Embed Size (px)
Citation preview

You are going to do WHAT
with that heart
Michelle A Grenier MD FACC FAAP
Pediatric and Sports Cardiology
Disclosure
Relevant Financial Relationship (s) None Off Label Usage None
Objectives bull Define the importance of the role of the Sportrsquos
Cardiologist bull Recognize the more common causes of sudden
cardiac death in athletes bull Identify and apply cardiac adaptations in Adults with
Congenital Heart Disease (ACHD)
Why Do We Need Sports Cardiologists
Ever-increasing number of US Athletes
bull Athletic participation has more than doubled in all demographic areas in the last decade Lawless at el JACC 2014
bull 44 million youth (lt 18 yrs of age) bull 77 million high school bull 463 202 NCAA bull Master athletes (gt 35 yrs of age) drawn to endurance sports bull 353000 Marathoners in 2000 has increased to 500000 in 2011 bull 21341 Triathletes in 2000 has increased to 146000 in 2011
Trends in United States race finishers 1990ndash2012
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Exercise as the Master Tonic
bull The Benefits of Exercise are Myriad
bull Exercise controls weight bull Exercise combats health conditions and
diseases bull Exercise improves mood bull Exercise boosts energy bull Exercise promotes better sleep bull Exercise puts the spark back into your
sex life bull Exercise can improve self-esteem
bull Exercise Prescriptions for the masses
There are More Adult CHD Survivors than Ever Before
A study of estimated prevalence of CHD in the US the year 2010- this is a mathematical construct
The Magnitude of the Affected Population(CHD) in 2010
bull Advancement of interventions has afforded improved survivorship bull asymp24 million people with CHDs in the US in 2010
bull 14 million adults bull 1 million children
bull Nearly 300 000 (12) of these individuals had severe CHDs
These CelebritiesAthletes havehad CHD
Match the Celebrity with the Defect
bull 1 Arnold Scwarzenegger bull 2 John Ritter bull 3 Flow Hyman bull 4 Reggie Lewis bull 5 Marfan Syndrome bull 6 Mark Fight Shark Miller bull 7 Robin Williams bull 8 Shaun White
bull 1 Hypertrophic Cardiomyopathy bull 2 Tetralogy of Fallot bull 3 Aortic Dissection bull 4 Marfan Syndrome bull 5 Aortic Stenosis bull 6 Atrial Septal Defect bull 7 Arrhythmogenic Right
Ventricular Cardiomyopathy bull 8 AAOCA
What is the role of the heart in exercise
bull Exercise must be accommodated by LARGE SHIFTS of blood to the pulmonary and muscle beds
bull This is accomplished by elevating cardiac output CO= SV X HR
bull Increased VO2 and VCO2 exchange ndash oxygen consumption bull Power worktime bull The heart adapts in many ways
Athletes are Unique Cardiovascular Patients
bull Cardiovascular demands of exercise bull Training related cardiovascular adaptations bull Interaction of the heart with internal and external
adaptations bull Athletes are different from the general population
from the physiologic and medical perspective
All Sports are not Created Equal
bull Dynamic (soccer long distance running racquet sports)
bull Static (weight-lifting
karate water skiing gymnastics field events)
bull Combination (football
sprint running watermelon seed spitting)
Courtesy Aaron Baggish MD
Normal Physiologic Changes in the Heart Courtesy Aaron Baggish MD
Courtesy Aaron Baggish MD
Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Disclosure
Relevant Financial Relationship (s) None Off Label Usage None
Objectives bull Define the importance of the role of the Sportrsquos
Cardiologist bull Recognize the more common causes of sudden
cardiac death in athletes bull Identify and apply cardiac adaptations in Adults with
Congenital Heart Disease (ACHD)
Why Do We Need Sports Cardiologists
Ever-increasing number of US Athletes
bull Athletic participation has more than doubled in all demographic areas in the last decade Lawless at el JACC 2014
bull 44 million youth (lt 18 yrs of age) bull 77 million high school bull 463 202 NCAA bull Master athletes (gt 35 yrs of age) drawn to endurance sports bull 353000 Marathoners in 2000 has increased to 500000 in 2011 bull 21341 Triathletes in 2000 has increased to 146000 in 2011
Trends in United States race finishers 1990ndash2012
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Exercise as the Master Tonic
bull The Benefits of Exercise are Myriad
bull Exercise controls weight bull Exercise combats health conditions and
diseases bull Exercise improves mood bull Exercise boosts energy bull Exercise promotes better sleep bull Exercise puts the spark back into your
sex life bull Exercise can improve self-esteem
bull Exercise Prescriptions for the masses
There are More Adult CHD Survivors than Ever Before
A study of estimated prevalence of CHD in the US the year 2010- this is a mathematical construct
The Magnitude of the Affected Population(CHD) in 2010
bull Advancement of interventions has afforded improved survivorship bull asymp24 million people with CHDs in the US in 2010
bull 14 million adults bull 1 million children
bull Nearly 300 000 (12) of these individuals had severe CHDs
These CelebritiesAthletes havehad CHD
Match the Celebrity with the Defect
bull 1 Arnold Scwarzenegger bull 2 John Ritter bull 3 Flow Hyman bull 4 Reggie Lewis bull 5 Marfan Syndrome bull 6 Mark Fight Shark Miller bull 7 Robin Williams bull 8 Shaun White
bull 1 Hypertrophic Cardiomyopathy bull 2 Tetralogy of Fallot bull 3 Aortic Dissection bull 4 Marfan Syndrome bull 5 Aortic Stenosis bull 6 Atrial Septal Defect bull 7 Arrhythmogenic Right
Ventricular Cardiomyopathy bull 8 AAOCA
What is the role of the heart in exercise
bull Exercise must be accommodated by LARGE SHIFTS of blood to the pulmonary and muscle beds
bull This is accomplished by elevating cardiac output CO= SV X HR
bull Increased VO2 and VCO2 exchange ndash oxygen consumption bull Power worktime bull The heart adapts in many ways
Athletes are Unique Cardiovascular Patients
bull Cardiovascular demands of exercise bull Training related cardiovascular adaptations bull Interaction of the heart with internal and external
adaptations bull Athletes are different from the general population
from the physiologic and medical perspective
All Sports are not Created Equal
bull Dynamic (soccer long distance running racquet sports)
bull Static (weight-lifting
karate water skiing gymnastics field events)
bull Combination (football
sprint running watermelon seed spitting)
Courtesy Aaron Baggish MD
Normal Physiologic Changes in the Heart Courtesy Aaron Baggish MD
Courtesy Aaron Baggish MD
Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs
Objectives bull Define the importance of the role of the Sportrsquos
Cardiologist bull Recognize the more common causes of sudden
cardiac death in athletes bull Identify and apply cardiac adaptations in Adults with
Congenital Heart Disease (ACHD)
Why Do We Need Sports Cardiologists
Ever-increasing number of US Athletes
bull Athletic participation has more than doubled in all demographic areas in the last decade Lawless at el JACC 2014
bull 44 million youth (lt 18 yrs of age) bull 77 million high school bull 463 202 NCAA bull Master athletes (gt 35 yrs of age) drawn to endurance sports bull 353000 Marathoners in 2000 has increased to 500000 in 2011 bull 21341 Triathletes in 2000 has increased to 146000 in 2011
Trends in United States race finishers 1990ndash2012
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Exercise as the Master Tonic
bull The Benefits of Exercise are Myriad
bull Exercise controls weight bull Exercise combats health conditions and
diseases bull Exercise improves mood bull Exercise boosts energy bull Exercise promotes better sleep bull Exercise puts the spark back into your
sex life bull Exercise can improve self-esteem
bull Exercise Prescriptions for the masses
There are More Adult CHD Survivors than Ever Before
A study of estimated prevalence of CHD in the US the year 2010- this is a mathematical construct
The Magnitude of the Affected Population(CHD) in 2010
bull Advancement of interventions has afforded improved survivorship bull asymp24 million people with CHDs in the US in 2010
bull 14 million adults bull 1 million children
bull Nearly 300 000 (12) of these individuals had severe CHDs
These CelebritiesAthletes havehad CHD
Match the Celebrity with the Defect
bull 1 Arnold Scwarzenegger bull 2 John Ritter bull 3 Flow Hyman bull 4 Reggie Lewis bull 5 Marfan Syndrome bull 6 Mark Fight Shark Miller bull 7 Robin Williams bull 8 Shaun White
bull 1 Hypertrophic Cardiomyopathy bull 2 Tetralogy of Fallot bull 3 Aortic Dissection bull 4 Marfan Syndrome bull 5 Aortic Stenosis bull 6 Atrial Septal Defect bull 7 Arrhythmogenic Right
Ventricular Cardiomyopathy bull 8 AAOCA
What is the role of the heart in exercise
bull Exercise must be accommodated by LARGE SHIFTS of blood to the pulmonary and muscle beds
bull This is accomplished by elevating cardiac output CO= SV X HR
bull Increased VO2 and VCO2 exchange ndash oxygen consumption bull Power worktime bull The heart adapts in many ways
Athletes are Unique Cardiovascular Patients
bull Cardiovascular demands of exercise bull Training related cardiovascular adaptations bull Interaction of the heart with internal and external
adaptations bull Athletes are different from the general population
from the physiologic and medical perspective
All Sports are not Created Equal
bull Dynamic (soccer long distance running racquet sports)
bull Static (weight-lifting
karate water skiing gymnastics field events)
bull Combination (football
sprint running watermelon seed spitting)
Courtesy Aaron Baggish MD
Normal Physiologic Changes in the Heart Courtesy Aaron Baggish MD
Courtesy Aaron Baggish MD
Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Why Do We Need Sports Cardiologists
Ever-increasing number of US Athletes
bull Athletic participation has more than doubled in all demographic areas in the last decade Lawless at el JACC 2014
bull 44 million youth (lt 18 yrs of age) bull 77 million high school bull 463 202 NCAA bull Master athletes (gt 35 yrs of age) drawn to endurance sports bull 353000 Marathoners in 2000 has increased to 500000 in 2011 bull 21341 Triathletes in 2000 has increased to 146000 in 2011
Trends in United States race finishers 1990ndash2012
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Exercise as the Master Tonic
bull The Benefits of Exercise are Myriad
bull Exercise controls weight bull Exercise combats health conditions and
diseases bull Exercise improves mood bull Exercise boosts energy bull Exercise promotes better sleep bull Exercise puts the spark back into your
sex life bull Exercise can improve self-esteem
bull Exercise Prescriptions for the masses
There are More Adult CHD Survivors than Ever Before
A study of estimated prevalence of CHD in the US the year 2010- this is a mathematical construct
The Magnitude of the Affected Population(CHD) in 2010
bull Advancement of interventions has afforded improved survivorship bull asymp24 million people with CHDs in the US in 2010
bull 14 million adults bull 1 million children
bull Nearly 300 000 (12) of these individuals had severe CHDs
These CelebritiesAthletes havehad CHD
Match the Celebrity with the Defect
bull 1 Arnold Scwarzenegger bull 2 John Ritter bull 3 Flow Hyman bull 4 Reggie Lewis bull 5 Marfan Syndrome bull 6 Mark Fight Shark Miller bull 7 Robin Williams bull 8 Shaun White
bull 1 Hypertrophic Cardiomyopathy bull 2 Tetralogy of Fallot bull 3 Aortic Dissection bull 4 Marfan Syndrome bull 5 Aortic Stenosis bull 6 Atrial Septal Defect bull 7 Arrhythmogenic Right
Ventricular Cardiomyopathy bull 8 AAOCA
What is the role of the heart in exercise
bull Exercise must be accommodated by LARGE SHIFTS of blood to the pulmonary and muscle beds
bull This is accomplished by elevating cardiac output CO= SV X HR
bull Increased VO2 and VCO2 exchange ndash oxygen consumption bull Power worktime bull The heart adapts in many ways
Athletes are Unique Cardiovascular Patients
bull Cardiovascular demands of exercise bull Training related cardiovascular adaptations bull Interaction of the heart with internal and external
adaptations bull Athletes are different from the general population
from the physiologic and medical perspective
All Sports are not Created Equal
bull Dynamic (soccer long distance running racquet sports)
bull Static (weight-lifting
karate water skiing gymnastics field events)
bull Combination (football
sprint running watermelon seed spitting)
Courtesy Aaron Baggish MD
Normal Physiologic Changes in the Heart Courtesy Aaron Baggish MD
Courtesy Aaron Baggish MD
Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Ever-increasing number of US Athletes
bull Athletic participation has more than doubled in all demographic areas in the last decade Lawless at el JACC 2014
bull 44 million youth (lt 18 yrs of age) bull 77 million high school bull 463 202 NCAA bull Master athletes (gt 35 yrs of age) drawn to endurance sports bull 353000 Marathoners in 2000 has increased to 500000 in 2011 bull 21341 Triathletes in 2000 has increased to 146000 in 2011
Trends in United States race finishers 1990ndash2012
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Exercise as the Master Tonic
bull The Benefits of Exercise are Myriad
bull Exercise controls weight bull Exercise combats health conditions and
diseases bull Exercise improves mood bull Exercise boosts energy bull Exercise promotes better sleep bull Exercise puts the spark back into your
sex life bull Exercise can improve self-esteem
bull Exercise Prescriptions for the masses
There are More Adult CHD Survivors than Ever Before
A study of estimated prevalence of CHD in the US the year 2010- this is a mathematical construct
The Magnitude of the Affected Population(CHD) in 2010
bull Advancement of interventions has afforded improved survivorship bull asymp24 million people with CHDs in the US in 2010
bull 14 million adults bull 1 million children
bull Nearly 300 000 (12) of these individuals had severe CHDs
These CelebritiesAthletes havehad CHD
Match the Celebrity with the Defect
bull 1 Arnold Scwarzenegger bull 2 John Ritter bull 3 Flow Hyman bull 4 Reggie Lewis bull 5 Marfan Syndrome bull 6 Mark Fight Shark Miller bull 7 Robin Williams bull 8 Shaun White
bull 1 Hypertrophic Cardiomyopathy bull 2 Tetralogy of Fallot bull 3 Aortic Dissection bull 4 Marfan Syndrome bull 5 Aortic Stenosis bull 6 Atrial Septal Defect bull 7 Arrhythmogenic Right
Ventricular Cardiomyopathy bull 8 AAOCA
What is the role of the heart in exercise
bull Exercise must be accommodated by LARGE SHIFTS of blood to the pulmonary and muscle beds
bull This is accomplished by elevating cardiac output CO= SV X HR
bull Increased VO2 and VCO2 exchange ndash oxygen consumption bull Power worktime bull The heart adapts in many ways
Athletes are Unique Cardiovascular Patients
bull Cardiovascular demands of exercise bull Training related cardiovascular adaptations bull Interaction of the heart with internal and external
adaptations bull Athletes are different from the general population
from the physiologic and medical perspective
All Sports are not Created Equal
bull Dynamic (soccer long distance running racquet sports)
bull Static (weight-lifting
karate water skiing gymnastics field events)
bull Combination (football
sprint running watermelon seed spitting)
Courtesy Aaron Baggish MD
Normal Physiologic Changes in the Heart Courtesy Aaron Baggish MD
Courtesy Aaron Baggish MD
Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Exercise as the Master Tonic
bull The Benefits of Exercise are Myriad
bull Exercise controls weight bull Exercise combats health conditions and
diseases bull Exercise improves mood bull Exercise boosts energy bull Exercise promotes better sleep bull Exercise puts the spark back into your
sex life bull Exercise can improve self-esteem
bull Exercise Prescriptions for the masses
There are More Adult CHD Survivors than Ever Before
A study of estimated prevalence of CHD in the US the year 2010- this is a mathematical construct
The Magnitude of the Affected Population(CHD) in 2010
bull Advancement of interventions has afforded improved survivorship bull asymp24 million people with CHDs in the US in 2010
bull 14 million adults bull 1 million children
bull Nearly 300 000 (12) of these individuals had severe CHDs
These CelebritiesAthletes havehad CHD
Match the Celebrity with the Defect
bull 1 Arnold Scwarzenegger bull 2 John Ritter bull 3 Flow Hyman bull 4 Reggie Lewis bull 5 Marfan Syndrome bull 6 Mark Fight Shark Miller bull 7 Robin Williams bull 8 Shaun White
bull 1 Hypertrophic Cardiomyopathy bull 2 Tetralogy of Fallot bull 3 Aortic Dissection bull 4 Marfan Syndrome bull 5 Aortic Stenosis bull 6 Atrial Septal Defect bull 7 Arrhythmogenic Right
Ventricular Cardiomyopathy bull 8 AAOCA
What is the role of the heart in exercise
bull Exercise must be accommodated by LARGE SHIFTS of blood to the pulmonary and muscle beds
bull This is accomplished by elevating cardiac output CO= SV X HR
bull Increased VO2 and VCO2 exchange ndash oxygen consumption bull Power worktime bull The heart adapts in many ways
Athletes are Unique Cardiovascular Patients
bull Cardiovascular demands of exercise bull Training related cardiovascular adaptations bull Interaction of the heart with internal and external
adaptations bull Athletes are different from the general population
from the physiologic and medical perspective
All Sports are not Created Equal
bull Dynamic (soccer long distance running racquet sports)
bull Static (weight-lifting
karate water skiing gymnastics field events)
bull Combination (football
sprint running watermelon seed spitting)
Courtesy Aaron Baggish MD
Normal Physiologic Changes in the Heart Courtesy Aaron Baggish MD
Courtesy Aaron Baggish MD
Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

There are More Adult CHD Survivors than Ever Before
A study of estimated prevalence of CHD in the US the year 2010- this is a mathematical construct
The Magnitude of the Affected Population(CHD) in 2010
bull Advancement of interventions has afforded improved survivorship bull asymp24 million people with CHDs in the US in 2010
bull 14 million adults bull 1 million children
bull Nearly 300 000 (12) of these individuals had severe CHDs
These CelebritiesAthletes havehad CHD
Match the Celebrity with the Defect
bull 1 Arnold Scwarzenegger bull 2 John Ritter bull 3 Flow Hyman bull 4 Reggie Lewis bull 5 Marfan Syndrome bull 6 Mark Fight Shark Miller bull 7 Robin Williams bull 8 Shaun White
bull 1 Hypertrophic Cardiomyopathy bull 2 Tetralogy of Fallot bull 3 Aortic Dissection bull 4 Marfan Syndrome bull 5 Aortic Stenosis bull 6 Atrial Septal Defect bull 7 Arrhythmogenic Right
Ventricular Cardiomyopathy bull 8 AAOCA
What is the role of the heart in exercise
bull Exercise must be accommodated by LARGE SHIFTS of blood to the pulmonary and muscle beds
bull This is accomplished by elevating cardiac output CO= SV X HR
bull Increased VO2 and VCO2 exchange ndash oxygen consumption bull Power worktime bull The heart adapts in many ways
Athletes are Unique Cardiovascular Patients
bull Cardiovascular demands of exercise bull Training related cardiovascular adaptations bull Interaction of the heart with internal and external
adaptations bull Athletes are different from the general population
from the physiologic and medical perspective
All Sports are not Created Equal
bull Dynamic (soccer long distance running racquet sports)
bull Static (weight-lifting
karate water skiing gymnastics field events)
bull Combination (football
sprint running watermelon seed spitting)
Courtesy Aaron Baggish MD
Normal Physiologic Changes in the Heart Courtesy Aaron Baggish MD
Courtesy Aaron Baggish MD
Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

The Magnitude of the Affected Population(CHD) in 2010
bull Advancement of interventions has afforded improved survivorship bull asymp24 million people with CHDs in the US in 2010
bull 14 million adults bull 1 million children
bull Nearly 300 000 (12) of these individuals had severe CHDs
These CelebritiesAthletes havehad CHD
Match the Celebrity with the Defect
bull 1 Arnold Scwarzenegger bull 2 John Ritter bull 3 Flow Hyman bull 4 Reggie Lewis bull 5 Marfan Syndrome bull 6 Mark Fight Shark Miller bull 7 Robin Williams bull 8 Shaun White
bull 1 Hypertrophic Cardiomyopathy bull 2 Tetralogy of Fallot bull 3 Aortic Dissection bull 4 Marfan Syndrome bull 5 Aortic Stenosis bull 6 Atrial Septal Defect bull 7 Arrhythmogenic Right
Ventricular Cardiomyopathy bull 8 AAOCA
What is the role of the heart in exercise
bull Exercise must be accommodated by LARGE SHIFTS of blood to the pulmonary and muscle beds
bull This is accomplished by elevating cardiac output CO= SV X HR
bull Increased VO2 and VCO2 exchange ndash oxygen consumption bull Power worktime bull The heart adapts in many ways
Athletes are Unique Cardiovascular Patients
bull Cardiovascular demands of exercise bull Training related cardiovascular adaptations bull Interaction of the heart with internal and external
adaptations bull Athletes are different from the general population
from the physiologic and medical perspective
All Sports are not Created Equal
bull Dynamic (soccer long distance running racquet sports)
bull Static (weight-lifting
karate water skiing gymnastics field events)
bull Combination (football
sprint running watermelon seed spitting)
Courtesy Aaron Baggish MD
Normal Physiologic Changes in the Heart Courtesy Aaron Baggish MD
Courtesy Aaron Baggish MD
Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

These CelebritiesAthletes havehad CHD
Match the Celebrity with the Defect
bull 1 Arnold Scwarzenegger bull 2 John Ritter bull 3 Flow Hyman bull 4 Reggie Lewis bull 5 Marfan Syndrome bull 6 Mark Fight Shark Miller bull 7 Robin Williams bull 8 Shaun White
bull 1 Hypertrophic Cardiomyopathy bull 2 Tetralogy of Fallot bull 3 Aortic Dissection bull 4 Marfan Syndrome bull 5 Aortic Stenosis bull 6 Atrial Septal Defect bull 7 Arrhythmogenic Right
Ventricular Cardiomyopathy bull 8 AAOCA
What is the role of the heart in exercise
bull Exercise must be accommodated by LARGE SHIFTS of blood to the pulmonary and muscle beds
bull This is accomplished by elevating cardiac output CO= SV X HR
bull Increased VO2 and VCO2 exchange ndash oxygen consumption bull Power worktime bull The heart adapts in many ways
Athletes are Unique Cardiovascular Patients
bull Cardiovascular demands of exercise bull Training related cardiovascular adaptations bull Interaction of the heart with internal and external
adaptations bull Athletes are different from the general population
from the physiologic and medical perspective
All Sports are not Created Equal
bull Dynamic (soccer long distance running racquet sports)
bull Static (weight-lifting
karate water skiing gymnastics field events)
bull Combination (football
sprint running watermelon seed spitting)
Courtesy Aaron Baggish MD
Normal Physiologic Changes in the Heart Courtesy Aaron Baggish MD
Courtesy Aaron Baggish MD
Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Match the Celebrity with the Defect
bull 1 Arnold Scwarzenegger bull 2 John Ritter bull 3 Flow Hyman bull 4 Reggie Lewis bull 5 Marfan Syndrome bull 6 Mark Fight Shark Miller bull 7 Robin Williams bull 8 Shaun White
bull 1 Hypertrophic Cardiomyopathy bull 2 Tetralogy of Fallot bull 3 Aortic Dissection bull 4 Marfan Syndrome bull 5 Aortic Stenosis bull 6 Atrial Septal Defect bull 7 Arrhythmogenic Right
Ventricular Cardiomyopathy bull 8 AAOCA
What is the role of the heart in exercise
bull Exercise must be accommodated by LARGE SHIFTS of blood to the pulmonary and muscle beds
bull This is accomplished by elevating cardiac output CO= SV X HR
bull Increased VO2 and VCO2 exchange ndash oxygen consumption bull Power worktime bull The heart adapts in many ways
Athletes are Unique Cardiovascular Patients
bull Cardiovascular demands of exercise bull Training related cardiovascular adaptations bull Interaction of the heart with internal and external
adaptations bull Athletes are different from the general population
from the physiologic and medical perspective
All Sports are not Created Equal
bull Dynamic (soccer long distance running racquet sports)
bull Static (weight-lifting
karate water skiing gymnastics field events)
bull Combination (football
sprint running watermelon seed spitting)
Courtesy Aaron Baggish MD
Normal Physiologic Changes in the Heart Courtesy Aaron Baggish MD
Courtesy Aaron Baggish MD
Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

What is the role of the heart in exercise
bull Exercise must be accommodated by LARGE SHIFTS of blood to the pulmonary and muscle beds
bull This is accomplished by elevating cardiac output CO= SV X HR
bull Increased VO2 and VCO2 exchange ndash oxygen consumption bull Power worktime bull The heart adapts in many ways
Athletes are Unique Cardiovascular Patients
bull Cardiovascular demands of exercise bull Training related cardiovascular adaptations bull Interaction of the heart with internal and external
adaptations bull Athletes are different from the general population
from the physiologic and medical perspective
All Sports are not Created Equal
bull Dynamic (soccer long distance running racquet sports)
bull Static (weight-lifting
karate water skiing gymnastics field events)
bull Combination (football
sprint running watermelon seed spitting)
Courtesy Aaron Baggish MD
Normal Physiologic Changes in the Heart Courtesy Aaron Baggish MD
Courtesy Aaron Baggish MD
Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Athletes are Unique Cardiovascular Patients
bull Cardiovascular demands of exercise bull Training related cardiovascular adaptations bull Interaction of the heart with internal and external
adaptations bull Athletes are different from the general population
from the physiologic and medical perspective
All Sports are not Created Equal
bull Dynamic (soccer long distance running racquet sports)
bull Static (weight-lifting
karate water skiing gymnastics field events)
bull Combination (football
sprint running watermelon seed spitting)
Courtesy Aaron Baggish MD
Normal Physiologic Changes in the Heart Courtesy Aaron Baggish MD
Courtesy Aaron Baggish MD
Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

All Sports are not Created Equal
bull Dynamic (soccer long distance running racquet sports)
bull Static (weight-lifting
karate water skiing gymnastics field events)
bull Combination (football
sprint running watermelon seed spitting)
Courtesy Aaron Baggish MD
Normal Physiologic Changes in the Heart Courtesy Aaron Baggish MD
Courtesy Aaron Baggish MD
Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Courtesy Aaron Baggish MD
Normal Physiologic Changes in the Heart Courtesy Aaron Baggish MD
Courtesy Aaron Baggish MD
Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs
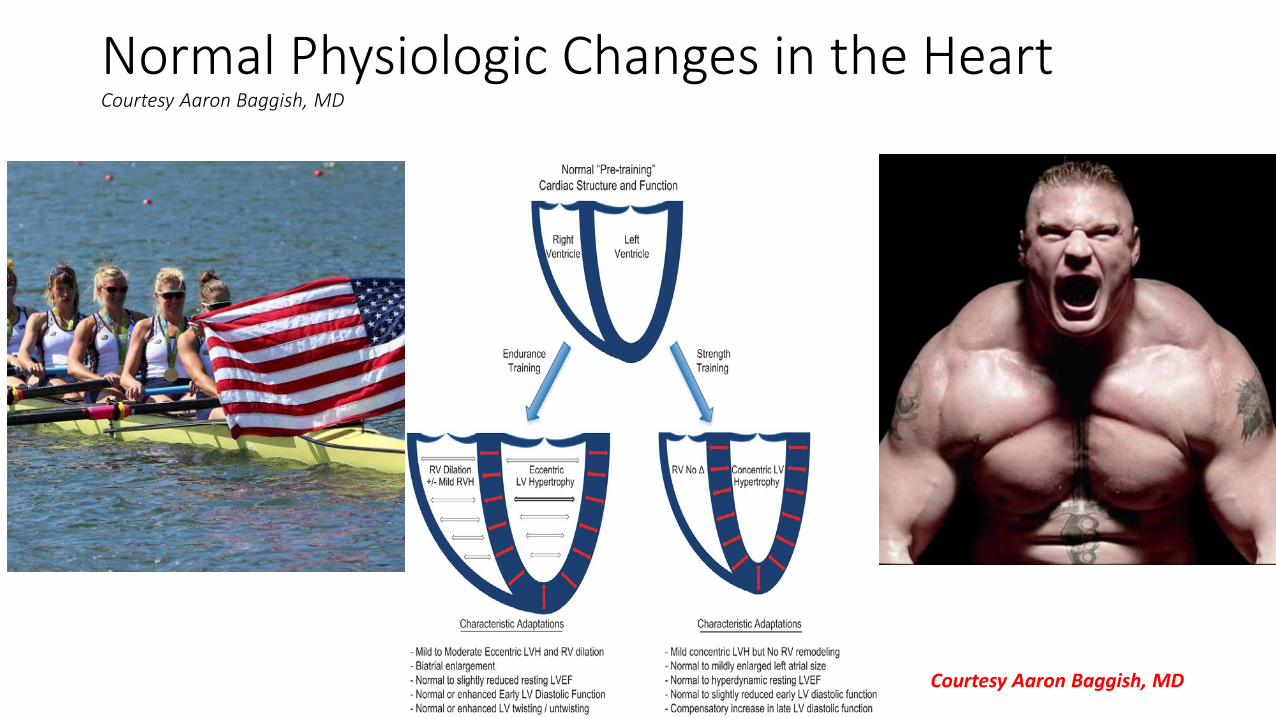
Normal Physiologic Changes in the Heart Courtesy Aaron Baggish MD
Courtesy Aaron Baggish MD
Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Changes in the Left Ventricle - the gray area
bull Extremely controversial area bull Is it HCM or not bull AfricanAmerican or Africo-Carribean males tend to show high
preponderance of bull LVH voltage J point elevations and T wave changes bull LVH+- LVNC by echo bull 5 X rate of SCASCD but consistent with non-athletes
bull Addition of EKG to screening has been a hot topic bull What is the best non-invasive method of distinguishing
A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

A better look
See International Interpretation of Electrocardiographic Data in Athletes JACC 2016
Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Caveat ndash When a C+ is not so bad bull JAMA 2003 Dec 3290(21)2803 bull Weight lifting and rupture of silent aortic aneurysms bull Elefteriades JA Hatzaras I Tranquilli MA Elefteriades AJ Stout R
Shaw RK Silverman D Barash P
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs
Training-Related EP Adaptations
bull Bradycardias bull Atrioventricular and
interventricular blocks bull Extrasystoles bull Interval prolongations bull Increased voltages bull Repolarization
abnormalities Vary according to gender ethnicity body size type of training and sport
Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Revised EKG Criteria- European and Seattle Criteria
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs
Why Do We Need Sports Cardiologists bulla They keep track of basic physiologic adaptations
of the heart bull b They give exercise prescriptions for people with
heart disease bull c They help prevent sudden cardiac arrestsudden
cardiac death bull d They are educated in the latest evaluative
techniques bull e They are the ldquovoice of reasonrdquo
The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

The Paradox Exercise can acutely bull Increase the risk of MI bull Aortic dissection bull Arrhythmias bull Sudden cardiac arrest (SCA) bull Sudden cardiac death (SCD) If there is underlying CVD risk of SCASCD increases 25 X Chronic changes caused by exercise may pose challenges to the cardiologist in evaluating athletes
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs
Prevention of Sudden Cardiac Death bull Sudden Cardiac Arrest in athletes
~ 1200000 bull Cardiac disease prevalence of 03 in
general athletic populations bull ~1333 These four athletes represent the major occult causes of SCASCD While rare it is impactful
Hank Gathers
Reggie Lewis
James Taylor
Reported data current US studies
Pistol Pete
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs
Most common cause of sudden death NCAA athletes
bulla Drug overdose bullb Sudden Cardiac Death bullc Homicide bulld Cancer bulle Motor Vehicle Accidents
Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Most common causes of sudden death in NCAA athletes
bull a
Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Most Common causes of SCASCD in the US those athletes lt35 years
a Tetralogy of Fallot b Aortic Stenosis c Hypertrophic Cardiomyopathy d Arrhythmogenic Right Ventricular
Cardiomyopathy e Anomalous Coronary Artery Origins
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs
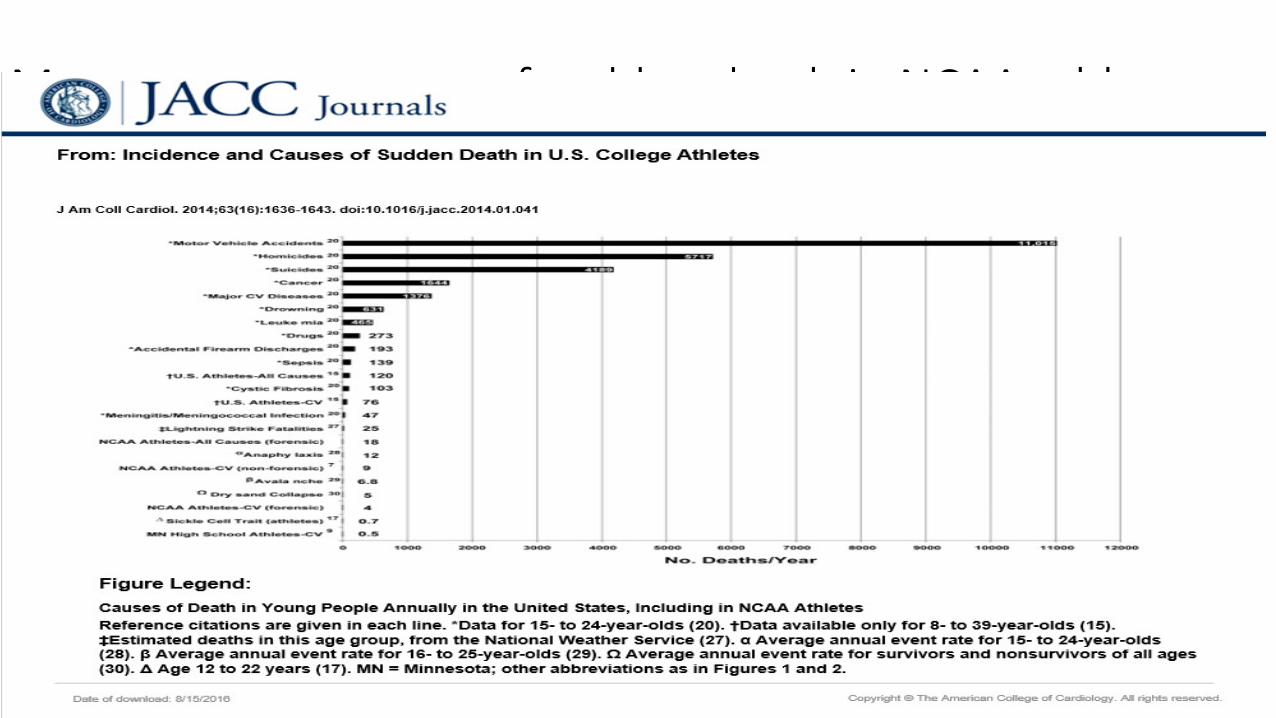
Hypertrophic cardiomyopathy ndash 1500 Long QT Syndrome ndash 17000 Marfanrsquos Syndrome ndash 15000
Cardiac Disease Incidence
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs
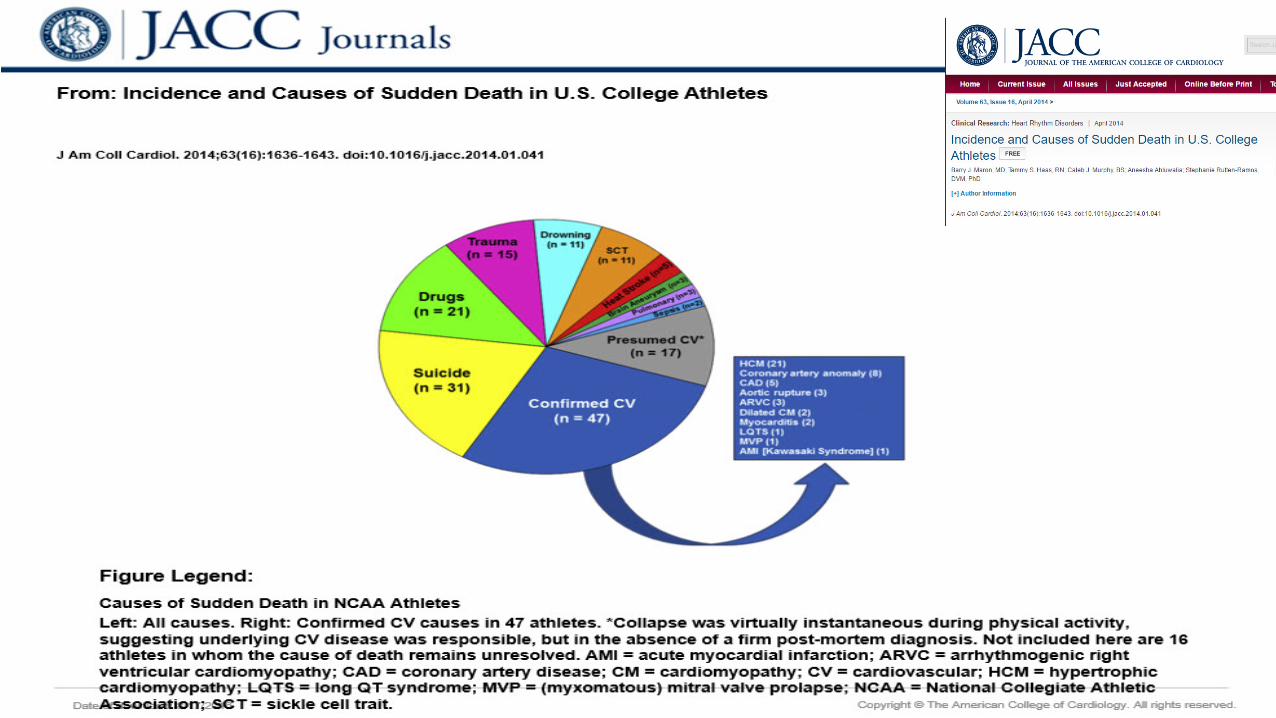
Coronary artery disease is the most common cause of SCD in athletes aged gt35 years Athletes lt 35 years attributed to inherited or congenital disorders of the heart that predispose to malignant ventricular arrhythmias
True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

True or False
bullYou can never have too much exercise
Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Too much of a good thing
Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Exercise-induced increases in high-sensitive cardiac troponin I (hsTnI) levels in participants in the 2011 Boston marathon (n = 71)
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Pathophysiology of myocardial fibrosis
Thijs M H Eijsvogels et al Physiol Rev 20169699-125
Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Atrial Fibrillation bull Extreme exercise ldquoseveral hours of vigorous exercise nearly every
dayrdquo bull Dr Andreacute La Gerche a sports cardiologist at the Baker IDI Heart and
Diabetes Institute in Melbourne Australia found patients admitted to University of Leuven Hospital in Belgium for atrial fibrillation with no risk factors
bull No hypertension heart disease obesity or diabetes bull Were four times more likely than the general population to have
engaged in endurance sports bull Proposed mechanism Fibrosis
Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Sanz-de la Garza M Grazioli G Bijnens BH et al Acute Exercise Dose-Dependent Impairment in Atrial Performance During an Endurance Race 2D Ultrasound Speckle-Tracking Strain Analysis JACC CARDIOVASCULAR IMAGING 2016 e-pub bull What is the acute atrial response to endurance exercise during a specified
time bull 55 healthy adults at 3 stages of running-SML bull Echo speckle tracking a-wave strainstrain rate (atrial contractile
function) and s-wave strainstrain rate (reservoir function) bull RA reservoir function decreased in M and further in L no changes in S bull RA contractile function decreased in L no changes in M increased in group
S bull CONCLUSION Acute exercise-dose dependent impairment in atrial
function was observed mostly in the RA which was related to RV systolic dysfunction The impact on atrial function of long-term endurance training might lead to atrial remodeling favoring arrhythmia development
Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Changes in the right ventricle
bull Does intense endurance exercise affect the RV more than the LV bull Does exposure to endurance competition influence cardiac remodeling
(including fibrosis) bull 40 well-trained athletes bull Acute dysfunction RV not LV
bull Tni BNP Echo CMR bull RV volumes increased all functional measures decreased bull LV volumes reduced and function was preserved
bull Short-term recovery appears complete but chronic structural changes and reduced RV function are evident in some of the most practiced athletes
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub
bull What is the impact of sex and different sports on right ventricular (RV) remodeling compared to the derived upper limits of widely used revised Task Force (TF) reference values
bull 1009 Olympic athletes (mean age 24 ` 6 years 64 males) in skill power mixed and endurance sport
bull Evaluated by 2-dimensional echocardiography and Dopplertissue Doppler imaging
bull Right ventricular outflow tract (RVOT) in parasternal long-axis (PLAX) and short-axis views fractional area change sʹ velocity and morphological features were assessed
DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

DrsquoAscenzi F Pisicchio C Caselli S et al RV Remodeling in Olympic Athletes JACC CARDIOVASCULAR IMAGING 2016 E pub bull Indexed RVOT PLAX was greater in females than in males
bull Both RVOT PLAX and parasternal short-axis view were significantly different among skill power mixed and endurance sports
bull Fractional area change and sʹ velocity did not differ among the groups bull RV enlargement compatible with major and minor TF diagnostic criteria for
arrhythmogenic RV cardiomyopathy was observed 32 bull A rounded apex was described in 823 (81) athletes prominent tra-
beculations in 378 (37) athletes and a prominenthyperreflective moderator band in 5 (05) athletes
bull MALE endurance athletes showed the greatest changes
Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Detrimental Effects of Endurance Exercise Include bull a Acute volume overload of the atria and right ventricle
with decreased RVEF bull b Release of biomarkers with return to normal in a week bull c Patchy myocardial fibrosis yielding a nidus for atrial
fibrillation bull d Large artery wall stiffness and increased coronary calcification bull e All of the above
Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Risk Factor for SCASCD- Aortic Stenosis Severe aortic stenosis (AS) can manifest as exertional angina even in the presence of unobstructed coronary arteries bull N = 22 patients with severe AS 38 controls- supine bike
bull Compared stress echo-myocardial work bull Intracoronary recordings bull Wave intensity analysis to quantify accelerationdeceleration coronary blood flow
Similarities Minimum microvascular resistance Differences Myocardial stress greater Hyperemic CBF was less Diastolic time fraction was greater AS Healthy Heart Exercise and hyperemia efficiency of perfusion improved-increase in the relative contribution of accelerating waves AS perfusion efficiency decreased due to augmentation of early systolic deceleration and an attenuated rise in systolic acceleration waves Conclusions AS angina is not related to microvascular disease but driven by abnormal cardiac-coronary coupling
Coronary Physiology During Exercise and Vasodilation in the Healthy
Heart and in Severe Aortic Stenosis Matthew Lumley et al J Am Coll Cardiol 201668(7)688-697
A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

A Cautionary Tale- A true story bull 16 yr 6 feet tall 130 basketball player ndash faints at least once per basketball game when he stops to shoot at free throw line bull Has never fainted in practice and keeps up with his team
members bull Has no other associated complaints no chest pain shortness of
breath or palpitations bull Feels absolutely nothing prior to his LOC and has nearly broken
his jaw bull Takes no medications or supplements drinks water alternating
with sports drinks at least a gallon a day and likes salty foods
Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Next Steps
a Ask for an echocardiogram to evaluate for Marfan syndrome
b Obtain EKG if normal advise him to continue to hydrate and allow him to play
c Test him for hypoglycemia d Obtain EKG and echo and if normal allow him to
play e Obtain a stress test and if normal allow him to play
as long as he maintains hydration
Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Anomalous Aortic Origin of Coronary Artery (AAOCA)
bull The story did not make sense bull Considered loop recorderEP
study bull But got MRIMRAhellip fibrosis of
subendocardium bull 01-07 prevalence SCD 17 bull AAOLCA- unroofing bull AAORCA- AHAACC guidelines
permit cmpetition
Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Keep these References 1 Van Hare GF Ackerman MJ Evangelista JA et al Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities Task Force 4 Congenital Heart Disease A Scientific Statement from the American Heart Association and American College of Cardiology Circulation 2015 132 e281-291 2 Poynter JA Williams WG McIntyre S Brothers JA Jacobs ML Congenital Heart Surgeons Society AWG Anomalous aortic origin of a coronary artery A report from the congenital heart surgeons society registry World J Pediatr Congenit Heart Surg 2014 522-30
Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Proportions of Adult Congenital Heart Defects Data from Nationwide Childrens Hospital
Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Application of Sports Cardiology
bull How do we evaluate these patients
bull How do we appropriately advise these patients
bull On a case-by-case basis
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs
Knowing Exercise ndashRelated Changes Prescribe Exercise for Shaun White
bull Factors involved bull Gender bull Ethnicity bull Age bull What does his heart look like bull What is the natural history of this defect without exercise bull Type and duration of exercise with exercise-related
changes bull What happens at altitude
1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

1 White Male 2 Dynamic and
Strength exercise 3 Dosing A lot 4 High Altitude 5 Endurance
athletes may have RV changes LV changes coronary artery changes atrial arrhythmia
6 Basic heart substrate
Repaired Tetralogy of Fallot
Exercise Factors
Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Tetralogy of Fallot bull Most common cyanotic CHD bull 30 year survival 90 bull Residual anatomic and hemodynamic abnormalities in ALL patients
bull Well tolerated initially bull Exercise intolerance bull Arrhythmias bull Heart Failure bull Sudden Death (late)
bull Routine surveillance is necessary
Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Consequences of TOF Repair bull Relief of RVOTO =gt PI=gtRV volume overload=gtTR=gt atrial arrhythmias bull Residual RVOTObranch stenosis=gt RV pressure overload bull Initial shunt =gt pulmonary hypertension =gt or branch artery stenosis bull Aortic root enlargement =gt AI bull RVOT patch plus RV volume overload =gt ventricular arrhythmias
1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

1 Anterior deviation of the Conal Septum causes
2 VSD 3 Over-riding aorta 4 Pulmonic stenosis 5 Right ventricular
hypertrophy 6 Other cardiac
associations a RAA 25 b Coronary
abnormalities 10 c ASD
7 Extracardiac associations- Di George
Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Articles for Reference
bull Warnes CA et al ACCAHA 2008 Guidelines for the Management of Adults with Congenital Heart Disease A Repor of the American Colleg of Cardiology American Heart Association Task Force on Practice Guidelines Circulation 2008118e714-e833
bull Bhatt AB et al Congenital Heart Disease in the Older Adult Circulation 201513100-00
bull Valente AM et al Multimodality Imaging Guidelines for Patients with Repaired Tetralogy of Fallot J Am Soc Echocardiogr 201427111-141
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs
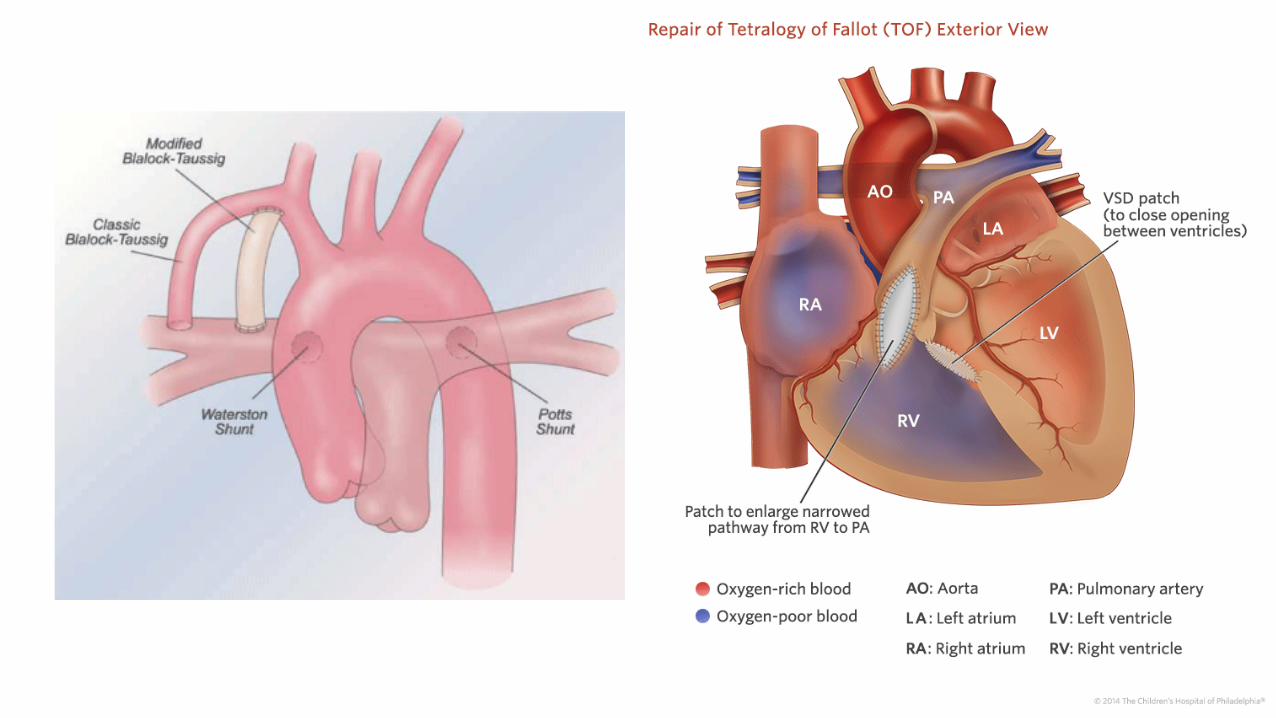
Summary Recommendations
bull Annual history and physical examination bull Annual ECG and evaluation of right ventricular size and function
bull Echo may not be enough bull MRI- RVEF and regurgitant fraction bull Angiography of the branch pulmonary arteries
bull Periodic ambulatory ECG monitor and exercise test bull Holters and events may be problematic in athletes bull Exercise stress tests may not be representative
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs
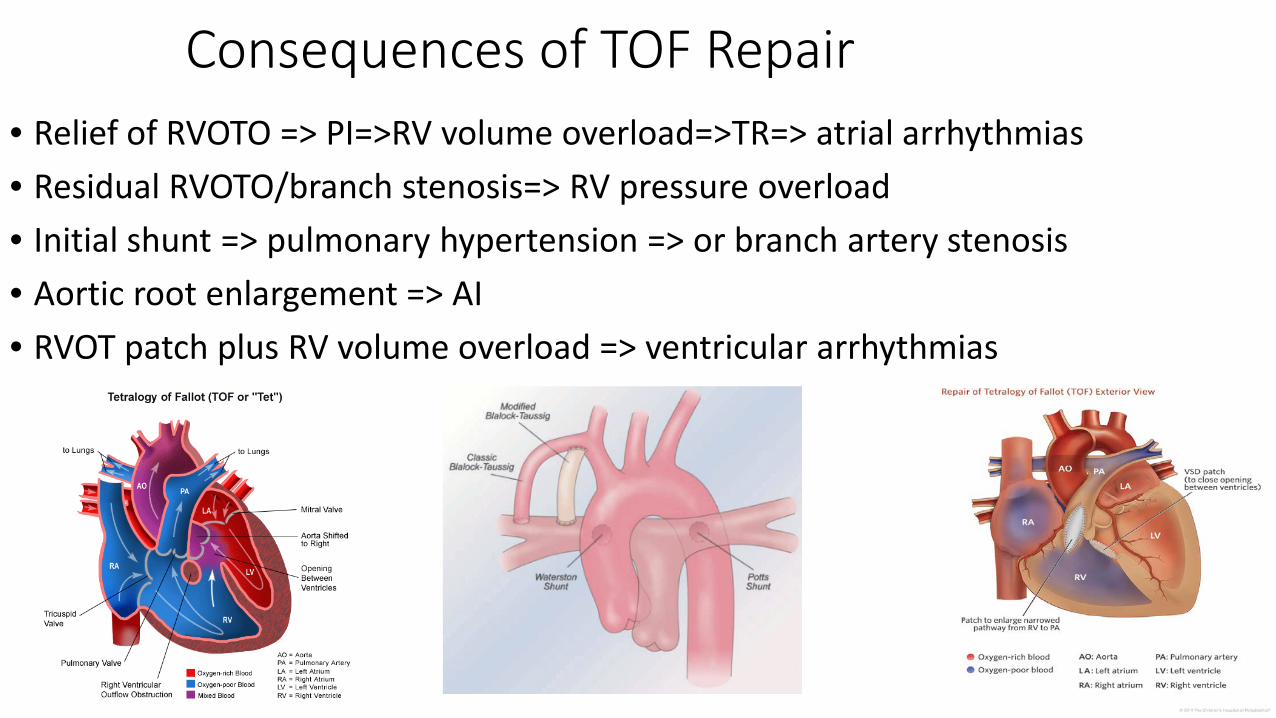
EKG- Follow QRS duration
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs
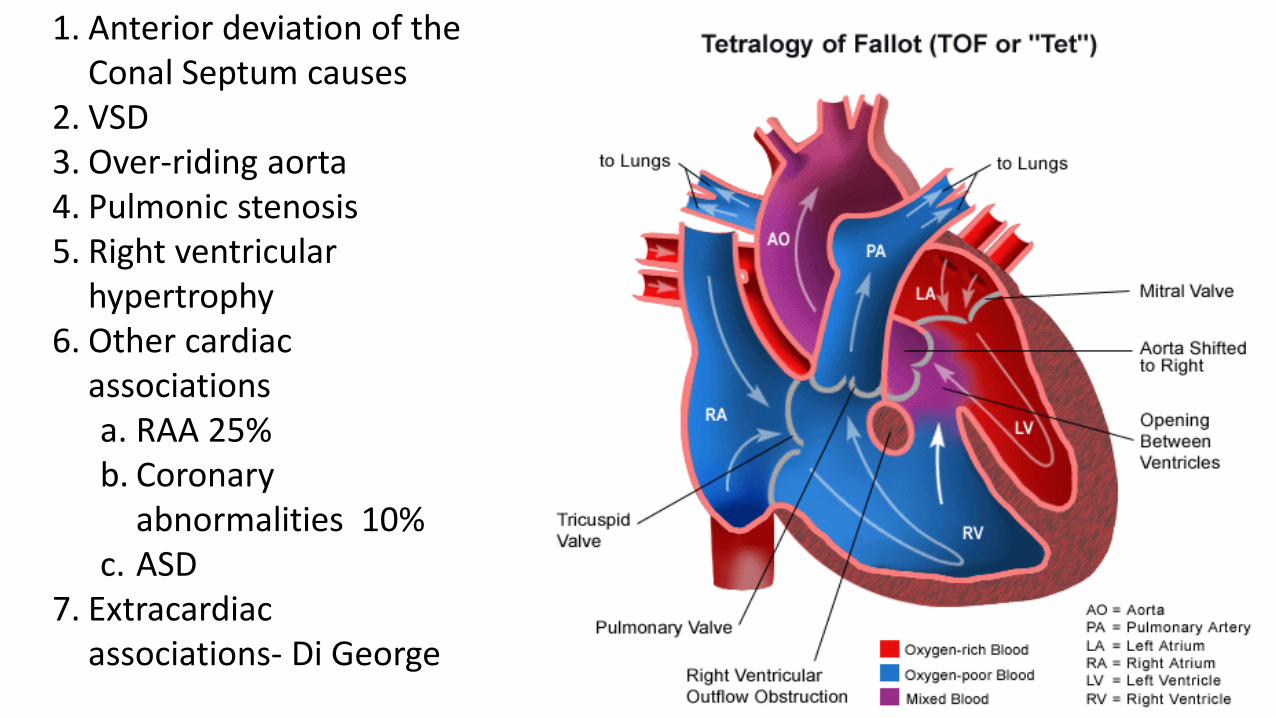
Typical Arrhythmias bull Atrial Flutter
bull IART- it doesnrsquot have to be fast to be bad bull Ventricular arrhythmias
bull SCD is the most common cause of late mortality bull Advanced RV dilation bull Presence of RVOT patch bull QRS duration gt180 ms with annual increase bull RV hypertrophy bull RV and LV dysfunction
bull Indications for EP study bull Unexplained syncope or high risk CHD (Class I) bull Need to rule out structuralhemodynamic abnormalities (Class I) bull Holter (Class I) or exercise test (Class IIa)
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs
IART bull Distinct from Flutter seen in normal hearts
bull Reentrant circuit may rotate around bull Surgical patches bull Atriotomy incisions bull Other atypical conduction obstacles
bull May have multiple different circuits bull Rate typically slower
bull Typically 130-220 BPM bull Frequently conduct 11 through AVN bull May result in hypotension or circulatory collapse
Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Things to Know About TOF
bull Severe pulmonary valve regurgitation is the most common residual abnormality
bull RV dilation and dysfunction bull May be due in part to branch PA stenosis bull Exercise intolerance is primary symptom bull Melody Valve is a great alternative bull MUST KNOW CORONARY STATUS
bull LV dysfunction occurs in up to 20 with prior repair of TOF bull Evaluate for risk factors for SCD bull Screen for DiGeorge
Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Ventricular Arrhythmias in repaired TOF bull SCD is the most common cause of late mortality (31 had no other risk factors) bull Macro re-entrant circuits involving scar in RVOT bull Factors associated with VTSCD
bull Moderate to severe PI bull Older age at repair bull QRS duration bull Use of transannular patch ventriculotomy bull Prior BTS bull LVEDP gt 12 mm Hg
Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Ventricular Tachycardia
Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Indications for ICD Therapy
bull1 Survivor of Cardiac Arrest bull2 Symptomatic sustained VT bull3 Recurrent syncope with ventricular dysfunction or inducible ventricular arrhythmias
bull4 No other specific guidelines in CHD
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs
Would you put an ICD in HIM
Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Exercise with Implantable Defibrillators- Athletes bull Athletes with ICDs (age 10-60 years) participating in organized (n=328) or high-risk (n=44) sports were
recruited bull Median age 33 years (89 lt20 yrs) 33 were female bull 60 competitive athletes (varsityjunior varsitytraveling team) bull Pre-ICD hx ventricular arrhythmia in 42 bull Running basketball and soccer bull 31-month fu bull No occurrences of -death or resuscitated arrest or arrhythmia- or shock-related injury-during sports bull There were 49 shocks in 37 participants (10 of study population) during competitionpractice bull 39 shocks in 29 participants (8) during other physical activity bull 33 shocks in 24 participants (6) at rest bull 8 ventricular arrhythmia episodes (device defined) multiple shocks were received bull Freedom from lead malfunction was 97 at 5 years (from implantation) and 90 at 10 years
ldquoMany athletes with ICDs can engage in vigorous and competitive sports without physical injury or failure to terminate the arrhythmia despite the occurrence of both inappropriate and appropriate shocks These data provide a basis for more informed physician and patient decision making in terms of sports participation for athletes with ICDsrdquo
Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Exercise with Implantable Defibrillators-Low CO bull Exercise typically avoided after implantable cardioverter defibrillator(ICD) for fear of
provocation of acute arrhythmias bull Prospective study effects of home aerobic exercise training and maintenance program
bull Aerobic performance bull ICD shocks bull Hospitalizations
bull 160 pts (124 men and 36 women) randomized to exercise (EX) vs usual care bull Primary outcome was peak oxygen consumption measured with cardiopulmonary exercise testing at
baseline and 8 and 24 weeks bull EX consisted of 8 weeks of home walking for 1 hd 5 dwk at 60 to 80 of heart rate reserve followed
by 16 weeks of maintenance home walking for 150 minwk bull EX significantly increased peak oxygen consumption (EX 267plusmn70 mLkg per minute) Prescribed home exercise is safe and significantly improves cardiovascular performance in ICD recipients without causing shocks or hospitalizations
Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs

Following Dr Baggishrsquos 7 Rules
bull 1 Address cardiovascular risk factors bull 2 Discuss health and performance bull 3 Plan for annual periodicity bull 4 Prioritize warm ups and cool downs bull 5 Practice careful event preparation bull 6 Respect a Virus bull 7 Listen to Warning Signs






























