-
cation of mitomycin C, with all radiotherapy treat-
ments completed within 72 hours. Exposure of
surrounding tissue to radiation was minimized
using custom lead cut-outs manufactured
postoperatively.
An antineoplastic agent derived from Streptomyces,
mitomycin C inhibits DNA synthesis by cross-link-
ing strands of the DNA double-helix, preventing
tissue proliferation.4 Historically, mitomycin C has
proven successful in the fields of ophthalmology
and tracheal surgery.5 Early case reports in the use
of resection and adjuvant mitomycin C to treat
keloids were equivocal,1 although the concentra-
tion of mitomycin C used in these early case
reports was low (0.4 mg/mL). Gupta and Narang5,
in a 2010 review, successfully treated 26 pinna
keloids by applying a higher concentration of mito-
mycin C (1 mg/mL) immediately postoperatively
and 3 weeks after surgery. We have also found
success with a higher concentration and staggered
application of mitomycin C.
Conclusion
Keloids are commonly encountered and notoriously
difficult to treat, representing a therapeutic
dilemma. Although many keloid treatment modali-
ties are available, monotherapy has historically
yielded poor results. The authors acknowledge that
the number of patients treated in this series is
small, and the follow-up period is limited; to fur-
ther validate these results, more patients should be
treated with the above protocol, and the follow-up
period should be extended to at least 5 years to
monitor long-term results. Multimodal therapies of
resection with adjuvant radiation and resection
with adjuvant mitomycin C have each shown
moderate success; the authors propose that
combination of these established therapies into a
triple therapy of resection with adjuvant mitomycin
C and radiotherapy needs to be further explored
and may represent a promising treatment algorithm
for this difficult disease.
References
1. Naylor M, Brissett A. Current concepts in the etiology
and treatment of keloids. Facial Plast Surg 2012;28:
50412.
2. Sidle D, Kim H. Keloids: prevention and management.
Facial
Plast Surg Clin North Am 2011;19:50515.
3. Kal H, Veen R. Biologically effective doses of
postoperative
radiotherapy in the prevention of keloids. Strahlenther
Onkol
2005;181:71723.
4. Shridharani SM, Magarakis M, Manson PN, Singh NK, et al.
The emerging role of antineoplastic agents in the treatment
of
keloids and hypertrophic scars. Ann Plast Surg
2010;64:35561.
5. Gupta M, Narang T. Role of mitomycin C in reducing keloid
recurrence: patient series and literature review. J Laryngol
Otol
2011;125:297300.
MATTHEW WILLETT, MD, MC USN
KENT HANDFIELD, MD, MC USN
JASON MARQUART, MD, MC USA
Walter Reed National Military Medical Center
Bethesda, Maryland
The views expressed in this manuscript are those of the
authors and do not reflect the official policy of the
Depart-
ment of Army/Navy/Air Force, Department of Defense, or
U.S. government.
Transient Median and Ulnar Neuropathy Associated with a
Microwave Device for Treating Axillary
Hyperhidrosis
Microwave-based devices are recently developed
technology to treat hyperhidrosis by selectively
heating the interface between dermis and subcu-
taneous fat. A few studies using a microwave-
based device for hyperhidrosis13 have
demonstrated significant sweat reduction without
serious complications. We report a case of tran-
sient median and ulnar neuropathy associated
with treatment of hyperhidrosis with the micro-
wave-based device.
LETTERS AND COMMUNICATIONS
DERMATOLOGIC SURGERY482
-
Case Report
A healthy 32-year-old man received treatment with
a microwave-based device with integrated vacuum
and cooling (miraDry System, Miramar Labs, Sun-
nyvale, CA) for axillary hyperhidrosis. Local injec-
tion of tumescent fluid (mixture of normal saline
100 mL, 0.2 mL epinephrine, 2% lidocaine
10 mL, and sodium bicarbonate 1 mL) was used
for pain management. Approximately 100 mL of
fluid was injected using a 10 mL syringe and 26-G
long needle for treatment of bilateral axillae. The
device has five energy settings. The power is con-
stant across all energy settings, and time is used to
adjust energy levels. Our patient was treated with
the lowest energy level (level 1, 2.4 seconds) in
each axilla. After treatment, he noticed numbness
and weakness in the left first and second fingers.
He could abduct his arm up to, but not above,
90. He recovered strength in left shoulder abduc-
tion 10 days after treatment, although distal numb-
ness and weakness of his first and second fingers
continued. His finger function did not return until
6 months after the microwave-based device treat-
ment. The rehabilitation department was consulted
for further treatment.
On physical examination, motor strength for
shoulder abduction, elbow flexion and extension,
and wrist dorsiflexion was normal, but wrist volar
flexion strength was grade 4 of 5 on the Medical
Research Council scale, flexion of first and second
fingers was 2 of 5, flexion of other fingers was 4 of
5, and finger abduction was 4 of 5. OK sign was
positive, but Froments sign was negative. Hypoes-
thesia of the median neurotome was evident, and
mild atrophy of the thenar muscles was observed.
Nerve conduction study and electromyography per-
formed to determine the injured area revealed med-
ian neuropathy with moderate partial axonotmesis
and ulnar neuropathy with mild partial
axonotmesis in his left arm. After nerve injuries
were confirmed, he underwent physiotherapy twice
daily, including neuromuscular electrical
stimulation for the flexor muscles in the forearm
and the thenar muscles and strengthening exercise
of the finger flexors.
After 6 months of rehabilitation, his motor power
and sensory deficit improved remarkably, but the
thenar muscles remained atrophic (Figure 1). Sec-
ond finger flexor strength recovered to 4 of 5, and
the other fingers recovered nearly to full strength.
On sensory examination, he demonstrated mild
paresthesia with minimal hypoesthesia of the
median neurotome.
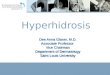
Follow-up electromyography revealed signs of
re-innervation and improved motor unit
recruitment in the median and ulnar nerves. Dener-
vation potentials disappeared, and the interference
pattern increased in the proximal median inner-
vated muscles, including the flexor carpi radialis,
signifying ongoing re-innervation in a proximal-to-
distal direction (Figure 2).
Patients are increasingly seeking treatment that
requires shorter recovery time and less
Figure 1. Thenar muscle of the patients left thumbshowed atrophy
after 12 months of treatment with amicrowave-based device for
axillary hyperhidrosis.
LETTERS AND COMMUNICATIONS
40 : 4 :APRIL 2014 483
-
treatment-related discomfort. Because hyperhidro-
sis is not life-threatening, these patients desire
simple treatments with no scars or complications.
Surgical removal of the sweat glands requires
postoperative immobilization and often results in
a scar. Botulinum toxin injection for hyperhidro-
sis has high cost and only 6-month duration of
effect.
Based on our experience, a microwave-based
device for axillary hyperhidrosis is safer than
surgical treatment.3 Only mild procedure-related
adverse events are known, such as vacuum acquisi-
tion marks, edema, and tenderness or altered
sensation in the treatment area; soreness; and dis-
comfort that do not last more than 2 weeks.13
Hong and colleagues2 reported a case of neuropa-
thy after microwave-based device treatment for
axillary hyperhidrosis. They commented that one
subject experienced transient neuropathy of the left
arm with associated muscle weakness that
improved after 6 months. They did not
describe the details of the subject who
experienced neuropathy.
The patient who experienced neuropathy in our
case was a thin, 1.8-m tall man weighing 60 kg,
for low body mass index of 18.5 kg/m2. It can be
assumed that microwave energy penetrated deep
enough to damage some nerve fibers of the bra-
chial plexus. From this case, we suggest that thin
patients with less fat have a higher risk of nerve
damage than normal-weight or obese patients.
Also, we think men are more vulnerable to nerve
injury than women because women have more fat
in the axillary area due to breast tissue. The
median and ulnar nerves are more susceptible to
injury because of their superficial anatomic loca-
tion relative to the radial nerve after branching off
the brachial plexus at the axillary level.
If the patient is a thin man, we recommend using
a lower energy level to avoid nerve injury. It is
also recommended that physicians monitor patient
.11977
1.198
1..199
110000ms 22mVV1.200
1.211
11.2222
1.222223
10000mms 1000VV11.244
1.199966
11.119977
1.1198
1.111999
10000mmss 200VV1111..2000
1.1196
11.19977
11.11988
1..1999
100ms 500V11.220000
(A) (B)(((
(C))C(C)CCC (D)((D)
Figure 2. Motor unit recruitment during effortful volition by
needle electromyography. (A) Flexor carpi radialis at6 months. (B)
Abductor pollicis brevis at 6 months. (C) Flexor carpi radialis, at
12 months. (D) Abductor pollicis brevis at12 months after treatment
with microwave-based device.
LETTERS AND COMMUNICATIONS
DERMATOLOGIC SURGERY484
-
hand and finger sensation during the procedure.
Although the target zone of action of a micro-
wave-based device is known to be independent of
skin thickness, as shown in a porcine model,4 the
thickness of the skin and subcutaneous fat seems
to influence the treatment depth of this device. In
patients with little subcutaneous fat, microwaves
penetrate deep enough to influence some nerves
that branch from the brachial plexus in the
axilla.
This case demonstrates that patients may develop
nerve injury even when using the lowest energy
level. Even in this case with nerve injury, the
long-term benefits of improved hyperhidrosis may
outweigh such adverse effects as weakness of the
left hand that recovered after 12 months. Also, the
patient improved, neurologically and functionally,
with intensive physiotherapy after 6 months of
persistent weakness and numbness. Based on this
observation, we recommend prompt and intensive
rehabilitation to accelerate recovery if neural
damage occurs unexpectedly. Moreover, more
caution is needed when treating thin male
patients.
References
1. Glaser DA, Coleman WP 3rd, Fan LK, Kaminer MS, et al. A
randonmized, blinded clinical evaluation of a novel
microwave
device for treating axillary hyperhidrosis: the dermatologic
reduction in underarm perspiration study. Dermatol Surg
2012;38:18591.
2. Hong HC, Lupin M, OShaughnessy KF. Clinical evaluation of
a
microwave device for treating axillary hyperhidrosis.
Dermatol
Surg 2012;38:72835.
3. Lee SJ, Chan KY, Suh DH, Song KY, et al. The efficacy of
a
microwave device for treating axillary hyperhidrosis and
osmidrosis in Asians: a preliminary study. J Cosmet Laser
Ther
2013;15:2559.
4. Johnson JE, OShaughnessy KF, Kim S. Microwave thermolysis
of sweat glands. Lasers Surg Med 2012;44:205.
DONG-HYE SUH, MD
SANG-JUN LEE, MD
Department of Dermatology
Arumdaun Nara Dermatologic Clinic
Seoul, Korea
KEEWON KIM, MD
Department of Rehabilitation Medicine
Seoul National University
Seoul, Korea
HWA JUNG RYU, MD, PHD
Department of Dermatology
Korea University College of Medicine
Seoul, Korea
The authors have indicated no significant interest with com-
mercial supporters.
Sudden Visual Loss and Multiple Cerebral Infarction After
Autologous Fat Injection into the Glabella
Soft tissue augmentation is a cosmetic procedure
that dermatologists commonly performed, but side
effects, including skin infections, necrosis, and
rarely, vascular occlusion, have been reported.
Retinal artery obstruction after autologous fat
injection is a devastating disease involving sudden
visual loss and, very rarely, cerebral infarction. We
report a case of retinal artery occlusion with multi-
ple cerebral infarctions caused by an autologous
fat injection into the glabellar area.
Case Report
A 31-year-old woman presented to our hospital
with sudden visual loss and arm weakness.
Twenty-four hours before the onset of these symp-
toms, she had received an autologous fat injection
in her glabella area to correct a cosmetic problem
performed under general anesthesia by a local
general practitioner. After she recovered from the
general anesthesia, the patient reported vision loss
LETTERS AND COMMUNICATIONS
40 : 4 :APRIL 2014 485