Embed Size (px)
DESCRIPTION
Socioeconomic and Racial/Ethnic Differences in the Discussion of Cancer Screening: “Between-” vs. “Within-” Physician Differences. Yuhua Bao, Ph.D. † , Sarah Fox, Ed.D. † , Jose Escarce, M.D., Ph.D. ‡ † Center for Community Partnerships in Health Promotion, - PowerPoint PPT Presentation
Citation preview

Socioeconomic and Racial/Ethnic Differences in the Discussion of Cancer
Screening: “Between-” vs. “Within-” Physician Differences
Yuhua Bao, Ph.D.†,
Sarah Fox, Ed.D.†,
Jose Escarce, M.D., Ph.D. ‡
† Center for Community Partnerships in Health Promotion,
UCLA General Internal Medicine/Health Services Research
‡ UCLA GIM/HSR
Funded by the NIH EXPORT Center at UCLA/DREW (YB), NCI (SAF) and AHRQ (JE)

2
Socioeconomic and Racial/Ethnic Disparities in Cancer and Cancer Screening
Recent years saw steady decline in cancer death rates and improvement in cancer survival
However, disparities by patient socioeconomic status (SES) are substantial in Adherence with cancer screening guidelines Stage of diagnoses Mortality and survival
Differences by patient race/ethnicity are less consistent, but Mortality from all cancers is highest among Blacks

3
The Role of Physician-Patient Communication
Differential adherence to cancer screening is partly due to differences in access to care. However,
Disparities in cancer screening utilization exist even among people with a usual source of care
People of low-SES more likely to cite “I didn’t know I need it” and “Dr did not recommend it”
as barriers to cancer screening (Finney et al. 2003) Disparities in cancer screening communication may
have played a role

4
The “Within-” vs. “Between-” Physician Differences
Once patients get access to health care, treatment disparities arise because Patients of different SES or race/ethnicity are
treated differently by the same physicians
(“within-physician” differences),
AND / OR They are treated by a different group of physicians
(“between-physician” differences)

5
“Within-physician” Differences

6
Possible Mechanisms for“Within- Physician” Differences
Patient-level factors Low-SES and/or racial/ethnic minority patients are less
aware of the need for cancer screening (Finney et al. 2003) They are less assertive / proactive in clinical encounters
Physician-level factors Physicians may perceive them to be less interested (van
Ryn and Burke 2000) Physicians may have greater difficulties in assessing their
needs and preferences (Balsa and McGuire 2001; 2003) Patient-physician interaction
Patient preferences and physician attitudes and perceptions are reinforced (IOM 2002)

7
“Between-physician” Differences
Dr. A
Dr. B

8
Possible Mechanisms for “Between- Physician” Differences
Physicians serving disproportionately more minority or low-SES patients May be less well trained Are less likely to be board-certified (Bach et al. 2004) Are more likely to be foreign medical school graduates
(Bellochs and Carter 1990) May be less knowledgeable about national preventive care
guidelines (Ashford et al. 2000) They may also have less resources in the community such
as Specialty groups with cancer screening capabilities Institutional support for preventive care
Some of the “within-physician” differences may be reinforced to become practice patterns

9
Research Question
How much of the differences in cancer screening discussion were due to “within-” vs. “between-“
physician differences?

10
Data: the Communication in Medical Care (CMC) Studies
A research series that promotes physician-patient communication on important preventive care topics
Aimed at developing and testing a physician-patient communication model to change patient health behaviors
The second and third studies in the series (CMC2&3) are both randomized controlled community trials that Teach the model in a Continuing Medical Education (CME)
program Focused on cancer screening behaviors

11
Data: Patient and Physician Samples Physicians: office-based, primary care, practicing at least
50% of the time CMC2: Los Angeles County CMC3: all southern California except LA County
Patients: having seen and expect to see study physician regularly, speaking either English or Spanish CMC2: 50-80 CMC3: 65-79
Data pooled from CMC2&3 baseline Physicians: N=191 Patients: N=5978 On average, patients had seen their physicians for 5 years Number of patients per physician: mean=31, median=30,
range: [2, 83]

12
Outcomes of Interest: Cancer Screening Discussion
“Did Dr. ever talk to you
about …”
Rate of Discussion (%)
Fecal Occult Blood Test (FOBT) 36.8
Sigmoidoscopy 30.9
Mammogram (female only) 67.1
Prostate Antigen Test (PSA)
(male only; CMC2)
46.0

13
Statistical Strategies
Probit model of cancer screening discussion Two specifications for each cancer screening discussion
outcome Model 1: Patient characteristics only
to assess the “overall” differences
Model 2: Model 1 + Physician Fixed Effects Differences that remain reflect “within-physician” differences “Between-physician” differences=“Overall” – “Within”
We report probabilities of discussion for each racial/ethnic or SES
group compared to a reference group Bootstrapped standard errors (and p-values) to provide
statistical inferences

14
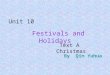
By Education: Discussion of FOBT
* p <0.05; ** p<0.01
Compared to college graduates
-0.13
-0.03
-0.09
-0.03-0.04
-0.02
-0.14
-0.12
-0.1
-0.08
-0.06
-0.04
-0.02
0
Diff
eren
ce in
FO
BT
Dis
s. R
ate
Lt high school High school Some college
"Within-" Differences "Between-" Differences
**
**
** **
*

15
By Education: Discussion of Mammogram
* p <0.05; ** p<0.01
Compared to college graduates
-0.071
-0.004
-0.028
-0.013
-0.037
-0.005
-0.08
-0.07
-0.06
-0.05
-0.04
-0.03
-0.02
-0.01
0
Diff
eren
ce in
Mam
mog
ram
Dis
s. R
ate
Lt high school High school Some college
"Within-" Differences "Between-" Differences*

16
By Education: Discussion of PSA
* p <0.05; ** p<0.01
Compared to college graduates
-0.192
-0.01
-0.144
0.026
-0.063
-0.012
-0.25
-0.2
-0.15
-0.1
-0.05
0
0.05
Diff
eren
ce in
PS
A D
iss.
Rat
e
Lt high school High school College graduates
"Within-" Differences "Between-" Differences
**
**

17
By Income: Discussion of FOBT
* p <0.05; ** p<0.01
Compared to annual income of $75+
-0.02
-0.06
-0.02
-0.04
0.02
-0.03
-0.07
-0.06
-0.05
-0.04
-0.03
-0.02
-0.01
0.00
0.01
0.02
0.03
Diff
eren
ce in
FO
BT
Dis
s. R
ate
Less than $15k $15k - $35k $35k - $75k
"Within-" Differences "Between-" Differences**
*
*

18
By Income: Discussion of Mammogram
* p <0.05; ** p<0.01
-0.001-0.007
0.013
-0.004
0.05
-0.003-0.01
0
0.01
0.02
0.03
0.04
0.05
0.06
Diff
eren
ce in
Mam
mog
ram
Dis
s. R
ate
Less than $15k $15k - $35k $35k - $75k
"Within-" Differences "Between-" Differences
Compared to annual income of $75+

19
By Income: Discussion of PSA
* p <0.05; ** p<0.01
-0.108
0.019
-0.021-0.028
0.023
-0.03
-0.12
-0.1
-0.08
-0.06
-0.04
-0.02
0
0.02
0.04
Dif
fere
nce
in
PS
A D
iss.
Rat
e
Less than $15k $15k - $35k $35k - $75k
"Within-" Differences "Between-" Differences
Compared to annual income of $75+

20
Summary of findings
Disparities by education Strong education gradient in the discussion of all three types of
cancer screening Most of the education differences arose within physicians
Disparities by income Less consistent across different screening methods, but Seemed to have arisen because of “between- physician”
differences Differences by race/ethnicity
Asian/white differences in the discussion of FOBT and PSA were mostly “within-physician” differences
Same physicians were much more likely to have discussed mammogram with black than white patients

21
Study Limitations
Patient self-report of clinical encounter experience may not be consistent with what really happened If low-SES patients tend to under-report physicians’ discussion
Both within- and between- differences by SES are biased up But hard to say how that might change the relative magnitude of
the two types of differences It depends on the distribution of low (vs. high) SES patients
across physicians
On the other hand, it is arguable that what patients recall is what matters
Small sample sizes for some racial/ethnic groups Findings regarding racial/ethnic differences should be
interpreted with caution

22
Implications
Patient education plays an important role in determining what happens in a clinical encounter Tailor patient informational materials to the needs of low-
education patients Raise the awareness of physicians about the challenges faced
by low-education patients
Physicians are not evenly distributed across communities of different levels of income Targeting physicians practicing in low-income communities may
be especially promising
Geographic accessibility of providers is important to low-income patients