Embed Size (px)
Citation preview
Case 11-13244-JKO Doc 119-1 F i led 05/20/1 1 Page 1 of 13
B
Y I r B Y-P NT
Name of Debtor: Case Number:
Reporting Period beginning I ~ t ( Period ending
Attach a copy of current month bank statement and bank reconciliation to this Summary of Bank Activity.A standard bank reconciliation form can be found at htt // . do' . ov /ust/r21 re info.htm.
NAME OF BANK; BRANCH:
ACCOUNT NAME: ACCOUNT NUMBEPURPOSE OF ACCOUNT: PAYROLL
Ending Balance per Bank StatementPlus Total Atnount of Outstanding DepositsMinus Total Amount of Outstanding Checks and oth debitsMinus Service Charges
Ending Balance per Check Register 0 4(a)
*Debit cards must not be issued on this account.
**If Closing Balance ls negative, provide expla tion:
The following disbursements were paid by Cas .,( 0 ec here if cash disbursements were authorized
b 'ted States Trustee)y Um
D ate Amou n t Payee Ulpo Reason for Cash Disbursement
The following non-payroll d' ursemen w ere made from this account:
Date A mount Payee Purpo se Reason for disbursement from thisaccount
(a) Ihe total of this line on Attachment 4A, 4B and 4C plus the total of 4D must equal the amount reported as"Ending Balance" on Schedule of Receipts and Disbursements (Page MOR-2, Line 7).
MOR-9
From Article at G
etOutO
fDebt.org
Case 11-13244-JKO Doc 119-1 F i led 05/20/11 Page 2 of 13
ATTACHMENT 58CHECK REGISTER - PAYROLL ACCOUNT
Name of Debtor: QoltJ wmw C N t : ~ / 'PX
Reporting Period beginning -/- 2-> l i Period ending -Q C
NAME OF BANK: BRANCH:
ACCOUNT NAME:
ACCOUNT NUMBER:
PURPOSE OF ACCOUNT: PAYROLL
Account for all disbursements, including voids, lost payments, stop payment, etc. In thealternative, a computer generated check register can be attached to this report, provided all theinformation requested below is included.
CHECK
~D T E ~ MBER PAYgE ~PRPgSE
TOTAL
From Article at G
etOutO
fDebt.org
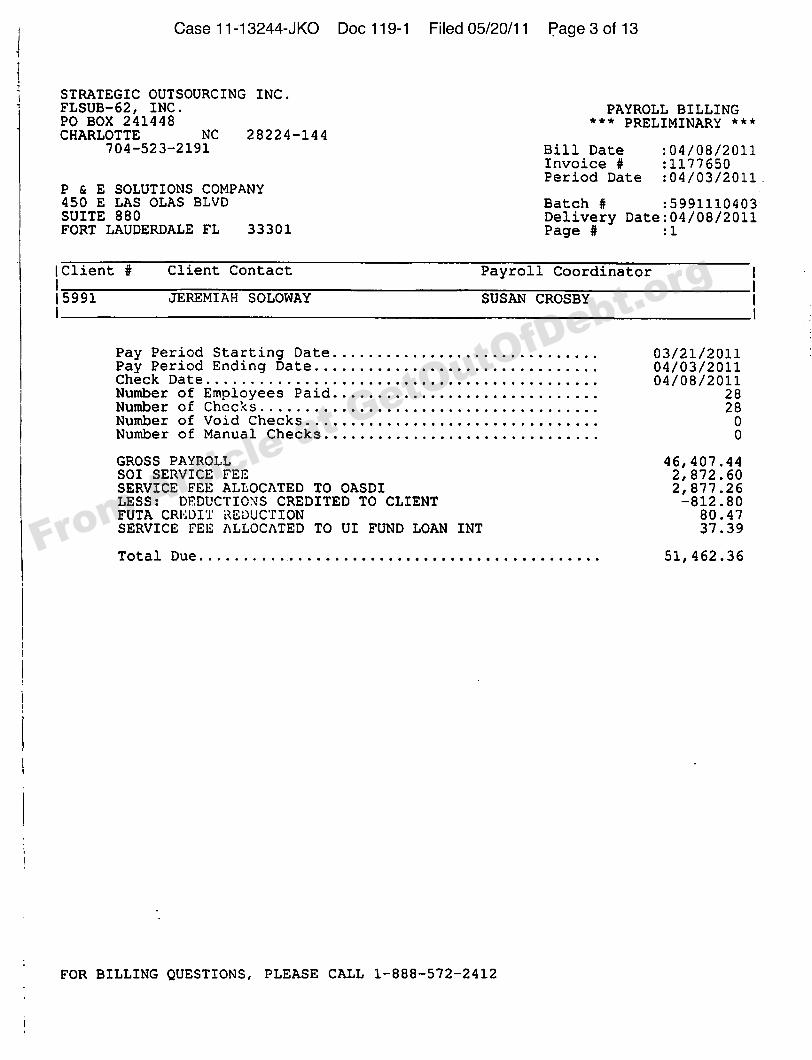
Case 11-13244-JKO Doc 119-1 F i led 05/20/1 1 Page 3 of 13
STRATEGIC OUTSOURCING INC.F LSUB-62, I N C . PAYROLL BILLINGPO BOX 241448 * * * PR E L IM I N ARY * * *CHARLOTTE NC 2 82 2 4 - 1 4 4
704-523- 2 1 91 Bill Date :04/0 8/2011I nvo i c e 0 : 1 17 7 6 50Period Date :04/03/2011 .
P & E SOLUTIONS COMPANY450 E LA S OLAS BLVD B atch f f :5991110403SUITE 880 Delivery Date:04/08/2011FORT LAUDERDALE FL 3 3 3 0 1 Page f f 0 ]
lClient ff Client Contact Payroll Coordinator
Il 5991 JEREMIAH SOLOWAY SUSAN CROSBYI
Pay Period Starting Date 0 3/21 / 2 0 1 1Pay Per i o d E n d i n g D at e 04/03/2011C heck Da t e 0 4/08 / 2 0 1 1Number of Employees Paid.. 28Number of Checks 28Number o f Vo i d Ch e c k sNumber of Manual Checks
0 0
GROSS PAYROLL 46, 407.44SOI SERVICE FEE 2, 872.60SERVICE FEE ALLOCATED TO OASDI 2 , 877.26LESS: DEDUCTIONS CREDITED TO CLIENT - 812 . 8 0FUTA CREDIT REDUCTION 80.47SERVICE FEE ALLOCATED TO UI FUND LOAN INT 37.39
T ota l D u e 51, 462.36
FOR BILLING QUESTIONS, PLEASE CALL 1-888-572-2412
From Article at G
etOutO
fDebt.org
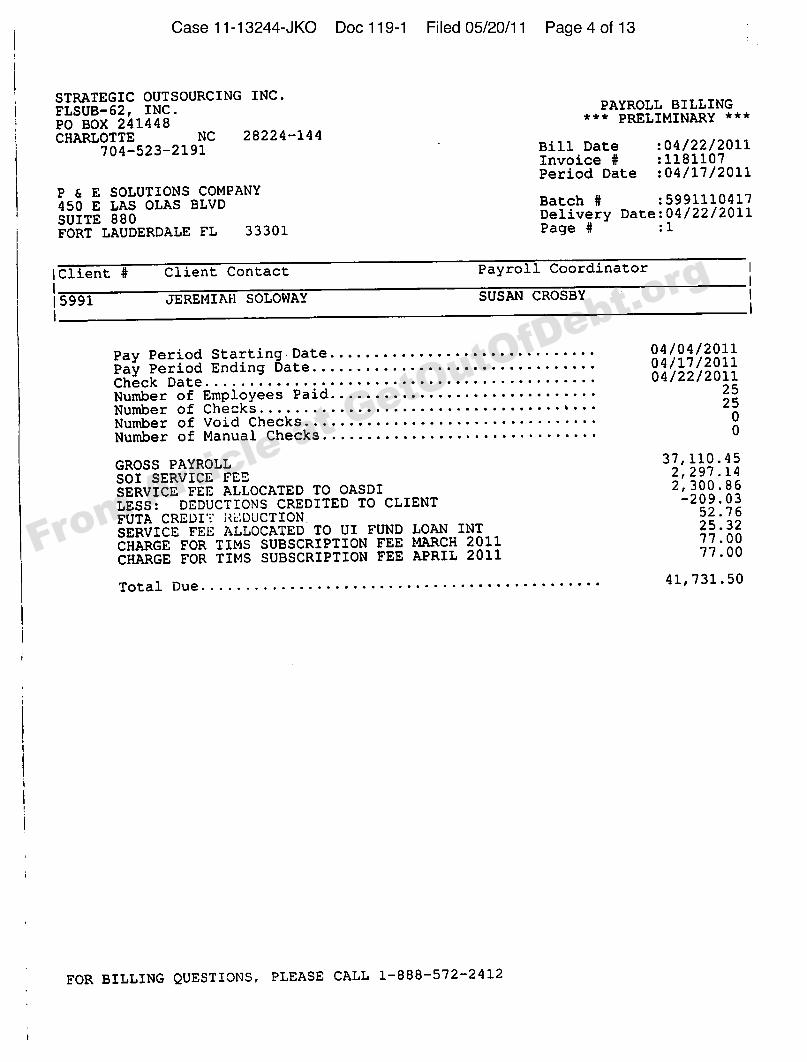
Case 11-13244-JKO Doc 119-1 F i led 05/20/1 1 Page 4 of 13
STRATEGIC OUTSOURCING INC.PAYROLL BILLING
F LSUB-62, I NC . " * * PR E L IM I N ARY * * *PO BOX 241448CHARLOTTE N C 2 82 2 4- 14 4
704-523-2191 Bill Date :04/22/2011I nvoice ¹ : 118110 7Period Date :04/17/2011
P 6 E SOLUTIONS COMPANY450 E LAS OLAS BLVD B atch ¹ :5991110417
SUITE 880 Delivery Date:04/22/2011
FORT LAUDERDALE FL 33301 Page ¹ :1
l Cl i en t ¹ Client Contact Payroll Coordinator
ll 5991 JE REMI Akl SOLOWAY SUSAN CROSBY
I
Pay Period Starting Date 04/04/2011
P ay Per iod End ing Da t e . .
0 4/17 / 2 0 1 104/22/2011Check Da t e . . . . . . . . . .
Number of Employees Paid. . . . . . . . .
2525
N umber o f Ch e c k s • b • •
N umber o f Vo i d Ch e c k s 0 0Number of Manual Checks. . . . . . • • . . . . . . . . .
. . • . . . . . . . • . .
GROSS PAYROLL3 7,110 . 4 5
SOI SERVICE FEE2, 297. 14
SERVICE FEE ALLOCATED TO OASDI 2, 300. 86
LESS: DEDUCTIONS CREDITED TO CLIENT- 209 . 0 3
52.76FUTA CREDI" J<i.'DUCTIONSERVICE FEE ALLOCATED TO UI FUND LOAN INT
25.32
CHARGE FOR TIMS SUBSCRIPTION FEE MARCH 201177.00
CHARGE FOR TIMS SUBSCRIPTION FEE APRIL 201177.00
4 1,731 . 5 0Tota l D u e.
FOR BILLING QUESTIONS, P LEASE CALL 1 - 8 8 8 - 5 7 2 - 2 4 1 2
From Article at G
etOutO
fDebt.org
Case 11-13244-JKO Doc 119-1 F i led 05/20/1 1 Page 5 of 13
A HMENT 4
YS OUNT
Nameof Debtor: P C S a t L. i o Case Number. -4(D
R eporting Period beginning / - A G I I Period ending
Attach a copy of current month bank statement and bank reconciliation to this Summary of Bank Activity. Astandard bank reconciliation form can be found on the United States Trustee website,http: //www.usdoj,gov/ust/r21/index.htm.
NAME OF BANK: BRANCH:
ACCOUNT NAME: ACCOUNT NUMBER:
PURPOSE OF ACCOUNT:
Ending Balance pcr Bank StatementPlus Total Amount of Outstanding DepositsMinus Total Amount of Oustanding Checks d other debitsMinus Service Charges
Ending Balance per Check Register (a)
*Debit cards must not be issued on this a ount.
**If Closing Balance ls negative, pro de explanation:
The following disbursements w e paid by Cash: ( 0 Check here if cash disbursements were authorized by
United States Trustee)Date A mount Payee Purpose Reason for Cash Disbursement
The following no -tax disbursements werc made from this account:
Date Am nt Payee Purpose Reason for disbursement from this account
(a)The total of this line on Attachment 4A, 4B and 4C plus the total of 4D must equal the amount reported as"Ending Balance" on Schedule of Receipts and Disbursements (Page MOR-2, Line 7).
MOR-11
From Article at G
etOutO
fDebt.org
Case 11-13244-JKO Doc 119-1 F i led 05/20/1 1 Page 6 of 13
ATTACXIlVIENT 5C
CHECK REGISTER - TAX ACCOUNT
Name of Debtor: Sot& l Case Number: 1 I -9 jr(o
Reporting Period beginning Period ending
NAME OF BANK: BRANCH:
ACCOUNT NAME: ACCOUNTS
PURPOSE OF ACCOUNT: TAX
Account for all disbursements, including voids, lost checks, pa y ments, etc. In thealternative, a computer-generated check register can be a hed to this report, provided all the
information requested below is included.htt://www.usdo'. ov/ust.
CHECKDATE N~Utm E1$ ~ Yg g PURPOSE AMOUNT
TOTAL (d)SUMMARY OF TAXES PAID
Payroll T es Paid (a)Sales 4 se Taxes Paid (b)Other axes Paid (c)TO AL (d)
(a) This number is reported in the "Current Month" column of Schedule of Receipts and Disbursements(Page MOR-2, Line 50).
(b) This number is reported in the "Current Month" column of Schedule or Receipts and Disbursements(Page MOR-2, Line SP).
(c) This number is reported in the "Current Month" column of Schedule of Receipts and Disbursements(Page MOR-2, Line 5Q).
(d) These two lines must be equal.
From Article at G
etOutO
fDebt.org
Case 11-13244-JKO Doc 119-1 F i led 05/20/1 1 Page 7 of 13
ATTACHME 4D
INVESTMENT ACC UNTS AND PETTY CASH REPORT
INVESTMUVT ACCOUNTS
Each savings and investment account, i.e. certificates of deposits, money market accounts, stocksand bonds, etc., should be listed separately. Attach copies of account statements.
Type of NegotiableCurrent
Instrument Face Value Pur chase Price Date Purchase Mar ket Value
TOTALPET C H REPO T
The following Petty Cash Drawers/ counts ae maintained:
(Column (Column 3) (Column 4)
Maxim Amount of Petty Diffe rence between
Location of Amo t of Cash Ca sh On Hand (Column 2) andBox/Account in D awer/Acct, At E n d of Month (Column 3)
TOTAL (b)
For any Pe Cash Disbursements over $100 per transaction, attach copies of receipts. If
there are no receipts, provide an explanation
TOTAL INVESTMENT ACCOUNTS AND PETTY CASH(a+ b) $ (c)
(c)The total of this line on Attachment 4A, 4B and 4C plus the total of 4D must equal theamount reported as "Ending Balance" on Schedule of Receipts and Disbursements (PageMOR-2, Line 7).
From Article at G
etOutO
fDebt.org
Case 11-13244-JKO Doc 119-1 F i led 05/20/1 1 Page 8 of 13
ATTACHMENT 6
M NTHLY TAX REPORT
Name of Debtor: c 44t> ~5 Cere Number: i i 8 l ( 4 k.O
Reporting Period beginning Period ending ZO-We l(
TAXES OWED AND DUE
Report all unpaid post-petition taxes including Federal and S withholding FICA, State sales
tax, property tax, unemployment tax, State workmen's corn nsation, etc.
Name of Date Date LastTaxing Payment Tax Return T a x ReturnAuthority Due Description Amo u nt Filed Period
TOTAL
MOR-14
From Article at G
etOutO
fDebt.org
Case 11-13244-JKO Doc 119-1 F i led 05/20/1 1 Page 9 of 13
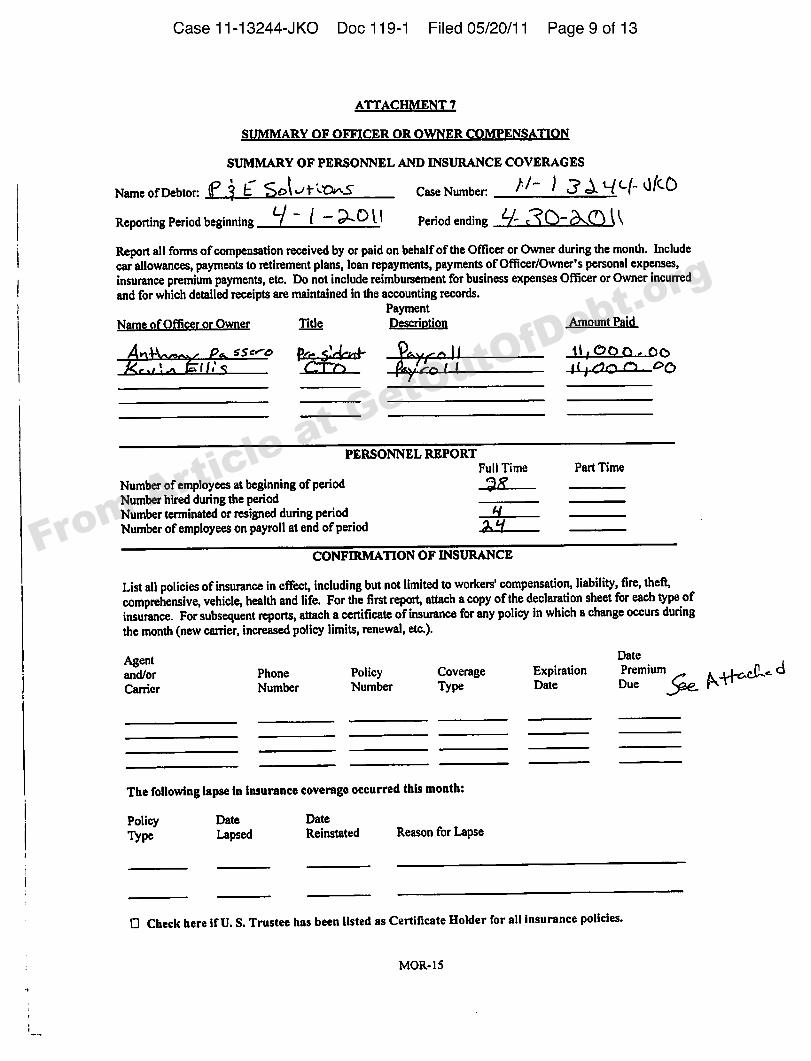
S M ARY OF O R OR K S T I O
SUMMARY OF PERSONNEL AND INSURANCE COVERAGES
Name of Debtor: 4 ~ I ~ t ~~> Case Number:
Reporting Period beginning ~ + © ~ l Period ending Q
Report all forms of compensation received by or paid on behalf of the Officer or Owner during the month. Includecar allowances, payments to retirement plans, loan repayments, payments of OIIicer/Owner's personal expenses,insurance premium payments, etc. Do not include reimbursement for business expenses Officer or Owner incurredand for which detailed receipts are maintained in the accounting records.
Payment
N e n O e Title QcscngttbJI ~ mount P 'd
O'Sc:wd )p~~l 4d OC l 0
PERSONNEL REPORTFull Time Part Time
Number of employees at beginning of periodNumber hired during the periodNumber terminated or resigned during periodNumber of employees on payroll at end of period
CONFIRMATION OF INSURANCE
List all policies of insurance in eIIect, including but not limited to workers' compensation, liability, fire, theft,comprehensive, vehicle, health and life. For the first report, attach a copy of the declaration sheet for each type ofinsurance. For subsequent reports, attach a certificate of insurance for any policy in which a change occurs duringthe month (new carrier, increased policy limits, renewal, etc.).
DateAgentand/or Phone Policy Coverage Expiration Prem i um dCarrier Number Number Type Date Due
The following lapse in insurance coverage occurred this month:
Policy Date DateLapsed Reinstated Reason for Lapse
0 Check here if U. S. Trustee has been listed as Certificate Holder for all insurance policies.
MOR-15
From Article at G
etOutO
fDebt.org
Case 11-13244- JKO Doc 119-1 F i led 05120/11 Page 10 of 13
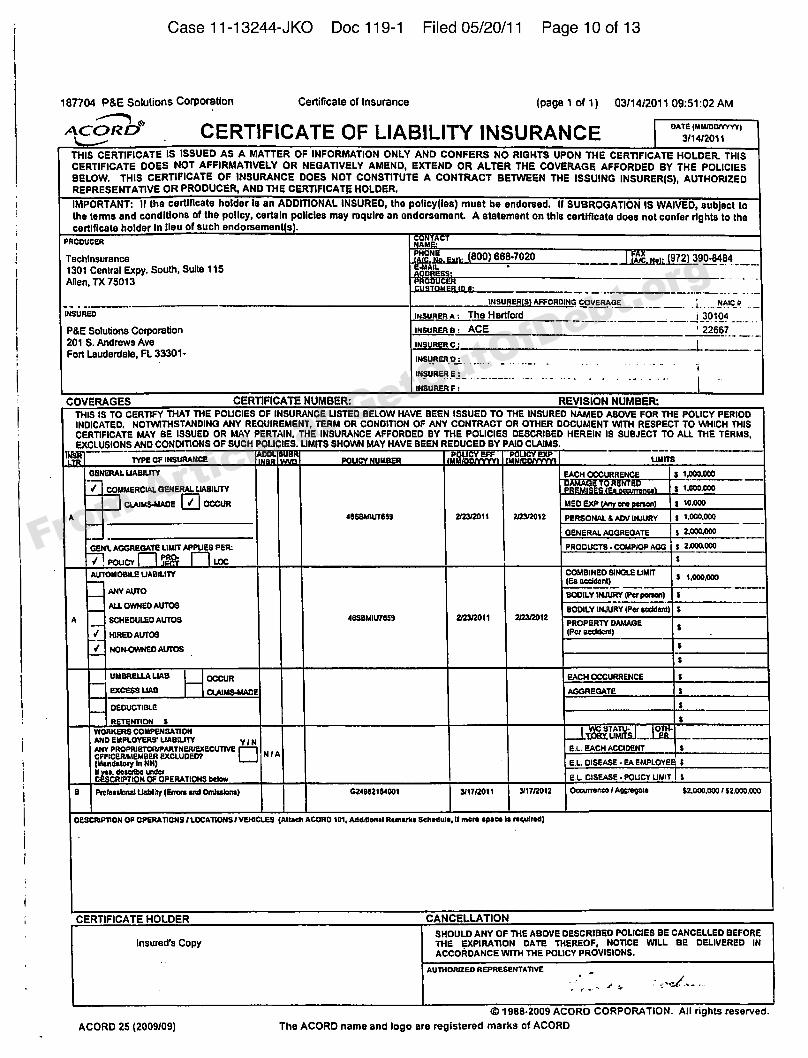
1B7704 P&E Solugons Corporation Certificate of Insurance (page 1 of 1) 03/14/2011 09:51;02 AIVI
CERTIFICATE OF LIABILITY INSURANCETH($ Qf RTIF(CATE IS ISSUED AS A MATTER OF INFORMATION ONLY AND CONFERS NO RIGHTS UPON THE CERTIFICATE HOLDER. THISQERTIFIQATE DDFS NOT AFFIRMATIVELY OR NEGATIVELY AMEND, EXTEND OR ALTER THE COVERAGE AFFORDED BY THE POLICIESBELOW. TH($ QFRT(FICATE OF INSURANCE DOES NDT CONSTITUTE A CONTRACT BETWEEN THE ISSUING INSURER[S), AUTHORIZEDREPRESENTATIVE DR PRODUCER, AND THE QERTIF)CAT/ HOLDER.
iMPDRTANT: If the certificate holder (0 an ADDITIONAL INSURED, the Policy((es) must be endorsed, If SUBROGATION IS WAIVED, subject tothe terms end conditions of the policy, certain policies msy require an endorsernent. A statement on this certificate does nol confer rights to thecertificate holder In lieu of such endorsemen s .
PRODUCER
Techlnsurence Atc NoJL972) 3390-84841301 Central Expy. South, SuRe 115 aAllen, TX 75013
1NSURER 0 AFFORDING COVERAGE. L . . NAiC O
INOUEEEA s The Hartford i 30104
P &E So(vdons Corporation INSURER e: ACE ' 22667
201 $. Andrews Ave INSURER c:
Fort Lauderdale, FL 33301 INSURER D:
INEURKR E:
INSUEER F:
COVERAGES CERTIFICATE NUMBER REVISION NUMBER
TH($ 1$ TP CERTIFY THAT THE POUQiES OF INSURANCE (JSTED SELOW HAVE BEEN ISSUED TO THE INSURED NAMED ABOVE FOR THK POLICY PERIODINDICATED, NOTWITHSTANDING AHY REQUIREMENT, TERM OR CONDITION OF AHY CONTRACT OR OTHER DOCUMENT WITH RESPECT TO WHICH THI$QFRTIFIQATE MAY BE ISSUED OR MAY PERTAIN, THE INSURANCE AFFORDED BY THE POLICIEB DESCRIBED HEREIN IS SUBJECT TO ALL THE TERMS,EXCLUSIONS AHD CONDITIONS OF SUCH PDLIC(ES. UMITS SHOWN MAY HAVE BEEN REDUCED BY PAID C(AIMS.
TYPE OF INEUEANCK P DU MEE n
GENERAL UAEILITY EACH OCCURRENCE $1,000,000X))X(28T(ITRIST
COMMERCIAL GENERAL UAKIUTY 2 tJO0,000
CIAIMKAIADK ~Y OCCUR Llf o KXP o ne $10,000
• esssbvr0$0 2I2212011 2l2$i20 (2 PERSONAL 0 ADY IaVURY I 1,000,000
GENERAL AGGREGATE I 2,000,000
Gf arL AGGEKGATK LIMIT Applffs ps n: paoDUCTS - coupop AGG
Y' . POUC LDCAutoid oeiLE UAE iLnv COMBINED SINGLE UMIT
I 1,000,000IKa accident)ANY AUTO SDDILV OUVRV (Pcr Person)ALL OWNED AUTOS SDO)LV INtunv (Per eccMeno
A SCHEDVLKD AUTOS 2I22r2011 2I22i2012PROPERTY DAMAGE
10EKD AUTOS (Pcr occtdone
s' No taOwNK D AUTOS
AGGREGATE
DEDUCTIBLE
RETENTiDN $Yronxfns coNFKNEATto» WC STATV I 0
TAX UMITSJAND EMPLOYERS' UAELITY Yl NANY PROPRtETCRIPAETNEEIEXKCUTIYK ~ K.L. EACH ACCIDENTCFFiCKEiuf MEKR KXCLVDKOT NIA(Mandatory In NN) K..L. DISEASE-KAKMPLDYK IE a. describe cadet
CEIPTiDN OPKRATICNS below K L GisEAsf - PDUGY Uair I
a p rotesstomduabter (fetus emt Omlseems) G24002 I OSOO I OI1T/2011 OrlrrI012 DcounoncelAoomtpao $200OOOOl$2000000
ofsctopnoN op opf RAnous I LOCATIotls I vftdcLES (Auach AODAD 101 • Add donai Nemeses schedule, lt moro space ie mcsdmd)
CERTIFICATE HOLDER CANCELLATIONSHOULD ANY OF THK ABOVE DESCRIBED POLICIES BE CANCELLED BEFORE
insured's Copy THE EXP(RATION DATE THEREOF, NOTICE 'WILL BK DELIVERED INACCORDANCE WITH THE POLICY PROVISID)ls.
AUTHORIZED A EPIIESEN YAT1YE
© 1988 2009 AQORD CORPORA TiOH. Ail rights reserved.
ACORD 25 [2009/09) The AQORO name and logo are regis(ared n)arks of AQORO
From Article at G
etOutO
fDebt.org
Case 11-13244-JKO Doc 119-1 F i led 05/20/1 1 Page 11 of 13
I
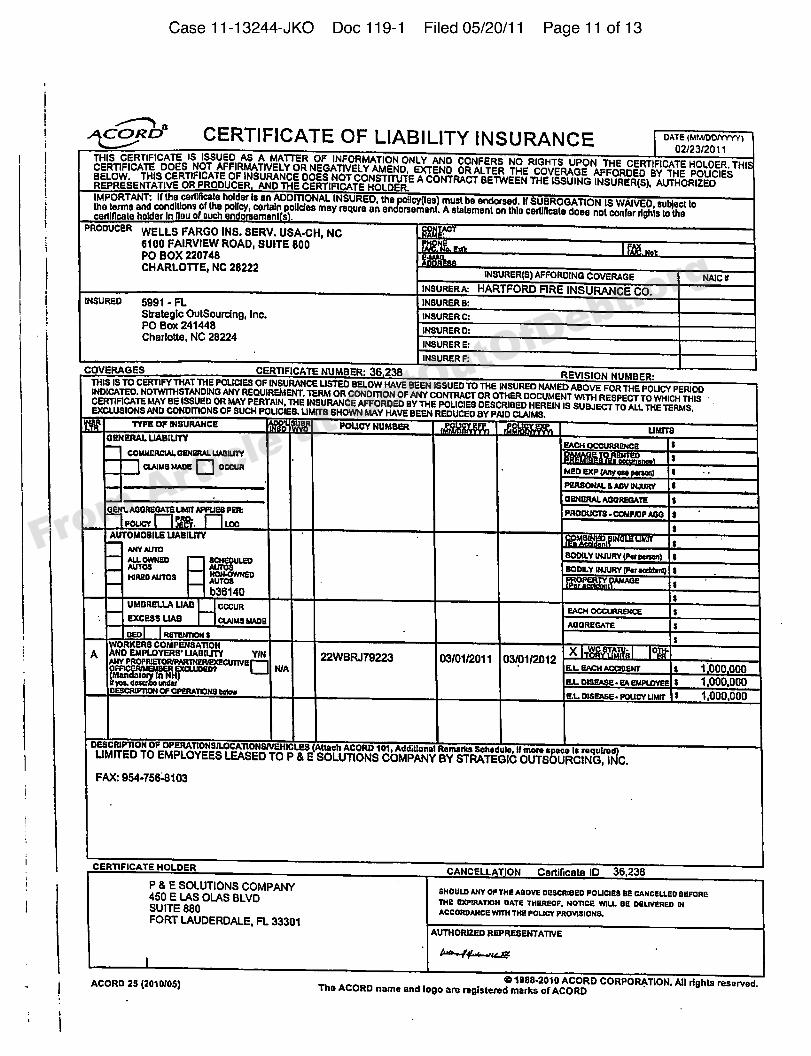
CERTIFICATE OF LIABILITY IN$URANQE >A> • wmamrv>
THIS CERTIFICATE IS ISSUED AS A MATTER OF INFORMATION ONLY ANO CONFERS fIO RIGHTS UPON THE CERTIRCATE HOLDER. THICERTIFICATE DOES NOT AFFIRMATIVELY OR NEGATIVELY AMEND, EXTEND OR ALTER THE COVERAGE AFFORDED BY THE PO'LICIESBELOW. THIS CERTIFICATE OF INSURANCE DOGS NOT CONSTITUTE A CONTRACT BETWEEN THE ISSUING INSURER(S), AUTHORIZEDREPRESENTATIVE OR PRODUCER AND THE CERTIFICATE HOLDER.IMPORTANT: lf Ihe certilicate holder Is an ADDITIONAL INSURED, the Pogcy(lss) must bs endorsed. If SUBROGATION IS WAIVED, subject lo
certllicalehclderlnlleuofsuch e do ament s.Iha lerms and conditions Df ths Policy, cerhdn poiicfes may requre an endorsement. A statemenl on this certiftca(e does nol confer
rights to the
WELLS FARGO INS. 6ERV. USA-CH, NC6100 FAIRVIEW ROAD, SUITE 800Po BOX 220748CHARLOTTE, NC 28222
INSURER(8) AFFORDING COVKRAQK
INSURKRA HARTFORD FIRE INSURANCE CO.INSURED 5991 - FL INSURER 8:
Strategic OutSourcfng, Irtc. INSURER C;pO Box 241448 tNSURER D:Charlotte, NC 28224
INSURER E:INSURER F:
COVERAGES CERTIFICATE NUMBER: 36 238 REVISION NUIIIBERTHIS IS TO CERTIFY THAT THE FOLLIES OF SI SURANCE USTED BELOW HAVE BEEN LSSUKD TO THK at SURKD NAMED ABOVE FOR THE PCUCY PERIODINDICATED, NOTWITHSTANDING ANY REQUIRKLIENT, TERM OR COND moN OF ANY CDNTRACT oR OTHER DQGUMENT wITH RE8pECT TO wHICH THISCERTIFICATE MAY SE ISSUED OR MAY PERTAIN, THE INSURANCE AFFORPED SY THE PCUCIES DESCRISED HEREIN IS SVLIKCT TO ALI. THE TERMS,EXCLUSIONS AND COND mONS OF SUCH PQIJCIES. UNITS SHOWN MAY HAVE BEEN REDUCED SY PAID CLAIMS.
TYPK OF IHSVRAHCK POLICY NUMSKROKRKRAL UASILITY
COIQfancuLL osKaRAL LIAaILDYCLAIMsMAca< occun MKO aturoerr oao perarrd
PKRSDKAL d ACV IMLRLY
oen. ACDRKDATK Lssrr AFFUse paa I'Rooucrs- CDMprop AooPOLCY . LOC
AUTOMOS ILK UAStUTY
ALL orluao scHaouLEDSDDILY IHIVRY IPor correct
AVTcs AUTOBUS aooILY IKIURY (For orcurrrsIonae Auros HDHCWKKD
b36140UMSRKLLA UAS cccuRHtcKSS UAS ClAIMs MACR
WORKERS COMPKK8ATIOIIAIIO EMPLOYERS' LIASILITY YIN
W 022WBRJ79223AKV PRDPICKTDRIPARTHatualracuTIVK ~ 03/01rt2011 03$1/2012SER aacluoaor F L KACH AcclcsÃr 1 000 000
KL DISFASK KA EMPLOYEE 1 OM,OMCESCSCPITOK CP OPERATIOKS crore
EI DISKAsa PDLICT LIMIT s 1,0 00,000
OKSCRIPTIO H OF OPERATIONaILOCATIONSIVEHICLKS (Attach ACORD 101, Addldonal Rornadra echo dulo, tf more space Io roqueedlLIMITED TO EIVIPLOYEES LEASEO TO P Er E SOLUTIONS COMPANY BY STRATEGIC OUTSOURCING, INC.
FAX: 954-7564103
I CERTIFICATE HOLDER CANCELLATION Certilicate ID 36,236P 8 E SOLUTIONS COMPANY450 E LAS OLAS BLVD
6HOULD ANY DF THR Aaova oasCRleED POLICIES ss CAKCELLKD BEFORE
THE EXPIRATICK DATE THEREOF, HDTIca TTILL es DELIVEREQ IKSUITE 880 AccDRDAKca wlrH THE pcvcT FRovlsIOKs.FORT LAUDERDALE, FL 33301
AUTHOR12KD REPRESENTATIVE
ACORD 25 (2010IOS) ID 1888-2010 ACORD CORPORATION. All rights reserved.The ACORD name and logo are rtgfstered marks of ACORD
From Article at G
etOutO
fDebt.org
Case 11-13244-JKO Doc 119-1 F i led 05/20/1 1 Page 12 of 13
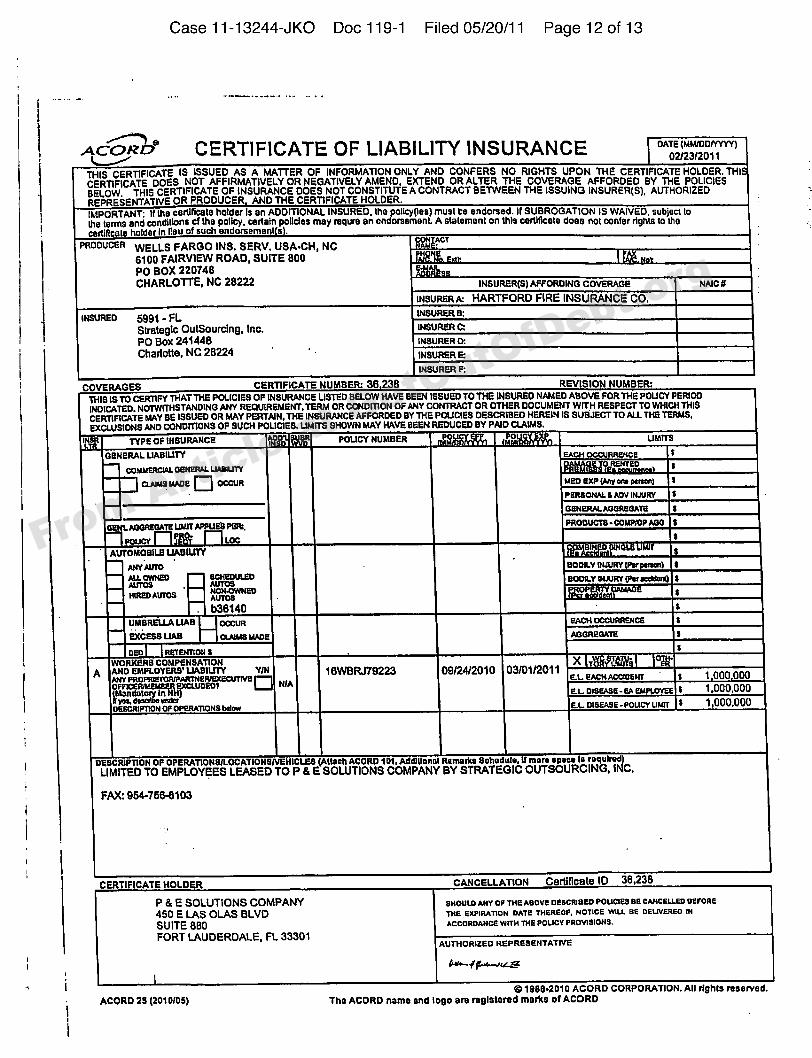
Accac" CERT)FICATE OF LIABIL)TY INSURANCE DATE IMM/DDIYYYY)02/23/2011
THIS CERTIFICATE IS ISSUED AS A MATTER OF INFORMATION ONLY AND CONFERS NO RIGHTS UPON THE CERTIFICATE HOLDER. THICERTIFICATE PDES NOT AFFIRMATIVELY OR NEGATIVELY AMEND, EXTEND OR ALTER THE COVERAGE AFFORDED BY THE POLICIESSELPW THf$ CERTIFICATE OF INSURANCE DOES NOT CONSTITUTE A CONTRACT BETWEEN THE ISSUING INSURER(B), AUTHORIZEDREPRESENTATIVE OR PRODUCER AND THE CERTIFICATE HOLDER.IMPPRTA,NT: lf Ihs certlficale holder is en ADDmONAL INSURED, the Pcifcyties) musl be endorsed. It SUBROGATION IS WAIVED, subject lodts terms end ccndlgons cf the policy. certain policies msy requrs en endorssmenL A stelsmenl on this ceItlftceie does not confer rights to IIIeceItfflcate holder In lieu of such endorsoms I s .
ACTWELLS FARGO Ike. BERV. USA-CH, NC6100 FAIRV)EW ROAD, SUITE 800PO BOX 220748CHARLOTTE, NC 28222 INSURERIS) AFFORDING COVERAGE
IffSURER A: HARTFORD FIRE INSURANCE CO.
INSURER 8:IHSIIRED egg1 - FLStrategic Outeourcfng, Inc. INSURER C:
PO Box 241448 INSURER D:
Charlotte, NC 28224
COVERAGES GERTIFIGATE NUMBER: 36 238 REVISION NUMBER:
lttfa IS TO CERTIFY THAT THE POUCIES OF INSURANCE LISTED BELOW HAVE BEEN ISSUED TO THE INSURED NAMED ABOVE FOR THE POUCY PERfCDINDICATED. NOTWITHSTAAIOING ANY REQUIREMENT, TERM OR CCNDITION OP ANY CONTRACT OR OTHER DOCUIdENT WITH RESPECT TO WHICH THISCERTIRCATE MAY BE ISSUED OR MAY PERTAIN, THE INSURANCE AFFORDED SY THE POUCIES DESCRIBED HEREIN IS SUBJECT TO ALL THE TERMS,EXCLUSIONS AIID CONDTTIONS OF SUCH POUCIES. UMITS SHOWN MAY HAVE SEEN REDUCED BY PAID CLAgd8.
uI TYPE OF IIISURARCE POUCY NUMBER Ualrra
GEIIBRAL UASILITYccurusRCIAL oaNRRAL UAS ILITY
CLAINs MADe + occuRI anaoNAL a Aov uLIVRY
PRODVCTS COMFRIP AOO
AUTOMOBILE LIABILITYArly AUTO BODILY INJVRY IPar Iocn)
SCNRDVLdo BOOILY SIRlRY IFor ooddonsop aIoaao Auros AVTOS
. b36140UMBRELLA UABsxcasa UAB CLAIMs MAoa
ceo R ETEIrnos sTYORKER8 COMPENSATIONAND EMPLOYERS' UABIUTY Y/ff 1BWBRJ79223 09/24/2010 03/01/2011 T 1 0 0 0000ANY pnopssYonwpARTNereaxscLITIva ~
IMon datae tn%~ R.L DISRAsd- sA dNPLOYKEt 1,00 0,000
R.L DIsaASE poLICY LesT 1,000,000ORSCRIPTION OF OPERATIONS Oofow
DBBCRIPIIOH OF OPBRATIQH9JLOCATIOHSNEHICLBB (Attsch ACORD 101, Addillonsl Remarks Schodulo, If moro seooo ls roqulrod)LIMITED TO EMPLOYEES LEASED TO P 8 E SOLUTIONS COMPANY BY STRATEGIC OUTSOURCING. INC
FAX: 954-7884)103
CERTIFICA'f E HOLDER CANCELLATION Certificate IO 36,238
P & E SOLUTIONS COMPANY snouLo ANY os TNe Aeove osscnfaeo poLcIss ss CANcsLLeo serosa450 E LAS OLAS BLVD Tne sIIPIRATIQN DATe THRRscn, NOTICE YNLL ss ORLIVARso IN
SUITE 880 ACCORDANCS WITH THS POLICY PROVISIONS.
FORT I.AUDEROALE, FL 33301AVTHORIZao RRPRESRNTATIVE
e1888-2010 ACQRD CORPORATION. All rfghls reserved.ACORD 28 (201 0/05) The ACDRD name snd logo are rogistered marks of ACCIRD
From Article at G
etOutO
fDebt.org
Case 11-13244-JKO Doc 119-1 F i led 05/20/1 1 Page 13 of 13
ATTACH T 8
S I NIFI ANT DEVE P NT S D U R I REPORTING PERIOD
Information to be provided on this page, includes, but is not limited to: (l) financial transactio that are notreported on this report, such as the sale of real estate (arruclt clcelrrg sraremenrj; (2) non-fi cial transactions, suchas the substitution of assets or collateral; (3) modifications to loan agreements; (4) chang n senior management,etc. Attach any relevant documents.
We anticipate filing a Plan of Reorganization and Disclosure Statement on or before
From Article at G
etOutO
fDebt.org





























