Embed Size (px)
Citation preview
1
Yorkshire and Humber Children and Young People’s Cancer Network
Constitution, Membership and Terms of Reference Yorkshire and Humber Children and Young People’s Cancer Network Group Constitution - Agreement Cover Sheet Authors: Martin Elliott & Rachel Hollis, Leeds Teaching Hospital Trust Review Date: February 2019 The Constitution has been revised and agreed by:
Position Chair of the Children’s Cancer Network
Name Martin Elliott
Organisation Leeds Teaching Hospitals Trust
Date Agreed 17/02/2017
Position
Name
Organisation Strategic Clinical Network/Cancer Alliance lead to be confirmed
Date Agreed
Position Head of Services for Chemotherapy within Children’s Cancer Network
Name Sue Picton
Organisation Leeds Teaching Hospitals Trust
Date Agreed 17/02/2017
Position Head of Services for Radiotherapy within Children’s Cancer Network
Name Baz (Hazel) Rodgers
Organisation Leeds Teaching Hospitals Trust
Date Agreed 21/02/2017
Position Lead for Late Effects MDT at Leeds Teaching Hospitals
Name Michelle Kwok-Williams
Organisation Leeds Teaching Hospitals Trust
Date Agreed 21/02/2017
Position Vice Chair and POSCU Lead Clinician
Name Gill Sharpe
Organisation Calderdale & Huddersfield NHS Foundation Trust
Date Agreed 17/02/2017
2
This revised Constitution was agreed by the YHCYPCN Coordinating Group on 22/02/2017
Yorkshire and Humber Children and Young People’s Cancer Network
1. Network Configuration of Teams and Scope of Service
1.1 Scope of Service The Guidance on Improving Outcomes in Children and Young People with Cancer (CYPIOG) and Children’s Cancer Measures (v4 2014) set out a framework to provide leadership and co-ordination of children’s cancer services through a Children’s Cancer Network (CCN). The term CCN refers to the whole collection of children’s cancer services in the children’s cancer network. The Yorkshire and the Humber Strategic Clinical Network (SCN) is unique, in that it has two Children’s Cancer Networks, reflecting the catchment areas served by two Principal Treatment Centres (PTCs), in Leeds and Sheffield. This constitution refers only to the Yorkshire and Humber Children and Young People’s Cancer Network (YHCYPCN). Continuing changes to the Strategic Clinical Networks (and the emergence of the Cancer Alliances are likely in the future to impact on this constitution. The group has continued to meet throughout the period from the closure of the Cancer Networks and the development of the SCN, and has maintained contact with SCN, who are aware of work plans and activities of the group. The input from the SCN, and from commissioners, to the work of the group has been limited by the changing organisational and commissioning context. The CCN encompasses West and North Yorkshire, and that part of the Humber which falls into the catchment area of the PTC at Leeds. It is provider led, with its focus on the Principal Treatment Centre in Leeds and has representation from across the network. The YHCYPCN is made up of members from the PTC at Leeds Teaching Hospitals Trust, those hospital trusts that provide shared care services, and those community and hospital trusts and organizations who provide community services for children and young people with cancer. 1.2 The configuration of MDTs within the PTC and Shared Care configuration
There is one designated PTC for children aged 0-15 (up to their 16th birthday) provided from the
Children’s Hospital at Leeds General Infirmary, Leeds Teaching Hospitals NHS Trust. The service is closely integrated with the Principal Treatment Centre for Teenagers and Young Adults. There are three paediatric diagnostic and treatment planning MDTs, one covering solid tumours, one for haematological malignancies and the other covering brain and CNS tumours.
There is one late effects MDT provided between Leeds General Infirmary, and St James’s Hospital in the Leeds Teaching Hospitals NHS Trust which covers the full range of patients whose cancers were diagnosed between birth and their 25th birthday.
There are five hospitals providing shared care across YHCYPCN. All have identified as level 1 and host monthly MDTs. Calderdale hospital opts out of IV bolus chemotherapy (option 2) but is actively working towards full Level 1 status. Hull opts out of IV bolus chemotherapy (option 2). Airedale hospital opts out of chemotherapy services, and has recently developed its services to provide in-patient supportive care (Option 2). York and Scarborough have merged as one organisation (York Teaching Hospital NHS Trust), with Shared Care services across the 2 sites, under a single Lead Clinician. This is described in the Shared Care agreement.
If any POSCU is unable to provide medical cover required to provide the service safely patients are referred back to the PTC. This is described in the Shared Care agreement between the PTC and each individual POSCU. The template for this agreement is found at Appendix 1.
The model of service provision which has been developed and is supported across the network is in line with the underlying principle of the CYPIOG to provide ‘safe and effective services as locally as possible’.
3
This model provides a centralised cancer service at the PTC, with responsive local services in the POSCUs which meet the more generic needs of children, young people and their families. This model of shared care is based on close collaborative working relationships, fostered through the network, and is described in the shared care agreement between the PTC and each local POSCU. The agreement describes in detail the responsibilities, leadership and governance arrangements that support the delivery of shared care across YHCYPCN. The POSCU at Hull works in collaboration with the Community Children's Nursing Services in City Health Care Partnership Community Interest Company (CIC) to provide a range of services for children at home. This includes blood tests, central line care, and working with the Outreach team and other local services in the provision of palliative care. They also administer low dose Cytarabine chemotherapy to children at home. This is recognised in the Shared Care agreement between Leeds and Hull.
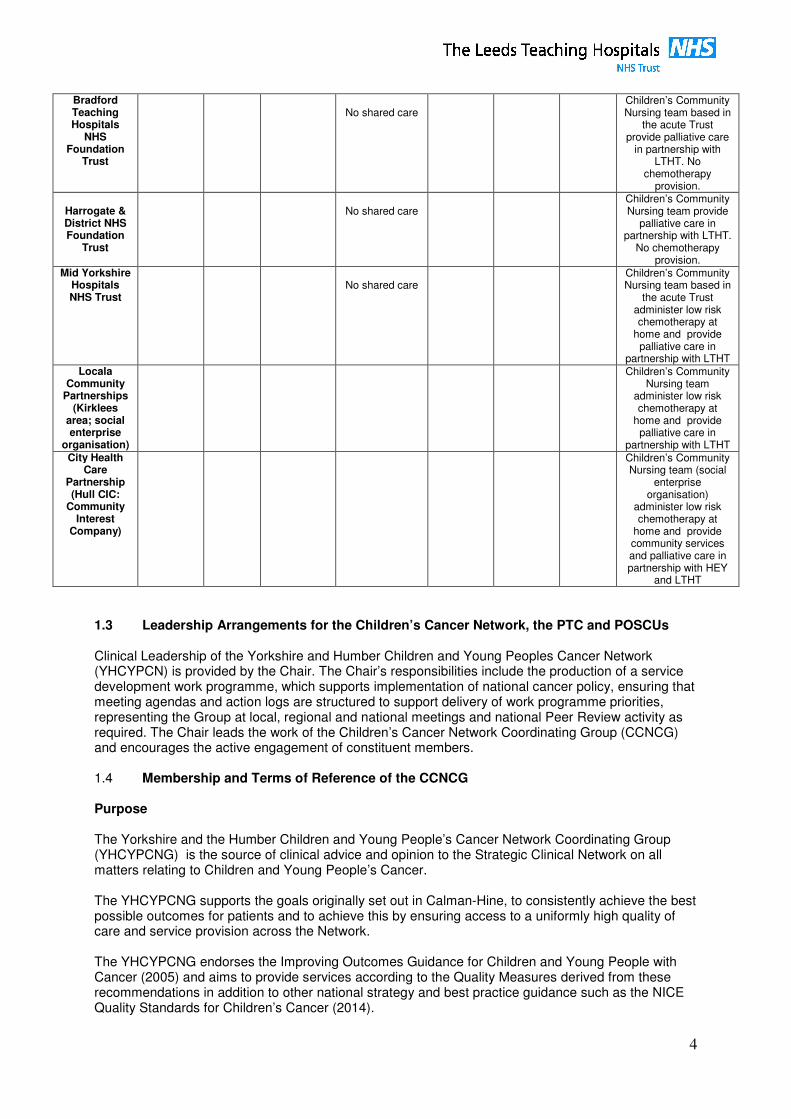
Bradford, Harrogate and Mid Yorkshire Foundation NHS Trusts do not provide shared care and children from these localities receive all in-patient care and support from the PTC in Leeds. Bradford Foundation NHS Trust is looking at the possibility of developing Level 1 Shared Care services in collaboration with the team at the PTC.
Children’s community nursing teams in these localities provide a range of services for children at home, working in liaison with the Children’s Cancer Outreach team at the PTC. This includes blood tests, central line care, and working with the Outreach team and other local services in the provision of palliative care. Children’s community nursing teams in Leeds, Wakefield and Kirklees administer low dose Cytarabine chemotherapy to children at home.
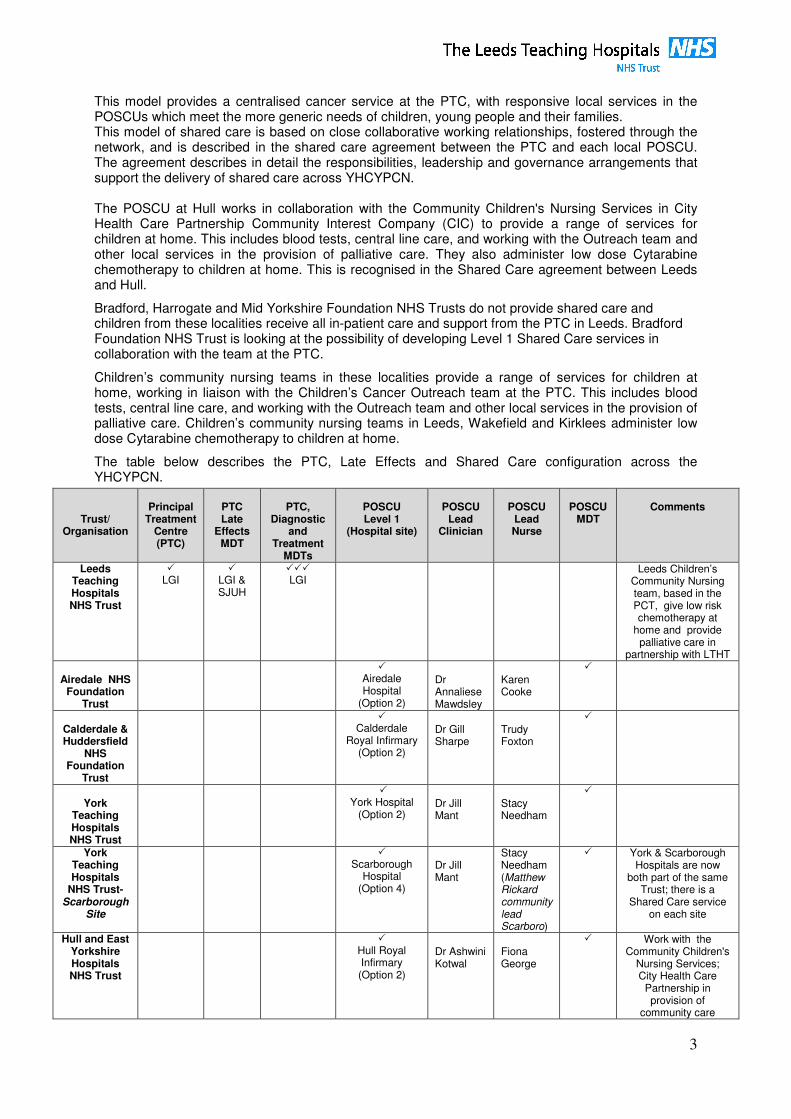
The table below describes the PTC, Late Effects and Shared Care configuration across the YHCYPCN.
Trust/ Organisation
Principal
Treatment Centre (PTC)
PTC Late
Effects MDT
PTC,
Diagnostic and
Treatment MDTs
POSCU Level 1
(Hospital site)
POSCU
Lead Clinician
POSCU
Lead Nurse
POSCU
MDT
Comments
Leeds Teaching Hospitals NHS Trust
� LGI
� LGI & SJUH
��� LGI
Leeds Children’s Community Nursing team, based in the PCT, give low risk chemotherapy at
home and provide palliative care in
partnership with LTHT
Airedale NHS Foundation
Trust
� Airedale Hospital
(Option 2)
Dr Annaliese Mawdsley
Karen Cooke
�
Calderdale & Huddersfield
NHS Foundation
Trust
� Calderdale
Royal Infirmary (Option 2)
Dr Gill Sharpe
Trudy Foxton
�
York
Teaching Hospitals NHS Trust
� York Hospital
(Option 2)
Dr Jill Mant
Stacy Needham
�
York Teaching Hospitals
NHS Trust- Scarborough
Site
� Scarborough
Hospital (Option 4)
Dr Jill Mant
Stacy Needham (Matthew Rickard community lead Scarboro)
�
York & Scarborough Hospitals are now
both part of the same Trust; there is a
Shared Care service on each site
Hull and East Yorkshire Hospitals NHS Trust
� Hull Royal Infirmary (Option 2)
Dr Ashwini Kotwal
Fiona George
�
Work with the Community Children's
Nursing Services; City Health Care
Partnership in provision of
community care
4
1.3 Leadership Arrangements for the Children’s Cancer Network, the PTC and POSCUs Clinical Leadership of the Yorkshire and Humber Children and Young Peoples Cancer Network (YHCYPCN) is provided by the Chair. The Chair’s responsibilities include the production of a service development work programme, which supports implementation of national cancer policy, ensuring that meeting agendas and action logs are structured to support delivery of work programme priorities, representing the Group at local, regional and national meetings and national Peer Review activity as required. The Chair leads the work of the Children’s Cancer Network Coordinating Group (CCNCG) and encourages the active engagement of constituent members. 1.4 Membership and Terms of Reference of the CCNCG
Purpose The Yorkshire and the Humber Children and Young People’s Cancer Network Coordinating Group (YHCYPCNG) is the source of clinical advice and opinion to the Strategic Clinical Network on all matters relating to Children and Young People’s Cancer. The YHCYPCNG supports the goals originally set out in Calman-Hine, to consistently achieve the best possible outcomes for patients and to achieve this by ensuring access to a uniformly high quality of care and service provision across the Network. The YHCYPCNG endorses the Improving Outcomes Guidance for Children and Young People with Cancer (2005) and aims to provide services according to the Quality Measures derived from these recommendations in addition to other national strategy and best practice guidance such as the NICE Quality Standards for Children’s Cancer (2014).
Bradford Teaching Hospitals
NHS Foundation
Trust
No shared care
Children’s Community Nursing team based in
the acute Trust provide palliative care
in partnership with LTHT. No
chemotherapy provision.
Harrogate & District NHS Foundation
Trust
No shared care
Children’s Community Nursing team provide
palliative care in partnership with LTHT.
No chemotherapy provision.
Mid Yorkshire Hospitals NHS Trust
No shared care
Children’s Community Nursing team based in
the acute Trust administer low risk chemotherapy at
home and provide palliative care in
partnership with LTHT Locala
Community Partnerships
(Kirklees area; social enterprise
organisation)
Children’s Community Nursing team
administer low risk chemotherapy at
home and provide palliative care in
partnership with LTHT City Health
Care Partnership (Hull CIC:
Community Interest
Company)
Children’s Community Nursing team (social
enterprise organisation)
administer low risk chemotherapy at
home and provide community services and palliative care in partnership with HEY
and LTHT
5
The YHCYPCNG endorses the Improving Outcomes Guidance for Children and Young People with cancer in providing ‘safe and effective care as close to home as possible’. The YHCYPCNG facilitates the collaboration of providers of services children with cancer to provide optimum and consistent care based on best clinical practice. It does this through the development of patient pathways and clinical guidelines. The YHCYPCNG works collaboratively with the Y&H Teenage and Young Adult Cancer Network Coordinating Group (TYACNCG). Membership The membership of the multidisciplinary group is open to all those across the network who care for children and young people with cancer, and includes the following:
• The Chair of the CCN (who is also the Chair of the Group)
• The Lead Clinician and Lead Nurse of the PTC
• A representative of the Teenage and Young Adult Cancer Network Coordinating Group
• The Lead Clinician and Lead Nurse from each Paediatric Oncology Shared Care Unit (POSCU).
• Airedale NHS Foundation Trust
• Calderdale and Huddersfield NHS Trust
• York Hospitals NHS Trust (York and Scarborough)
• Hull and East Yorkshire Hospitals NHS Trust
• Representatives from local Trusts in the CCN with children’s services which do not currently provide Shared Care services
• Bradford Teaching Hospitals NHS Foundation Trust
• Harrogate and District NHS Foundation Trust
• Mid Yorkshire Hospitals NHS Trust
• Representatives from Children’s Community Nursing teams/Primary Care Trusts within the network from localities which do not provide shared care
• User/carer representative
• In addition, the Team Leader for the Children’s Haematology and Oncology Outreach team at the PTC also has specific responsibility for users’ issues and information for patients and carers
• Representation from the cancer team at the Yorkshire and the Humber Strategic Clinical Network An ‘Executive Group’ has been formed from the wider membership in order to progress the work of the group more effectively. This group is made up of:
• The Chair and Vice Chair of the YHCYPCN
• PTC Lead Clinician
• PTC Lead Nurse
• POSCU Lead Clinician
• POSCU Lead Nurse
• User/carer representative, or individual with responsibility for user/carer issues There is a CYP Lead Nurses Group which functions as a sub-group of the Network, and is attended by the POSCU and Community Lead Nurses, the Lead Nurse and Clinical Educator of the PTC, the Paediatric Macmillan Nursing team, and representative(s) of the TYA Nurse Specialist team.
6
Chair and Vice chair The chair and vice chair roles are each two years duration. The vice chair will succeed to the chair. The vice chair will be nominated by members of the committee. If there are two people nominated, there will be a vote to decide who is elected to vice chair. Frequency of Meetings Full meetings of the whole network group are held twice a year. There is a shorter ‘business meeting’ of the whole group on the day of the Network Educational Update. The ‘Executive Group’ will attend the whole group meetings and will in addition meet twice a year to review and maintain the activities of the group. Work Programme and Annual Report The group produces an annual Work Programme in discussion with the Strategic Clinical Network. This work programme focuses on the following areas: Service development
1. To develop, review, agree and update referral and clinical guidelines. To audit their implementation as agreed by the group.
2. To develop recommendations for cross boundary integrated care pathways across primary,
secondary and tertiary care provision. 3. To advise on service provision for CYP with cancer to the Strategic Clinical Network and to
commissioners and to make recommendations for service improvement or development, including the implementation of appropriate Improving Outcomes Guidance and further national strategy and best practice documents.
4. To identify and address with the Strategic Clinical Network and commissioners any
inequalities in care and service provision. Service improvement and redesign
5. To stimulate and lead local service improvement initiatives for CYP cancer
Service quality monitoring and evaluation
6. To monitor progress on meeting national cancer measures and ensure action plans agreed following peer review are implemented.
7. To monitor the quality and effectiveness of CYP cancer services across the Network through
the review of outcome indicators and audits required or undertaken at Network/PTC/POSCU level.
8. To receive reports on performance, cancer waiting times and other indicators
9. To monitor the implications of national and regional issues affecting CYP cancer and develop
recommendations for cross network action.
10. To review patient feedback from the MDTs across the network, and actions taken in response to that feedback; to identify common themes and work together to improve patient experience
Workforce development
11. To promote education on CYP cancer across the Network and organise Network events.
12. To maintain an awareness of educational activities in adjacent cancer networks and nationally.
7
Research and Development
13. To agree a list of clinical trials of National Institute for Health Research portfolio and other ‘local’ trials and facilitate the means by which patients from across the Network may be entered. To review and update this list on an annual basis and to record the number of patients entered into trials from the diagnostic and treatment MDTs at the PTC.
14. To work collaboratively with the Yorkshire Cancer Research Network, in maintaining and
improving entry into clinical trials. The CCNCG will review its Work Programme each year, and produce an Annual Report. This report will be sent to the Strategic Clinical Network and the Local Area team who will send it on to local authorities, statutory and voluntary health care providers, and commissioners. Training and Education There is a network nurse’s training programme in oncology skills and chemotherapy administration which has been developed by the Network Lead Nurses group, and which also covers medical staff who are required to administer systemic intravenous chemotherapy. There is a 24 hour telephone advice service which is provided by the PTC in Leeds. The network agreed standard operating policy for this service sets out the level of training of those nurses who are the first line in providing this service, and is available on the SCN Website at: http://www.yhscn.nhs.uk/cancer/cancer-UsefulInformation/ChildrenandYoungPeople.php Chemotherapy – Leadership and Service Provision The chemotherapy service for the whole of the Children’s Cancer Network is directed by the Principal Treatment Centre in Leeds. It is coordinated by the multidisciplinary Leeds Children’s Chemotherapy Group (LCCG). All in-patient chemotherapy is given in Leeds, in line with the level of Shared Care being offered by the POSCUs with which it works. POSCU services currently administer only ‘low risk’ chemotherapy treatments which have been prescribed, made up and dispensed in Leeds. They are administered by nurses who have undergone the network agreed training programme. This is governed by a policy for Shared Care Chemotherapy Administration, which is currently under review. The Head of Chemotherapy Service for Paediatric Oncology and Haematology in Leeds is Dr Susan Picton, Consultant Paediatric Oncologist. There is a list of responsibilities of the Head of Chemotherapy Services, which has been agreed with the Lead Cancer Clinician of the Trust and can be found in the Operational Policy for the Principal Treatment Centre. The Lead Pharmacist for the Principal Treatment Centre in Leeds is Vicky Holden. There is a list of responsibilities of the Lead Pharmacist, agreed with the Lead Cancer Clinician of the Trust and this can again be found in the Operational Policy for the PTC. Each of the POSCU MDTs has an identified pharmacist who supports the service, and they have access to specialist advice from the designated specialist pharmacy team at the PTC. There is an agreed list of acceptable Regimens for use across the Children’s Cancer Network. This is reviewed and updated on an annual basis by the Leeds Children’s Chemotherapy Group (LCCG), chaired by Sue Picton PTC Lead Clinician and Chemotherapy Head of Service. It is agreed by the Executive Group of the YHCYPCN. It covers all agreed chemotherapy regimens, and specifies which may be delivered in a POSCU or in the community. It includes those low risk regimens or part of regimens which may be delivered by nurses in the community, or working in Level 1 POSCUs without a chemotherapy service, who are trained to the ‘low risk’ level set out in the network training policy. In exceptional circumstances a patient may need to receive specific therapy not on the accepted list of Regimens. This chemotherapy would only be given at the PTC, authorised by the responsible consultant and reviewed at the relevant MDT meeting. In the event that an unlisted Regimen is used
8
for management of patient, the PTC Lead Pharmacist will notify the LCCG, where it will be recorded which Regimen has been used and the indication. This is set out in more detail within the Operational Policy of the PTC and the Terms of Reference of the LCCG. The records of such use are reviewed annually by the Executive Group of the YHCYPCN. Co-ordination of Care/Patient Pathways The Group have developed the following high level pathways for the diagnosis and management of Children’s Cancer and individual localities are working towards achieving these pathways:
• YHCYPCN Children's Cancer (0-16) pathway
• YHCYPCN Pathway for Children (0-16) with Brain and CNS Tumours
• YHCYPCN Pathway for Children with Bone Tumours
• YHCYPCN Pathway for Children with Retinoblastoma
• YHCYPCN Pathway for Children with Differentiated Thyroid cancer
• YHCYPCN Pathway for Children and Young People with Skin cancer
Where the pathway requires referral to nationally designated specialist centres (as is the case for bone tumours and retinoblastoma) this is identified within the pathway, and in the clinical management protocols for each tumour type (see below). These pathways are hosted on the Yorkshire and the Humber Strategic Clinical Network website to preserve version control, and can be found at: http://www.yhscn.nhs.uk/cancer/cancer-UsefulInformation/ChildrenandYoungPeople.php The YHCYPCN Group has agreed referral guidelines, and a diagnosis and staging policy for the service between all relevant teams across the network. This sets out the responsibilities of both the PTC and POSCUs in the process of investigation and referral of patients with suspected cancers. Clinical guidelines (or clinical management protocols) which outline the overall management of children’s cancer have been agreed, and cover in detail those cancers most commonly found in children and young people. Leukaemia Lymphoma and reticulo-endothelial malignancy CNS Tumours Sympathetic Nervous System Tumours Retinoblastoma Renal Tumours Hepatic Tumours Malignant Bone and Soft Tissue Sarcomas All other malignancies are covered by the children’s cancer pathway document. Where referral is required to nationally designated specialist centres (as is the case for bone tumours, retinoblastoma, and primary hepatic tumours) this is identified within the guideline. The clinical management protocols and the referral, diagnosis and staging policy are available on the YCN Website at http://www.yhscn.nhs.uk/cancer/cancer-UsefulInformation/ChildrenandYoungPeople.php Network-wide Guidelines The network has a guideline development and review group, which reports to the main network group. It is chaired by Dr Bob Phillips, paediatric oncology consultant in Leeds. It has representatives on it from the PTC, POSCUs and Community teams. This group has developed common network guidance and protocols on:
� Guidelines for Cytotoxic Administration � Guidelines on the management of Central Venous Access Devices (including the recognition
and treatment of complications)
9
� Guidelines on the management of infection o Recognition and treatment of neutropoenic sepsis
� Guideline for the treatment of chemotherapy induced nausea and vomiting � Guideline for recognition and treatment of stomatitis, diarrhoea and other mucositis � Guidelines on prevention, recognition and management of extravasation � Guideline for the recognition and treatment of chemotherapy, blood product or other drug
induced allergic reactions � Guideline for the use of blood product support
Guidelines related to the complications of chemotherapy (e.g. management of CVADs; management of nausea and vomiting) have within them information regarding referral of patients suffering from these complications. Patient Pathways for Radiotherapy All children in the YHCYPCN requiring radiotherapy treatment, whether radical or palliative, will be referred to the children’s radiotherapy service at the PTC in Leeds. This is a dedicated paediatric facility within the radiotherapy department in the Institute of Oncology in the Bexley Wing at St James’s Hospital; this facility is supported by the Paediatric Radiotherapy team ( a specialist Paediatric Radiographer, Clinical Nurse Specialist and Play Specialist. Children are referred to one of two 2 Consultant Clinical Oncologists, Dr Michelle Kwok-Williams and Dr Karen Dyker, who are core members of the PTC Solid Tumour and Brain and CNS diagnostic and treatment MDTs.
Radiotherapy is delivered according to the Royal College of Radiographers Good practice Guide for Paediatric Radiotherapy: https://www.rcr.ac.uk/system/files/publication/field_publication_files/BFCO%2812%295_Good_practice_1.pdf
Children who are unable to keep still or tolerate the treatment position for the duration of their radiotherapy treatments, and very young children, may require general anaesthesia (GA) for both planning and delivery of their RT. There is an expert and dedicated Paediatric Anaesthetic team at LTHT who provide this service. If children and young people meet the criteria for treatment by Proton Beam Radiotherapy, they are referred to the NHS England Proton Beam panel by the Clinical Oncologists. If Proton Beam therapy is agreed, this will usually require referral to one of the designated centres in the United States of America, under NHS England commissioning arrangements. Guidelines for psychosocial assessment
The group has agreed network wide psychosocial assessment guidelines which are available on the SCN Website at http://www.yhscn.nhs.uk/cancer/cancer/UsefulInformation/ChildrenandYoungPeople.php These guidelines specify the time points when a holistic needs assessment of the child and family should be undertaken.
Follow up and long term sequelae
On completion of treatment all follow up is directed by the PTC; this has been agreed by the PTC Diagnostic and Treatment MDT and the POSCU MDT leads through their representation at the CCNCG, and with the Late Effects MDT Lead, and is outlined in the Follow Up pathway found on the SCN Website at http://www.yhscn.nhs.uk/cancer/cancer/UsefulInformation/ChildrenandYoungPeople.php After completion of treatment all patients and their families are invited to an ‘End of Treatment’ meeting with their treating consultant and Key Worker at the PTC. Representation is also invited from the POSCU MDT, and any other involved professionals. This meeting will take place once the
10
immediate effects of acute treatment have passed; in the majority of cases this will be within 6-12 weeks of completing treatment. In all cases it will take place within six months of the completion of treatment. At (or prior to) the meeting the consultant will produce an End of Treatment summary, which is shared with the family, with the POSCU (or referring) consultant, and with the patient/family. At the meeting the Consultant and Key Worker will agree with the family a follow-up care plan which specifies the role of the POSCU MDT and the PTC MDT. This follow-up plan is explained to the child and family and kept in the clinical notes, with a copy going to the GP, POSCU or referring hospital, and to the family. This follow up care plan includes the frequency of clinical review as well as surveillance radiology, pathology investigations, including blood tests, and chemotherapy toxicity investigations for 5 years after treatment has finished. The schedule of this follow-up is disease and clinical trial specific. At present follow up is primarily undertaken in the PTC, but there is an increasing move towards shared follow up with the medical team in the POSCU, and this is agreed at or following the End of Treatment meeting. After 5 years the care of the patient is at present referred to the Long Term follow up team at the PTC in Leeds; there is a network agreed pathway for Follow Up and Referral; found on the SCN Website at http://www.yhscn.nhs.uk/cancer/cancer/UsefulInformation/ChildrenandYoungPeople.php A long term sequelae protocol is in place which is fully described in the PTC Late Effects operational policy. This follow-up follows the ‘Best Practice’ guidance for Long Term follow-up, which specifies the methods of surveillance used for the late effects of treatment, and to monitor for relapse. As shared ‘off treatment’ follow-up with local (POSCU) services becomes more established, this will impact on the patterns of long-term follow-up across the network.
Research and Clinical Trails
The YHCYPCN works closely with the Yorkshire and the Humber Comprehensive Research Network, (CRN) and with the NCRI Childhood Cancer Study Group to ensure that all children and young people have access to clinical trails and studies. There is a network agreed list of NIHR portfolio trials and studies, as well as a range of non-portfolio studies that has been developed in the PTC, and agreed by the network. There is an annual discussion of clinical trial activity at the full meeting of the Network group, in the presence of a representative of the CRN.
11
Appendix 1
Shared Care Agreement Template
Aim of the Agreement
The aim of this document is to describe in a formal agreement the respective responsibilities
of the Principal Treatment Centres (PTC) at Leeds and its partner Paediatric Oncology Shared
Care Units (POSCUs), as required by the NICE Improving Outcomes Guidance (IOG) in
Children & Young People with Cancer (August 2005). It highlights the essential role played
by Shared Care Units in providing local care to children and young people with cancer and
their families. This in line with the guiding principle of the IOG is to ensure “safe and
effective services as locally as possible, not local services as safely as possible”.
For the purposes of this agreement, children are 0-15 (up to their 16th birthday). All patients
from 0-15 (up to 16th birthday) will be referred to the Paediatric Oncology service at the
PTC. This agreement endorses this principle and describes PTC directed and co-ordinated
shared care across Yorkshire and Humber Children and Young People’s Cancer Network
(YHCYPCN).
Objectives
• To formalise the relationship between the Leeds Teaching Hospitals NHS Trust PTC
and POSCUs within the Yorkshire and the Humber Children and Young People’s
Cancer Network.
• To agree and document the level of shared care to be provided, with exclusions, the
model of service, the governance and leadership arrangements and the YHCYPCN
guidelines, protocols and care pathways that the service will work within.
• To enable the smooth and timely progression of patients and carers between all care
settings.
• To ensure that information about individual patients is communicated effectively and
shared appropriately to all those involved in the patient’s care.
• To promote on-going development of shared care services across children and young
people’s cancer services.
• To support the requirements of clinical trial governance where patients are recruited and
entered into clinical trials by the PTC, and treatment is also delivered by the POSCUs.
12
Governance Structures
Children’s Cancer Networks
The Improving Outcomes in Children and Young People with Cancer (CYPIOG) and
Children’s Cancer Measures ( v4 2014) set out a framework to provide leadership and co-
ordination of children’s cancer services through a Children’s Cancer Network (CCN).
The Yorkshire and Humber Children and Young People’s Cancer Network (YHCYPCN) is
made up of the Leeds THT PTC, Hospital Trusts who provide shared care services, PCTs who
provide community cancer services, representatives from the Strategic Clincal Network
(Cancer) and commissioning representative from the Yorkshire and the Humber Local Area
Team.
The role and function of the CCN is to:
• In collaboration with the Local Area team and the Strategic Clinical Network , agree
the configuration of PTC and POSCUs in the CCN
• Provide governance and leadership
• Ensure formal sign off of shared care agreements, in addition to sign off between the
PTC and POSCU.
• Ensure referral protocols and guidelines are agreed
• Ensure communication and co-ordination of care
• Ensure recruitment and entry into clinical trials and treatment on agreed regimens
The Shared Care agreement will be between the PTC and POSCU and agreed by the Lead
Clinician, Lead Nurse, Locality Cancer Managers and Chief Executive. The agreement is a
clinical agreement designed to support shared care and operates within the organisations’
governance mechanisms. It also clarifies the responsibilities relating to trial governance,
including responsibilities for dealing with submissions for local regulatory approvals.
Through this agreement both PTC and POSCU are committed to maintaining high standards
of professional practice and complying with all applicable legislation and good practice
guidelines including but not limited to:
• Data Protection Act 1998
• NHS Confidentiality Code of Practice
• NHS Caldecott Report and Caldecott Guardians
• GMC’s Guidance on Good Medical Practice
• Principles of Good Clinical Research Practice (ICH-GCP)
• Human Tissue Act 2004
• NHS Research Governance Framework for Health and Social Care 2nd
Ed April 2005
Both PTC and POSCU agree to have mechanisms in place to ensure that all patient
data/information is kept confidential and secure in accordance with all applicable legislation
and good practice guidelines.
Both PTC and POSCU acknowledge that in the normal course of their shared care
arrangements they will exchange patient identifiable and sensitive information in accordance
with the Data Protection Act 1998.
13
Responsibilities
PRINCIPAL TREATMENT CENTRE
Paediatric oncology / malignant haematology
Clinical Leadership & essential resources:
The children’s cancer service at LTHT complies with the requirements to be recognised
as a Principal Treatment Centre .
• In order to facilitate support between Shared Care Units and PTCs there is a defined
link person ( a named member of the Paediatric Macmillan Nurse team) at the PTC for
each POSCU,with additional support from the Shared Care Liaison Nurse.
LTHT PTC has staff and resources as described in the NICE Improving Outcomes
Guidance in Children and Young People with Cancer (August 2005), and the Children’s
Cancer Measures Cancer Measures (v3 2013).
• LTHT PTC has staff and resources to provide a cancer chemotherapy service to
children and young people and an identified lead pharmacist for the service.
• LTHT meets and complies with governance requirements to recruit and enter
children and young people into clinical trials.
• LTHT will work effectively with commissioners, networks and other stakeholders in
planning of services, and meeting operational standards such as monitoring of pathways.
• LTHT will develop and review supportive care protocols agreed by a multi-
professional group including shared care representation
Lead Clinician for the PTC: Dr Sue Picton.
Critical Mass:
• LTHT PTC manage sufficient numbers of patients to maintain a workforce with
cancer expertise across the full range of paediatric cancers and adolescent cancers with
appropriate clinical support services and age appropriate facilities. The average
number of new patients (0-16) a year is 105 (average over five years).
Service Provision:
Referral, diagnosis and treatment
LTHT PTC will
• Arrange timely access of any child with a new diagnosis or suspected cancer to the
PTC or, exceptionally, to locate a bed in another tertiary oncology centre.
• Host two diagnostic and treatment MDTs for the PTC (one for brain and CNS
tumours, and the other for all other solid tumours and haemato-oncology).
Membership and meeting organisation is described in the PTC operational policy.
• Manage the investigation, diagnosis and staging of disease in accordance with the
YHCCN referral, diagnosis and staging protocol.
(http://www.ycn.nhs.uk/html/publications/guidelines_paediatric.php)
• Manage treatment decisions and initiate cancer therapy, offering inclusion in relevant
national or international therapeutic trials in accordance with the YHCYPCN clinical
14
management protocols.
(http://www.ycn.nhs.uk/html/publications/guidelines_paediatric.php)
• Enter patients in clinical trials and retain responsibility for conduct of the clinical trials
• Provide a treatment plan and flow sheet for each patient
• Obtain consent for treatment and deliver chemotherapy in an inpatient / daycare / and
outpatient setting.
• Initiate and provide radiotherapy whether radical or palliative,
• Undertake all therapeutic surgery
• Manage procedures requiring specific technical support e.g. line insertions / removals
• Undertake Stem Cell transplants for children and young people as part of the West
Yorkshire Bone Marrow Transplant programme.
• Provide the clinical haematological and immunology support to manage children and
young people undergoing stem cell procedures
• Provide appropriate clinical support services, equipment and laboratory infrastructure
to meet JACIE standards including, selection of donors, handling of transplant materials,
patient selection and treatment and audit.
• Provide an appropriate physical environment to support immuno-compromised
patients.
• Provide support to POSCU in the management of clinical problems arising from
treatment, where appropriate admitting patients to the PTC for ongoing care.
• Manage clinical problems arising from treatment for the patients at highest risk of serious
complications
• Provide high dependency / critical care support as required
24 Hour Advice Line
• LTHT will provide a 24 hour advice service to patients, parents and carers, and to
health professionals from across the network.
• The PTC at Leeds is the common access point to this service across the Network, and
is responsible for ensuring that all parents are given the appropriate telephone
numbers.
• This service is available 24 hours a day, 7 days a week, 52 weeks a year
• It is governed by a network agreed specification
(http://www.ycn.nhs.uk/html/publications/guidelines_paediatric.php)
Medical cover arrangements
• If the POSCU is unable to provide medical cover required to provide the service safely
patients should be referred back to the PTC following discussion between the
respective clinical teams.
PTCs role in co-ordination of care with POSCU
Communication and information sharing
The PTC will:
• Ensure there is an identified key worker for each patient
• Provide specific, written patient / parent information including information on the
relevant protocol, or clinical trial, including side effects of treatment
• Ensure attendance of the PTC Macmillan ‘Link’ Nurse at POSCU MDT meetings.
15
• Keep POSCU team informed and updated on all matters relating to patients and relevant
modifications or changes in treatment
• Provide timely, written communication to the POSCU team for individual patients
• Work effectively with POSCU and community nursing teams to plan and deliver
patient care
• Chemotherapy Service:
• Direct all chemotherapy prescribing; where chemotherapy is administered in Shared
Care Unit, ensure relevant information and documentation is forwarded to the
appropriate personnel in POSCU.
• Record all chemotherapy administered in Shared Care Units.
Clinical Trials
The majority of children with cancer are entered into National Cancer Research Network
(NCRN) adopted national or international clinical trials sponsored either by:
• Cancer Research UK Clinical Trials Unit (CR-CTU) – University of Birmingham
• International sponsor, and co-ordinated by CRCTU at Birmingham
• Other university based clinical trials units
• Pharmaceutical companies
All new trials are approved by the National Research Ethics Service (NRES) within the UK
prior to application for Site Specific Assessment (SSA) by participating sites. In keeping
with the document of Good Clinical Practice, (the EU directive May 2004) and in accordance
with the Clinical Trials Act of 1987 and the 1990 amendment, it is necessary that the
Principal Treatment Centre (PTC) stipulates the responsibilities of the Shared Care Unit
(POSCU) in relation to patient care and reporting of data. This will vary slightly with each
particular trial, but general principles will apply.
The PTC team will:
• Be responsible for the initiation, set up and conduct of all clinical trials into which
patients treated at the PTC are entered
• Seek local regulatory approval including Research and Development (R&D), and Site
Specific Asessment (SSA) for ethical approval by NRES.
• Be responsible for Pharmacovigilence and Data collection for all clinical trials into
which patients treated at the PTC are entered
• Ensure that copies of informed consent forms are forwarded to the Shared-Care Centre promptly for inclusion in Shared-Care Patient’s notes.
• Support the POSCU lead consultant in research governance issues around paediatric
oncology clinical trials in which patients cared for by the POSCU are entered
• Ensure and document appropriate delegation of any research related activities to the Shared-Care Centre.
• Ensure all SAE’s, occurring on any Shared-Care Patients enrolled onto the study by the PTC is reported to the Sponsor in line with protocol specific time frames
• Agree with the POSCU Lead Clinician where there is a need for a particular trial to open as a study site in the POSCU and support that process from the PTC
16
Education and training
• Support education and training for POSCU staff, after dialogue on needs for each
POSCU.
• Continue to update and inform the POSCU through visits from PTC team members
and annual study days.
• Provide education, social and psychological support to patients and families
• Teenagers: PTC
All patients from 0-15 (up to 16th birthday) will be referred to the Paediatric Oncology
service at the PTC, where teenagers will come under the care of the TYA service. Patients
from 16 to 18 (up until 19th birthday), may be referred to either the Paediatric Oncology
service, or the relevant site-specific adult service, but will all be referred to the PTC TYA
MDT for discussion. The majority of patients between 16 and 18 years old will be cared for
within the Paediatric Oncology and Haematology service, (as above). Referrals should be
made in accordance with the YHCYPCN clinical management protocols.
(http://www.ycn.nhs.uk/html/publications/guidelines_paediatric.php)
Peer group support is pivotal to teenagers with cancer. The TYA service will continue to
provide this link whilst the teenager is being cared for in the POSCU. This will be via links
with the TYA Service, and in particular, with the Youth Support Worker and the Key Worker.
The TYA Service will:
• Maintain close links with the POSCU
• Maintain close liaison with the nursing and medical teams at the POSCU
• Maintain close liaison with the community teams and local services e.g. education,
peer groups
• Provide a link for advice/expertise on the management of teenagers with cancer
• Notify any changes of care/treatment to the POSCU
• Provide up to date information/education about TYA with cancer
• Provide psychosocial support for the young person and their families/friends/carers.
Follow up and long term sequelae: PTC
On completion of treatment disease specific follow up is directed by the PTC and provided on
a shared basis with the POSCU. This includes the frequency of clinical review as well as
surveillance radiology and chemotherapy toxicity investigations for 5 years after treatment
has finished. The schedule of this follow-up is disease specific and clinical trial specific.
The PTC will arrange an ‘End of Treatment’ appointment for the child and family, to which
POSCU representatives will be invited. The PTC consultant will provide an End of Treatment
summary and a Follow-Up Care Plan to the child and family and the POSCU team. The care
plan will include follow up arrangements at both PTC and POSCU.
Where children require ongoing support there will be occasions where this is best provided by
the local POSCU teams, and this will be agreed with them on an individual basis by the
responsible consultant from the PTC. The POSCU Lead Clinician will be informed where
they do not themselves take on local follow-up.
After five years patients are referred to the Long Term Follow- Up service, and this is
currently provided at the PTC only, ensuring consistency of approach across the YHCYPCN.
Models of care are being established to enable effective, appropriate care in view of the
17
increasing numbers of survivors, the range of ages and individual risks of recurrence and long
term sequelae. Work will be undertaken to review local provision of this service.
The Late Effects MDT at the PTC is currently transforming the pathway in Long term follow
up. Pathway mapping has been undertaken. A transformed pathway of care, involving risk
stratification, enhanced supported self management, increased delivery of care in primary care
setting is proposed.
Community and Palliative Care Services: PTC
• Services for children with cancer in the community are provided byXXXXX. The
Link Macmillan Nurse works closely with the local team in accessing additional
community services for patients.
• The Link Macmillan Nurse from the PTC will provide specialist symptom control and
palliative care support working with the POSCU team and additional community
services as required. An on-call service is provided by the Macmillan team at the PTC
for all patients requiring palliative care.
• The Link Macmillan Nurse from the PTC will work together with XXXX (ie Local
Services as available/applicable) in the coordination and provision of End of Life
care.
PAEDIATRIC ONCOLOGY SHARED CARE UNIT (POSCU)
Paediatric oncology / malignant haematology
POSCU Role – for children aged 0-15 treated within the Calderdale and Huddersfield NHS
Foundation Trust
Level of POSCU Service Please tick level provided and for Level 1 POSCU
detail which option (see below) is agreed
Level 1
���� Level 1: Option 2
POSCU Level 1 Services
• inpatient supportive care including care of children with febrile neutropoenia
• outpatient supportive care
• outpatient follow up
• outpatient oral chemotherapy
• outpatient IV bolus chemotherapy
Allowable options from the above:
1. all the above services
2. opt out of outpatient IV bolus chemotherapy only
3. opt out of outpatient IV bolus chemotherapy and inpatient supportive care including care of
children with febrile neutropoenia
18
4. opt out of all chemotherapy and inpatient supportive care including care of children with
febrile neutropenia.
Clinical Leadership and essential resources: POSCU
• POSCU Lead Clinician and Head of Chemotherapy service:
• POSCU Lead Nurse (Role Share):
• XXXX POSCU has a work programme and action plan in place to support compliance
with the NICE IOG for Children and Young People with Cancer (2005) and
Children’s Cancer Measures Cancer Measures (v3 2013).
• XXXX POSCU holds a monthly MDT with membership and meeting organisation as
described in their operational policy
• Lead staff attend appropriate network and local forums relating to children’s & young
people’s cancer services
• Lead staff should identify and liaise with the lead for Teenage and Young Adult
(TYA) cancer services
• Medical staff at the POSCUs do not take take part in the network medical cover rota
• Nursing skill mix should ensure that sufficient numbers of nursing staff have the
relevant clinical competencies, as agreed in the YHCYPCN Nurse Training programme,
to provide the level of Shared Care agreed
• One person should be designated as document controller, responsible for receiving,
acknowledging, archiving and distributing treatment related documentation.
Service Provision
The POSCU team at XXXX aims to support a holistic approach to local care and to
co-ordinate the different clinical, psychological and social supports required by the patients
and their families in partnership with the PTC.
• To identify the child with suspected cancer and ensure appropriate and timely referral to
the PTC in accordance with the YHCYPCN referral protocol
• To provide supportive care according to Supportive Care Guidelines according to the level
of Shared Care agreed.
• To admit and manage patients with febrile neutropenia in line with YHCYPCN guidelines
and with appropriate communication with the PTC.
• To manage continuing treatment and other problems arising during treatment with
appropriate support from the PTC
• To manage scheduled tests and investigations such as blood tests
• To administer only ‘low risk’ chemotherapy treatments (see Appendix 1). which have
been prescribed, made up and dispensed in Leeds in line with the network policy on
‘Chemotherapy Administration in Paediatric Oncology Shared Care Units and the
Community’ (http://www.ycn.nhs.uk/html/publications/guidelines_cyp_policies.php
• Any chemotherapy will only be administered by nurses who have undergone the network
agreed training programme. The Lead Clinician takes on the role of ‘head of
chemotherapy service’ and the link pharmacist will liase as required with the pharmacy
team at the PTC.
• To provide local follow-up in discussion with responsible consultant at the PTC and
agreement with families.
19
Co-ordination of care:
• To provide timely, written communication with PTC about issues encountered in the
POSCU.
• To notify changes in treatment to the PTC
• To report any Serious Adverse Events or other incidents occurring in the POSCU to the
clinical team, and to the research team where patients are enrolled in clinical trials
• To provide support for families and choice for patients regarding social and
psychological support.
• To provide patient information about local services.
• To maintain effective links with palliative care services, Social Services, schools,
hospices and other community based services,
• To work effectively with PTC, Community and local services when planning
palliative care for patients.
Follow up and long term sequelae: see section 2.1.3
On completion of treatment disease specific follow up is directed by the PTC and provided
according to the End of Treatment Care Plan by both PTC and POSCU. Where there are
ongoing medical and nursing needs additional follow-up may be provided by the POSCU in
agreement with the responsible consultant from the PTC.
Such follow up may be undertaken by other consultants in the POSCU but will be coordinated
through the POSCU Lead Clinician.
After five years patients are referred to the Long Term Follow- Up service, and this is
currently provided at the PTC only, ensuring consistency of approach across the YHCYPCN.
Models of care are being established to enable effective, appropriate care more locally in view
of the increasing numbers of survivors, the range of ages and individual risks of recurrence
and long term sequelae.
Teenagers: POSCU
Peer group support is pivotal to teenagers with cancer. The TYA service will continue to
provide this link whilst the teenager is being cared for in the POSCU. This will be via links
with the TYA Service, and in particular, with the Youth Support Worker and Key Worker.
The POSCU team will:
• Maintain close links with the TYA professional in the PTC
• Develop links with the TYA leads in Calderdale
• Seek advice/expertise on the management of the teenager with cancer when required
• Maintain close liaison with the community teams and local services e.g. education,
peer groups
• Notify any changes of care/treatment to the PTC
• Provide psychosocial support for the young person and their families/friends/carers.
20
Community and Palliative Care Services: POSCU
• To provide local support for children with cancer and their families at home.
• To work with the PTC Link Macmillan Nurse and with other community teams, in the
provision of palliative care.
Clinical Trials
The majority of children with cancer are entered into National Cancer Research Network
(NCRN) adopted national or international clinical trials sponsored either by:
• Cancer Research UK Clinical Trials Unit (CR-CTU) – University of Birmingham
• International sponsor, and co-ordinated by CRCTU at Birmingham
• Other university based clinical trials units
• Pharmaceutical companies
All new trials are approved by the National Research Ethics Service (NRES) within the UK
prior to application for Site Specific Assessment by participating sites. In keeping with the
document of Good Clinical Practice, (the EU directive May 2004) and in accordance with the
Clinical Trials Act of 1987 and the 1990 amendment, it is necessary that the Principal
Treatment Centre (PTC) stipulates the responsibilities of the Shared Care Unit (POSCU) in
relation to patient care and reporting of data. This will vary slightly with each particular trial,
but general principles will apply.
• To provide data for patients on clinical trials (e.g. hospital admissions, radiological
images, lab tests, blood product administration) as requested by data managers and
research nurses at the PTCs
• To keep health records on all medical events, including possible side effects of
treatment experienced and their severity.
• Immediate and close liaison with the PTC in response to any medical event for
assessment by the PTC as to the need for Severe Adverse Event (SAE) reporting as
defined by each protocol and to enable evaluation and report to the Sponsor within the
required time frames.
• The Shared-Care Centre shall permit the Sponsor or any third party acting on behalf of
the Sponsor or any auditor or inspector access to all relevant clinical data of Shared-
Care Patients for monitoring and source data verification. Such access to be arranged
at mutually convenient times and on reasonable notice. Such monitoring may take
such form as the Sponsor reasonably thinks appropriate including the right to inspect
any facility being used for the conduct of the trial and to examine any procedures or
records relating to the trial.
Leeds Principal Treatment Centre & XXXX Foundation Trust Paediatric Oncology Shared
Care Unit Shared Care Agreement
1) PTC Responsibilities
As defined above
2) POSCU Responsibilities
As defined above and as agreed below
POSCU Role – for children and teenagers treated within the service
Level of POSCU Service Please tick level provided and specify option
for Level 1
Level 3
Level 2
Level 1
Opt Out Option (Level 1 POSCUs only) as defined above:
We have read and understand the responsibilities of PTCs and POSCUs and we are satisfied
there is agreement about the level and type of care to be provided.
___________________________ _________________________
Lead Consultant Lead Clinician
POSCU PTC
Date
___________________________ ___________________________
Chief Executive Chief Executive
Trust Trust
Sign off by Chair C&YP Cancer Network
____________________________________ Date
A copy will be sent to:
Specialist Commissioning Group Representative
Specialist Commissioner Lead Children & Young People with Cancer
Network Directors