Embed Size (px)
Citation preview

Zahra Khudeira, PharmD, MA Medication Safety Manager Sinai Health System - Chicago, Illinois February 1, 2012 Webinar for Pharmacy One Source

Describe potential vulnerabilities in the medication use process
Discuss various strategies that can improve the medication use process and increase patient safety
Share implemented improvement strategies Provide a practical medication safety
initiative checklist for possible implementation at your site

Mount Sinai Hospital – community teaching and research hospital
Licensed 319 bed
Safety Net Hospital Level I Trauma Center Pediatric Hospital – Level III NICU All services except transplant and burn Schwab Rehabilitation Hospital
Licensed 102 beds

Serve both hospitals Open 24/7 No satellites 1.9 million doses dispensed
annually Orders processed daily Hybrid CPOE and paper orders ADC and carts Management Hierarchy
Director Operations Manager Clinical Coordinator Medication Safety Manager
▪ IS Pharmacist
Clinical Specialists MICU ED Pediatrics
Decentralized Pharmacists M – F AM shift only SICU Medicine Telemetry Oncology
PM shift – centralized Overnight shift – centralized, two
pharmacists, two technicians Two PGY1 residents Twenty technicians (delivery tech) One lead technician Offer several student rotations

Computerized Prescriber Order Entry (CPOE) except peds, am care and ED
Bar-Code Medication Administration (BCMA) for Rehab and Psych unit only
Automated Dispensing Cabinets (ADC) MedCarousel® High Speed Packager - PacMed Smart infusion pumps

Each site is unique Every pharmacy department is unique Some of the suggestions may involve capital
funds and it will not be feasible to implement at your site
Other interventions have no financial investment associated with their implementation
Some initiatives involve hospital wide implementation
You need to analyze your site and adopt what is practical

A discipline of pharmacy that focuses on the entire medication use process and tries to reduce adverse events and mitigate risks to maximize optimal patient outcomes
▪ Errors will happen. Humans are involved.
Errors can be prevented by designing systems that make it
hard for people to do the wrong thing and easy for people to do the right thing. Adapted from To Err is Human- Building a Safer Health System
We are perfecting the medication delivery system to be safe
for every patient, every time, while making it easy for caregivers to do the right thing, and impossible to do the wrong thing.

Medical errors are the eighth leading cause of death and are estimated to account for somewhere between 44,000 and 98,000 deaths in the United States each year (IOM, 1999).
Where are we now? Preventing medication errors, which account for
nearly 20% of adverse events overall and affect about 4% of all hospital stays, is a goal among patient safety organizations, and healthcare providers.


Do not forget the procurement stage=inventory management
Many look alike items can be eliminated at the purchasing stage Think of ‘system’ changes Accept that errors will happen and build a system around that Perform DUEs around the monitoring stage

High Risk Areas
NICU, Chemo Clinic High Risk Processes
Chemo, TPNs High Risk Routes
Epidurals, IV Complex processes
PCA, Chemo Complex Treatments
Chemo, TPNs, weight based heparin, argatroban High Risk Patient Populations
Peds, NICU, Oncology, Geriatrics, HD High Risk Medications
Heparin, chemo, PCAs, anticoagulants, anesthetics, NMB, thrombolytics

From most effective to least
ISMP 2006

Favorites list for physicians Orders limited based on unit (ICU meds are
not viewable in general medicine unit) Check order sentences Use q12 hrs not BID, when appropriate (anti-
arrhythmics, anti-hypertensives, etc) Streamline products Order sets that reflex labs Clinical decision support

Most disregarded phase of med use process Pharmacists – please do not forget this phase Analyze sedation, pain, BP, infection cure rates,
length of therapy, etc. Analysis of amp/gent use in neonates length of therapy of amp/gent vancomycin monitoring vitamin K routes/doses – adherence to ACCP
guidelines darbepoeitin appropriateness


Personnel and technology Drug information software Communication Drug storage Environmental factors Employees – competency, education, CE,
modules. Hire well. Patient information available to staff IS – lock out any order entry if height and weight
is not documented Scales – now locked to ‘kg’ only
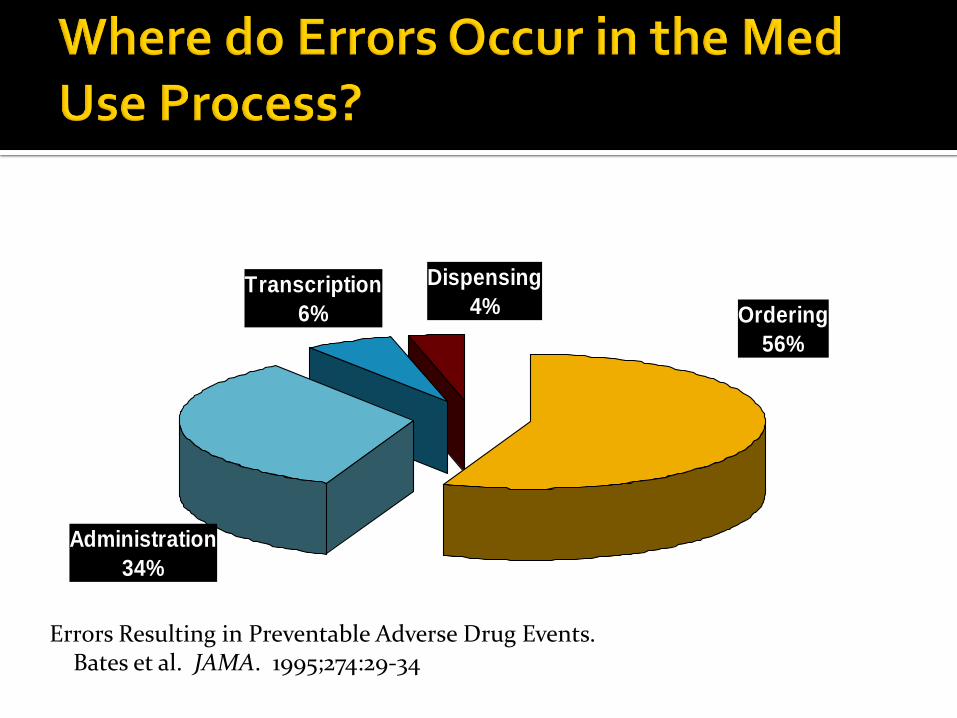
Dispensing
4%Transcription
6% Ordering
56%
Administration
34%
Errors Resulting in Preventable Adverse Drug Events. Bates et al. JAMA. 1995;274:29-34

ICU Pharmacists rounding reduced preventable ADEs by 66% Leape LL, Cullen DJ, Dempsey Clapp M, et al. Pharmacist participation on physician rounds
and adverse drug events in the intensive care unit. JAMA 1999;282:267-70.
Med/Surg pharmacist rounding reduced preventable ADEs by 78% Arch Intern Med. 2003;163:2014-2018
ER Med Rec for patients that are admitted
Choosing appropriate therapy and reducing costs
Decreasing medication errors and ADRs Pediatrics
Continuous reinforcement of safety I am known as the ‘safety queen’ by other depts
Always on stage for staff to highlight safety issues
Discuss errors and how we can prevent them
Email, staff meetings, morning huddles All new employees receive a two-hour session during orientation
Medication errors, ADRs, human errors, examples of actual pharmacy errors
Discuss policies and procedures Educate nurses during orientation about reporting ADRs and
medication errors In a just culture, reckless behavior is not tolerated, but mistakes
caused by system failures are seen as learning opportunities.

Manager Expectations & Actions Promoting Patient Safety 1. My manager says a good word when he/she sees a job done
according to established patient safety procedures. 68% agree, 11% disagree 2. My manager seriously considers staff suggestions for improving
patient safety. 79% agree, 8% disagree 3. Whenever pressure builds up, my manager wants us to work faster,
even if it means taking shortcuts. (negatively worded) 79% disagree, 3% agree 4. My manager overlooks patient safety problems that happen over
and over. (negatively worded) 63% disagree, 18% agree
Lucian Leape, MD, Harvard School of public Health
The single greatest impediment to error prevention in the medical industry is “that we punish people for making mistakes.”
▪ Story of Eric Cropp
Healthcare can be safe but not risk-free

Creating an open, fair, and just culture Creating a learning culture Designing safe systems Managing behavioral choices

Every one must report ‘near misses’, medication errors and ADRs
Data collection leads to the identification of a problem
Authorized personnel need to take action on data and provide feedback to reporter

Internally developed system Minimal data is asked in report Used for trending The goals of reporting is to analyze the
information and identify ways to prevent future errors from occurring
Most staff members provide details in person The reporting of incidents is tied to the annual
pharmacist performance review (ADRs, and pharmacist interventions are also included in annual review).

Operations must be solid Analyze categories of interventions Determine if a P & T approved intervention
can be endorsed by P & T. It will save time for pharmacists. Example – simvastatin and amiodarone
interaction – pharmacist can decrease dose of simvastatin to 20 mg.
Example – no baseline INR available – pharmacist can order baseline INR if warfarin is needed

Use data to prioritize and improve medication management
Transform data into information Reduce variation in med management process Do not be a ‘drip’
Data-rich, information poor
Use the data to prioritize and improve medication safety
Use the data to improve processes not punish staff

Anticoagulation – INR greater than 5, PTT greater than 120
Digoxin levels above 2 Use of kayexylate Use of naloxone BG levels less than 50

0
2
4
6
8
10
12
14
16
18
20
JAN FEB MAR APR MAY JUN JUL AUG SEP OCT NOV DEC
Pe
rce
nta
ge
of
dig
ox
in le
vels
ab
ove
2
mg
/dL
Supratherapeutic Digoxin Levels for MSH 2011

Trigger tool INR > 5 or PTT >120
Monthly review presented to pharmacists, Med Exec team Weight issues – scales now locked to kg only Weight must be documented per visit – no medications can be
verified until the patient’s weight is in the demographic area Order form revised Pharmacist reviews, calculates dose, monitors nurse as she
programs pump Heparin vials for boluses no longer on units
▪ Pharmacy draws up boluses ▪ Hand delivered to nurse ▪ Heparin drip only stocked in pharmacy

Chemicals in the pharmacy - Glacial acetic acid Oral keterolac Bicillin Propoxyphene/APAP (Darvocet) Rosiglitazone before the FDA’s action Heparin variety – no 10,000 units/mL vials!
5000 units vial for VTE prophylaxis
1,000 units/mL (10 mL vial) for boluses and HD area
1,000 units/0.5 mL PF for NICU TPNs

Metformin/Metronidazole 500 mg Stocked next to each other Some mistakes did occur in picking ISMP recommends to stock only the
metronidazole 250 mg tablets to avoid error Brought issue and resolution to the Med Safety
Committee ID physician did not agree to extra pill burden Pharmacy manually highlighted and segregated
metronidazole 500 mg until new technology implement (now – MedCarousel – barcoding)

Administer the drug at a rate no greater than 25 mg/minute.
If the patient reports burning at the injection site, stop the IV immediately to evaluate for possible arterial placement or perivascular extravasation
FROM ISMP WEBSITE

Removed vials from ADCs, except in ED (for IM only)
Built an order set for IV administration only Dispensed from the main pharmacy only Use has decreased


New ‘confused medications’ now are stocked
Communicate with nurses
Post flyer on ADC

Colors: Midazolam 2mg/2mL, Lorazepam 2mg/mL, Morphine 2mg/mL, Morphine 10 mg/mL

Streamline stock Design, layout Open line of communication with staff NMB in separate refrigerator Clearly labeled Outsourcing of cardioplegia, PCAs, epidurals,
etc. Separate location for pediatric/NICU
medications

IV medications are associated with 61% serious and life threatening errors
IV push boluses are administered too fast 73% Harmful errors occur most often as the
administration phase

The most impactful strategy to improve patient safety
Share a story of one patient and how the pump prevented an error from reaching the patient – at a staff meeting or morning huddle

Buretrols increase the risk of medication being infused without being properly prepared and labeled in the pharmacy.
Smart pumps made buretrols obsolete.
Used in OR/PACU area Spoke to stakeholders Agreed to remove stock

No financial commitment Naloxone – dilution Clinimix bag – activate bag Phenytoin – use filter Ampules – use filter needle/straw

A two year review of medication errors revealed 12 errors or near-misses
Clear and brief alerts were formulated to avoid alert fatigue
Alerts addressed: ▪ Drug dosing ▪ Preparation ▪ Administration ▪ Appropriateness ▪ Peer-checking
One year review revealed one error Acetaminophen dose miscalculated, no harm

Fentanyl patches in ED Alteplase 50 mg and 100 mg – housewide Atypical antipsychotics depot from Psych unit
Pharmacy prepares individual doses in syringe
Hand deliver to nurse
Parenteral vitamin K (newborn doses are an exception)

Immediate huddle with all involved individuals
COO
CMO
CNO
Risk Manager
Patient Safety Officer
Others depending on error

F = Find a problem O = Organize a team C = Clarify the problem U = Understand a problem S = Select an intervention P = Plan D = Do S = Study A = Act


How will the next patient in your work area be harmed?
How can we prevent this harm? Please provide a suggestion or solution to address
this issue
Ask questions at a staff meeting – written - anonymous


Streamline Chemical Stock
Organize pediatric stock
TALLman lettering implemented in ADC and order entry system
Use oral syringes
Optimize patient labels

Anesthesia trays – look alike labels, sealed with tamper proof tape, high alert labels, quantities determined with OR staff
Changed daily Wrapped in plastic Back ups in pharmacy and Anesthesia stock
room


Two chamber amino acid and dextrose • Needs to be activated (mixed) before infusing • Different concentrations • Used for day 1 of life for preemies • ISMP reported on several cases that occurred • Was that ISMP newsletter shared with NICU staff? • Did it occur at Mount Sinai? • Now an ADC alert and picture of activation in ADC

95% NICU, 5% Adult Review order form first Is all pertinent labs/information on form? Analyze one month’s worth of forms
Did any patient develop high triglyceride?
Overfeeding?
Refeeding syndrome
TPN panel in lab can now be ordered

Outsource High Risk Compounds Heparin 2 units/ml – NICU Epidurals Fentanyl drips PCAs – morphine and hydromorphone

Infusion bags are not stocked on unit Heparin boluses drawn up in Pharmacy and
hand delivered to the nurse Pharmacists also dose heparin and monitor
PTTs

PCA Argatroban Alteplase for vascular patients Heparin for vascular patients

Medications that have the highest risk of causing injury when misused are known as high-alert medications.
The top five high-alert medications identified by the ISMP study are insulin; opiates and narcotics; injectable potassium chloride (or phosphate) concentrate; intravenous anticoagulants (heparin); and sodium chloride solutions above 0.9 percent.

ISMP Sound-alike Look-alike Highlighted in med rooms Note on MAR and labels Note on Med Carousels Note on ADC pockets

Proper destruction of patches ISMP articles Policy
FDA alert about patches and burns
Fentanyl, scopolamine, clonidine, nicotine, etc
Built in the CPOE system ADC alert Flyers in MRI suite

Individualized doses Batched in pharmacy Protects patients from over dosing on long
acting and intermediate acting insulins Saves money

Implemented several hard stops in CPOE
Pregnant status and statins, warfarin, sedatives
Beer’s criteria STARRT and STOPP Black box warnings CrCl with antibiotics Metformin Glyburide – Glipizide in patients over 65 year Zolpidem dose in over 65 years old patients

Anna’s slide
One hour session discussing Medication Safety
Powerpoint presentation for new pharmacy employees detailing our common errors
Sign off for accountability Pharmacy resident and pharmacy manager
prepared it Took about two hours total time to prepare
presentation with pictures One hour session on USP 797

Reviewed at Med Safety Committee Prepared by PGY1 resident
US FDA Patient Safety News videos on youtube – ≈ 2 minute videos
Mistakenly swallowing Spirvia and Foradil capsules
Mix-up between Insulin U-500 and U-100
Preventing dosing errors with alteplase
Reporting adverse events to FDA Medwatch
Beyond Blame video from ISMP – 8 minute video

Outpatient areas Imaging Department Cath Labs Hemodialysis center Inpatient areas where there is no pharmacist
assigned to the unit

Assign each pharmacist a topic per year to own and work on during slow times Due date prior to annual review
Each gets a standing order assigned to them Each gets a policy to update/ keep current Let them choose a topic of their interest Lead a journal club Organize an area in pharmacy – peds, liquids,
prepacking, chemo, IV, overstock, supplies, perform sterile technique assessment of techs, etc.

Standing Items
ADRs
Anticoagulation ADEs and other ADEs
Medication errors
FDA warnings
▪ Actions taken at Sinai Health System
IS corner
▪ CPOE improvements

My soldiers at the frontline Deputized and entrusted Report back to me if they can not handle an
issue Rely on quick feedback and communication
Leader – competency and trust

IOM – To Err is Human ismp.org patientsafetyauthority.org npsf.org cdc.gov fda.gov asmso.org

Statewide mandatory reporting began in June 2004 for hospitals, ambulatory surgical facilities and birthing centers.
A few examples below: Anticoagulation Management Service Clostridium Difficile Strategies Contrast-Induced Nephropathy Diagnostic Error Falls in Radiology HYDROmorphone Risk Reduction Insulin Therapy Managing Clinical Emergencies Patient Flow in the Emergency Department Patient Safety Practices Verbal Orders

Nurse AdvisERR Acute Care Quarterly report ASSESS-ERR worksheet
STERILE WATER FOR IRRIGATION
Could not eliminate it
Shared mental model Relationships Respectful Make the right connections/contacts Good observers/listeners Choose the ‘low hanging fruit’ first
Builds credibility
Celebrate small successes with staff. It will motivate the staff for bigger initiatives.

Status quo is not acceptable Take some action….any action Commit to make a change Consider one project every six months or even
year ..multiply by the number of pharmacists
The patient is at the center of everything that we do!
“By failing to prepare, you are preparing to fail.”
Benjamin Franklin

Special thanks to the pharmacy staff for continuously providing ideas on improving medication and patient safety
Safety begins with you! Every one owns quality and safety.

Challenge – too much to do! Resolve missing medication conundrum More clinical services Initiate ambulatory care pharmacist roles Disease state education to patients – asthma, diabetes, HF Implement iv room software FMEA on implementing new iv room technology Build new library for pediatric syringe pump Re-design medication rooms using lean methodology Fully implement TeamSTEPPS & CUSP Imaging dyes dosing tables Fully implement culture of safety Integrate smart pumps with CPOE Roll out CPOE in ED and Peds Implement EMAR house-wide Become 100% cartless Implement scanners at ADC Pharmacist driven Med Rec Utilize lean methodology in central pharmacy processes Shadow nurses on each unit performing medication pass – one unit/month Focus on areas where no pharmacist is present – IR, imaging, Cath lab, GI lab, etc Join Morbidity and Mortality discussions ICD 9 Codes for Medication Related ADRs Pharmacist to monitor vanco, AMG, warfarin