Embed Size (px)
Citation preview

Xpert MTB/RIF Roll Out in Indonesia Interim ReportInterim Report
Bachti Alisjahbana, Sanne van Kampen, Santo Nugroho, Shinta, Sumanto Simon, Diah E. Mustikawati
TORG Indonesian National TB Program
KNCV / TB CARE IC / C

Indonesia
TB Situation in Indonesia
• 4th Highest TB case load world wide? MDR TB • ? MDR TB,
• Very few MDR-TB on treatment
• HIV concentrated epidemic• Very few confirmed TB (~ 4% in HIV cohort)• Very few confirmed TB ( 4% in HIV cohort)
TB CARE I GeneXpert Core Project Indonesia:Indonesia:1. Intensified introduction of Xpert MTB/RIF in 3 selected
countries: Nigeria Vietnam Indonesiacountries: Nigeria, Vietnam, Indonesia2. Document lessons learnt and collect evidence for further
planning and scaling up of Xpert MTB/RIF
Input▫ Xpert machines , 1,700 cartridges ▫ TA for roll out in coordination with NTP incl site▫ TA for roll-out in coordination with NTP, incl. site▫ Assessments, training, supervision, M&E ▫ Op. Research Monitoring implementation and collecting evidence for further scale-
up of Xpert in collaboration with local research group (TORG)
Operational research objective
Key research question & outcomes
Operational research objectiveBased on the WHO ‘Rapid Implementation’ (March 2011)
Key research question & outcomes
What is the impact of Xpert on programmatic outcomes related to TB & MDR TB diagnosis and
Expected key outcomes:
outcomes related to TB & MDR-TB diagnosis and treatment among high risk groups?
Expected key outcomes:1. Increased TB and MDR-TB case notification2. Increased TB and MDR-TB treatment initiation3 R d ti i h lth t d l3. Reduction in health system delays4. Additional yield of Xpert over smear microscopy5. Reliability of Xpert as marker for MDR-TB
Methodology• Pre-Post comparative analysis• Outcome 1-3: Comparing retrospective to prospective▫ Retrospectve: March – August 2011 data (no Xpert)
P i M h A 2012 ( i h X )▫ Prospective: March - August 2012 (with Xpert)▫ # diagnosed ▫ # starting on treatment
• Comparative analysis• Outcomes 4-5: Comparing Xpert with conventional
TB HIV X t Zi hl N l▫ TB HIV: Xpert vs. Ziehl Neelsen▫ MDR TB: xpert vs. Culture (MGIT & LJ)▫ # additional yield by Xpert▫ # sens-spec for MDR detection▫ # sens-spec for MDR detection
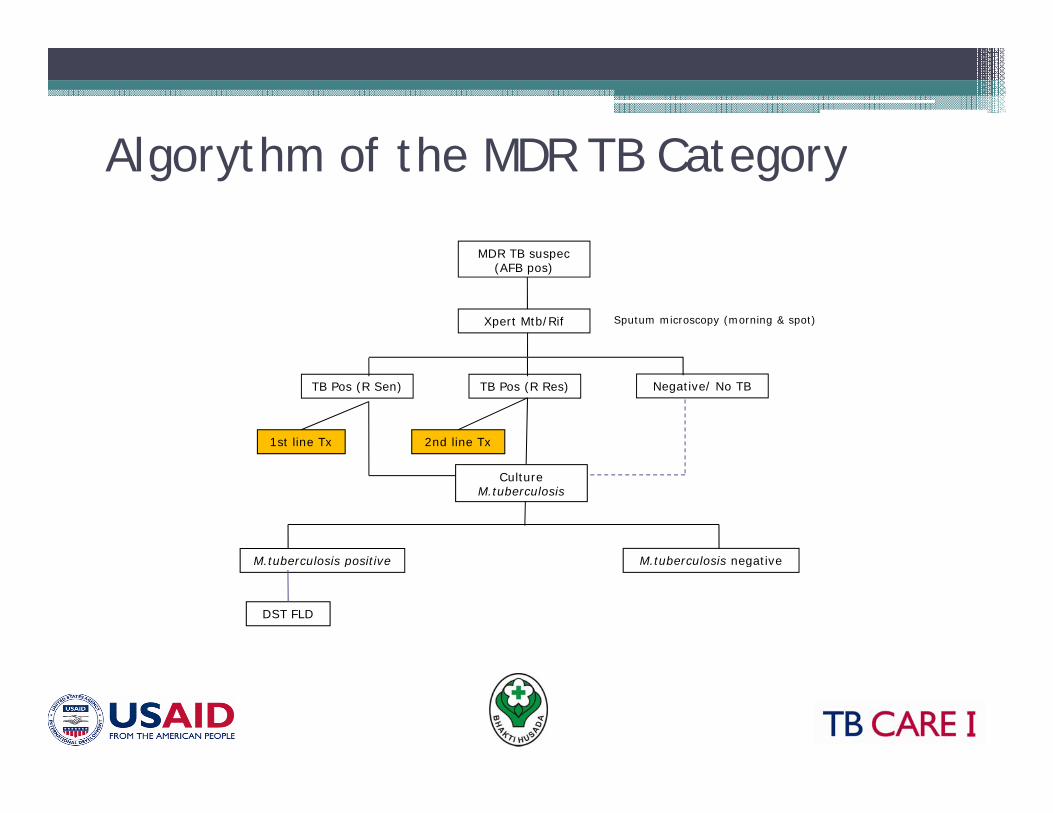
Algorythm of the MDR TB CategoryAlgorythm of the MDR TB Category
MDR TB suspecMDR TB suspec(AFB pos)
Sputum microscopy (morning & spot)Xpert Mtb/Rif
TB Pos (R Sen) TB Pos (R Res) Negative/ No TB
1st line Tx 2nd line Tx
M tuberculosis positive M tuberculosis negative
Culture M.tuberculosis
M.tuberculosis positive M.tuberculosis negative
DST FLD
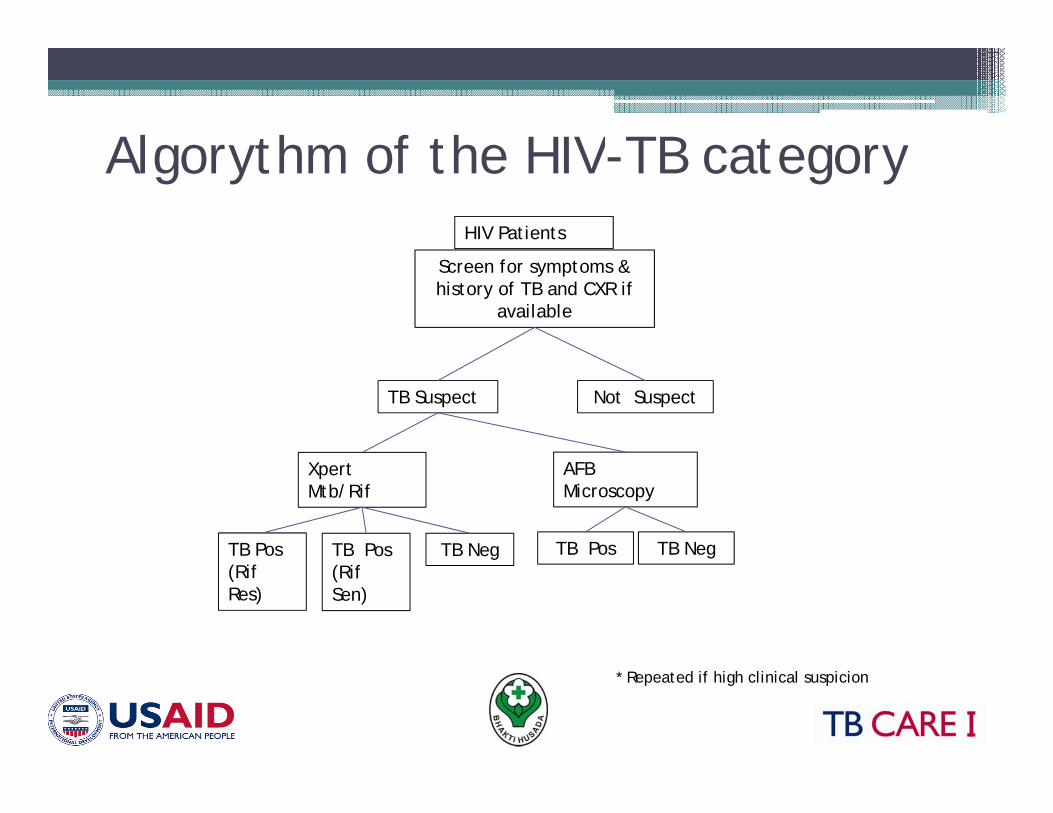
Algorythm of the HIV TB categoryAlgorythm of the HIV-TB categoryHIV Patients
Screen for symptoms & history of TB and CXR if
available
TB Suspect Not Suspect
Xpert Mtb/Rif
AFB Microscopy
TB Pos TB NegTB Pos TB Pos TB Neg(Rif Res)
(Rif Sen)
* Repeated if high clinical suspicion
Sites & periodSites & period
1. Mikro UI & RSCM (Jakarta) 1. Mikro UI & RSCM (Jakarta) 2. RS Persahabatan (Jakarta)3. RS Soetomo & BLK (Surabaya)( y )4. RS Moewardi (Solo)5. RSHS and BLK (Bandung)( g)
Data gathered from routine registersData analysis using stataAim for final analysis after in Mar 2013
ResultsP ti d t 1073Prospective data n=1073• Excluded 117 (reg date, double entries,
treatment before test)treatment before test)• Included in prospective data: n=956▫ MDR-TB Suspect n= 673MDR TB Suspect n 673▫ HIV-TB n= 283
Retrospective data: pTotal year 2011 n = 989Included n=507
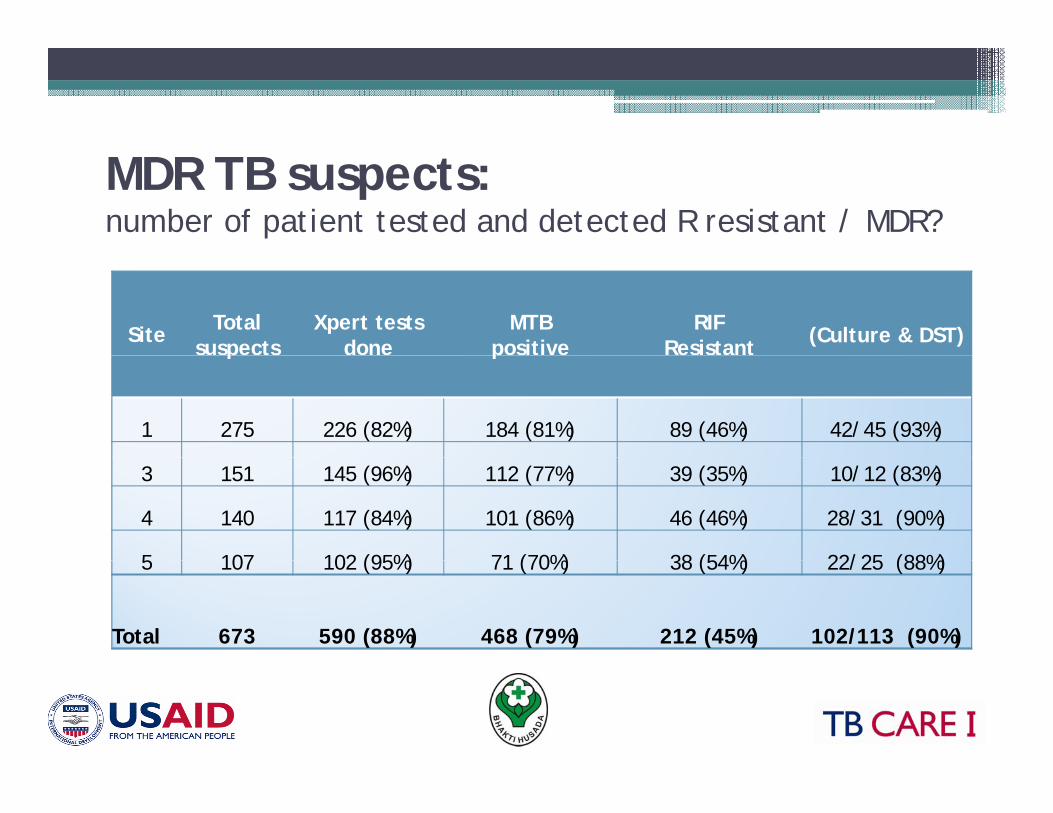
MDR TB suspects:number of patient tested and detected R resistant / MDR?
Site Total suspects
Xpert tests done
MTB positive
RIF Resistant (Culture & DST)p p
1 275 226 (82%) 184 (81%) 89 (46%) 42/45 (93%)
3 151 145 (96%) 112 (77%) 39 (35%) 10/12 (83%)
4 140 117 (84%) 101 (86%) 46 (46%) 28/31 (90%)
5 107 102 (95%) 71 (70%) 38 (54%) 22/25 (88%)5 107 102 (95%) 71 (70%) 38 (54%) 22/25 (88%)
Total 673 590 (88%) 468 (79%) 212 (45%) 102/113 (90%)
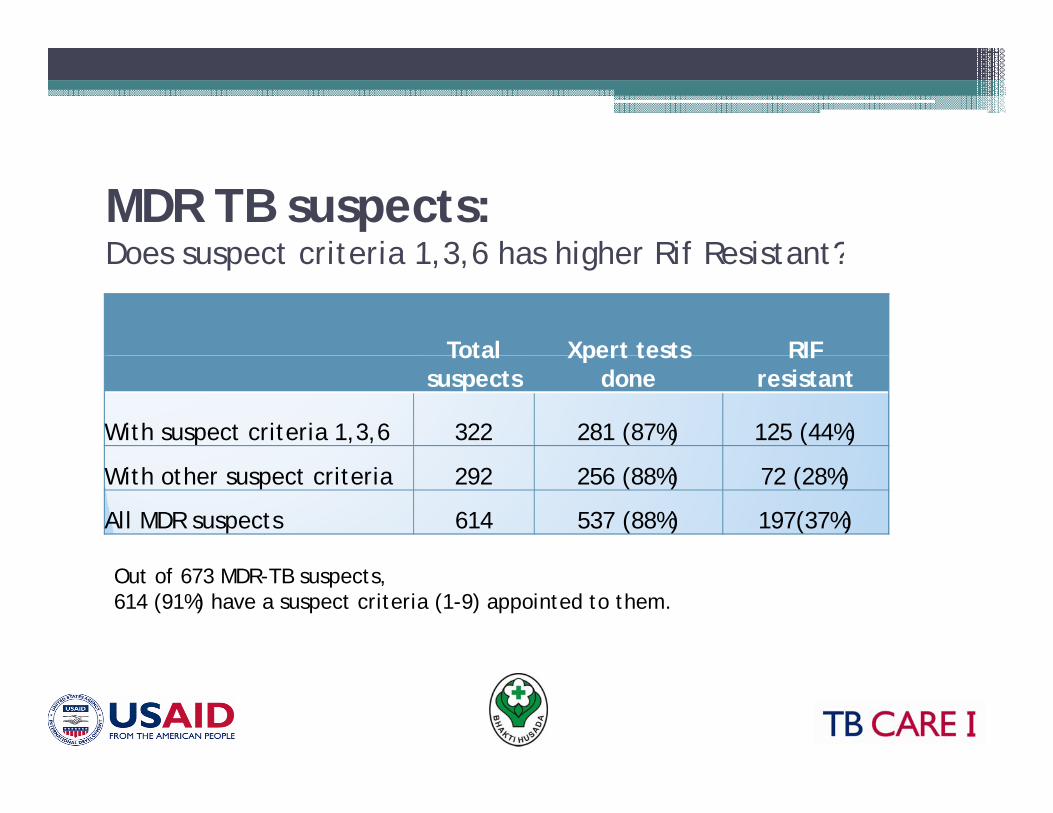
MDR TB suspects:Does suspect criteria 1 3 6 has higher Rif Resistant?Does suspect criteria 1,3,6 has higher Rif Resistant?
Total Xpert tests RIF Total suspects
Xpert tests done
RIF resistant
With suspect criteria 1,3,6 322 281 (87%) 125 (44%)
With other suspect criteria 292 256 (88%) 72 (28%)
All MDR suspects 614 537 (88%) 197(37%)
Out of 673 MDR-TB suspects, 614 (91%) have a suspect criteria (1-9) appointed to them.
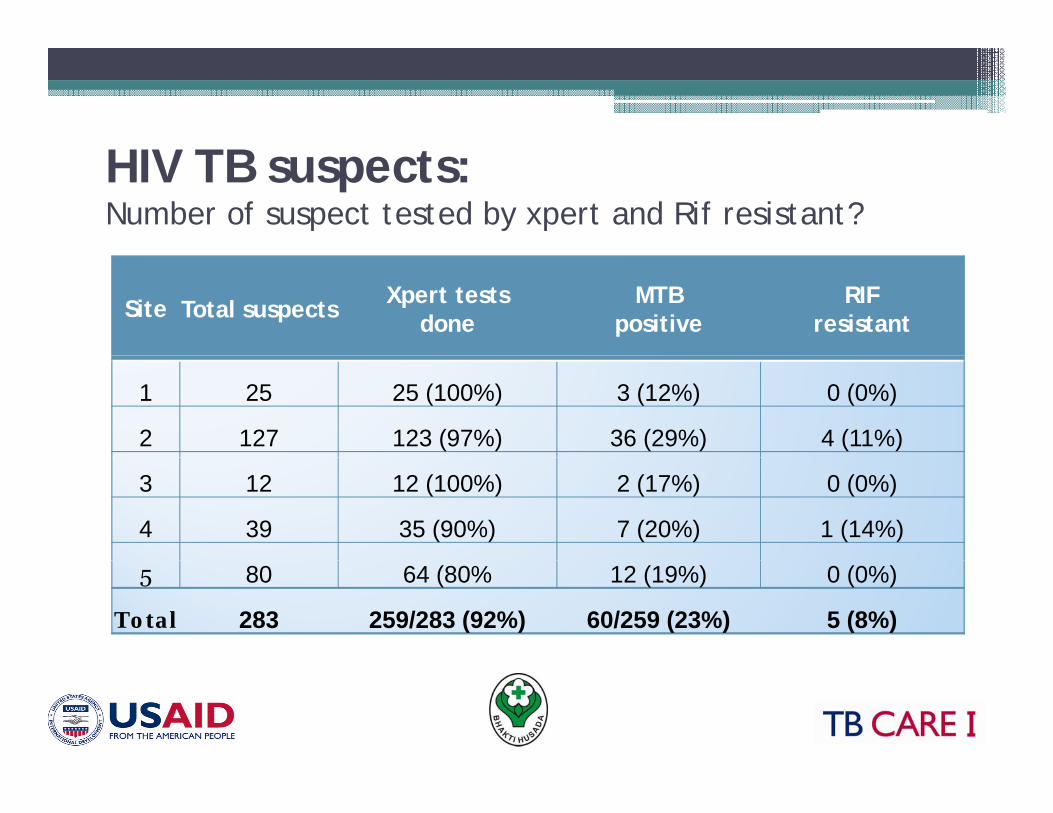
HIV TB tHIV TB suspects:Number of suspect tested by xpert and Rif resistant?
Site Total suspects Xpert tests done
MTB positive
RIF resistant
1 25 25 (100%) 3 (12%) 0 (0%)
2 127 123 (97%) 36 (29%) 4 (11%)
3 12 12 (100%) 2 (17%) 0 (0%)
4 39 35 (90%) 7 (20%) 1 (14%)
5 80 64 (80% 12 (19%) 0 (0%)
Total 283 259/283 (92%) 60/259 (23%) 5 (8%)
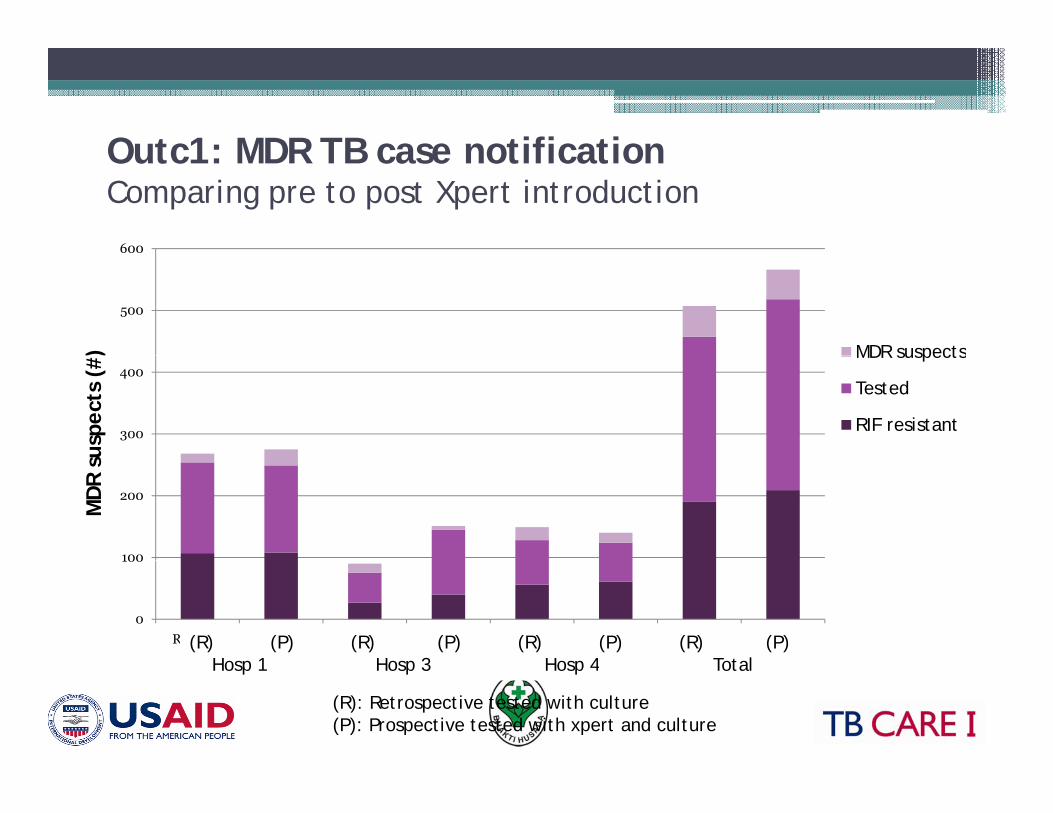
Outc1: MDR TB case notificationOutc1: MDR TB case notificationComparing pre to post Xpert introduction
600
500
600
) MDR suspects
300
400
uspe
cts
(#
MDR suspects
Tested
RIF resistant
100
200
MD
R s
0
100
RSP (R ) RSP (P) Moewardi (R )
Moewardi (P) Soetomo (R ) Soetomo (P) Total (R ) Total (P)(R) (P) (R) (P) (R) (P) (R) (P)Hosp 1 Hosp 3 Hosp 4 Total
(R): Retrospective tested with culture (P): Prospective tested with xpert and culture
Hosp 1 Hosp 3 Hosp 4 Total
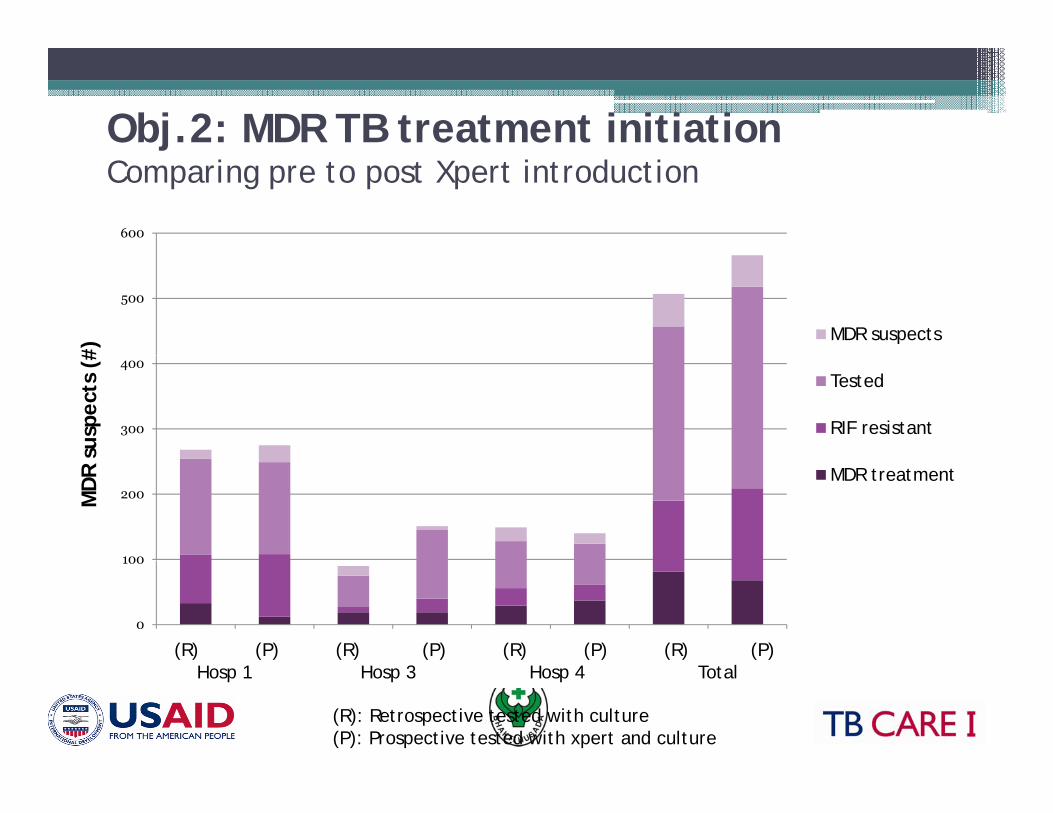
Obj.2: MDR TB treatment initiationjComparing pre to post Xpert introduction
600
500
#)
MDR suspects
300
400
susp
ects
(#
Tested
RIF resistant
100
200MD
R s
MDR treatment
0
100
RSP (R ) RSP (P) Moewardi (R )Moewardi (P)Soetomo (R ) Soetomo (P) Total (R ) Total (P)(R) (P) (R) (P) (R) (P) (R) (P)Hosp 1 Hosp 3 Hosp 4 Total
(R): Retrospective tested with culture (P): Prospective tested with xpert and culture
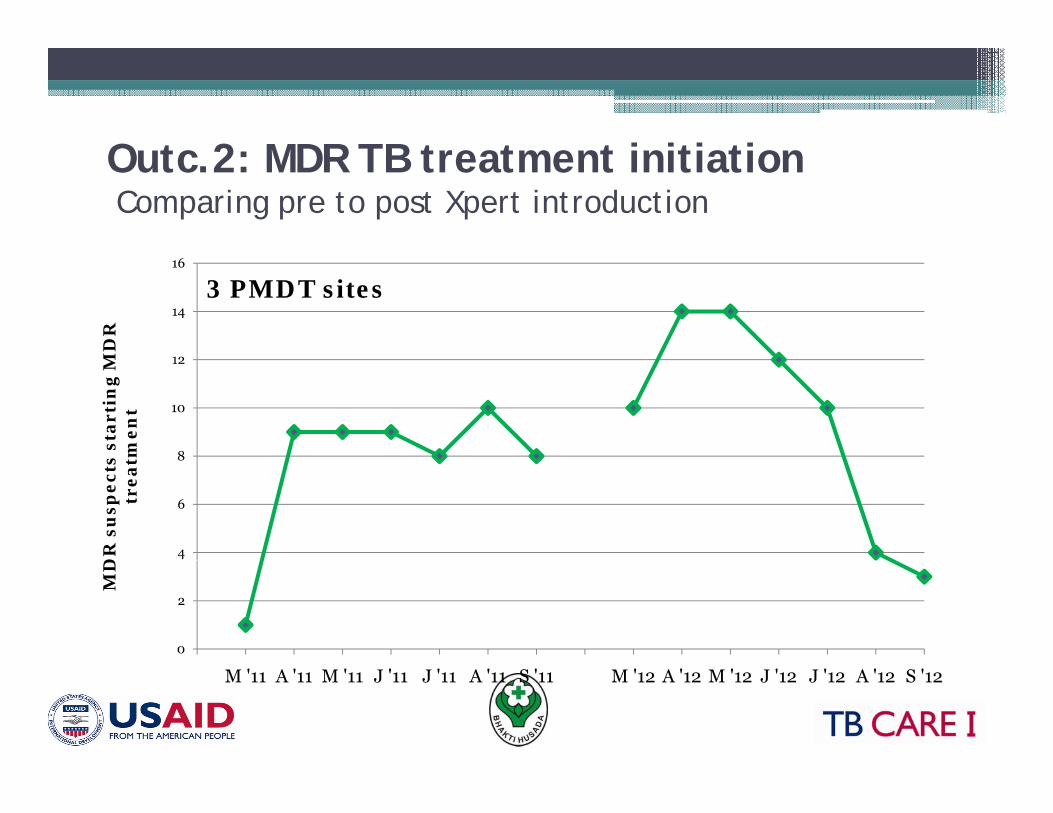
O tc 2: MDR TB treatment initiationOutc.2: MDR TB treatment initiationComparing pre to post Xpert introduction
14
16
MD
R
3 PMDT sites
8
10
12
s st
arti
ng
Mm
ent
4
6
8
DR
su
spec
tstr
eat
0
2
MD
M '11 A '11 M '11 J '11 J '11 A '11 S '11 M '12 A '12 M '12 J '12 J '12 A '12 S '12
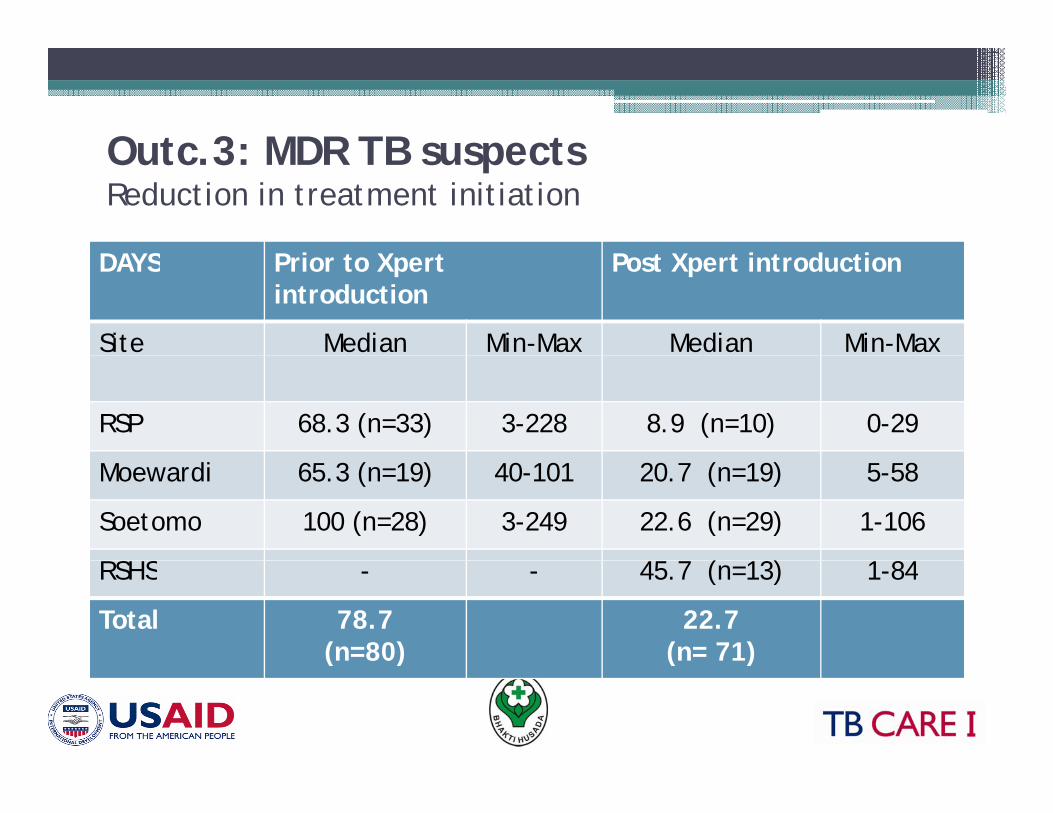
Outc 3: MDR TB suspects Outc.3: MDR TB suspects Reduction in treatment initiation
DAYS P i X P X i d iDAYS Prior to Xpertintroduction
Post Xpert introduction
Site Median Min-Max Median Min-Max
RSP 68.3 (n=33) 3-228 8.9 (n=10) 0-29
Moewardi 65.3 (n=19) 40-101 20.7 (n=19) 5-58
Soetomo 100 (n=28) 3-249 22.6 (n=29) 1-106
RSHS 45 7 ( 13) 1 84RSHS - - 45.7 (n=13) 1-84
Total 78.7(n=80)
22.7 (n= 71) ( ) ( )
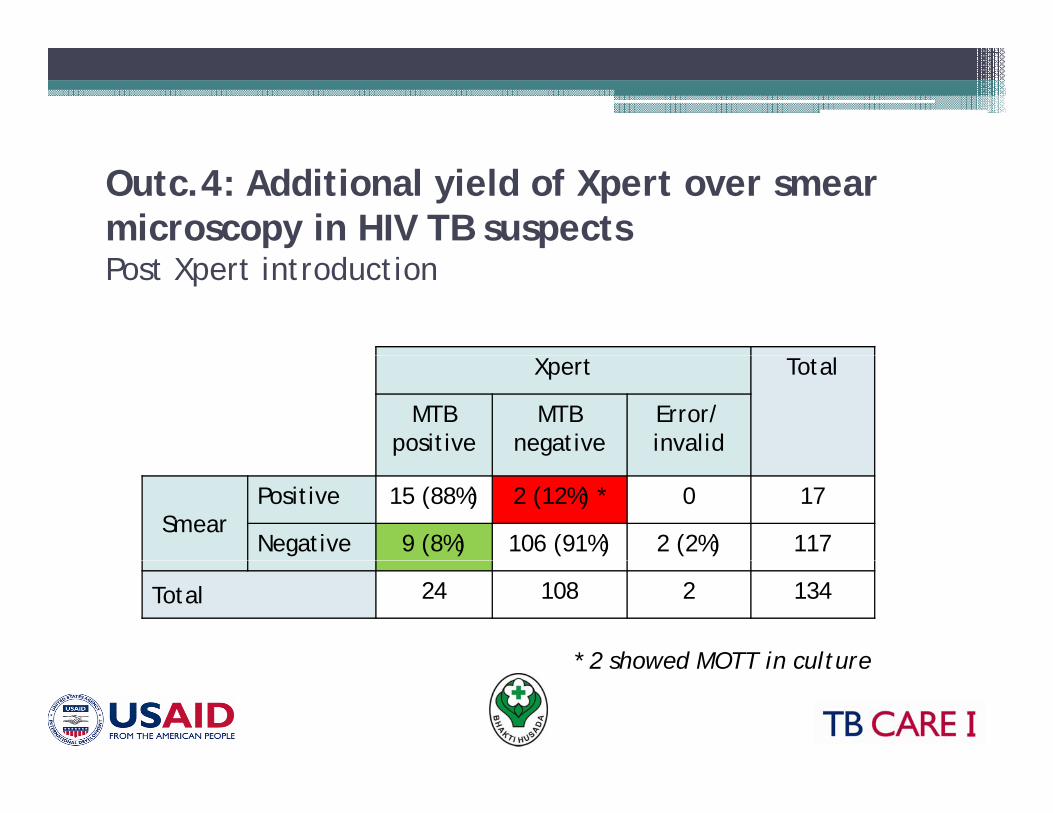
Outc.4: Additional yield of Xpert over smear microscopy in HIV TB suspectsPost Xpert introduction
Xpert Total
MTBpositive
MTB negative
Error/ invalid
SmearPositive 15 (88%) 2 (12%) * 0 17
Negative 9 (8%) 106 (91%) 2 (2%) 117
Total 24 108 2 134
* 2 showed MOTT in culture 2 showed MOTT in culture
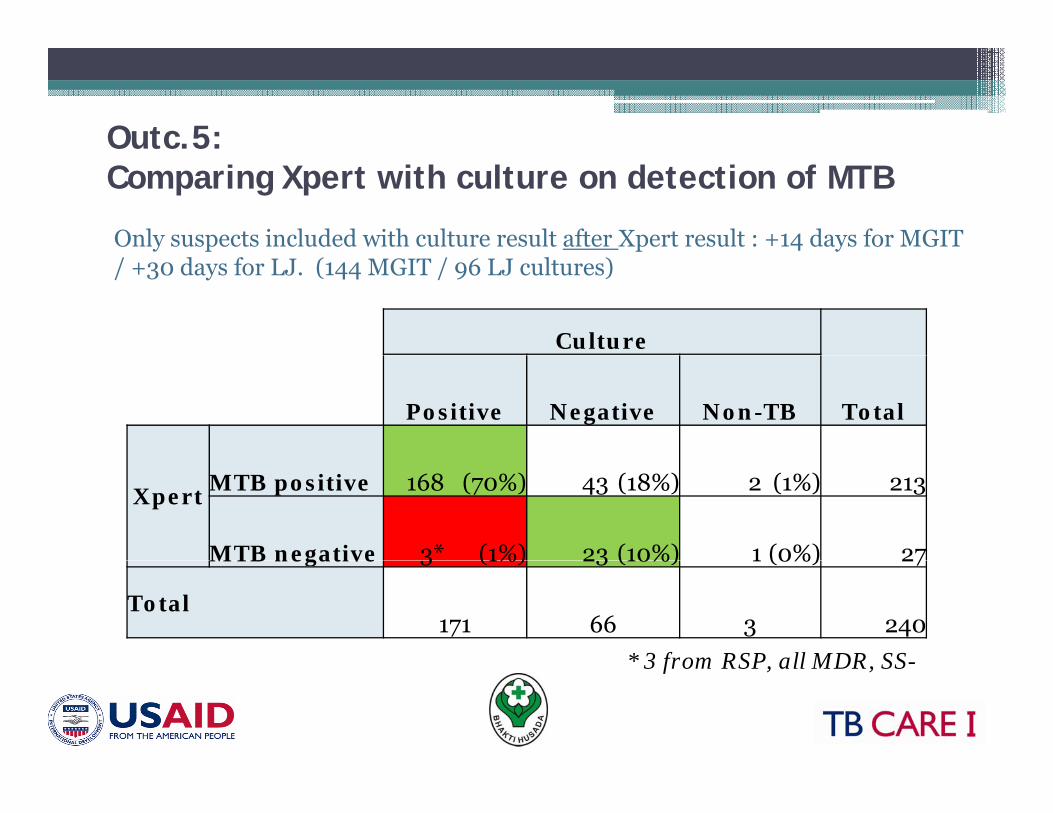
Outc.5: Comparing Xpert with culture on detection of MTB
Only suspects included with culture result after Xpert result : +14 days for MGIT / +30 days for LJ. (144 MGIT / 96 LJ cultures)
Culture
TotalPositive Negative Non-TB
Xpert MTB positive 168 (70%) 43 (18%) 2 (1%) 213
MTB negative 3* (1%) 23 (10%) 1 (0%) 27
* 3 from RSP all MDR SS-
MTB negative 3 (1%) 23 (10%) 1 (0%) 27
Total171 66 3 240
3 from RSP, all MDR, SS-
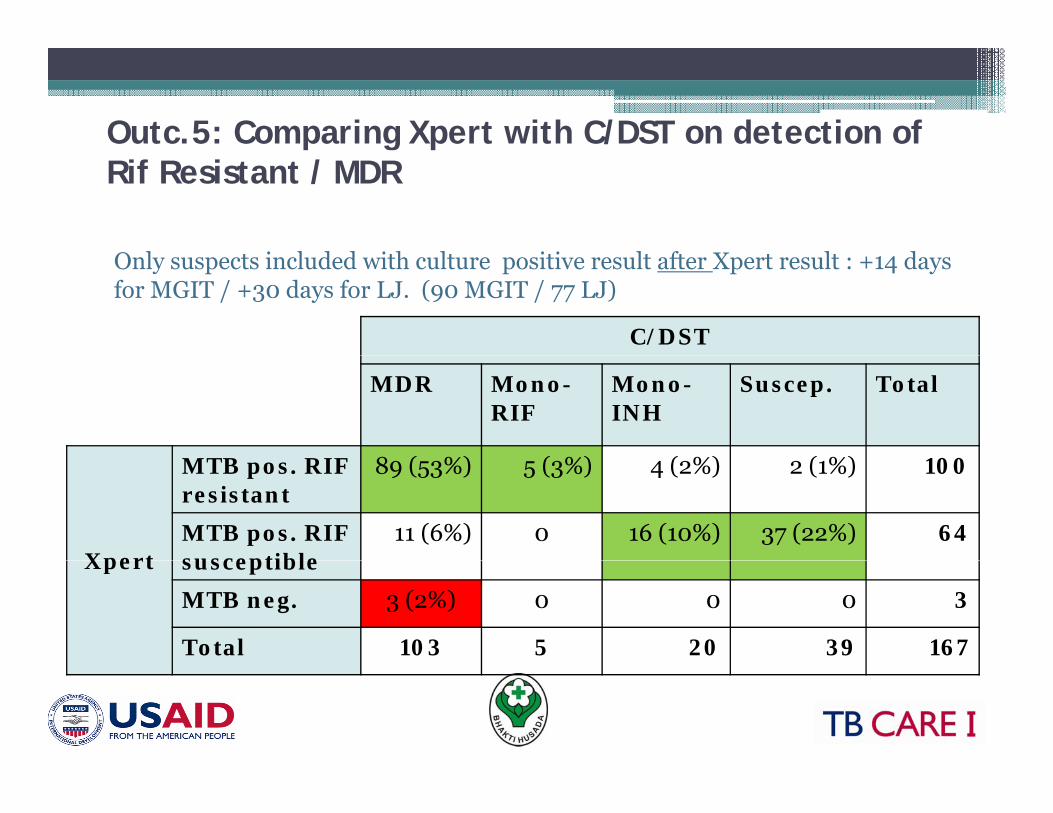
Outc.5: Comparing Xpert with C/DST on detection of Rif Resistant / MDR
O l i l d d i h l i i l f X l d
C/DST
Only suspects included with culture positive result after Xpert result : +14 daysfor MGIT / +30 days for LJ. (90 MGIT / 77 LJ)
MDR Mono-RIF
Mono-INH
Suscep. Total
MTB RIF 8 ( %) ( %) ( %) ( %)
Xpert
MTB pos. RIF resistant
89 (53%) 5 (3%) 4 (2%) 2 (1%) 100
MTB pos. RIF susceptible
11 (6%) 0 16 (10%) 37 (22%) 64Xpert susceptible
MTB neg. 3 (2%) 0 0 0 3
Total 103 5 20 39 167
C l iConclusionsPromising results of Xpert • Promising results of Xpert
• High % of MDR TB supports need for rapid diagnosis
• Implication on clinical care?
▫ Confirmatory test needs improvement (culture/DST)
▫ Hesitation of clinicians
▫ Lack of experience and resources
• Expansion?
▫ Capacity vs. coveragep y g
• Indonesian National TB Programg• Lab WG/PMDT/TORG, • BPPM mikro, WHO, FHI, MSH, • Coordinating partner: PMU TB CARE I• Coordinating partner: PMU TB CARE I• Collaborating partners: KNCV, WHO• Facilitation: TB CARE Country Office• USAID Jakarta









![Xpert MTB/RIF test for detection of pulmonary tuberculosis ... Cochrane Review... · [Diagnostic Test Accuracy Protocol] Xpert MTB/RIF test for detection of pulmonary tuberculosis](https://img.pdfslide.us/doc/110x75/5b1f73977f8b9a34458b49bc/xpert-mtbrif-test-for-detection-of-pulmonary-tuberculosis-cochrane-review.jpg)




![Xpert(R) MTB/RIF assay for pulmonary tuberculosis and ......[Diagnostic Test Accuracy Review] Xpert® MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults Karen](https://img.pdfslide.us/doc/110x75/6089b4043886915fb625acf3/xpertr-mtbrif-assay-for-pulmonary-tuberculosis-and-diagnostic-test-accuracy.jpg)













