Embed Size (px)
Citation preview
578
therapy, which possibly enhances zinc absorption in this disease,!was not begun until the third trimester of her first pregnancy.The second patient 11 was delivered of a 5 lb. 2 oz. (2523 g.)normal male infant. She was said to have a mild form of thedisease and had been treated with diiodohydroxyquin throughoutpregnancy.The only other case known to us is a 22-year-old woman, the
subject of a report from this centre. 12 She has had 2 pregnancies.The first terminated in spontaneous abortion during the firsttrimester. The second, in 1973, resulted in a stillborn anenceph-alic infant. Thus, out of a total of 7 pregnancies, there were 1abortion and 2 major congenital malformations. These 2 hadclose similarities to the congenital malformations of the skeletaland central nervous systems in the offspring of zinc-deficient rats.
It has been suggested 7,8,13-16 that dietary zinc deficiencymay be teratogenic in man. In particular, it has been
postulated that maternal deficiency of this essential tracemetal may be an important environmental factor contribut-ing to the high incidence of anencephaly in certain geo-graphical regions.13 There is now evidence 17-19 thatrelatively larger sections of the population in Westerncountries, as well as in the Mid-East, are at risk from sub-optimal zinc nutrition.
In animals, maternal zinc deficiency need only be tran-sient to have deleterious implications for the fetus."" Thistransient deficiency may be totally undetectable withrespect to maternal health. The pregnant rat is unable tomobilise sufficient zinc from her own tissues to supplythe needs of normal fetal development during periods ofinadequate dietary zinc. 20 Maternal zinc stores may be
depleted during pregnancy even in women who are other-wise well-nourished. 21
These obstetric histories of patients with A.E. providestrong evidence that the human fetus is also susceptibleto teratogenic effects from zinc deficiency. In addition to
emphasising the importance of adequate zinc therapy forwomen with A.E. of childbearing age, these observationsprovide a strong incentive for further research into thepossible teratogenic role of dietary zinc deficiency inotherwise healthy women.
Departments of Pædiatricsand Medicine,
University of ColoradoMedical Center,
Denver, Colorado 80220, U.S.A.
K. M. HAMBIDGEK. H. NELDNERP. A. WALRAVENS.
ZINC DURING DIURETIC TREATMENT
SIR,-Raised urinary excretion of zinc has been foundduring treatment with thiazides,22 chlorthalidone,23.24 andfrusemide.25 Increased excretion of zinc persisted even afterlong-term treatment 22,26 and the question arises whethertreatment with diuretics may cause zinc deficiency. I havedetermined serum-zinc by atomic absorption (Varian-Techtron Modell 1100) in 96 apparently healthy subjects
12. Neldner, K. H., Hagler, L., Wise, W. Archs Derm. 1974, 110, 711.13. Sever, L. E., Emanuel, I. Teratology, 1973, 7, 117.14. Sever, L. E. Lancet, 1973, i, 887.15. Hurley, L. S. Nutr. Today, 1968, 3, 2.16. Hurley, L. S., Shrader, R. E. in Neurobiology of the Trace Metals
Zinc and Copper (edited by C. C. Pfeiffer); p. 7. New York, 1972.17. Food and Nutrition Board: Zinc in Human Nutrition. Summary of
Proceedings of a Workshop, National Academy of Sciences,Washington, D.C., 1970.
18. Sandstead, H. H. Am. J. clin. Nutr. 1973, 26, 1251.19. Hambidge, K. M., Walravens, P. Proceedings of the International
Symposium on Trace Elements and Human Disease, Wayne State,Detroit, June, 1974.
20. Hurley, L. S., Gowan, J., Swenerton, H. Teratology, 1971, 4, 199.21. Hambidge, K. M., Droegemueller, W. Obstet. Gynec. 1974, 44, 666.22. Pak, C. Y. C., Ruskin, B., Diller, E. Clinica chim. Acta, 1973, 39,
511.23. Wester, P. O. Meeting of Swedish Society of Medical Sciences,
November, 1970 (abstr.).24. Wester, P. O. Acta med. scand. 1973, 194, 505.25. Steele, T. H. J. Lab. clin. Med. 1971, 78, 1019.26. Wester, P. O. Acta med. scand. (in the press).
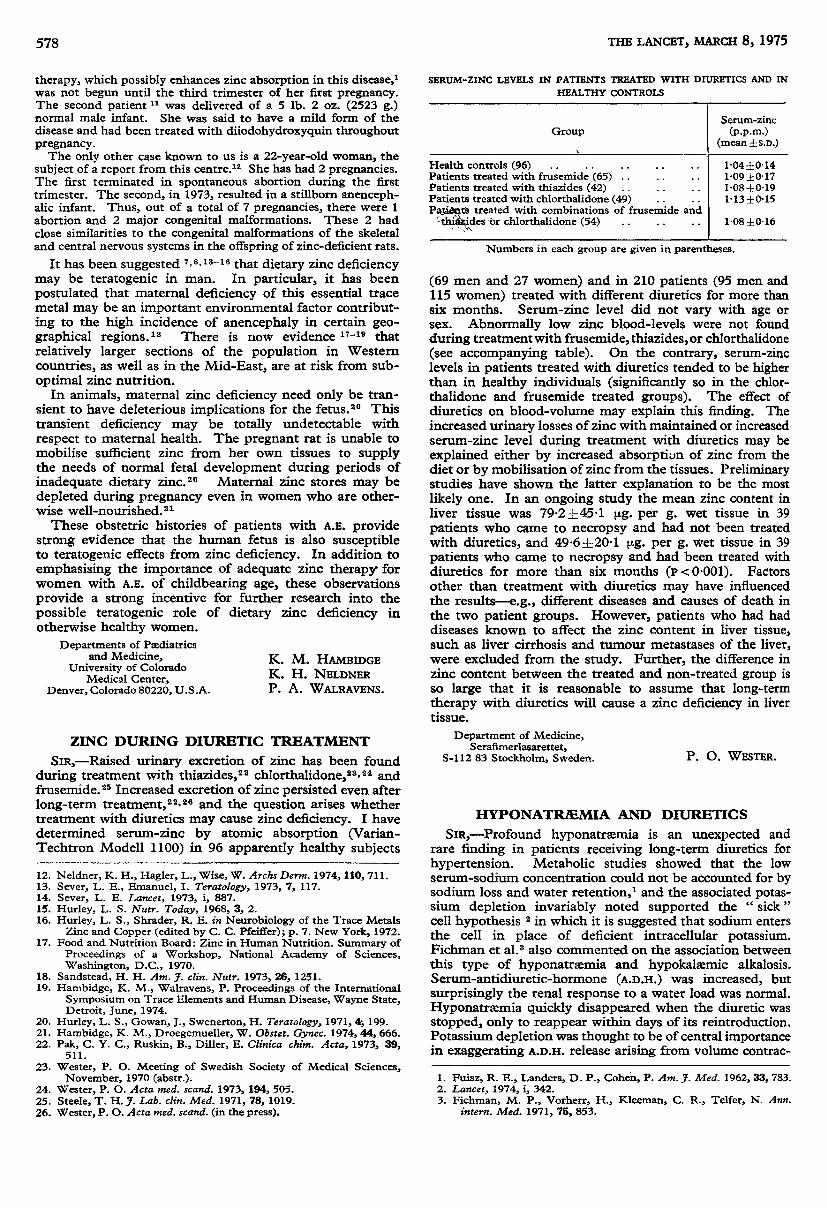
SBRUM-ZINC LEVELS IN PATIENTS TREATED WITH DIURETICS AND IN
HEALTHY CONTROLS
Numbers in each group are given in parentheses.
(69 men and 27 women) and in 210 patients (95 men and115 women) treated with different diuretics for more thansix months. Serum-zinc level did not vary with age orsex. Abnormally low zinc blood-levels were not foundduring treatment with frusemide, thiazides,or chlorthalidone(see accompanying table). On the contrary, serum-zinclevels in patients treated with diuretics tended to be higherthan in healthy individuals (significantly so in the chlor-thalidone and frusemide treated groups). The effect ofdiuretics on blood-volume may explain this finding. Theincreased urinary losses of zinc with maintained or increasedserum-zinc level during treatment with diuretics may beexplained either by increased absorption of zinc from thediet or by mobilisation of zinc from the tissues. Preliminarystudies have shown the latter explanation to be the mostlikely one. In an ongoing study the mean zinc content inliver tissue was 79-2 ±45-1 µg. per g. -wet tissue in 39
patients who came to necropsy and had not been treatedwith diuretics, and 49.6 ± 20.1 ;jt.g. per g. wet tissue in 39
patients who came to necropsy and had been treated withdiuretics for more than six months (P<0.001). Factorsother than treatment with diuretics may have influencedthe results-e.g., different diseases and causes of death inthe two patient groups. However, patients who had haddiseases known to affect the zinc content in liver tissue,such as liver cirrhosis and tumour metastases of the liver,were excluded from the study. Further, the difference inzinc content between the treated and non-treated group isso large that it is reasonable to assume that long-termtherapy with diuretics will cause a zinc deficiency in livertissue.
Department of Medicine,Serafimerlasarettet,
S-112 83 Stockholm, Sweden. P. O. WESTER.
HYPONATRÆMIA AND DIURETICS
SIR,—Profound hyponatrasmia is an unexpected andrare finding in patients receiving long-term diuretics forhypertension. Metabolic studies showed that the lowserum-sodium concentration could not be accounted for bysodium loss and water retention,l and the associated potas-sium depletion invariably noted supported the " sick
"
cell hypothesis 2 in which it is suggested that sodium entersthe cell in place of deficient intracellular potassium.Fichman et al. 3 also commented on the association betweenthis type of hyponatrsemia and hypokalæmic alkalosis.Serum-antidiuretic-hormone (A.D.H.) was increased, butsurprisingly the renal response to a water load was normal.Hyponatrxmia quickly disappeared when the diuretic wasstopped, only to reappear within days of its reintroduction.Potassium depletion was thought to be of central importancein exaggerating A.D.H. release arising from volume contrac-
1. Fuisz, R. E., Landers, D. P., Cohen, P. Am. J. Med. 1962, 33, 783.2. Lancet, 1974, i, 342.3. Fichman, M. P., Vorherr, H., Kleeman, C. R., Telfer, N. Ann.
intern. Med. 1971, 75, 853.





























