Embed Size (px)
Citation preview

You are asked to review Mr X a 78year old gentleman in ICU who is in the process of being weaned off the ventilator
The nurse calls you because Mr X is trying to jump out of bedAssess and manage Mr X
Alex Yartsev 1542011
Delirium in the ICU
Ohrsquos Intensive Care manual 6th edition ch 42
Why is Mr X doing that- Inability to communicate something - Pain ndash he is lying on top of a forgotten 10ml syringe
- Dementia ndash this is what he is normally like at the nursing home- Psychosis ndash we accidentally stopped his risperidone and started an MAOI
- Intoxication ndash APS team started ketamine- Withdrawal ndash he drinks - Delirium Tremensndash he REALLY drinks
- ENCEPHALOPATHY An alteration in the level or content of consciousness due to a process extrinsic to the brain
metabolic vs structural
Ohrsquos Intensive Care manual 6th edition ch 42
A moment for Encephalopathy
-SEPSIS-ICU DELIRIUMhellipalsohellip-Hepatic failure-Renal Failure-Hypoxia or hypercapnea-Hyper or hyponatremia-Hyper or hypoglycaemia-Hyper or hypothyroidism-Acidosis-Addisonian crisishelliphelliphelliphelliphelliphelliphellipmany others
Ohrsquos Intensive Care manual 6th edition ch 42
Septic Encephalopathy-A flavour almost exclusive to the ICU- according to Ohs 8-80 of septic patients are affected- Defined as encephalopathy in the presence of extracranial infection without any other good reason to explain it- Lots of theories regarding pathogenesis
-Cerebral oedema due to leaky capillaries-Damaged BBB-Endotoxin-induced decrease in O2 consumption in the brain
-No lateralizing signs-Rarely is there flap or myoclonus
-Treatment ought to focus on the infectious cause
Ohrsquos Intensive Care manual 6th edition ch 42
ldquoICU Encephalopathyrdquo- so itrsquos the 5th-7th day of your admission Or you are the night reg and its your 5th - 7th night shift
- You havent slept- Your circadian rhythm is disturbed- You are full of mind-altering drugs- You are constantly uncomfortable- Your environment is noisy and monotonous
-Diagnosis of exclusion
Why is this a problem-Irritates the nurse-Staff may get attacked-Tubes and lines get dislodged - damage to the patient and to the budget
-Total tissue oxygen consumption increases-Quality of monitoring is compromised-Duration of stay is increased -Extubation is delayed (bolusbolusbolus)- Higher incidence of nosocomial pneumonia (aspiration or otherwise)
Delirium is an independent predictor of-increased mortality-length of stay-cost of care
Equivalent to organ failure Weirdly aggressive delirium has a better prognosis than ldquoquietrdquo delirium
GL Fraser RR Riker The frequency and cost of patient-initiated device removal in the ICU - Pharmacotherapy 2001 vol 21 issue 1Pun BT et al The importance of diagnosing and managing ICU delirium Chest 2007 Aug132(2)624-36Pandharipande P Delirium acute cognitive dysfunction in the critically ill Curr Opin Crit Care 2005 Aug11(4)360-8Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141
Risk factors for ICU delirium - Prolonged sedation mechanical ventilation- Severity of illness- Use of sedatives and analgesics (benzos gt opiates)- Age
- Most studies donrsquot seem to differentiate between causes of delirium -Their list of risk factors includes history of smoking alcoholism liver dysfunction sepsis and other causes of metabolic or toxic encephalopathy
Lin SM et al Risk factors for the development of early-onset delirium and the subsequent clinical outcome in mechanically ventilated patients J Crit Care 2008 Sep23(3)372-9 Epub 2007 Jan 31Ouimet S et al Incidence risk factors and consequences of ICU delirium Intensive Care Med 2007 Jan33(1)66-73 Epub 2006 Nov 11
Assessment of delirium in the ICU-Is Mr X actually delirious
-Jacobi etal (2002) recommends the use of the Confusion Assessment Method in the ICU (CAM-ICU)
-Apparently 2 minutes to complete -Requires some degree of cooperation
-According to a 2008 survey only 9 of all Australian units use any sort of scale like this
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8
Alex Yartsev 1542011
Diagnosis of ICU delirium - Diagnosis of exclusion- Imaging excludes structural causes of encephalopathy- Bloods exclude many of the metabolic causes- What remains is excluded with history- Easier said than done
-Address the cause
-ldquoMultifactorialrdquo is a safe guess
The CAM-ICU
Just calm down Sir You are in hospital-MANAGEMENT OF ICU DELIRIUM
-Preventative vs reactive-Non-pharmacological vs pharmacological
Prevention of ICU delirium - Sedation Holidays
-2000 study by Kress landmark paper 128 pts -length of stay reduced from 99 to 66 days-9 vs 16 pts needed delirium workup-According to a 2008 survey only 30 of Australian units use sedation holidays
- Frequent reproducible assessment for pain and delirium-Jacobi et a (2002 multidisciplinary task force) -recommend the use of a validated agitationsedation measurement tool -eg Richmond Agitation-Sedation Scale
- Quiet environment thus good sleep - Music thus reduced anxiety improved relaxationKress JP Pohlman AS OConner MF et al Daily interruption of sedation infusions in critically ill patients undergoing mechanical ventilation N Engl J Med 2000 342
1471ndash7Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Freedman NS et al Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit Am J Resp Crit Care Med 1999159 1155ndash1162Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8Chlan L Effectiveness of a music therapy intervention on relaxation and anxiety for patients receiving ventilatory assistance Heart Lung 199827169ndash176
Pharmacological Arsenal
How shall I most effectively drug Mr X-Jacobi et al (2002) recommends Haloperidol (level C data small studies and case report series)
-Cochrane library agrees to some extent
Lonergan etal (2007) haloperidol is better than placebo buthellip - no better then olanzapine at low doses- and with more side effects at high dosesErgo use olanzapine where possible
Lonergan etal (2009) ndash no evidence to support benzos in delirium unless alcohol withdrawal is the cause
-Everyone agrees monitor QTc (level B evidence)
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Lonergan etal Benzodiazepines for delirium Cochrane Database of Systematic Reviews 2009 Issue 4Lonergan E Britton AM Luxenberg J Antipsychotics for delirium Cochrane Database of Systematic Reviews 2007 Issue 2Milbrandt etal Haloperidol use is associated with lower hospital mortality in mechanically ventilated patients Crit Care Med 2005 Jan33(1)226-9 discussion 263-5
How shall I adjust Mr Xrsquos sedation cocktailKeeping in mind the goal is to wean him off the ventilator
-Unless he is withdrawing from alcohol change midazolam to propofol
-ADD DEXMEDETOMIDINE
-Dex vs propofol Ruokonen et al (2009) 87 pts adding Dex has no effect on length of stay but decreases length of
ventilation
-Dex vs Midazolam Riker et al (2009) 375 ptsprevalence of delirium 54(dex) vs 76 (midaz) also faster extubation
- CORRECT MAGNESIUM- target range 10-20 in addition to remi + midaz 63 pts 2009 RCT by Esen
-Of the delirious pts the magnesium group had fewer days of delirium (55 vs 89) and consumed less sedatives
Mirski et al Cognitive improvement during continuous sedation in critically ill awake and responsive patients The Acute Neurological ICU Sedation Trial (ANIST) Intensive Care Medicine 2010 vol 36 issue 9 1505-1513Ruokonen et alDexmedetomidine versus propofolmidazolam for long-term sedation during mechanical ventilation Intensive Care Medicine 2009 vol 35 issue 2 282-90Riker RR et al Dexmedetomidine vs midazolam for sedation of critically ill patients a randomized trial JAMA the journal of the American Medical Association 2009 Feb 301 issue 5 Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Esen F et al Effect of magnesium on the incidence of delirium occurrence in the ICU Critical Care 2009 vol 13 supp 1P412
When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please

Ohrsquos Intensive Care manual 6th edition ch 42
Why is Mr X doing that- Inability to communicate something - Pain ndash he is lying on top of a forgotten 10ml syringe
- Dementia ndash this is what he is normally like at the nursing home- Psychosis ndash we accidentally stopped his risperidone and started an MAOI
- Intoxication ndash APS team started ketamine- Withdrawal ndash he drinks - Delirium Tremensndash he REALLY drinks
- ENCEPHALOPATHY An alteration in the level or content of consciousness due to a process extrinsic to the brain
metabolic vs structural
Ohrsquos Intensive Care manual 6th edition ch 42
A moment for Encephalopathy
-SEPSIS-ICU DELIRIUMhellipalsohellip-Hepatic failure-Renal Failure-Hypoxia or hypercapnea-Hyper or hyponatremia-Hyper or hypoglycaemia-Hyper or hypothyroidism-Acidosis-Addisonian crisishelliphelliphelliphelliphelliphelliphellipmany others
Ohrsquos Intensive Care manual 6th edition ch 42
Septic Encephalopathy-A flavour almost exclusive to the ICU- according to Ohs 8-80 of septic patients are affected- Defined as encephalopathy in the presence of extracranial infection without any other good reason to explain it- Lots of theories regarding pathogenesis
-Cerebral oedema due to leaky capillaries-Damaged BBB-Endotoxin-induced decrease in O2 consumption in the brain
-No lateralizing signs-Rarely is there flap or myoclonus
-Treatment ought to focus on the infectious cause
Ohrsquos Intensive Care manual 6th edition ch 42
ldquoICU Encephalopathyrdquo- so itrsquos the 5th-7th day of your admission Or you are the night reg and its your 5th - 7th night shift
- You havent slept- Your circadian rhythm is disturbed- You are full of mind-altering drugs- You are constantly uncomfortable- Your environment is noisy and monotonous
-Diagnosis of exclusion
Why is this a problem-Irritates the nurse-Staff may get attacked-Tubes and lines get dislodged - damage to the patient and to the budget
-Total tissue oxygen consumption increases-Quality of monitoring is compromised-Duration of stay is increased -Extubation is delayed (bolusbolusbolus)- Higher incidence of nosocomial pneumonia (aspiration or otherwise)
Delirium is an independent predictor of-increased mortality-length of stay-cost of care
Equivalent to organ failure Weirdly aggressive delirium has a better prognosis than ldquoquietrdquo delirium
GL Fraser RR Riker The frequency and cost of patient-initiated device removal in the ICU - Pharmacotherapy 2001 vol 21 issue 1Pun BT et al The importance of diagnosing and managing ICU delirium Chest 2007 Aug132(2)624-36Pandharipande P Delirium acute cognitive dysfunction in the critically ill Curr Opin Crit Care 2005 Aug11(4)360-8Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141
Risk factors for ICU delirium - Prolonged sedation mechanical ventilation- Severity of illness- Use of sedatives and analgesics (benzos gt opiates)- Age
- Most studies donrsquot seem to differentiate between causes of delirium -Their list of risk factors includes history of smoking alcoholism liver dysfunction sepsis and other causes of metabolic or toxic encephalopathy
Lin SM et al Risk factors for the development of early-onset delirium and the subsequent clinical outcome in mechanically ventilated patients J Crit Care 2008 Sep23(3)372-9 Epub 2007 Jan 31Ouimet S et al Incidence risk factors and consequences of ICU delirium Intensive Care Med 2007 Jan33(1)66-73 Epub 2006 Nov 11
Assessment of delirium in the ICU-Is Mr X actually delirious
-Jacobi etal (2002) recommends the use of the Confusion Assessment Method in the ICU (CAM-ICU)
-Apparently 2 minutes to complete -Requires some degree of cooperation
-According to a 2008 survey only 9 of all Australian units use any sort of scale like this
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8
Alex Yartsev 1542011
Diagnosis of ICU delirium - Diagnosis of exclusion- Imaging excludes structural causes of encephalopathy- Bloods exclude many of the metabolic causes- What remains is excluded with history- Easier said than done
-Address the cause
-ldquoMultifactorialrdquo is a safe guess
The CAM-ICU
Just calm down Sir You are in hospital-MANAGEMENT OF ICU DELIRIUM
-Preventative vs reactive-Non-pharmacological vs pharmacological
Prevention of ICU delirium - Sedation Holidays
-2000 study by Kress landmark paper 128 pts -length of stay reduced from 99 to 66 days-9 vs 16 pts needed delirium workup-According to a 2008 survey only 30 of Australian units use sedation holidays
- Frequent reproducible assessment for pain and delirium-Jacobi et a (2002 multidisciplinary task force) -recommend the use of a validated agitationsedation measurement tool -eg Richmond Agitation-Sedation Scale
- Quiet environment thus good sleep - Music thus reduced anxiety improved relaxationKress JP Pohlman AS OConner MF et al Daily interruption of sedation infusions in critically ill patients undergoing mechanical ventilation N Engl J Med 2000 342
1471ndash7Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Freedman NS et al Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit Am J Resp Crit Care Med 1999159 1155ndash1162Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8Chlan L Effectiveness of a music therapy intervention on relaxation and anxiety for patients receiving ventilatory assistance Heart Lung 199827169ndash176
Pharmacological Arsenal
How shall I most effectively drug Mr X-Jacobi et al (2002) recommends Haloperidol (level C data small studies and case report series)
-Cochrane library agrees to some extent
Lonergan etal (2007) haloperidol is better than placebo buthellip - no better then olanzapine at low doses- and with more side effects at high dosesErgo use olanzapine where possible
Lonergan etal (2009) ndash no evidence to support benzos in delirium unless alcohol withdrawal is the cause
-Everyone agrees monitor QTc (level B evidence)
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Lonergan etal Benzodiazepines for delirium Cochrane Database of Systematic Reviews 2009 Issue 4Lonergan E Britton AM Luxenberg J Antipsychotics for delirium Cochrane Database of Systematic Reviews 2007 Issue 2Milbrandt etal Haloperidol use is associated with lower hospital mortality in mechanically ventilated patients Crit Care Med 2005 Jan33(1)226-9 discussion 263-5
How shall I adjust Mr Xrsquos sedation cocktailKeeping in mind the goal is to wean him off the ventilator
-Unless he is withdrawing from alcohol change midazolam to propofol
-ADD DEXMEDETOMIDINE
-Dex vs propofol Ruokonen et al (2009) 87 pts adding Dex has no effect on length of stay but decreases length of
ventilation
-Dex vs Midazolam Riker et al (2009) 375 ptsprevalence of delirium 54(dex) vs 76 (midaz) also faster extubation
- CORRECT MAGNESIUM- target range 10-20 in addition to remi + midaz 63 pts 2009 RCT by Esen
-Of the delirious pts the magnesium group had fewer days of delirium (55 vs 89) and consumed less sedatives
Mirski et al Cognitive improvement during continuous sedation in critically ill awake and responsive patients The Acute Neurological ICU Sedation Trial (ANIST) Intensive Care Medicine 2010 vol 36 issue 9 1505-1513Ruokonen et alDexmedetomidine versus propofolmidazolam for long-term sedation during mechanical ventilation Intensive Care Medicine 2009 vol 35 issue 2 282-90Riker RR et al Dexmedetomidine vs midazolam for sedation of critically ill patients a randomized trial JAMA the journal of the American Medical Association 2009 Feb 301 issue 5 Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Esen F et al Effect of magnesium on the incidence of delirium occurrence in the ICU Critical Care 2009 vol 13 supp 1P412
When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please
Ohrsquos Intensive Care manual 6th edition ch 42
A moment for Encephalopathy
-SEPSIS-ICU DELIRIUMhellipalsohellip-Hepatic failure-Renal Failure-Hypoxia or hypercapnea-Hyper or hyponatremia-Hyper or hypoglycaemia-Hyper or hypothyroidism-Acidosis-Addisonian crisishelliphelliphelliphelliphelliphelliphellipmany others
Ohrsquos Intensive Care manual 6th edition ch 42
Septic Encephalopathy-A flavour almost exclusive to the ICU- according to Ohs 8-80 of septic patients are affected- Defined as encephalopathy in the presence of extracranial infection without any other good reason to explain it- Lots of theories regarding pathogenesis
-Cerebral oedema due to leaky capillaries-Damaged BBB-Endotoxin-induced decrease in O2 consumption in the brain
-No lateralizing signs-Rarely is there flap or myoclonus
-Treatment ought to focus on the infectious cause
Ohrsquos Intensive Care manual 6th edition ch 42
ldquoICU Encephalopathyrdquo- so itrsquos the 5th-7th day of your admission Or you are the night reg and its your 5th - 7th night shift
- You havent slept- Your circadian rhythm is disturbed- You are full of mind-altering drugs- You are constantly uncomfortable- Your environment is noisy and monotonous
-Diagnosis of exclusion
Why is this a problem-Irritates the nurse-Staff may get attacked-Tubes and lines get dislodged - damage to the patient and to the budget
-Total tissue oxygen consumption increases-Quality of monitoring is compromised-Duration of stay is increased -Extubation is delayed (bolusbolusbolus)- Higher incidence of nosocomial pneumonia (aspiration or otherwise)
Delirium is an independent predictor of-increased mortality-length of stay-cost of care
Equivalent to organ failure Weirdly aggressive delirium has a better prognosis than ldquoquietrdquo delirium
GL Fraser RR Riker The frequency and cost of patient-initiated device removal in the ICU - Pharmacotherapy 2001 vol 21 issue 1Pun BT et al The importance of diagnosing and managing ICU delirium Chest 2007 Aug132(2)624-36Pandharipande P Delirium acute cognitive dysfunction in the critically ill Curr Opin Crit Care 2005 Aug11(4)360-8Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141
Risk factors for ICU delirium - Prolonged sedation mechanical ventilation- Severity of illness- Use of sedatives and analgesics (benzos gt opiates)- Age
- Most studies donrsquot seem to differentiate between causes of delirium -Their list of risk factors includes history of smoking alcoholism liver dysfunction sepsis and other causes of metabolic or toxic encephalopathy
Lin SM et al Risk factors for the development of early-onset delirium and the subsequent clinical outcome in mechanically ventilated patients J Crit Care 2008 Sep23(3)372-9 Epub 2007 Jan 31Ouimet S et al Incidence risk factors and consequences of ICU delirium Intensive Care Med 2007 Jan33(1)66-73 Epub 2006 Nov 11
Assessment of delirium in the ICU-Is Mr X actually delirious
-Jacobi etal (2002) recommends the use of the Confusion Assessment Method in the ICU (CAM-ICU)
-Apparently 2 minutes to complete -Requires some degree of cooperation
-According to a 2008 survey only 9 of all Australian units use any sort of scale like this
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8
Alex Yartsev 1542011
Diagnosis of ICU delirium - Diagnosis of exclusion- Imaging excludes structural causes of encephalopathy- Bloods exclude many of the metabolic causes- What remains is excluded with history- Easier said than done
-Address the cause
-ldquoMultifactorialrdquo is a safe guess
The CAM-ICU
Just calm down Sir You are in hospital-MANAGEMENT OF ICU DELIRIUM
-Preventative vs reactive-Non-pharmacological vs pharmacological
Prevention of ICU delirium - Sedation Holidays
-2000 study by Kress landmark paper 128 pts -length of stay reduced from 99 to 66 days-9 vs 16 pts needed delirium workup-According to a 2008 survey only 30 of Australian units use sedation holidays
- Frequent reproducible assessment for pain and delirium-Jacobi et a (2002 multidisciplinary task force) -recommend the use of a validated agitationsedation measurement tool -eg Richmond Agitation-Sedation Scale
- Quiet environment thus good sleep - Music thus reduced anxiety improved relaxationKress JP Pohlman AS OConner MF et al Daily interruption of sedation infusions in critically ill patients undergoing mechanical ventilation N Engl J Med 2000 342
1471ndash7Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Freedman NS et al Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit Am J Resp Crit Care Med 1999159 1155ndash1162Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8Chlan L Effectiveness of a music therapy intervention on relaxation and anxiety for patients receiving ventilatory assistance Heart Lung 199827169ndash176
Pharmacological Arsenal
How shall I most effectively drug Mr X-Jacobi et al (2002) recommends Haloperidol (level C data small studies and case report series)
-Cochrane library agrees to some extent
Lonergan etal (2007) haloperidol is better than placebo buthellip - no better then olanzapine at low doses- and with more side effects at high dosesErgo use olanzapine where possible
Lonergan etal (2009) ndash no evidence to support benzos in delirium unless alcohol withdrawal is the cause
-Everyone agrees monitor QTc (level B evidence)
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Lonergan etal Benzodiazepines for delirium Cochrane Database of Systematic Reviews 2009 Issue 4Lonergan E Britton AM Luxenberg J Antipsychotics for delirium Cochrane Database of Systematic Reviews 2007 Issue 2Milbrandt etal Haloperidol use is associated with lower hospital mortality in mechanically ventilated patients Crit Care Med 2005 Jan33(1)226-9 discussion 263-5
How shall I adjust Mr Xrsquos sedation cocktailKeeping in mind the goal is to wean him off the ventilator
-Unless he is withdrawing from alcohol change midazolam to propofol
-ADD DEXMEDETOMIDINE
-Dex vs propofol Ruokonen et al (2009) 87 pts adding Dex has no effect on length of stay but decreases length of
ventilation
-Dex vs Midazolam Riker et al (2009) 375 ptsprevalence of delirium 54(dex) vs 76 (midaz) also faster extubation
- CORRECT MAGNESIUM- target range 10-20 in addition to remi + midaz 63 pts 2009 RCT by Esen
-Of the delirious pts the magnesium group had fewer days of delirium (55 vs 89) and consumed less sedatives
Mirski et al Cognitive improvement during continuous sedation in critically ill awake and responsive patients The Acute Neurological ICU Sedation Trial (ANIST) Intensive Care Medicine 2010 vol 36 issue 9 1505-1513Ruokonen et alDexmedetomidine versus propofolmidazolam for long-term sedation during mechanical ventilation Intensive Care Medicine 2009 vol 35 issue 2 282-90Riker RR et al Dexmedetomidine vs midazolam for sedation of critically ill patients a randomized trial JAMA the journal of the American Medical Association 2009 Feb 301 issue 5 Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Esen F et al Effect of magnesium on the incidence of delirium occurrence in the ICU Critical Care 2009 vol 13 supp 1P412
When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please

Ohrsquos Intensive Care manual 6th edition ch 42
Septic Encephalopathy-A flavour almost exclusive to the ICU- according to Ohs 8-80 of septic patients are affected- Defined as encephalopathy in the presence of extracranial infection without any other good reason to explain it- Lots of theories regarding pathogenesis
-Cerebral oedema due to leaky capillaries-Damaged BBB-Endotoxin-induced decrease in O2 consumption in the brain
-No lateralizing signs-Rarely is there flap or myoclonus
-Treatment ought to focus on the infectious cause
Ohrsquos Intensive Care manual 6th edition ch 42
ldquoICU Encephalopathyrdquo- so itrsquos the 5th-7th day of your admission Or you are the night reg and its your 5th - 7th night shift
- You havent slept- Your circadian rhythm is disturbed- You are full of mind-altering drugs- You are constantly uncomfortable- Your environment is noisy and monotonous
-Diagnosis of exclusion
Why is this a problem-Irritates the nurse-Staff may get attacked-Tubes and lines get dislodged - damage to the patient and to the budget
-Total tissue oxygen consumption increases-Quality of monitoring is compromised-Duration of stay is increased -Extubation is delayed (bolusbolusbolus)- Higher incidence of nosocomial pneumonia (aspiration or otherwise)
Delirium is an independent predictor of-increased mortality-length of stay-cost of care
Equivalent to organ failure Weirdly aggressive delirium has a better prognosis than ldquoquietrdquo delirium
GL Fraser RR Riker The frequency and cost of patient-initiated device removal in the ICU - Pharmacotherapy 2001 vol 21 issue 1Pun BT et al The importance of diagnosing and managing ICU delirium Chest 2007 Aug132(2)624-36Pandharipande P Delirium acute cognitive dysfunction in the critically ill Curr Opin Crit Care 2005 Aug11(4)360-8Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141
Risk factors for ICU delirium - Prolonged sedation mechanical ventilation- Severity of illness- Use of sedatives and analgesics (benzos gt opiates)- Age
- Most studies donrsquot seem to differentiate between causes of delirium -Their list of risk factors includes history of smoking alcoholism liver dysfunction sepsis and other causes of metabolic or toxic encephalopathy
Lin SM et al Risk factors for the development of early-onset delirium and the subsequent clinical outcome in mechanically ventilated patients J Crit Care 2008 Sep23(3)372-9 Epub 2007 Jan 31Ouimet S et al Incidence risk factors and consequences of ICU delirium Intensive Care Med 2007 Jan33(1)66-73 Epub 2006 Nov 11
Assessment of delirium in the ICU-Is Mr X actually delirious
-Jacobi etal (2002) recommends the use of the Confusion Assessment Method in the ICU (CAM-ICU)
-Apparently 2 minutes to complete -Requires some degree of cooperation
-According to a 2008 survey only 9 of all Australian units use any sort of scale like this
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8
Alex Yartsev 1542011
Diagnosis of ICU delirium - Diagnosis of exclusion- Imaging excludes structural causes of encephalopathy- Bloods exclude many of the metabolic causes- What remains is excluded with history- Easier said than done
-Address the cause
-ldquoMultifactorialrdquo is a safe guess
The CAM-ICU
Just calm down Sir You are in hospital-MANAGEMENT OF ICU DELIRIUM
-Preventative vs reactive-Non-pharmacological vs pharmacological
Prevention of ICU delirium - Sedation Holidays
-2000 study by Kress landmark paper 128 pts -length of stay reduced from 99 to 66 days-9 vs 16 pts needed delirium workup-According to a 2008 survey only 30 of Australian units use sedation holidays
- Frequent reproducible assessment for pain and delirium-Jacobi et a (2002 multidisciplinary task force) -recommend the use of a validated agitationsedation measurement tool -eg Richmond Agitation-Sedation Scale
- Quiet environment thus good sleep - Music thus reduced anxiety improved relaxationKress JP Pohlman AS OConner MF et al Daily interruption of sedation infusions in critically ill patients undergoing mechanical ventilation N Engl J Med 2000 342
1471ndash7Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Freedman NS et al Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit Am J Resp Crit Care Med 1999159 1155ndash1162Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8Chlan L Effectiveness of a music therapy intervention on relaxation and anxiety for patients receiving ventilatory assistance Heart Lung 199827169ndash176
Pharmacological Arsenal
How shall I most effectively drug Mr X-Jacobi et al (2002) recommends Haloperidol (level C data small studies and case report series)
-Cochrane library agrees to some extent
Lonergan etal (2007) haloperidol is better than placebo buthellip - no better then olanzapine at low doses- and with more side effects at high dosesErgo use olanzapine where possible
Lonergan etal (2009) ndash no evidence to support benzos in delirium unless alcohol withdrawal is the cause
-Everyone agrees monitor QTc (level B evidence)
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Lonergan etal Benzodiazepines for delirium Cochrane Database of Systematic Reviews 2009 Issue 4Lonergan E Britton AM Luxenberg J Antipsychotics for delirium Cochrane Database of Systematic Reviews 2007 Issue 2Milbrandt etal Haloperidol use is associated with lower hospital mortality in mechanically ventilated patients Crit Care Med 2005 Jan33(1)226-9 discussion 263-5
How shall I adjust Mr Xrsquos sedation cocktailKeeping in mind the goal is to wean him off the ventilator
-Unless he is withdrawing from alcohol change midazolam to propofol
-ADD DEXMEDETOMIDINE
-Dex vs propofol Ruokonen et al (2009) 87 pts adding Dex has no effect on length of stay but decreases length of
ventilation
-Dex vs Midazolam Riker et al (2009) 375 ptsprevalence of delirium 54(dex) vs 76 (midaz) also faster extubation
- CORRECT MAGNESIUM- target range 10-20 in addition to remi + midaz 63 pts 2009 RCT by Esen
-Of the delirious pts the magnesium group had fewer days of delirium (55 vs 89) and consumed less sedatives
Mirski et al Cognitive improvement during continuous sedation in critically ill awake and responsive patients The Acute Neurological ICU Sedation Trial (ANIST) Intensive Care Medicine 2010 vol 36 issue 9 1505-1513Ruokonen et alDexmedetomidine versus propofolmidazolam for long-term sedation during mechanical ventilation Intensive Care Medicine 2009 vol 35 issue 2 282-90Riker RR et al Dexmedetomidine vs midazolam for sedation of critically ill patients a randomized trial JAMA the journal of the American Medical Association 2009 Feb 301 issue 5 Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Esen F et al Effect of magnesium on the incidence of delirium occurrence in the ICU Critical Care 2009 vol 13 supp 1P412
When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please
Ohrsquos Intensive Care manual 6th edition ch 42
ldquoICU Encephalopathyrdquo- so itrsquos the 5th-7th day of your admission Or you are the night reg and its your 5th - 7th night shift
- You havent slept- Your circadian rhythm is disturbed- You are full of mind-altering drugs- You are constantly uncomfortable- Your environment is noisy and monotonous
-Diagnosis of exclusion
Why is this a problem-Irritates the nurse-Staff may get attacked-Tubes and lines get dislodged - damage to the patient and to the budget
-Total tissue oxygen consumption increases-Quality of monitoring is compromised-Duration of stay is increased -Extubation is delayed (bolusbolusbolus)- Higher incidence of nosocomial pneumonia (aspiration or otherwise)
Delirium is an independent predictor of-increased mortality-length of stay-cost of care
Equivalent to organ failure Weirdly aggressive delirium has a better prognosis than ldquoquietrdquo delirium
GL Fraser RR Riker The frequency and cost of patient-initiated device removal in the ICU - Pharmacotherapy 2001 vol 21 issue 1Pun BT et al The importance of diagnosing and managing ICU delirium Chest 2007 Aug132(2)624-36Pandharipande P Delirium acute cognitive dysfunction in the critically ill Curr Opin Crit Care 2005 Aug11(4)360-8Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141
Risk factors for ICU delirium - Prolonged sedation mechanical ventilation- Severity of illness- Use of sedatives and analgesics (benzos gt opiates)- Age
- Most studies donrsquot seem to differentiate between causes of delirium -Their list of risk factors includes history of smoking alcoholism liver dysfunction sepsis and other causes of metabolic or toxic encephalopathy
Lin SM et al Risk factors for the development of early-onset delirium and the subsequent clinical outcome in mechanically ventilated patients J Crit Care 2008 Sep23(3)372-9 Epub 2007 Jan 31Ouimet S et al Incidence risk factors and consequences of ICU delirium Intensive Care Med 2007 Jan33(1)66-73 Epub 2006 Nov 11
Assessment of delirium in the ICU-Is Mr X actually delirious
-Jacobi etal (2002) recommends the use of the Confusion Assessment Method in the ICU (CAM-ICU)
-Apparently 2 minutes to complete -Requires some degree of cooperation
-According to a 2008 survey only 9 of all Australian units use any sort of scale like this
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8
Alex Yartsev 1542011
Diagnosis of ICU delirium - Diagnosis of exclusion- Imaging excludes structural causes of encephalopathy- Bloods exclude many of the metabolic causes- What remains is excluded with history- Easier said than done
-Address the cause
-ldquoMultifactorialrdquo is a safe guess
The CAM-ICU
Just calm down Sir You are in hospital-MANAGEMENT OF ICU DELIRIUM
-Preventative vs reactive-Non-pharmacological vs pharmacological
Prevention of ICU delirium - Sedation Holidays
-2000 study by Kress landmark paper 128 pts -length of stay reduced from 99 to 66 days-9 vs 16 pts needed delirium workup-According to a 2008 survey only 30 of Australian units use sedation holidays
- Frequent reproducible assessment for pain and delirium-Jacobi et a (2002 multidisciplinary task force) -recommend the use of a validated agitationsedation measurement tool -eg Richmond Agitation-Sedation Scale
- Quiet environment thus good sleep - Music thus reduced anxiety improved relaxationKress JP Pohlman AS OConner MF et al Daily interruption of sedation infusions in critically ill patients undergoing mechanical ventilation N Engl J Med 2000 342
1471ndash7Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Freedman NS et al Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit Am J Resp Crit Care Med 1999159 1155ndash1162Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8Chlan L Effectiveness of a music therapy intervention on relaxation and anxiety for patients receiving ventilatory assistance Heart Lung 199827169ndash176
Pharmacological Arsenal
How shall I most effectively drug Mr X-Jacobi et al (2002) recommends Haloperidol (level C data small studies and case report series)
-Cochrane library agrees to some extent
Lonergan etal (2007) haloperidol is better than placebo buthellip - no better then olanzapine at low doses- and with more side effects at high dosesErgo use olanzapine where possible
Lonergan etal (2009) ndash no evidence to support benzos in delirium unless alcohol withdrawal is the cause
-Everyone agrees monitor QTc (level B evidence)
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Lonergan etal Benzodiazepines for delirium Cochrane Database of Systematic Reviews 2009 Issue 4Lonergan E Britton AM Luxenberg J Antipsychotics for delirium Cochrane Database of Systematic Reviews 2007 Issue 2Milbrandt etal Haloperidol use is associated with lower hospital mortality in mechanically ventilated patients Crit Care Med 2005 Jan33(1)226-9 discussion 263-5
How shall I adjust Mr Xrsquos sedation cocktailKeeping in mind the goal is to wean him off the ventilator
-Unless he is withdrawing from alcohol change midazolam to propofol
-ADD DEXMEDETOMIDINE
-Dex vs propofol Ruokonen et al (2009) 87 pts adding Dex has no effect on length of stay but decreases length of
ventilation
-Dex vs Midazolam Riker et al (2009) 375 ptsprevalence of delirium 54(dex) vs 76 (midaz) also faster extubation
- CORRECT MAGNESIUM- target range 10-20 in addition to remi + midaz 63 pts 2009 RCT by Esen
-Of the delirious pts the magnesium group had fewer days of delirium (55 vs 89) and consumed less sedatives
Mirski et al Cognitive improvement during continuous sedation in critically ill awake and responsive patients The Acute Neurological ICU Sedation Trial (ANIST) Intensive Care Medicine 2010 vol 36 issue 9 1505-1513Ruokonen et alDexmedetomidine versus propofolmidazolam for long-term sedation during mechanical ventilation Intensive Care Medicine 2009 vol 35 issue 2 282-90Riker RR et al Dexmedetomidine vs midazolam for sedation of critically ill patients a randomized trial JAMA the journal of the American Medical Association 2009 Feb 301 issue 5 Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Esen F et al Effect of magnesium on the incidence of delirium occurrence in the ICU Critical Care 2009 vol 13 supp 1P412
When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please

Why is this a problem-Irritates the nurse-Staff may get attacked-Tubes and lines get dislodged - damage to the patient and to the budget
-Total tissue oxygen consumption increases-Quality of monitoring is compromised-Duration of stay is increased -Extubation is delayed (bolusbolusbolus)- Higher incidence of nosocomial pneumonia (aspiration or otherwise)
Delirium is an independent predictor of-increased mortality-length of stay-cost of care
Equivalent to organ failure Weirdly aggressive delirium has a better prognosis than ldquoquietrdquo delirium
GL Fraser RR Riker The frequency and cost of patient-initiated device removal in the ICU - Pharmacotherapy 2001 vol 21 issue 1Pun BT et al The importance of diagnosing and managing ICU delirium Chest 2007 Aug132(2)624-36Pandharipande P Delirium acute cognitive dysfunction in the critically ill Curr Opin Crit Care 2005 Aug11(4)360-8Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141
Risk factors for ICU delirium - Prolonged sedation mechanical ventilation- Severity of illness- Use of sedatives and analgesics (benzos gt opiates)- Age
- Most studies donrsquot seem to differentiate between causes of delirium -Their list of risk factors includes history of smoking alcoholism liver dysfunction sepsis and other causes of metabolic or toxic encephalopathy
Lin SM et al Risk factors for the development of early-onset delirium and the subsequent clinical outcome in mechanically ventilated patients J Crit Care 2008 Sep23(3)372-9 Epub 2007 Jan 31Ouimet S et al Incidence risk factors and consequences of ICU delirium Intensive Care Med 2007 Jan33(1)66-73 Epub 2006 Nov 11
Assessment of delirium in the ICU-Is Mr X actually delirious
-Jacobi etal (2002) recommends the use of the Confusion Assessment Method in the ICU (CAM-ICU)
-Apparently 2 minutes to complete -Requires some degree of cooperation
-According to a 2008 survey only 9 of all Australian units use any sort of scale like this
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8
Alex Yartsev 1542011
Diagnosis of ICU delirium - Diagnosis of exclusion- Imaging excludes structural causes of encephalopathy- Bloods exclude many of the metabolic causes- What remains is excluded with history- Easier said than done
-Address the cause
-ldquoMultifactorialrdquo is a safe guess
The CAM-ICU
Just calm down Sir You are in hospital-MANAGEMENT OF ICU DELIRIUM
-Preventative vs reactive-Non-pharmacological vs pharmacological
Prevention of ICU delirium - Sedation Holidays
-2000 study by Kress landmark paper 128 pts -length of stay reduced from 99 to 66 days-9 vs 16 pts needed delirium workup-According to a 2008 survey only 30 of Australian units use sedation holidays
- Frequent reproducible assessment for pain and delirium-Jacobi et a (2002 multidisciplinary task force) -recommend the use of a validated agitationsedation measurement tool -eg Richmond Agitation-Sedation Scale
- Quiet environment thus good sleep - Music thus reduced anxiety improved relaxationKress JP Pohlman AS OConner MF et al Daily interruption of sedation infusions in critically ill patients undergoing mechanical ventilation N Engl J Med 2000 342
1471ndash7Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Freedman NS et al Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit Am J Resp Crit Care Med 1999159 1155ndash1162Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8Chlan L Effectiveness of a music therapy intervention on relaxation and anxiety for patients receiving ventilatory assistance Heart Lung 199827169ndash176
Pharmacological Arsenal
How shall I most effectively drug Mr X-Jacobi et al (2002) recommends Haloperidol (level C data small studies and case report series)
-Cochrane library agrees to some extent
Lonergan etal (2007) haloperidol is better than placebo buthellip - no better then olanzapine at low doses- and with more side effects at high dosesErgo use olanzapine where possible
Lonergan etal (2009) ndash no evidence to support benzos in delirium unless alcohol withdrawal is the cause
-Everyone agrees monitor QTc (level B evidence)
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Lonergan etal Benzodiazepines for delirium Cochrane Database of Systematic Reviews 2009 Issue 4Lonergan E Britton AM Luxenberg J Antipsychotics for delirium Cochrane Database of Systematic Reviews 2007 Issue 2Milbrandt etal Haloperidol use is associated with lower hospital mortality in mechanically ventilated patients Crit Care Med 2005 Jan33(1)226-9 discussion 263-5
How shall I adjust Mr Xrsquos sedation cocktailKeeping in mind the goal is to wean him off the ventilator
-Unless he is withdrawing from alcohol change midazolam to propofol
-ADD DEXMEDETOMIDINE
-Dex vs propofol Ruokonen et al (2009) 87 pts adding Dex has no effect on length of stay but decreases length of
ventilation
-Dex vs Midazolam Riker et al (2009) 375 ptsprevalence of delirium 54(dex) vs 76 (midaz) also faster extubation
- CORRECT MAGNESIUM- target range 10-20 in addition to remi + midaz 63 pts 2009 RCT by Esen
-Of the delirious pts the magnesium group had fewer days of delirium (55 vs 89) and consumed less sedatives
Mirski et al Cognitive improvement during continuous sedation in critically ill awake and responsive patients The Acute Neurological ICU Sedation Trial (ANIST) Intensive Care Medicine 2010 vol 36 issue 9 1505-1513Ruokonen et alDexmedetomidine versus propofolmidazolam for long-term sedation during mechanical ventilation Intensive Care Medicine 2009 vol 35 issue 2 282-90Riker RR et al Dexmedetomidine vs midazolam for sedation of critically ill patients a randomized trial JAMA the journal of the American Medical Association 2009 Feb 301 issue 5 Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Esen F et al Effect of magnesium on the incidence of delirium occurrence in the ICU Critical Care 2009 vol 13 supp 1P412
When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please

Risk factors for ICU delirium - Prolonged sedation mechanical ventilation- Severity of illness- Use of sedatives and analgesics (benzos gt opiates)- Age
- Most studies donrsquot seem to differentiate between causes of delirium -Their list of risk factors includes history of smoking alcoholism liver dysfunction sepsis and other causes of metabolic or toxic encephalopathy
Lin SM et al Risk factors for the development of early-onset delirium and the subsequent clinical outcome in mechanically ventilated patients J Crit Care 2008 Sep23(3)372-9 Epub 2007 Jan 31Ouimet S et al Incidence risk factors and consequences of ICU delirium Intensive Care Med 2007 Jan33(1)66-73 Epub 2006 Nov 11
Assessment of delirium in the ICU-Is Mr X actually delirious
-Jacobi etal (2002) recommends the use of the Confusion Assessment Method in the ICU (CAM-ICU)
-Apparently 2 minutes to complete -Requires some degree of cooperation
-According to a 2008 survey only 9 of all Australian units use any sort of scale like this
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8
Alex Yartsev 1542011
Diagnosis of ICU delirium - Diagnosis of exclusion- Imaging excludes structural causes of encephalopathy- Bloods exclude many of the metabolic causes- What remains is excluded with history- Easier said than done
-Address the cause
-ldquoMultifactorialrdquo is a safe guess
The CAM-ICU
Just calm down Sir You are in hospital-MANAGEMENT OF ICU DELIRIUM
-Preventative vs reactive-Non-pharmacological vs pharmacological
Prevention of ICU delirium - Sedation Holidays
-2000 study by Kress landmark paper 128 pts -length of stay reduced from 99 to 66 days-9 vs 16 pts needed delirium workup-According to a 2008 survey only 30 of Australian units use sedation holidays
- Frequent reproducible assessment for pain and delirium-Jacobi et a (2002 multidisciplinary task force) -recommend the use of a validated agitationsedation measurement tool -eg Richmond Agitation-Sedation Scale
- Quiet environment thus good sleep - Music thus reduced anxiety improved relaxationKress JP Pohlman AS OConner MF et al Daily interruption of sedation infusions in critically ill patients undergoing mechanical ventilation N Engl J Med 2000 342
1471ndash7Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Freedman NS et al Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit Am J Resp Crit Care Med 1999159 1155ndash1162Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8Chlan L Effectiveness of a music therapy intervention on relaxation and anxiety for patients receiving ventilatory assistance Heart Lung 199827169ndash176
Pharmacological Arsenal
How shall I most effectively drug Mr X-Jacobi et al (2002) recommends Haloperidol (level C data small studies and case report series)
-Cochrane library agrees to some extent
Lonergan etal (2007) haloperidol is better than placebo buthellip - no better then olanzapine at low doses- and with more side effects at high dosesErgo use olanzapine where possible
Lonergan etal (2009) ndash no evidence to support benzos in delirium unless alcohol withdrawal is the cause
-Everyone agrees monitor QTc (level B evidence)
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Lonergan etal Benzodiazepines for delirium Cochrane Database of Systematic Reviews 2009 Issue 4Lonergan E Britton AM Luxenberg J Antipsychotics for delirium Cochrane Database of Systematic Reviews 2007 Issue 2Milbrandt etal Haloperidol use is associated with lower hospital mortality in mechanically ventilated patients Crit Care Med 2005 Jan33(1)226-9 discussion 263-5
How shall I adjust Mr Xrsquos sedation cocktailKeeping in mind the goal is to wean him off the ventilator
-Unless he is withdrawing from alcohol change midazolam to propofol
-ADD DEXMEDETOMIDINE
-Dex vs propofol Ruokonen et al (2009) 87 pts adding Dex has no effect on length of stay but decreases length of
ventilation
-Dex vs Midazolam Riker et al (2009) 375 ptsprevalence of delirium 54(dex) vs 76 (midaz) also faster extubation
- CORRECT MAGNESIUM- target range 10-20 in addition to remi + midaz 63 pts 2009 RCT by Esen
-Of the delirious pts the magnesium group had fewer days of delirium (55 vs 89) and consumed less sedatives
Mirski et al Cognitive improvement during continuous sedation in critically ill awake and responsive patients The Acute Neurological ICU Sedation Trial (ANIST) Intensive Care Medicine 2010 vol 36 issue 9 1505-1513Ruokonen et alDexmedetomidine versus propofolmidazolam for long-term sedation during mechanical ventilation Intensive Care Medicine 2009 vol 35 issue 2 282-90Riker RR et al Dexmedetomidine vs midazolam for sedation of critically ill patients a randomized trial JAMA the journal of the American Medical Association 2009 Feb 301 issue 5 Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Esen F et al Effect of magnesium on the incidence of delirium occurrence in the ICU Critical Care 2009 vol 13 supp 1P412
When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please
Assessment of delirium in the ICU-Is Mr X actually delirious
-Jacobi etal (2002) recommends the use of the Confusion Assessment Method in the ICU (CAM-ICU)
-Apparently 2 minutes to complete -Requires some degree of cooperation
-According to a 2008 survey only 9 of all Australian units use any sort of scale like this
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8
Alex Yartsev 1542011
Diagnosis of ICU delirium - Diagnosis of exclusion- Imaging excludes structural causes of encephalopathy- Bloods exclude many of the metabolic causes- What remains is excluded with history- Easier said than done
-Address the cause
-ldquoMultifactorialrdquo is a safe guess
The CAM-ICU
Just calm down Sir You are in hospital-MANAGEMENT OF ICU DELIRIUM
-Preventative vs reactive-Non-pharmacological vs pharmacological
Prevention of ICU delirium - Sedation Holidays
-2000 study by Kress landmark paper 128 pts -length of stay reduced from 99 to 66 days-9 vs 16 pts needed delirium workup-According to a 2008 survey only 30 of Australian units use sedation holidays
- Frequent reproducible assessment for pain and delirium-Jacobi et a (2002 multidisciplinary task force) -recommend the use of a validated agitationsedation measurement tool -eg Richmond Agitation-Sedation Scale
- Quiet environment thus good sleep - Music thus reduced anxiety improved relaxationKress JP Pohlman AS OConner MF et al Daily interruption of sedation infusions in critically ill patients undergoing mechanical ventilation N Engl J Med 2000 342
1471ndash7Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Freedman NS et al Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit Am J Resp Crit Care Med 1999159 1155ndash1162Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8Chlan L Effectiveness of a music therapy intervention on relaxation and anxiety for patients receiving ventilatory assistance Heart Lung 199827169ndash176
Pharmacological Arsenal
How shall I most effectively drug Mr X-Jacobi et al (2002) recommends Haloperidol (level C data small studies and case report series)
-Cochrane library agrees to some extent
Lonergan etal (2007) haloperidol is better than placebo buthellip - no better then olanzapine at low doses- and with more side effects at high dosesErgo use olanzapine where possible
Lonergan etal (2009) ndash no evidence to support benzos in delirium unless alcohol withdrawal is the cause
-Everyone agrees monitor QTc (level B evidence)
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Lonergan etal Benzodiazepines for delirium Cochrane Database of Systematic Reviews 2009 Issue 4Lonergan E Britton AM Luxenberg J Antipsychotics for delirium Cochrane Database of Systematic Reviews 2007 Issue 2Milbrandt etal Haloperidol use is associated with lower hospital mortality in mechanically ventilated patients Crit Care Med 2005 Jan33(1)226-9 discussion 263-5
How shall I adjust Mr Xrsquos sedation cocktailKeeping in mind the goal is to wean him off the ventilator
-Unless he is withdrawing from alcohol change midazolam to propofol
-ADD DEXMEDETOMIDINE
-Dex vs propofol Ruokonen et al (2009) 87 pts adding Dex has no effect on length of stay but decreases length of
ventilation
-Dex vs Midazolam Riker et al (2009) 375 ptsprevalence of delirium 54(dex) vs 76 (midaz) also faster extubation
- CORRECT MAGNESIUM- target range 10-20 in addition to remi + midaz 63 pts 2009 RCT by Esen
-Of the delirious pts the magnesium group had fewer days of delirium (55 vs 89) and consumed less sedatives
Mirski et al Cognitive improvement during continuous sedation in critically ill awake and responsive patients The Acute Neurological ICU Sedation Trial (ANIST) Intensive Care Medicine 2010 vol 36 issue 9 1505-1513Ruokonen et alDexmedetomidine versus propofolmidazolam for long-term sedation during mechanical ventilation Intensive Care Medicine 2009 vol 35 issue 2 282-90Riker RR et al Dexmedetomidine vs midazolam for sedation of critically ill patients a randomized trial JAMA the journal of the American Medical Association 2009 Feb 301 issue 5 Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Esen F et al Effect of magnesium on the incidence of delirium occurrence in the ICU Critical Care 2009 vol 13 supp 1P412
When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please

Alex Yartsev 1542011
Diagnosis of ICU delirium - Diagnosis of exclusion- Imaging excludes structural causes of encephalopathy- Bloods exclude many of the metabolic causes- What remains is excluded with history- Easier said than done
-Address the cause
-ldquoMultifactorialrdquo is a safe guess
The CAM-ICU
Just calm down Sir You are in hospital-MANAGEMENT OF ICU DELIRIUM
-Preventative vs reactive-Non-pharmacological vs pharmacological
Prevention of ICU delirium - Sedation Holidays
-2000 study by Kress landmark paper 128 pts -length of stay reduced from 99 to 66 days-9 vs 16 pts needed delirium workup-According to a 2008 survey only 30 of Australian units use sedation holidays
- Frequent reproducible assessment for pain and delirium-Jacobi et a (2002 multidisciplinary task force) -recommend the use of a validated agitationsedation measurement tool -eg Richmond Agitation-Sedation Scale
- Quiet environment thus good sleep - Music thus reduced anxiety improved relaxationKress JP Pohlman AS OConner MF et al Daily interruption of sedation infusions in critically ill patients undergoing mechanical ventilation N Engl J Med 2000 342
1471ndash7Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Freedman NS et al Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit Am J Resp Crit Care Med 1999159 1155ndash1162Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8Chlan L Effectiveness of a music therapy intervention on relaxation and anxiety for patients receiving ventilatory assistance Heart Lung 199827169ndash176
Pharmacological Arsenal
How shall I most effectively drug Mr X-Jacobi et al (2002) recommends Haloperidol (level C data small studies and case report series)
-Cochrane library agrees to some extent
Lonergan etal (2007) haloperidol is better than placebo buthellip - no better then olanzapine at low doses- and with more side effects at high dosesErgo use olanzapine where possible
Lonergan etal (2009) ndash no evidence to support benzos in delirium unless alcohol withdrawal is the cause
-Everyone agrees monitor QTc (level B evidence)
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Lonergan etal Benzodiazepines for delirium Cochrane Database of Systematic Reviews 2009 Issue 4Lonergan E Britton AM Luxenberg J Antipsychotics for delirium Cochrane Database of Systematic Reviews 2007 Issue 2Milbrandt etal Haloperidol use is associated with lower hospital mortality in mechanically ventilated patients Crit Care Med 2005 Jan33(1)226-9 discussion 263-5
How shall I adjust Mr Xrsquos sedation cocktailKeeping in mind the goal is to wean him off the ventilator
-Unless he is withdrawing from alcohol change midazolam to propofol
-ADD DEXMEDETOMIDINE
-Dex vs propofol Ruokonen et al (2009) 87 pts adding Dex has no effect on length of stay but decreases length of
ventilation
-Dex vs Midazolam Riker et al (2009) 375 ptsprevalence of delirium 54(dex) vs 76 (midaz) also faster extubation
- CORRECT MAGNESIUM- target range 10-20 in addition to remi + midaz 63 pts 2009 RCT by Esen
-Of the delirious pts the magnesium group had fewer days of delirium (55 vs 89) and consumed less sedatives
Mirski et al Cognitive improvement during continuous sedation in critically ill awake and responsive patients The Acute Neurological ICU Sedation Trial (ANIST) Intensive Care Medicine 2010 vol 36 issue 9 1505-1513Ruokonen et alDexmedetomidine versus propofolmidazolam for long-term sedation during mechanical ventilation Intensive Care Medicine 2009 vol 35 issue 2 282-90Riker RR et al Dexmedetomidine vs midazolam for sedation of critically ill patients a randomized trial JAMA the journal of the American Medical Association 2009 Feb 301 issue 5 Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Esen F et al Effect of magnesium on the incidence of delirium occurrence in the ICU Critical Care 2009 vol 13 supp 1P412
When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please
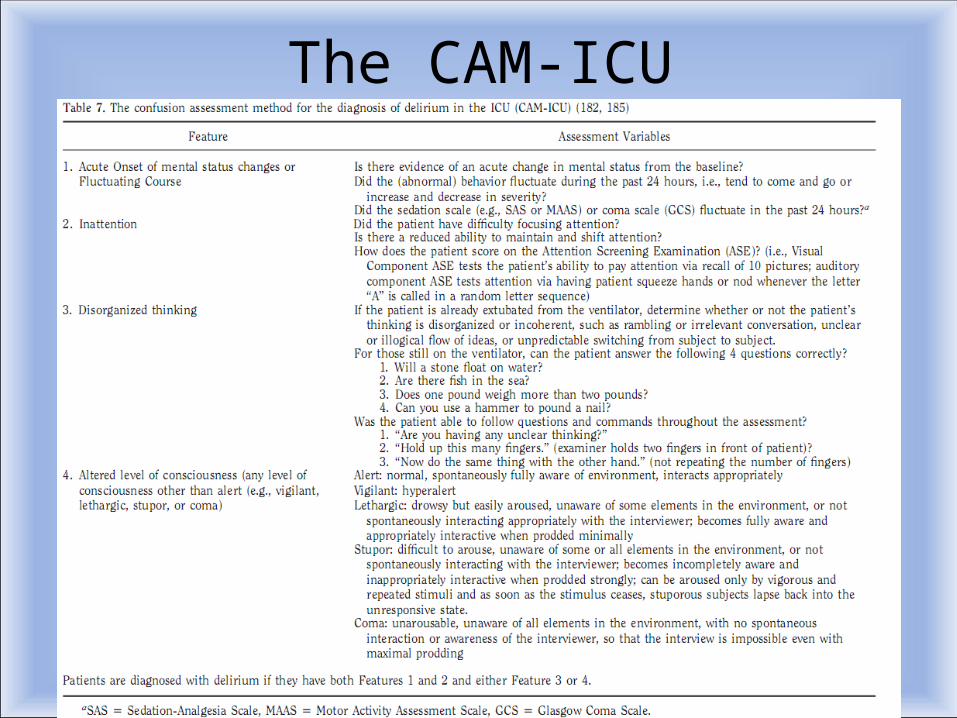
The CAM-ICU
Just calm down Sir You are in hospital-MANAGEMENT OF ICU DELIRIUM
-Preventative vs reactive-Non-pharmacological vs pharmacological
Prevention of ICU delirium - Sedation Holidays
-2000 study by Kress landmark paper 128 pts -length of stay reduced from 99 to 66 days-9 vs 16 pts needed delirium workup-According to a 2008 survey only 30 of Australian units use sedation holidays
- Frequent reproducible assessment for pain and delirium-Jacobi et a (2002 multidisciplinary task force) -recommend the use of a validated agitationsedation measurement tool -eg Richmond Agitation-Sedation Scale
- Quiet environment thus good sleep - Music thus reduced anxiety improved relaxationKress JP Pohlman AS OConner MF et al Daily interruption of sedation infusions in critically ill patients undergoing mechanical ventilation N Engl J Med 2000 342
1471ndash7Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Freedman NS et al Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit Am J Resp Crit Care Med 1999159 1155ndash1162Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8Chlan L Effectiveness of a music therapy intervention on relaxation and anxiety for patients receiving ventilatory assistance Heart Lung 199827169ndash176
Pharmacological Arsenal
How shall I most effectively drug Mr X-Jacobi et al (2002) recommends Haloperidol (level C data small studies and case report series)
-Cochrane library agrees to some extent
Lonergan etal (2007) haloperidol is better than placebo buthellip - no better then olanzapine at low doses- and with more side effects at high dosesErgo use olanzapine where possible
Lonergan etal (2009) ndash no evidence to support benzos in delirium unless alcohol withdrawal is the cause
-Everyone agrees monitor QTc (level B evidence)
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Lonergan etal Benzodiazepines for delirium Cochrane Database of Systematic Reviews 2009 Issue 4Lonergan E Britton AM Luxenberg J Antipsychotics for delirium Cochrane Database of Systematic Reviews 2007 Issue 2Milbrandt etal Haloperidol use is associated with lower hospital mortality in mechanically ventilated patients Crit Care Med 2005 Jan33(1)226-9 discussion 263-5
How shall I adjust Mr Xrsquos sedation cocktailKeeping in mind the goal is to wean him off the ventilator
-Unless he is withdrawing from alcohol change midazolam to propofol
-ADD DEXMEDETOMIDINE
-Dex vs propofol Ruokonen et al (2009) 87 pts adding Dex has no effect on length of stay but decreases length of
ventilation
-Dex vs Midazolam Riker et al (2009) 375 ptsprevalence of delirium 54(dex) vs 76 (midaz) also faster extubation
- CORRECT MAGNESIUM- target range 10-20 in addition to remi + midaz 63 pts 2009 RCT by Esen
-Of the delirious pts the magnesium group had fewer days of delirium (55 vs 89) and consumed less sedatives
Mirski et al Cognitive improvement during continuous sedation in critically ill awake and responsive patients The Acute Neurological ICU Sedation Trial (ANIST) Intensive Care Medicine 2010 vol 36 issue 9 1505-1513Ruokonen et alDexmedetomidine versus propofolmidazolam for long-term sedation during mechanical ventilation Intensive Care Medicine 2009 vol 35 issue 2 282-90Riker RR et al Dexmedetomidine vs midazolam for sedation of critically ill patients a randomized trial JAMA the journal of the American Medical Association 2009 Feb 301 issue 5 Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Esen F et al Effect of magnesium on the incidence of delirium occurrence in the ICU Critical Care 2009 vol 13 supp 1P412
When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please

Just calm down Sir You are in hospital-MANAGEMENT OF ICU DELIRIUM
-Preventative vs reactive-Non-pharmacological vs pharmacological
Prevention of ICU delirium - Sedation Holidays
-2000 study by Kress landmark paper 128 pts -length of stay reduced from 99 to 66 days-9 vs 16 pts needed delirium workup-According to a 2008 survey only 30 of Australian units use sedation holidays
- Frequent reproducible assessment for pain and delirium-Jacobi et a (2002 multidisciplinary task force) -recommend the use of a validated agitationsedation measurement tool -eg Richmond Agitation-Sedation Scale
- Quiet environment thus good sleep - Music thus reduced anxiety improved relaxationKress JP Pohlman AS OConner MF et al Daily interruption of sedation infusions in critically ill patients undergoing mechanical ventilation N Engl J Med 2000 342
1471ndash7Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Freedman NS et al Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit Am J Resp Crit Care Med 1999159 1155ndash1162Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8Chlan L Effectiveness of a music therapy intervention on relaxation and anxiety for patients receiving ventilatory assistance Heart Lung 199827169ndash176
Pharmacological Arsenal
How shall I most effectively drug Mr X-Jacobi et al (2002) recommends Haloperidol (level C data small studies and case report series)
-Cochrane library agrees to some extent
Lonergan etal (2007) haloperidol is better than placebo buthellip - no better then olanzapine at low doses- and with more side effects at high dosesErgo use olanzapine where possible
Lonergan etal (2009) ndash no evidence to support benzos in delirium unless alcohol withdrawal is the cause
-Everyone agrees monitor QTc (level B evidence)
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Lonergan etal Benzodiazepines for delirium Cochrane Database of Systematic Reviews 2009 Issue 4Lonergan E Britton AM Luxenberg J Antipsychotics for delirium Cochrane Database of Systematic Reviews 2007 Issue 2Milbrandt etal Haloperidol use is associated with lower hospital mortality in mechanically ventilated patients Crit Care Med 2005 Jan33(1)226-9 discussion 263-5
How shall I adjust Mr Xrsquos sedation cocktailKeeping in mind the goal is to wean him off the ventilator
-Unless he is withdrawing from alcohol change midazolam to propofol
-ADD DEXMEDETOMIDINE
-Dex vs propofol Ruokonen et al (2009) 87 pts adding Dex has no effect on length of stay but decreases length of
ventilation
-Dex vs Midazolam Riker et al (2009) 375 ptsprevalence of delirium 54(dex) vs 76 (midaz) also faster extubation
- CORRECT MAGNESIUM- target range 10-20 in addition to remi + midaz 63 pts 2009 RCT by Esen
-Of the delirious pts the magnesium group had fewer days of delirium (55 vs 89) and consumed less sedatives
Mirski et al Cognitive improvement during continuous sedation in critically ill awake and responsive patients The Acute Neurological ICU Sedation Trial (ANIST) Intensive Care Medicine 2010 vol 36 issue 9 1505-1513Ruokonen et alDexmedetomidine versus propofolmidazolam for long-term sedation during mechanical ventilation Intensive Care Medicine 2009 vol 35 issue 2 282-90Riker RR et al Dexmedetomidine vs midazolam for sedation of critically ill patients a randomized trial JAMA the journal of the American Medical Association 2009 Feb 301 issue 5 Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Esen F et al Effect of magnesium on the incidence of delirium occurrence in the ICU Critical Care 2009 vol 13 supp 1P412
When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please

Prevention of ICU delirium - Sedation Holidays
-2000 study by Kress landmark paper 128 pts -length of stay reduced from 99 to 66 days-9 vs 16 pts needed delirium workup-According to a 2008 survey only 30 of Australian units use sedation holidays
- Frequent reproducible assessment for pain and delirium-Jacobi et a (2002 multidisciplinary task force) -recommend the use of a validated agitationsedation measurement tool -eg Richmond Agitation-Sedation Scale
- Quiet environment thus good sleep - Music thus reduced anxiety improved relaxationKress JP Pohlman AS OConner MF et al Daily interruption of sedation infusions in critically ill patients undergoing mechanical ventilation N Engl J Med 2000 342
1471ndash7Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Freedman NS et al Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit Am J Resp Crit Care Med 1999159 1155ndash1162Shehabi Y Sedation and delirium in the intensive care unit an Australian and New Zealand perspective Botha JA Boyle MS Ernest D Freebairn RC Jenkins IR Roberts BL Seppelt IM Anaesth Intensive Care 2008 Jul36(4)570-8Chlan L Effectiveness of a music therapy intervention on relaxation and anxiety for patients receiving ventilatory assistance Heart Lung 199827169ndash176
Pharmacological Arsenal
How shall I most effectively drug Mr X-Jacobi et al (2002) recommends Haloperidol (level C data small studies and case report series)
-Cochrane library agrees to some extent
Lonergan etal (2007) haloperidol is better than placebo buthellip - no better then olanzapine at low doses- and with more side effects at high dosesErgo use olanzapine where possible
Lonergan etal (2009) ndash no evidence to support benzos in delirium unless alcohol withdrawal is the cause
-Everyone agrees monitor QTc (level B evidence)
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Lonergan etal Benzodiazepines for delirium Cochrane Database of Systematic Reviews 2009 Issue 4Lonergan E Britton AM Luxenberg J Antipsychotics for delirium Cochrane Database of Systematic Reviews 2007 Issue 2Milbrandt etal Haloperidol use is associated with lower hospital mortality in mechanically ventilated patients Crit Care Med 2005 Jan33(1)226-9 discussion 263-5
How shall I adjust Mr Xrsquos sedation cocktailKeeping in mind the goal is to wean him off the ventilator
-Unless he is withdrawing from alcohol change midazolam to propofol
-ADD DEXMEDETOMIDINE
-Dex vs propofol Ruokonen et al (2009) 87 pts adding Dex has no effect on length of stay but decreases length of
ventilation
-Dex vs Midazolam Riker et al (2009) 375 ptsprevalence of delirium 54(dex) vs 76 (midaz) also faster extubation
- CORRECT MAGNESIUM- target range 10-20 in addition to remi + midaz 63 pts 2009 RCT by Esen
-Of the delirious pts the magnesium group had fewer days of delirium (55 vs 89) and consumed less sedatives
Mirski et al Cognitive improvement during continuous sedation in critically ill awake and responsive patients The Acute Neurological ICU Sedation Trial (ANIST) Intensive Care Medicine 2010 vol 36 issue 9 1505-1513Ruokonen et alDexmedetomidine versus propofolmidazolam for long-term sedation during mechanical ventilation Intensive Care Medicine 2009 vol 35 issue 2 282-90Riker RR et al Dexmedetomidine vs midazolam for sedation of critically ill patients a randomized trial JAMA the journal of the American Medical Association 2009 Feb 301 issue 5 Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Esen F et al Effect of magnesium on the incidence of delirium occurrence in the ICU Critical Care 2009 vol 13 supp 1P412
When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please

Pharmacological Arsenal
How shall I most effectively drug Mr X-Jacobi et al (2002) recommends Haloperidol (level C data small studies and case report series)
-Cochrane library agrees to some extent
Lonergan etal (2007) haloperidol is better than placebo buthellip - no better then olanzapine at low doses- and with more side effects at high dosesErgo use olanzapine where possible
Lonergan etal (2009) ndash no evidence to support benzos in delirium unless alcohol withdrawal is the cause
-Everyone agrees monitor QTc (level B evidence)
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Lonergan etal Benzodiazepines for delirium Cochrane Database of Systematic Reviews 2009 Issue 4Lonergan E Britton AM Luxenberg J Antipsychotics for delirium Cochrane Database of Systematic Reviews 2007 Issue 2Milbrandt etal Haloperidol use is associated with lower hospital mortality in mechanically ventilated patients Crit Care Med 2005 Jan33(1)226-9 discussion 263-5
How shall I adjust Mr Xrsquos sedation cocktailKeeping in mind the goal is to wean him off the ventilator
-Unless he is withdrawing from alcohol change midazolam to propofol
-ADD DEXMEDETOMIDINE
-Dex vs propofol Ruokonen et al (2009) 87 pts adding Dex has no effect on length of stay but decreases length of
ventilation
-Dex vs Midazolam Riker et al (2009) 375 ptsprevalence of delirium 54(dex) vs 76 (midaz) also faster extubation
- CORRECT MAGNESIUM- target range 10-20 in addition to remi + midaz 63 pts 2009 RCT by Esen
-Of the delirious pts the magnesium group had fewer days of delirium (55 vs 89) and consumed less sedatives
Mirski et al Cognitive improvement during continuous sedation in critically ill awake and responsive patients The Acute Neurological ICU Sedation Trial (ANIST) Intensive Care Medicine 2010 vol 36 issue 9 1505-1513Ruokonen et alDexmedetomidine versus propofolmidazolam for long-term sedation during mechanical ventilation Intensive Care Medicine 2009 vol 35 issue 2 282-90Riker RR et al Dexmedetomidine vs midazolam for sedation of critically ill patients a randomized trial JAMA the journal of the American Medical Association 2009 Feb 301 issue 5 Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Esen F et al Effect of magnesium on the incidence of delirium occurrence in the ICU Critical Care 2009 vol 13 supp 1P412
When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please

How shall I most effectively drug Mr X-Jacobi et al (2002) recommends Haloperidol (level C data small studies and case report series)
-Cochrane library agrees to some extent
Lonergan etal (2007) haloperidol is better than placebo buthellip - no better then olanzapine at low doses- and with more side effects at high dosesErgo use olanzapine where possible
Lonergan etal (2009) ndash no evidence to support benzos in delirium unless alcohol withdrawal is the cause
-Everyone agrees monitor QTc (level B evidence)
Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Lonergan etal Benzodiazepines for delirium Cochrane Database of Systematic Reviews 2009 Issue 4Lonergan E Britton AM Luxenberg J Antipsychotics for delirium Cochrane Database of Systematic Reviews 2007 Issue 2Milbrandt etal Haloperidol use is associated with lower hospital mortality in mechanically ventilated patients Crit Care Med 2005 Jan33(1)226-9 discussion 263-5
How shall I adjust Mr Xrsquos sedation cocktailKeeping in mind the goal is to wean him off the ventilator
-Unless he is withdrawing from alcohol change midazolam to propofol
-ADD DEXMEDETOMIDINE
-Dex vs propofol Ruokonen et al (2009) 87 pts adding Dex has no effect on length of stay but decreases length of
ventilation
-Dex vs Midazolam Riker et al (2009) 375 ptsprevalence of delirium 54(dex) vs 76 (midaz) also faster extubation
- CORRECT MAGNESIUM- target range 10-20 in addition to remi + midaz 63 pts 2009 RCT by Esen
-Of the delirious pts the magnesium group had fewer days of delirium (55 vs 89) and consumed less sedatives
Mirski et al Cognitive improvement during continuous sedation in critically ill awake and responsive patients The Acute Neurological ICU Sedation Trial (ANIST) Intensive Care Medicine 2010 vol 36 issue 9 1505-1513Ruokonen et alDexmedetomidine versus propofolmidazolam for long-term sedation during mechanical ventilation Intensive Care Medicine 2009 vol 35 issue 2 282-90Riker RR et al Dexmedetomidine vs midazolam for sedation of critically ill patients a randomized trial JAMA the journal of the American Medical Association 2009 Feb 301 issue 5 Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Esen F et al Effect of magnesium on the incidence of delirium occurrence in the ICU Critical Care 2009 vol 13 supp 1P412
When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please

How shall I adjust Mr Xrsquos sedation cocktailKeeping in mind the goal is to wean him off the ventilator
-Unless he is withdrawing from alcohol change midazolam to propofol
-ADD DEXMEDETOMIDINE
-Dex vs propofol Ruokonen et al (2009) 87 pts adding Dex has no effect on length of stay but decreases length of
ventilation
-Dex vs Midazolam Riker et al (2009) 375 ptsprevalence of delirium 54(dex) vs 76 (midaz) also faster extubation
- CORRECT MAGNESIUM- target range 10-20 in addition to remi + midaz 63 pts 2009 RCT by Esen
-Of the delirious pts the magnesium group had fewer days of delirium (55 vs 89) and consumed less sedatives
Mirski et al Cognitive improvement during continuous sedation in critically ill awake and responsive patients The Acute Neurological ICU Sedation Trial (ANIST) Intensive Care Medicine 2010 vol 36 issue 9 1505-1513Ruokonen et alDexmedetomidine versus propofolmidazolam for long-term sedation during mechanical ventilation Intensive Care Medicine 2009 vol 35 issue 2 282-90Riker RR et al Dexmedetomidine vs midazolam for sedation of critically ill patients a randomized trial JAMA the journal of the American Medical Association 2009 Feb 301 issue 5 Jacobi J Fraser GL Coursin DB Riker RR Fontaine D Wittbrodt ET Chalfin DB Masica MF Bjerke HS Coplin WM Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adultCrit Care Med 200230119ndash141Esen F et al Effect of magnesium on the incidence of delirium occurrence in the ICU Critical Care 2009 vol 13 supp 1P412
When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please

When is it OK to restrain Mr X
-NOT IDEAL-Increases the risk of PTSD tissue injury pressure areas Inhumane
-Consensus use the least restrictive therapy available Goal is to minimize harm from discontinuation of life-supporting therapies
-HOWEVER-Tominaga etal (1995) ndash no restraints = significant increase in self-extubations-Carrion et al (2000) ndash hand restraints = significantly reduced self-extubations
LY Chang KWK Wanghellip Influence of physical restraint on unplanned extubation of adult intensive care patients a case-control study - American Journal of Critical Care 2008 ndash AACN 200817 408-415 George J Annas JD MPH The Last Resort mdash The Use of Physical Restraints in Medical Emergencies N Engl J Med 1999 3411408-141Jones C Backman C Capuzzo M Flaatten H Rylander C Griffiths RD (2007) Precipitants of post-traumatic stress disorder following intensive care a hypothesis generating study of diversity in care Intensive Care Med33978-85 Macciolli etal Clinical practice guidelines for the maintenance of patient physical safety in the intensive care unit Use of restraining therapiesmdashAmerican College of Critical Care Medicine Task Force 2001ndash2002 Crit Care Med 2003 Vol 31 No 11Carrion MI Ayuso D Marcos M et al Accidental removal of endotracheal and nasogastric tubes and intravascular catheters Crit Care Med 2000 2863ndash 66Tominaga GT Rduzwick H Scannell G et al Decreasing unplanned extubations in the surgical intensive care unit Am J Surg 1995 170586 ndash590 Girard et al Risk factors for post-traumatic stress disorder symptoms following critical illness requiring mechanical ventilation a prospective cohort study Crit Care 200711(1)R28
No questions please
No questions please