Embed Size (px)
Citation preview

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
The Radiobiology Behind Alternate The Radiobiology Behind Alternate Physical Forms of Radiation Delivery Physical Forms of Radiation Delivery
Bill McBrideBill McBrideDept. Radiation OncologyDept. Radiation Oncology
David Geffen School MedicineDavid Geffen School MedicineUCLA, Los Angeles, Ca.UCLA, Los Angeles, Ca.
[email protected]@mednet.ucla.edu

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
Alternatives Forms of Radiation Alternatives Forms of Radiation DeliveryDelivery
Sometimes called plesiocurie therapy

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
PhotonPhoton
PhotonPhoton
ParticleParticle
TomotherapyTomotherapy®®
CyberKnifeCyberKnife®®
X-KnifeX-Knife®®
SRT, 3D-CRT, IMRT, IGRTSRT, 3D-CRT, IMRT, IGRT
Linear Linear AcceleratorAccelerator
SRS - GammaKnifeSRS - GammaKnife®®CobaltCobalt6060 Based Based
Heavy IonHeavy Ion
ProtonProton
Heavy Ion CentersHeavy Ion Centers
Synchrotron Synchrotron
ParticleParticle
ImplementationImplementationCategoryCategory
The Alternatives are Growing!The Alternatives are Growing!
BrachytherapyBrachytherapy Isotope BasedIsotope Based Ultra low dose rate, LDR, HDRUltra low dose rate, LDR, HDR

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
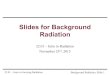
BrachytherapyBrachytherapy
Dose falls off with one upon the square of distance Dose falls off with one upon the square of distance
rr22
rr11
SeedSeed
0.10.1
11
1010
100100
Rel
ativ
e do
seR
elat
ive
dose
00 11 22 33 44 55 66
125I
Distance (cm)
NormalNormaltissuetissue
Therapeutically relevant range 3-20mm
Potential radiobiological Potential radiobiological advantage in reduced advantage in reduced exposed normal tissue exposed normal tissue volume and dose volume and dose distribution fall-off. distribution fall-off.

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
BrachytherapyBrachytherapy
• Potential radiobiological advantages of brachytherapy Potential radiobiological advantages of brachytherapy include varying treatment times include varying treatment times – Short treatment time could prevent tumor Short treatment time could prevent tumor
repopulation, repopulation, – Longer could redistribute cells into sensitive cell Longer could redistribute cells into sensitive cell
cycle phases, cycle phases, – Longer could allow re-oxygenation with time after Longer could allow re-oxygenation with time after
implantation.implantation.

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
• ULDRULDR– 0.01 - 0.3 Gy/hr0.01 - 0.3 Gy/hr– permanent implantspermanent implants– 125125I, I, 103103 Pd Pd
• LDR LDR – 0.4 - 2 Gy/hr0.4 - 2 Gy/hr– treatment times of 24 - 144 hrstreatment times of 24 - 144 hrs– 226226 Ra, Ra, 137137 Cs Cs
• HDRHDR
– 12 - 430 Gy/hr at 1 cm12 - 430 Gy/hr at 1 cm– treatment time in mins to hrstreatment time in mins to hrs
– 6060Co, Co, 192192IrIr

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
LDR and HDR BrachytherapyLDR and HDR Brachytherapy
• LDR differentially spares late-responding tissues LDR differentially spares late-responding tissues compared to early-responding normal tissue and compared to early-responding normal tissue and tumorstumors
• HDR is assumed to compromise the radiobiological HDR is assumed to compromise the radiobiological advantage of LDR in favor of patient convenience, advantage of LDR in favor of patient convenience, minimizing risk to staff, and better dosimetryminimizing risk to staff, and better dosimetry

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
Dose Rate EffectsDose Rate Effects
• In general decreasing dose rate decreases In general decreasing dose rate decreases killing, however in some cases there is an killing, however in some cases there is an inverse dose rate effect, which is thought to inverse dose rate effect, which is thought to be due to redistribution and cells piling up in be due to redistribution and cells piling up in the radiosensitive G2 cell cycle check point.the radiosensitive G2 cell cycle check point.

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
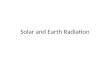
Inverse Dose Rate EffectInverse Dose Rate Effect
Mitchell J.B. et al., Rad. Res. 79:552, 1979
V79 cells log phase
HeLa cells log phase
0.55 Gy/hr
1.43 Gy/hr
Dose (cGy) Dose (cGy)
1.54 Gy/hr
1.43 Gy/hr
1.54 Gy/hr
0.55 Gy/hr

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
Inverse Dose Rate EffectInverse Dose Rate Effect = 10= 101/2 1/2 2 2 = 0.02= 0.02T1/2 repair = 0.7 hrT1/2 repair = 0.7 hrT1/2 resens. = 4 hrT1/2 resens. = 4 hr
T1/2 pot = 33 hrT1/2 pot = 33 hr
Dose (Gy)Dose (Gy)
0.0010.001
0.010.01
0.10.1
11
S.F.S.F.
00 1010 2020 3030 4040
0.1Gy/hr0.1Gy/hr
0.15 Gy/hr0.15 Gy/hr1 Gy/hr1 Gy/hr
0.75 Gy/hr0.75 Gy/hr0.25 Gy/hr0.25 Gy/hr
R. Suwinski

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
Determinants of Radiation ResponseDeterminants of Radiation Response
• RepairRepair
• RepopulationRepopulation
• RedistributionRedistribution
ResensitizationResensitization• ReoxygenationReoxygenation

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
LQR ModelLQR Model
• A LQR model that takes into account repair, repopulation, and A LQR model that takes into account repair, repopulation, and resensitizationresensitization
• Assumes decrease in radiosensitivity immediately after Assumes decrease in radiosensitivity immediately after irradiation followed by a resensitization phaseirradiation followed by a resensitization phase
• Assumes intratumoral heterogeneity that averages out Assumes intratumoral heterogeneity that averages out oscillations in the process of resensitizationoscillations in the process of resensitization
• Assumes resensitization can be described by a single amplitude Assumes resensitization can be described by a single amplitude and a single characteristic timeand a single characteristic time
Brenner et al. Int. J. Rad. Oncol. Biol. Phys. 32:379, 1995Brenner et al. Int. J. Rad. Oncol. Biol. Phys. 32:379, 1995

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
A Mathematical ModelA Mathematical Model
S = exp [ - S = exp [ - D D one-track killing one-track killing
- - G(G(rr).D).D22 two-track killingtwo-track killing
+ (1/2+ (1/222).G().G(s).Ds).D22 resensitization resensitization
+ T/+ T/pp]] repopulationrepopulation
where:where: is average of a Gaussian distribution with variance is average of a Gaussian distribution with variance 22,,
G is the generalized Lea-Catcheside function, and represents reduction in damage due to repair or G is the generalized Lea-Catcheside function, and represents reduction in damage due to repair or resensitizationresensitization
rr is repair time in min.- hrs., is repair time in min.- hrs.,
s is resensitization time in hrs.- dys.,s is resensitization time in hrs.- dys.,
pp is the repopulation time, is the repopulation time,
and a total dose D is delivered in time T.and a total dose D is delivered in time T.

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
Suggested ParametersSuggested Parameters
Tpot T1/2repair
T1/2sens
1/22
Early 0.3 0.03 10 2 dys 1 hr 4 hr 0.01
Late 0.15 0.075 2 60 dys 4 hr 4 hr 0.01
ProstateCa
0.225 0.053 4.3 30 dys 3 hr 4 hr 0.01
FastGrowing
Tumor0.3 0.03 10 10 dys 2 hr 4 hr 0.02

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
00..00
00..55
11..00
11..55
22..00
22..55
33..00
33..55
0.060.060.080.080.100.10
0.200.20
0.400.40
0.600.600.800.801.001.00
2.002.00
4.004.00
6.006.00
8.008.00
10.0010.00
20.0020.00
30.0030.0040.0040.00
TTUUMMOORR ((//==1100,, TTdd==3300 ddaayyss))
vvss..LLAATTEE EEFFFFEECCTT
((//==22,, TTdd>>330000 ddaayyss))
Dose Rate (Gy/dy)Dose Rate (Gy/dy)
A Mathematical ModelA Mathematical Model
The The ““Golden ZoneGolden Zone””
TherapeuticTherapeuticBenefitBenefit
R. Suwinski

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
125125I ImplantsI Implants
0.0010.001
0.010.01
0.10.1
11
00 1010 2020 3030 4040 5050
SFSF
Dose (Gy)Dose (Gy)
Fast GrowingFast GrowingTumorTumor
Normal tissueNormal tissueSlow Growing Slow Growing
TumorTumor
Initial dose rate ofInitial dose rate of1.68 Gy/day1.68 Gy/day
R. Suwinski

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
• Spatial distribution of dose Spatial distribution of dose
– advantage can be taken of dose fall off and optimizing dose advantage can be taken of dose fall off and optimizing dose distributions. The geometric sparing factor (f)= effective normal tissue distributions. The geometric sparing factor (f)= effective normal tissue dose/effective tumor dose, varies with timedose/effective tumor dose, varies with time
• RBE (RBE (125125I may be 1.4, but hard to estimate)I may be 1.4, but hard to estimate)
• Dose inhomogeneity, including, associated dose rate effects, can Dose inhomogeneity, including, associated dose rate effects, can however, be particularly severe in brachytherapyhowever, be particularly severe in brachytherapy
• Inhomogeneity may be beneficial when implant is sub-optimal and tumor Inhomogeneity may be beneficial when implant is sub-optimal and tumor rapidly growingrapidly growing
• Adequate dosage to the whole tumor is paramountAdequate dosage to the whole tumor is paramount

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
Energetic Protons (65-250 MeV)Energetic Protons (65-250 MeV)• AdvantagesAdvantages
– Good dose distribution with finite range in tissue and Good dose distribution with finite range in tissue and rapid fall off (Bragg peak), but not laterally due to rapid fall off (Bragg peak), but not laterally due to scatteringscattering
– But need to spread out the Bragg peak - SOBPBut need to spread out the Bragg peak - SOBP• Active scattering using deflecting magnets and scanning Active scattering using deflecting magnets and scanning
(IMPT)(IMPT)• Passive scattering Passive scattering
• DisadvantagesDisadvantages• Best use of fall off depends on knowing the tumor marginsBest use of fall off depends on knowing the tumor margins• Tissue density issuesTissue density issues• Limited clinical data, no randomized clinical trialsLimited clinical data, no randomized clinical trials• High energy secondary neutrons with passive scattering High energy secondary neutrons with passive scattering
from materials in the beamline may carry increased from materials in the beamline may carry increased cancer risk with high Q factor cancer risk with high Q factor
– Brenner and Hall Radiotherapy Oncol. 86: 165-170, 2000Brenner and Hall Radiotherapy Oncol. 86: 165-170, 2000
Biological properties of Biological properties of protonsprotons (RBE and (RBE and OER) OER) similar to X-rays similar to X-rays RBE=1.1 but may be 2 at RBE=1.1 but may be 2 at distal edge of Bragg peakdistal edge of Bragg peak
From Chen Neurosurg 23: 1-5, 2007

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
ProtonsProtons• About 25 facilities operating world-About 25 facilities operating world-
wide, and growing. wide, and growing. – Over 50,000 patients have Over 50,000 patients have
been treatedbeen treated• Due to excellent dose distributions, Due to excellent dose distributions,
have shown clear efficacy for:have shown clear efficacy for:– Choroidal melanomaChoroidal melanoma– Some spinal cord and brain Some spinal cord and brain
tumorstumors– Sphenoid sinus tumorsSphenoid sinus tumors
• Also being used for a wide Also being used for a wide spectrum of tumors (e.g., prostate, spectrum of tumors (e.g., prostate, pediatric, lung, breast, head and pediatric, lung, breast, head and neck, etc.) neck, etc.)

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
Heavy Charged ParticlesHeavy Charged Particles
• Helium ions in UCB-LBL since 1954 to treat AVMs but the beams Helium ions in UCB-LBL since 1954 to treat AVMs but the beams were contaminated with photons and alpha particleswere contaminated with photons and alpha particles
• Helium ions have biophysical properties like protonsHelium ions have biophysical properties like protons– Good dose localization (Bragg peak)Good dose localization (Bragg peak)– Must use spread out Bragg peak (SOBP)Must use spread out Bragg peak (SOBP)
• Carbon ions have the biological advantages of high LETCarbon ions have the biological advantages of high LET– Less OER and cell cycle dependency Less OER and cell cycle dependency – RBE increases strongly with LET and therefore depth doses are RBE increases strongly with LET and therefore depth doses are
hard to calculatehard to calculate• An additional advantage may be ability to use PET to image target An additional advantage may be ability to use PET to image target
volumevolume• Currently, only Japan and Germany heavy ion clinical facilitiesCurrently, only Japan and Germany heavy ion clinical facilities
– Over 5,000 patients now treated with heavy carbon ionsOver 5,000 patients now treated with heavy carbon ions– Very good efficacy reported, e.g., chondrosarcoma at the base of skull, spinal Very good efficacy reported, e.g., chondrosarcoma at the base of skull, spinal
tumors, adeno cystic ca, locally advanced HNSCC.tumors, adeno cystic ca, locally advanced HNSCC.

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
H2
High energy deuterons captured by beryllium target
n
Be9
NeutronsNeutrons
Stone, at LBL between 1938 and 1943, used Cyclotron neutrons to treat 240 patients using the wrong RBE with severe late sequelae.

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
Potential Biological Advantages of High Potential Biological Advantages of High LET RadiationsLET Radiations
• Reduced influence of hypoxiaReduced influence of hypoxia– OER 1.4-1.7OER 1.4-1.7
• Reduced influence of repairReduced influence of repair• Reduced cell cycle differentialReduced cell cycle differential• Higher RBE for slowly cycling tumorsHigher RBE for slowly cycling tumors
– RBE for most normal tissues 3.0-3.5RBE for most normal tissues 3.0-3.5– RBE for CNS 4.0-4.5RBE for CNS 4.0-4.5– RBE for salivary gland tumors = 8RBE for salivary gland tumors = 8
(Larimore, G. Adv Radiat Biol 15:153, 1992)(Larimore, G. Adv Radiat Biol 15:153, 1992)RBE varies with the energyRBE varies with the energy

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
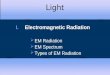
Poor Depth Dose Distribution of NeutronsPoor Depth Dose Distribution of Neutrons
(from Hall 2000)

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
Isoeffect Curves for NeutronsIsoeffect Curves for Neutrons
Withers et al. Int J Radiat Oncol Biol Phys. 8:2071-6, 1982

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
Clinical Trials with NeutronsClinical Trials with Neutrons
• Have been tested at a number of centers world-wideHave been tested at a number of centers world-wide• Disappointing resultsDisappointing results
– high incidence of late complications high incidence of late complications – relatively poor depth dose distribution; fixed relatively poor depth dose distribution; fixed
horizontal beamshorizontal beams– reoxygenation in conventional radiation may reoxygenation in conventional radiation may
reduce importance of hypoxic cellsreduce importance of hypoxic cells– poor patient selectionpoor patient selection– Currently only about 5 centersCurrently only about 5 centers
• Current uses primarily limited to salivary gland and Current uses primarily limited to salivary gland and prostate cancers, and (limited) soft tissue sarcomasprostate cancers, and (limited) soft tissue sarcomas

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
Boron Neutron Capture Therapy (BNCT)Boron Neutron Capture Therapy (BNCT)
LET ~ 200-300 keV/mm RBE highOER low

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
BNCTBNCT
• LimitationsLimitations– Lack of boron compounds with specificity Lack of boron compounds with specificity
for tumor rather than normal tissuefor tumor rather than normal tissue– Getting enough into tumorGetting enough into tumor– Thermal neutrons are poorly penetratingThermal neutrons are poorly penetrating
• Tumors tested clinicallyTumors tested clinically– Glioblastoma multiformeGlioblastoma multiforme– Cutaneous melanomaCutaneous melanoma
• Currently few sites conducting studiesCurrently few sites conducting studies

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
SRS and SRTSRS and SRT
• SRS - one fractionSRS - one fraction– First proposed by Leksell First proposed by Leksell
• Arch Chir Scand 102:316-319, 1951Arch Chir Scand 102:316-319, 1951
– SRS loses the advantage of dose fractionation SRS loses the advantage of dose fractionation and often ends up as SRTand often ends up as SRT
• SRT - fractionatedSRT - fractionated• There may be no advantage to dose fractionation There may be no advantage to dose fractionation
based on differences between tumor and normal based on differences between tumor and normal tissue in terms of tissue in terms of values, but this is based on values, but this is based on values around 2Gy. Other differences may exist values around 2Gy. Other differences may exist between large fraction size and single doses. between large fraction size and single doses.

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
IMRT etc.IMRT etc.• Since mid 1990s IMRT and related procedures have Since mid 1990s IMRT and related procedures have
been use to conform high dose areas to target been use to conform high dose areas to target volumes with sharp dose fall-off to organs at risk volumes with sharp dose fall-off to organs at risk (OARs), potentially reducing morbidity(OARs), potentially reducing morbidity
• This raises questionsThis raises questions– How do you best define GTV? CT, PET, MRI…How do you best define GTV? CT, PET, MRI…
• Geometric miss a problem as margins decrease?Geometric miss a problem as margins decrease?
– Higher volume receiving lower doseHigher volume receiving lower dose– Higher Higher ‘‘integralintegral’’ dose dose
• Increased risk of cancer inductionIncreased risk of cancer induction• Should IMRT be used for pediatric patients?Should IMRT be used for pediatric patients?
– Increased time for delivery may decrease efficacyIncreased time for delivery may decrease efficacy

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
2. Diagnostic Imaging2. Diagnostic Imaging
~ 10 Gy~ 10 Gy~100 Gy~100 Gy< 5 MeV< 5 MeVPhotons, electrons, alphas (Y-90, Bi-214, Photons, electrons, alphas (Y-90, Bi-214, etc)etc)
c. Radioimmuno-c. Radioimmuno-therapy (RIT)therapy (RIT)
~ 1 Gy~ 1 Gy~60 Gy~60 Gy< 2 MeV< 2 MeVGamma-ray photons, electrons, and Gamma-ray photons, electrons, and neutrons (neutrons (Ra-226, Cs-137, Ir-192, I-Ra-226, Cs-137, Ir-192, I-125, etc)125, etc)
b. Brachytherapy b. Brachytherapy
Low dose region:Low dose region:D< 5 Gy D< 5 Gy Intermediate dose regionIntermediate dose region5 Gy < D < 45 Gy 5 Gy < D < 45 Gy High dose regionHigh dose regionD > 45 GyD > 45 Gy
Up to 100 Gy Up to 100 Gy (or Gy x RBE)(or Gy x RBE)
6-250 MeV6-250 MeVX-ray photons, electrons, protons and X-ray photons, electrons, protons and neutronsneutrons
a. External Beam a. External Beam
1. Radiotherapy1. Radiotherapy
Approx. dose to tissue Approx. dose to tissue outside the treatment outside the treatment
volumevolume
Approx. dose to Approx. dose to primary primary targettarget
EnergyEnergyRadiation TypeRadiation Type
0.02 – 0.1 Sv per scan0.02 – 0.1 Sv per scanKV or MVKV or MVX-ray photonsX-ray photonse. Cone beam CT e. Cone beam CT IGTRIGTR
~ 0.02 Sv ~ 0.02 Sv 0.511 keV0.511 keVPhotons/positronsPhotons/positronsd. Hybrid PET/CTd. Hybrid PET/CT
~ 0.5 Sv~ 0.5 Sv<140 kVp<140 kVpX-rays photonsX-rays photonsc. Interventional c. Interventional FluoroscopyFluoroscopy
~ 0.05 – 0.1 Sv~ 0.05 – 0.1 Sv<140 kVp<140 kVpX-ray photonsX-ray photonsa.a.Multi-slice CT (4D)Multi-slice CT (4D)
~ 0.01 Sv~ 0.01 Sv<150 kVp<150 kVpX-ray photonsX-ray photonsa.a.Radiography Radiography
Xu et al. Phys. Med. Biol. 53 (2008) R193–R241

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
Non-Homogeneous Dose Non-Homogeneous Dose DistributionsDistributions
• Historically, in RT homogeneous dose Historically, in RT homogeneous dose distributions have been used. With IMRT, distributions have been used. With IMRT, more opportunities exist to use non-more opportunities exist to use non-homogeneous dose distributionshomogeneous dose distributions– Dose painting eg hypoxic regions, PET Dose painting eg hypoxic regions, PET
positive regions, etc.positive regions, etc.– Simultaneous boost techniqueSimultaneous boost technique

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
Simultaneous Integrated Boost (SIB) Technique Simultaneous Integrated Boost (SIB) Technique • Dose > 2 Gy/fraction to the tumor and < 2 Gy/fraction on Dose > 2 Gy/fraction to the tumor and < 2 Gy/fraction on
the normal tissuesthe normal tissues
• Small volume with dose/fraction > 2 GySmall volume with dose/fraction > 2 Gy
• Benefit of a reduced overall treatment timeBenefit of a reduced overall treatment time

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
SIB IMRT(49.9 Gy + 19.7 Gy)
Two-phase IMRT(50 Gy + 20 Gy)
Courtesy of Ph. Maingon

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
Final ThoughtsFinal Thoughts
• How much are we going to gain by pushing How much are we going to gain by pushing the limits of conformal types of therapy?the limits of conformal types of therapy?
• Will the gains ever be properly evaluated?Will the gains ever be properly evaluated?• What about the economics?What about the economics?• The greatest gain may come from being sure The greatest gain may come from being sure
we hit the tumor…….we hit the tumor…….• The radiobiology of low dose and high dose The radiobiology of low dose and high dose
delivery, and low dose rate and high dose delivery, and low dose rate and high dose rate, are very likely different rate, are very likely different

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
Questions:Questions: The Radiobiology of Alternate Physical Forms of Radiation DeliveryThe Radiobiology of Alternate Physical Forms of Radiation Delivery

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
139. Low dose rate implants deliver139. Low dose rate implants deliver– <0.01 Gy/hr<0.01 Gy/hr– 0.1-0.4 Gy/hr0.1-0.4 Gy/hr– 0.4-2.0Gy/hr0.4-2.0Gy/hr– 2.0-4.0 Gy/hr 2.0-4.0 Gy/hr
#3 – A generally accepted figure…

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
140. What is least likely to give a radiobiological 140. What is least likely to give a radiobiological advantage for low dose rate implantsadvantage for low dose rate implants– Increased reoxygenation during treatmentIncreased reoxygenation during treatment– Sparing of late effect tissuesSparing of late effect tissues– Sparing of acute effects tissuesSparing of acute effects tissues– Cell cycle redistributionCell cycle redistribution– Decreased dose heterogeneityDecreased dose heterogeneity
#5 – Dose heterogeneity is an advantage with implantsDose heterogeneity is an advantage with implants

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
141. The RBE of protons compared to standard 141. The RBE of protons compared to standard forms of RT isforms of RT is– 1.01.0– 1.1-1.21.1-1.2– 1.4-1.51.4-1.5– 2.0-2.52.0-2.5– 3.0-3.53.0-3.5
#2 – The advantage, if there is one, is in dose The advantage, if there is one, is in dose distributiondistribution

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
142. The RBE of fast neutrons compared to standard 142. The RBE of fast neutrons compared to standard forms of RT isforms of RT is– 1.01.0– 1.1-1.21.1-1.2– 1.4-1.51.4-1.5– 2.0-2.52.0-2.5– 3.0-3.53.0-3.5
#5 – However, for CNS it may be over 4.0 However, for CNS it may be over 4.0

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
143. Which is an advantages of fast neutrons143. Which is an advantages of fast neutrons• Increased influence of oxygenIncreased influence of oxygen• They are more potent if given as a fractionated They are more potent if given as a fractionated
coursecourse• They are more effective against rapidly cycling They are more effective against rapidly cycling
tumorstumors• They are particularly effective against salivary tumorsThey are particularly effective against salivary tumors
#4 – The data from Seattle (G. Larimore) suggests an The data from Seattle (G. Larimore) suggests an RBE of 8 for salivary gland tumorsRBE of 8 for salivary gland tumors

www.rwww.radbioladbiol.ucla.edu.ucla.edu
WMcB2008
144. The OER of fast neutrons for most normal 144. The OER of fast neutrons for most normal tissues istissues is– 1.01.0– 1.1-1.21.1-1.2– 1.4-1.71.4-1.7– 2.0-2.52.0-2.5– 3.0-3.53.0-3.5
#3 – This may be due in part to beam contaminationThis may be due in part to beam contamination