Embed Size (px)
Citation preview

Zelen Randomization: Attitudes of ParentsParticipating in a Neonatal Clinical Trial
Claire Snowdon, MA, Diana Elbourne, PhD,and Jo Garcia, MScMedical Statistics Unit, London School of Hygiene and Tropical Medicine, University ofLondon (C.S., D.E.); Centre for Family Research, University of Cambridge (C.S.); andNational Perinatal Epidemiology Unit, University of Oxford, Radcliffe Infirmary, UnitedKingdom (D.E., J.G.)
ABSTRACT: Recruitment to randomized controlled trials can be difficult for all parties involved.An alternative to the standard process has been suggested for trials in which the controlgroup receives standard treatment or nontreatment. In this approach (the Zelen design),randomization precedes consent, which is only sought from those allocated to theexperimental arm of a trial. The control group is thus unaware that randomization hastaken place. As a controversial method, this approach has been often suggested butrarely used. Here we describe how 44 parents recruited to a difficult neonatal trialthat used conventional randomization reacted to the idea of Zelen randomization. Thearguments they gave for and against the method pertain to four areas: the giving orwithholding of information, the effect on decision making, the use of data withoutparental knowledge, and the long-term impact for parents. The parents were evenlydivided in accepting or rejecting the method. Further analysis showed that those rejectingZelen randomization were more likely to be parents of infants allocated to the controlgroup. This suggests that those from whom consent would not be sought, the groupthat this approach is primarily meant to protect, are most likely to find it unaccept-able. Controlled Clin Trials 1999;20:149–171 Elsevier Science Inc. 1999
KEY WORDS: Informed consent, randomization, ethics, clinical trials, attitudes, interviews
INTRODUCTION
The giving of informed consent is a prerequisite to participation in mostrandomized clinical trials (RCTs). In theory, it is appropriate and desirable thatconsent is given; in practice, informing a person fully about medical uncertaintyand about the random allocation of treatment can be difficult and distressingfor all parties involved. These inherent difficulties are further exacerbated inspecialties where patients or their proxies are already experiencing a highdegree of emotional strain. Discomfort with the process of consent can lead to
Address reprint requests to: Ms. C. Snowdon, Centre for Family Research, University of Cambridge,Free School Lane, Cambridge CB2 3RF.
Received December 30, 1997; accepted September 7, 1998.
Controlled Clinical Trials 20:149–171 (1998) Elsevier Science Inc. 1999 0197-2456/99/$–see front matter655 Avenue of the Americas, New York, NY 10010 PII S0197-2456(98)00049-X

150 C. Snowdon, et al.
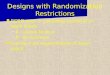
Figure 1 Conventional randomization.
poor rates of participation among professionals and therefore slow or inade-quate rates of accrual of patients [1–6]. Fully informed consent in some circum-stances has been described as “needlessly cruel,” with a statement that “at-tempts to gain the ‘informed’ participation of patients in randomized clinicaltrials are already doing harm in many individual cases [7].” Problems withconsent therefore have serious implications for the success of RCTs, for profes-sional morale, and also for the well-being of the participants.
Zelen addressed these difficulties by proposing a controversial departurefrom the conventional approach [8–12]. Ordinarily, a clinician informs potentialparticipants about a trial, and if consent is given, randomization follows. Ifconsent is withheld, the standard treatment options (including no treatment)will usually be offered (Figure 1). In Zelen’s design, the clinician randomizesbefore asking for consent, if asking for consent at all. Consent, where sought,is for the randomly allocated treatment and for trial participation but not forrandomization. This method has been termed variously randomized consentdesign, prerandomization design, and postrandomization design. In this article,we use the term “Zelen randomization.”
Two types of Zelen designs exist: “single consent” and “double consent.”In the single-consent design, the patients allocated to the control arm of thetrial are not asked for consent—they simply receive the standard treatmentwithout mention of the trial. Clinicians ask those allocated to the experimentalarm of the trial whether they consent to receive the experimental treatment. Ifthey decline, they may be receive the standard (or another) treatment (Figure2). The double consent design differs in that the patients allocated to the controlarm are asked for consent for the standard treatment and those among themwho decline may receive the experimental (or some other) treatment. Thoseallocated to the experimental arm are asked for consent for experimental treat-ment. If they decline, they may receive standard (or some other) treatment(Figure 3).
Zelen’s designs are limited in that they are applicable only to certain trials.The single consent design is suitable only when the experimental treatment is

Zelen Randomization 151
Figure 2 Zelen randomization, single-consent design.
compared with a best-known standard treatment. For a treatment to be consid-ered experimental, it is unlikely to have been fully evaluated. So in this study,we concentrate on the situation in which the experimental treatment is onlyavailable within the trial, although the double consent design is suitable onlywhen the experimental treatment is also available outside the trial.
Trials that use the Zelen approaches cannot be “blind” because the clinicianis made aware of the treatment allocation to approach patients for consent toreceive that specified treatment [13]. An assessment can, however, be madeblind to allocation. Finally, trials requiring the active cooperation of the patientin a nonstandard protocol or follow-up are inappropriate when patients havenot consented to participation.
Although there has been wide discussion of Zelen randomization, only afew trials are known to have used it, and most were conducted in the United
Figure 3 Zelen randomization, double-consent design.

152 C. Snowdon, et al.
States [for reviews, see 12, 14, and 15]. Some use cluster randomizations [e.g.,see 16], and we do not list these here. Most are in the field of cancer [17–31],but there are also examples from osteoarthritis [32] and neonatology [33, 34].
Zelen randomization has ethical and statistical advantages and disadvan-tages. Its appeal lies in the fact that in difficult circumstances a clinician neednot ask for consent for the trial or for randomization, only for treatment. Whenstress levels are high, such simplification could ease both information givingand decision making. It might also improve rates of accrual, and thereforestatistical power, in trials in which recruitment might be difficult. This mightbe because it leads to options that could be more acceptable to some patientsand clinicians, but mainly because its design is weighted to include those whomight otherwise have refused. In a conventional trial, all consenting patientsare followed-up in an intention-to-treat-analysis; that is, they are analyzed inaccordance with their allocation, regardless of whether they actually go on toreceive the allocated treatment [35]. In Zelen’s designs, all randomized patientsare followed on an intention-to-treat basis. All data are therefore appropriatefor analysis as, in both of Zelen’s designs, trialists may analyze data even fromthose who decline the offered treatment.
Concerns about Zelen randomization arise from the fact that consent forrandomization is not given in advance by any patients and that consent fortreatment on protocol is not given by all. A proportion of the patients remainunaware of their role and are automatically included in the trial. The remainderhave no explicit option to refuse to participate. Although it is widely acceptedthat patients whose data are used in epidemiologic studies are not necessarilyinformed of their roles in research, the acceptability of research without consentis less clear for RCTs. Of particular concern is the fact that not all patients aretold that their treatment is chosen by chance [36, 37].
Moreover, there may be statistical concerns over bias. If, for instance, theexperimental group of patients are required to attend for more follow-up thanthe control group, their relapses may be detected sooner. Lack of blindingmay cause differential provision of concomitant treatments and/or differentialrecruitment into the two treatment arms. The largest statistical problem maybe a reduction in power where an intention-to-treat analysis is used, the veryconcern that Zelen randomization aims to address. Power may be lost because ofa dilution effect if a large proportion of patients reject their allocated treatment(termed crossover or transfer). Theoretical and empirical studies have shownthat reduction in power resulting from crossover can be considerable, and theproblem is compounded if the extent of dilution differs between the two trialarms [38–40]. Because trialists cannot usually know the extent of crossover inadvance, sample size calculations can be underestimated.
Although ethicists and statisticians have discussed the use of Zelen random-ization, an important perspective is clearly missing from the debate: that ofthe participants themselves. Although studies have considered the views ofhealthy volunteers, [41] no evidence has yet demonstrated how those withexperience of trials feel about the Zelen approach.
This article describes the responses to Zelen randomization from parentswho had consented for their critically ill infants to participate in a conventional

Zelen Randomization 153
neonatal trial in which informed consent preceded random allocation of treat-ment. RCTs in such circumstances are of particular interest, because they inevi-tably involve persons who are extremely stressed. Parents are not only con-cerned for the well-being of their sick infants but are often within days oreven hours of their birth and any associated traumas. They may be physicallyexhausted or deprived of sleep, and the mothers may be experiencing theeffects of pain-killing or sedative drugs. Some have argued that consent forneonatal trials is not only difficult to obtain but may be inadequate, amountingto “an elaborate ritual” [42] or a “sham” [43]. In such a context, Zelen’s approachhas been seen as appropriate [43].
THE UK COLLABORATIVE TRIAL OF EXTRA CORPOREALMEMBRANE OXYGENATION
The UK Collaborative Trial of Extra Corporeal Membrane Oxygenation (TheECMO Trial) compared two methods of life support for mature neonates withacute but potentially reversible respiratory failure. The infants recruited to thetrial were at high risk of death. At randomization they were already in aneonatal intensive care unit and receiving ventilatory support (“conventionalmanagement” or CM), one of the two methods the trial evaluated. Researcherscompared CM to oxygenation of the blood via an external circuit (ECMO).Treatment using ECMO usually involved transportation of the infant, some-times by air ambulance, to one of five specialist centers. As an unevaluatedtreatment, neonatal ECMO was only available within the trial.
Discussion of procedures for recruitment involved parents’ groups at anearly stage of considering the trial. These discussions included the possibilityof Zelen randomization, especially because the two previous trials that hadbeen conducted in the United States had used it [33, 34]. As these trials hadbeen small and unusually designed in other ways, the findings were not easyto interpret. The ECMO trial team decided to use conventional recruitment,with consent preceding randomization.
Recruitment took place from January 1993 to November 1995 in over 80centers. Of the 185 trial infants involved, 101 survived to 1 year. Of those whodied, 30 were allocated to ECMO and 54 to CM. Among the survivors, oneinfant in each treatment arm was severely disabled, as assessed at 1 year ofage [44, 45]. A number of parents of surviving infants took part in the qualitativeinterview study reported here.
Sample
A pilot study for the Zelen randomization research was carried out bytelephone with eight parents (one man and seven women) of seven infantsinvolved in the ECMO trial. These parents had participated in an earlier studyassessing their responses to the trial more generally [46]. The description ofZelen randomization and the proposed questions for the main study underwentonly minor modifications after the pilot study, and so we report the views ofthese parents along with the main sample.
The questions about Zelen randomization were not the primary researchinterest for this study. We selected the sample with another research question

154 C. Snowdon, et al.
in mind, namely, how the participants responded to the results of the ECMOtrial [47]. The results showed that infants who received CM were less likely tosurvive, a finding that could have distressed some patients. We thereforeneeded to handle the study of parents’ views of the results as carefully aspossible. The primary research question necessarily shaped the sample in animportant way in that only those parents of surviving infants who had indicatedat an earlier point in the trial that they wished to see the results were includedin the study.
Parents of 71 of 95 surviving infants had indicated that they wished toreceive a copy of the findings. Practical constraints meant that not all of theseparents could be asked to take part in the study. Invitations to join the studywere dispatched in small waves, starting with those more recently recruitedto the trial, until the target of 20 interviews was reached. Other selection criteriawere that a member of the trial staff who knew something of the circumstancesof the families did not object to their inclusion, and that, for practical reasons,English should be their first language. In total, parents of 33 surviving infantswere contracted. Parents of 20 infants accepted, parents of 5 declined andparents of 8 did not reply, giving a positive response rate for this group of 61%.
The 20 in-depth interviews were carried out with parents resident in England,Scotland, Wales, and the Republic of Ireland. In all interviews, both parentswere present. We excluded from our analysis data from two cases (in both ofwhich the babies were allocated to CM). The researcher judged during theinterviews that these parents were insufficiently aware of randomization andtheir own role within the trial for the questions about Zelen randomization tobe meaningful, and so these questions were omitted.
The pilot and main study data combine to give a valid sample of 25 womenand 19 men (parents of 25 infants). The women were aged from 25 to 41 years(mean 31); the men were aged from 28 to 48 (mean 34). The interviews wereheld at variable times after recruitment to the trial: the youngest infant was 69weeks old and the oldest 234 (median 121). The disability status of the 25infants, as measured for the trial at 1 year, was that none was severely disabled;five had signs of impairment and disability not classed as severe; two had animpairment without disability, and the remaining 18 had no signs of impair-ment or disability. In the trial, 10 infants represented had been allocated tocontinue with CM and 15 to transfer for consideration for ECMO (in two casesthe infants were actually managed conventionally after transfer to an ECMOcenter). References to each set of parents in the text are followed by [CM] or[E] to indicate their infant’s allocation. All names are pseudonyms.
Methods
The interviews took place from December 1996 to September 1997. Theywere carried out by one of the authors (C.S.) either in the parents’ own homes(n 5 17) or by telephone (n 5 9; eight pilot, one main study). All were taperecorded with the parents’ permission. The interviews had a chronologic struc-ture, following the sequence of events from birth to the 1-year follow-up forthe trial. A chronologic approach helped parents tell their stories naturallyrather than responding to an obviously predefined list of questions. The fullytranscribed interviews were analyzed using a textual analysis computer pack-age, Atlas-ti [see 48].

Zelen Randomization 155
Figure 4 Description of postrandomization consent.
The discussion of Zelen randomization came at the end of the interview.The interviewer read aloud the single consent method, as shown in Figure 4,to ensure that all interviewees should receive the same basic information. Forclarity, the description outlined first the usual recruitment procedure for theECMO trial and then the way in which recruitment would have differed hadZelen randomization applied. This description thus reminded parents of theactual process and highlighted the ways in which the two approaches wouldhave differed. The interviewer asked whether any parts were unclear andreread them if necessary. Although it is not possible to say accurately howwell parents understood the concept of Zelen randomization, the interviewerexplained and clarified further when she sensed uncertainty. The interviewproceeded only when parents said they believed they understood the method.
The interviewer asked the parents to assess the notion of Zelen randomiza-tion in the light of their actual experiences of taking part in a trial (albeit withconventional randomization). She asked the parents of infants allocated toECMO to think about the issue as if they had been asked for their consent fortheir infants to be considered for ECMO, whereas she asked the parents ofinfants allocated to CM to think about the issue as if they had not been ap-proached for consent. The parents expressed their views from these perspectivesbut also frequently gave their opinions on the likely impact of Zelen randomiza-tion for those in situations different from their own.
Results
The issue of Zelen randomization engaged the interests of the parents andoften aroused strong views. All but three parents expressed an opinion on itsuse. When accepting or rejecting it, they gave reasons spontaneously and not

156 C. Snowdon, et al.
in response to predefined options. Most parents considered the ethical andpractical issues. The opinions of some reflected a belief in a general rightto information, whereas those of others were firmly grounded in personalexperience. In some interviews, parents unequivocally supported or rejectedthe approach. Others arrived at their views more gradually as various pointswere discussed. As discussion proceeded and the feelings of both members ofa couple were elicited, views were sometimes modified.
Commonly, a parent would express a clear view along with sympathy withthe opposite position. For instance, those rejecting Zelen randomization oftenappreciated the aim of easing a difficult situation. To reflect the full and multidi-mensional discussions that often took place, we present the data in such away as to show parents’ arguments for and against Zelen randomization.The opinions revolve around the method’s impact on information giving anddecision making, around the use of data, and around the longer term effects.We present the final acceptance or rejection of Zelen randomization separately.
Impact on information giving
Argument for Zelen randomization: it offers protection from dangerous informa-tion. There was a strong theme in the data that the essential value of Zelenrandomization was the avoidance of emotionally dangerous information. Par-ents perceived several different areas of danger, in the light of the particularaspects of the trial that they had personally found most difficult. The chiefdangers or difficulties posed by particular items of information lay in theirpotential to disrupt; to cause fear, anger, or regret; and to impede coping bothat the time offered and later. The various items of dangerous informationpresented by the parents were that an alternative treatment would be availablebut possibly unobtainable (i.e., the threat of no additional treatment), thatthe potentially life-changing decision about treatment would be made by acomputer, and that infants allocated to CM would not receive the alternativetreatment (i.e, the realization of the threat of no additional treatment).
Knowledge of an alternative treatment. Infants enrolled in the ECMO trialwere critically ill and already receiving CM at the time of randomization.Randomization was between continuing with CM or transferring for consider-ation for ECMO. Not surprisingly, parents who had seen their infants eitherfail to progress or actually deteriorate on CM often believed that ECMO offeredan important alternative. It was not unusual for parents to say that their doctorsalso saw ECMO as their infants’ last or only chance. In such circumstances itis difficult to avoid a perception that the experimental treatment is the onlyhope, and those interviewed for this and an earlier study certainly expresseda strong preference for ECMO at the time of consent. One parent, Jim [CM],argued that simply the knowledge of the existence of an alternative inevitablyencourages preferences: “as soon as somebody mentions they’re trying some-thing else, it means they’re trying to improve what they’ve actually got at thepresent moment.” Similarly, Rose [E] felt that it was “obvious” that their doctorssaw randomization as a means to access an alternative treatment, needed be-cause “they didn’t see much hope” with the conventional treatment.

Zelen Randomization 157
In such circumstances, the wait to find out which treatment an infant willhave can be extremely stressful, as Valerie and Jim [CM] described:
Valerie: You’re sitting there and . . . you’re on tenterhooks, like every timethe phone rang you thought it was them . . . coming back to tellyou what she was gonna get.
Jim: It was a long fifteen minutes. (Valerie: Oh aye!) I mean you thoughtit was sort of hours, you know, waiting, but it was only fifteenminutes, but having to wait for a decision like that when you knowtime’s against her anyway. I mean we were just waiting, waiting,waiting, come on, hurry up, phone rings, hope it’s them, hopeit’s them!
Zelen randomization removes the waiting time, something that appealed toHugh [CM]. Lee [E] also felt the advantage of removing this particular stressor.He found this time difficult, precisely because he was told that ECMO “probablyis the best option.”
Knowledge of randomization. Some parents found the knowledge that theirinfants’ treatments would be determined by a computer disconcerting, if notupsetting. Liz [E] was against randomization and believed that it would compli-cate an already difficult situation as so much would seem to depend on theallocation: “Not are you only faced with your daughter’s death but you’re facedwith knowing for the rest of your life that the computer made that decision.”
Rose [E] believed that the whole nature of a trial is undermining in suchstressful circumstances. She argued not that there should be no trials but thatinforming parents about them might possibly be inappropriate, in part becauseof the nature of the treatment decision:
I think being totally informed about the trial isn’t always a good thing either. . . . Initially it feels like it’s just practice or research or you know they’rejust doing things for the sake of figures and numbers. I know obviouslythey have the baby’s welfare at heart but the very word “trial,” and thenthe fact that a computer decides is making it all the more clinical, clinicaland very unreal, and almost leaving a very big major decision to a pieceof apparatus that’s plugged in is just completely wrong.
Knowledge of allocation. Zelen randomization offers the opportunity for par-ents to be spared the knowledge that another, potentially life-saving, treatmentis possible and available but not for their own infants. As shown earlier, merelythe threat of not gaining access to ECMO created difficulties for parents. Forthose whose infants were allocated to CM, this possibility became real. Jim[CM] described the process of information and allocation as “somebody buildsyour hopes up and then drops you like a ton o’ bricks.” Because nothingactually changes for these parents, this process could seem “pointless” (Valerie[CM]). Martin [E] implied that randomization was a form of deciding whichof several infants should be given a treatment in the context of scarce resources.He was not the only parent to draw such a conclusion [46]. Parents who holdthis view believe that introducing the possibility and then the impossibility oftreatment is inconsiderate. Martin preferred the idea of Zelen randomization,

158 C. Snowdon, et al.
arguing that “at least you’d not be offered it first and then refused.” Anna [E]believed similarly that “it would make it harder knowing that she could havethis treatment and she couldn’t get on it.”
Frequently, parents described allocation to CM as a form of rejection. Janet[CM] argued that it is difficult to have a sense of perspective at the time:
Your mind isn’t able to cope . . . [and] it feels like a rejection when you’retold your baby isn’t going, it does feel like a rejection, and you can onlyreflect when things are a lot more calm.
Hilary and John [CM] believed that hope for their daughter was actuallyslipping away when she was assigned to CM. John describes how knowing ofthe existence of another treatment complicated his experience:
I remember when they told us she wasn’t going to have the ECMO treatmentand how we felt then. That’s when we started to, you know, you could seethat she was getting worse and of course not going to have this treatmentthat’s so successful in America, then that’s when alarm bells started to ring. . . and then seeing her get worse. I thought well, hold on, you know, ifshe’d been on this ECMO would this be different?
Argument against Zelen randomization: It is a deprivation of essential informa-tion. The counterargument was that Zelen randomization would deprive par-ents of information to which they have a right. However difficult such knowl-edge might be, some parents believed they ought to be told about the trial atthe time of randomization. Ellen [E] believed that protection was not a realbenefit, saying categorically, “I don’t think you are protecting them though.You’re just not informing them.”
Some interviewees thought it inappropriate deliberately to withhold infor-mation from parents, judging it simply important to know what was happening.For instance, Valerie [CM] said, “it’s your baby, you want to know if they’redoing something.” Andrea [E] argued, “I would want to know what all myoptions were up front,” and Gail [CM] commented: “I’m somebody who thinksthat you should know everything that’s going on, and if your child’s health isgoing to be part of some trial, that you should know about it.”
Mary [E] believed the information that they were part of a trial was importantin its own right:
I can understand that [for] parents who aren’t randomized on to ECMO itwould be a great disappointment. It would have been terrible for us becausewe did feel like it was her last hope but I still think we would have likedto have known and to have been part of the project.
Information gathering can be an important coping mechanism, and someparents, such as Russell [E], wanted every piece of available information. Under-standing the problem could help them gain some sense of control. They talkedwith great appreciation about how valuable it had been to have their questionsanswered, sometimes over and over again if they had been unable to absorbcertain details. Some had also valued the answers they had received, such asGrant [E], who had said to his child’s doctor, “I want it straight, I want itblunt.” Those who valued information objected to the deliberate withholding

Zelen Randomization 159
of details of the trial and characterized the Zelen approach as “underhand”(Tina [E]), “morally wrong” (Lorna [CM]), not “ethically right” (Adam [E]),and not “very fair” (Sandra [CM]). Liam [E] argued that not informing thosein the control group would be discriminatory: “I say that you’re really discrimi-nating . . . against that branch of the trial and that you’re depriving them ofthe information, depriving them of knowledge.”
Some also perceived a wider consequence of Zelen randomization: the cre-ation of a climate of suspicion, in which parents could not trust those on whomthey had to rely. Neil [CM] described Zelen randomization as occurring “behindthe parents’ back” and believed it had implications for the way doctors wouldbe seen:
They are kind of messing around with your child’s life a bit, whereas Ithink the way we had it, which was quite up front, face to face with thedoctor, him explaining what it was about, was a more honest approach andyou know exactly what you’re dealing with.
Russell [E] thought it a compromise that was “kinder but less honest.” Hethought it would undermine trust in hospitals and the medical profession asa whole, commenting: “It does cast a shadow over everything that you’re toldin a hospital and is that right?” Tina [E] believed it would be detrimental toher relationship with staff: “Whatever the outcome, I think I would feel, ifthey’d kept that from me, what else have they kept from me? . . . I’d find itvery hard to trust the people that were involved.” Lorna [CM] felt similarly:“As much as it protects the parents from getting involved into all the worriesand all the ins and outs of the trial, it’s the other side, the hiding informationstarts to come into my mind.”
Impact on decision making
There were two very different perceptions of the impact of Zelen randomiza-tion on decision making, which derived from parents’ focus either on thecontrol or on the experimental group. For those focusing on the control group,the Zelen approach appeared to remove a decision. For those focusing on theexperimental group, one decision replaced another. Lorna [CM] made thislatter point in the first pilot interview of the study. She argued that parents inthe experimental group would effectively be given a choice between treatmentsas they were offered the option of ECMO and trial participation, or turningdown the trial and continuing with CM. We incorporated this issue into thestudy and put it to the rest of the parents.
Argument in favor of Zelen randomization: Parents would not have to decidewhether or not to accept randomization. The decision to take part in the trial andto accept randomization had not been particularly easy for many of the parents.If parents saw the trial as their infants’ last or only chance, they commonlyrepresented it as having constituted great personal responsibility, even if theyhad made it very quickly. The decision was burdensome and some would havepreferred to avoid it. Zelen randomization was attractive to two of the parents,Duncan [E] and Helen [CM]. Helen believed that it would have simplified her

160 C. Snowdon, et al.
family’s situation: “At least the parents haven’t got to make that decision, thatbig decision, do we go for it or don’t we? Somebody else is making that decisionfor you.”
Argument against Zelen randomization: Parents have a right to make a decision. Al-though parents would not be able to choose which treatment their childrenwould have, some argued unequivocally that the decision about trial entry andpermission for randomization should still be theirs. Hilary [CM] argued thatin not knowing about the trial and randomization, parents are denied thechance to exercise their responsibilities for their children:
I mean, it was our child and we had to make that decision, hard as it was,and much as we didn’t want to do that. . . . You’re taking that choice outof their hands by not telling them in a way. . . . We knew the facts and wewere told to make a choice, so it was our choice to do that. You’re takingthat away to a certain extent because you’re not telling anyone unless theyactually get on to the trial.1
John’s [CM] description of the time when they learned their daughter wouldnot have ECMO is quoted above. It was then that “alarm bells started to ring.”Despite his difficulties, he too did not believe he would have preferred not toknow about ECMO and the trial at all:
John: Very difficult, isn’t it really, very difficult for everybody. I thinkthe way they told us was best, don’t you?
Hilary: Yes.
John: Give you that choice and then you can live with that. We madethe choice and we had to live with it. If things had gone againstus then, we could handle that, but not to be given that, not to betold. . . . (John shook his head and did not finish his sentence).
Tina [E] stated clearly that she and her husband had had a difficult timebut did not see Zelen randomization as the answer:
It was very hard the way it was done, but I’m not sure if it’s . . . I’m notsure that not telling parents until after they’ve made the decision is righteither because parents have the right to know if someone is making adecision behind their back. I mean as hard as the decision was to make I’mglad that I actually had the chance to make the decision. . . . I would wantto know what was actually going on even if . . . my baby stayed on aventilator. If I was in a trial I would want to know I was in a trial.
Argument in favor of Zelen randomization: Parents in the experimental groupwould have an opportunity to make a decision about treatment. Views on the shiftin the nature of decision making for those in the experimental group weregiven by 20 parents, 6 of whom merely indicated the choice they would havemade. All except Angela [E] said they would have chosen ECMO.
1 It was common for parents to use the term “trial” and ECMO interchangeably or to believethat infants allocated to CM were not part of the trial.

Zelen Randomization 161
Moira [CM] believed that, despite the difficulties, parents should be able tochoose treatment themselves. Ellen [E] would have welcomed the opportunityto have made that choice, even in the face of uncertainty:
I think it would have been nice to have had a choice, just because that wasone of the things I found difficult, the fact that the final decision was outof my hands. It wouldn’t have made the decision any easier though, Isuppose, because you don’t know the results of ECMO and conventionaltreatment. You’re still making a blind decision.
Tina [E] argued that the decision might be easier for parents if it were astraightforward choice between accepting or rejecting ECMO but went on toreject any possible benefit as it is outweighed by the withholding of informationfrom some parents:
I would hate to find out that I had been in a trial . . . however hard thedecision was to make about putting him forward for the randomization bythe computer as opposed to making a straightforward yes or no decision.I realize that would have been easier at the time but I still think I wouldhave felt very angry to have been in a trial and to have found out afterthe event.
Russell [E] and Duncan [E] both thought that decision making after random-ization might be easier because they believed the doctors would not maintaina neutral stance in these circumstances. This would not necessarily be the casebecause the condition of equipoise (uncertainty) would still pertain. Russelland Duncan, however, perceived neutrality not as a response to uncertaintybut as a means of protecting parents whose infants might be subsequentlyallocated to CM from the certainty that ECMO is the better treatment. In thismodel, there would be no need for neutrality, because ECMO would be readilyaccessible to the parents who were asked to make a choice. Duncan said:
They might try to sell ECMO more to you, you see, because the way it wasgiven to us, they weren’t allowed to show a bias towards ECMO, and therewas like a witness with the consultant to make sure he was unbiased, butif our doctor had the ECMO and was to have told us about the ECMO, hewould have sold it to us more forcefully.
Frank [CM] drew attention to a possible complication that can arise whenparticipants can choose the treatment, the dilution effect mentioned earlier: “Ifthe trial had been run, as in the second method there, and we’d have beenoffered ECMO and hadn’t taken it . . . is that not gonna disrupt the . . . results?”
Argument against Zelen randomization: Parents in the experimental group wouldface a difficult decision. Lorna [CM], who had immediately pointed to thiscrucial way in which Zelen randomization would change the nature of consent,argued that the experience would be more rather than less complicated. Shebelieved that if parents were told that their infants had already been allocatedto ECMO, their situation would not necessarily be easier than with conventionalconsent before randomization:
Then you are really making a decision. Yes, you’ve got ECMO, but if youdon’t want it you’ve got conventional treatment, then they really are making

162 C. Snowdon, et al.
a decision, whereas we found it quite a relief to put that decision on therandomization of the computer. That helped us live with what might havehappened at that time. It took that feeling away that we were deciding thefate of what could happen.
Lorna’s husband Neil argued that he had always seen randomization assomething helpful and positive and saw Zelen randomization as regressive.He believed that parents would face an almost impossible decision: “if a doctorhad come in and said to me, ‘Right there’s ECMO treatment and traditionaltreatment, you choose,’ I mean, how could I choose?”
Bill [CM] did not like the idea of having to make a choice either, “I think ifyou make the choice and you made the wrong one, in your own mind youwill forever be reproaching yourself.” Andrea [E] saw randomization as prefera-ble to the responsibility she would feel in such circumstances: “I just wouldn’twant to have to make that choice to say, whether yes you take him off conven-tional, or you put him on ECMO. I think randomization is better.”
At the time of the interview, Angela [E] was convinced that ECMO savedher son’s life but said that when she had consented to the trial she had beenvery wary of it. She had been swayed by his deterioration and the confidenceof the recruiting doctor. She was disconcerted to feel that she might not havemade the “right” decision if she had had to make it herself: “To be perfectlyhonest, I didn’t know what was best for him. . . . When they told me it wasan incision in the neck and he was going to be connected to a machine, myinstinct said no! no! They are going to experiment on your baby!” Andrea [E]also believed the conditions at the time were not conducive to clear decisionmaking and said, “You’re not thinking totally straight, . . . 95% of you is totallynumb anyway.”
Although Hilary and John [CM] had wanted to make the decision to enrollin the trial, they did not believe that it would have been better, if allocated toECMO, to have chosen the treatment themselves. They both believed that thedifficulty lay in the unevaluated nature of ECMO. Hilary likened it to a decisionto take an experimental drug and John commented, “Regardless of what’shappened in America, it was still considered experimental here.”
These parents believed that Zelen randomization would deny those allocatedto ECMO the protection afforded by randomization. From their reactions, it isclear that Zelen randomization only benefits those who reject randomizationor who view it negatively.
Use of data
Argument supporting Zelen randomization: Use of data is of no conse-quence. Some accepted that information about their infants would be used inthe trial without their knowledge. Shirley [CM] stated simply: “It wouldn’thave made a difference.” The saying “what you don’t know doesn’t hurt you”was used by three parents, Duncan [E], Liz [E], and Jerry [E]. Duncan andDoug [E] both saw the information as important to the advancement of scienceand were not concerned about the situation. Liz, Jim [CM], and Doug talkedspontaneously about other situations in which information had been recordedwithout a subject’s knowledge and permission and believed was not a problem:

Zelen Randomization 163
Liz [E]: There are all sorts of organizations out there who know about yourfinances. They know everything about you. You don’t know whothey are or where they are. We get letters through in the mail, andwe think what’s that, you know. I can’t see a problem with that. Itwouldn’t harm them in any way.
Hugh [CM] thought it would not be a problem as long as the name of theinfant would not be included, and Grant [E] did not believe that there was aproblem in using data from children without their parents’ knowledge:
I guess it’s a case of what the eyes don’t see, it doesn’t bother the mind,may be very naive, I don’t know. I . . . I . . . it wouldn’t have bothered mehad they used Jonathan’s notes and things. If he had died, if it meant thatit would go towards proving that maybe ECMO was right or the other waywas right, if it meant saving children’s lives.
Argument against Zelen randomization: Parents have a right to permit or prohibitthe use of data. In contrast to the views described above, Liam [E] distinguishedbetween information used without permission in other contexts and in the caseput to him:
Maybe it happens in every walk of life. Consequently statistics are gatheredabout what you do. You’re on such a study and you’re unaware of that,but it seems where you have such a significant report, you’re not talkingabout, you know, how much people spend or watching them shopping . . .you’re talking [about] a treatment of babies, a treatment of people.
Others also rejected the idea (Lee [E], Lorna [CM], Adam [E], and Ellen[E]. The idea of using information without parental permission made Ellenuncomfortable: “You’re using people in a way . . . that’s just using informationfrom people when they don’t know they’re being watched.”
The decision to become involved in the trial did have certain benefits forparents that would have been lost through Zelen randomization. They couldfeel commitment to the trial and often welcomed the opportunity to be involvedin follow-up. Ellen [E], Shirley [CM], and Neil [CM] mentioned the practicaldifficulties of getting information for the follow-up that would arise if parentsdid not know their infants were in a trial. Neil [CM] extended the consequencesof having only limited follow-up for the trial to the qualitative interview study:
I mean, at the time, fair enough, you don’t know what’s going on behindthe scenes if you like, but eventually these things have a nasty habit ofcoming out, and from your point of view, if you want to have some furtherfeedback from the parents, you can’t do that, because you can’t say to them,“well, look, you’ve entered into this trial but you didn’t know about it. Canyou tell me how you feel about it now?”
At a later date, the ECMO trial results were announced and sent to thoseparents who had requested a copy. Knowledge of the outcome of the trial gavesome an important sense of having contributed to medicine and to the well-being of other families who might benefit [47]. Crucially, this contribution hadcome about through an active decision rather than by default. Access to theresults of the trial was not only desirable to many but was seen by Adam [E]

164 C. Snowdon, et al.
as an argument against Zelen randomization: “I don’t think it’s ultimately fairon the, on the parents either to never know that they were in a trial and neverknow the results of it if they wanted to know.”
Adam went on to make the point that Zelen randomization can also denya parent the opportunity of an altruistic decision and the possible benefits thatcould have held, particularly should the infant die: “In a way, if he didn’tsurvive, the fact that you’d been in a trial . . . at least you’re knowing that youare actually, in a way, you are helping others. I think that’s one consolationyou could have if your child didn’t survive.” Rita [E] made this point also.
Long-term impact
Information for trial participants can be managed after Zelen randomizationin two ways. Participants allocated to the control group can be left unawareof their roles in the trial or at a later date may be informed to facilitate follow-up. The crucial aspect for this study would have been that parents would nothave known about randomization as it was carried out. The description ofZelen randomization used in the study did not address what would havehappened in the future.
Argument supporting Zelen randomization: Bereaved and control-group parentsmay be better able to cope in the long term. Some parents addressed the fact thatthe current system of recruitment has implications that go beyond possibledistress at the point of allocation. Parents of infants allocated to CM wereoften seen as more vulnerable, especially if their infants went on to die. Thoseattracted to the idea of Zelen randomization often believed that its value layin the protection it offered this group from further emotional difficulties. Sophieand Ray [E] created a scenario in which a baby treated with CM was deterio-rating:
Ray: I think you’d feel more upset knowing that there’s a possibilitythat there was something else out there they could do, but youjust haven’t, you just haven’t been the lucky one.
Sophie: Not been chosen . . . it definitely would have been a different kettleof fish if they’d said to you about it and then . . . come back andsaid, “I’m sorry, she can’t go on it anyway.”
Ray: Yeah. And then it had got to such a stage where she was maybe,God forbid, slipping away, and you’d say “well do something else.”
Sophie: Yeah. You’d be desperate for the chance to be on the trial then,wouldn’t you, and you’d know about it, but you’d know shecouldn’t be on it.
Ray: I think you’d be ranting and raving really, then, wouldn’t you.
Parents saw the information as particularly difficult in cases where infantsdied after treatment with CM. Although parents were originally asked to con-sider this situation in terms of the allocation that was made for their owninfants, they frequently shifted the focus instead to the bereaved parents, andimagined vividly how they would have felt themselves. Jerry [E] said: “I think

Zelen Randomization 165
you might be a little bit bitter in that respect, knowing there might have beensomething out there to save your child’s life and it wasn’t used, whether it beon the trial or not.”
For Tina [E], Melanie and Lee [E], and Emma [E], the whole success of theZelen approach hinged on never learning about the trial, an alternative treat-ment or randomization. Clearly, any protection offered by Zelen randomizationis undermined if parents holding this opinion receive this information at alater date. For these parents, Zelen’s double consent design would simply undoany benefits that randomization without consent might offer.
Argument against Zelen randomization: Parents may be upset to learn later thattheir infants are in a trial. Parents often raised the issue of learning about thetrial later and speculated how they and others would feel. Grant [E] pointedout that if parents learned later about their child’s involvement in a trial, theirreactions would be shaped by the means by which they found out. He believedthat it would be acceptable to parents if it was done “properly by letter,” buthis wife Rita commented that if he were in that position himself he would“probably still have gone spare.”
These parents had accepted the trial and random allocation of treatment atthe time of consent, but some believed that they would be angry if they wereonly informed retrospectively. Mary believed that if she had found out aboutECMO at a later time she would have been “up in arms” and would have goneback to the consultant to demand an explanation of why her daughter had notreceived ECMO. Valerie [CM] said she would have “flipped.” Lorna [CM]would have wondered whether they were not told at the time “because therewas something they were hiding from us. Was there something more sinister?”Andrea [E] would have been “devastated” and “gutted” had her son died onCM and she learned afterward about the possibility of ECMO:
If it hadn’t been known to me, though it hadn’t been available to us . . . Ithink I would have been even more devastated. Again, just because—notthat it’s making you any guarantees, but it’s just that extra door that I thinkat the time like—that you just need to do down as many avenues as youpossibly can to satisfy—it’s selfish but it’s just to satisfy yourself, knowing,well, at least we did everything absolutely possible for him.
Angela [E] believed that the effort to ease the short-term situation wouldgenerate long-term problems:
At the time it would be kinder to the parents . . . especially if you are goingto be given a hope and then have it taken away from you, but later I thinkyou would get very, very angry people who would somehow feel that ifthey had known they could have done something about it, and I think ifat the time you know it is happening it just adds to the heartache . . . Butif someone was to actually find out that their child was used for the trialand they weren’t even told about it or something like that, I think youwould get very, very angry people, because it’s like—it’s like a wound ifsomebody—if you—if something reopens that later and you were to havelost a child and then find out that they had done this without your knowl-edge, I think you could be dealing with people’s anger then.

166 C. Snowdon, et al.
All parents included in this study had been through the allocation of treat-ment. Even if the rationale behind randomization was not clear, all knew thataccess to ECMO was not guaranteed. Yet only three parents (Jim [CM], Lorna[CM], and Tina [E]) pointed out that the allocation and the outcome wouldnot have been any different, regardless of the system used for consent. Parentsof babies allocated to CM would not have been able to change the allocation.Parents may possibly believe that it would be difficult to take on board issuesabout allocation at a later date because they would be angry, with their focuson deprivation of a treatment rather than anything else.
Acceptance and rejection of Zelen randomization
After discussing at length, the parents were asked whether or not they wouldsupport the use of Zelen randomization. They were very evenly split, with 21in favor and 20 against, 1 unable to decide, and 2 giving insufficiently clearstatements to categorize. In some cases the interviewer was surprised to hearsupport for Zelen randomization, given earlier accounts of a need for informa-tion (Russell [E], Bill [CM], Grant [E], Rose [E], and Frank [CM]).
Being of a qualitative nature, this study involves examining the views of asmall group of persons in depth. Data from such studies are not usually condu-cive to statistical analysis. The views expressed here are, however, readilygrouped into categories of support or rejection of Zelen randomization. Thesedata are based on the treatment of each parent individually rather than inpairs, because the views within a pair were not always the same. As Table 1shows, there were no particular differences between men and women in theirviews, but parents of infants allocated to CM were likelier to reject Zelen ran-domization.
DISCUSSION
Zelen randomization has been the subject of professional debate, but noattention has previously been paid to the views of those with actual experienceof trial participation. The way in which parents in this study often engagedwith and extended the issues involved in the subject was impressive andindicated the value of their particular perspective. Their interest was rooted inpersonal experience, and they empathized highly with others in similar situa-tions. Despite the short time available for consideration of the concept, theyassessed in a rounded and full way how Zelen randomization might succeedor fail.
Although evenly divided in how they summed up their view of Zelenrandomization, parents often appreciated both sides of the arguments. Somethought it highly disappointing and cruel to inform worried parents about atreatment that may not be possible. Because such a process was thought likelyto have major ramifications for those whose infants did not survive, some sawZelen randomization as a kinder approach. In the opposing view, by whichthe gathering of information is a coping strategy or access to information wasconsidered a right, parents saw the withholding of crucial details not only asundermining but also denying the active and protective role of a parent onbehalf of a sick infant. Essentially, parental views about Zelen randomization

Zelen Randomization 167
Table 1 Distribution of Views of Parents According to Treatment AllocationECMO CM Total
For Zelen Emma* Janet [P] 21Eileen and Jerry Helen [P]Melanie and Lee Jim†Anna and Eric Shirley and HughJulie and MartinSophie and RayDuncan‡Liz§Rose and LiamGrant‖
Against Andrea [P] Gail and Bill 20Zelen Ellen and Adam Hilary and John
Tina and Doug Valerie†Mary [P] Sandra [P]Rita‖ Jo and FrankAngela [P] Lorna and Neil [P]
Moira and Dan
Other Russell* 3Penny‡Carl§
Total 27 17 44
The symbols *†‡§ and ‖ are used to link members of a couple where they have differed in theiropinions. Parents interviewed for the pilot study (see text under Sample) are indicated by [P].
stemmed from the importance they attached to access to information, and itis precisely this variable element that makes the process so difficult to adaptto individual cases. Clearly, one cannot find out whether or not a person wantsinformation without first alerting him or her to the fact that information isavailable. The feature that was so desirable for approximately half of the parentsin the sample was not that they would actively have chosen not to accessdangerous information but that they would have preferred not to have beenaware of it at all.
The concept of dangerous information was complicated and existed on bothsides of the debate. It could relate to the impact of the revelation that howeversick an infant may be, he or she could not access an available treatment; itcould also relate to the revelation at a later time, to those in the control group,that the situation was not as it had seemed. Parents saw both approaches toconsent as having consequences for those involved, both in terms of their well-being and in terms of their relationships with medical professionals.
One might consider this research with parents to have done little to indicatehow to manage such a difficult situation, given the even division in the viewsexpressed. Perhaps this is due to the fact that, as Liam [E] pointed out, thereis “no perfect answer.” Ultimately, we cannot devise a system that will incorpo-rate the opposing views presented here. Ellen [E], for instance, argues that ifher infant was allocated to CM in a trial using a Zelen randomization, shewould prefer never to be informed about the trial, whereas Hilary and John

168 C. Snowdon, et al.
[CM] rejected the use of Zelen randomization outright, even though they hadexperienced a time of thinking that their daughter would die once allocatedto CM. These views cannot be reconciled. Instead, one view must take prece-dence over another.
Several finding have emerged from this research that may further the debate.First, it became clear that Zelen randomization would not necessarily minimizestress for those allocated to an intervention group. One of the functions ofrandomization is to deal with equipoise. When it is not known which treatmentis most beneficial (clinical equipoise), it serves to distribute fairly the unevalu-ated risks and benefits among participants. It removes from clinicians andpotential participants the need to decide which treatment they believe will bemost efficacious when there is insufficient evidence to make the choice clear.The decision each participant makes in a trial is, in theory at least, whether ornot to accepted randomization and whichever treatment one is allocated to.With single-consent Zelen randomization, potential participants allocated toan experimental treatment would, however, be faced effectively with a straight-forward choice between experimental treatment on protocol or standard careoff protocol, despite the context of medical uncertainty. In effect, the potentialparticipants have to make precisely the choice the trial is set up to avoid. Someparents saw this as an impossible decision. When a choice is unwelcome, theZelen randomization itself could cause stress and difficult decision making.
Second, we must look more closely at the views of those who are seen toneed most protection. Zelen randomization is designed with the intention ofminimizing emotional difficulty in RCTs involving standard or nontreatment,particularly for those allocated to the control group. In some circumstances,as in the ECMO trial, the standard treatment administered to the control groupcan be seen not as the safe, tested, and established approach, as might havebeen predicted, but as an inferior treatment. In this study, parents belongingto precisely the group that Zelen randomization was partly designed to protectwere most likely to reject it. This happened despite the fact that these parentswere also aware that the trial showed that infants who received CM were lesslikely to survive.
If we must favor one view over another on the basis of the evidence presentedhere, then the arguments against Zelen randomization from this sample wouldseem compelling, not because they represent a majority’s view but because thedissenters are more likely to have been those in the control group.
A recent editorial suggested that Zelen randomization ought to have beenused for the ECMO trial [43]. In response, Meren [49] disagreed and put forwardthe same arguments that some of the parents in this study articulated strongly:
Your argument seems to suggest the need for sensitive information practiceand skilled support rather than depriving frightened and confused parentsof information. . . . [T]hey, rather than the law, should decide how muchinformation they receive—but withholding information deprives them ofthis particular decision and betrays their trust.
Although rejecting of the use of Zelen randomization does mean that thosepreferring not to be informed about a trial, if allocated to a control group, willhave to face unwelcome information, it also highlights the need for attentionto be paid the process of seeking consent to ease the situation as far as possible.

Zelen Randomization 169
CONCLUSION
The subject of Zelen randomization proved to be a highly engaging topicfor the parents in this study, who were divided in its acceptance or rejection.They saw a trade-off of protection and information, desirable to some, anathemato others. They also saw an opposition of the short-term benefits and long-term consequences. It became clear from their responses that Zelen randomiza-tion would create very different circumstances for participants depending ontheir allocation. Those who found this method, and the circumstances it wouldcreate, to be unacceptable were most likely to be parents of infants allocatedto the control group. Had this system been used for the ECMO trial, theseparents would not have been informed of their allocation at the time, andknowing this may have afforded them a higher degree of empathy with others insuch a situation. Their particular rejection of Zelen randomization is importantbecause their perspective is unique; although the questions are to some degreehypothetical, these parents speak from personal experience. In cases whereparticipants perceive standard treatment as the less desirable option, Zelenrandomization may well widen rather than narrow any perceived inequitiesbetween the groups in a trial.
This study was funded by the Department of Health and the Nuffield Foundation and developedfrom research funded by the Wellcome Trust. We thank Carole Harris from the ECMO Trial officeand Sally Roberts at the Centre for Family Research for their help. Our thanks also go to theparents who kindly gave the information upon which this research is based.
REFERENCES1. Benson AB, Pregler JP, Bean JA, et al. Oncologists’ reluctance to accrue patients
onto clinical trials: an Illinois Cancer Center study. J Clin Oncol 1991;9:2067–2075.2. Renfrew MJ, McCandish R. With women: new steps in research in midwifery. In:
Roberts H, ed. Women’s Health Matters. London: Routledge; 1992:81–98.3. Taylor KM. Integrating conflicting professional roles: physician participation in
randomized clinical trials. Soc Sci Med 1992;35:217–224.4. Taylor KM, Margolese RG, Soskolne CL. Physicians’ reasons for not entering eligible
patients in a randomized clinical trial of surgery for breast cancer. N Engl J Med1984;310:1363–1367.
5. Taylor KM, Feldstein ML, Skeel RT, et al. Fundamental dilemmas of the randomizedclinical trial process: results of a survey of the 1737 Eastern Cooperative OncologyGroup investigators. J Clin Oncol 1994;12:1796–1805.
6. Tognoni G, Alli C, Avanzini F, et al. Randomized clinical trials in general practice:lessons from a failure. BMJ 1991;303:969–971.
7. Tobias JS, Souhami RL. Fully informed consent can be needlessly cruel. BMJ1993;307:1199–1201.
8. Zelen M. Statistical options in clinical trials. Semin Oncol 1997;4:441–446.9. Zelen M. A new design for randomized clinical trials. N Engl J Med 1979;300:
1242–1245.10. Zelen M. Alternatives to classic randomized trials. Surg Clin North Am 1981;
61:1425–1432.11. Zelen M. Strategy and alternate designs in cancer clinical trials. 1982;66:1095–1100.12. Zelen M. Randomized consent designs for clinical trials: an update. Stat Med
1990;9:645–656.

170 C. Snowdon, et al.
13. Horwitz RI, Feinstein AR. Advantages and drawbacks of the Zelen design forrandomized clinical trials. J Clin Pharmacol 1980;20:425–427.
14. Ellenberg SS. Randomization designs in comparative clinical trials. N Engl J Med1984;310:1404–1408.
15. Altman DG, Whitehead J, Parmar MK, et al. Randomised consent designs in cancerclinical trials. Eur J Cancer 1995;31A:1934–1944.
16. Grant AM, Elbourne DR, Valentin L, et al. Routine formal fetal movement countingand risk of antepartum late death in normally-formed singletons. Lancet 1989;2:345–349.
17. Moertel CG, Child DS, O’Fallon JR, et al. Combined 5-fluorouracil and radiationtherapy as a surgical adjuvant for poor prognosis gastric carcinoma. J Clin Oncol1984;2:1249–1254.
18. Fisher B, Bauer M, Margolese R, et al. Five year results of a randomised clinical trialcomparing total mastectomy and segmental mastectomy with or without radiation inthe treatment of breast cancer. N Engl J Med 1985;312:665–673.
19. Wolmark N, Fisher B, Rockette H, et al. Post operative adjuvant chemotherapy orradiation therapy for rectal cancer: results from NSAPB protocol C-01. J Natl CancerInst 1988;80:30–36.
20. Fisher B, Wolmark N, Rockette H, et al. Post operative adjuvant chemotherapy orradiation therapy for rectal cancer: results from NSAPB protocol R-01. J Natl CancerInst 1988;80:21–29.
21. Fisher B, Redmond C, Poisson R, et al. Eight year results of a randomised clinicaltrial comparing total mastectomy and lumpectomy with or without irradiation inthe treatment of breast cancer. N Engl J Med 1989;320:822–882.
22. Santen RJ, Worgul TJ, Samojlik E, et al. A randomized trial comparing surgicaladrenalectomy with aminoglutethimide plus hydrocortisone in women with ad-vanced breast cancer. N Engl J Med 1981;305:545–551.
23. Wells SA, Worgul TJ, Samojlik E, et al. Comparison of surgical adrenalectomy tomedical adrenalectomy in patients with metastatic carcinoma of the breast. CancerRes 1982;42(Suppl):3454s–3457s.
24. Lange B, Halpern S, Gale G, et al. Trimethoprim-sulfamethoxazole and nystatinprophylaxis in children with acute lymphoblastic leukaemia. Eur Paediatr HaematolOncol 1984;1:231–238.
25. Mansour EG, Gray R, Shatila AH, et al. Efficacy of adjuvant chemotherapy in high-risk node negative breast cancer. N Engl J Med 1989;320:485–490.
26. Blichert-Toft M, Brinker H, Andersen JA, et al. A randomized trial comparingbreast-preserving therapy with mastectomy in mammary carcinoma. Acta Oncol1988; 27:671–677.
27. Blichert-Toft M, Rose C, Andersen JA, et al. Danish randomized trial comparingbreast-conservation therapy with mastectomy: six years of life-table analysis. J NatlCancer Inst Monogr 1992;11:19–25.
28. Sell A, Jakobsen A, Nerstrøm B, et al. Treatment of advanced bladder cancer categoryT2 T3 and T42. Scand J Urol Nephrol Suppl 1991;138:193–201.
29. Ganz PA, Haskell CM, Figlin RA, et al. Estimating the quality of life in a clinicaltrial of patients with metastatic lung cancer using the Karnofsky performance statusand the Functional Living Index—Cancer. Cancer 1988;61:849–856.
30. Riethmuller G, Schneider-Gadicke E, Schlimok G, et al. Randomised trial of mono-clonal antibody for adjuvant therapy of resected Dukes’ C colorectal carcinoma.German Cancer Aid 17-1A Study Group. Lancet 1994;343:1177–1183.
31. Antman K, Amato D, Wood D, et al. Selection bias in clinical trials. J Clin Oncol1985;3:1142–1147.

Zelen Randomization 171
32. Chang RW, Falconer J, Stulberg SD, et al. Prerandomization: an alternative to classicrandomization. The effects on recruitment in a controlled trial of arthroscopy forosteoarthrosis of the knee. J Bone Joint Surg 1990;72A:1451–1455.
33. Bartlett RH, Roloff DW, Cornell RG, et al. Extracorporeal circulation in neonatalrespiratory failure: a prospective randomized controlled study. Pediatrics 1985;76:479–487.
34. O’Rourke PP, et al. Extracorporeal membrane oxygenation and conventional medicaltherapy in neonates with persistant pulmonary hypertension of the newborn: aprospective randomized study. Pediatrics 1989;84:957–963.
35. Lewis JA, Machin D. Intention to treat—who should use ITT? Br J Cancer1994;68:647–650.
36. Ellenberg SS. Randomized consent designs in comparative clinical trials. Stat Med1992;1:131–132.
37. Marquis D. An argument that all prerandomized clinical trials are unethical. J MedPhilos 1986;11:367–383.
38. Anbar D. The relative efficiency of Zelen’s pre-randomization design for clinicaltrials. Biometrics 1983;39:711–718.
39. Brunner E, Neumann N. On the mathematical basis of Zelen’s prerandomizeddesigns. Meth Inform Med 1985;24:120–130.
40. Matts J, McHugh R. Randomization and efficiency in Zelen’s single-consent design.Biometrics 1987;43:885–894.
41. Gallo C, Perrone F, De Placido S, et al. Informed versus randomized consent toclinical trials. Lancet 1995;346:1060–1064.
42. Mason S. Obtaining informed consent for neonatal randomised controlled trials—“an elaborate ritual”? Arch Dis Child 1997;76:F143–F145.
43. Anon. Your baby is in a trial [editorial]. Lancet 1995;345:805–806.44. UK Collaborative Trial Group. UK collaborative randomised trial of neonatal extra-
corporeal membrane oxygenation. Lancet 1996;348:75–82.45. UK Collaborative Trial Group. UK collaborative randomised trial of neonatal extra-
corporeal membrane oxygenation: follow up to one year of age. Pediatrics 1998;101:690.
46. Snowdon C, Garcia J, Elbourne D. Making sense of randomization: responses ofparents of critically ill babies to random allocation of treatment in a clinical trial.Soc Sci Med 1997;45:1337–1355.
47. Snowdon C, Gardia J, Elbourne D. Reactions of participants to the results of arandomized controlled trial: an exploratory study. BMJ 1998;317:21–26.
48. Muhr T. A prototype for the support of text interpretation. In: Tesch R, ed. QualitativeSociology. New York: Human Science Press; 1991.
49. Meren JG. Ethics of consent for babies in randomised clinical trials [letter]. Lancet1995;345:1370.