Embed Size (px)
Citation preview

X-Ray RoundsChris McCrossin

Presentation
45 y/o M
presents with progressive SOB over past week
RR now 60!!
T 38.9, HR 130, BP 120/80
Can’t get much of a history because he’s too SOB to talk
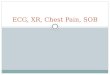
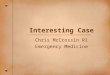
You order a stat portable CXR



Diagnosis Now?

Principles of Pleural Effusions & CXR’s
Effusions when free-flowing follow the force of gravity and accumulate in the most dependent parts of the thoracic cavity
Lungs recoil proportionately when they collapse secondary to elastic recoil and maintains its original shape. The lung floats on the fluid
Fluid layers evenly anterior to posterior in an upright position

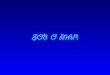
CXR Features of Subpulmonic
EffusionsUp to 1 liter can be present without blunting of the diaphragms
Elevated hemidiaphragm peaks more laterally than expected with a steep lateral slope
Pulmonary vessels are not clearly visible below the surface of the hemidiaphragm on lateral projection
A lateral decubitus view will show free flowing pleural fluid parallel to the xray table





Patient Outcome
ICU Called
Taken to the unit
Small chest tube inserted in R thorax
Drained > 1 liter of frank pus
RR 30 min post chest tube: 16 bpm

Take-Home Points
Pleural effusions and subpulmonic effusions/abscess can look very different
Both can be confused as infiltrates or atelectasis
When you have a patient who is in extremis and you suspect a infiltrative process in the lungs, ask yourself if there is something you can possibly drain, consider a lateral decubitus if you are uncertain