1, Glu 5.2, Na 139, K4.0
O/E moderate recession, more marked on handling. Resp effort slightly irreg. Tracheal tug & head bobbing. Decreased AE all areas esp RUZ. Widespread fine creps. Crt 3 sec. Irritable on handling.
Plan: normal saline bolus 10ml/kgregular CBGNG tube, aspirate airrepeat CXRexplained to family, may deteriorate further or become tired necessitating respiratory support +/- transferliase with PICU LGI
D2

Wd 170309101047

Liaison with PICU consultant LGI:Made aware of possible need for transfer; no further suggestions regarding Mx.PICU team spoke to virologists, nil to add.
CBGpH 7.27, pCO2 9.0, pO2 5.8, HCO3 30.3, BE +1.3, Glu 5.5, Na 140, K3.6
Oxygen requirement unchanged. Repeat CXR reviewed, RUZ consolidation improved, still extensive pneumonitis
Plan:Needs CPAPMay need PICU for ventilation
1430hrs D2
Consultant reviews on three further occasions with CBG sampling during the afternoon.
Tolerated nasal CPAP, less tachycardic, improved tachypnoeic, crt <2 sec, O2 100%
Day 2

D2CBG results day 2
time 0900 1430 1725 2000 2245
pH 7.30 7.27 7.33 7.31 7.36
pCO2 8.2 9.0 7.8 7.38 6.54
pO2 5.8 4.28 5.24
HCO3 29.5 30.3 30.3 27.8 27.6
BE +1.1 +1.3 +2.6 +0.8 +1.6
Na 139 140 141 140 140
K 4.0 3.6 4.8 4.4 4.1
Ca 1.05 1.03
Cl 102 102
Glu 5.2 5.5 4.9 4.5 3.5
CPAP

D2
Further liaison with PICU consultant LGI throughout the afternoon. Decided that in view of CPAP and possible requirement for ventilation to transfer to LGI. EMBRACE transfer arranged.
Arrived at PICU apyrexial and normal obs except RR 55 and O2 94% CPAP.CPAP discontinued as unsettled. Flow-by 5L O2 started.
PICU plan : Iv fluids 100 ml/kg/day (0.45% NaCl + 10% dextrose)Start feeds EBM via NGT 2ml/hr and gradually increase if tolerating Continue iv fluclox + aciclovirSwitch iv cefotaxime to ceforoximeD/W microbiology maneCBG. Leave off CPAP for time being.Monitor BMs
Transferred to PICU

D3Transferred from PICU day 3
Reviewed mane, no CPAP overnight. Less respiratory distress. O2 96% with flow-by O2 5L. CBG CO2 7.7, pH 7.32.
D/W Micro consultant Since ceforoxime has good Step & Staph coverage the fluclox can beStopped. Ceforoxime is preferred choice over cefotaxime. Recommends send respiratory secretions for viral & bacterial culture.
Transferred back to AGH by EMBRACE after only one night at LGI
Aciclovir and cefuroxime iv.Ivf and NG feed of EBM at 100ml/kg/dayFlow-by O2. Stable

Summary of WR review D4
O2 requirement still needing 0.2L/min, afebrile, RR 45-60, HR 140-160Feeding 3 hourly bolus via NGT, 120ml/kg/day, on aciclovir and ceforoxime.
O/E settled, asleep, no resp distress, chest clear, CVS NAD, crt <2 sec, Abdo NAD with 1-2cm liver, healing skin lesions
Plan: try breast feedingcontinue iv meds

Summary of WR review D5
Sats 100% on 3L O2. Some short bradycardias overnight. Now on C&G prem.Tolerating some oral feeds. PU’ing. BO. Parents feel she is much better.
O/E alert and moving all limbs. Chest clear with some subcostal recession. CVS NAD. ABDO NAD. Fontanelle normotensive. Oral thrush. Clinically nappy rash. Skin lesions heeling well.
Plan: start oral nystatindactarin gel for nappy areacontinue aciclovir, stop tomorrow on D5continue iv abx to complete 7/7 course then for oral abx for 7/7chase blood cultures (NAD)monitor feeding, if struggling then may need to return to NGT feeds

Summary of WR review D6
No oxygen requirement overnight. No respiratory distress. Feeding well.
Discharged on oral ceforoxime 7/748 hr ward accessFor OPD r/v with Paed consultant in 3/52, repeat CXR

OPD2709101522

Varicella
Chickenpox is a highly infectious, acute contagious disease predominantly of children under 10 years old, though it may occur at any age. Peak incidence Mar – May. It is characterised by fever and a rash, and is caused by varicella zoster virus
Around 90% of people who come into contact will develop the disease.Transmission is through 1) direct person to person contact 2) airborne droplet infection 3) through contact with infected articles such as clothing and bedding
Around 90% of adults over the age of 18 years have immunity for VZV in the UK
Reactivation of latent VZV will result in shingles which is more common in adults
In England and Wales, the incidence of chickenpox is approximately 1290 cases per 100,000 person-years
gpnotebook.co.uk

Varicella – clinical features
The incubation period is from 14 up to 21 days
chicken pox is infectious from a few days before the onset of rash develops and not more than six days after first lesions appear
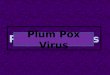
the rash begins as macular lesions which develop into papular, or vesicular lesions (filled with fluid) and later becomes pustular
chickenpox rash has a centripetal distribution - mostly on the face and trunk and sparsely on the limbs
there is erythema around the lesions and they are intensely itchy
usually the rash peaks at around 48 hours in immunocompetent people
vesicles dry and crust over, and sometimes scar if scratched to excess oropharynx and genital tract mucous membranes may be involved as well
new lesions can emerge for up to 5 days
gpnotebook.co.uk


In children under 10 years, the disease is usually mild and self limiting, but a more severe infection can be seen in
1) adults - especially in pregnant women and in smokers since they are at an increased risk of developing fulminanting varicella pneumonia 2) neonates 3) immunosupressed individuals – there is an increased risk of developing disseminated or haemorrhagic varicella
Signs of severe infections include:•respiratory symptoms (clinical respiratory signs are often absent). •densely cropping vesicles •haemorrhagic rash •bleeding from gums, haemoptysis, GI bleeding •any neurological changes - cerebellar signs, encephalopathy •persisting fever with new vesicles >6 days after onset
Varicella
General recommendationis for school exclusion for 5 days from onset of rash
gpnotebook.co.uk

• herpes simplex • disseminated herpes zoster • impetigo • drug related eruptions • contact dermatitis • erythema multiforme • Stevens Johnson syndrome • hand, foot and mouth disease • scabies • disseminated molluscum contagiosum
Differential diagnosis
gpnotebook.co.uk

Treatment
Treatment is usually symptomatic in milder disease paracetamol or ibuprofen can be given to reduce flu like symptoms, fever and pain
antivirals should be considered for patients who presents within 24-48 hours of new vesicles (indicating an evolving disease) antiviral therapy should be continued for at least 1 week
oral aciclovir may also be given to 1) immuocompetent adults and older adolescents2) Infants 3) severe infection at any age 4) immunosuppression 5)severe cardiorespiratory disease 6) chronic skin disorder
Varicella zoster immune globulin (VZIG) VZIG prophylaxis can be used in individuals who complete all of the following criteria: •significant exposure to chickenpox or herpes zoster
•a clinical condition that increases the risk of severe varicella, this includes immunosuppressed patients, neonates and pregnant women •no antibodies to VZ virus
Immunosuppressed patients should be given immunoglobulin to varicella zoster and aciclovir within two days of contact with varicella. If they develop chicken pox they should be treated with aciclovir.
Antibiotics should be given for secondary infections
gpnotebook.co.uk

Majority of children recover without any complications but neonates, adults, pregnant women and those who are immunocompromised may have more serious complications
Complications
Pulmonary involvement…….5-14% of adults
CNS involvement…….cerebellar ataxia and/or encephalitis
Secondary bacterial infections….inc osteomyelitis
Haemorrhagic complications…..GI bleeds, DIC, cerebral bleeds
In pregnancy…..significant maternal mortality and congenital VAR syndrome
Others….. arthritis, glomerulonephritis, myocarditis, and purpura fulminans
gpnotebook.co.uk

Varicella vaccination
Varicella vaccine is a lyophilised preparation which contains live attenuated organisms of the Oka strain of varicella zoster virus.
•should be administered as deep subcutaneous injection and can be given together with other live vaccines such as MMR
•children from one year to under 13 years of age; a single dose of varicella vaccine will give protection for around 90% of children
•children aged 13 years or older and adults - should receive two doses of varicella vaccine four to eight weeks apart, around 75% will have protection against clinical chickenpox (1)
gpnotebook.co.uk