Embed Size (px)
Citation preview

INTERNATIONAL JOURNAL OF LEPROSY^ Volume 64, Number 2
Printed in the U.S.A.
Fixed-Duration Therapy (EDT) in MultibacillaryLeprosy; Efficacy and Complications'
Palanisamy Vijayakumaran, Kumar Jesudasan, and Natarajan Manimozhi 2
The World Health Organization (WHO)introduced a multidrug therapy (MDT) reg-imen for multibacillary (MB) leprosy in 1982containing rifampin, dapsone (DDS) andclofazimine. The recommended durationwas for a minimum period of 2 years oruntil the skin smears were negative for acid-fast bacilli (AFB), whichever was later.
One of the disadvantages of DDS mon-otherapy was the long duration of therapy,i.e., 5 to 10 years or more. The risk of re-l apse (1,2,9, 18 ) varied from 0.7% per year to4.9% per year after DDS monotherapy. Inaddition, a proportion of DDS-resistant re-lapseW 5) might be receiving only DDSmonotherapy. The introduction of MDThad remarkably shortened the duration oftherapy, but still a considerable proportionof them had to be treated for longer than 2years(`'). The revised recommendations ofWHO stated that the proviso to continueMDT beyond 2 years until smear negativitycould be dropped.
We present the outcome of fixed durationtherapy (FDT) in MB leprosy where the du-ration of therapy was limited to only 2 years.
MATERIALS AND METHODSAt the Schieffelin Leprosy Research &
Training Center (SLR&T), Karigiri, India,all of the newly detected MB leprosy pa-tients have been treated with FDT since1984, as per the following criteria for theselection of MB cases: a) skin-smear posi-tive (for AFB) lepromatous (LL) and bor-derline lepromatous (BL) cases; b) previ-ously untreated; c) received DDS monoth-erapy for <24 weeks; and d) no contrain-
' Received for publication on 14 June 1995; ac-cepted for publication on 13 December 1995.
2 P. Vijayakumaran, M.B.B.S., D.P.H., AssociateEpidemiologist; N. Manimozhi, M.B.B.S., D.H.E., As-sociate Epidemiologist; K. Jesudasan, M.B.B.S.,D.T.P.H., Ph.D. (London), Head, Branch of Epide-miology and Leprosy Control, Schielfelin Leprosy Re-search & Training Center, Karigiri 632106, South In-dia.
dications to antileprosy drugs used in theregimen.
Duration of therapy. WHO-recom-mended MDT was administered for 2 yearsonly. The therapy was terminated [patientswere released from treatment (RFT)] at theend of 2 years, irrespective of clinical andbacteriological status.
Relapse. Relapse was defined as an in-crease in the bacterial index (BI; Ridley'sscale) of more than 1+ with or without clin-ical signs.
Surveillance. These patients were clini-cally reviewed every month (during sur-veillance) until they became skin-smearnegative for AFB and once every third orsixth month subsequently. A skin-smear ex-amination was done once every year.
RESULTSDuring the period from 1984 to 1994, 360
MB leprosy patients were included in thestudy. Among these patients, 18.9% had LLand 81.1% had BL leprosy. The BI was upto 2+ in 59.16% of them, and 40.83% hada BI of >2+ at the start of therapy.
The prescribed treatment was successful-ly completed by 262 patients, 19.5% LL and80.5% BL. The BI was up to 2+ in 60.7%of them, and 39.3% had a BI of >2+ at thestart of therapy. Some of these patients(27.2%) did not complete treatment for thefollowing reasons: migrated = 6.7%, death= 3.3%, refusal of therapy = 4.7%; 10.6%of the study patients were on treatment and1.9% had to be removed from the trial sincethey had to be given an alternate regimendue to drug allergy or lepra reactions.
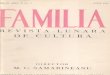
Bacteriological status/clearance. Thesepatients were grouped according to the ini-tial BI. The annual skin-smear results (meanBI) of each group are compared with thatof similar groups of patients who receivedMDT until bacteriological negativity (Figs.1 and 2). The mean BI of the annual skin-smear results showed a decline even aftercessation of therapy, and the decline was
123

124^ International Journal of Leprosy^ 1996
*Mean BI5 -
BI group
0.1 - 1.0
1.1 - 2.0
• 2.1 - 3.0
3.1 -4.0
- 4 plus
*Mean BI5
3
BI group
0.1 - 1.0
1.1 - 2.0
• 2.1 - 3.0
3.1 -4.0
- 4 plus
2
01^2^3^4^5^6^7^8^9^10^11
Year
FIG. 1. Bacteriological clearance (fixed durationtherapy in MB leprosy).
01^2^3^4^5^6
^7^8^9^10
Year
FIG. 2. Bacteriological clearance (MDT until smearnegativity in MB leprosy).
faster during the initial few years. A major-ity (71.6%) of the patients with an initial BIof up to 2.0+ became smear negative within3 years after starting therapy (FDT); for thosewith a BI of >2+, 26.2% became 'smearnegative.
Lepra reaction during therapy. Lepra re-actions were experienced by 22.8% of thepatients during therapy. Type 1 reactionswere observed in 12.3% of the patients, ENLreactions in 3.8% and pure neuritis in 6.7%(The Table). Lepra reactions presenting withonly skin manifestations were seen in 8.3%of the patients; 7.8% had both skin and nervemanifestations. Lepra reactions involvingnerves with or without skin manifestationswere seen in 14.4% of the study patients.
The occurrence of lepra reactions wassimilar in both BL and LL patients (22.3%BL, 25% LL) during treatment. The occur-rence of neuritis in BL patients was 15.3%;in LL patients it was 10.3%. There was nosignificant difference in the occurrence oflepra reaction among the different BI groups,e.g., the group with a BI of 3 +. A majorityof the reactive episodes (86.6%) occurredduring the first year after starting therapy;13.4% of lepra reactions occurred during thesecond year. All of the episodes of leprareactions were treated with steroids (pred-nisolone).
Among BL patients who had lepra reac-tions, 26.2% developed a new disability/de-formity (10.8% with motor paralysis and15.4% with residual motor weakness). Therest of the patients recovered without anynew deformity. Only two LL patients de-veloped motor weakness. Overall, 8.5% oflepra reactions resulted in motor paralysis
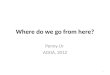
and 14.6% resulted in motor weakness.Among the total study patients, 5.2% de-veloped a new deformity (Fig. 3) as a resultof lepra reaction during treatment (5.8% ofBL, 2.9% of LL patients).
Lepra reaction during surveillance. A to-tal of 28 (10.7%) patients developed leprareactions during surveillance (8.5% BL,19.6% LL). Type 1 lepra reactions consti-tuted 46.4% of the episodes; 28.6% wereENL reactions and 25.0% were pure neuritis(The Table). Overall, 16 patients had neu-ritis with or without skin manifestations.Skin smears were positive in 53.6% of themat the time of the reactive episode. A ma-jority (65.5%) of the reactive episodes oc-curred within the first year of surveillance.All of the episodes of lepra reactions weretreated with steroids.
Among the 28 patients with lepra reactionduring surveillance, 1 patient (0.4% of totalpatients completing therapy) had motor pa-ralysis (Fig. 3) and 6 patients (2.3% of totalpatients completing therapy) were left withresidual motor weakness. Among the totalstudy patients who completed therapy, 2.7%developed a new deformity as a result oflepra reaction during surveillance. None ofthe patients revealed an increase in the BIeither during the lepra reaction or duringthe subsequent follow up (1 to 8 years).
Observations. 1. The BI continues to de-cline after completion of FDT. 2. Duringtreatment 22.8% of MB patients had leprareaction, 86.6% of which occurred duringthe first year of therapy. 3. Occurrence oflepra reaction was similar in BL and LLpatients and in patients with different BIs.4. During surveillance, 10.7% of MB pa-

30^12 33^9
Nil^* Motor Paralysis
Nil^* Motor weakness
7^1
12^6
NIL RELAPSE
30^Skin^12
Mli Patients with Lepra reactions
T : 82^ s:28
Steroid Therapy
52^S N 16
COMPLETE RECOVERY
64, 2^Vijayakumaran, et al.: Fixed-Duration Therapy^125
THE TABLE. Lepra reaction (S, SN, Al) during fixed-duration treatment (FDT) andsurveillance.
Year Type l -Sb ENL-S Type 1-SN' ENL-SN Neuritis Total 0/0
1 22 4 20 8 17 71 19.7 (86.6)d2 2 2 7 11 3.1 (13.4)
Subtotal 24 6 20 8 24 82 22.8 (100)Total cases 360 100
3 4 5 3 1 5 18 6.9 (64.3)4 1 3 1 1 6 2.3 (21.4)5 1 _ _ _ 1 2 0.8 (7.1)6 1 0.4 (3.6)7 — 1 — 1 0.4 (3.6)8
Subtotal 6 6 7 7 28 10.7 (100)Total cases 262 100
° Years 1 and 2 = During therapy; years 3 to 8 = during surveillance.b S = Skin.
SN = Skin and nerve.d Figures in parentheses = percent of total reactions during therapy or surveillance.
tients developed lepra reactions; a majority(64.3%) of the episodes occurred during thefirst year of surveillance. 5. Among the totallepra reactions, 96.4% (106/110) occurredduring the first 4 years after starting com-bined chemotherapy. 6. New deformity/disability occurred in 5.2% of our study pa-tients during therapy and 2.7% during sur-veillance as a result of lepra reaction. Noneof those patients with motor weakness hadvisible deformity.
DISCUSSIONBacteriostatic antileprosy drugs are very
slow in action, and thus the release of bac-terial debris/dead bacilli is also presumablyless and continues for a long duration. MBleprosy patients generally have a very min-imal capability to mount an immune re-sponse to Mycobacterium leprae. Hence,even if bacterial killing is brought about byeffective chemotherapy, clearance of thebacterial debris/dead bacilli may take placein a slow phase( 5 ).
The duration of therapy in MB leprosy isgenerally based on the attainment of smearnegativity, in other words "complete" elim-ination of bacilli from the infected person(<10,000 bacilli per ml of infected tissue).It has been shown that a single dose of rif-ampin can bring about a bacterial killing tothe extent of 99.9%. Chemotherapeutic reg-imens of various durations have been stud-ied. Relapse rates after combined chemo-
therapy regimens administered for morethan 18 months have been shown to be less( 6 )when compared to a shorter duration ofMDT. The relapse rate after WHO-rec-ommended MDT(4 ' 7 8. 14 17 ) was reportedto vary from <1% per year to 17.7%. Thewide variation in the relapse rates is mainlydue to the different criteria employed fordiagnosing relapse.
FIG. 3. Outcome of lepra reactions (MB leprosy onFDT). T = During therapy; S = during surveillance;SRN = skin and/or nerve.

1 "? 6^ International Journal of Leprosy^ 1996
In this study, the WHO-recommendedMB regimen was administered to MB lep-rosy patients for 2 years only. All of thesepatients continue to show a decline in theirBIs even after cessation of therapy and nocase of relapse has been encountered.
The WHO-recommended MDT regimencontaining rifampin plus DDS and clofa-zimine given for 2 years is expected toachieve 100% bacterial killing. Use of anypotent antimycobacterial agent may bringabout a lepra reaction, probably due to theeffective bacterial killing and the release ofa larger load of bacterial debris/dead bacilli.It has been reported that 30% to 53% of LLpatients seemed to have developed lepra re-actions( 13,18 ) during DDS monotherapy and10.4% and 41% in MDT( 3 • ' 2 ) groups. In thisstudy, 30.5% of the MB leprosy patients whoreceived FDT developed lepra reaction(during therapy and surveillance).
Due to the slow clearance of bacterial de-bris/dead bacilli and the short duration ofchemotherapy, the possibility of late leprareaction(" , 16) still exists even after comple-tion of chemotherapy (FDT). Even thougha relapse can manifest as a reactive episode,it need not always be an indicator of relapse.A therapeutic trial with steroids( 10) and closeobservation is necessary to rule out or iden-tify relapse at an early stage.
Conclusion. 1. Bacterial clearance, al-though slow, continues to occur even aftercessation of therapy (FDT). 2. None of theMB patients revealed evidence of relapseduring 886 person-years of surveillance. 3.MB patients need to be monitored for theoccurrence of lepra reaction for a minimumperiod of 5 years after commencement ofFDT with a combined drug regimen. Thefindings of this study indicate that 2 yearsof treatment with the WHO-recommendedregimen may be adequate to effect bacterialkilling.
SUMMARYThe World Health Organization (WHO)
recommended a multidrug therapy (MDT)regimen for multibacillary (MB) leprosy pa-tients in 1982 which was to be administeredfor a minimum period of 2 years or until askin smear was negative for acid-fast bacilli,whichever was later. This regimen containsrifampin, dapsonc and clofazi mine. A single
dose of rifampin was shown to effect a highdegree of bacterial killing (99.9%). The com-bined therapy administered for 2 years maybe adequate to bring about "total" bacterialkilling and to prevent the emergence of drugresistance and persisters. In this study, 360smear-positive and previously untreated MBleprosy patients were treated with WHO/MDT for 2 years; 22.8% of these MB pa-tients developed lepra reaction during ther-apy and 10.7% during surveillance. Thebacterial index continued to decline evenafter termination of fixed-duration therapy.None of these patients relapsed during 886person-years of surveillance.
RESUMENLa OrganizaciOn Mundial de Ia Salud (OMS) reco-
mendO en 1982 el tratamiento con poliquimiotcrapia(PQT) de Ia lepra multibacilar (MB). La PQT debiaadministrarse durantc un periodo minimo de 2 afioso hasta que las extensiones de linfa cutanea se tornarannegativas para bacilos acido-resistentes (BAAR). LaPQT incluye rifampina, dapsona y clofazimina. Ya quesc ha demostrado que una sola dosis do rifampina tieneun alto grado de actividad bactericida (99.9%) sc consi-dera que la terapia combinada administrada durantc2 afios, pucdc conducir a la mucrtc de la totalidad delos microorganismos y pucdc ayudar a prcvcnir Iaemergcncia de la resistencia a Ia droga y de los casospersistentes. En cstc cstudio, se trataron 360 pacicntcsMB, BAAR positivos y sin tratamiento prcvio, conPQT durantc 2 afios; el 22.8% de los pacicntcs des-arrollaron algian tipo de reacciOn leprosa durantc eltratamiento y 9.6% durantc el seguimiento. Ningunade estos pacicntcs mostrO evidencias de rccaida du-rante los 864 personas-afios de seguimiento.
RESUMEL'Organisation Mondialc de la Sante. (OMS) a re-
command& en 1982 pour la lepre multibacillaire (MB)unc polychimiotherapie (PCT) qui dcvait etre admi-nistrec pour unc periode minimalc de 2 ans ou jusqu'ànegativation des frottis cutanes, si ceux-ci n'êtaient pasnegatives apres deux ans. Cc regime conticnt de Iarifampicinc, de la dapsonc et de Ia clofazimine. On amontre qu'une dose unique de rifampicinc avail unpouvoir bactericide important (99.9%). Le traitementcombine de deux ans peut etre adequat pour parvenira unc destruction bacterienne "totale" et pour prevenir('apparition de la resistance bacterienne et de germes"persistants." Dans cette etude, on a trait& avec uncPCT de deux ans 360 maladcs de la lepre MB, positifsaux frottis cutanês et non encore traites anterieure-ment; 22.8% de ces patients MB ont developpe uncreaction lepreuse durant le traitcmcnt, et 9.6% durant

64, 2^Vijayaktnaran, et al.: Fixed-Duration Therapy^127
la periode de surveillance. Aucun de ces patients n'arecidivê au cours de 864 personnes-annees de surveil-lance.
Acknowledgment. This investigation received fi-nancial support from the UNDP/World Bank/WHOSpecial Programme for Research and Training in Trop-ical Diseases (TDR). We extend our sincere thanks tothe World Health Organization for the financial sup-port provided for this project. We also thank Mr. P.Samuel (Project Coordinator), Mr. Raja Samuel (As-sistant Statistician), Mr. Lewis Kumar (Office Secre-tary) and all of our staff who contributed their effortand skills for successful implementation of the project.
REFERENCES1. ALMEIDA, J. G., CHRISTIAN, M. and Chacko, C. J.
G. Follow-up of lepromatous (LL and BL) pa-tients on dapsone (DDS) monotherapy after at-tainment of smear negativity in Gudiyatham Ta-luk, South India. Int. J. Lepr. 51 (1983) 382-384.
2. ALMEIDA, J. G., JESUDASAN, K., CHRISTIAN, M. andCHACKO, C. J. G. Relapse rates in lepromatousleprosy according to treatment regularity. Int. J.Lepr. 54 (1986) 16-20.
3. BECX-BLEUMINK, M. and BERHE, D. Occurrenceof reactions, their diagnosis and management inleprosy patients treated with multidrug therapy;experience in the leprosy control program of theAll Africa Leprosy and Rehabilitation TrainingCenter (ALERT) in Ethiopia. Int. J. Lepr. 60 (1992)173-184.
4. CHOPRA, N. K., AGARWAL, J. S. and PANDYA, P. G.Impact of multidrug therapy on leprosy in Barodadistrict (Gujarat). Indian J. Lepr. 61 (1989) 179-189.
5. GANAPATHI, R., PAI, R., GANDEWAR, K. L. andTHRESSIA, X. J. For how long should a multiba-cillary leprosy patient be treated? Indian J. Lepr.61 (1989) 467-471.
6. KATOCH, K., NATARAJAN, M., BAGGA, A. andKATOCH, V. M. Clinical and bacteriological prog-ress of highly bacillated BL-LL patients discontin-uing treatment after different periods of MDT. Int.J. Lepr. 59 (1991) 248-254.
7. LEPROSY UNIT, WHO, DIVISION OF CONTROL OF
TROPICAL DISEASES. Risk of relapse in leprosy.Geneva: World Health Organization, 1994. WHO/CTD/94. I.
8. MARCHOUX CHEMOTHERAPY STUDY GROUP. Relapses in multibacillary leprosy patients after stop-ping treatment with rifampin-containing com-bined regimens. Int. J. Lepr. 60 (1992) 525-535.
9. NOORDEEN, S. K. Relapse in lepromatous leprosy.Lepr. Rev. 42 (1971) 43-48.
10. PANNIKAR, V., JESUDASAN, K., VUAYAKUMARAN,
P. and CHRISTIAN, M. Relapse or late reversalreaction? Int. J. Lepr. 57 (1989) 526-528.
11. PATTYN, S. R., EYCKMANS, L. and GIGASE, P. Latereversal reaction after combined treatment of apatient with multibacillary leprosy. Ann. Soc. Belg.Med. Trop. 64 (1984) 291-294.
12. RAMESH, V., MISRA, R. S. and SAXENA, U. Mul-
tidrug therapy in multibacillary leprosy; experi-ence in an urban leprosy center. Int. J. Lepr. 60(1992) 13-17.
13. SUSMAN, I. A. Clinical observations on erythemanodosum leprosum (ENL). Lepr. Rev. 29 (1958)227-231.
14. VAN BRAKEL, W., KIST, P., NOBLE, S. and O'TooLE,L. Relapses after multidrug therapy for leprosy:a preliminary report of 22 cases in west Nepal.Lepr. Rev. 60 (1989) 45-50.
15. VAN DIEPEN, T. W. and MENGISTU, G. Relapserate and incidence of dapsone resistance in lep-romatous leprosy patients in Addis Ababa: riskfactors and effect of short-term supplementarytreatment. Int. J. Lepr. 53 (1985) 189-197.
16. VIJAYAKUMARAN, P., MANIMOZHI, N. and JESUDA-
SAN, K. Incidence of late lepra reaction amongmultibacillary leprosy patients after MDT. Int. J.Lepr. 63 (1995) 18-22.
17. WATERS, M. F. R. Relapse following various typesof multidrug therapy in multibacillary leprosy.(Editorial) Lepr. Rev. 66 (1995) 1-9.
18. WATERS, M. F. R., REES, R. J. W., LIANG, A. B.G., KHOO, K. F., MEADE, T. W., PARIKSHAK, N.and NORTH, W. R. S. The rate or relapse in lep-romatous leprosy following completion of twentyyears of supervised sulphone therapy. Lepr. Rev.57 (1986) 101-109.
19. WHO STUDY GROUP. Chemotherapy of leprosyfor control programmes. Geneva: World HealthOrganization, 1982. Tech. Rep. Ser. 675.
20. WHO STUDY GROUP. Chemotherapy of leprosy.Geneva: World Health Organization, 1994, pp. 5-7. Tech. Rep. Ser. 847.