Embed Size (px)
Citation preview
NAAR Funding Played Key Role in Yale STAART Grant
Pilot Studies on Visual Scanning, Joint Attention & ProsodyPivotal to Earning Major NIH Award
NAARRATIVEThe Journal of the National Alliance for Autism Research
SPRING 2003
www.naar.org
Yale Leverages NAAR-fundedResearch into STAART Grant
Pharmacological Interventions
Latest CDC Prevalence Study
What’s InsideWhat’s InsideNAARRATIVE is publishedfour times a year by the NationalAlliance for Autism Research(NAAR).
If you would like to receiveNAARRATIVE and join theNAAR mailing list, please call(888) 777 - NAAR.
To suggest a story idea for NAAR-RATIVE, or for more informa-tion about an article thatappeared in NAARRATIVE,please contact Joe Guzzardo at(888) 777 - NAAR, or via e-mail [email protected].
Established in 1994, NAAR isthe first organization in the coun-try dedicated to funding andaccelerating autism research thatseeks to determine the causes,prevention, effective treatmentsand, ultimately, cure for autismspectrum disorders. To date,NAAR has committed more than$10 million to directly fund 119autism research projects world-wide - more than any other non-governmental organization.
Science & ResearchNAAR PLAYED KEY ROLE IN YALE STAART GRANT - PAGE 4Yale’s Fred Volkmar, M.D. and Ami Klin, Ph.D., discuss the Child Study Center’srecent STAART program and the important role NAAR played in their NIH applica-tion for funding.
AUTISM TISSUE PROGRAM EXPANDED - PAGE 6Jane Pickett, Ph.D., Director of the Autism Tissue Program, talks about the latest ini-tiative to expand the Autism Tissue Program and enhance tissue collection andstorage protocols.
EXPLORING AUTISM WEBSITE TRANSLATED TO SPANISH & FRENCH - PAGE 7NAAR recently funded the translation of the award-winning Exploring Autism web-site into Spanish and French.
PHARMACOLOGICAL INTERVENTIONS FOR AUTISM - PAGE 8In the first of a two-part series on pharmacological interventions for autism, TrusteeC.T. Gordon, III, M.D., of the NAAR Medical Affairs Committee, provides a detailedsummary on neuroleptic drugs available to help individuals with autism spectrumdisorders.
SAB MEMBER LEADS CDC’S PREVALENCE STUDY - PAGE 11A new study led by NAAR SAB member Marshalyn Yeargin-Allsopp, M.D., showsthe prevalence for autism is approximately 10 times higher than the rates fromstudies conducted in the United States 10 years ago.
NAAR AUTISM POLL: AMERICANS WANT MORE ACTION ON AUTISM - PAGE 12A new poll conducted by NAAR reveals that Americans want much more infor-mation and a far greater research commitment focusing on the causes andtreatment of autism spectrum disorders. Also, learn your “Autism IQ” by taking theNAAR Autism Test.
RESULTS OF THE DANISH STUDY ON MMR - PAGE 14Andy Shih, Ph.D., NAAR’s Director of Research & Programs, reviews the findings ofthe Danish study focusing on the MMR vaccine and autism, co-funded by NAAR.
Progressions - Development & Fundraising News
FALL 2002 WALK F.A.R. FOR NAAR - PAGE 16 Photos & results from the 2002 Fall Walk F.A.R. for NAAR events from Long Island,New England, Buffalo, New Jersey and Florida.
RESEARCH.HOPE.
COMMITMENT.
99 Wall StreetResearch Park
Princeton, NJ 08540(888) 777-NAARWWW.NAAR.ORG
NAARRATIVESpring 2003
NAAR is a member of the MedicalResearch Agencies of America(MRAA) and is included in theCombined Federal Campaign
(CFC). Encourage your family andfriends in the military, postal system
and those who are civilian government employees to support
NAAR through the CFC.
CFC #1717All Rights Reserved. Copyright 2003 National Alliance for Autism Research.The contents of NAARRATIVE cannot be reproduced without prior written permission of the National Alliance for Autism Research.

BOARD OF TRUSTEESPatricia Menendez Cambo, Esq. Andy Cerise H. Eric CushingGary K. Duberstein, Esq.Ann Boeker GibbonsC.T. Gordon, III, M.D.W. Donald GoughVictoria J. Hennelly, Esq.Deborah Hilibrand, MBAMark J. Krinsky, CPAEric London, M.D.Karen Margulis London, Esq.Cathy J. LurieJeffrey R. Lurie, Ph.D.Prisca Chen Marvin, Esq.The Hon. Sally J. PedersonDavid C. PhiferBarri RindDaniel F. Ryan, Jr.Martin A. Schwartzman, CFE, CIE, CPCUSCIENTIFIC ADVISORY BOARDMelissa D. Begg, Ph.D., Sc.D.Columbia UniversityWilliam E. Bunney, Jr., M.D.University of California-IrvineManuel F. Casanova, M.D.The Medical College of GeorgiaVerne S. Caviness, Jr., M.D., D. Phil.Harvard Medical SchoolJoseph T. Coyle, M.D.Harvard Medical SchoolThomas Curran, Ph.D.St. Jude Children’s Research HospitalStephen R. Dager, M.D.University of Washington School of MedicineMony J. de Leon, Ed. D.New York University Medical CenterEmanuel DiCicco-Bloom, M.D.UMDNJ - Robert Wood Johnson Medical SchoolMartha Bridge Denckla, M.D.Johns Hopkins University School of MedicineSalvatore J. Enna, Ph.D.University of Kansas School of MedicineLynn W. Enquist, Ph.D.Princeton UniversityJames F. Gusella, Ph.D.Harvard Medical SchoolMary Beth Hatten, Ph.D.Rockefeller UniversitySusan L. Hyman, M.D.University of Rochester School of MedicineBarry Jacobs, Ph.D.Princeton UniversityKathleen A. Mahon, Ph.D.Baylor College of MedicineWilliam C. Mobley, M.D., Ph.D.Stanford University Medical CenterEric J. Nestler, M.D., Ph.D.University of Texas - Southwestern Medical CenterRichard S. Nowakowski, Ph.D.UMDNJ - Robert Wood Johnson Medical SchoolPasko Rakic, M.D., Sc.D.Yale University School of MedicineJudith M. Rumsey, Ph.D.Georgetown University Medical CenterNational Institute of Mental Health Robert Schultz, Ph.D.Yale University Child Study Center Peter Tanguay, M.D.University of LouisvilleJames T. Winslow, Ph.D.Emory University Marshalyn Yeargin-Allsopp, M.D.Centers for Disease Control and PreventionHONORARY BOARDLisa and Will ClarkAudrey FlackLaurie and Doug FlutieTemple Grandin, Ph.D.Lisa and Dustin HoffmanArlene and Joe MantegnaClaire and Dan MarinoNancy Lurie MarksBranford MarsalisWynton MarsalisSue and Scott MellanbyElizabeth and Aidan QuinnThe Hon. Barbara RobertsLynn and Bret SaberhagenOliver Sacks, M.D.CHIEF OPERATING OFFICERGlenn R. Tringali
AA LeLetttter frer from Marom Mark J. Krinskyk J. Krinsky, C.P, C.P.A.ATreasurer, National Alliance for Autism Research
As the father of a 16-year-old son, David, who has autism, I know first-hand thatparents of children with autism are faced with many difficult choices, and ques-tions with very few answers. Why does David have autism? What is the besttreatment? What type of future will David have? How can I help best help him?These are just a handful of the questions I have grappled with since David wasdiagnosed 14 years ago.
Naturally, such serious dilemmas are often overwhelming. Sometimes my courage wavers.When it does, I look to David - and I am inspired by the courage he shows each and every dayof his life. I see how hard he works at things we take for granted - the way he copes in an envi-ronment where people may be staring at him. David defines perseverance and unconditionallove. He makes it all worthwhile.
As we continue to search for answers, my greatest hope for David is kept alive through theresearch that is being funded by the National Alliance for Autism Research (NAAR). Researchis the only way we will ever come to understand what causes autism, and learn to diagnoseautism earlier. Research will also allow us to develop more targeted interventions and effectivemedical treatments and - someday - find a cure. By supporting this biomedical research, we aredoing something that actively helps our children, which many times is something we feel we areunable to do.
When considering giving support to a charitable organization, it is common to wonder whatour hard earned dollars will be used for, and if the organization we choose is responsible withthe funds it raises.
Supporting NAAR has proven to be a sound investment. The research initially funded byNAAR has made a dramatic impact on the autism research landscape in the United States,Canada and Europe and has been leveraged to attract more than $23 million in autism researchawards by the National Institutes of Health (NIH) and other funding sources. Every $1 NAARhas committed to research has resulted in approximately $8 invested by the federal governmentand other funding sources in large autism research projects.
As NAAR's treasurer for the past seven years, I can honestly say that since our earliest days, wehave tried to be a "transparent organization" dedicated to efficiency and getting the "biggestbang for the buck." My fellow trustees - all unpaid volunteers and most with children or sib-lings with autism - work tirelessly to see that this is so. In its first official annual report, pub-lished just weeks ago, NAAR details its full audited financial statements, as well as informationon its varied research programs and development initiatives. In addition, I'm pleased andproud to report that NAAR was recently evaluated by the Better Business Bureau Wise GivingAlliance and has met all 23 of the organization's standards for charitable organizations.
While I am NAAR's treasurer and a CPA by training, first and foremost I am David's father. Itis because of David and what I've seen over the course of the past seven years that I believe somuch in the work that NAAR does every day. But we still have a long way to go. Financial sup-port is critical if we are to continue accelerating the pace of autism research.
On behalf of all the hard working volunteers, trustees and staff that bring NAAR to life, Davidand I invite you to join us in our continuing search for answers to the mysteries of autism and in supporting the work of NAAR.
Mark

NAARRATIVE - Spring 2003 Page 4
Science &Science & Research:Research: Leveraging NAARLeveraging NAAR Pilot Studies Pilot Studies
NNAARAAR-F-Funded Pilounded Pilot St Studies Platudies Playyed Ked Keey Ry Role ole in Yin Yale Sale STTAARAART GrT Grant ant By Fred Volkmar, M.D., Principal Investigator & Ami Klin, Ph.D., Co-Principal Investigator, Yale University Child Study Center STAART Grant
The autism research group at the Yale UniversityChild Study Center was recently awarded one of thefirst Studies to Advance Autism Research andTreatment (STAART) grants by the National Institutesof Health (NIH). Three of the five projects in the YaleSTAART grant program originated from pilot studiesinitially funded by the National Alliance for AutismResearch (NAAR).
Our initial awards from NAARwere instrumental in buildingan important line of research,which we could capitalize uponfor the STAART application.Having this support was essen-tial since it enabled us to showsome of our initial results, andthe viability and utility of thiswork. We are particularlypleased with this support since itreaffirms our notion that highquality research and patient carego hand in hand.
The Yale STAART grant isadministered by the NationalInstitute of Mental Health (NIMH) and will providefive years of support for a broad-based program ofresearch on the neurobiology of social difficulties inautism. Only one other grant, directed by JosephPiven, M.D. at the University of North Carolina,Chapel Hill, was funded in the initial round of com-petition. Eventually, a network of centers will be fund-ed around the country through this vital program.
Our original NAAR awards supported important pilotstudies that focused on early mechanisms of socializa-tion. These pilot studies were funded in 2000 and2001 and led by Dr. Ami Klin, Dr. Fred Volkmar,Warren Jones, Dr. Kasia Chawarska, and Dr. RheaPaul.
The first project builds on the development of a newmethod to study the way that toddlers at risk forautism seek social meaning in what they see, which wasmade possible through the study, Visual ScanningPatterns and Mental Representations of Social Interaction inInfants and Toddlers Suspected of Having Autism, fundedby NAAR in 2000.
Using an eye-tracking technology, we’ve shown thatadolescents and adults withautism fail to visually attend toessential aspects of social sceneswhile focusing on stimuli thatare either irrelevant for under-standing a social situation orprovide them with a very smallwindow into the intentions andfeelings of others. Specifically,individuals with autism aremore likely to focus on people'smouths rather than eyes. Sinceso much of a person's intentionsand emotions are conveyedthrough eye expressions, it isvery likely that individuals with
autism are able to obtain only a very partial under-standing of what they experience when watching oth-ers.
The NAAR award, and the subsequent project inSTAART, adapted the eye-tracking paradigms for usewith very small children. Since orientation to people(vs. the inanimate environment) and to eyes (ratherthan mouths) are skills emerging in the first weeks oflife, we hope to develop this methodology as a way ofidentifying vulnerabilities for autism in the first 12months of life and learn to diagnose autism earlier.
The second NAAR award funded the pilot study,Precursors of Joint Attention Skills in Autism and RelatedConditions - also a 2000 grant - that focused on animportant precursor of joint attention skills, a groupof abilities that are the building blocks of social reci-
(please see Yale STAART on page 5)
Fred Volkmar, M.D. Ami Klin, Ph.D.
NAAR-funded studies on visual scanning, jointattention and prosody were pivotal to Yale in
securing the STAART grant from the NIH.

NAARRATIVE - Spring 2003 Page 5
Into Major NIHInto Major NIH Award for Autism ResearchAward for Autism ResearchYale STAARTYale STAART (continued from page 4)
procity, language, andsymbolic development.Deficits in joint attentionskills are known to beamong the most centraldisabilities in young chil-dren with autism. In thefirst months of life, typi-cal children are alreadyable to discern gaze direc-tion, using it, almostreflexively, to learn abouttheir environment. In the experimental paradigm used, neurotypicalbabies shift their visual attention to an object in the distance muchmore quickly if another person is looking at that object than if theperson is looking in the other direction.
In the STAART grant, these studies of visual cueing will help us bet-ter understand what might be the developmental factors accountingfor the eventual disruption of joint attention skills, and the cascadeof disabilities that seem to originate from it.
The third NAAR award, The Development of Prosody in Young Childrenwith Autism and Related Conditions, which was awarded in 2001, sup-ported the work on listening preferences for speech sounds and sim-ilar auditory behaviors that facilitate social engagement in typicalbabies. From the very first few days of life, babies are attracted tospeech sounds. In contrast, the lack of orientation to speech, evenwhen one's name is called repeatedly, is one of the most robust pre-dictors of a subsequent diagnosis of autism in toddlers at risk. In theSTAART grant, the study of these early auditory mechanisms ofsocial engagement, as well as other early speech-processing accom-plishments of the first year of life, is examined in detail in a cohortof toddlers at risk for autism.
In addition to the projects that originated in the NAAR start-upawards, the Yale STAART grant will include projects on behavioraland neural plasticity in face recognition (i.e. modification in the wayan individual learns or processes information), led by Robert Schultz,Ph.D., and a study of the drug fluvoxamine in children and adoles-cents with autism and anxiety disorders, led by Larry Scahill, Ph.D.and George Anderson, Ph.D.
Editor’s Note: NAAR's commitment to funding mentor-based fellowships for autismresearchers correlates well to the STAART program, which includes a strong assessment corethat creates the opportunity to train young investigators to focus on autism research. Drs.Klin, Volkmar, Schultz and Paul all serve as mentors to NAAR-funded fellows. The NAAR-funded pilot study on visual scanning also helped the Yale group receive an NICHD-fundedCPEA (Collaborative Programs of Excellence in Autism) award.
Leveraging Research & Hope:The Fruits of Our Labor
News of the Yale Child Study Center'saward as one the first two STAART grants inthe U.S. electrified the autism community,particularly at NAAR - both in the nationaloffice and throughout the country, whereNAAR volunteers and supporters are chang-ing the course of autism research.
Essentially, the Yale team leveragedapproximately $256,000 in NAAR researchawards into a five-year grant from theNational Institutes of Health (NIH) encom-passing an estimated $6.5 million.
Yale's recent accomplishment is the latestexample of how supporting NAAR hasproven to be a sound investment. To date,NAAR-funded research has been leveragedinto more than $23 million in larger, multi-year autism research grants from the NIHand other sources.
The pilot studies funded by NAAR thatplayed a key role in Yale's STAART grantapplication include:
Ami Klin, Ph.D."Visual Scanning Patterns and Mental
Representations of Social Interaction in Infantsand Toddlers Suspected of Having Autism"
Research Partner: Toys R Us, Inc.
Fred R. Volkmar, M.D. & Kasia Chawarska, Ph.D."Precursors of Joint Attention Skills in Autism
and Related Conditions" Research Partner:
Nancy Lurie Marks Family Foundation
Rhea Paul, Ph.D."The Development of Prosody in Young Children
with Autism and Related Conditions"
Funding grants for new, innovative pilotstudies that allow researchers the opportuni-ty to leverage their initial research into larg-er, multi-year grants from the NIH and othersources is at the core of NAAR's mission.
NAAR's work in this area, however, is not lim-ited to fundraising alone.
The STAART Centers Program was estab-lished in response to the Children's HealthAct of 2000. NAAR played a pivotal role inthe development and eventual passage ofthe Children's Health Act of 2000 and ensur-ing the legislation had a strong focus onautism research.
“Our initial awards fromNAAR were instrumental in buildingan important line of research, which
we could capitalize upon for the STAART application...
We are particularly pleased with thissupport since it reaffirms our notion
that high quality research and patientcare go hand in hand.”

NAARRATIVE - Spring 2003 Page 6
Science &Science & Research:Research: Autism Tissue Program Expansion Autism Tissue Program Expansion
NNAAR FAAR Funds Nunds Neew Initiativw Initiative te to Expand Ao Expand Autism Tutism Tissue Prissue Progrogramam
By Jane Pickett, Ph.D.Director, Autism Tissue Program
TThe National Alliance for Autism Research (NAAR)has recently funded a new collaborative program thatbrings together the autism community with profes-sional organ procurement organizations and medicalexaminer's offices in four states to increase theamount of brain tissue available to scientists focusingon autism research.
NAAR has committed $140,000 to launchthe initiative - a new component of theAutism Tissue Program, which NAAR firstestablished and funded in 1998 with theAutism Society of America (ASA)Foundation. The collaborative new pro-gram will develop a standard protocol foroutreach, registration, tissue collection andstorage and increase the acquisition of high-quality, post-mortem tissue for autismresearch.
"In the field of neuroscience, as it pertainsto autism research, brain tissue is the mostvaluable material on the planet, enablingscientists to go far beyond the constraints of othertechnologies allowing us to study autism on both a cel-lular and molecular level," said Prisca Chen Marvin,NAAR president. "We are very excited about this newelement of the Autism Tissue Program, which willresult in more tissue for research and improved proto-cols that benefit donor families and researchers."
In Iowa, Lt. Governor Sally J. Pederson, a NAARtrustee, has played a critical role in getting the AutismTissue Program listed on the Iowa Donor Network, anon-profit organization that operates as the primarycontact for organ, tissue and eye donation services forthe state of Iowa. Sally also helped facilitate relationsbetween the program and the Iowa state ASA chapter.
Along with Iowa, the new initiative will partner withASA chapters in Maine, Michigan and New Mexicothat will focus on outreach, education and awareness.The Autism Tissue Program has already held prelimi-nary meetings in these four states.
"We believe the Autism Tissue Program is an importantcomponent in our understanding of the autism puzzleand are excited to continue our collaboration in thisexciting new stage of the program," said Rob Beck, exec-utive director of the ASA and ASA Foundation. "ASA'schapters, which are the backbone of our awarenessefforts on behalf of the autism community, will play acritical role in helping move this initiative forward.
Together, we can become an effective forcein increasing autism research over the nextdecade and beyond."
Additionally, the program will work withorgan procurement organizations, medicalexaminer's offices and statewide develop-mental disability programs to develop uni-form standards that are more sensitive to theneeds of donor families and result in proto-cols that will yield higher quality tissue thatis more conducive to broad applications ofautism research.
The Autism Tissue Program is a science-driv-en brain tissue donation program that makes post-mortem brain tissue available to as many qualified sci-entists as possible to advance autism research.
Without brain tissue, studies that could lead to meth-ods to diagnose autism earlier, medical treatments andan eventual cure for autism spectrum disorders cannotbe done.
Iowa Lt. Gov. Sally J.Pederson, a NAAR trustee,has played a critical role
expanding the Autism TissueProgram in Iowa.
The Autism Tissue Program is co-sponsored by NAAR, theAutism Society of America and the M.I.N.D. (Medical
Investigation of Neurodevelopmental Disorders) Institute atUC Davis, with the National Institutes of Child Health &Human Development (NICHD), Mental Health (NIMH),
and Neurological Disorders & Stroke (NINDS).
To enroll or for more information, call (877) 333 - 0999
or visit www.MemoriesofHope.org
Science &Science & Research:Research: Exploring Autism Website Translated Exploring Autism Website Translated
NAARRATIVE - Spring 2003 Page 7
NNAAR FAAR Funds Tunds Trranslation of “Exploring Aanslation of “Exploring Autism” Wutism” Websitebsite e intinto Spanish & Fo Spanish & Frrencenchh
AAn acclaimed web-based genetics education tool forparents and family members of individuals withautism that was originally funded by the NationalAlliance for Autism Research (NAAR) has now beentranslated into Spanish and French.
The website, www.exploringautism.org, is designed topromote genomic literacy among families with a histo-ry of autism spectrum disorders so that they can betterunderstand the genetic components of autism, the lat-est genetic research advances and the potential impli-cations of those advances. The website is dedicated tohelping families who are living with the challenges ofautism stay informed aboutbreakthroughs involving thegenetics of autism.
The Exploring Autism websiterecently received an "A" grade ina review by Education World, aleading online resource forteachers and parents.
NAAR funded the translation of the site, which wascoordinated by the Center for Human Genetics atDuke University Medical Center in Durham, N.C.and Tufts University/New England Medical Center inBoston, MA.
"The availability of Spanish, French and English lan-guage versions of Exploring Autism will greatly improveaccess to this important information for families andhealth care providers throughout the world," said Dr.Margaret Pericak-Vance, professor and director of theCenter of Human Genetics at Duke UniversityMedical Center. "Families whose lives have beentouched by autism desperately seek information aboutthis neuro-developmental disorder. Exploring Autismoffers families seeking information up-to-date, accu-rate and understandable information about the genet-ic basis of autism."
Dr. Pericak-Vance noted that the web site is the resultof a collaborative effort among the Autism GeneticsCooperative (AGC), an international group of autismresearchers throughout North America and Europe.
The website's architecture allows users to navigate the siteeasily and and locate useful information, read currentnews on autism and take part in an online surveydesigned to help researchers evaluate the genetic educa-tional needs of families and other people who visit thesite.
The website is organized by the following key sections:
What is Autism - Provides an overall description of the autismspectrum disorders, including diagnosis information and genet-ic conditions associated with autism.
Genetics Overview - Features a glossary of terms and anexplanation of tools used to help researchers locate suscepti-
bility genes and informa-tion on recent investiga-tions on certain chromo-somes.
History of Autism -Includes a timeline ofimportant advances inautism diagnosis and
research.
Autism & Environmental Factors - Explores the theory of com-plex inheritance and the possible relationship between theenvironment and autism.
Family Stories - Shares the stories of families with children withautism.
Frequently Asked Questions - Lists questions and answers onautism and inheritance, what genes are thought to beinvolved in autism spectrum disorders, and ongoing geneticautism studies.
Survey - Online survey open to all users that is being used tohelp the Autism Genetics Cooperative determine the educa-tional needs of families and develop additional educationalmaterials.
NAAR initially funded the website through a $41,912grant awarded in 2001 to Dr. Pericak-Vance, at DukeUniversity Medical Center, and Dr. Susan Folstein,Department of Psychiatry, Tufts University/New EnglandMedical University. In 2002, NAAR provided additionalfunding for the translation of the website, which was com-pleted by Dr. Catalina Betancur, a member of the AGC.
For more information: www.exploringautism.org

Science &Science & Research: Pharmacological Interventions Research: Pharmacological Interventions
NAARRATIVE - Spring 2003 Page 8
Pharmacological TPharmacological Trreatment Opeatment Options ftions for Aor Autism utism Using Neuroleptic Medications - PART ONE OF TWO
By C.T. Gordon, III, M.D.NAAR Medical Affairs Committee
PPsychopharmacologic research over the past severaldecades has given us a safe and effective supply ofmedications that can be applied to the treatment ofautism. Many stem from the treatment of such con-ditions as attention deficit hyperactivity disorder(ADHD), anxiety disorders, depressive and bipolardisorders and psychotic disorders.
These medications effectively treat anumber of symptoms and behaviors fre-quently present in individuals withautism.* These include hyperactivity,impulsivity, attentional difficulties, anxi-ety, obsessive-compulsive symptomatol-ogy, repetitive motor behaviors (for exam-ple, tics and stereotypies), depression,mood swings, agitation, aggression, self-injurious behavior and insomnia.
Most of these clinical characteristics areconsidered "associated behaviors" inautism. Impairments in certain aspects ofattention (for example, joint attention) and repetitive,ritualized behaviors are examples of core autisticsymptomatology, which can be positively affected bymedication.
The ultimate goal of medication in an individual whohas autism is to prepare the brain's physiology to takeoptimal advantage of other aspects of treatment.These efforts include behavioral, educational andother experiential learning that can directly addresscore autistic cognitive impairments such as receptive,expressive, and pragmatic language abilities, socialdeficits and self-directed, repetitive behavior.
In other words, pharmacologic intervention shouldtypically be viewed as only one part of a multi-modaltreatment plan for an individual with autism. Thegoal of medication as well as all other treatments inautism is to maximize the individual's functioning.
There are currently no "cures."
OVERVIEW OF MEDICATIONS
In this two-part series, we will focus on three majorgroups of medications: neuroleptics, anti-depressant/anti-anxiety agents and stimulants. In partone, we will focus on neuroleptics.
It will become readily apparent that many ofthese medications affect more than onesymptom or behavior. That is, they are rel-atively nonspecific in terms of their bene-fits. For each of these commonly prescribedgroups of medications, general indicationsand side effects will be discussed.
As the medical community gains a betterunderstanding of the genetics and biochem-istry of autism, it will be possible to developpharmacologic therapies which directlyaddress underlying abnormalities; ie, morespecific treatments. However, the potentialbenefits of these nonspecific medicationsshould not be underestimated. In someindividuals they can result in a significant
increase in the rate of learning or reduce aggressivebehavior for an individual with autism so that institu-tionalization can be avoided.
It must be recognized that different people may respondto the same medication quite differently and an indi-vidual's response at different stages of brain develop-ment may vary depending upon age, associated medicalconditions and other factors.
For example, a medication that produces a behavioralside effect preventing its use for a child at age seven maynot produce this side effect and be quite useful at ageten. The brain is continually developing, especially dur-ing the first 21 years of life, and this needs to be takeninto account. Because of individual differences in brainchemistry as well as differences in the rate of metabo-lism (breakdown) of medications, markedly differentdoses may be required for different individuals.
(please see Pharmacological Interventions on page 9)
* for the purposes of this article, autism refers to all autism spectrum disorders.
The goal of medication as wellas all other treatments in autism is to maximize an individual's functioning.
There are currently no "cures."

NAARRATIVE - Spring 2003 Page 9
Science &Science & Research:Research: Pharmacological Interventions Pharmacological Interventions Pharmacological Interventions Pharmacological Interventions (continued from page 8)
NO GUESSING
Even though the situation is quite complex, the pre-scription of medication for autism is not purely a "shotin the dark." Patients are not guinea pigs, and a physi-cian should not simply prescribe whatever first comesto mind as an experiment.
There have been many scientifically sound, double-blind, controlled studies of all thesemedications. Most have been done onadults with other conditions; however,there is a sound base of information onpsychopharmacologic agents from stud-ies in children and a growing body ofscientific data on medications in chil-dren and adolescents with autism. Theprescribing physician needs to be awareof these studies and experienced in thepharmacologic treatment of patientswith severe neuro-developmental disor-ders, including autism.
Optimizing the benefits of the available medicationsrequires that the physician bring to bear both art andscience. Accurate conceptualization of symptoms andbehaviors into groups of treatment-relevant target symp-toms is necessary for medications to be effective. Theseinterpretations and judgments are based on historyfrom parents, teachers and other therapists, as well asdirect observation of the individual with autism.
Clear target symptoms need to be established, informa-tion about transient and long-lasting possible sideeffects should be outlined, dosing should start low andescalate carefully, and a trial needs to be conducted foran adequate length of time.
Furthermore, medications need to be prescribed sys-tematically. There is no room for "magic concoctions."Medications need to be prescribed one at a time so thateffectiveness and side effects can be accurately deter-mined.
There are certainly times when a patient benefits froma combination of medications, but excessive polyphar-macy should be avoided to minimize side effects andprevent drug interactions.
NEUROLEPTICS
Neuroleptics, also called anti-psychotic medications,have been the most widely studied class of psychophar-macologic agents in autism over the past 35 years. Thedrugs were originally developed for the treatment ofschizophrenia, a psychotic illness with prominent delu-sions, hallucinations and disorganized, illogical think-ing.
Until the mid 1970s, autism was hypothesized to be avery early onset form of schizophrenia;this formed part of the rationale forusing these agents in autism.Neuroleptics are effective in treatingsevere anxiety, agitation and aggressionin several non-schizophrenic popula-tions and there was hope they wouldprovide similar benefits to individualswith autism. In addition, neurolepticsare strong blockers of the neurotrans-mitter dopamine. (During the 1960sand early 1970s, a "dopamine theory"was used to explain autism, suggestingthat excessive dopamine was responsi-
ble for much autistic symptomatology.)
Since the 1960s, there have been multiple controlledstudies of neuroleptics in children and adolescentswith autism, with the majority involving drugs likehaloperidol (Haldol) and lesser numbers with thiori-dazine (Mellaril) and trifluoperizine (Stelazine). Theseneuroleptic agents were found to decrease hyperactivi-ty, stereotypic behavior (self-stimulatory, simple andcomplex movements), withdrawal, aggression and tem-per outbursts, and facilitate learning in children withautism.
The problem with these neuroleptics is their side-effectprofile, which includes sedation as well as acute andchronic neurologic side effects. Acute neurologiceffects include tremors, slowing down of movementsand stiffening of the muscles (a Parkinson-like syn-drome). More chronic neurologic side effects includewithdrawal or tardive dyskinesias. Dyskinesia is a syn-drome that causes potentially irreversible, involuntarymovements, which may develop in patients who havebeen treated with neuroleptic medications.
Withdrawal dyskinesia involves abnormal movementsthat occur for several weeks to months when the dosage
(please see Pharmacological Interventions on page 10)
There are certainly times when a patientbenefits from a combination of medica-
tions, but excessive polypharmacy shouldbe avoided to minimize side effects and
prevent drug interactions.

Science &Science & Research: Research: Pharmacological Interventions Pharmacological Interventions
NAARRATIVE - Spring 2003 Page 10
Pharmacological Interventions Pharmacological Interventions (continued from page 9)
of the neuroleptic is lowered too rapidly. Tardive dysk-inesia is a similar involuntary movement disorderwhich may occur, usually, after years of neuroleptictreatment. However, it can sometimes occur withshorter courses of treatment. In some cases, even if theneuroleptic is discontinued, the tardive dyskinesia cancontinue and become permanent.
HALDOL AND THE NEWER NARCOLEPTICS
Despite their adverse effects, Haldol and similar neu-roleptics remained the major medicationsused in autism until the 1990s. Over thepast ten years or so, a new generation ofneuroleptics has been introduced on themarket with equal or better effectivenessfor schizophrenia and far fewer side effects.
This new group of neuroleptics sharessome similar chemical effects with theolder neuroleptic group, but there are alsoimportant differences. In general, the newgeneration of neuroleptics has less success in blockingdopamine type II brain receptors but more in blockingdopamine type I receptors, and much more blockade ofseveral different types of serotonin receptors. Thesedrugs have been called "atypical neuroleptics" becauseof their similar clinical effects but differing neuro-chemical profile. Presently, the six that have beenapproved by the FDA and widely available are risperi-done (Risperdal), olanzapine (Zyprexa), clozapine(Clozaril), quetiapine (Seroquel), ziprasidone (Geodon)and the newest, aripiprazole (Abilify).
Risperidone Of the five atypical neuroleptics, risperidone has beenthe most investigated in a controlled study of autism.Researchers found risperidone to effectively treatmotor stereotypies, hyperactivity, impulsivity, agitationand aggression in several studies. Last year, the NewEngland Journal of Medicine published a controlled studyof risperidone in children with autism that reportedthe drug was useful in controlling aggression and self-injurious behavior in children with autism and relateddisorders. This large-scale study was funded by theNational Institute of Mental Health (NIMH), which iscurrently sponsoring several childhood psychopharma-cologic studies as part of its research units for
pediatric psychopharmacology (RUPPs). Thus far, theside effect profile of risperidone in individuals withautism has been favorable. Neurologic side effects areshown to be drastically reduced, although acuteextrapyramidal symptoms, such as tremors, the slowingdown of movements and the stiffening of muscles, stilloccur. The potential for tardive dyskinesia is as yetunclear, since risperidone has not been on the marketlong enough for it to be fully assessed. The most com-mon side effects of risperidone have been increasedappetite and, less often, sedation.
OlanzapineOlanzapine is probably the second-mostprescribed atypical neuroleptic (after risperi-done) for autism, although, to date, thereare no published controlled studies involv-ing individuals with autism. In my experi-ence, benefits and side effects are similar tothose seen with risperidone overall.However, an individual patient oftenresponds much better to one versus theother, and there is no way to predict which
of the two may be more beneficial.
ClozapineClozapine is more rarely used because it has a possiblelife-threatening side effect of lowering the white bloodcell count, so that regular blood testing is required aslong as the patient continues to take the medication.However, in my experience, clozapine has been anextremely effective medication for severe aggressionand agitation in very affected, treatment-resistant ado-lescents with autism. It has worked when nothing elsehas.
QuetiapineCurrently, there is little published data regarding que-tiapine for autism, but my clinical experience is that itmay be a useful alternative, especially when patientshave prohibitive side effects with the other atypical neu-roleptics. Thus, even though its role in autism is yet tobe established, it is showing some initial promise.
ZiprasidoneZiprasidone is the fifth and most recently released atyp-ical neuroleptic available in the U.S. There have beenno controlled studies to date on ziprasidone, but datafrom a series of 12 cases recently published as well as
(Please see Pharmacological Interventions on page 13)
Even though the situationis quite complex, the pre-
scription of medication forautism is not purely a "shotin the dark." A physician
should not simply prescribewhatever first comes tomind as an experiment.
NAARRATIVE - Spring 2003 Page 11
Science &Science & Research:Research: CDCCDC Prevalence Study Prevalence Study
New CDC Study Shows New CDC Study Shows Prevalence of Autism is Higher Prevalence of Autism is Higher
SAB Member Marshalyn Yeargin-Allsopp, M.D. is Lead Author
AAn important study on the prevalence of autism in metropolitan Atlanta con-ducted by the National Center on Birth Defects and DevelopmentalDisabilities (NCBDDD) showed the prevalence was approximately 10 timeshigher than the rates from studies conducted in the United States 10 yearsago.
The lead author of the NCBDDD prevalence study, Marshalyn Yeargin-Allsopp, M.D., a member of the NAAR Scientific Advisory Board, said theprevalence rate in metropolitan Atlanta confirms the impressions from com-munity service providers that autism is more common today.
"Autism is not a rare condition," she said. "More children with autism are receiv-ing specialized services from school systems and other service providers."
According to the study, published in the Jan. 1, 2003 edition of the Journal ofthe American Medical Association (JAMA), the prevalence for autism in met-ropolitan Atlanta is 3.4 per 1,000. The population-based study included anestimated 290,000 children from five counties in metropolitan Atlanta (ages 3to 10 years old) to determine the prevalence of autism. Children were iden-tified through screening and abstraction of records at multiple medical andeducational sources, with expert review to determine autism case status.
Dr. Yeargin-Allsopp noted that the NCBDDD study is probably conservative,due to the fact that 91% of the children included in the study met the study'sdiagnostic criteria for “autistic disorder” and many children on the milder endof the spectrum, who are typically diagnosed with Pervasive DevelopmentalDisorder Not-Otherwise-Specified (PDDNOS) or Asperger Syndrome, were notincluded.
To get a better idea of the national prevalence of autism, the NCBDDD isconducting similar studies in communities in Colorado, California,Maryland/Delaware, Pennsylvania, North Carolina, Florida, Arizona, WestVirginia, South Carolina, New Jersey, Arkansas, and Utah.
"This is a wide geographic distribution of study sites with very different socieo-economic characteristics that will give us a good idea of how the prevalencerates may vary across the country," said Dr. Yeargin-Allsopp.
Along with prevalence, the NCBDDD is also focusing on the etiology, orcause, of autism through its CADDRE study (Centers for Autism andDevelopmental Disabilities Research and Epidemiology), which is takingplace in Colorado, California, Maryland/Delaware, Pennsylvania and NorthCarolina.
The CADDRE study is a collaborative case control study that includes metro-politan Atlanta, which is serving as a model for these five sites that are look-ing at potential causes. The same methods are being used for all sites, whichwill focus on a wide variety of risk factors, including immunological, nutrition-al and genetic factors.
NNAAR PlaAAR Playyed ed KKeey Ry Role in theole in theGenesis of CDCGenesis of CDCPrPreevvalence Salence Studytudy
TThe results of CDC’s latestprevalence study on autismreveal eye-opening statisticsthat help confirm what manyparents and loved ones havelong suspected: autism is nota rare disorder - it is a serioushealth problem facing thenation.
NAAR’s early efforts to getthe CDC interested in theprevalence of autism can betraced to a groundbreakingconference that took place inNov. 1997, which was held inAtlanta and co-sponsored byNAAR and the CDC.
The conference, Autism:Emerging Issues in Prevalence &Etiology, was the first meetingever to examine the preva-lence of autism in the U.S.and served as the main cata-lyst for the CDC’s subse-quent investigations andinterest in the epidemiologyof autism. Several monthsafter the conference, at therequest of concerned parentsand with the help of NAAR,the CDC began its landmarkstudy of autism prevalence inBrick, NJ.
Today, just over five yearsafter that first conference inAtlanta, we are beginning tosee the benefits of NAAR’searly efforts working with theCDC and fostering its focuson autism.

NAARRATIVE - Spring 2003 Page 12
NAAR’s Autism PollNAAR’s Autism Poll
NNAAR AAAR Autism Putism Poll: oll: Americans WAmericans Want Morant More Ae Action on Action on Autismutism
Most Feel Autism is a Serious Problem & Call for Increased Investments in Research
NOTE: Before reading this story, learn your “autism IQ,” by takingNAAR’s autism IQ test on page 13 and see how your answers comparewith the American public’s responses.
AAmericans want much more information and a fargreater research commitment focusing on the causesand treatment of autism spectrum disorders, accord-ing to a new poll conducted by the National Alliancefor Autism Research (NAAR). The poll was designedto gauge the general public's awareness of autism anddetermine what concerns the coun-try has regarding autism and thestate of autism research.
The poll results have identified thata gap exists in autism awareness andknowledge among the Americanpublic, even though manyAmericans either have autism intheir family or have a close friendwith autism in the family.
The NAAR poll indicates that 87%of Americans feel that autism is a serious problem,and 71% of Americans want to learn more about thedevelopmental disorder.
In addition, almost a fifth of the U.S. populationknows someone affected by an autism spectrum dis-order. The poll also shows that Americans stronglysupport an increase in research, funding for researchand information sharing that can enable the medicalcommunity in the U.S. to address autism at the levelit deserves.
"The findings of this poll call to mind the hunger forinformation that I felt when my son was first diag-nosed," said Karen London, NAAR co-founder. "Youdon't have to be a parent to see that autism is some-thing about which we all need to be better informed."
The poll uncovered a sense of urgency that Americansfeel regarding autism:
· 62% of Americans are aware of the rising autism prevalence level
· 69% of Americans worry about autism going undiagnosedbecause there is no reliable (biological) test to diagnose thedisorder
When asked about research funding to find treat-ments and a cure for autism, 89% of Americans sup-port an increase in the amount spent. A majority ofAmericans (53%) think the Federal governmentshould play a major role in ensuring that this increase
occurs, and a large majority ofAmericans (81%) would like privatecorporations, including pharmaceu-tical companies, to play a larger rolein autism research funding.
Autism research currently has verylittle commitment from private cor-porations, and is approximately the50th lowest area of medical researchout of 60 areas funded by theNational Institutes of Health.
Americans are familiar with some aspects of autism,such as potential causes, however they are largely unfa-miliar with many basic facts about the disorder.
For example, even though they feel there is a growingproblem, 77% of Americans undercount the numberof people in the U.S. who have autism. Recent stud-ies suggest that over one million people in the U.S.have autism spectrum disorders, which occur in anestimated one out of every 250 births. This makesautism the second most common developmental dis-order, second only to mental retardation.
The survey found other common misperceptions:
· 55% of Americans are not sure or think there is a clinicaltest for autism
· 69% of Americans do not know that autism is more preva-lent in boys than girls
Currently, there is no way to biologically diagnoseautism. A variety of symptoms and warning signs areused to determine whether a child has autism,
(please see NAAR Poll on page 13)
NAAR’s poll identified a gap in autism awareness and
knowledge among the general public and uncovered
a sense of urgency that Americans feels regarding autism.
NAARRATIVE - Spring 2003 Page 13
NAAR’s Autism Poll NAAR’s Autism Poll NAARNAAR pollpoll (continued from page 12)
particularly a delay in developing language skills. Autismis approximately four times as prevalent in boys than girls.
While Americans are generally proving themselves to besavvy consumers of medical information, there still existmajor misperceptions about autism that may be rooted inthe sources of information about the disorder. Accordingto the poll, 35% of Americans receive information aboutautism from television programs, while just three percentreceive information from their doctors.
To view the complete major findings from the poll,
visit www.naar.org NAAR's autism poll was a comprehensive, nationally representative telephonestudy among 500 Americans 18 years of age and older and was conducted byGlobal Strategy Group in conjunction with Widmeyer Communications forNAAR. The margin of error for the study is +/- 4.4% at the 95th percent confi-dence interval level.
What is your Autism IQ?What is your Autism IQ?DD id you know that approximately one in fiveAmericans has a relative with an autism spectrumdisorder or close friend with autism in their family, yetan estimated 30% of the American population can-not identify a single warning sign or symptom ofautism? *
Interested in determining your "Autism IQ ?" Takethis short true/false test and find out:
TRUE OR FALSE?
1) There is currently no medical test to diagnoseautism.
2) The biggest problem with diagnosing autism isthat symptoms do not appear until age five orolder.
3) Autism occurs in roughly equal numbers of boysand girls.
4) There is no one recognized treatment for autism.
5) Typically, autistic children can outgrow autism.
6) Autistic children have poor communication andsocial skills because they are geniuses in math.
7) Many scientists think that heredity and genesplay a role in the cause of autism.
8) Most scientists and doctors know what causesautism.
9) It is estimated that as many as 1 millionAmericans suffer from autism.
10) Over half of the number of children with autismhave been found to be the result of poorparenting.
For the answers and to see the results of how the American public answered these
questions, please turn to page 15.
For the purposes of this test, autism refers to all autism spectrum disorders,including Asperger Syndrome, Autistic Disorder, Childhood DisintegrativeDisorder (CDD), Pervasive Developmental Disorder Not Otherwise Specified(PDDNOS) and Rett Syndrome.
*Based on a recent poll conducted in U.S. designed to gauge America'sawareness of autism.
Pharmacological IntPharmacological Interer vventions entions (con’t. from page 10)
my clinical experience suggest that it has potential forimproving symptoms of aggression, agitation and irritabilityin children with autism. It does not seem to cause weightgain as do the other atypical neuroleptics and has not beenassociated with major side effects, in my experience.
Aripiprazole Another anti-psychotic medication called aripiprazole hasrecently been approved by the FDA. This medication has anovel mechanism of action. While all of the other abovementioned medications block receptors, aripiprazole par-tially blocks and partially stimulates receptors. Thus it ishypothesized that it stabilizes the functioning of the neuro-transmitters dopamine and serotonin. Aripiprazole appearsto have a very favorable side effect profile. It does not havethe weight gain or cardiac side effects that have limited theutility of the others. At this time this medication is too new toreport on efficacy in autism, but may be an important addi-tion to the existing arsenal of medications.
To summarize, neuroleptics are very useful for a group ofchildren with autism who have prominent hyperactivity,impulsivity, agitation, temper outbursts or aggressiontowards self or others. Often, once these behaviors arereduced, these individuals can benefit from their behavioraland educational interventions. Atypical neuroleptics gen-erally are equal to or better than the old group of neu-roleptics in terms of effectiveness and superior in terms ofside effects. Usually, in clinical practice, one or more atypi-cal agents are first tried before the older neuroleptics areconsidered. However, to date, there has not been a studydirectly comparing atypical to typical neuroleptics inautism. In Part II: Using Anti-Depressants, Anti-Anxiety Agents, Stimulants &
Other ADHD Medications in the treatment of autism
Dr. Gordon is a child psychiatrist in private practice
and a NAAR trustee. He is also the father of a teenage son with autism.

Science &Science & Research Research
NNAAR Co-FAAR Co-Funds Larunds Largesgest St Study ttudy to Dato Date on MMR & Ae on MMR & AutismutismInvestigators Report No Association with Autism on a Population Basis By Andy Shih, Ph.D., Director of Research & Programs
RResults of the largest study to date focusing on theMMR (measles, mumps, rubella) vaccine and autism,co-funded by the Danish National ResearchFoundation, the Centers for Disease Control &Prevention (CDC) and NAAR, and published in theNew England Journal of Medicine, indicate no increasedrisk for developing autism among children whoreceived the MMR vaccine as compared to childrenwho did not receive the vaccine.
The registry-based study, conducted by researchers atthe Danish Epidemiology ScienceCenter at Aarhus University inDenmark, focused on more than530,000 children born inDenmark between 1991 and 1998.Approximately one-fifth of thosechildren did not receive the MMRvaccination. The design and popu-lation size of this study are at thecore of its strength, which separates it from any previ-ous studies focusing on MMR and autism.
The project, Risk Factors for NeurodevelopmentalDisorders: MMR Vaccine & Childhood Autism, utilizesDenmark's unique health registry data - which tracksbirth records, vaccination records and records indicat-ing a diagnosis for autism spectrum disorders. Byusing this comprehensive system, researchers were ableto take advantage of a very large population base andcompare risk for autism between children who receivedthe MMR vaccination, and those who did not. Manyother studies focusing on MMR and autism have notbeen able to make this type of detailed comparison dueto the limits of the health records involved with thosestudies.
The Danish study provides the most solid statisticalevidence to date against the association between theMMR vaccine and autism on a population basis. However, more research is needed to address the issueof whether smaller subgroups of the population arevulnerable to the vaccine. While the study did notfocus exclusively on children with regressive autism, itdoes suggest the MMR vaccine does not contribute
to regressive autism. If such a trend had emerged, itwould have clearly been reflected in an overall increasein the number of autism cases listed in the study -therefore increasing the relative risk. As the authorsthemselves have stated, this was not the case.
The study does not support the hypothesis that theMMR vaccine is associated with regressive autism,based on the relative risk stated in the study (.92),which is calculated from findings that examine thenumber of children with autism who received the vac-cine and those with autism who did not. If the MMR
vaccine is widely associated withregressive autism, the study wouldhave indicated a relative risk ofover 1.0
In other words, if a link existsbetween regressive autism and theMMR vaccine, the total number ofcases of children with autism who
received the vaccine would be higher, especially basedon the statistic that between 10-20% of children withautism have the regressive form of the disorder. A pop-ulation-based study of this size (over 530,000 children)would have clearly suggested such a trend. It is alsoimportant to emphasize that the Danish study wasdesigned to specifically examine the alleged linkbetween MMR and autism and no other vaccines.
In 2002, NAAR awarded an additional grant to theDanish research team to further delineate and analyzerelevant clinical parameters. Specifically, the 2002grant is allocated to further validation of the diagnosisof autism in the Danish Psychiatric Central Registerbased on diagnostic standards of the CDC. Results ofthe validation study are expected to generate a separatepaper that will likely be submitted for publication.
Additional studies focusing on vaccines and autism arecurrently being conducted in the U.S. The collectiveresults from all these studies will provide a clearer pic-ture on vaccines and autism and help the researchcommunity and the general public to develop a moreaccurate understanding of this controversial issue anda responsible public health policy.
NAAR funds and supports research that investigates all theories surrounding
potential causes of autism, includingwhether there is a link between vaccinesand autism, and encourages researchers
to submit proposals in this area.
NAARRATIVE - Spring 2003 Page 14

NAARRATIVE - Spring 2003 Page 15
Progressions Progressions
Answers to NAAR’sAnswers to NAAR’s Autism IQAutism IQ TestTest1) TRUE - Unlike other medical conditions, such as cancer, dia-betes and cystic fibrosis, physicians have no blood test or diag-nostic scan available to biologically diagnose autism spectrumdisorders. The diagnosis of autism is currently based solely on theobservation of behaviors. Autism is a complex biological disorderof the brain. (70% of respondents either got this question wrong ordid not know the answer)
2) FALSE - The most significant problem with the diagnosis ofautism is that there is no way to biologically diagnose the disorder.Children with an autism spectrum disorder will usually begin toshow clear, identifiable symptoms by the age of 18 months. Manyparents and experts can usually detect symptoms before thistime, however a formal diagnosis is typically made when the childexhibits a noticeable delay in developing language skills - nor-mally between the ages of two and three. Early diagnosis is essen-tial for autism spectrum disorders because interventions are mosteffective the earlier they are implemented. (63% of respondentseither got this question wrong or did not know the answer)
3) FALSE - Autism is approximately four times more prevalent inboys than in girls. Autism spectrum disorders affect people of allracial, ethnic and socioeconomic backgrounds. (66% of respon-dents either got this question wrong or did not know the answer)
4) TRUE - There is no medical protocol for the treatment of autism.While behavioral interventions and educational approaches,such as Applied Behavioral Analysis (ABA), are widely used to suc-cessfully mitigate symptoms, no one treatment has been recog-nized by any medical association as a specific medical treatmentfor autism spectrum disorders. (41% of respondents either got thisquestion wrong or did not know the answer)
5) FALSE - In most cases, autism is a lifelong condition. Most peo-ple with autism spectrum disorders require lifelong supervision andcare - and the most severely affected may never be able tospeak to tell their parents that they love them. (37% of respon-dents either got this question wrong or did not know the answer)
6) FALSE - Children and adults with autism spectrum disorders typ-ically have poor communications and social skills because autismis a brain disorder that impairs a person's ability to communicate,
respond to their surroundings or form relationships with others.While a small percentage of people with autism spectrum disor-ders display savant-like skills in math or art, most do not demon-strate such abilities. (46% of respondents either got this questionwrong or did not know the answer)
7) TRUE - A vast majority of the scientific community agrees thatgenes play a role in the cause of autism, which is considered tobe the most heritable of all neurological disorders. According toresearch: in identical twins, if one twin has an autism spectrum dis-order, the other twin has it between 60-90% of the time; and in fra-ternal twins, if one twin has an autism spectrum disorder, the othertwin has it about 10% of the time. (32% of respondents either gotthis question wrong or did not know the answer)
8) FALSE - Currently, the causes of autism are unknown and thereare no specific medical treatments or cures for the disorder.Despite research that has focused on a wide range of disciplines,including genetics, environmental factors and the neurosciences,no conclusive evidence has yet determined the cause or causesof autism. (32% of respondents either got this question wrong ordid not know the answer)
9) TRUE - Recent epidemiology studies have shown that autismspectrum disorders are ten times more prevalent than they werejust ten years ago. Autism spectrum disorders are considereddevelopmental disorders - encompassing physical, cognitive, psy-chological, sensory and speech impairments. Autism is the sec-ond most common developmental disability, next to mental retar-dation. Autism spectrum disorders occur in an estimated one inevery 250 births. Some studies place the prevalence even higher.(33% of respondents either got this question wrong or did notknow the answer)
10) FALSE - Poor parenting does not cause autism. In the 1950sand 1960s, however, the medical community generally believedthat autism was a psychological disturbance caused by emo-tionally detached or uncaring mothers. This belief - presented byDr. Bruno Bettleheim, who coined the phrase "refrigerator moth-ers" - was later proven totally incorrect. This profound misconcep-tion contributed to why the scientific research community neg-lected autism for decades. (19% of respondents either got thisquestion wrong or did not know the answer)
Board Update
Patricia Menendez Cambo, Esq., is a shareholderand chair of Greenberg Traurig LLP's InternationalPractice Group. She was formerly the Chief U.S.Legal Counsel for Telefonica, S.A., and is the motherof two children with autism spectrum disorders.
Andy Cerise has been a member of the New YorkStock Exchange since 1992 and is Managing Directorof the firm, Bear Wagner Specialists, LLC. He is amember of NAAR’s Long Island Board and the fatherof five children, including one who has autism.
Ann Boeker Gibbons, a former attorney andinvestment banker, is an information technology con-sultant and founder of the Maryland Autism Project,a school-based intensive behavioral program. She isalso the mother of child with autism.
Barri Rind has been influential in paving the roadfor inclusion of children with autism in the LakeWashington and Mercer Island school districts inWashington state. She is active with numerous Seattlearea charities and is the mother of a child with autism.
Daniel F. Ryan, Jr., is a member of the New YorkStock Exchange and Executive Director for S.G.Cowen Inc. He is active with the David Center, theYoung Autism Program Charitable Foundation andNAAR’s Long Island Board, and is the father of achild with autism.
NAAR is honored to announce that the following keyvolunteers have joined NAAR’s Board of Trustees tohelp shape and guide the development of NAAR.
NAARRATIVE - Spring 2003 Page 16
Progressions:Progressions: Walk F.A.R. for NAARWalk F.A.R. for NAAR
2002 Fall Walk F.A.R. for NAARFall Events Raise More Than $2.8 million for Autism Research !!!
MMany thanks go out to all our walk chairs, walk committee members, volunteers, sponsors and walk participants whomade the 2002 Fall Walk season such a tremendous success. You are the people making it happen.
Thank you!
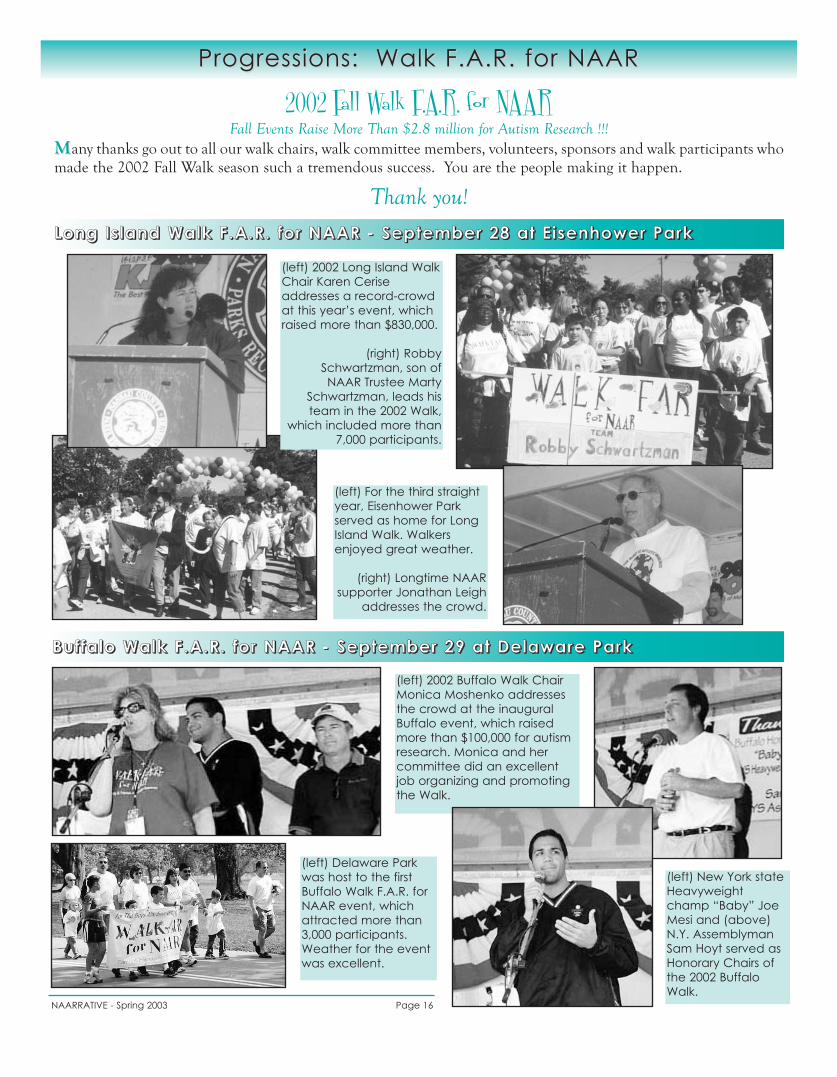
LLLLoooonnnngggg IIII ssss llllaaaannnndddd WWWWaaaallllkkkk FFFF ....AAAA....RRRR.... ffffoooorrrr NNNNAAAAAAAARRRR -- SSSSeeeepppptttteeeemmmmbbbbeeeerrrr 22228888 aaaatttt EEEE iiii sssseeeennnnhhhhoooowwwweeeerrrr PPPPaaaarrrrkkkk
BBBBuuuuffff ffffaaaalllloooo WWWWaaaallllkkkk FFFF ....AAAA....RRRR.... ffffoooorrrr NNNNAAAAAAAARRRR -- SSSSeeeepppptttteeeemmmmbbbbeeeerrrr 22229999 aaaatttt DDDDeeeellllaaaawwwwaaaarrrreeee PPPPaaaarrrrkkkk
(left) 2002 Long Island WalkChair Karen Ceriseaddresses a record-crowdat this year’s event, whichraised more than $830,000.
(right) RobbySchwartzman, son of NAAR Trustee Marty
Schwartzman, leads histeam in the 2002 Walk,
which included more than7,000 participants.
(left) For the third straightyear, Eisenhower Parkserved as home for LongIsland Walk. Walkersenjoyed great weather.
(right) Longtime NAARsupporter Jonathan Leigh
addresses the crowd.
(left) 2002 Buffalo Walk ChairMonica Moshenko addressesthe crowd at the inauguralBuffalo event, which raisedmore than $100,000 for autismresearch. Monica and hercommittee did an excellentjob organizing and promotingthe Walk.
(left) Delaware Parkwas host to the firstBuffalo Walk F.A.R. forNAAR event, whichattracted more than3,000 participants.Weather for the eventwas excellent.
(left) New York stateHeavyweightchamp “Baby” JoeMesi and (above)N.Y. AssemblymanSam Hoyt served asHonorary Chairs ofthe 2002 BuffaloWalk.
NAARRATIVE - Spring 2003 Page 17
Progressions:Progressions: Walk F.A.R. for NAARWalk F.A.R. for NAAR
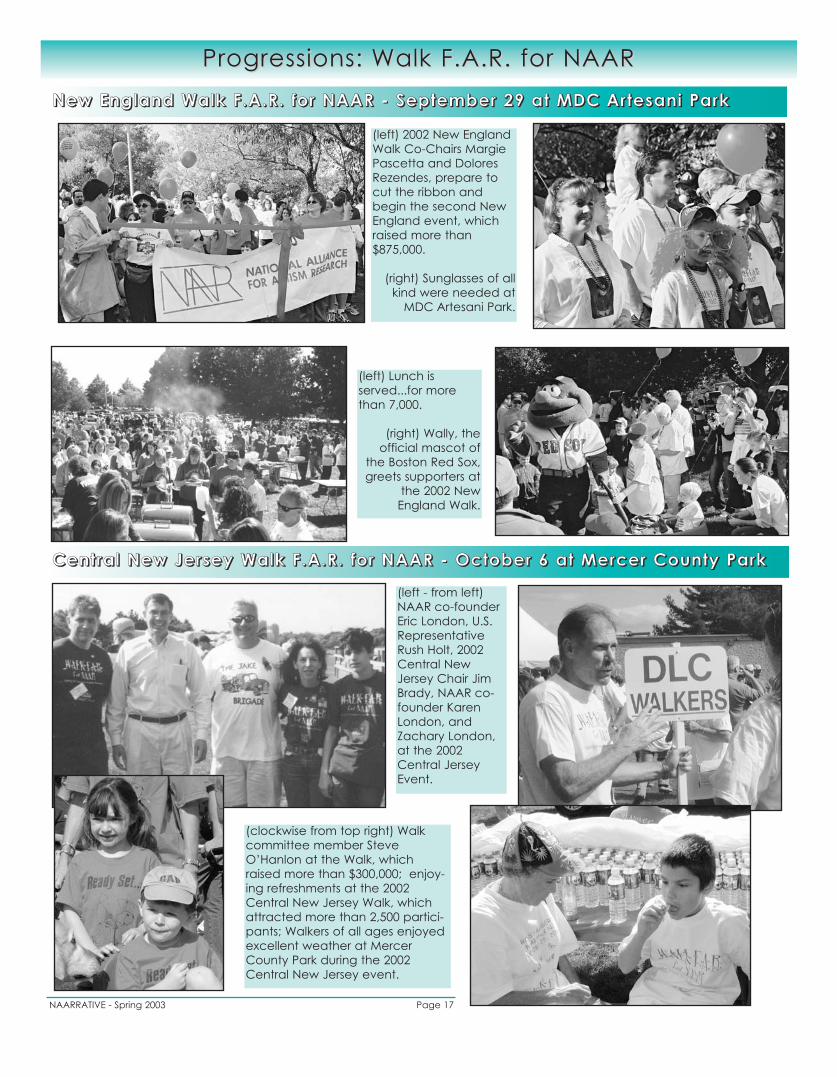
CCCCeeeennnntttt rrrraaaallll NNNNeeeewwww JJJJeeeerrrr sssseeeeyyyy WWWWaaaallllkkkk FFFF ....AAAA....RRRR.... ffffoooorrrr NNNNAAAAAAAARRRR -- OOOOccccttttoooobbbbeeeerrrr 6666 aaaatttt MMMMeeeerrrrcccceeeerrrr CCCCoooouuuunnnnttttyyyy PPPPaaaarrrrkkkk
NNNNeeeewwww EEEEnnnnggggllllaaaannnndddd WWWWaaaallllkkkk FFFF ....AAAA....RRRR.... ffffoooorrrr NNNNAAAAAAAARRRR -- SSSSeeeepppptttteeeemmmmbbbbeeeerrrr 22229999 aaaatttt MMMMDDDDCCCC AAAArrrr tttteeeessssaaaannnniiii PPPPaaaarrrrkkkk
(left) 2002 New EnglandWalk Co-Chairs MargiePascetta and DoloresRezendes, prepare tocut the ribbon andbegin the second NewEngland event, whichraised more than$875,000.
(right) Sunglasses of allkind were needed at
MDC Artesani Park.
(left) Lunch isserved...for morethan 7,000.
(right) Wally, the official mascot of
the Boston Red Sox,greets supporters at
the 2002 NewEngland Walk.
(left - from left)NAAR co-founderEric London, U.S.RepresentativeRush Holt, 2002Central NewJersey Chair JimBrady, NAAR co-founder KarenLondon, andZachary London,at the 2002Central JerseyEvent.
(clockwise from top right) Walkcommittee member SteveO’Hanlon at the Walk, whichraised more than $300,000; enjoy-ing refreshments at the 2002Central New Jersey Walk, whichattracted more than 2,500 partici-pants; Walkers of all ages enjoyedexcellent weather at MercerCounty Park during the 2002Central New Jersey event.
NAARRATIVE - Spring 2003 Page 18
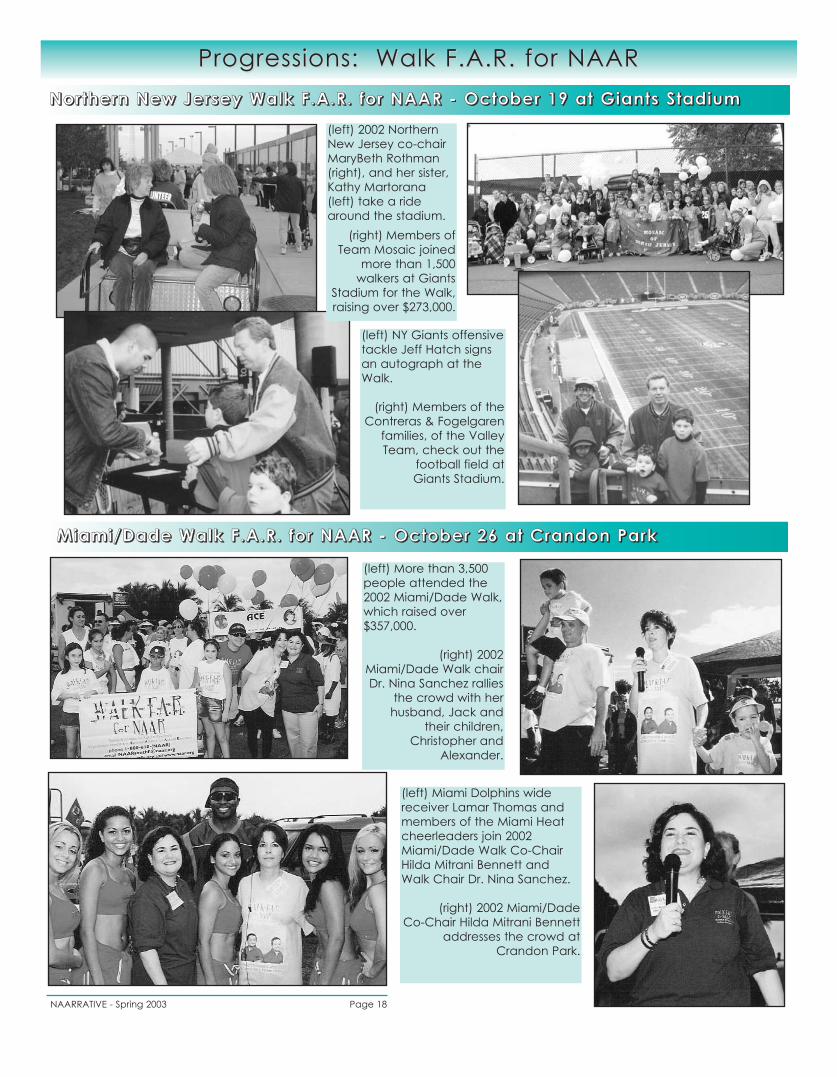
Progressions:Progressions: Walk F.A.R. for NAARWalk F.A.R. for NAARNNNNoooorrrr tttthhhheeeerrrrnnnn NNNNeeeewwww JJJJeeeerrrr sssseeeeyyyy WWWWaaaallllkkkk FFFF ....AAAA....RRRR.... ffffoooorrrr NNNNAAAAAAAARRRR -- OOOOccccttttoooobbbbeeeerrrr 11119999 aaaatttt GGGGiiiiaaaannnntttt ssss SSSSttttaaaaddddiiiiuuuummmm
MMMMiiiiaaaammmmiiii ////DDDDaaaaddddeeee WWWWaaaallllkkkk FFFF ....AAAA....RRRR.... ffffoooorrrr NNNNAAAAAAAARRRR -- OOOOccccttttoooobbbbeeeerrrr 22226666 aaaatttt CCCCrrrraaaannnnddddoooonnnn PPPPaaaarrrrkkkk
(left) 2002 NorthernNew Jersey co-chairMaryBeth Rothman(right), and her sister,Kathy Martorana(left) take a ridearound the stadium.
(right) Members ofTeam Mosaic joined
more than 1,500walkers at Giants
Stadium for the Walk,raising over $273,000.
(left) NY Giants offensivetackle Jeff Hatch signsan autograph at theWalk.
(right) Members of theContreras & Fogelgaren
families, of the ValleyTeam, check out the
football field at Giants Stadium.
(left) More than 3,500people attended the2002 Miami/Dade Walk,which raised over$357,000.
(right) 2002Miami/Dade Walk chairDr. Nina Sanchez rallies
the crowd with her husband, Jack and
their children,Christopher and
Alexander.
(left) Miami Dolphins widereceiver Lamar Thomas andmembers of the Miami Heatcheerleaders join 2002Miami/Dade Walk Co-ChairHilda Mitrani Bennett andWalk Chair Dr. Nina Sanchez.
(right) 2002 Miami/Dade Co-Chair Hilda Mitrani Bennett
addresses the crowd atCrandon Park.
NAARRATIVE - Spring 2003 Page 19
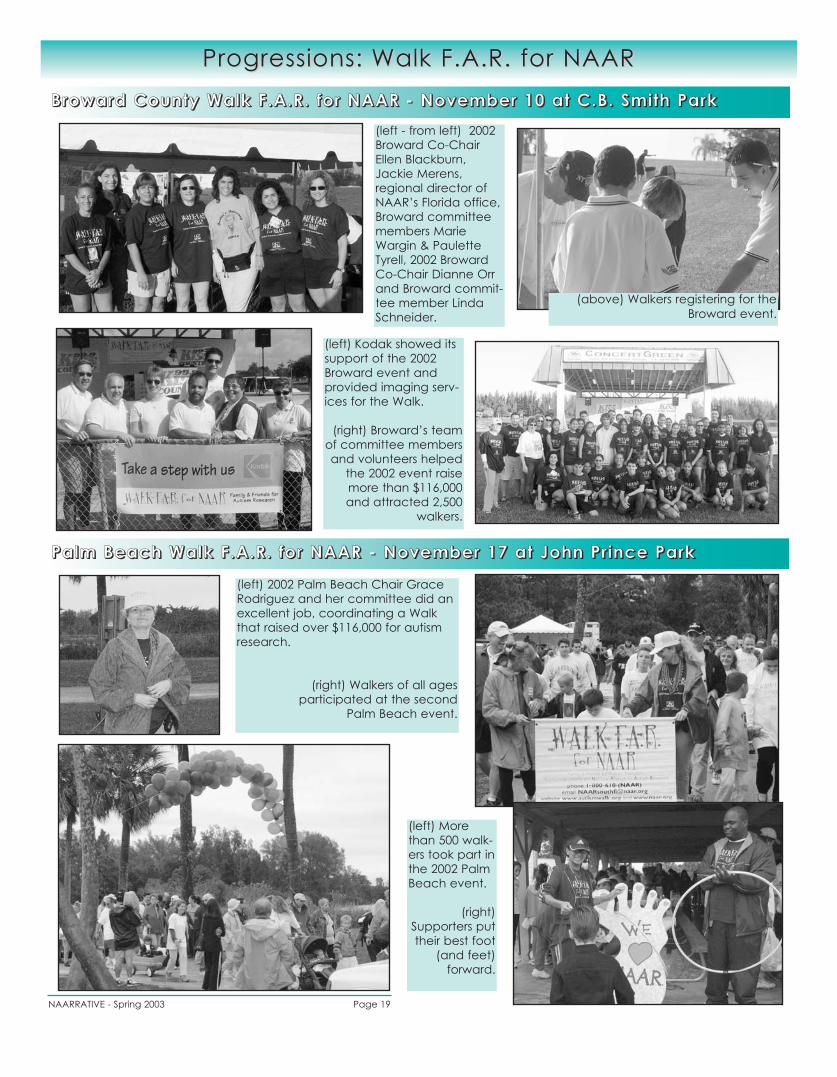
Progressions:Progressions: Walk F.A.R. for NAARWalk F.A.R. for NAARBBBBrrrroooowwwwaaaarrrrdddd CCCCoooouuuunnnnttttyyyy WWWWaaaallllkkkk FFFF ....AAAA....RRRR.... ffffoooorrrr NNNNAAAAAAAARRRR -- NNNNoooovvvveeeemmmmbbbbeeeerrrr 11110000 aaaatttt CCCC....BBBB.... SSSSmmmmiiii tttthhhh PPPPaaaarrrrkkkk
PPPPaaaallllmmmm BBBBeeeeaaaacccchhhh WWWWaaaallllkkkk FFFF ....AAAA....RRRR.... ffffoooorrrr NNNNAAAAAAAARRRR -- NNNNoooovvvveeeemmmmbbbbeeeerrrr 11117777 aaaatttt JJJJoooohhhhnnnn PPPPrrrr iiiinnnncccceeee PPPPaaaarrrrkkkk
(left - from left) 2002Broward Co-ChairEllen Blackburn,Jackie Merens,regional director ofNAAR’s Florida office,Broward committeemembers MarieWargin & PauletteTyrell, 2002 BrowardCo-Chair Dianne Orrand Broward commit-tee member LindaSchneider.
(left) Kodak showed itssupport of the 2002Broward event andprovided imaging serv-ices for the Walk.
(right) Broward’s teamof committee membersand volunteers helped
the 2002 event raisemore than $116,000and attracted 2,500
walkers.
(left) 2002 Palm Beach Chair GraceRodriguez and her committee did anexcellent job, coordinating a Walkthat raised over $116,000 for autismresearch.
(right) Walkers of all ages participated at the second
Palm Beach event.
(above) Walkers registering for theBroward event.
(left) Morethan 500 walk-ers took part inthe 2002 PalmBeach event.
(right)Supporters puttheir best foot
(and feet) forward.
National Office 99 Wall Street Research ParkPrinceton, NJ 08540www.naar.org888 - 777 - NAAR
RESEARCH. HOPE. COMMITMENT.
Address Correction Requested
Walk F.AR. for NAAR - 2003 Spring Schedule
For more information on any Walk F.A.R. for NAAR event, call (888) 777-NAAR or visit www.autismwalk.org
Greater Seattle Walk F.A.R. for NAARSunday, June 8thMarymoor Park, Redmond, WATo register, call (206) 464-5182
Pittsburgh Walk F.A.R. for NAARSunday, June 8thHeinz Field, Pittsburgh, PATo register, call (412) 487-6851
Westchester, NY / Fairfield, CT Walk F.A.R. for NAARSunday, June 8thManhattanville College, Purchase, NYTo register, call (203) 552-8980
Iowa Walk F.A.R. for NAARSaturday, June 14thGray’s Lake, Des Moines, IATo register, call (888) 777-NAAR
Cumberland, Maryland Walk F.A.R. for NAARSaturday, April 5thAllegany College, Cumberland, MDTo register, call (301) 697-2543
Carolina Walk F.A.R. for NAARSaturday, May 10thLowe's Motor Speedway, Charlotte, NCTo register, call (704) 333-0051
Rochester Walk F.A.R. for NAARSunday, May 18thThe Marketplace Mall, Rochester, NYTo register, call (888) 777-NAAR
National Capital Area Walk F.A.R. for NAARSunday, May 18thMontgomery County Fairgrounds, Gaithersburg, MDTo register, call (301) 519-0770
Greater Delaware Valley Walk F.A.R. for NAARSaturday, June 7thCooper River Park, Pennsauken, NJTo register, call (888) 777-NAAR
Nonprofit OrgUS Postage PaidParkesburg PA
Permit #27