Embed Size (px)
Citation preview

W.C. Tsai, C.M. Tiu, Y.H. Chou, et al
16 J Med Ultrasound 2004 • Vol 12 • No 1
Departments of Radiology and 1Pathology, Veterans General Hospital-Taipei and National Yang-Ming UniversitySchool of Medicine, Taipei, Taiwan.Address correspondence and reprint requests to: Dr. Yi-Hong Chou, Department of Radiology, Veterans GeneralHospital-Taipei, 201, Section 2, Shih-Pai Road, Taipei 112, Taiwan. E-mail: [email protected]
©2004 Elsevier. All rights reserved.
Xanthogranulomatous Cholecystitis —Sonographic and Computed Tomographic
Findings: A Case ReportWan-Chen Tsai, Chui-Mei Tiu, Yi-Hong Chou, Chun-Ru Lai,1 See-Ying Chiou,
Hong-Jen Chiou, Cheng-Yen Chang, Jen-Huay Chiang and Chun Yu
Xanthogranulomatous cholecystitis (XGC) is an unusual but not rare disease entitythat has attracted particular attention in recent years. We report a case of XGCand describe the imaging findings on ultrasound (US) and computed tomography(CT). Abdominal US demonstrated diffuse wall thickening of the gallbladder withan indistinct boundary, hypoechoic bands and nodules inside the thickened gallbladderwall, and multiple gallstones. Abdominal CT revealed similar findings. The thickenedgallbladder wall was well enhanced on contrast CT scan.
(J Med Ultrasound 2004;12:16–20)
KEY WORDS: • xanthogranulomatous cholecystitis • gallbladder disease• chronic inflammation • computed tomography • ultrasound
INTRODUCTION
Xanthogranulomatous cholecystitis (XGC) is anunusual but not rare disease characterized by grayishyellow nodules or streaks in the gallbladder wall,mainly caused by lipid-laden macrophages with anestimated incidence of about 1–2% of all cases ofcholecystitis [1,2]. This entity was first describedby Christensen and Ishak in 1970 [3], and hasattracted particular attention in recent years. XGCis a chronic focal or diffuse destructive inflammatoryprocess of the gallbladder that may occasionally beconfused with a malignant neoplasm on the basisof imaging studies. XGC may lead to complicationssuch as perforation, abscess and fistula if not treatedproperly. Therefore, it is important to make a correctdiagnosis preoperatively, especially using medicalimaging such as ultrasound (US) and computed
tomography (CT). However, only a few studies havecharacterized the radiologic characteristics of XGC.We present a case of XGC and describe the findingsof US and CT.
CASE REPORT
A 78-year-old female presented to our hospital withthe chief complaints of intermittent right upperquadrant pain, nausea, vomiting and poor appetitefor 3 months. Her medical history included hyper-tension and duodenal ulcer with bleeding; both wereunder regular treatment and clinical follow-up. Shehad lost 10 kg in body weight in the past 3 months.
Her vital signs were unremarkable. On physicalexamination, the lungs were clear and heartbeat wasregular. There was no audible precordial murmur.There was right upper quadrant tenderness, but no

J Med Ultrasound 2004 • Vol 12 • No 1 17
Xanthogranulomatous Cholecystitis
palpable mass or Murphy’s sign. Normal bowelsounds were present and there was no reboundingpain or muscle guarding. After admission, routinelaboratory studies including white cell counts anddifferential counts were within normal limits. Chestradiograph revealed old pulmonary tuberculosis.
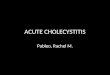
US of the abdomen revealed generalized wallthickening and an indistinct gallbladder boundary(Fig. 1). The gallbladder lumen was comparativelysmall. There were multiple echogenic structures in thegallbladder, representing gallstones (Fig. 1B). Theadjacent duodenum and colon had thickened walls.
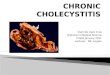
CT of the upper abdomen demonstrated similarfindings (Fig. 2). The thickened gallbladder wall was
enhanced at the inner surface (probably) epitheliallayer on contrast CT scan (Figs. 2C, D). Hypodensebands were evident in the gallbladder wall (Figs. 2C,D). There was an indistinct boundary between thegallbladder and liver. The boundary of the gallbladderand duodenum was ill defined. There was no evidenceof enlarged lymph nodes in the upper abdominalcavity. Percutaneous US-guided needle biopsy of thegallbladder wall was performed and histologic studyshowed xanthogranulomatous inflammatory changeswithout evidence of malignancy.
After antibiotic treatment for 2 weeks, she un-derwent selected open cholecystectomy. A severelyinflamed and contracted gallbladder with small
Fig. 1. Ultrasonography of the right upper abdomen. (A) The gallbladder wall is diffusely thickened with an indistinctboundary (arrows). (B) Layering echogenic material in the dependent portion is demonstrated in the more caudalpart of the gallbladder, representing gallstones (arrows). (C, D) Color Doppler ultrasound of the gallbladderdemonstrates increased flow in the wall (arrows). The hyperemic change is suggestive of inflammatory reactionor cholecystitis.
A B
C D

W.C. Tsai, C.M. Tiu, Y.H. Chou, et al
18 J Med Ultrasound 2004 • Vol 12 • No 1
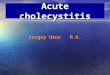
gallstones was noted. There was severe adhesionbetween the gallbladder and the duodenum. Thegallbladder was removed after adhesiolysis. Intra-operative cholangiogram showed no dilatation of thecommon bile duct and bilateral intrahepatic ductswithout stone, stricture, or irregularity. The grossspecimen showed an opened gallbladder measuringabout 12 10 7 cm with a 1.2 cm thick wall.The mucosal folds were coarse and the serosa wasdull. Histopathologic study revealed diffuse chronicinflammatory cell infiltration with focal lipid-ladenmacrophage accumulation in the gallbladder wall(Fig. 3), consistent with XGC. There was no evidenceof malignant cells, abscess or bacteria in the surgicalspecimen.
The patient had an uneventful clinical course af-ter surgery and was discharged in a stable condition.
DISCUSSION
According to the clinical manifestation in our patient,the complex nature of the gallbladder, the adjacentabnormality, and the history of weight loss, thedifferential diagnoses included acute cholecystitis,chronic cholecystitis, XGC, gallbladder carcinoma,adenomatosis, and metastasis. All these disordersare associated with gallstones and are more com-mon in women. These gallbladder diseases cannot bereliably distinguished from each other preoperative-ly using clinical or imaging modalities. Moreover,in a minority of patients, they may even coexist [4].
The exact etiology of XGC is uncertain. It maybe caused by chronic infection and calculi formationin association with bile stasis, since recurrent in-flammation and calculi provoke degeneration and
Fig. 2. Computed tomography (CT) of the upper abdomen. (A, B) Non-contrast CT shows diffuse thickening of thegallbladder wall (A, arrows). Hyperdense gallstones are also evident (B, arrows). (C, D) Contrast CT demonstratessignificant enhancement of the thick wall (arrows), which contains hypodense bands (arrowhead) with uneventhickness.
A B
C D

J Med Ultrasound 2004 • Vol 12 • No 1 19
Xanthogranulomatous Cholecystitis
necrosis of the gallbladder wall and subsequent in-tramural microabscess formation. These intramuralmicroabscesses are occupied by histiocytes in reac-tion to the extravasated bile, eventually replaced byxanthogranulomatous nodules [5].
The presence of gallstones, moderate-to-markedthickening of the gallbladder wall and a complexpoorly marginated mass on US and CT is suggestiveof carcinoma [6]. Itai et al reported gallbladder wallthickening on CT in six of 27 cases (22.2%) withgallbladder carcinoma, but wall thickening was focalin most cases [7]. However, the gallbladder wall cansometimes be diffusely thickened in malignancy andfocally thickened in XGC and simple cholecystitis,so the usefulness of this finding is limited. Chunet al concluded that carcinoma was more probableif there were enlarged regional lymph nodes orheterogeneous adenopathy or if there were multiplemasses or a large heterogeneous mass extending tothe liver [8]. Four groups have reported that thepresence of hypoechoic nodules and bands in athickened gallbladder wall, together with calculi ina patient with chronic gallbladder disease, is highlysuggestive of XGC [5,9–11], as in our patient. Thenodules and bands can behave as xanthogran-ulomatous nodules [11]. A more recent study byShuto et al concluded that luminal surface en-hancement (LSE) of the gallbladder wall representsan intact epithelial layer, and intramural low-attenuation areas correspond to xanthogran-
ulomatous lesions or abscesses on CT [12]. Theyalso found that very high signal intensity on T2-weighted magnetic resonance images were helpfulin differentiating XGC from gallbladder cancer.Although we did not use magnetic resonance imagingfor our patient, the presence of LSE and intramurallow-attenuation areas on CT are highly suggestiveof XGC (Figs. 2C, D).
The pathologic features of XGC parallel xan-thogranulomatous pyelonephritis, and the clinicalpresentation is usually one of chronic cholecystitis[2]. An association with diabetes and obesity issuggested in some series [10]. Most patients presentin their sixth or seventh decade of life [13]. Patientswith XGC may present with a high comorbid factorsuch as perforated gallbladder, abscess formation,or enterobiliary fistula, which were seen in 23% ofpatients with XGC [1,11]. A high rate of postopera-tive morbidity has also been reported [14]. Fortu-nately, these did not happen in our patient.
The role of needle biopsy in the diagnosis ofXGC is controversial. The diagnosis may not be re-liably established with fine needle aspiration biopsy(FNAB) or core biopsy and, if carcinoma is alsopresent, there is concern that the needle track maybe seeded with tumor [10,13]. Demonstration offoamy histiocytes on percutaneous FNAB should behelpful in surgical planning. However, as XGC hasthe potential for fistula formation, some investigatorsbelieve that it is probably contraindicated. It has
Fig. 3. Histopathologic study of a representative specimen. (A) Diffuse chronic inflammatory cell infiltration of thegallbladder wall is associated with focal areas of lipid-laden macrophage accumulation (arrows). (B) In some areas,the lipid-laden macrophages disperse diffusely in the wall.
A B

W.C. Tsai, C.M. Tiu, Y.H. Chou, et al
20 J Med Ultrasound 2004 • Vol 12 • No 1
been suggested that the benign nature of the lesionshould be confirmed by intraoperative frozen sectionfor a preliminary histologic diagnosis [14]. Twocases of XGC were diagnosed by FNAB withoutcomplication [10,15]. In our patient, there were onlytransient fever and mild leukocytosis with left shift.These symptoms and signs disappeared in a fewdays. Further complicating matters, the incidence ofcarcinoma in XGC is up to 10% [11]. Although pre-operative FNAB in our patient demonstrated XGC,there was still some concern about occult malignancy.A negative result on percutaneous FNAB of thegallbladder mass should be interpreted with caution,as almost 50% of cases with negative results in onelarge series had malignancy [16]. Therefore, if aneoplasm is proximal to the body of the gallbladderand is not infiltrating the wall, a secondarily inflamedgallbladder could be misdiagnosed as XGC [10].There is general consensus that percutaneous FNABcan be used in patients with suspicious advancedgallbladder carcinoma to avoid unnecessary lapa-rotomy [10].
In conclusion, XGC has certain characteristic USand CT findings, which reflect the histopathologicfindings. Knowledge of these findings is helpful inthe diagnosis of XGC.
REFERENCES
1. Houston JP, Collins MC, Cameron I, et al. Xanthogran-ulomatous cholecystitis. Br J Surg 1994;81:1030–2.
2. Ros PR, Goodman ZD. Xanthogranulomatouscholecystitis versus gallbladder carcinoma. Radiology1997;203:10–2.
3. Christensen AH, Ishak KG. Benign tumors andpseudotumors of the gallbladder: report of 180 cases.Arch Pathol 1970;90:423–32.
4. Levy AD, Murakata LA, Rohrmann CA. Gallbladder
carcinoma: radiologic-pathologic correlation.Radiographics 2001;21:295–314.
5. Kim PN, Ha HK, Kim YH, et al. US findings ofxanthogranulomatous cholecystitis. Clin Radiol 1998;53:290–2.
6. Hanada K, Nakata H, Nakayama T, et al. Radiographicfindings in xanthogranulomatous cholecystitis. AJRAm J Roentgenol 1987;148:727–30.
7. Itai Y, Araki T, Yoshikawa K, et al. Computedtomography of gallbladder carcinoma. Radiology 1980;137:713–8.
8. Chun KA, Ha HK, Yu ES, et al. Xanthogranulomatouscholecystitis: CT features with emphasis on differen-tiation from gallbladder carcinoma. Radiology 1997;203:93–7.
9. Lichtman JB, Varma VA. Ultrasound demonstrationof xanthogranulomatous cholecystitis. J Clin Ultra-sound 1987;15:342–5.
10. Casas D, Perez-Andres R, Jimenez JA, et al.Xanthogranulomatous cholecystitis: a radiologicalstudy of 12 cases and a review of the literature.Abdom Imaging 1996;21:456–60.
11. Parra JA, Acinas O, Bueno J, et al. Xanthogran-ulomatous cholecystitis: clinical, sonographic, and CTfindings in 26 patients. AJR Am J Roentgenol 2000;174:979–83.
12. Shuto R, Kiyosue H, Komatsu S, et al. CT and MRimaging of xanthogranulomatous cholecystitis:correlation with pathologic findings. Eur Radiol 2004;14:440–6.
13. Reed A, Ryan C, Schwartz SI. Xanthogranulomatouscholecystitis. J Am Coll Surg 1994;179:249–52.
14. Roberts KM, Parsons MA. Xanthogranulomatouscholecystitis: clinicopathological study of 13 cases.J Clin Pathol 1987;40:412–7.
15. Hales MS, Miller TR. Diagnosis of xanthogran-ulomatous cholecystitis by fine needle aspirationbiopsy. A case report. Acta Cytol 1987;31:493–6.
16. Zargar SA, Khuroo MS, Mahajan R, et al. US-guidedfine needle aspiration biopsy of GB masses. Radiology1991;179:275–8.