Embed Size (px)
Citation preview

514 JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION NOVEMBER, 1976
X-ray Pelvimetry: Useful Procedure or Medical NonsenseJ. A. CAMPBELL, M.D.,
Martint Luther King Hospital,Los Angeles, California
pHYSICIANS are becoming increasinglyaware of the growing problem of over
utilization of radiologic and laboratoryprocedures. The proliferation of these isone of the major causes of the upward spi-ral of medical patient costs by requiringlarger investments in equipment, suppliesand personnel. Unproductive radiologicexaminations waste manpower and de-crease the efficiency of patient care deliv-ery. The causes of the over utilization ofdiagnostic procedures are numerous. Theseinclude insurance indemnification, fear ofmalpractice suits, training of physicians byprotocol, and the rationalization by clini-cians and radiologists of the usefulness oftraditional procedures or those which du-plicate other findings.
Control of the over utilization of exami-nations requires agreement by cliniciansand radiologists on the worthiness of anygiven procedure based on a medical auditof its effectiveness. If the present escalationof costs continues, we can look to a timewhen economic factors may necessitate thatlicensure or accreditation of physicians belinked to the positive yield of their diagnos-tic laboratory examinations in a mannersimilar to the College of Surgery's accredi-tation of surgeries on the basis of the per-centage of operations yielding pathology.In certain Canadian Provincial health caresystems, payments of insurance benefits toattending physicians, clinicians and radiol-ogists alike, are discounted when the an-nual yield of their diagnostic proceduresexceeds the percentage of the normal pre-scribed by auditing standards.No definitive harm to patients from di-
agnostic radiography has been validated.There is a steady annual increase in thenumber of such examinations. The fact that
the majority of such studies show normalfindings, and that a greater number ofhealthy persons are exposed by screeningprograms causes some public health agen-cies to be concerned about the risk-benefitratio of these diagnostic procedures.
THE PROBLEM
In recent years, ultrasonic technics,where available, have largely replaced ra-diographic examinations in obstetrical di-agnosis. Pelvimetry remains the majorsource of ionizing radiation to the fetus.Understandably, radiologists and obstetri-cians differ in their attitudes toward theusefulness of pelvimetry. Radiologists arechiefly concerned with the discovery of fe-tal, uterine, and placental abnormalities andhaving a growing distrust of pelvimetry asa valid method of determining true ceph-alopelvic disproportion. Obstetricians havebecome more aggressive in their manage-ment of labor with an increased use of in-duction and caesarean section, and there-fore view pelvimetry as an aid in avoidingthe theoretical risk of birth injury duringvaginal delivery through an abnormal pel-vis. To adjust for these philosophical dif-ferences, some radiologists have modifiedtheir pelvimetry technics to include an im-age of the entire uterine contour in theanteroposterior and erect lateral views inorder to improve detection of fetal abnor-malities. It often appears that obstetriciansutilize pelvimetry as a means of reassuringthemselves that the pelvic measurements arenormal in much the same way as a bloodcount or urinalysis is used to exclude ane-mia or diabetes. The question raised byradiologists is whether pelvimetry is accu-rate enough in sorting out those cases which
Vol. 68, No. 6 X-ray Pelvimetry 515
are at risk in vaginal delivery to justify itsuse. It is easy to find statistical evidence tosupport their skepticism.
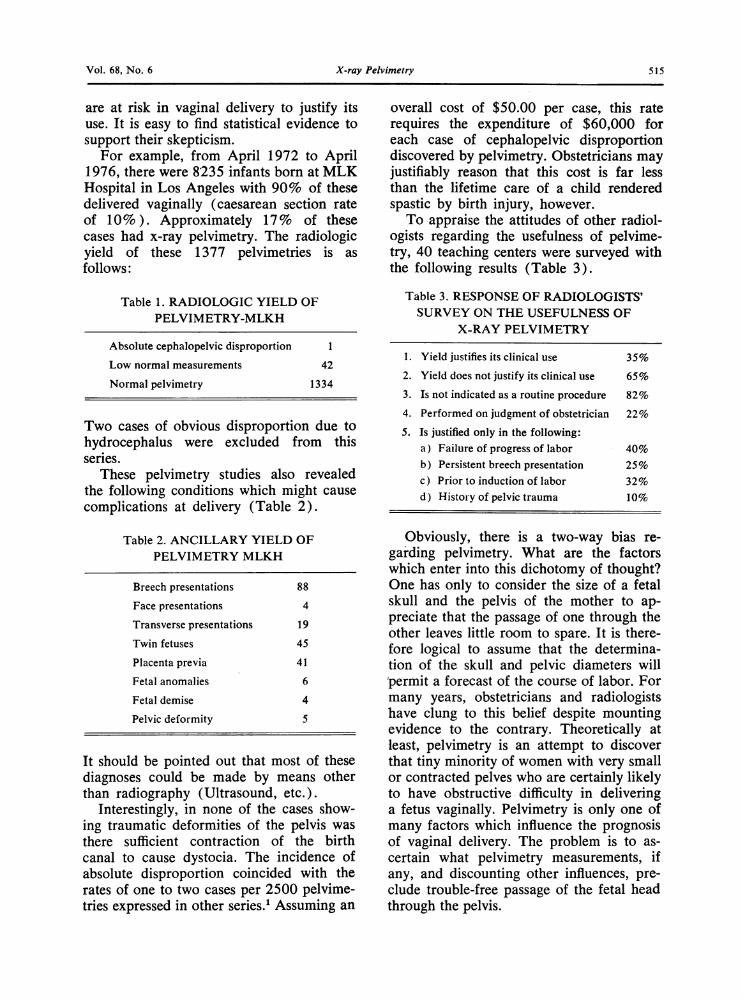
For example, from April 1972 to April1976, there were 8235 infants born at MLKHospital in Los Angeles with 90% of thesedelivered vaginally (caesarean section rateof 10%). Approximately 17% of thesecases had x-ray pelvimetry. The radiologicyield of these 1377 pelvimetries is asfollows:
Table 1. RADIOLOGIC YIELD OFPELVIMETRY-MLKH
Absolute cephalopelvic disproportion 1
Low normal measurements 42
Normal pelvimetry 1334
Two cases of obvious disproportion due tohydrocephalus were excluded from thisseries.
These pelvimetry studies also revealedthe following conditions which might causecomplications at delivery (Table 2).
Table 2. ANCILLARY YIELD OFPELVIMETRY MLKH
Breech presentations 88
Face presentations 4
Transverse presentations 19
Twin fetuses 45
Placenta previa 41
Fetal anomalies 6
Fetal demise 4
Pelvic deformity S
It should be pointed out that most of thesediagnoses could be made by means otherthan radiography (Ultrasound, etc.).
Interestingly, in none of the cases show-ing traumatic deformities of the pelvis wasthere sufficient contraction of the birthcanal to cause dystocia. The incidence ofabsolute disproportion coincided with therates of one to two cases per 2500 pelvime-tries expressed in other series.' Assuming an
overall cost of $50.00 per case, this raterequires the expenditure of $60,000 foreach case of cephalopelvic disproportiondiscovered by pelvimetry. Obstetricians mayjustifiably reason that this cost is far lessthan the lifetime care of a child renderedspastic by birth injury, however.To appraise the attitudes of other radiol-
ogists regarding the usefulness of pelvime-try, 40 teaching centers were surveyed withthe following results (Table 3).
Table 3. RESPONSE OF RADIOLOGISTS'SURVEY ON THE USEFULNESS OF
X-RAY PELVIMETRY
1. Yield justifies its clinical use 35%
2. Yield does not justify its clinical use 65%
3. Is not indicated as a routine procedure 82%
4. Performed on judgment of obstetrician 22%
5. Is justified only in the following:a) Failure of progress of labor 40%b) Persistent breech presentation 25%c) Prior to induction of labor 32%d) History of pelvic trauma 10%
Obviously, there is a two-way bias re-garding pelvimetry. What are the factorswhich enter into this dichotomy of thought?One has only to consider the size of a fetalskull and the pelvis of the mother to ap-preciate that the passage of one through theother leaves little room to spare. It is there-fore logical to assume that the determina-tion of the skull and pelvic diameters willpermit a forecast of the course of labor. Formany years, obstetricians and radiologistshave clung to this belief despite mountingevidence to the contrary. Theoretically atleast, pelvimetry is an attempt to discoverthat tiny minority of women with very smallor contracted pelves who are certainly likelyto have obstructive difficulty in deliveringa fetus vaginally. Pelvimetry is only one ofmany factors which influence the prognosisof vaginal delivery. The problem is to as-certain what pelvimetry measurements, ifany, and discounting other influences, pre-clude trouble-free passage of the fetal headthrough the pelvis.
516 JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION NOVEMBER, 1976
FACTORS INVOLVED IN THE
CLINICAL BIAS
It is the obstetrician who chiefly governsthe indications for pelvimetry. He selects,by clinical assessment, the woman whom hesuspects has a small pelvis. This process isdifficult and highly imperfect. Russell andRichards2 compared the pelvic sizes ofwomen referred for pelvimetry with thoseof a control group and revealed only small,differences in the two groups. The pelvime-try patients showed 6% with at least onemeasurement smaller by 2 standard devia-tions than the mean. In the control group,this figure was also 6%. The caesarean sec-tion rate for the pelvimetry group was 29%.while the section rate for all patients in thehospital for the same period was 8.1%. Itwas noted that this high section rate oc-curred even in patients with average orlarger than average pelvic measurements.
Similarly, these authors noted that theforceps rate for women with cephalic vagi-nal deliveries was 23%, more than fourtimes the average for those with similar ver-tex deliveries who did not have pelvimetry.It would appear that the obstetricians inthis series were chiefly selecting for radio-logic pelvimetry those patients who weregoing to have difficulty in labor rather thanthose with small pelves. Russell2 felt that inthe large majority of referrals, pelvic sizewas not the important factor, nor was fetalsize, because he found no difference in thebirth weight between pelvimetry patientsand those of the normal hospital popula-tion. From this study, this author concludedthat the factor causing referral is likely tobe tightness or poor relaxation of the softtissues which make digital pelvic assessmentdifficult and give rise to soft tissue dystociawith poor pelvic molding. Pelvimetry is ofno help in evaluating this factor. This evi-dence would support the thesis that thebony pelvis is responsible for dystocia inonly a very small minority of cases. Thusit would appear that in considering patientsfor pelvimetry there is need for a moreaccurate clinical assessment of pelvic size
in an effort to identify the larger group ofdystocic patients who have normal pelvicsize. The radiologists surveyed often ex-pressed the opinion that younger obstetri-cians order normal pelvimetries more fre-quently than their more experienced col-leagues, probably reflecting their insecurityin clinical assessment of the patient. Inmany institutions, residents in obstetrics aretaught to request pelvimetry by protocol,rather than by clinical decision. It seemsreasonable to insist that pelvimetry be car-ried out only after clinical assessment by asenior obstetrician if over-utilization of thisexamination is to be curbed.
Clinicians can assess the ability of thefetal head to enter the pelvic inlet as a meas-ure of disproportion, but they should notconclude that the head "won't push in" un-less the patient has been examined whilestanding. Frequently, when such patientsare referred for pelvimetry, the erect lateralfilm shows the head to be easily engaged.
Because the engagement of the head isoften delayed in the teenage mother, fear ofdisproportion may arise. Mussio3 showedthat there is little change in the size andshape of the pelvis after puberty, and anygrowth is completed within a year. Thusthe incidence of cephalopelvic disproportionis not increased in adolescence, and youthin itself is not an indication for pelvimetry.A persistent breech presentation in a primipdoes need careful clinical consideration. Itshould be poined out, however, that per-sistence of the breech position usually oc-curs in women with a large, not a small pel-vic inlet, which more readily accommodatesthe breech. Thus the probability is that thetransverse inlet diameter is usually widerthan normal in such presentations. Toddand Steer4 found in a review of 1006 breechdeliveries that a sagittal inlet of 11.0 cm(which can be estimated by vaginal exami-nation), allowed safe vaginal delivery.Since molding of the fetal head is chieflycaused by uterine pressures, not the bonypelvis, the diameter of the head is capableof about as much reduction in diameter inbreech as with vertex deliveries.
Vol. 68, No. 6 X-ray Pelvimetry 517
Another interesting observation in ourseries was the 80% incidence of definitediastasis of the symphysis pubis in cases ofbreech presentation even when the fetal pel-vis was not engaged in the inlet. This find-ing is further evidence that pelvic moldingis not necessarily the result of mechanicalintrapelvic forces. A small group of womenneeding special attention are those with ahistory of trauma or other deforming dis-ease affecting the pelvis. A review of pre-vious pelvic films during prenatal care ismost valuable in deciding if pelvimetry isneeded.An obstetrician, with a "favorite" meas-
urement associated with difficult vaginal de-livery, is strongly biased toward interferencewith the natural labor of a woman in whomhe knows this measurement to be outside ofhis normal limit. However, retrospectiveanalyses (by Borell and Fernstrom5) madeon data which were not used to prove thespecific value of some measurement, failedto justify such a correlation. In line withthis, Russell6 points out that, if a smallpelvis is defined as one with a measurementassociated with an increased rate of for-ceps delivery, 4% of women who had pel-vimetry have a small pelvis. However, 2%of women who did not have pelvimetry,have a small pelvis similarly defined. Ourseries showed even less difference in therate of low forceps deliveries between thepelvimetry and non-pelvimetry groups.
FACTORS INVOLVED IN THE
RADIOLOGIC BIAS
There are several important factorswhich significantly offset the precision ofpelvimetry measurements as an indicator ofdystocia. The first of these is the reshapingof the fetal head diameters during labor asa result of molding. Head molding is mostmarked when the head is above the outlet.In the great majority of instances, the bonypelvis is large enough to transmit the un-molded head. Lindgren7 pointed out thatmolding of the head is a response to softtissue pressure. The fact that head moldingis not infrequently seen in breer- resen-
tations would suggest that the uterine mus-culature forcibly pushes the uppermost partof the fetus downward. Molding of the headis capable of reducing the biparietal andoccipitofrontal diameters by more than 1cm. Evaluation of the fetal skull area orvolume in relationship to the pelvic sizewas made by King, who found no convinc-ing evidence that this approach added to theaccuracy of predicting dystocia.A second factor, often not fully appre-
ciated, is molding of the maternal pelviswhich produces alterations in its dimen-sions. Graham8 noted that even in the Hip-pocratic era, it was assumed that the pelvisexpanded during delivery. This was firstthought to be a simple diastasis of the sym-physis pubis, but later recognized that asthe pressures separated the ischial spines,
..........~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ ..
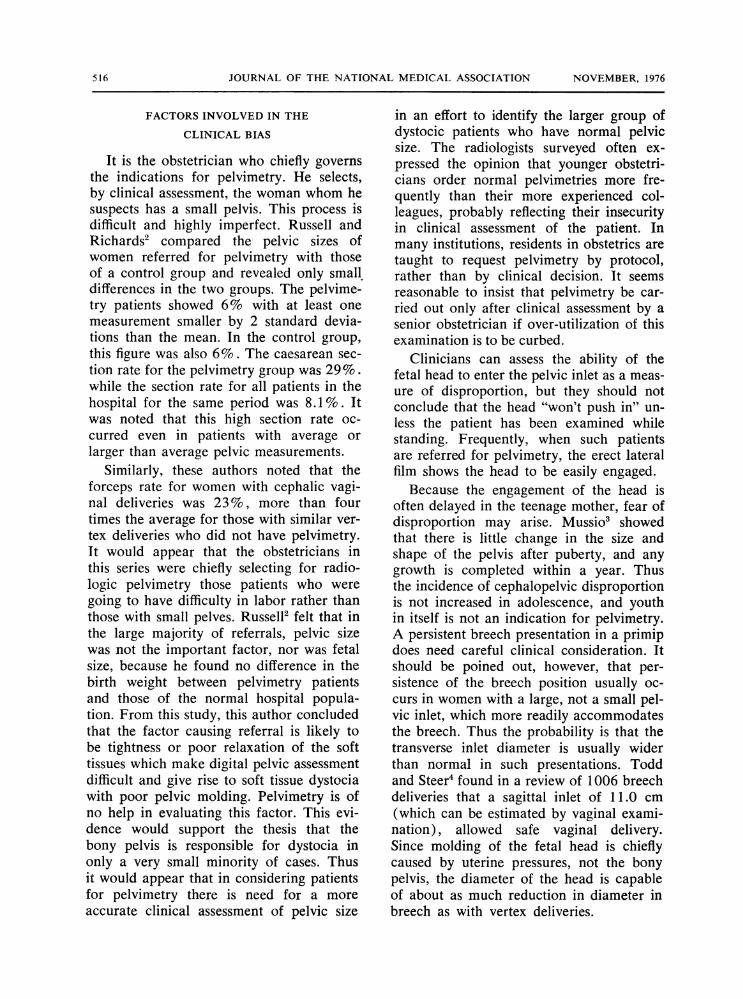
Fig. 1. Pelvic Molding in Vertex Presentation. Thereis wide separation of the symphysis pubis, eventhough the fetal head is high in the pelvis.
the iliac crests moved inwards to produce arocking motion of the symphysis, effectingits separation. The sacroiliac is a synovialtype of joint capable of considerable mo-tion in both males and females, but theseare greatly increased in pregnancy. Sacro-iliac motion is either sliding or rotatory incharacter relative to the pelvis girdle. Thesemotions are visible on successive lateralradiographs of the pelvis on a subject ex-posed in different postures. Movements ofthe legs and trunk cause sacroiliac motiondepending on the stresses exerted such asthe asymmetrical one commonly observedin walking. These rotary or sliding move-ments of the sacroiliac joints alter the coro-nal and sagittal diameters of the pelvis.
518 JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION NOVEMBER, 1976
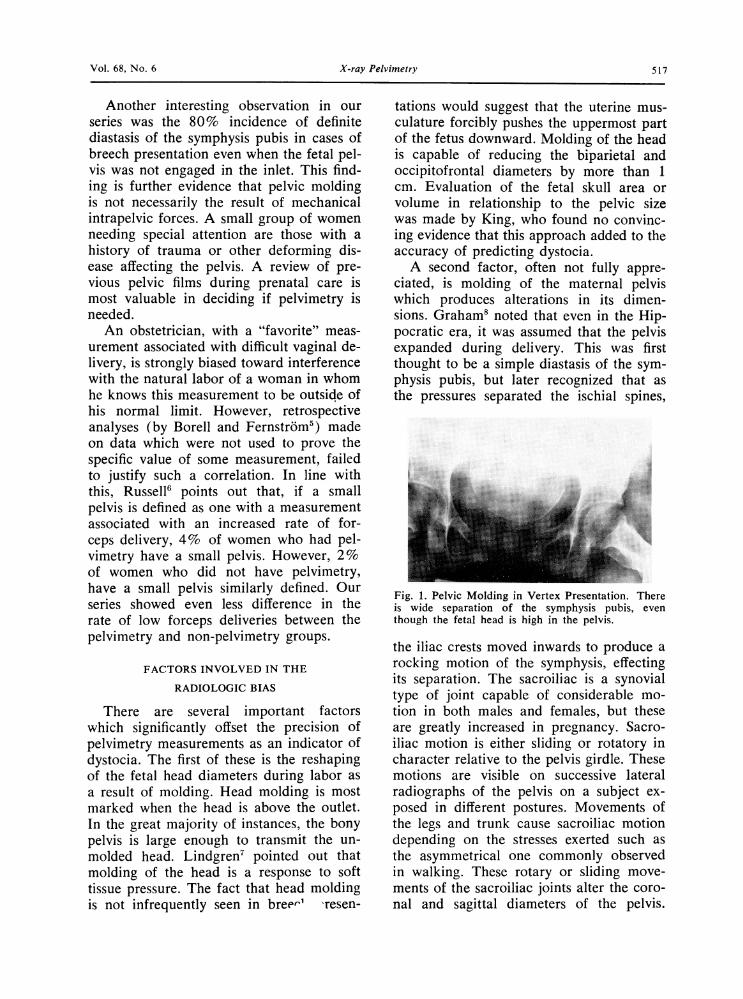
During pregnancy, the iliac crests move in-ward or outward causing separation of theischial spines and the symphysis. This sep-aration is considerably greater than theactual movement of the sacroiliac becauseof the principle of levers (Figs. 1 and 2).
Fig. 2. Pelvic Molding in Breech Presentation. Thesymphysis pubis is widely separated even though thefetal breech lies in the pelvic inlet.
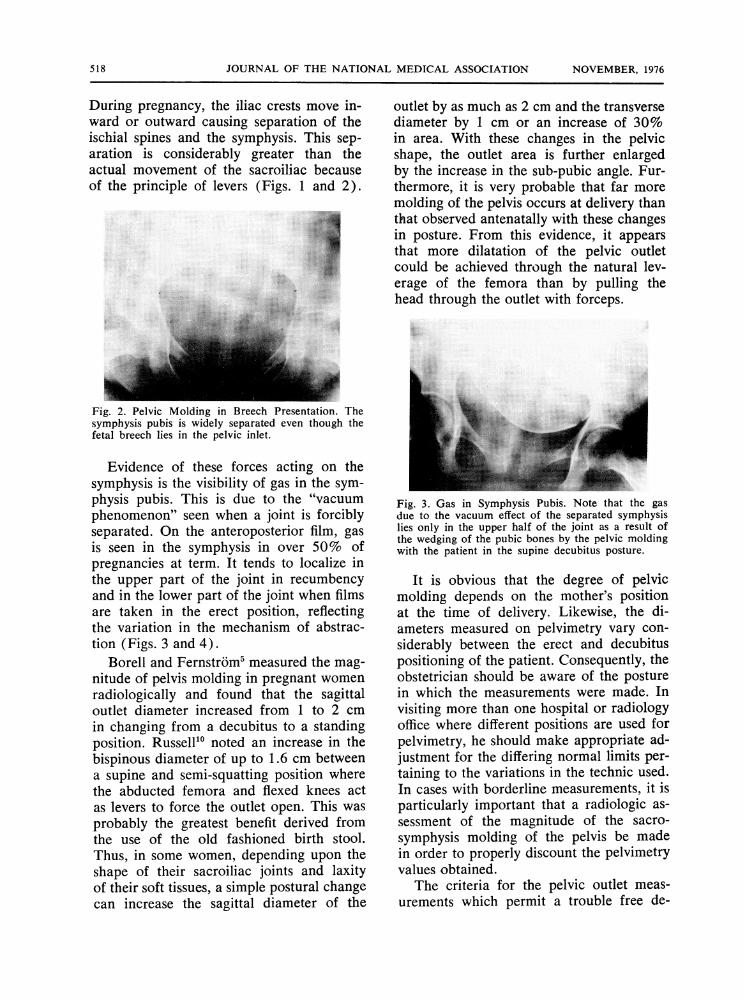
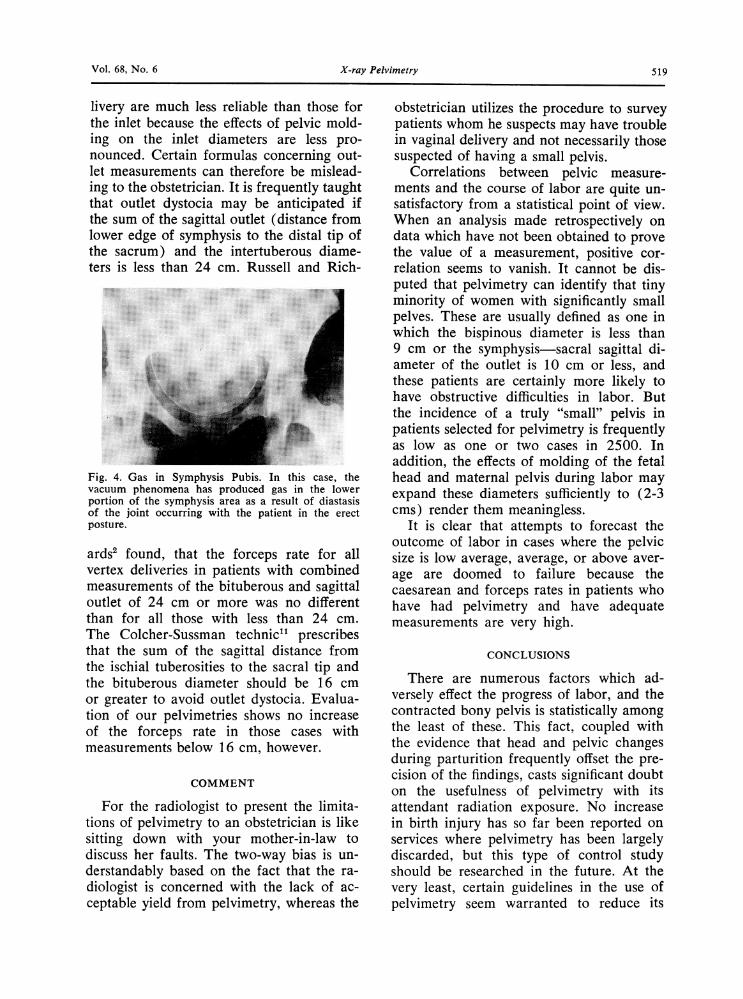
Evidence of these forces acting on thesymphysis is the visibility of gas in the sym-physis pubis. This is due to the "vacuumphenomenon" seen when a joint is forciblyseparated. On the anteroposterior film, gasis seen in the symphysis in over 50% ofpregnancies at term. It tends to localize inthe upper part of the joint in recumbencyand in the lower part of the joint when filmsare taken in the erect position, reflectingthe variation in the mechanism of abstrac-tion (Figs. 3 and 4).
Borell and Fernstrdm' measured the mag-nitude of pelvis molding in pregnant womenradiologically and found that the sagittaloutlet diameter increased from 1 to 2 cmin changing from a decubitus to a standingposition. Russell" noted an increase in thebispinous diameter of up to 1.6 cm betweena supine and semi-squatting position wherethe abducted femora and flexed knees actas levers to force the outlet open. This wasprobably the greatest benefit derived fromthe use of the old fashioned birth stool.Thus, in some women, depending upon theshape of their sacroiliac joints and laxityof their soft tissues, a simple postural changecan increase the sagittal diameter of the
outlet by as much as 2 cm and the transversediameter by 1 cm or an increase of 30%in area. With these changes in the pelvicshape, the outlet area is further enlargedby the increase in the sub-pubic angle. Fur-thermore, it is very probable that far moremolding of the pelvis occurs at delivery thanthat observed antenatally with these changesin posture. From this evidence, it appearsthat more dilatation of the pelvic outletcould be achieved through the natural lev-erage of the femora than by pulling thehead through the outlet with forceps.
:~~ ~~~~~~~~~~~~~~. .. .........
Fig. 3. Gas in Symphysis Pubis. Note that the gasdue to the vacuum effect of the separated symphysislies only in the upper half of the joint as a result ofthe wedging of the pubic bones by the pelvic moldingwith the patient in the supine decubitus posture.
It is obvious that the degree of pelvicmolding depends on the mother's positionat the time of delivery. Likewise, the di-ameters measured on pelvimetry vary con-siderably between the erect and decubituspositioning of the patient. Consequently, theobstetrician should be aware of the posturein which the measurements were made. Invisiting more than one hospital or radiologyoffice where different positions are used forpelvimetry, he should make appropriate ad-justment for the differing normal limits per-taining to the variations in the technic used.In cases with borderline measurements, it isparticularly important that a radiologic as-sessment of the magnitude of the sacro-symphysis molding of the pelvis be madein order to properly discount the pelvimetryvalues obtained.
The criteria for the pelvic outlet meas-urements which permit a trouble free de-
Vol. 68, No. 6 X-ray Pelvimetry 519
livery are much less reliable than those forthe inlet because the effects of pelvic mold-ing on the inlet diameters are less pro-nounced. Certain formulas concerning out-let measurements can therefore be mislead-ing to the obstetrician. It is frequently taughtthat outlet dystocia may be anticipated ifthe sum of the sagittal outlet (distance fromlower edge of symphysis to the distal tip ofthe sacrum) and the intertuberous diame-ters is less than 24 cm. Russell and Rich-
Fig. 4. Ga iSypssPus. Inths.as,.h
vacuum phenomena has produced gas in. the lowe
........................̂,0.X-'s'B.,.'° 8~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~...............
.o.....joit. in .h.p i the erc
... .. ...o3.<.|- S.*~~~~~~~~~~~~~~~~~~. ...S .. t...Fig. 4. Gas in Symphysis Pubis. In this case, thevacuum phenomena has produced gas in the lowerportion of the symphysis area as a result of diastasisof the joint occurring with the patient in the erectposture.
ardst found, that the forceps rate for allvertex deliveries in patients with combinedmeasurements of the bituberous and sagittaloutlet of 24 cm or more was no differentthan for all those with less than 24 cm.The Colcher-Sussman technic"l prescribesthat the sum of the sagittal distance fromthe ischial tuberosities to the sacral tip andthe bituberous diameter should be 16 cmor greater to avoid outlet dystocia. Evalua-tion of our pelvimetries shows no increaseof the forceps rate in those cases withmeasurements below 16 cm, however.
COMMENT
For the radiologist to present the limita-tions of pelvimetry to an obstetrician is likesitting down with your mother-in-law todiscuss her faults. The two-way bias is un-derstandably based on the fact that the ra-diologist is concerned with the lack of ac-ceptable yield from pelvimetry, whereas the
obstetrician utilizes the procedure to surveypatients whom he suspects may have troublein vaginal delivery and not necessarily thosesuspected of having a small pelvis.
Correlations between pelvic measure-ments and the course of labor are quite un-satisfactory from a statistical point of view.When an analysis made retrospectively ondata which have not been obtained to provethe value of a measurement, positive cor-relation seems to vanish. It cannot be dis-puted that pelvimetry can identify that tinyminority of women with significantly smallpelves. These are usually defined as one inwhich the bispinous diameter is less than9 cm or the symphysis-sacral sagittal di-ameter of the outlet is 10 cm or less, andthese patients are certainly more likely tohave obstructive difficulties in labor. Butthe incidence of a truly "small" pelvis inpatients selected for pelvimetry is frequentlyas low as one or two cases in 2500. Inaddition, the effects of molding of the fetalhead and maternal pelvis during labor mayexpand these diameters sufficiently to (2-3cms) render them meaningless.
It is clear that attempts to forecast theoutcome of labor in cases where the pelvicsize is low average, average, or above aver-age are doomed to failure because thecaesarean and forceps rates in patients whohave had pelvimetry and have adequatemeasurements are very high.
CONCLUSIONS
There are numerous factors which ad-versely effect the progress of labor, and thecontracted bony pelvis is statistically amongthe least of these. This fact, coupled withthe evidence that head and pelvic changesduring parturition frequently offset the pre-cision of the findings, casts significant doubton the usefulness of pelvimetry with itsattendant radiation exposure. No increasein birth injury has so far been reported onservices where pelvimetry has been largelydiscarded, but this type of control studyshould be researched in the future. At thevery least, certain guidelines in the use ofpelvimetry seem warranted to reduce its
520 JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION NOVEMBER, 1976
overutilization. The following suggestionsare offered.
1. Select patients on the basis of indi-vidual clinical assessment, not by protocol.
2. Other causes for failure of progressof labor should be excluded, by other meth-ods when possible, prior to pelvimetry.
3. The possibility of inlet dystocia shouldbe assessed clinically or by ultrasoundmethods, with the patient erect, prior toemploying pelvimetry.
4. Dystocia due to fetal anomalies, pla-centa previa, multiple pregnancy, and fetaldemise can usually be diagnosed by ultra-sound without resort to pelvimetry.
5. The magnitude of pelvic moldingshould be assessed in all cases with lowpelvimetry measurements.
6. The significance of pelvic deformi-ties can be assessed on prior films withoutresort to pelvimetry.
7. Induction of labor is not in itself anindication for pelvimetry.
8. Breech presentation is not in itself anindication for pelvimetry.
9. Youth (adolescence) is not in itselfan indication for pelvimetry.
LITERATURE CITED
1. Quoted by SANDERS, R. C. on experience at
Johns Hopkins Hospital, Baltimore, Md.,1976.
2. RUSSELL, J. G. B. and B. RICHARDS. A Re-view of Pelvimetry Data. Brit. J. Radiol.,44:780-784, 1971.
3. Mussio, T. J. Primigravidas Under Fourteen.Am. Jour. Obstet. Gynecol., 84:442-444,1962.
4. TODD, W. D. and C. M. STEER. Term Breech:A Review of 1,006 Term Breech Deliveries.Obstet. Gynecol., 22:583-595.
5. BORELL, U. and K. FERNSTROM. RadiologicPelvimetry. Acta Radiologica, Supplement,191:1960.
6. RUSSELL, J. G. B. Radiology in Obstetricsand Antenatal Pediatrics, Radiology in Clini-cal Diagnosis Series, Butterworth and Co.Ltd., London, 1973.
7. LINDGREN, L. The lower Part of the UterusDuring the First Stage of Labor in the Oc-cipitoanterior Vertex Presentation. Acta Ob-stetrica et Gynecologica, 34: Supplement 2,1955.
8. GRAHAM, H. Quoted by Eternal Eve., London,Hein1emann, 49, 1950.
9. BORELL, U. and K. FERNSTROM. The Move-ments at the Sacroiliac Joints and Their Im-portance to Changes in the Pelvic DimensionsDuring Parturition. Acta Obstetrica et Gyne-cologica, 36:42-57, 1957.
10. RUSSELL, J. G. B. Moulding of the PelvicOutlet. J. Obstet. Gynecol. Brit. Common-wealth, 76:817-820, 1969.
11. COLCHER, A. E. and W. SUSSMAN. PracticalTechnique for Roentgen Pelvimetry withNew Positioning. Am. J. Roentgenol., 51:207, 1944.
(Thompson et al., from page 539)
ease Syllabus, Waverly Press, Inc., Baltimore,Maryland 1973.
3. PAUL, L. and K. JUHL. Essentials of Roent-gen Interpretation: Harper and Row Pub-lishers, Hagerstown, Maryland 1972.
4. BEASON, P. and W. McDERMOTT. Textbookof Medicine. W. B. Saunders, Philadelphia1971, p. 644.
5. WILSON, J. J. and H. H. MARKS. Calcifica-tion of the vas deferens: Its relation to dia-betes mellitus and arteriosclerosis. New Engl.J. Med., 245:321-325, 1951.
6. WEBBE, G. ET AL. Schistosomia hematobiumin the Baboon. Ann. Tropical Med. Parasitol.,68:187-201, 1974.
7. YOUNG ET AL. Urinary Schistosomasis: AFive Year Clinical Radiological and Func-
tional Evaluation. Transactions of the RoyalSociety of Tropical Medicine and Hygiene,67:379-382, 1973.
8. FARRID, Z. ET AL. Urinary Schistosomiasis.Transactions of the Royal Society of TropicalMedicine and Hygiene, 64:122, 1970.
9. FORSYTH, D. and M. HUGHES. Some Long-Term Results of Treating Urinary Schistoso-miasis in Kuwait. Transactions of the RoyalSociety of Tropical Medicine and Hygiene,67:671-673, 1973.
10. LEHMAN, J. S. et al. Urinary Schistosomia-sis in Egypt. Clinical, Radiological, Bacterio-logical and Parasitological Correlations.Transactions of the Royal Society of Tropi-cal Medicine and Hygiene, 65:384-399, 1973.