Embed Size (px)
Citation preview

The role of Recombinant human activated protein C in the treatment of sepsis in the I.C.U
Essay Submitted for fulfillment of master degree
in I.C.U
ByRanda Reda Ahmed Abd El Hafez
(MB,B.CH)
Supervised byProf.Dr.Hamdy Hassan Eliwa
Professor of Anesthesia and Intensive care Faculty of Medicine
Benha University
Dr.Ahmed Hamdy Abd El RahmanLecturer of Anesthesia and Intensive care
Faculty of MedicineBenha University
Faculty of MedicineBenha University
2015
1

2

Acknowledgement First of all, thanks to God who granted me the ability to
finish this work.
Words can never express my deepest gratitude and sincere
appreciation to Prof. Dr HamdyEliwaProfessor of Anesthesia and
Intensive care, Benha University for her continuous
encouragement , powerful support , extreme patient and faithful
advice
My deepest thanks and appreciation and sincere gratitude to
Dr. Ahmed Hamdy Lecturer of Anesthesia and Intensive care
Dept., Benha University , who spared no time and effort to provide
me with there valuable instructions and expert touches .
My truthful love to my family who were and will always be by
my side, all my life.
Randa Reda
3

List of AbbreviationsACTH : AdrenoCorticotrophic Hormone
ADP : Adenosine Diphosphate
ALI : Acute Lung Injury
ALB : Albumin
APACHE II : Acute Physiology and Chronic Health evaluation
APTT : Activated Partial thromboplastine time
ARDS : Acute respiratory distress syndrome
ATP : Adenosine Triphosphate
C1 : Complement fragment 1
CAP : Community Acquired Pneumonia
CLP : Ceacal Ligation&Puncture
CNS : Central Nervous System
CRH : Corticotropine Releasing Hormone
CRP : C Reactive Protein
CT : Computed Tomography
CVC : Central Venous Catheter
CVP : Central Venous Pressure
CVS : Cerebrovascular stroke
DC : Dentretic cells
DIC : Dissemenated Intravascular Coagulopathy
DM : Diabetes Mellites
Dob : Dobutrex
DOP : Dopamine
4

DVT : Deep Venous Thrombosis
E Coli : Escherichia Coli
EPI : Epinephrine
FDP : Fibrin Degradation Products
FFP : Fresh Frozen Plasma
G.CSF : Granulocyte Colony Stimulating Factors
GNBs : Gram Negative Bacilli
HAP : Hospital Aquired Pneumonia
Hb : Hemoglobin
HIV : Human Immunodeffiecincy Virus
HTN : Hypertension
ICU : Intensive Care Unite
IL2 : Interlukine 2
IL6 : Interlukine 6
LPS : Lipopolysaccharid
LOS : Length Of Stay
MAP : Mean Arterial Pressure
MDF : Myocardial Depressent Factor
MHC : Major Histocompitability Complex
MODS : Multi Organ Dysfunction Syndrome
MRSA : Methicillin Resistant Staph Aureus
MSSA : Methicillin Sensitive Staph Aureus
rAPC : Tecombant Activated protien C
NO : Nitric Oxide
NP : Nosocomial pneumonia
5

PAC : Pulmonary Artery Catheter
PAI : Plasminogen Activator Inhibitor
PAOP : Pulmonary Artery Occlusive Pressure
PCT : Procalcitonine
PE : Pulmonary Embolism
PEEP : Positive End Expiratory Pressure
PIRO : Predisposition,Infection,Response,Organ dysfunction
PMF : Polymorphneuclear leucocyte
ScVO2 : Central Venous Oxyhemoglobin saturation
SIRS : Systemic Inflammatory Response Syndrome
SLE : Systemic lupus Erythromatosis
SMX : Sulfamethoxazole
SNP : Single neucleotide polymorphism
SOFA : Sequential Organ Failure Assessment
TH2 : Type 2 Helper t cells
TLC : Total Leucocytic Count
TLR : Toll like Receptors
TLR4 : Toll like Receptors 4 gene
TMP : Trimethoprime
TNF : Tumor Necrosis Factor
t-PA : Tissue Plasminogen Activator
TSS : Toxic Shock Syndrome
VAP : Ventilator Assosciated Pneumonia
VRE : Vancomycine rResistant Enterococcus
VSE : Vancomycine Sensitive Enterococcus
6

List of Tables
Table No.TitlePag
eTable (1): Inflammatory mediators in sepsis7Table (2): SOFA score32Table (3): Vasopressor in sepsis55
7

List of FiguresFigure
No.TitlePage
Figure (1):Potential outcomes of mediator release in sepsis up to
date 20088
Figure (2):Complement activation in sepsis11
Figure (3):
The Response to Pathogens, Involving “Cross-Talk”
among Many Immune Cells, Including Macrophages,
Dendritic Cells, and CD4 T Cells.21
Figure (4):PIRO33Figure (5):Protocol for early gold directed therapy48Figure (6):
Action of Activated protein C 70
8

Introduction
IntroductionSepsis is defined as acomplex activation of immune system with a
documented infection, systemic inflammatory response syndrome (SIRS)
as acomplex activation of immune system regardless of
eatiology ,infection ,trauma ,burns ,or asterile inflammatory
process ,Sever sepsis is as sepsis plus organ dysfunction and Septic shock
is as sepsis plus unexplained acute circulatory collapse with organ
dysfunction, hypotention,and tissue hypoperfusion. (Browser 2008)
Sepsis has been referred to as aprocess of malignant intravascular
inflammation .It is considered malignant because it is
uncontrolled ,unregulated,and self sustaining .It is considered
intravascular because it represents the blood –borne spread of what is
usually acell-to-cell interaction in the interstitial space .It is considered
inflammatory because all characteristics of the septic response are
exaggerations of the normal inflammatory response.(Mesiner 2002)
When tissue is injured or infected, there is simultaneous release of
pro-inflammatory and anti- inflammatory elements .The balance of these
contrasting signals helps to facilitate tissue repair and
healing .However ,remote tissue injury may ensue when this equilibrium
in the inflammatory process is lost ,and these mediators exert systemic
effects .The significant consequences of a systemic pro-inflammatory
reaction include endothelial damage ,microvascular dysfunction ,and
impaired tissue oxygenation and organ injury .The significant
consequences of an excessive anti- inflammatory process include
immunosuppression .In addition,pro-and anti-inflammatory process may
interfere with each other,creating astate of destructive immunologic
process. (Mesiner 2001)
1

Introduction
The occurrence of sepsis in the united states from 1979 to 2000
using representive samples showed that the incidence and the number of
sepsis related deaths increased ,despite a decline in the overall in hospital
mortality among sepsis patients.(Hebert 2008)
Sepsis is associated with increased hospital and ICU
stays ,expensive antimicrobial therapies ,and prolonged duration of
mechanical ventilation .As such, the economic impact of sepsis is
considerable.
(Angus 2004)
Sepsis is clearly associated with high morbidity and mortality.
Importantly,the prognosis of septic patients is influenced not only by the
severity of infection ,but also by the previous health status and the host
response and diagnosis of sepsis affects not only immediate mortality, but
has an effect on longer-term death rates as well.(Mesiner 2000)
Studies in the past year have documented sepsis rate in cancer
patients to be 10 times higher than non cancer patients ,making cancer
potentially the greatest contributor to the risk for sepsis among co-
morbid conditions greater even than HIV and diabetes.(Luce 2008)
The lungs are the most commen source of infection .The most
commonly isolated organisms in nosocomial infections ,an important
cause of sepsis in ICU patients ,are staphylococcus
aureus,klebesilla ,pseudomonas aregenosa,Ecoli.Over recent years , there
has been a change in the eatiology of septic shock with chest related
infection becoming more important than abdominal infection ,possibly
related to increased and often prolonged use of mechanical ventilation.
(Martin 2004)
2

Introduction
In the last half of the 20th century, the use of antibiotics for the
treatment of bacterial infections transformed the practice of medicine,
resulting in sharp reductions in morbidity and mortality from acute and
chronic infections. However, mortality has remained high when an acute
bacterial infection induces sepsis with shock, metabolic acidosis, oliguria,
or hypoxemia. In fact, in the United States alone, there are at least
500,000 episodes of sepsis annually, and the resultant mortality rate
ranges from 30 to 50 percent, even with intensive medical care, including
antibiotics, intravenous fluids, nutrition, mechanical ventilation for
respiratory failure, and surgery when indicated to eradicate the source of
the infection. (Rangel Frausto ,et al 2003)
In the past 15 years several treatments designed to reduce the
mortality rate associated with sepsis have been unsuccessful, leading
some investigators to conclude that any adjunctive therapy is destined to
fail because once the clinical signs of severe sepsis are present,
irreversible organ injury has already occurred. At last, however, there has
been progress in finding an effective new therapy for sepsis. It is reported
the results of a large clinical trial in which recombinant human activated
protein C significantly reduced mortality in patients with severe sepsis.
(Bernard ,et aL 2000)
Activated protein C, a component of the natural anticoagulant
system, is a potent antithrombotic serine protease with substantial
antiinflammatory properties. What has the efficacy of this treatment
taught us about the pathogenesis of sepsis, and what are the strengths and
limitations of this important clinical trial.(Gandrel ,et al 2001)
3

Aim of the Work
AIM OF THE WORKThe aim of this work is to determine the effect of intravenous
activated protein C therapy in the treatment of patients with severe sepsis
and septic shock in the ICU.
4

Chapter I
Chapter I
The pathophysiology of sepsis
Sepsis has been referred to as a process of malignant intravascular
inflammation .It is considered malignant because it is uncontrolled,
unregulated, and self-sustaining. It is considered intravascular because it
represents the blood-borne spread of what is usually a cell-to-cell
interaction in the interstitial space. It is considered inflammatory because
all characteristics of the septic response are exaggerations of the normal
inflammatory response.(pinsky, et al 2008)
When tissue is injured or infected, there is simultaneous release of
pro-inflammatory and anti-inflammatory elements. The balance of these
contrasting signals helps to facilitate tissue repair and healing. However,
remote tissue injury may ensue when this equilibrium in the
inflammatory process is lost, and these mediators exert systemic effects .
(Bone 2008)
The significant consequences of a systemic pro-inflammatory
reaction include endothelial damage, microvascular dysfunction, and
impaired tissue oxygenation and organ injury. The significant
consequences of an excessive anti-inflammatory response include
immunosuppression. In addition, pro- and anti-inflammatory processes
may interfere with each other, creating a state of destructive immunologic
dissonance. (Bone 2008)
Normal inflammation:
5

Chapter I
Inflammation is intended to be a local and contained response to
infection. While initiating insults may be numerous, the inflammatory
processes are qualitatively similar. At the site of injury, the endothelium
expresses adherence molecules to attract leukocytes. At the same time,
polymorphonuclear leukocytes (PMNs) are activated and express
adhesion molecules that cause their aggregation and margination to the
vascular endothelium. A prerequisite for subsequent phagocytosis of
invading bacteria and debris from injured tissue is diapedesis and then
migration of these PMNs to the site of injury. (Movat ,et al 2008).
The release of mediators by PMNs at the site of injury or
infection is responsible for the cardinal signs of local inflammation e.g
Local vasodilation and hyperemia ,Increased microvascular permeability,
resulting in protein-rich edema. (Monatt ,et al 2005)
The primitive, but effective, local inflammatory processes
(adherence, chemotaxis, phagocytosis, bacterial killing) are highly
regulated at various levels, mainly through the production of cytokines by
macrophages. Once a macrophage has been triggered and activated
during the invasion of tissue by bacteria, it secretes cytokines (eg, tumor
necrosis factor, interleukins) and other mediators into the cell's
microenvironment .(Michard ,et al 2008).
Tumor necrosis factor (TNF) release becomes self-stimulating (an
autocrine process), and cytokine levels are further increased by the
release of other inflammatory mediators, including table (3). This leads to
continued activation of PMNs, macrophages and lymphocytes. In
addition, the proinflammatory mediators recruit more PMNs and
macrophages (a paracrine process). The net effect is clearing of bacteria
and debris, which is followed by tissue repair (Fekety , et al 2008).
6

Chapter I
Table (1): Inflammatory mediators in sepsis
Mediator Source Main Effect
Histamine Mast cells, basophils, platelets
Vasodilatation, increased vascular permeability
Serotonin Platelets Increased vascular permeability, platelet aggregation
Prostaglandins All leucocytes, platelets, endothelial cells
Most cause vasodilatation Thromboxane – vasoconstriction
Leukotrienes All leucocytes Vasoconstriction, bronchospasm, increased vascular permeability
Platelet activating factor (PAF)
All leucocytes, platelets, endothelial cells
Platelet aggregation and degranulation, vasodilatation, increased vascular permeability, leukocyte adherence
Nitric oxide (NO) Endothelial cells, macrophages, platelets
Vasodilatation
Cytokines (interleukin eg IL1, Tumour necrosis factor TNF)
Macrophages, lymphocytes
Vasodilatation, fever, lethargy, attracts leucocytes
Kinin system(Bradykinin)
Circulates in plasma inactive
Increased vascular permeability, vasodilatation
Complement System Cascade of inactive plasma proteins
Leukocyte activation, phagocytosisC3a and C5a cause increased vascular permeability and vasodilatation
In some cases, mediator release exceeds the boundaries of the local
environment. This may lead to a more generalized response that affects
otherwise normal tissue fig 1). This process is referred to as sepsis when
it occurs in association with infection, and as SIRS when it is induced by
noninfectious conditions, such as pancreatitis, severe trauma, and
aspiration.
7

Chapter I
Figure (1): Potential outcomes of mediator release in sepsis up to date
2008.(poeze ,et al 2008)
Inflammation in sepsis: Normal inflammation involves the regulation of PMN rolling,
adhesion, diapedesis, chemotaxis, phagocytosis, and killing of invading
bacteria. These processes are highly controlled, with regulation through
pro- and anti-inflammatory cytokines released by activated macrophages.
When sepsis occurs, these actions may lead to remote tissue injury
(Van Der Poll 2008)
Proinflammatory cytokines:The important proinflammatory cytokines include TNF-alpha
(TFNα) and IL-1, which share a remarkable array of biological effects .
Evidence supporting a role for TNFα in sepsis includes circulating TNFα
levels are elevated in septic patients. This may be due in part to the
8

Chapter I
binding of endotoxin to lipopolysaccharide (LPS)-binding protein and its
subsequent transfer to CD14 on macrophages, which stimulates the
release of TNFα.TNFα infusion produces symptoms similar to those
observed in septic shock. Anti-TNFα antibodies protect animals from
lethal challenge with endotoxin. (Lamping ,et al 2008)
Several cytokines, referred to as antiinflammatory cytokines, inhibit
the production of TNFα and IL-1; however, their effects are not
universally antiinflammatory. Examples include IL- 10 and IL-6, both of
which have the following actions .They stimulate the immune system by
enhancing B cell function (proliferation, immunoglobulin secretion) and
encouraging the development of cytotoxic T cells. They suppress the
immune system by inhibiting cytokine production by mononuclear cells
and monocyte-dependent T helper cells. (Szabo ,et al 2008)
Bacterial factors:Direct effects of invading microorganisms or their toxic products
may also contribute to the pathogenesis of sepsis. Among the potentially
offending factors are endotoxin, cell wall components of bacteria
(peptidoglycan, muramyl dipeptide, and lipoteichoic acid), and bacterial
products such as staphylococcal enterotoxin B, toxic shock syndrome
toxin-1, Pseudomonas exotoxin A, and M protein of hemolytic group A
streptococci .(Pugin 2008).
There is substantial evidence to suggest that endotoxin is an
important exogenous mediator of sepsis in gram negative bacterial
infections. Endotoxin, a lipopolysaccharide found in the cell wall of gram
negative bacteria, tends to reproduce many of the features of sepsis when
infused in humans. The coagulation, complement, and contact and
fibrinolytic systems are all activated by endotoxin, This may lead to the
9

Chapter I
production of vasoactive products (such as bradykinin) and to
complement activation, both of which can enhance endothelial
permeability. Complement activation and disruption of the normal
coagulation/lysis equilibrium can also lead to microvascular thrombosis.
(Liu,et al 2008)
Endotoxemia is detectable in septic patients. Furthermore, elevated
plasma levels of endotoxin are associated with shock and multiple organ
dysfunction. (Tapper , et al 2008).
Complement activation:The complement system is a protein cascade that helps clear
pathogens from an organism .The best evidence that complement
activation plays an important role in the pathogenesis of sepsis is that
inhibition of the complement cascade decreases inflammation and
improves mortality in animals.(Walport 2001).
In a rodent model of sepsis, complement fragment 5a receptor
(C5aR) antagonist decreases mortality, inflammation, and vascular
permeability The intervention is based on data that indicate that increased
production of complement fragment 5a (C5a) and increased expression
of C5aR alters neutrophil trafficking during sepsis. (Huber Lang ,et al
2002)
In several animal models of sepsis LPS injection in mice and rats,
Escherichia coli infusion in dogs and baboons, cecal ligation and
puncture in mice complement fragment 1 (C1) inhibitor decreases
mortality, inflammation, and vascular permeability, compared to
untreated controls. (Liu , et al 2008).
10

Chapter I
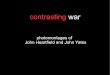
Diffuse complement activation (left) and complement in the lung
(right) figure 2
Figure (2): Complement activation in sepsis
In diffuse complement activation (sepsis), diffuse intravascular
complement C5a "paralyzes" polymorphonuclear neutrophils, making
them unable to respond to C5a or other chemoattractants. Furthermore,
aggregation of leukocytes in the microvasculature occurs secondary to the
up-regulation of adhesion molecules by C5a. During local compliment
activation (pneumonia), localized generation of C5a establishes a gradient
for chemotaxis of leukocytes. Higher local concentrations of C5a arrest
chemotaxis and cause the cells to produce toxic oxygen radicals and to
11

Chapter I
release granule-bound enzymes and mediators relevant to innate
immunity. The function of the C5a receptor on parenchymal cells is
unclear. LTB4 denotes leukotriene B4.(Freudenberg ,et al 2001)
Effects on coagulation: Activation of coagulation:
The coagulation cascade is activated by damage to the capillary
endothelium (the inner lining of the capillary), caused by pathogens and a
number of inflammatory mediators. The coagulation cascade involves
many circulating factors in a cascade mechanism, where one factor
activates the next in turn, resulting in the creation of a fibrin plug. In
health, a delicate balance exists between coagulation and fibrinolysis (the
breakdown of fibrin clots) to ensure that clotting occurs only where it is
needed. In severe sepsis, this balance becomes disordered.(Carvalho ,et
al 1998).
In sepsis multiple cytokines, including interleukins 1 and 6 (IL1,
IL6) and tumour necrosis factor alpha (TNF-α) induce the expression of
tissue factor (TF) on endothelial cells and monocytes, initiating
coagulation. Microthrombi form and build up in the capillaries. These
microthrombi eventually obstruct the capillaries, compromising blood
supply and leading to tissue necrosis. When these capillaries are involved
in the supply of end organs, multi-organ failure may occur.(Esmon
1998).
Inhibitors of coagulation and suppression of fibrinolysis:
Fibrinolysis is the breakdown of fibrin by plasmin. Plasmin is
formed when tissue plasminogen activating factor (t-PA) triggers the
conversion of plasminogen to plasmin. Excessive fibrinolysis is normally
12

Chapter I
inhibited by plasminogen activator inhibitor (PAI -1) and thrombin
activatable fibrinolysis inhibitor (TAF1).(Esmon 1998).
In sepsis there is increased PAI-1, decreased t-PA and decreased
plasminogen, causing a decrease in fibrinolysis. There are also natural
inhibitors of coagulation including protein C and S, antithrombin, and
tissue factor pathway inhibitors, which under normal conditions prevent
coagulation from becoming generalised. Anti-thrombin forms complexes
with thrombin, factors Xa, XIIa, XIa and IXa inactivating them before
being removed by the liver. Activated protein C inactivates cofactors Va
and VIIIa impeding the clotting process, as well as enhancing fibrinolysis
by neutralizing PAI-1 and by accelerating clot breakdown. Activated
protein C also has a direct anti-inflammatory effect, decreasing cytokine
production and inhibiting leukocyte attachment to endothelium. This is
the basis of the use of recombinant activated protein C in severe sepsis.
(Carvalho ,et al 1994)
Disseminated intravascular Coagulation (DIC):
As explained above, sepsis triggers the coagulation cascade. This
widespread clotting causes consumption of platelets, clotting factors and
fibrinogen, causing impaired coagulation and therefore increases risk of
bleeding. Clotting tests such as APTT and INR, are therefore raised and
fibrinogen levels are decreased. After the increased coagulation and fibrin
formation there is secondary fibrinolysis resulting in increased fibrin
degradation products (FDPs) including D-Dimer, which can be measured.
(Steinman ,et al 2002)
DIC can cause bleeding, large vessel thrombosis, haemorrhagic
tissue necrosis and microthrombi leading to organ failure. The patients
will bruise easily and bleed from various sites: cannula sites, surgical
13

Chapter I
wounds, gastro-intestinal tract, lungs and urinary tract.(Carvalho ,et al
1994).
The treatment for DIC is to treat the underlying sepsis, prevent
bleeding (eg. H2 receptor antagonists to reduce risk of gastro-intestinal
tract bleed) and replace clotting factors using fresh frozen plasma (FFP)
and cryoprecipitate (factor VIII and fibrinogen) and replace platelets as
needed. Prophylactic heparin is also needed as the increased coagulation
increase the septic patient’s risk of deep vein thrombosis (DVT) and
pulmonary embolism (PE). (Schuler , et al 2002).
Cellular injury: The precise mechanisms of cell injury and resulting organ
dysfunction in sepsis are not fully understood. Autopsy studies show that
multiple organ dysfunction syndrome, the common precursor of death in
sepsis, is associated with widespread endothelial and parenchymal cell
injury. Mechanisms proposed to explain these findings
include ,Ischemia (oxygen lack relative to oxygen need), Cytopathic
injury (direct cell injury by proinflammatory mediators and/or other
products of inflammation) ,An increased rate of apoptosis (programmed
cell death).
(Brealey ,et al 2008)
Hypoxic hypoxia: The septic microcirculatory lesion disrupts tissue oxygenation,
suggesting that disturbances in the metabolic regulation of tissue oxygen
delivery contribute to the pathogenesis of organ dysfunction. As noted
above, both microvascular and endothelial abnormalities contribute to the
septic microcirculatory defect in sepsis. (Piagnerelli ,et al 2003).
14

Chapter I
An interaction between endothelial cells and PMNs is directly
involved in this uncontrolled inflammatory state in sepsis. The increase in
receptor-mediated neutrophil-endothelial cell adherence results in the
secretion of reactive oxygen species, lytic enzymes, and vasoactive
substances (nitric oxide, endothelin, platelet-derived growth factor, and
platelet activating factor) into the extracellular milieu. The ensuing
microcirculatory injury leads to impaired cellular oxygen diffusion, due
to a reduction in the cross-sectional area available for tissue oxygen
exchange (Cruz ,et al 2003).
Another contributing factor in sepsis is that erythrocytes lose their
normal ability to deform within the systemic microcirculation "Rigid"
erythrocytes find it difficult to navigate the septic microcirculation.
These combined microcirculatory events, including reduction of surface
area available for gas exchange, cause excessive heterogeneity in
microcirculatory blood flow and depressed tissue oxygen flux.
(Piagnerelli ,et al 2003)
Direct cytotoxicity: Cell culture experiments have shown that the cytotoxicity of
endotoxin, TNFα, and nitric oxide involves direct damage to
mitochondrial electron transport. This functional change is accompanied
by degeneration of the mitochondrial ultrastructure, which precedes
measurable changes in other cellular organelles by several hours.
(Crouser ,et al 2008)
The net effect is that disordered energy metabolism in sepsis may
be partly due to structural disruption of electron transport as a result of
destruction or dysfunction of both inner membrane and matrix proteins.
(Roselle ,et al 2008)
15

Chapter I
The clinical relevance of mitochondrial dysfunction in septic shock
was suggested in a clinicopathologic study of 28 critically ill septic
patients who underwent skeletal muscle biopsy within 24 hours of
admission to the ICU. (Brealey ,et al 2008).
Skeletal muscle ATP concentrations, a marker of mitochondrial
oxidative phosphorylation, were significantly lower in the 12 patients
who died of sepsis than in 16 survivors. In addition, there was an
association between nitric oxide overproduction, antioxidant depletion,
and severity of clinical outcome. Thus, cell injury and death in sepsis may
be explained by cytopathic (or histotoxic) anoxia, an inability to utilize
oxygen even when present .(Settia ,et al 2008 ).
Apoptosis:Apoptosis (programmed cell death) describes a set of regulated
physiologic and morphologic changes leading to cellular death. This is
the principal mechanism by which senescent or dysfunctional cells are
normally eliminated. In addition, cell death via apoptosis is the dominant
process leading to the termination of inflammation once infection has
subsided. However, proinflammatory cytokines may delay apoptosis in
activated macrophages and neutrophils. This effect may prolong or
augment the inflammatory response, thereby contributing to the
development of multiple organ failure. (Marshall ,et al 2008).
Derangements of apoptotic cell death are also believed to play a
critical role in the tissue injury of sepsis . Apoptosis is normally a
physiologic mechanism to selectively limit cell populations with rapid
proliferation (eg, gut epithelium). When exposed to various inflammatory
mediators, such as endotoxin, cytokines, and reactive oxygen species,
16

Chapter I
parenchymal and endothelial cells respond by the induction of one of two
programs of stress gene expression. When subsequently exposed to
endotoxin, these cells undergo accelerated apoptosis. Gut epithelial
apoptosis was an important factor in an animal model of Pseudomonas
sepsis. (Coopersmith ,et al 2002).
Proinflammatory and antiinflammatory balance:The interaction between proinflammatory and antiinflammatory
mediators can be viewed as a struggle between opposing influences.
Different scenarios can result from the combined effects of the sepsis
syndrome and the host's compensatory antiinflammatory response to it.
(Bone 2008).
If the mediators balance each other and the initial infectious insult
is overcome, homeostasis will be restored. The initial insult may be so
severe that it is sufficient to directly induce SIRS and multiple organ
dysfunction. In most patients who survive the initial insult, a balance
between proinflammatory and antiinflammatory processes is not
established, and a massive systemic inflammatory response or an
antiinflammatory reaction may ensue. A wide range of clinical sequelae
may occur in which either SIRS or an antiinflammatory reaction
("immune paralysis" or a "window of immunodeficiency") predominates,
or both may be present. (Brownlee,et al 2008 )
Sepsis is unique in its ability to evolve from other inflammatory
illnesses, such as SIRS. As an example, thermal injury to rats induces
priming of alveolar macrophages; this may lead to a significant increase
in macrophage TNF production, which may then exacerbate the response
to subsequent exposure to endotoxin. In addition, the systemic effects of
the excess cytokine load may induce tissue injury. (Bone 2008).
17

Chapter I
FAILURE OF IMMUNE SYSTEM:Patients with sepsis have features consistent with immuno-
suppression, including a loss of delayed hypersensitivity, an inability to
clear infection, and a predisposition to nosocomial infections . One reason
for the failure of antiinflammatory strategies in patients with sepsis may
be a change in the syndrome over time. Initially, sepsis may be
characterized by increases in inflammatory mediators; but as sepsis
persists, there is a shift toward an antiinflammatory immunosuppressive
state .(Lederer ,et al 1999).
There is evidence of immunosuppression in sepsis from studies
showing that lipopolysaccharide-stimulated whole blood from patients
with sepsis releases markedly smaller quantities of the inflammatory
cytokinesTNF and interleukin-1 b than does that of control patients.
(James, et al 2007)
The adverse sequelae of sepsis induced immunosuppression were
reversed with the administration of interferong in patients with sepsis.
This immune stimulant restored macrophage TNFα production and
improved survival .(Opal ,et al 2000).
MECHANISMS OF IMMUNE SUPPRESSION IN SEPSIS:
A shift to antiinflammatory cytokines:
Activated CD4 T cells are programmed to secrete cytokines with
either of two distinct and antagonistic profiles (173). They secrete
eithercytokines with inflammatory (type 1 helper T-cell [Th1]) properties,
including TNFα, interferon, and interleukin- 2, or cytokines with
18

Chapter I
antiinflammatory (type 2 helper T-cell [Th2]) properties for example,
interleukin- 4 and interleukin-10 .(Lederer ,et al 1999).
The factors that determine whether CD4 T cells have Th1 or Th2
responses are unknown but may be influenced by the type of pathogen,
the size of the bacterial inoculum, and the site of infection. Mononuclear
cells from patients with burns or trauma have reduced levels of Th1
cytokines but increased levels of the Th2 cytokines interleukin-4 and
interleukin-10, and reversal of the Th2 response improves survival among
patients with sepsis . Other studies have demonstrated that the level of
interleukin-10 is increased in patients with sepsis and that this level
predicts mortality rate.(Gogos,et al 2000)
Anergy: Anergy is a state of nonresponsiveness to antigen. T cells are
anergic when they fail to proliferate or secrete cytokines in response to
their specific antigens. Heidecke et al. examined T-cell function in
patients with peritonitis and found that they had decreased Th1 function
without increased Th2 cytokine production, which is consistent with
anergy (Pellergini ,et al 2000).
Defective T-cell proliferation and cytokine secretion correlated
with mortality. Patients with trauma or burns have reduced levels of
circulating T cells, and their surviving T cells are anergic. (Haslett , et al
2001).
19

Chapter I
Apoptotic cell death may trigger sepsis-induced anergy. Although
the conventional belief was that cells die by necrosis, recent work has
shown that cells can die by apoptosis genetically programmed cell death.
In apoptosis, cells “commit suicide” by the activation of proteases that
disassemble the cell. (Hotchkiss ,et al 2001).
Large numbers of lymphocytes and gastrointestinal epithelial cells
die by apoptosis during sepsis.(Fukuzuka ,et al 2000).
A potential mechanism of lymphocyte apoptosis may be stress-
induced endogenous release of glucocorticoids (Green DR ,et al 2000).
The type of cell death determines the immunologic function of surviving
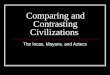
immune cells (Fig. 3) .(Fodok ,et al 2000).
Apoptotic cells induce anergy or antiinflammatory cytokines that
impair the response to pathogens, whereas necrotic cells cause immune
stimulation and enhance antimicrobial defenses (Fig. 3).(Osterman,et al
2002)
20

neutrophil
bacteria
Dentritic cellmacrophage+/-
+/- +/- Necrotic cell
Apoptotic cellApoptotic cellNecrotic cell
Inflammatory product
CD4T cell
+
anergy
(TH2) Antiinflammatory cytokines
(TH1) inflammatory cytokines
(Th1) inflammatory cytokinescytokines
(Th2) Antiinflammatory cytokines
anergy
Chapter I
Figure (3): The Response to Pathogens, Involving “Cross-Talk” among
Many Immune Cells, Including Macrophages, Dendritic Cells, and CD4
T Cells.(Dombroveskiy 2005)
Macrophages and dendritic cells are activated by the ingestion of
bacteria and by stimulation through cytokines secreted by CD4 T cells.
Alternatively, CD4 T cells that have an antiinflammatory profile (type 2
helper T cells [Th2]) secrete interleukin-10, which suppresses
macrophage activation. CD4 T cells become activated by stimulation
through macrophages or dendritic cells. For example, macrophages and
dendritic cells secrete interleukin-12, which activates CD4 T cells to
secrete inflammatory (type 1 helper T-cell [Th1]) cytokines. Depending
21

Chapter I
on numerous factors (e.g., the type of organism and the site of infection),
macrophages and dendritic cells will respond by inducing either
inflammatory or antiinflammatory cytokines or causing a global reduction
in cytokine production (anergy). Macrophages or dendritic cells that have
previously ingested necrotic cells will induce an inflammatory cytokine
profile (Th1). Ingestion of apoptotic cells can induce either an
antiinflammatory cytokine profile or anergy. A plus sign indicates up-
regulation, and a minus sign indicates down-regulation; in cases where
both a plus sign and a minus sign appear, either up-regulation or down-
regulation may occur, depending on a variety of factors.(Weinstien 2005)
22

Chapter II
Chapter IIThe Microbiology of Sepsis
Bacterial infections are the commonest aetiological agents of both
community-acquired and hospital related sepsis, but a causative organism
is confirmed in only 60% cases. Disease progression is similar regardless
of organism. However, there has been a rise in multiply resistant bacteria
such as Acinobacter species, Enterococci and methicillin-resistant
Staphylococcus aureus (MRSA). (Martin , et al 2003).
The microbiology and primary sources of infection have undergone
a remarkable transition over the past 30 years. The predominant pathogen
responsible for sepsis in the 1960s and 1970s were Gram-negative bacilli;
however, over the past few decades there has been a progressive increase
in the incidence of sepsis caused by Gram-positive and opportunistic
fungal pathogens. (Annane ,et al 2005).
Data from the large sepsis trials published during the past decade
indicate that Gram-positive and Gram-negative pathogens are responsible
for about 25% of infections each, with a further 15% due to mixed Gram-
positive, Gram-negative organisms, with fungal pathogens accounting for
between 5% to 10% of cases. This evolution in the spectrum of pathogens
has been associated with an increase in the incidence of multiresistant
organisms. Although the abdomen was the major source of infection in
sepsis from 1970 to 1990, in the past decade pulmonary infections have
emerged as the most frequent site of infection. (Martin ,et al 2003 ).
23

Chapter II
Patients admitted with symptoms prior to hospitalization are
considered to have community-acquired infections, and those who
develop infection more than 48 hours following admission are considered
to have hospital-acquired, or nosocomial, infection. (Dellinger ,et al
2008).
The most common organisms identified in community acquired
Infection requiring intensive care hospitalization are S. pneumoniae,
Legionella, and Haemophilus influenzae, with S. aureus, Early-onset
nosocomial Infection (<4–7 days) in patients who have not received prior
antibiotic therapy is typically caused by Enterobacteriaceae, Haemophilus
species, S. aureus, and pneumococci E coli. Patients who develop late-
onset Infection (>4–7 days) and who have received prior antibiotic
therapy are at risk for infection with P. aeruginosa, A. baumanii,
Stenotropomonas maltophilia, and MRSA, Enterobacteriaceae, including
Citrobacter, Klebsiella, Enterobacter, Serratia, Proteus, Morganella, and
Providencia spp. Approximately 20–40% of nosocomial Infection are
polymicrobial in etiology. (Kinai ,et al 2008 ).
Infection has been and remains a leading cause of death in patients
with leukemia and lymphoma and a major cause of morbidity and
mortality in patients with solid tumors or transplants. Rapid progression
of fungal, bacterial, and mycobacterial infections occurs in patients given
monoclonal antibodies to treat Crohn's disease and autoimmune diseases
such as rheumatoid arthritis. (Keane 2005)
The epidemic of human immunodeficiency virus (HIV)-1 infection
has added to the numbers of immunocompromised hosts. Traditionally,
infection has accounted for up to 75% of deaths in patients with acute
leukemia or Hodgkin's disease or in transplant recipients, but with
24

Chapter II
advances in prophylaxis and management, deaths due to infections have
decreased to about 50%. Once patients require intensive care unit (ICU)
care the mortality increases. (Yoo ,et al 2005 ).
Although a great variety of microorganisms have been noted to
cause severe, life-threatening infections in immunocompromised hosts,
the clinician can formulate a diagnostic plan and decide on empiric
therapy by giving careful consideration to the nature, duration, and
severity of the immunosuppression that is causing the patient's
predisposition to infection. Additionally, immunocompromised patients
and Elderly patients, uremic patients, and patients with end-stage liver
disease or those receiving corticosteroids often will fail to mount a
significant febrile response even to serious infection. (Theiry ,et al
2005).
Impaired splenic function:Overwhelming pneumococcal sepsis occurs in patients with
asplenia or diminished splenic function. Such patients usually present
with overwhelming pneumococcal sepsis rather than pneumococcal
pneumonia even if the initial site of infection is the lungs or upper
respiratory tract. Patients who have overwhelming pneumococcal sepsis,
unlike those who have other pneumonias, present with a diffuse petechial
or ecchymotic rash and shock. (Cunha 2006).
Sepsis sources: Central venous catheters:
For CVC sepsisinfection mainly caused by Staphylococcus aureus.
If methicillin-sensitive S aureus (MSSA) strains predominate in an
institution, anti–methicillin-resistant S aureus (anti-MRSA) is not
necessary after catheter removal . (Gill ,et al 1998).
25

Chapter II
CVC breaches the normal skin barrier to infection and bacteria
may be directly introduced into the bloodstream and if present in
sufficient numbers will result in clinical sepsis. (Cunha 1998).
Genitourinary tract:
Urosepsis is sepsis originating from the urinary tract, where the
organism cultured from the urine is the same as the organism cultured
from the blood. The urinary tract, like other organ systems, is designed to
prevent infection. (Cunha 1996).
Urosepsis occurs only in the setting of pre-existing renal disease,
abnormal urinary tract anatomy, foreign bodies (stents), renal or bladder
stones, or genitourinary instrumentation with infected urine.
Uropathogens causing urosepsis originate from the gastrointestinal tract
and expectedly are aerobic GNBs or group D enterococci, usually
Enteroccoccus faecalis (i.e., vancomycin- sensitive enterococci [VSE].
(Cunha 2007).
Gastrointestinal tract:
Another important source of sepsis is the distal gastrointestinal
tract. The colon contains more bacteria than any other organ. The fecal
flora is predominantly (w75%) Bacteroidesfragilis. Most of the remaining
anaerobic fecal flora are common coliforms (w20%) and less common
aerobic GNBs, excluding Pseudomonas aeruginosa. The remaining
portion of fecal flora (w5%) is comprised of group D enterococci. Of this,
about 95% are E faecalis (VSE) and about 5% are Enterococcus faecium,
which are virtually all vancomycin resistant (VRE). Because group D
enterococci are ‘‘permissive’’ pathogens in the gastrointestinal tract
26

Chapter II
(excluding the biliary tract), specific anti-VSE coverage is unnecessary in
intra-abdominal infections. (Hardaway 2000).
The predominant organism in the colonic flora is B fragilis.
Making up the other component of the fecal flora are aerobic GNBs,
which are the organisms that cause bacteremia and peritonitis. (Cruz , et
al 2002).
B fragilis is the predominant pathogen in lower intra-abdominal
andpelvic abscesses. When the integrity of the colon is breached and high
numbers of GNBs are released into the peritoneum or bloodstream by
infection (e.g., diverticulitis) or trauma (e.g., surgery or colitis), sepsis is
predictably frequent. (Sacks Berg ,et al 1992 ).
Biliary tract sepsis is usually due to Escherichia coli, Klebsiella
pneumoniae, or VSE. Optimal empiric monotherapy is with meropenem,
piperacillin- tazobactam, levofloxacin, or tigecycline. (Marshall 2002 ).
Pulmonary:
Pneumonias may be classified in many ways by causative organism
or by site of acquisition (ie, community-acquired pneumonias [CAPs] or
nosocomial pneumonia [NP]. A subset of hospital-acquired pneumonia
(HAP) or NP is ventilator-associated pneumonia (VAP). (Cunha 2007).
From the infectious disease perspective, NP, HAP, and VAP are
caused by the same pathogens. Occasionally, patients with HAP, NP, or
VAP may be complicated by septic shock. There are three NP, HAP, and
VAP pathogens that have the potential to cause sepsis and septic shock.
These are K pneumoniae, S aureus.(Bouza ,et al 2007).
27

Chapter II
CAPs are not associated with sepsis or septic shock except in
threecircumstances. Firstly, K pneumoniae is seen virtually only in
chronic alcoholics. (Cunha 2007).
K pneumoniae CAP is similar to K pneumoniae NP in terms of its
clinical characteristics and radiograph appearance. Nosocomial K
pneumoniae is more likely to present with sepsis and shock then its
community-acquired counterpart. P aeruginosa is not a cause of CAP
except in patients with cystic fibrosis or chronic bronchiectasis and even
in these patients does not present with sepsis or septic shock. Patients
who have febrile neutropenia who are predisposed to Pseudomonas
bacteremia do not present with Pseudomonas pneumonia with sepsis or
septic shock.(Steven 2005)
CAP due to MSSA or MRSA, either community-onset MRSA
(COMRSA)or community-acquired MRSA (CA-MRSA), may present
with sepsis and shock in patients with viral influenza or an influenza like
illness.(Magira , et al 2007).
Most staphylococcal pneumonias seen in the hospital are
communityacquired and superimposed upon viral influenza. In the
absence of influenza, S aureus is rarely, if ever, a CAP pathogen. Viral
influenzawith associated tracheo-bronchial damage predispose to
necrotizing hemorrhagic MSSA and MRSA CAP. Viral influenza alone is
associatedwith a high mortality and morbidity even in young healthy
adults. Certainlypatients with viral influenza and superimposed MSSA or
28

Chapter II
MRSA pneumonia are critically ill. However, it is difficult to factor out
the relative contributions of the bacterial versus the viral component in
terms of its virulence potential which, if not synergistic, is certainly
additive. (DiNubile ,et al 2004).
Skin, soft tissue, bones and joints:
Uncomplicated skin and soft-tissue infections including septic
arthritis and osteomyelitis, are rare causes of sepsis and septic shock, but
sepsis and septic shock may result from complicated skin and skin
structure infections, especially in compromised hosts, such as patients
with diabetes mellitus. Important example include toxic shock syndrome
(TSS) due to TSS-I–producing strains of group A streptococci or S
aureus. TSS is characterized by multiorgan dysfunction and may be fatal,
but TSS is primarily a toxin-mediated disorder rather than a septic
process per se. Necrotizing fasciitis may be accompanied by sepsis and
septic shock if untreated. Necrotizing fasciitis may be complicated by
TSS when due to group A streptocci or S aureus.(Owa ,et al 2003)
29

Chapter III
Chapter III
Diagnosis of SepsisSevere sepsis is a common and commonly fatal disease and is
essentially an exaggerated inflammatory response. The epidemiology of
severe sepsis and septic shock has been difficult to determine because of
an inconsistent approach to definitions and diagnosis. Patients with sepsis
account for approximately a third of hospital and intensive care unit bed
days in the UK and mortality ranges from 25% to 80%. (Angus,et al
2003).
The word sepsis is derived from the Greek word sepein, meaning
to putrefy or make rotten. In the past, physicians disagreed on definitions
for sepsis, septicemia, and septic shock, making clinical diagnosis,
research, and communication difficult. Then in 1992, the American
College of Chest Physicians and the Society of Critical Care Medicine
established some common ground. (Rangel ,et al 1995).
Patients are given a diagnosis of sepsis when they develop clinical
signs of infections or systemic inflammation; sepsis is not diagnosed
based on the location of the infection, or by the name of the causative
microbe. Physicians draw from a list of signs and symptoms in order to
make a diagnosis of sepsis, including abnormalities of body temperature,
heart rate, respiratory rate, and white blood cell count. There are many
so-called signs of sepsis which could be used in developing a ‘sepsis’
definition or to aid diagnosis, but none on their own are specific for
sepsis. (Bone ,et al 1989).
30

Chapter III
Sepsis is considered present if infection is highly suspected or
proven and two or more of the following, systemic inflammatory
response syndrome (SIRS) criteria are :Heart rate> 90 beats per
minute ,Body temperature < 36 (96.8 °F) or > 38 °C (100.4
°F) ,Hyperventilation (high respiratory rate) > 20 breaths per minute or,
on blood gas, a PaCO2 less than 32 mm Hg ,White blood cell count <
4000 cells/mm³ or > 12000 cells/mm³ (< 4 x 109 or > 12 x 109 cells/L), or
greater than 10% band forms (immature white blood cells).,Increased C
reactive protein.,Increased cardiac output, low systemic vascular
resistance.,Increased oxygen consumption.,Increased procalcitonine
concentration.,Increased interleukin 6 (IL6), IL8,…,Otherwise
unexplained alternation in coagulation parameter.,Otherwise unexplained
alternation in mental status.,Otherwise unexplained
hyperbilirubinemia.,Increased insulin requirement. (Bone ,et al 1992)
Sepsis is defined as a complex activation of the immune system
with a documented infection, SIRS is a complex activation of the immune
system regardless of etiology, infection, trauma, burns, or a sterile
inflammatory process, severe sepsis is sepsis plus organ dysfunction,
while septic shock is defined as sepsis plus unexplained acute circulatory
collapse with organ dysfunction, hypotension, and tissue hypo perfusion.
( Levy ,et al 2003)
The epidemiology of severe sepsis and septic shock has been
difficult to determine because of an inconsistent approach to definitions
and diagnosis. Not all patients are admitted to the intensive care unit
(ICU), many are elderly, and sepsis may be the final stage in a chronic
disease, especially in patients with immunosuppression. More than half of
all patients treated in hospital for severe sepsis are managed exclusively
in the general ward and some elderly, chronically sick patients may be
31

Chapter III
treated at home or in nursing homes. When a patient dies as a result of an
infectious disease, sepsis may not appear on the death certificate;
associated conditions such as bronchopneumonia, perforated viscous, or
malignancy may be recorded instead. ( Angus ,et al 2001).
For severe sepsis, the associated organ dysfunction can be
quantified using an organ dysfunction score such as the sequential organ
failure assessment (SOFA) scores (Table 2). This enables more
homogeneous groups of patients to be identified for epidemiological and
clinical trial purposes.
Table(2):The SOFA score (Vincent ,et al 1998)
SOFA score 0 1 2 3 4
Respiratory
PaO2/FiO2 mmHg
> 400 < 400 < 300 < 200 < 100
-- With respiratory support --
Coagulation Platelets x 103/mm3 > 150 < 150 < 100 < 50 < 20
LiverBilirubin, md/dl (µmol/l) <1.2 1.2-1.9 2.0-5.9 6.0-11.9 >12.0
CVSHypertension No
hypotensionMAP < 70
mmHg
Dop < 5,Or
dob (any dose)*
Dop > 5, epi < 0.1, or
norepi < 0.1*
Dop > 15, epi > 0.1, or
norepi > 0.1*
CNS GlasgowComa score
15 13-14 10-12 6-9 < 6
Renal Creatinine, mg/dl (µmol/l)
or urine output
< 1.2(< 110)
1.2 – 1.9(110 -170)
2.0-3.4(171-299)
3.5-4.9(300-440)
or < 500 ml/d
> 5.0(> 440)
or < 200 ml/d
32

Chapter III
Although the consensus criteria have help to establish common
definitions, these common definitions have several problems. First
almost all patient admitted to acute care hospitals will meet two of SIRS
criteria, although most of them will not have sepsis. For example a patient
with acute myocardial infarction is likely to have tachycardia,and
leucocytosis, and patient with alcohol withdrawal may have tachypnia,
tachycardia and fever. Second it is sometimes difficult to define evidence
of infection , and between 25%-50% of all patient who meet the sepsis
criteria will have negative cultures in the sitting of previous antibiotics or
fastidious organism. Other classification schemes have been offered,
including the predisposition, infection,response,and organ failure (PIRO)
system. (Levy ,et al 2001).
Although the (PIRO) system may lead to better models of sepsis
and better testing for patients, it does not currently appear to have role in
the diagnosis of patients with sepsis and septic shock. (Levy ,et al 2001).
Figure (4):PIRO
33

Chapter III
It is important to remember that even simple ‘flu is typically
associated with a septic response. However, it may not always be possible
to document the infection, particularly in ICU patients who are frequently
already on antibiotic therapy that interferes with microbiological culture
results. This does not mean that such patients do not have sepsis, and
indeed this group of patients have a higher mortality than patients in
whom infection is clearly identified presumably because a diagnosis of
sepsis may be delayed if no obvious source of infection presents itself,
and without microbiological data, it is not possible to target antibiotic
therapy. (Reyes ,et al 1999).
Procalcitonin (PCT) is a 116-amino acid propeptide, which
undergoes proteolysis into the hormone calcitonin . An increasing number
of clinical studies have been performed, since a commercial assay has
become available. Although the source of calcitonin has been generally
considered to be the thyroid cell (and other neuroendocrine cells), this
cell is probably not the source of PCT, as an infection-associated rise in
PCT has also been shown in thyroidectomized sepsis patients. The source
of PCT in sepsis is currently unclear. (Assicot ,et al 1993).
PCT has been suggested as an excellent early and discriminating
marker of bacteria-associated sepsis. (Gendrel ,et al 1997).
Reith et al. reported significant falls in plasma PCT concentrations
in patients with peritonitis after successful focal ablation. When surgical
removal of septic foci failed and patients died, mean PCT levels remained
high.PCT clearly discriminated between an infectious and a non
infectious etiology of acute respiratory distress syndrome (ARDS), while
IL-6 and C-reactive protein (CRP) proved inadequate .(Mesiner 2000).
34

Chapter III
INCIDENCE:Using the 1992 guidelines, Angus and Wax published an update
on the epidemiology of sepsis in 2001. They reported an increase in the
annual incidence from 73.6 to 175.9 per 100 000 of the population in the
United States between 1979 and 1989. (Angus ,et al 2001).
This represents up to 11% of all hospital admissions. The financial
costs of care are high, especially in the most critically ill patients and
non-survivors. Angus and colleagues estimated the average cost per case
as $22 000. The incidence of the condition is expected to increase by
1.5% per annum to 2010 .(Angus ,et al 2001).
The annual incidence of severe sepsis in patients admitted to ICUs
and meeting severe sepsis criteria at 24 h, was 51 per 10, 000 of the
population and the mortality rate was 47%. Patients with sepsis accounted
for 45% of ICU bed days and 33% of hospital bed days. The ICU length
of stay was between 4 and 8 days and the median hospital length of stay
was 18 days. (Padkin ,et al 2003).
Predisposing Factors: Age participates in modifying the host response to sepsis, as
infections in neonates, children, and adults may be quite different. Past
history is another feature, as patients with particular comorbidities (e.g.,
cirrhosis) or receiving immunosuppressive drugs may have different
characteristics. Genetic factors likely play an important role in
determining who develops sepsis, as well as its severity, and also
modulate the response to treatment. (Villar ,et al 2004).
35

Chapter III
Genetic susceptibility to septic shock: There are racial and gender differences in the propensity to develop
severe sepsis. Therefore it is not surprising that much interest has been
focused on whether the presence of specific genetic factors may influence
the development of severe sepsis and septic shock. Mira and colleagues
demonstrate that the presence of a particular single neucleotide
polymorphism (SNP) in the promoter for the Tumer necrotizing factor
(TNF) alpha receptor was found more frequently in patient who admitted
to I.C.U with septic shock than in normal controls patients who had this
particular genetic polymorphism (TNFα) were also more likely to die of
septic shock than those who did not have this SNP As TNF alpha has
been known to be involved with the pathogenesis of septic shock.
(Schaf ,et al 2003).
A study of patients with pneumococcal bacteremia showed that the
patients who develop septic shock were more likely to have a specific
polymorphisms in the interleukin -10 (IL-10) gene. This study did not
duplicate the findings of the relationship between the TNFα allele and the
mortality that was shown in the study by Mira et al, however there where
only a few patients in this study homozygose for this particular allele..
Blood from this patients stimulated with endotoxin were more likely to
have higher level of IL-10 than where heterozygous patients or patients
with a different polymorphism . (Esnaashari ,et al 2003).
Once there is a better understanding of a patient’s clinical a
genetic risk to develop septic shock targeted therapy might be directed
toward patients at high risk of death. (Fink , et al 2003).
Early and appropriate identification of patients with septic shock
and rapid transfer to locations capable of critical care monitoring and
36

Chapter III
early aggressive resuscitation are crucial for beginning targeted therapies
for these patients.Adequate provision of fluids, antimicrobial therapy,and
maintenance of organ perfusion all are essential to improving outcomes.
Most patients with septic shock appear to benefit from physiologic doses
of corticosteroids, and patients who meet criteria and are likely to benefit
should receive rAPC. Further studies involving potential genetic
predisposition to develop septic shock may allow better identification and
targeting of patients who require anti inflammatory or anticoagulation
therapy. (Schaf ,et al 2003).
FEATURES OF SEPSIS:- Hemodynamic Alterations :
The distinguishing hemodynamic features of septic shock are
elevated cardiac output, decreased systemic vascular resistance, and
decreased blood pressure. Tachycardia is partially responsible for
maintaining the blood pressure. Earlier investigators described
hyperdynamic and hypodynamic phases of septic shock. More recent
investigations have shown, however, that cardiac output remains elevated
until decreased output develops as a preterminal event. (Snell ,et al
1991).
Right and left ventricular ejection fractions are decreased in septic
shock, . In contrast to hypovolemic shock, increasing preload by
administering volume only minimally increases left ventricular stroke
work. This may be due to altered compliance characteristics of the
ventricles. Pulmonary artery hypertension, which frequently develops
early, also may be partially responsible for right ventricular dysfunction .
(Vercueil ,et al 2005).
37

Chapter III
Cardiac adrenergic down regulation also occurs. The number of
receptors and their affinities are reduced. Patients who recover from
septic shock increase their left ventricular stroke work index, whereas
those who deteriorate do not. (Vercueil ,et al 2005).
Radionuclide scans have shown that left ventricular dilation occurs
within 1–2 days of the onset of shock. This increased end-diastolic
volume permits a greater stroke volume in the face of decreased ejection
fraction. Left ventricular dilation improves as patients recover. Despite
the ventricular abnormalities, the coronary circulation exhibits above-
normalflow, normal myocardial oxygen consumption. (Garcott ,et al
2005).
The myocardial depressant factor (MDF) of sepsis has been
characterized as a low-molecular-weight protein. Patients with cardiac
disease and sepsis without shock fail to exhibit such activity. MDF may
originate from the intestinal tract in patients with hypovolemic shock
(Mythen ,et al 2005)
The decrease in circulatingplasma volume owing to increased
capillary permeabilityis a major influence in the hemodynamic
pathophysiology ofsepsis. In addition to actual transudation of fluid from
the intravascular into the interstitial space, peripheral pooling,
hepatosplanchnic venous pooling, and gastrointestinal and wound losses
along with idiopathic polyuria also reduce cardiac preload. Changes in
the pattern of blood flow distribution are characteristic of septic shock.
(Snell ,et al 1991)
Rather, it is likely that a mismatching of blood flow and metabolic
demand occurs. Thus some organs receive supernormal oxygen delivery,
whereas others are rendered ischemic. This is of particular importance in
38

Chapter III
the splanchnic circulation, where hepatic venous desaturation has been
reported in septic patients. (Cantraine ,et al 1998)
Metabolic Alterations :
Many studies have addressed the question of vascular shunting
versus metabolic alterations to account for the alterations in cellular
metabolism in septic shock. Some studies refer to a defective oxygen
consumption in septic shock. The concept of “cytopathic hypoxia” to
account for an abnormal cellular metabolism even after resuscitation
appears to be complete. It is likely that hemodynamic and metabolic
alterations coexist.(Marshall 2001)
SPECIFIC ORGAN INVOLVEMENT:It is not uncommon for organ dysfunction or organ failure to be the
first clinical sign of sepsis. No organ system is immune from the
consequences of the inflammatory excesses of sepsis, but those listed
below are most commonly involved:(Bohun ,et al 1997)
Circulation :
Significant derangement in metabolic autoregulation, the process
that matches oxygen availability to change tissue oxygen needs, is typical
of sepsis. Vasoactive mediators that are released with inflammation cause
an appropriate vasodilation and an increase in microvascular permeability
at the site of infection. Among these mediators are the vasodilators
prostacyclin and nitric oxide (NO), produced by endothelial cells.
(Vincet , ,et al 2008).
NO is believed to play a central role in the vasodilation
accompanying septic shock. Induction of an inducible form of NO
synthase can be demonstrated after incubating vascular endothelium and
smooth muscle with endotoxin. When this process extends to involve the
39

Chapter III
systemic circulation, mediators like NO depress the control mechanisms
that match oxygen delivery to oxygen needs at all the central, regional,
and microregional levels of the circulation. In addition, the inducible
form of NO may trigger injury in the central nervous system localized to
areas that regulate autonomic control. (Sharshar ,et al 2003).
A potential factor that may contribute to persistence of vasodilation
is impaired compensatory secretion of antidiuretic hormone(vasopressin).
In one report, plasma vasopressin levels were much lower in 19 patients
with septic shock than in 12 with cardiogenic shock who had similar
systemic blood pressures. Why this might occur is not clear. However,
numerous small studies have suggested that vasopressin may be helpful
in improving hemodynamics and allowing other pressors to be
withdrawn.(Carsin ,et al 2008)
In the central circulation, changes in both systolic and diastolic
ventricular performance are early manifestations of sepsis Nevertheless,
ventricular function may initially be able to increase the cardiac output
through use of the Frank Starling mechanism. This increase in output is
necessary to maintain the blood pressure in the presence of the systemic
vasodilatation that complicates sepsis. Patients with preexisting cardiac
disease may be unable to increase their cardiac output appropriately. This
may be a particular problem in elderly subjects. (Price , et al 1999).
In the regional circulation, the vascular hypo responsiveness induced by
sepsis leads to considerable heterogeneity in the normal distribution of
systemic blood flow among organ systems. As an example, sepsis
interferes with the normal ability to redistribute blood flow from the
splanchnic organs to the core organs (heart and brain) when oxygen
delivery is depressed. (Nevier ,et al 2008).
40

Chapter III
The microcirculation is a key (if not the most important) target
organ for injury in the sepsis syndrome. Sepsis is associated with a
decrease in the number of functional capillaries (capillarity), which
causes an inability to extract oxygen maximally .Depressed capillarity
includes "no flow" and excessive intermittent flow capillaries.
(De Backer ,et al 2008)
Compared to normal controls or critically ill patients without
sepsis, patients with severe sepsis have a overall decrease in vessel
density. These changes may be due to extrinsic compression of the
capillary by tissue edema, endothelial swelling, and plugging of the
capillary lumen by leukocytes or red blood cells (which lose their normal
deformability properties in sepsis. (De Backer , et al 2008).
Panendothelial activation in sepsis also leads to widespread tissue
edema, which is rich in protein. Other adverse effects of endothelial
dysfunction in sepsis include impaired anticoagulant properties and
upregulation of adhesion molecules. (Aird ,et al 2003 ).
Hypotension is the most severe expression of circulatory
dysfunction in sepsis. This is in part due to a redistribution of
intravascular fluid volume resulting from reduced arterial vascular tone
(leading to increased capillary pressure) and increased endothelial
permeability. Other changes that occur include venous dilation (thereby
diminishing venous return to the heart) and the release of myocardial
depressant substances. When hypotension complicates sepsis, anomalies
in the distribution of flow at the regional and microregional circulation
are accentuated, thereby accelerating the progression of tissue injury.
(Aird ,et al 2003)
41

Chapter III
Lung :
Endothelial injury in the pulmonary vasculature leads to disturbed
capillary blood flow and enhanced microvascular permeability, resulting
in interstitial and alveolar edema. (Ghosh ,et al 2003).
Neutrophil entrapment within the lung's microcirculation initiates
and/or amplifies this injury to the alveolocapillary membrane. Pulmonary
edema is the clinical consequence, and is accompanied by ventilation-
perfusion mismatch and arterial hypoxemia. The prominence of the lung
injury that is often seen in sepsis probably reflects the lung's large
microvascular surface area. The acute respiratory distress syndrome is a
frequent manifestation of these effects. (Ghosh ,et al 2003).
Gastrointestinal tract :
The gastrointestinal tract is a particularly important target organ
system for injury in sepsis since it has the potential to provide a positive
feedback loop in propagation of the injury . Particularly when the septic
patient is intubated and unable to eat, bacteria may overgrow the upper
gastrointestinal tract and may be aspirated into the lungs, producing
nosocomial pneumonia. Furthermore, the circulatory abnormalities
typical of sepsis may depress the gut's normal barrier function, allowing
translocation of bacteria and endotoxin into the systemic circulation
(possibly via lymphatics, rather than the portal vein) and extending the
septic response. (Upperman ,et al 2008).
L iver :
By virtue of the liver's role in host defense and synthetic functions,
liver dysfunction can contribute to both the initiation and progression of
sepsis. The reticuloendothelial system of the liver normally acts as the
first line of defense in clearing bacteria and bacteria-derived products that
42

Chapter III
have entered the portal system from the gut. Liver dysfunction can
prevent the elimination of enteric-derived endotoxin and bacteria-derived
products, which precludes the appropriate local cytokine response and
permits direct spillover of these potentially injurious products into the
systemic circulation(Luce ,et al 2008).
Kidney :
Sepsis is often accompanied by acute renal failure due to acute
tubular necrosis).The mechanisms by which sepsis and endotoxinemia
might lead to acute renal failure are incompletely understood. Systemic
hypotension, direct renal vasoconstriction, release of cytokines such as
tumor necrosis factor, and activation of neutrophils by endotoxin.
(Ghosh ,et al 2008)
The likelihood of death is increased in patients with sepsis who
develop renal failure. Why this occurs is not well understood. One factor
that may contribute is the release of proinflammatory mediators as a
result of leukocyte-dialysis membrane interactions when hemodialysis is
necessary. Use of biocompatible membranes can prevent these
interactions and may improve survival and the recovery of renal function.
(Hakim ,et al 2007)
Nervous system :
Clinically, involvement of the central nervous system in sepsis can
produce an altered sensorium (encephalopathy) and a peripheral
neuropathy. The pathogenesis of the encephalopathy is poorly defined.
Although a high incidence of brain micro abscesses was noted in one
study, the significance of hematogenous infection as the principal
mechanism has been questioned because of considerable heterogeneity in
the observed pathology. (Hund 2001).
43

Chapter III
Epidemiological studies suggest that at least 25 percent of patients
admitted to medical or surgical intensive care units have some degree of
acquired paresis. (De Jonghe 2002).
Most episodes present seven or more days after the onset of critical
illness. Affected patients manifest a sensorimotor polyneuropathy
characterized clinically by,Limb muscle weakness and atrophy ,Reduced
or absent deep tendon reflexes ,Loss of peripheral sensation to light touch
and pin prick, Relative preservation of cranial nerve function.
(Fleshner,et al 1998)
Critical illness polyneuropathy is strongly associated with sepsis
and probably represents a neurologic manifestation of the systemic
inflammatory response syndrome. The mechanism of axonal injury in this
condition is unknown. (Deem , et al 2003)
There is growing recognition of the influence of the
parasympathetic nervous system as a mediator of systemic inflammation.
In experimental models, afferent vagus nerve stimulation during sepsis
increases the secretion of corticotropin-releasing hormone (CRH),
ACTH, and cortisol; the last effect is suppressed by subdiaphragmatic
vagotomy. (Fleshner ,et al 1998 ).
Parasympathetic tone also affects thermoregulation, as
experimental vagotomy results in an attenuated hyperthermic response to
IL-1(Romanovsky 1997).
Efferent parasympathetic activity, mediated by acetylcholine, also
has an anti-inflammatory effect on the cytokine profile, with decreased in
vitro expression of the proinflammatory cytokines TNF, IL-1, IL-6 and
IL-18. Furthermore, in mouse models of endotoxemia, external vagal
44

Chapter III
stimulation prevented the onset of shock in animals following vagotomy .
A similar murine model used nicotine, a cetylcholine receptor agonist, to
diminish the pathologic response to sepsis. (Wang ,et aL 2004).
Sepsis may therefore be described as an auto-destructive process
that permits the extension of a normal patho-physiologic response to
infection to involve otherwise normal tissue. This can result in the
multiple organ dysfunction syndrome (MODS). (Wang ,et al 2004).
Death of patients with sepsis:No autopsy studies have revealed why patients with sepsis die.
Occasionally, a patient with sepsis may die of refractory shock, but this is
exceptional. (Martin , et al 2003 ).
Although patients with sepsis have profound myocardial
depression, cardiac output is usually maintained because of cardiac
dilatation and tachycardia. Although the acute respiratory distress
syndrome frequently develops in patients with sepsis, such patients rarely
die of hypoxemia or hypercarbia .(Van Amersfoort , et al 2003 ).
Renal failure is common, but that alone is not fatal, because
dialysis may be used. Liver dysfunction rarely progresses to hepatic
encephalopathy. Thus, the exact cause of death in patients with sepsis
remains elusive. Many patients die when care is withdrawn or not when
families, in consultation with physicians, decide that continued therapy is
futile. (Van Amersfoort ,et al 2003).
45

Chapter V
CHAPTER IV
Management of SepsisEarly Management:
The first priority in any patient with severe sepsis or septic shock is
stabilization of their airway and breathing. Next, perfusion to the
peripheral tissues should be restored. (Dellinger ,et al 2008).
Early goal directed therapy:
The cornerstone of emergency management of sepsis is early goal
directed therapy plus lung protective ventilation, broad spectrum
antibiotics, and possibly activated protein C. In early goal directed
therapy, central venous oxygen saturation is monitored continuously with
the use of a central venous catheter. (Wheeler ,et al 2004).
In early goal directed therapy, Crystalloids were administered to
maintain central venous pressure at 8 to 12 mmHg. Vassopressors were
added if the mean arterial pressure was less than 65mmHg; if central
venous oxygen saturation was less than 70%, erythrocyte were transfused
to maintain a hematocrit of more than 30%. Dobutamine was added if the
central venous pressure, mean arterial pressure, and hematocrit were
optimized yet venous oxygen saturation remain below 70% .(Russel
2006) .
Stabilize respiration:
46

Chapter V
Supplemental oxygen should be supplied to all patients with sepsis
and oxygenation should be monitored continuously with pulse oximetry.
Intubation and mechanical ventilation may be required to support the
increased work of breathing that typically accompanies sepsis, or for
airway protection since encephalopathy and a depressed level of
consciousness frequently complicate sepsis. (Luce 2008)
Chest radiographs and arterial blood analysis should be obtained
following initial stabilization. These studies are used in combination with
other clinical parameters to diagnose acute lung injury (ALI) or acute
respiratory distress syndrome (ARDS), which frequently complicate
sepsis (Ghosh ,et al 2008).
Acute lung injury often complicate sepsis and lung protective
ventilation meaning the use of relatively low tidal volume is so another
important aspect of management .Furthermore lung protective decrease
mortality and is beneficial in septic acute lung injury. (Eisner ,et al
2001).
47

Chapter V
Figure (5): Protocol for early goal directed therapy
48
Supplemental oxygen ± endotracheal intubation and
mechanical ventilation
Central venous and arterial
catheterization
Sedation& paralysis or both
CVP
Goals achieved
Hospital admission
Crystalloid
Colloid
Vasoactive agents
Trans1fusion of red cells until hematocrit 30%
Inotropic agents
MAP
Scov2
8-12mmHg
8mmHg
< 65 mmHg
>90 mmHg
>65 and<90mmHg
70%
<70% <70%
no

Chapter V
Excessive tidal volume and repeated opening and closing of alveoli
during mechanical ventilation cause lung injury. Lung protective
mechanical ventilation with use of low tidal volume of 6 ml per Kg of
ideal body weight (or as low as 4 ml per Kg if the plateau pressure
exceeds 30 cm H2O) as compared with 12 ml per Kg of ideal body
weight has been shown to decrease the mortality rate from 40 to 31%, to
lessen organ dysfunction, and to lower level of cytokines. (Engl 2000).
Positive end expiratory pressure (PEEP) decrease oxygen
requirements, however there is no significant difference in mortality
between patients treated with the usual PEEP regimen of the acute
respiratory distress syndrome (ARDS) and those treated with higher
levels (Browser ,et al 2004).
Patients receiving ventilation require appropriate but not excessive
sedation, given the risks of prolonged ventilation and nosocomial
pneumonia. Titrating sedation and interrupting sedation daily until
patients are awake .Decrease the risks associated with sedation.
Neuromascular blocking agent should be avoided to reduce the risk of
prolonged neuromascular dysfunction .(Segredo ,et al 1992).
Assess perfusion: Once the patient's respiratory status has been stabilized, the
adequacy of perfusion should be assessed. Hypotension is the most
common indicator that perfusion is inadequate. Therefore, it is important
that the blood pressure be assessed early and often. An arterial catheter
may be inserted if blood pressure is labile or restoration of arterial
perfusion pressures is expected to be a protracted process, because a
sphygmomanometer may be unreliable in hypotensive patients. Attempts
49

Chapter V
to insert an arterial line should not be allowed to delay the prompt
management of shock .(Hollenberg ,et al 1992).
Critical hypoperfusion can also occur in the absence of
hypotension, especially during early sepsis. Thus, clinical evidence of
impaired perfusion should be sought in all patients with sepsis.
(Hollenberg ,et al 2004)
Common signs of hypoperfusion include cool, vasoconstricted skin
due to redirection of blood flow to core organs (although warm, flushed
skin may be present in the early phases of sepsis), restlessness, oliguria or
anuria, and lactic acidosis. These findings may be modified by
preexisting disease or medications. As an example, elderly patients,
diabetic patients, and patients who take beta-blockers may not exhibit an
appropriate tachycardia as blood pressure falls. Patients with chronic
hypertension may develop critical hypoperfusion at a higher blood
pressure than healthy patients (i.e., relative hypotension). (Hollenberg,et
al 2004).
Catheters:- After initial assessment, a central venous catheter (CVC) should be
inserted in most patients with severe sepsis or septic shock. A CVC can
be used to infuse intravenous fluids, infuse medications, infuse blood
products, and draw blood. In addition, it can be used for hemodynamic
monitoring by measuring the central venous pressure (CVP) and the
central venous oxyhemoglobin saturation (ScvO2). In one clinical trial,
treatment of septic shock guided by the ScvO2 reduced mortality.
(Rivers,et al 2008)
50

Chapter V
We believe that pulmonary artery catheters (PACs) should not be
used in the routine management of patients with severe sepsis or septic
shock. PACs can measure the pulmonary artery occlusion pressure
(PAOP) and mixed venous oxyhemoglobin saturation (SvO2). In theory,
this may be helpful to guide circulatory resuscitation. However, the
PAOP has proven to be a poor predictor of fluid responsiveness in sepsis
and the SvO2 is similar to the ScvO2, which can be obtained from a
CVC. PACs increase complications and have not been shown to improve
outcome. (Harveys ,et al 2008).
Respiratory changes in the radial artery pulse pressure, aortic blood
flow peak velocity, and brachial artery blood flow velocity are considered
dynamic hemodynamic measures, whereas CVP and PAOP are
considered static hemodynamic measures. (Brennan ,et al 2007).
There is increasing evidence that dynamic measures are more
accurate predictors of fluid responsiveness than static measures, as long
as the patients are in sinus rhythm and passively ventilated with a
sufficient tidal volume. It seems likely that dynamic measures will
become more common and be used to identify patients who are likely to
increase organ perfusion in response to intravenous fluids. (Reuter ,et al
2008)
Restore perfusion:- Once it has been established that hypoperfusion exists, early
restoration of perfusion is necessary to prevent or limit multiple organ
dysfunction, as well as reduce mortality. Hypoperfusion results from loss
of plasma volume into the interstitial space, decreased vascular tone, and
myocardial depression. The increase in the cardiac output that is
51

Chapter V
necessary to compensate for the diminished vascular tone may be limited
by the myocardial depression. (Dellinger ,et al 2008).
Resuscitation of the circulation should target a ScvO2 or SvO2 ≥70
percent. Other reasonable goals include a central venous pressure 8 to 12
mmHg, a mean arterial pressure (MAP) ≥65 mmHg, and a urine output
≥0.5 mL/kg per hour. (Dellinger ,et al 2008).
These goals derive from a clinical trial in which 263 patients with
severe sepsis or septic shock were randomly assigned to therapy targeting
a ScvO2 ≥70 percent, or conventional therapy that did not target a ScvO2.
Both groups initiated therapy within six hours of presentation and
targeted the same CVP, MAP, and urine output. Mortality was lower in
the group that targeted a ScvO2 ≥70 percent (31 versus 47 percent).
Earlier studies of critically ill patients that used similar targets (SvO2 ≥70
percent) found no mortality benefit, probably because these studies were
not conducted during the crucial initial hours .(Gattinoni ,et al 2008.).
The approach employed in this trial is known as "early goal-
directed therapy" (ie, administered within the first six hours of
presentation). In our clinical practice, we adhere to the principles of early
goal-directed therapy; that is, we initiate aggressive therapy early to
restore perfusion and we target a ScvO2 ≥70 percent. However, we
consider the numeric goals for CVP, MAP, and urine output guidelines
and always consider additional clinical signs of hypoperfusion when
assessing the patient's response to a therapy and need for more of a
therapy. (Gattinoni ,et al 2008).
Intravenous fluids: Relative intravascular hypovolemia is typical and may be severe.
As an example, early goal-directed therapy required a mean infusion
52

Chapter V
volume of approximately five liters within the initial six hours of therapy
in the trial described above. As a result, rapid, large volume infusions of
intravenous fluids are indicated as initial therapy for severe sepsis or
septic shock, unless there is coexisting clinical or radiographic evidence
of heart failure. (Rivers ,et al 2008).
Fluid therapy should be administered in well-defined (eg, 500 mL),
rapidly infused boluses. Volume status, tissue perfusion, blood pressure,
and the presence or absence of pulmonary edema must be assessed before
and after each bolus. Intravenous fluid challenges can be repeated until
blood pressure is acceptable, tissue perfusion is acceptable, pulmonary
edema ensues, or fluid fails to augment perfusion. (Hollenberg 2004).
Careful monitoring is essential in this approach because patients
with sepsis typically develop noncardiogenic pulmonary edema (ie, ALI,
ARDS). In patients with ALI or ARDS who are hemodynamically
resuscitated, a liberal approach to intravenous fluid administration
prolongs the duration of mechanical ventilation, compared to a more
restrictive approach that typically requires large doses of furosemide.
(Snell ,et al 2006)
Thus, while the early, aggressive fluid therapy is appropriate in
severe sepsis and septic shock, fluids may be unhelpful or harmful when
the circulation is no longer fluid-Crystalloid versus colloid Clinical trials
have failed to consistently demonstrate a difference between colloid and
crystalloid in the treatment of septic shock. (Wilkes 2001).
In the saline versus albumin fluid evaluation (SAFE) trial, 6997
critically ill patients were randomly assigned to receive 4 percent albumin
or normal saline for up to 28 days. There were no differences between
groups for any endpoint, including the primary endpoint, mortality.
53

Chapter V
Among the patients with severe sepsis (18 percent of the total group),
there were also no differences in outcome. (Finfer ,et al 2004).
Another randomized trial compared pentastarch (a colloid) to
modified Ringer's lactate (a crystalloid) in patients with severe sepsis the
Efficacy of Volume Substitution and Insulin Therapy in Severe Sepsis
(VISEP) trial. There was no difference in 28-day mortality, but the trial
was stopped early because there was a trend toward increased 90-day
mortality among patients who received pentastarch. (Brunkhorst ,et al
2008).
In our clinical practice, we generally use crystalloid because of the
higher cost of colloid. We believe that giving a sufficient quantity of
intravenous fluids rapidly and targeting appropriate goals is more
important than the type of fluid chosen. (Brunkhorst ,et al 2008).
Vasopressors: Vasopressors are second line agents in the treatment of severe
sepsis and septic shock; we prefer intravenous fluids as long as they
increase perfusion without seriously impairing gas exchange . However,
intravenous Vasopressors are useful in patients who remain hypotensive
despite adequate fluid resuscitation or who develop cardiogenic
pulmonary edema (Reinhart ,et al 2008).
There is no definitive evidence of the superiority of one
vasopressor over another. We prefer norepinephrine, although dopamine
is also a reasonable first-choice among vasopressors .Phenylephrine, a
pure alpha-adrenergic agonist, may be particularly useful when
tachycardia or arrhythmias preclude the use of agents with beta-
adrenergic activity. Limited experience with vasopressin (antidiuretic
54

Chapter V
hormone) suggests that this agent may be useful in vasodilatory septic
shock. table (3). ( Herber ,et al 2008).
Table (3): Vasopressor in sepsis
Drug DosageDobutamine 2.5-20Mic/kg/minDopamine 1-5Mic/kg/min
5-10 Mic/kg/min
10-20 Mic/kg/minEpinephrine 1-10 Mic/minNorepinephrine 0.5-30 Mic/minVasopressin 0.04 units/min
Additional therapies:When the ScvO2 remains <70 percent after optimization of
intravenous fluid and vasopressor therapy, it is reasonable to consider
additional therapies, such as inotropic therapy or red blood cell
transfusion.
Inotropic therapy For patients who have myocardial dysfunction, a
trial of inotropic therapy is warranted if ScvO2 remains <70 percent after
all of the interventions discussed above . Inotropic therapy should not be
used to increase the cardiac index to supranormal levels (Dellinger
2008).
Dobutamine is the usual inotropic agent. At low doses, dobutamine
may cause the blood pressure to decrease because it can dilate the
systemic arteries. However, as the dose is increased, blood pressure
usually rises because cardiac output increases out of proportion to the fall
in vascular resistance. (Dellinger 2008).
55

Chapter V
Red blood cell transfusions:Early goal-directed therapy aggressively
utilizes red blood cell transfusions to raise the ScvO2. In the trial
discussed above, nearly 70 percent of patients in the early goal-directed
therapy group received transfusions, compared to 45 percent in the
conventional therapy group . However, other data support a more
cautious approach to transfusion in critically ill patients. (Herber ,et al
2008).
There are several possible explanations for the conflicting data.
Outcome may be related to when a red blood cell transfusion is
given. Transfusions administered as part of early goal-directed therapy
were given early in the course of illness, whereas studies that support a
more cautious approach typically gave transfusions later in the course of
illness.(Gosh ,et al 2003)
The apparent benefit of red blood cell transfusions may be due to
other interventions. In other words, red blood cell transfusion was just
one of several interventions during early goal-directed therapy and it is
possible that the benefit was due to one or more of the other
interventions, not the red blood cell transfusion per se. (Herber 2008)
Ongoing management: There are two possible outcomes following the interventions described
above:
Despite aggressive therapy, the patient may have persistent
hypoperfusion and progressive organ failure. This should prompt
reassessment of the adequacy of the above therapies, antimicrobial
regimen, and control of the septic focus, as well as the accuracy of the
56

Chapter V
diagnosis and the possibility that unexpected complications or coexisting
problems have intervened (eg, pneumothorax following CVC insertion).
(Rivers ,et al 2008)
The patient may have responded to the above interventions with
restored perfusion and a ScvO2 greater than 70 percent. Such patients
should continue to have their clinical and laboratory parameters followed
closely. These include blood pressure, arterial lactate, urine output,
creatinine, platelet count, Glasgow coma score, serum bilirubin, liver
enzymes, oxygenation (ie, arterial oxygen tension or oxyhemoglobin
saturation), and gut function. Gastric tonometry may also be helpful, if
available. Reevaluation is indicated if any of these parameters worsen or
fail to improve (Kumar ,et al 2008).
In early sepsis, most lactate is probably a byproduct of anaerobic
metabolism due to organ hypoperfusion. Supporting this view, early goal-
directed therapy decreases lactate levels faster than conventional therapy .
After the restoration of perfusion, however, lactate is probably due to
causes other than anaerobic metabolism and further increasing oxygen
delivery to the peripheral tissues is unlikely to decrease its levels . As a
result, lactate values are generally unhelpful following restoration of
perfusion, with one exception a rising lactate level should prompt
reevaluation of perfusion (Rivers ,et al 2008).
It would be ideal if hypoxia could be detected for individual
organs, because tests that combine output from many organs (eg, arterial
lactate) may obscure the presence of significant ischemia in an individual
organ (Richard ,et al 2008).
57

Chapter V
Gastric tonometry indirectly measures perfusion to the gut by
estimating the gastric mucosal PCO2. It can be used to detect gut hypoxia
by calculating the gastric to arterial PCO2 gap. But, gastric tonometry is
not widely available and it is uncertain whether it can successfully guide
therapy. Additional studies and clinical experience are needed .
(Gutierrez ,et al 2002)
CONTROL OF THE SEPTIC FOCUS:- Prompt identification and treatment of the culprit site of infection
are essential. Source control is the critical, targeted intervention in the
treatment of sepsis and septic shock, whereas most other therapies are
purely supportive.( Buisson ,et al 2008)
Identification of the septic focus: A careful history and physical examination may yield clues to the
source of sepsis and help guide subsequent microbiologic evaluation.
Gram stain of material from sites of possible infection may give early
clues to the etiology of infection while cultures are incubating. As
examples, urine should be routinely Gram stained and cultured, sputum
should be examined in a patient with a productive cough, and an intra-
abdominal collection in a postoperative patient should be percutaneously
sampled under radiologic guidance.Blood should be taken from two
distinct venipuncture sites and inoculated into standard blood culture
media.(Gibot 2004).
There is no single test that immediately confirms the diagnosis of
severe sepsis or septic shock. However, several laboratory tests, which
are still investigational, have been studied as diagnostic markers of active
bacterial infection. (Tang ,et al 2007).
58

Chapter V
The plasma concentration of soluble TREM-1 (triggering receptor
expressed on myeloid cells), a member of the immunoglobulin
superfamily that is specifically up regulated in the presence of bacterial
products, is increased in patients with sepsis . In a small trial, increased
TREM-1 levels were both sensitive and specific for the diagnosis of
bacterial sepsis (96 and 89 percent, respectively). Serial monitoring of
TREM-1 may also provide prognostic information in patients with
established sepsis.(Gibot ,et al 2005).
Elevated serum procalcitonin levels are associated with bacterial
infection and sepsis. But, a meta-analysis of 18 studies found that
procalcitonin distinguished sepsis from nonseptic systemic inflammation
poorly (sensitivity of 71 percent and specificity of 71 percent). (Tang ,et
al 2007)
Evaluation of the clinical usefulness of both TREM-1 and
procalcitonin is still in its earliest stages and should be considered
preliminary. Until additional clinical investigations have been performed,
we do not suggest the routine use of either. (Tang ,et al 2007).
Eradication of infection:Eradication of the inciting infection is essential to the successful
treatment of severe sepsis and septic shock. Source control (physical
measures undertaken to eradicate a focus of infection and eliminate
ongoing microbial contamination) should be undertaken since undrained
foci of infection may not respond to antibiotics alone. As examples,
potentially infected foreign bodies (eg, vascular access devices) should be
removed when possible, and abscesses should undergo percutaneous or
surgical drainage. Some patients require extensive soft tissue debridement
59

Chapter V
or amputation; in rare cases, fulminant Clostridium difficile-associated
colitis may necessitate colectomy. (Fekety ,et al 2008).
Antimicrobial regimen: Intravenous antibiotic therapy should be initiated immediately after
obtaining appropriate cultures. The choice of antibiotics can be complex
and should consider the patient's history, comorbidities, clinical
syndrome, Gram's stain data, and local resistance patterns. (Sibbald ,et al
1995).
Delayed, inadequate, or inappropriate antimicrobial therapy (ie,
treatment with antibiotics to which the pathogen was later shown to be
resistant in vitro) is associated with poor outcome. (Kumar 2006).
A prospective cohort study of 2124 patients demonstrated that
inappropriate antibiotic selection was surprisingly common (32 percent).
Mortality was markedly increased in these patients compared to those
who had received appropriate antibiotics (34 versus 18 percent).
(LeibovociL ,et al 1997)
A retrospective analysis of 2731 patients with septic shock
demonstrated that the time to initiation of appropriate antimicrobial
therapy was the strongest predictor of mortality .(Kumar ,et al 2007).
When the potential pathogen or infection source is not immediately
obvious, we favor broad spectrum antibiotic coverage directed against
both gram-positive and gram-negative bacteria. Few guidelines exist for
the initial selection of empiric antibiotics in severe sepsis or septic shock.
In our practice, if Pseudomonas is an unlikely pathogen, we favor
combining vancomycinCephalosporin, 3rd or 4th generation (eg,
ceftriaxone or cefotaxime), or Beta-lactam/beta-lactamase inhibitor (eg,
60

Chapter V
piperacillin-tazobactam, ticarcillin-clavulanate, or ampicillin-sulbactam),
or Carbapenem (eg, imipenem or meropenem). (Price,et al 2003)
Alternatively, if Pseudomonas is a possible pathogen, we combine
vancomycin with Antipseudomonal cephalosporin (eg, ceftazidime or
cefoperazone), or Antipseudomonal carbapenem (eg, imipenem,
meropenem), or Antipseudomonal beta – lactam/beta-lactamase inhibitor
(eg, piperacillin-tazobactam,ticarcillin-clavulanate), or Fluoroquinolone
with good anti-pseudomonal activity (eg, ciprofloxacin), or
Aminoglycoside (eg, gentamicin, amikacin), or Monobactam (eg,
aztreonam).(Price ,et al 2003)
Selection of two agents from the same class, for example, two beta-
lactams, should be avoided. We emphasize the importance of considering
local susceptibility patterns when choosing an empiric antibiotic regimen
(McDonald ,et al 2005)
Staphylococcus aureus is associated with significant morbidity if
not treated early in the course of infection . There is growing recognition
that methicillin-resistant S. aureus (MRSA) is a cause of sepsis not only
in hospitalized patients, but also in community dwelling individuals
without recent hospitalization . Many of these Staphylococci have the
Panton-Valentine leukocidin virulence factor, which causes severe,
necrotizing infections. For these reasons, we recommend that severely ill
patients presenting with sepsis of unclear etiology be treated with
intravenous vancomycin (adjusted for renal function) until the possibility
of MRSA sepsis has been excluded. (Francis ,et al 2005).
After culture results and antimicrobial susceptibility data return, we
recommend that therapy be pathogen-directed, even if there has been
clinical improvement while on the initial antimicrobial regimen. Gram-
61

Chapter V
negative pathogens have historically been covered with two agents from
different antibiotic classes. However, several clinical trials and two meta-
analyses have failed to demonstrate superior overall efficacy of
combination therapy compared to monotherapy with a third generation
cephalosporin or a carbapenem . Furthermore, one meta-analysis found
double coverage was associated with an increased incidence of adverse
events. For this reason, we recommend use of a single agent with proven
efficacy and the least possible toxicity, except in patients who are
neutropenic or whose severe sepsis is due to a known or suspected
Pseudomonas infection. (Safdar ,et al 2004).
Regardless of the antibiotic regimen selected, patients should be
observed closely for toxicity, evidence of response, and the development
of nosocomial superinfection . The duration of therapy is typically 7 to 10
days, although longer courses may be appropriate in patients who have a
slow clinical response, an undrainable focus of infection, or immunologic
deficiencies. In patients who are neutropenic, antibiotic treatment should
continue until the neutropenia has resolved. If infection is thoroughly
excluded, antibiotics should be discontinued to minimize colonization or
infection with drug-resistant microorganisms and superinfection with
other pathogens. (Dellinger , et al 2008).
Glucocorticoids: One of the most controversial areas of sepsis therapy the use of
corticosteroids has seen tremendous change in the past few years. Despite
an initial study suggesting that the prognosis of septic shock patients
could be determined by their response to adrenocorticotropic hormone
(ACTH) stimulation , and a follow-up study suggesting that treatment of
septic shock patients with relative adrenal insufficiency improved
62

Chapter V
survival, there has been continued debate about the appropriate use of
corticosteroids in septic shock. (Luce 2004).
The landmark Corticosteroid Therapy of Septic Shock Corticus
trial has been presented at meetings of the American College of Chest
Physicians, the Society of Critical Care Medicine. Corticus randomized
500 septic shock patients from 52 European centers to receive either
intravenous hydrocortisone or placebo. The trial was suspended prior to
reaching its goal of 800 patients, for both slow recruitment and futility
(no difference in 28-day mortality, 33% for hydrocortisone patients vs
31% for placebo patients). Of importance, ACTH stimulation results were
not prognostic for ultimate survival, and even patients with relative
adrenal insufficiency did not benefit from hydrocortisone therapy.
(Annane ,et al 2002).
Although the duration of shock was shorter in patients who
received corticosteroids, there was also a higher incidence of
hyperglycemia, nosocomial sepsis, and recurrent septic shock in the
hydrocortisone-treated patients. The best explanation for the difference in
outcomes seen between the Annane study and the Corticus study may lie
in the patient populations. The Annane study enrolled patients with septic
shock and refractory hypotension despite fluid resuscitation and
vasopressor administration. In contrast, the Corticus study enrolled septic
shock patients requiring vasopressor administration, but without the
requirement for ongoing hypotension. Thus, the Annane study enrolled a
more severely ill population, which may behave differently and respond
to corticosteroids differently, compared with the more traditional septic
shock population in the Corticus study. (Annane ,et al 2002)
63

Chapter V
Nutrition: There is consensus that nutritional support improves nutritional
outcomes in critically ill patients, such as body weight and mid-arm
muscle mass. However, it is uncertain whether nutritional support
improves important clinical outcomes (eg, duration of mechanical
ventilation, length of stay, mortality), or when nutritional support should
be initiated. (Dellinger ,et al 2008).
Intensive insulin therapy: Hyperglycemia and insulin resistance are virtually universal in
sepsis. Hyperglycemia is potentially harmful because it act as
progoagulant induce apoptosis, impair neutrophli function, increase the
risk of infection, impairs wound healing, and is associated with an
increase risk of death.
Conversely insulin can control hyperglycemia and improve lipid level,
insulin has anti-inflammatory, anticoagulant, and anti apoptotic action
and protects endothelial and mitochondrial function. (Langouch ,et al
2005).
Intensive insulin therapy decreased the rate of death in ICU,
especially among the patient who significantly decreased the prevalence
of prolonged ventillatory support, renal replacement therapy, peripheral
neuromuscular dysfunction, and bacteremia. (Vanhorebebeek ,et al
2005).
The appropriate target glucose range and insulin dose in patients
with sepsis are unknown, because no randomized, controlled trial has
been conducted to specifically study patients with sepsis. The results of
randomized, controlled trial of insulin in surgical patients suggested that
intensive insulin therapy might be of benefit in sepsis. Van den Berghe
64

Chapter V
and colleages, 2006 randomly assigned critically ill surgical patients to
receive insulin infusion. The study involved intubated surgical patients
(primarily those under going cardiac surgery) not patients with sepsis.
(Van den Berghe . et al 2006 )
A recent trial by the same group in medical ICU patients showed
no significant difference in mortality with the use of intensive or
conventional insulin therapy; intensive insulin therapy decreased the rate
of death among patients whose stay lasted fewer than 3 days .( Berghe,et
al 2006).
The 2008 guidelines stress on the tight glycemic control in patient
with long I.C.U stay to decrease mortality and morbidity and recommend
that patients with severe sepsis & hyperglycemia receive intravenous
insulin therapy to a target blood glucose level of less than 150mg/dl .
(Gandhi , et al 2007)
Vasopressin:Vasopressin deficiency and down regulation of vasopressin
receptors are common in septic shock. Vasopressin dilates renal,
pulmonary, cerebral and coronary arteries. Intravenous infusion of low
dose of vasopressin(0.03 to 0.04 U per minute)has been reported to
increase blood pressure, urine output and creatinine clearance, permitting
dramatic decrease in vasopressor therapy. However vasopressin therapy
may cause intestinal ischemia, decreased cardiac output, skin necrosis,
even cardiac arrest especially at doses greater than 0.04 U per minute.
Q (Fisher ,et al 1996).
65

Chapter V
Immunotherapy:Although cytokines are considered to be culprits, they also have
beneficial effects in sepsis. Studies in an animal model of peritonitis
demonstrated that blocking TNFα worsens survival.
(Echtenacher ,et al 2001)
Combination immunotherapy against TNFα and interleukin-1
receptors was fatal in a neutropenic model of sepsis. (Opal ,et al 1996).
In clinical trials, a TNF antagonist increased mortality. The role of
TNFα in combating infection has recently been underscored by the
finding that sepsis and other infectious complications developed in
patients with rheumatoid arthritis who were treated with TNF antagonists.
(Keane ,et al 2001)
The debate about the merits of inhibiting cytokines in patients with
sepsis has been rekindled by a recent trial that indicated that a subgroup
of patients with sepsis who had therapy directed against TNFα had
improved survival. Also, a meta-analysis of clinical trials of
antiinflammatory agents in patients with sepsis showed that although high
doses of antiinflammatory agents were generally harmful in such patients,
a subgroup of patients (approximately 10 percent) benefited. (Keane ,et
al 2001).
Advances in our understanding of cell-signaling pathways that
mediate the response to microbes have demonstrated that the concept of
blocking endotoxin in order to prevent septic complications may be
simplistic. Cells of the innate immune system recognize microorganisms
and initiate responses through pattern-recognition receptors called toll-
likereceptors (TLRs). (Underhill,et al 2002).
66

Chapter V
Insight into the role of TLRs in combating infection has been
provided by studies in C3H/HeJ mice,(141) which are resistant to
endotoxin because of a mutation in the toll-like receptor 4 gene
(TLR4).Despite their resistance to endotoxin, these mice have increased
mortality with authentic sepsis . TLR4 mutations have been identified in
humans and may make persons more susceptible to infection.
(Arbour ,et al 2000)
Therefore, although endotoxin has deleterious effects, total
blockade of endotoxin may be detrimental. Reasons for the failure of
monoclonal antiendotoxin antibodies to improve outcomes in trials
involving patients with sepsis are complex. (Arbour ,et al 2000).
Renal dysfunction and dialysis:Acute renal failure is associated with increased mortality and
morbidity, and resources use in patients with sepsis.(Schrier, et al 2004).
Continuous renal replacement therapy decrease the incidence of
adverse biomarkers, but there is little evidence that it changes outcome.
Low dose of dopamine (2 to 4 Mic per kg per minute) neither decrease
the need for renal support nor improves survival and consequently, is not
recommended. lactic acidosis is a common complication of septic shock,
however sodium bicarbonate improves neither hemodynamics nor the
response to vassopressors medications. (Bellomo , et al 2000).
NEW TREND IN THE TREATMENTRecombinant human activated protein C
67

Chapter V
Chapter VActivated Protien C
In the last half of the 20th century, the use of antibiotics for the
treatment of bacterial infections transformed the practice of medicine,
resulting in sharp reductions in morbidity and mortality from acute and
chronic infections. However, mortality has remained high when an acute
bacterial infection induces sepsis with shock, metabolic acidosis, oliguria,
or hypoxemia. In fact, in the United States alone, there are at least
500,000 episodes of sepsis annually, and the resultant mortality rate
ranges from 30 to 50 percent, even with intensive medical care, including
antibiotics, intravenous fluids, nutrition, mechanical ventilation for
respiratory failure, and surgery when indicated to eradicate the source of
the infection. (Rangel Frausto ,et al 2003)
In the past 15 years several treatments designed to reduce the
mortality rate associated with sepsis have been unsuccessful, leading
some investigators to conclude that any adjunctive therapy is destined to
fail because once the clinical signs of severe sepsis are present,
irreversible organ injury has already occurred. At last, however, there has
been progress in finding an effective new therapy for sepsis. It is reported
the results of a large clinical trial in which recombinant human activated
protein C significantly reduced mortality in patients with severe sepsis.
(Bernard ,et aL 2001)
Activated protein C, a component of the natural anticoagulant
system, is a potent antithrombotic serine protease with substantial
antiinflammatory properties. What has the efficacy of this treatment
68

Chapter V
taught us about the pathogenesis of sepsis, and what are the strengths and
limitations of this important clinical trial. (Bernard ,et al 2001)
In the initial response to a localized infection, as in pneumonia or
an intraabdominal abscess, the release of endotoxins or exotoxins by a
bacterial infection induces tissue macrophages to generate inflammatory
cytokines, including tumor necrosis factor α, interleukin-1β, and
interleukin-8 Although these early-response cytokines play an important
part in host defense by attracting activated neutrophils to the site of
infection, the entry of these cytokines and bacterial products into the
systemic circulation can bring about widespread microvascular injury,
leading to multiorgan failure. Most prior clinical trials evaluated
pharmacologic agents designed to attenuate these early inflammatory
events in sepsis, including glucocorticoids and drugs designed to
neutralize endotoxin, tumor necrosis factor α, or interleukin-1β. None of
these treatments were effective, perhaps in part because the importance of
the coagulation cascade in sepsis was not recognized.(Daniei 2011)
Several procoagulant mechanisms have been associated with
decreased survival among patients with sepsis. Patients who died had
elevated levels of plasminogen activator inhibitor type 1, an inhibitor of
normal fibrinolysis, as well as decreased levels of the natural circulating
anticoagulants antithrombin III and protein C. Endotoxins and early-
response cytokines generate an environment that favors coagulation by
means of a number of mechanisms, including activation of the extrinsic
coagulation pathway through the expression of tissue factor. There are
also important molecular links between the procoagulant and
inflammatory mechanisms in the pathogenesis of organ failure in patients
with sepsis. Furthermore, some components of the coagulation system
have the capacity to be inflammatory. For example, the generation of
69

Chapter V
thrombin can activate receptors on platelets and the vascular endothelium
that can lead to inflammation and tissue injury. Thus, there are several
synergistic pathways by which inflammatory and procoagulant
mechanisms can initiate and perpetuate organ injury in patients with
sepsis. (Andere 2008)
Drotrecogin alfa: Drug information
Fig 6 (Proposed action of Activated protein C in modulating the
Systemic Inflammatory,Procoagulant and Fibrinolytic Host Responses to
infection)
70

Chapter V
There are a number of compelling reasons why activated protein C
might be an effective therapy in patients with sepsis. First, most patients
with severe sepsis have diminished levels of activated protein C, in part
because the inflammatory cytokines generated in sepsis down-regulate
thrombomodulin and the endothelial-cell protein C receptor, components
of the coagulation system that are necessary for the conversion of inactive
protein C to activated protein C. Second, activated protein C inhibits
activated factors V and VIII, thereby decreasing the formation of
thrombin. Third, activated protein C stimulates fibrinolysis by reducing
the concentration of plasminogen-activator inhibitor type 1. Fourth, the
administration of activated protein C to baboons with gram-negative
sepsis reverses the procoagulant and inflammatory effects of sepsis and
increases survival. Finally, there is recent evidence that treatment with
protein C may improve clinical outcomes in patients with severe
meningococcemia.(Grubers,et al 2012)
In the study by Bernard et al2001., the administration of activated
protein C was associated with a reduction in plasma d-dimer levels,
evidence that the procoagulant effects of sepsis were diminished by this
therapy. There was also a reduction in the serum levels of interleukin-6,
indicating that treatment attenuated the inflammatory cascade. This result
agrees well with the evidence that activated protein C reduces the
production of tumor necrosis factor α by monocytes by inhibiting the
coupling of endotoxin and CD14, without affecting the antimicrobial
properties of monocytes. Moreover, activated protein C reduces
interactions between neutrophils and endothelial cells and decreases
tissue ischemia, in part by reducing the endothelial expression of E-
selectin. Thus, several mechanisms may account for the combined
71

Chapter V
anticoagulant and antiinflammatory effects of this new drug .(Joseph
2009)
From a clinical perspective, the study by Bernard et al. was well
conducted. It was a large, randomized, double-blind international study of
1690 patients. The base-line characteristics and risk factors of the patients
in the placebo group and the group assigned to receive activated protein C
were well matched. Also, protein C deficiency was detected in nearly 90
percent of the patients in whom levels were measured. The absolute
reduction in the 28-day mortality rate was 6.1 percent (the rate in the
placebo group was 30.8 percent, as compared with a rate of 24.7 percent
in the group assigned to receive activated protein C), and the relative risk
of death in the treated group was reduced by nearly 20 percent. The
treatment was effective regardless of age, severity of illness, the number
of dysfunctional organs or systems, the site of infection (pulmonary or
extrapulmonary), and the type of infecting organism (gram-positive,
gram-negative, or mixed). It is also remarkable that treatment with
activated protein C reduced mortality even though, at the time of initial
treatment, more than 70 percent of the patients were in shock and 75
percent were already receiving mechanical ventilation. It is likely that the
majority of the patients who were receiving mechanical ventilation
already had acute lung injury, the most important cause of acute
respiratory failure in patients with sepsis.(ZhuQing ,et al 2011)
Since activated protein C has anticoagulant properties, did the
administration of this therapy increase the risk of bleeding? The incidence
of serious bleeding was 3.5 percent in the treated patients and 2.0 percent
in the patients in the placebo group, a difference that almost reached
statistical significance (P=0.06). Overall, the increased risk of bleeding
72

Chapter V
was small and the blood-transfusion requirements were similar in the two
groups.(Angus ,et al 2012)
Nevertheless, it should be noted that by design, we exclude patients
with a higher risk of bleeding, such as patients with chronic liver disease,
those with chronic renal failure who were dependent on dialysis, those
who had undergone recent surgery, organ-transplant recipients, patients
with thrombocytopenia (defined as a platelet count of less than 30,000 per
cubic millimeter), and those who had taken acetylsalicylic acid at a dose
of more than 650 mg per day within three days before the study. Many
patients with severe sepsis meet one or more of these criteria. Also,
patients who were younger than 18 years of age were not included in the
trial. Therefore, physicians who use activated protein C need to be alert to
the possibility of bleeding, and further studies will be needed to assess the
safety of activated protein C in these groups of patients.(Vincet ,et al
2011)
Activated protein C should be given to patients who meet all the
inclusion criteria, including evidence of end-organ dysfunction with
shock, acidosis, oliguria, or hypoxemia. The drug should not be given to
patients with clinical signs of mild-to-moderate sepsis who do not have
evidence of end-organ injury, unless a future trial shows a clear benefit in
these patients. Furthermore, the risks and benefits of the agent must be
studied in patients at a higher risk of bleeding, in children, and in
immunosuppressed patients, especially those with thrombocytopenia or
neutropenia. Because the cost of this new therapy will be substantial,
ways to make this drug affordable throughout the world should be
identified.(Bernard ,et al 2001)
73

Chapter V
Other trials of agents designed to inhibit coagulation and
inflammation are under way, raising hope that there may someday be
additional options for the treatment of sepsis. However, in this landmark
trial, Bernard et al. have provided evidence that mortality can be reduced
among patients with severe sepsis through the use of a new therapy that
inhibits both the procoagulant and the inflammatory cascades.(Lattere,et
al 2007)
Recombinant human activated protein C, an anticoagulant is the
first anti-inflammatory agent that has proved effective in the treatment of
sepsis. In patients with sepsis, the administration of activated protein C in
a dose of 24Mic/kg/hr resulted in a 19.4 percent reduction in the relative
risk of death and an absolute risk reduction of 6.1 percent. (Bernard ,et al
2001).
Dosing: Adult
Severe sepsis: I.V.: 24 mcg/kg/hour for a total of 96 hours; stop infusion
immediately if clinically-important bleeding is identified. Note: Use
actual body weight for dosing.There is no specific adjustment
recomended in patients with renal impairment.(Bernard ,et al 2001).
Administration
Infuse separately from all other medications. Only dextrose,
normal saline, dextrose/saline combinations, and lactated Ringer's
solution may be infused through the same line. May administer via
infusion pump. Administration of prepared solution must be completed
within 12 hours of preparation. Suspend administration for 2 hours prior
to invasive procedures or other procedure with significant bleeding risk;
may continue treatment immediately following uncomplicated,
74

Chapter V
minimally-invasive procedures, but delay for 12 hours after major
invasive procedures/surgery.(Levy ,et al 2005).
Compatibility
Stable in NS(normal saline); only NS, dextrose, LR(lactate
Ringer), or dextrose/saline mixtures may Activated protein C inactivates
factors Va and VIIIa, thereby preventing the generation of thrombin.
(Matthay 2001).
The efficacy of an anticoagulant agent in patients with sepsis has
been attributed to feedback between the coagulation system and the
inflammatory cascade . Inhibition of thrombin generation by activated
protein C decreases inflammation by inhibiting platelet activation,
neutrophil recruitment, and mast-cell degranulation. Activated protein C
has direct anti-inflammatory properties, including blocking of the
production of cytokines by monocytes and blocking cell adhesion. Also,
activated protein C has antiapoptotic actions that may contribute to its
efficacy (Joyce 2001).
The debate regarding the appropriate use of activated protein C, as
well as its potential adverse effects, particularly bleeding, has been
discussed in many articles. A major risk associated with activated protein
C is hemorrhage; in a study of activated protein C, 3.5 percent of patients
had serious bleeding (intracranial hemorrhage, a life-threatening bleeding
episode, or a requirement for 3 or more units of blood), as compared with
2 percent of patients who received placebo (P < 0.06). (Warren ,et al
2002).
The use of activated protein C after the trial, 13 of 520 patients (2.5
percent) had intracranial hemorrhage . Caution is advised in the use of
activated protein C in patients with an international normalized ratio
75

Chapter V
greater than 3.0 or a platelet count of less than 30,000 per cubic
millimeter. Currently, activated protein C is approved only for use in
patients with sepsis who have the most severe organ compromise and the
highest likelihood of death.(Manns ,et al 2002).
Use of activated protein C is restricted in many hospitals to the
more seriously ill patients who meet the criteria for sepsis specified by
the Acute Physiology and Chronic Health Evaluation (APACHE II)
scoring system (Siegel 2002).
Activated protein C is compatible with Cisatracurium,
fluconazole, nitroglycerin, potassium chloride,
vasopressin.,Incompatible with Amiodarone, ciprofloxacin,
cyclosporine, gentamicin, imipenem/cilastatin sodium, insulin (regular),
levofloxacin, magnesium sulfate, metronidazole, midazolam,
nitroprusside, norepinephrine, piperacillin/tazobactam,
ticarcillin/clavulanate, tobramycin, vancomycin.Variable compatible
with Albumin, ampicillin/sulbactam sodium, ceftazidime, ceftriaxone,
clindamycin, dobutamine, dopamine, epinephrine, fosphenytoin,
furosemide, heparin, potassium phosphate, ranitidine.(sweeny ,et al 2009)
Use
Reduction of mortality from severe sepsis (associated with organ
dysfunction) in adults at high risk of death (e.g., APACHE II score ≥25).
.Use – Unlabeled in Purpura fulminans (Bachli ,et al 2001).
Adverse Reactions Significant
As with all drugs which may affect hemostasis, bleeding is the major
adverse effect associated with drotrecogin alfa. Hemorrhage may occur at
virtually any site. Risk is dependent on multiple variables, including the
76

Chapter V
dosage administered, concurrent use of multiple agents which alter
hemostasis, and patient predisposition. (Bachli ,et al 2001)
More than10% of complications are in the form of Dermatological
Bruising and Gastrointestinal bleeding ,1% to 10%: Bleeding (serious
2.4% during infusion vs. 3.5% during 28-day study period; individual
events listed as <1%). ,<1% (Limited to important or life-threatening):
Gastrointestinal hemorrhage, genitourinary bleeding, immune reaction
(antibody production), intracranial hemorrhage (0.2%; frequencies up to
2% noted in a previous trial without placebo control), intrathoracic
hemorrhage, retroperitoneal bleeding, skin/soft tissue bleeding.(Manns,et
al 2002)
Contraindications
Hypersensitivity to drotrecogin alfa or any component of the
formulation.,active internal bleeding.,recent hemorrhagic stroke (within 3
months).,severe head trauma (within 2 months). ,recent intracranial or
intraspinal surgery (within 2 months). intracranial neoplasm or mass
lesion. ,evidence of cerebral herniation.,presence of an epidural
catheter.,trauma with an increased risk of life-threatening bleeding.
(Sweeny ,et al 2009)
Warnings/Precautions
Bleeding: Increases risk of bleeding; careful evaluation of risks and
benefit is required prior to initiation. Bleeding risk is increased in patients
receiving concurrent therapeutic heparin, oral anticoagulants,
glycoprotein IIb/IIIa antagonists, platelet aggregation inhibitors, or
aspirin at a dosage of >650 mg/day (within 7 days). In addition, an
increased bleeding risk is associated with prolonged INR (>3),
gastrointestinal bleeding (within 6 weeks), decreased platelet count
77

Chapter V
(<30,000/mm3), thrombolytic therapy (within 3 days), recent ischemic
stroke (within 3 months), intracranial AV malformation or aneurysm,
known bleeding diathesis, severe hepatic disease (chronic), or other
condition where bleeding is a significant hazard or difficult to manage
due to its location. Discontinue if significant bleeding occurs (may
consider continued use after stabilization). Suspend administration for 2
hours prior to invasive procedures or other procedure with significant
bleeding risk; may continue treatment immediately following
uncomplicated, minimally-invasive procedures, but delay for 12 hours
after major invasive procedures/surgery. During treatment, aPTT cannot
be used to assess coagulopathy (PT/INR not affected. (Sweeney ,et al
2009).
Disease-related concerns:
Efficacy not established in adult patients at a low risk of death
(APACHE II score <25). Patients with pre-existing nonsepsis-related
medical conditions with a poor prognosis (anticipated survival <28 days),
patients with acute pancreatitis (no established source of infection), HIV-
infected patients with a CD4 count ≤50 cells/mm3, chronic dialysis
patients, pre-existing hypercoagulable conditions, and patients who had
received bone marrow, liver, lung, pancreas, or small bowel transplants
were excluded from the clinical trial which established benefit. In
addition, patients weighing >135 kg were not evaluated.( Hotchkiss ,et
al 2007)
Safety and efficacy have not been established in
children.Metabolism and transport of Recombinant human activated
protein c is not known.(Grubers,et al 2012)
78

Chapter V
Drug Interactions:
Anticoagulants, May enhance the anticoagulant effect of other
Anticoagulants,Antiplatelet Agents: May enhance the adverse/toxic effect
of Drotrecogin Alfa (Activated) and bleeding may occur. Management
When possible, avoid use of drotrecogin within 7 days of use of any
IIb/IIIa antagonists, higher dose aspirin (more than 650 mg/day), or use
of other antiplatelet agents.,Antithrombin: May enhance the adverse/toxic
effect of Drotrecogin Alfa (Activated). Bleeding may occur.
Management: When possible, avoid use of drotrecogin in patients who
have recently received treatment with antithrombin.Collagenase
(Systemic): Anticoagulants may enhance the adverse/toxic effect of
Collagenase (Systemic). Specifically, the risk of injection site bruising
and/or bleeding may be increased. Fondaparinux: Drotrecogin Alfa
(Activated) may enhance the adverse/toxic effect of Fondaparinux.
Bleeding may occur. Management: Monitor for increased risk of bleeding
during concomitant therapy. Consider avoiding concomitant use, when
possible.Heparin: May enhance the adverse/toxic effect of Drotrecogin
Alfa (Activated). Bleeding may occur. Management: Potential benefits of
therapeutic heparin doses should be weighed against an increased risk of
bleeding in patients who receive drotrecogin alfa. In patients receiving
prophylactic heparin doses consider continuing this during
drotrecogin.Heparin (Low Molecular Weight): May enhance the
adverse/toxic effect of Drotrecogin Alfa (Activated). Bleeding may occur.
Management: Potential benefits of therapeutic doses of LMW heparins
should be weighed against an increased risk of bleeding in patients who
receive drotrecogin alfa. In patients receiving prophylactic LMW heparin
doses consider continuing this during
drotrecogin.Herbs(Anticoagulant/Antiplatelet Properties) (eg, Alfalfa,
Anise, Bilberry): May enhance the adverse/toxic effect of Anticoagulants.
79

Chapter V
Bleeding may occur.Ibritumomab: Anticoagulants may enhance the
adverse/toxic effect of Ibritumomab. Both agents may contribute to an
increased risk of bleeding. Nonsteroidal Anti-Inflammatory Agents: May
enhance the anticoagulant effect of Anticoagulants.Pentosan Polysulfate
Sodium: May enhance the anticoagulant effect of
Anticoagulants.Prostacyclin Analogues: May enhance the adverse/toxic
effect of Anticoagulants. Specifically, the antiplatelet effects of these
agents may lead to an increased risk of bleeding with the
combination.Rivaroxaban: Anticoagulants may enhance the anticoagulant
effect of Rivaroxaban. Salicylates: May enhance the adverse/toxic effect
of Drotrecogin Alfa (Activated). Bleeding may occur. Management:
Weigh potential benefits of drotrecogin against increased bleeding risk in
patients who have received platelet inhibitors including aspirin (over 650
mg daily within 1 week). Monitor for bleeding and stop infusion if
clinically important bleeding occurs.Thrombolytic Agents: May enhance
the adverse/toxic effect of Drotrecogin Alfa (Activated). Bleeding may
occur. Management: Whenever possible, avoid use of drotrecogin within
3 days of a thrombolytic agent.Vitamin K Antagonists (eg, warfarin):
May enhance the adverse/toxic effect of Drotrecogin Alfa (Activated).
Bleeding may occur. Management: Weigh potential benefits of
drotrecogin against increased bleeding risk in patients who have received
oral anticoagulants within 1 week or have INR 3 or greater. Monitor for
bleeding and immediately stop infusion if clinically important bleeding
occurs.(Bernard ,et al 2001)
Ethanol/Nutrition/Herb Interactions:
Herb/Nutraceutical: Recent use/intake of herbs with anticoagulant or
antiplatelet activity (including cat's claw, feverfew, garlic, ginkgo,
80

Chapter V
ginseng, and horse chestnut seed) may increase the risk of bleeding.
(Gupta 2011)
Pregnancy Implications:
Animal reproduction studies have not been conducted. No adverse
effects were seen in a limited number of case reports using drotrecogin
alfa in pregnant women .Excretion in breast milk unknown so not
recommended in lactated women.(Eppert, 2011).
Mechanism of Action
Inhibits factors Va and VIIIa, limiting thrombotic effects.
Additional in vitro data suggest inhibition of plasminogen activator
inhibitor-1 (PAF-1) resulting in profibrinolytic activity, inhibition of
macrophage production of tumor necrosis factor, blocking of leukocyte
adhesion, and limitation of thrombin-induced inflammatory responses.
Relative contribution of effects on the reduction of mortality from sepsis
is not completely understood. (Barton ,et al 2004)
Pharmacodynamics/Kinetics:
Duration: Plasma nondetectable within 2 hours of
discontinuation.Metabolism: Inactivated by endogenous plasma protease
inhibitors; mean clearance: 40 L/hour; increased with severe sepsis
(~50%) .Half-life elimination: 1.6 hours.(Siege 2002)
81

Summary
SummaryThe word sepsis is derived from the Greek word sepein, meaning
to putrefy or make rotten. In the past, physicians disagreed on definitions
for sepsis, septicemia, and septic shock, making clinical diagnosis,
research, and communication difficult. Then in 1992, the American
College of Chest Physicians and the Society of Critical Care Medicine
established some common ground.(Rangel,et al 2001)
Sepsis is defined as a complex activation of the immune system
with a documented infection, Systemic inflammatory response syndrome
(SIRS) is a complex activation of the immune system regardless of
etiology, infection, trauma, burns, or a sterile inflammatory process,
severe sepsis is sepsis plus organ dysfunction, while septic shock is
defined as sepsis plus unexplained acute circulatory collapse with organ
dysfunction, hypotension, and tissue hypo perfusion.(Levy,et al 2001)
Sepsis is associated with increased hospital and ICU stays,
expensive antimicrobial therapies, and prolonged duration of mechanical
ventilation. As such, the economic impact of sepsis is considerable.
(Vincet,et al 2002)
Sepsis is clearly associated with high morbidity and mortality.
Importantly, the prognosis of septic patients is influenced not only by the
severity of infection, but also by the previous health status and the host
response. Diagnosis of sepsis affects not only immediate mortality, but
has an effect on longer-term death rates as well.(Lyne 2003)
82

Summary
Polymicrobial diseases, caused by combinations of viruses,
bacteria, fungi, and parasites, are being recognized with increasing
frequency. In these infections, the presence of one micro-organism
generates a niche for other pathogenic micro-organisms to colonize; one
micro-organism predisposes the host to colonization by other
microorganisms, or two or more non-pathogenic micro-organisms
together cause disease.(Angus,et al2004)
In the last half of the 20th century, the use of antibiotics for the
treatment of bacterial infections transformed the practice of medicine,
resulting in sharp reductions in morbidity and mortality from acute and
chronic infections. However, mortality has remained high when an acute
bacterial infection induces sepsis with shock, metabolic acidosis, oliguria,
or hypoxemia. In fact, in the United States alone, there are at least
500,000 episodes of sepsis annually, and the resultant mortality rate
ranges from 30 to 50 percent, even with intensive medical care, including
antibiotics, intravenous fluids, nutrition, mechanical ventilation for
respiratory failure, and surgery when indicated to eradicate the source of
the infection. (Rangel ,et al 2003)
In the past 15 years several treatments designed to reduce the
mortality rate associated with sepsis have been unsuccessful, leading
some investigators to conclude that any adjunctive therapy is destined to
fail because once the clinical signs of severe sepsis are present,
irreversible organ injury has already occurred. At last, however, there has
been progress in finding an effective new therapy for sepsis. It is reported
the results of a large clinical trial in which recombinant human activated
protein C significantly reduced mortality in patients with severe sepsis.
(Bernard ,et aL 2001)
83

Summary
In the study by Bernard et al 2001., the administration of activated
protein C was associated with a reduction in plasma d-dimer levels,
evidence that the procoagulant effects of sepsis were diminished by this
therapy. There was also a reduction in the serum levels of interleukin-6,
indicating that treatment attenuated the inflammatory cascade. This result
agrees well with the evidence that activated protein C reduces the
production of tumor necrosis factor α by monocytes by inhibiting the
coupling of endotoxin and CD14, without affecting the antimicrobial
properties of monocytes. Moreover, activated protein C reduces
interactions between neutrophils and endothelial cells and decreases
tissue ischemia, in part by reducing the endothelial expression of E-
selectin. Thus, several mechanisms may account for the combined
anticoagulant and antiinflammatory effects of this new drug.(Joseph
2009)
In the last half of the 20th century, the use of antibiotics for the
treatment of bacterial infections transformed the practice of medicine,
resulting in sharp reductions in morbidity and mortality from acute and
chronic infections. However, mortality has remained high when an acute
bacterial infection induces sepsis with shock, metabolic acidosis, oliguria,
or hypoxemia. In fact, in the United States alone, there are at least
500,000 episodes of sepsis annually, and the resultant mortality rate
ranges from 30 to 50 percent, even with intensive medical care, including
antibiotics, intravenous fluids, nutrition, mechanical ventilation for
respiratory failure, and surgery when indicated to eradicate the source of
the infection. (Rangel Frausto ,et al 2003)
Clinical perspective, the study by Bernard et al. was well
conducted. It was a large, randomized, double-blind international study of
1690 patients. The base-line characteristics and risk factors of the patients
84

Summary
in the placebo group and the group assigned to receive activated protein C
were well matched. Also, protein C deficiency was detected in nearly 90
percent of the patients in whom levels were measured. The absolute
reduction in the 28-day mortality rate was 6.1 percent (the rate in the
placebo group was 30.8 percent, as compared with a rate of 24.7 percent
in the group assigned to receive activated protein C), and the relative risk
of death in the treated group was reduced by nearly 20 percent. The
treatment was effective regardless of age, severity of illness, the number
of dysfunctional organs or systems, the site of infection (pulmonary or
extrapulmonary), and the type of infecting organism (gram-positive,
gram-negative, or mixed). It is also remarkable that treatment with
activated protein C reduced mortality even though, at the time of initial
treatment, more than 70 percent of the patients were in shock and 75
percent were already receiving mechanical ventilation. It is likely that the
majority of the patients who were receiving mechanical ventilation
already had acute lung injury, the most important cause of acute
respiratory failure in patients with sepsis.(ZhuQing ,et al 2011)
On the basis of the results of this trial, activated protein C should
be given to patients who meet all the inclusion criteria, including
evidence of end-organ dysfunction with shock, acidosis, oliguria, or
hypoxemia. The drug should not be given to patients with clinical signs
of mild-to-moderate sepsis who do not have evidence of end-organ
injury, unless a future trial shows a clear benefit in these patients.
Furthermore, the risks and benefits of the agent must be studied in
patients at a higher risk of bleeding, in children, and in
immunosuppressed patients, especially those with thrombocytopenia or
neutropenia. Because the cost of this new therapy will be substantial,
85

Summary
ways to make this drug affordable throughout the world should be
identified.(Bernard ,et al 2001)
Use of activated protein C is restricted in many hospitals to the
more seriously ill patients who meet the criteria for sepsis specified by
the Acute Physiology and Chronic Health Evaluation (APACHE II)
scoring system (Siegel 2002).
86

References
ReferencesAcute respiratory distress syndrome network. Ventilation with lower tidal
volumes as compared with traditional tidal volumes for acute lung
injury and acute respiratory distress syndrome N Engl J Med 2000;
342:1301-1308.
Adrie C, Alberti C, Chaix-Couturier C, Azoulay E, Lassence A, Cohen Y,
Meshaka P, Cheval C, Thuong M, Troché G, Garrouste-Orgeas
M, Timsit J-F. Epidemiology and economic evaluation of severe
sepsis in France: age, severity, infection site, and place of
acquisition (community, hospital, or intensive care unit) as
determinant of workload and cost. Journal of Critical Care 2005;
20: 46-58.
Aird WC. The role of the endothelium in severe sepsis and multiple organ
dysfunction syndrome. Blood 2003; 101:3765.
Alberti C, Brun-Buisson C, Burchardi H, et al. Epidemiology of sepsis and
infection in ICU patients from an international multi-
centre cohort study. Intensive Care Med 2002; 28:108-21.
[Erratum, Intensive Care Med 2002;28:525-6.
Alberti C, Brun-Buisson C, Burchardi H, et al: Epidemiology of sepsis and
infection in ICU patients from an international multicentre cohort
study. Intensive Care Med 2002; 28:108-121
Ali M. Elbashier, Abdul G. Malik Anil P. Blood Stream Infections: Micro-
Organisms, Risk Factorsand Mortality Rate In Qatif Central
Hospital 1998.
Aline Pâmela Vieira de Oliveira, Cristina Hueb Barata, Eddie Fernando
Candido Murta and Beatriz Martins. Tavares-Murta1
Comparative study of survivor and nonsurvivor sepsispatients in a
university hospital 2008.
87

References
Angus DC, Linde-Zwirble WT, Lidecker J, et al.Epidemiology of severe
sepsis in the United States: analysis of incidence, outcome and
associated costs of care. Crit Care Med 2001; 29 (7):1303–10.
Angus DC, Linde-Zwirble WT, Lidecker J, et al.Epidemiology of severe
sepsis in the United States: analysis of incidence, outcome and
associated costs ofcare. Crit Care Med 2001; 29 (7):1303–10.
Angus DC, Wax RS. Epidemiology of sepsis: an update. Crit Care Med 2001;
29 (7):S109–16.
Annane D, Bellisant E, Cavaillon JR. Septic shock. Lancet 2005; 365:63–78.
Annane D, Sebille V, Charpentier C, et al.Effect of treatment with low doses
of hydrocortisone and fludrocortisone on mortality in patients with
septic shock. JAMA 2002; 288:862-871.
Annane D, Sebille V, Troche G, et al. A 3-level prognostic classification in
septic shock based on cortisol levels and cortisol response to
corticotropin. JAMA. 2000; 283:1038-1045.
Arbour NC, Lorenz E, Schutte BC, et al.TLR4 mutations are associated with
endotoxin hyporesponsiveness in humans. Nat Genet 2000;
25:187-91.
Arraes SM, Freitas MS, Silva SV, Paula Neto H, Alves-Filho JC, Martins
MA, Basile-Filho A, Tavares-Murta BM, Barja-Fidalgo C,
Cunha FQ. Impaired neutrophil chemotaxis in sepsis associates
with GRK expression and inhibition of actin assembly and tyrosine
phosphorylation. Blood 2006; 108: 2906-2913.
Assicot M, Gendrel D, Carsin H, et al. High serum procalcitonin concentration
in patients with sepsis and infection. Lancet 1993; 341:515-518.
Ayala A, Chung CS, Song GY, Chaudry IH. IL-10 mediation of activation-
induced TH1 cell apoptosis and lymphoid dysfunction in
polymicrobial sepsis Cytokine 2001; 14,37-48.
88

References
Ayala A, Deol ZK, Lehman DL, Herdon CD, Chaudry IH. Polymicrobial
sepsis but not low-dose endotoxin infusion causes decreased
splenocyte IL-2/IFN- release while increasing IL-4/IL-10
production J. Surg. Res. 1994; 56,579-585.
Bakaletz LO. Otitis Media. In: Brogden KA, Guthmiller JM, eds.
Polymicrobial diseases. Washington, DC: ASM Press, 2002: 259–
98.
Banchereau J, Steinman RM. Dendritic cells and the control of immunity
Nature 1998; 392, 245-252.
Bellomo R, Champan M, Finfer S,Hickling K, Myburgh J. Low dose
dopamine in patients with early renal dysfunction: a placebo-
controlled randomized trial. Lancent 2000; 356:2139-2143.
BenoiˆT Ruot, Denis Breuille, Fabienne Rambourdin, Gerard Bayle, Pierre
Capitan, Christiane Obled. Synthesis rate of plasma albumin is a
good indicator of liver albumin synthesis in sepsis
Bernard GR, Vincent J-L, Laterre P-F, et al.Efficacy and safety of
recombinant human activated protein C for severe sepsis. N Engl J
Med 2001; 344:699-709.
Bodey GP, Bolivar R, Fainstein V: Infectious complications in leukemic
patients. Semin Hematol 1982; 19:193.
Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein
RM, Sibbald WJ. Definitions for sepsis and organ failure and
guidelines for the use of innovative therapies in sepsis. The
ACCP/SCCM Consensus Conference Committee. American
College of Chest Physicians/Society of Critical Care Medicine.
Chest. 1992 Jun; 101 (6):1644-55. PMID 1303622.
Bone RC, Fisher CJ, Clemmer TP, Slotman GJ, Metz CA, Balk RA. Sepsis
syndrome: A valid clinical entity. Crit Care Med 1989; 17:389-393
89

References
Bone RC. Immunologic dissonance: A continuing evolution in our
understanding of the systemic inflammatory response syndrome
(SIRS) and the multiple organ dysfunction syndrome (MODS).
Ann Intern Med 1996; 125:680.(up todate 2008)
Bone RC. Immunologic dissonance: A continuing evolution in our
understanding of the systemic inflammatory response syndrome
(SIRS) and the multiple organ dysfunction syndrome (MODS).
Ann Intern Med 1996; 125:680. (Q up to date 2008)
Bone RC. The pathogenesis of sepsis. Ann Intern Med 1991; 115:457. (Q up
todate 2008).
Borovikova LV, Ivanova S, Zhang M, et al. Vagus nerve stimulation
attenuates the systemic inflammatory response to endotoxin.
Nature 2000; 405:458.
Bouza E, Burilla A, Torres MV. Nosocomial pneumonia in the critical care
unit. In: Cunha BA, editor. Infectious disease in critical care
medicine.NewYork: Informa Healthcare; 2007; P 169–204.
Brealey D, Brand M, Hargreaves I, et al. Association between mitochondrial
dysfunction and severity and outcome of septic shock. Lancet
2002; 360:219. (Q up todate 2008)
Brennan, JM, Blair, JE, Hampole, C, et al. Radial artery pulse pressure
variation correlates with brachial artery peak velocity variation in
ventilated subjects when measured by internal medicine residents
using hand-carried ultrasound devices. Chest 2007; 131:1301.
Bridgen ML, Pattullo AL. Prevention and management of overwhelming
postsplenectomy infectiondan update. Crit Care Med 1999;
27:836–42.
Brower RG, Lanken PN, MacIntyre N, et al. Higher versus lower positive end
expiratory pressures in patients with the acute respiratory distress
syndrome. N Engl J Med 2004; 351:327-336.
90

References
Brownlee M. Biochemistry and molecular cell biology of diabetic
complications. Nature 44: 813-820, komar and clark 2008.
Brun-Buisson C, Doyon F, Carlet J, et al. Incidence, risk factors, and outcome
of severe sepsis and septic shock in adults. JAMA 1995; 247:968-
974
Brun-Buisson C, Doyon F, Carlet J, et al. Incidence, risk factors, and
outcome of severe sepsis and septic shock in adults: a multicenter
prospective study in intensive care units. JAMA 1995; 274:968. (Q
up to date 2008).
Brunkhorst FM, Engel C, Bloos F, et al. Intensive insulin therapy and
pentastarch resuscitation in severe sepsis. N Engl J Med 2008;
358:125.
Brunkhorst FM, Forycki ZF, Wagner J. Frühe Identifizierung der biliären
akuten Pancreatitis durch Procalcitonin-Immunreaktivität -
vorläufige Ergebnisse. Chir Gastroenterol 1995; 11 (Suppl. 2):42-
46
Carr ME. Diabetes mellitus :a hypercoaulable state . J Diabetes complications
2001; 15:44-45.
Carvalho AC, Freeman NJ. How coagulation defects alter outcome in sepsis.
Survival may depend on reversing procoagulant conditions. J Crit
Illness. 1994; 9:51-75.
Choi PT, Yip G, Quinonez LG, Cook DJ. Crystalloids vs. colloids in fluid
resuscitation: A systematic review. Crit Care Med 1999; 27:200.
Clec'h C, Fosse JP, Karoubi P, et al. Differential diagnostic value of
procalcitonin in surgical and medical patients with septic shock.
Crit Care Med 2006; 34:102.
Clinical importance of polymicrobial bacteremia.Diagn Microbiol Infect Dis.
1986; 5(3):185-96 (ISSN: 0732-8893)
91

References
Coopersmith CM, Stromberg PE, Dunne WM, et al. Inhibition of intestinal
epithelial apoptosis and survival in a murine model of pneumonia-
induced sepsis. JAMA 2002; 287:1716.
Crouser ED, Julian MW, Blaho DV, Pfeiffer DR. Endotoxin-induced
mitochondrial damage correlates with impaired respiratory activity.
Crit Care Med 2002; 30:276. (Q up todate 2008)
Cruz K, Dellinger RP.Diagnosis and source of sepsis: the utility of clinical
findings. In: Vincent CL, Carlet J, Opal SM, editors. The sepsis
test. Boston: Kluwer Academic Publishers; 2002; P 11–28
Cruz K, Dellinger RP. Diagnosis and source of sepsis: the utility of clinical
findings. In: Vincent CL, Carlet J, Opal SM, editors. The sepsis
test. Boston: Kluwer Academic Publishers; 2002; P 11–28.
Cunha BA. Clinical manifestations and antimicrobial therapy of methicillin
resistant Staphylococcus aureus (MRSA). Clin Microbiol Infect
2005; 11:33–42.
Cunha BA. Intravenous line infections. Crit Care Clin 1998; 339–46. SEPSIS
& SEPTIC SHOCK 331
Cunha BA. Severe community-acquired pneumonia in the critical care unit. In:
Cunha BA, editor. Infectious disease in critical care medicine. New
York: Informa Healthcare; 2007; P 157–68.
Cunha BA. Urosepsis in the CCU. In: Cunha BA, editor. Infectious diseases in
critical care medicine. 2nd edition. New York: Informa Healthcare;
2007.
Cunha BA. Urosepsisddiagnostic and therapeutic approach. Intern Med 1996;
17:85–93.
Cunha BA. Ventilator associated pneumonia: Monotherapy is optimal if
chosen wisely. Crit Care Med 2006; 10:e141–2.
92

References
Danai PA, Mannino DM, Moss M, Martin GS. The epidemiology of sepsis
among patients with cancer. Chest. 2006; 129:1432-1440 1303-
1310, 2001.
De Backer D, Creteur J, Preiser JC, et al. Microvascular blood flow is altered
in patients with sepsis. Am J Respir Crit Care Med 2002; 166:98.
(Q up to date 2008)
De Jonghe B, Sharshar T, Lefaucheur JP, et al. Paresis acquired in the
intensive care unit: a prospective multicenter study. JAMA 2002;
288:2859.
Deem S, Lee CM, Curtis JR. Acquired neuromuscular disorders in the
intensive care unit. Am J Respir Crit Care Med 2003; 168:735.
Dellinger RP et al, for the International Surviving Sepsis Campaign Guidelines
Committee: Surviving Sepsis Campaign: International guidelines
for management of severe sepsis and septic shock: 2008. Crit Care
Med 2008; 36:296–327. [PMID: 18158437]
Dellinger RP, Levy MM, Carlet, JM, et al. Surviving Sepsis Campaign:
International guidelines for management of severe sepsis and septic
shock: 2008. Crit Care Med 2008; 36:296.
Dellinger, RP, Levy, MM, Carlet, JM, et al.Surviving Sepsis Campaign:
International guidelines for management of severe sepsis and septic
shock: 2008. Crit Care Med 2008; 36:296.
Diagn Microbiol Infect Dis. 1986; 5(3):185-96 (ISSN: 0732-8893)
DiNubile MJ, Lipsky BA. Complicated infections of skin and skin structures:
when the infections is more than skin deep. J Antimicrob
Chemother 2004; 53:37–50.
DiNubile MJ, Lipsky BA. Complicated infections of skin and skin structures:
when the infections is more than skin deep. J Antimicrob
Chemother 2004; 53:37–50.
93

References
Doig CJ, Sutherland LR, Sandham JD, et al. Increased intestinal permeability
is associated with the development of multiple organ dysfunction
syndrome in critically ill ICU patients. Am J Respir Crit Care Med
1998; 158:444. (Q up to date 2008)
Dombrovskiy VY, Martin AA, Sunderram J, et al: Facing the challenge:
Decreasing case fatality rates in severe sepsis despite increasing
hospitalization. Crit Care Med 2005; 33:2555-2562
Dupont HL, Spink WW. Infections due to gram-negative organisms: an
analysis of 860 patients with bacteremia at the University of
Minnesota Medical Center, 1958-1966. Medicine (Baltimore)
48:307.nt HL, Spink WW 1969; Infections due to gram.
ECC Guidelines: Part 6: Advanced Cardiovascular Life Support: Section 6:
Pharmacology II: Agents to optimize cardiac output and blood
pressure. Circulation 2000; 102: I-129-I-135. Recent consensus
recommendations for the use of pressors and inotropes in
emergency cardiovascular care.
Echtenacher B, Freudenberg MA, Jack RS, Männel DN. Differences in
innate defense mechanisms in endotoxemia and polymicrobial
septic peritonitis Infect. Immun. 2001; 69,7271-7276.
Echtenacher B, Weigl K, Lehn N, Mannel DN. Tumor necrosis factor-
dependent adhesions as a major protective mechanism early in
septic peritonitis in mice. Infect Immun 2001; 69:3550-5.
Efron PA, Martins A, Minnich D, Tinsley K, Ungaro R, Bahjat FR,
Hotchkiss R, Clare-Salzler M, Moldawer LL. Characterization of
the systemic loss of dendritic cells in murine lymph nodes during
polymicrobial sepsis J. Immunol. 2004; 173, 3035-3043 by Society
for Leukocyte Biology.
Eisner MD Thompson T Hudson LD, et al. Efficacy of low tidal volume
ventilation in patient with different clinical risk factors for acute
94

References
lung injury and acute respiratory distress syndrome. Am J Respir
Crit Care Med 2001; 164:231-236.
Esmon CT. Inflammation and thrombosis. Mutual regulation by Protein C.
Immunologist. 1998; 6:84-89.
Esper AM, Moss M, Lewis CA, Nisbet R, Mannino DM, Martin GS. The role
of infection and comorbidity: Factors that influence disparities in
sepsis. Critical Care Medicine 2006; 34: 2576-2582.
Esper AM, Moss M, Lewis CA, Nisbet R, Mannino DM, Martin GS. The role
of infection and comorbidity: Factors that influence disparities in
sepsis. Critical Care Medicine 2006; 34: 2576-2582.
Fadok VA, Bratton DL, Rose DM, Pearson A, Ezekewitz RA, Henson PM. A
receptor for phosphatidylserine-specific clearance of apoptotic
cells. Nature 2000; 405:85- 90.
Fekety R. Guidelines for the diagnosis and management of Clostridium
difficile-associated diarrhea and colitis. American College of
Gastroenterology, Practice Parameters Committee. Am J
Gastroenterol 1997; 92:739. (Q up to date2008)
Finfer S, Bellomo R, Boyce N, et al.A comparison of albumin and saline for
fluid resuscitation in the intensive care unit. N Engl J Med 2004;
350:2247.
Fink MP. Bench-to-bedside review: cytopathic hypoxia. Crit Care 2002; 6:
491–499.
Fisher CJ Jr, Agosti JM, Opal SM, et al.Treatment of septic shock with tumor
necrosis factor receptors: Fc fusion protein. N Engl J Med 1996;
334:1697-1702.
Fishman JA, Rubin RH: Infection in organ-transplant recipients. N Engl J
Med 1998; 338:1741.
95

References
Fleshner M, Goehler LE, Schwartz BA, et al. Thermogenic and corticosterone
responses to intravenous cytokines (IL-1beta and TNF-alpha) are
attenuated by subdiaphragmatic vagotomy. J Neuroimmunol 1998;
86:134.
Fontes RA Jr, Ogilvie CM, Miclau T. Necrotizing soft tissue infections. J Am
Acad Orthop Surg 2000; 8:151–8.
Forsythe SM, Schmidt GA. Sodium bicarbonate for the treatment of lactic
acidosis. Chest 2000; 117:260. (Q up to date2008)
Francis JS, Doherty MC, Lopatin U, et al.Severe community-onset
pneumonia in healthy adults caused by methicillin-resistant
Staphylococcus aureus carrying the Panton-Valentine leukocidin
genes. Clin Infect Dis 2005; 40:100.
Fridkin SK, Hageman JC, Morrison M, et al. Methicillin-resistant
Staphylococcus aureus disease in three communities. N Engl J
Med 2005; 352:1436.
Friedman G, Silva E, Vincent JL. Has the mortality of septic shock changed
with time? Crit Care Med 1998; 26:2078-2086.
Friedman G, Silva E, Vincent JL.Has the mortality of septic shock changed
with time? Crit Care Med 1998; 26:2078-2086
Friedman G, Silva E, Vincent JL. Has the mortality of septic shock changed
withtime ?Crit Care Med 1998; 26:2078–2086.
Fukuzuka K, Edwards CK III, Clare- Salzler M, Copeland EM III, Moldawer
LL, Mozingo DW. Glucocorticoid-induced, caspase-dependent
organ apoptosis early after burn injury. Am J Physiol Regul Integr
Comp Physiol 2000; 278:R1005-R1018.
Gandhi GY, Nuttall GA, Abel MD, et al.Intensive intraoperative insulin
therapy versus conventional glucose management during cardiac
surgery: a randomized trial. Ann Intern Med. 2007; 146:233-243.
96

References
Gattinoni L, Brazzi L, Pelosi P, et al. A trial of goal-oriented hemodynamic
therapy in critically ill patients. N Engl J Med 1995; 333:1025. (Q
up to date 2008).
Gendrel D, Bohuon C. Procalcitonin, a marker of bacterial infection. Infection
1997; 25:133-134
Ghosh S, Latimer RD, Gray BM, et al. Endotoxin-induced organ injury. Crit
Care Med 1993; 21:S19. (Q up to date 2008)
Ghosh, S, Latimer, RD, Gray, BM, et al. Endotoxin-induced organ injury. Crit
Care Med 1993; 21:S19. (Q up to date 2008)
Ghosh, S, Latimer, RD, Gray, BM, et al. Endotoxin-induced organ injury. Crit
Care Med 1993; 21:S19. (Q up to date2008)
Gibot S, Cravoisy A, Kolopp-Sarda MN, et al. Time-course of sTREM
(soluble triggering receptor expressed on myeloid cells)-1,
procalcitonin, and C-reactive protein plasma concentrations during
sepsis. Crit Care Med 2005; 33:792.
Gibot S, Kolopp-Sarda MN, Bene MC, et al. Plasma level of a triggering
receptor expressed on myeloid cells-1: its diagnostic accuracy in
patients with suspected sepsis. Ann Intern Med 2004; 141:9.
Gibot S, Le Renard PE, Bollaert PE, et al.Surface triggering receptor
expressed on myeloid cells 1 expression patterns in septic shock.
Intensive Care Med 2005; 31:594.
Gill MV, Cunha BA. IV line sepsis. In: Cunha BA, editor. Infectious diseases
in critical care medicine. New York: Marcel Dekker; 1998. p. 57–
65.
Gogos CA, Drosou E, Bassaris HP, Skoutelis A. Pro- versus anti-
inflammatory cytokine profile in patients with severe sepsis: a
marker for prognosis and future therapeutic options. J Infect Dis
2000; 181:176- 80.
97

References
Green DR, Beere HM. Apoptosis: gone but not forgotten. Nature 2000;
405:28-9.
Greg S. Martin, David M. Mannino, Stephanie Eaton, Marc Moss. The
Epidemiology of Sepsis in the United States from 1979 through
2000; The new england journal of med 348:16
Guery JC, Adorini L. Dendritic cells are the most efficient in presenting
endogenous naturally processed self-epitopes to class II-restricted
T cells J. Immunol. 1995; 154,536-544.
Gutierrez G, Palizas F, Doglio G, et al. Gastric intramucosal pH as a
therapeutic index of tissue oxygenation in critically ill patients.
Lancet 1992; 339:195. (Q up to date2008)
Hakim RM, Wingard RL, Parker RA. Effect of the dialysis membrane in the
treatment of patients with acute renal failure. N Engl J Med 1994;
331:1338. (Q up to date 2008)
Hardaway RM. A review of septic shock. Am Surg 2000; 66:22–9.
Harvey, S, Harrison, DA, Singer, M, et al. Assessment of the clinical
effectiveness of pulmonary artery catheters in management of
patients in intensive care (PAC-Man): a randomised controlled
trial. Lancet 2005; 366:472. (Q up to date2008)
Haslett C, Savill J. Why is apoptosis important to clinicians? BMJ 2001; 322:
1499-500.
Hassoun HT, Kone BC, Mercer DW, et al.Post-injury multiple organ failure:
The role of the gut. Shock 2001; 15:1. (Q up to date 2008)
Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized
controlled clinical trial of transfusion requirements in critical care.
N Engl J Med 1999; 340:409. (Q up to date2008)
98

References
Heidecke C-D, Hensler T, Weighardt H, et al.Selective defects of T
lymphocyte function in patients with lethal intraabdominal
infection. Am J Surg 1999; 178:288-92.
Hermans PE, Washington JE II. Polymicrobial bacteremia. Ann Inter Med
1970; 73:387.
Hermans PE, Washington JEII. Polymicrobial bacteremia. Ann Intern Med
1970; 73:387.
Heyland DK, Hopman W, Coo H, Tranmer J, McColl MA. Long-term health-
related quality of life in survivors of sepsis: Short Form-36: a valid
and reliable measure of health-related quality of life. Crit Care
Med 2000;28:3599-605
Hodgin UG, Sanford JP. Gram-negative bacteremia: an analysis of 100
patients. Am Med 39:952.negative organisms: an analysis opatients
with bacteremia at the University 1965.
Hollenberg SM, Ahrens TS, Annane D, et al. Practice parameters for
hemodynamic support of sepsis in adult patients: 2004 update. Crit
Care Med 2004; 32:1928.
Hollenberg, SM, Ahrens, TS, Annane, D, et al. Practice parameters for
hemodynamic support of sepsis in adult patients: 2004 update. Crit
Care Med 2004; 32:1928.
Hotchkiss RS, Swanson PE, Knudson CM, et al.Overexpression of Bcl-2 in
transgenic mice decreases apoptosis and improves survival in
sepsis. J Immunol 1999; 162: 4148-56.
Hotchkiss RS, Tinsley KW, Swanson PE, et al. Depletion of dendritic cells,
but not macrophages, in patients with sepsis. J Immunol 2002;
168:2493-500.
Hotchkiss RS, Tinsley KW, Swanson PE, et al. Sepsis-induced apoptosis
causes progressive profound depletion of B and CD4+ T
lymphocytes in humans. J Immunol 2001; 166:6952-63.
99

References
Hotchkiss RS, Tinsley KW, Swanson PE, et al. Sepsis-induced apoptosis
causes progressive profound depletion of B and CD4+ T
lymphocytes in humans. J Immunol 2001; 166:6952-63.
Hotchkiss RS, Tinsley KW, Swanson PE, Grayson MH, Osborne DF,
Wagner TH, Cobb JP, Coopersmith C, Karl IE. Depletion of
dendritic cells, but not macrophages, in patients with sepsis J.
Immunol. 2002; 168,2493-2500.
Hotchkiss RS, Tinsley KW, Swanson PE, Schmieg RE, Jr Hui JJ, Chang KC,
Osborne DF, Freeman BD, Cobb JP, Buchman TG, Karl IE.
Sepsis-induced apoptosis causes progressive profound depletion of
B and CD4+ T lymphocytes in humans J. Immunol. 2001;
166,6952-6963
Hoyert DL, Arias E, Smith BL, Murphy SL, Kochanek KD. Deaths: final data
for 1999. National vital statistics reports. Vol. 49. No. 8.
Hyattsville, Md.: National Center for Health Statistics, 2001.
(DHHS publication no. (PHS) 2001-1120 PRS 01-0573.)
Huber-Lang MS, Riedeman NC, Sarma JV, et al. Protection of innate
immunity by C5aR antagonist in septic mice. FASEB J 2002;
16:1567.
Hund E. Neurological complications of sepsis: critical illness polyneuropathy
and myopathy. J Neurol 2001; 248:929. 173.Hund, E. Neurological
complications of sepsis: critical illness polyneuropathy and
myopathy. J Neurol 2001; 248:929.
Hyattsville, Md.: National Center for Health Statistics, 2002. (Accessed March
25, 2003; at
http://www.cdc.gov/nchsabout/major/hdasd/nhdsdes.htm).
James M. O’Brien, Jr, MD, MSc,a Naeem A. Ali, MD,a Scott K. Aberegg,
MD, MPH,a Edward Abraham, MDb. Sepsis The American
Journal of Medicine 2007; 120, 1012-1022.
100

References
Journal of Leukocyte Biology. 2006; 79:473-481.) © 2006 by Society for
Leukocyte Biology.
Joyce DE, Gelbert L, Ciaccia A, DeHoff B, Grinnell BW. Gene expression
profile of antithrombotic protein C defines new mechanisms
modulating inflammation and apoptosis. J Biol Chem 2001;
276:11199-203.
Keane J, Gershon S, Wise RP, et al. Tuberculosis associated with infliximab, a
tumor necrosis factor a–neutralizing agent. N Engl J Med 2001;
345:1098-104.
Keane J: TNF-blocking agents and tuberculosis: new drugs illuminate an old
topic. Rheumatology (Oxford) 2005; 44:714.
Kiani D , Quinn EL, Burch KH , Madhavan T, Saravoltaz LD, Neblett TR.
The increasing importance of polymicrobial bacteremia. JAMA
1979; 242:1044.
Kiani D, Quinn EL, Butch KH, Madhavan T, Saravolatz LD, Neblett TR.
The increasing importance of polymicrobial bacteremia. JAMA
242:1044 1979; (Baltimore) 48:307.
Kreger BE, Craven DE, McCabe WR. Gram-negative bacteremia. IV. Re-
evaluation of clinical features and treatment in 612 patients. Am J
Med 1980b; 68:344.
Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before
initiation of effective antimicrobial therapy is the critical
determinant of survival in human septic shock. Crit Care Med
2006; 34:1589.
L. Aliaga, J.D. Mediavilla, J. Llosá, C. Miranda, M. Rosa-Fraile. Clinical
Significance of Polymicrobial Versus Monomicrobial Bacteremia
Involving Pseudomonas aeruginosaEur J Clin Microbiol Infect Dis
2000; 19 :871–874.
101

References
Lamping N, Dettmere R, Schröder NWJ, et al.LPS-binding protein protects
mice from septic shock caused by LPS or gram-negative bacteria. J
Clin Invest 1998; 101:2065. (Q up todate 2008)
Langouch L, Vanhorebebeek I, Vlasselaers D, et al. Intensive insulin therapy
protects the endothelium of critically ill patients. J Clin Invest
2005; 115:2277-2286
Larson AN, Mir M, Cogbill CL, Campana HA. Bacterial septicemia. Military
IVied 1974; 139:527.
Latifi SQ, O’Riordan MA, Levine AD. Interleukin-10 controls the onset of
irreversible septic shock Infect. Immun. 2002; 70,4441-4446.
Lazaron V, Barke RA. Gram-negative bacterial sepsis and the sepsis
syndrome. Urol Clin North Am 1999; 26:687–99.
Lederer JA, Rodrick ML, Mannick JA.The effects of injury on the adaptive
immune response. Shock 1999; 11:153-9.
Lederer JA, Rodrick ML, Mannick JA.The effects of injury on the adaptive
immune response. Shock 1999; 11:153-9.
Leibovici L, Paul M, Poznanski O, et al. Monotherapy versus beta-lactam-
aminoglycoside combination treatment for gram-negative
bacteremia: A prospective, observational study. Antimicrob Agents
Chemother 1997; 41:1127.
Levi M , van der Poll T, ten Cate H, et al: The cytokine-mediated imbalance
between coagulant and anticoagulant mechanisms in sepsis and
endotoxaemia. Eur J Clin Invest 1997; 27:3-9, Kidokoro A, Iba T,
Fkunaga M, et al: Alterations in coagulation and fibrinolysis
during sepsis. Shock 1996; 5:223-228).
Levy B, Bollaert PE. Clinical manifestations and complications of septic
shock. In: Dhainaut JG, Thijs LG, Park G, editors. Septic shock.
Philadelphia: WB Saunders; 2000; P 339–52. bacteremia. Ann
Intern Med 73:387.
102

References
Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J,
Opal SM, Vincent JL, Ramsay G; SCCM/ESICM/ ACCP/ ATS/
SIS. Crit Care Med. 2003 Apr; 31(4):12506.
Levy MM, Fink MP, Marshall JC, et al. 2001 SCCM/ ESICM/ ACCP/ ATS/
SIS International sepsis definitions Conference. Crit Care Med
2003
Levy MM, Fink MP, Marshall JC, et al. SCCM/ ESIEM/ ACCP/ ATS/ SI.
International Sepsis Definitions Conference. Critical Care
Medicine 2001; 31:1250,20
Liu D, Lu F, Qin G, et al. C1 inhibitor-mediated protection from sepsis. J
Immunol 2007; 179:3966. (Q up todate 2008)
Luce JM. Physicians should administer low-dose corticosteroids selectively to
septic patients until an ongoing trial is completed. Ann Intern Med.
2004; 141:70-72.
Luce, JM. Pathogenesis and management of septic shock. Chest 1987; 91:883.
(Q up to date 2008)
Luce, JM. Pathogenesis and management of septic shock. Chest 1987; 91:883.
(Q up to date2008)
Lutz MB, Schuler G. Immature, semi-mature and fully mature dendritic cells:
which signals induce tolerance or immunity? Trends Immunol.
2002; 23,445-449.
Lynn WA. Anti-endotoxin therapeutic options for the treatment of sepsis. J
Antimicrob Chemother 1998; 41:71-80
Mackowiak PA, Browne RH, Southern PM Jr, Smith JW. polymicrobial
sepsis: an analysis of 184 cases using log linear models. am J Med
Sci 1980; 280:73.
Magira EE, Zervakis D, Routsi C, et al.Community-acquired methicillin-
resistant Staphylococcus aureus carrying Panton-Valentine
103

References
leukocidin genes: a lethal cause of pneumonia in an adult
immunocompetent patient. Scand J Infect Dis 2007; 39:466–9.
Malhotra, A, Eikermann, M, Magder, S. Is brachial artery peak velocity
variation ready for prime time?. Chest 2007; 131:1279.
Manns BJ, Lee H, Doig CJ, Johnson D, Donaldson C. An economic
evaluation of activated protein C treatment for severe sepsis. N
Engl J Med 2002; 347:993-1000.
Marshall J, Lowry S. Evaluation of the adequacy of source control. In: Clinical
Trials for the treatment of sepsis, Sibbald, WJ, Vincent, JL (Eds),
Springer Verlag, Berlin, 1995, p. 329. (Q up to date2008)
Marshall JC, Watson RW. Apoptosis in the resolution of systemic
inflammation. In: Yearbook of Intensive Care and Emergency
Medicine, Vincent, JL (Eds), Springer-Verlag, Berlin, 1997; p.100.
(Q up todate 2008)
Marshall JC. Control of the source of sepsis. In: Vincent JL, Carlet J, Opal
SM, editors. The sepsis text. Boston: Kluwer Academic Publishers;
2002; P 525–38.
Martin GS Mannino DM, Eaton S, et al: The epidemiology of sepsis in the
United States from 1979 through 2000. N Engl J Med 2003;
348:1548-1564
Martin GS, Mannino DM, Eaton S, et al: The epidemiology of sepsis in the
United States from 1979 through 2000. N Engl J Med 2003;
348:1546–1554.
Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in
the United States from 1979 through 2000. The New England
Journal of Medicine 2003; 348: 1546-1554.
Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in
the United States from 1979 through 2000. N Engl J Med 2003;
348:1546–54.
104

References
Matthay MA. Severe sepsis a new treatment with both anticoagulant and anti-
inflammatory properties. N Engl J Med 2001; 344:759-62.
Mavrommatis AC, Theodoridis T, Orfanidou A, Roussos C, Christopoulou-
Kokkinou V, Zakynthinos S. Coagulation system and platelets are
fully activated in uncomplicated sepsis. Crit Care Med. 2000;
28:451–457. doi: 10.1097/00003246-200002000-00027. [PubMed]
{q coagulation abnormalities in critical ill patient 2006}
McCabe WR, Jackson GG. Gram-negative bacteremia. I. Etiology and
ecology. Arch Intern Med 1962; 110:847.
McDonald JR, Friedman ND, Stout JE, et al. Risk factors for ineffective
therapy in patients with bloodstream infection. Arch Intern Med
2005; 165:308.
Meisner M, Procalcitonin (PCT): Ein neuer, innovativer Infektionsparameter.
Biochemische und klinische Aspekte. Thieme, Stuttgart, 2000.
Michard, F, Boussat, S, Chemla, D, et al.Relation between respiratory
changes in arterial pulse pressure and fluid responsiveness in septic
patients with acute circulatory failure. Am J Respir Crit Care Med
2000; 162:134. (Q up to date2008)
Miller LG, Perdreau-Remington F, Rieg G, et al.Necrotizing fasciitis caused
by community - associated methicillin - resistant Staphylococcus
aureus in Los Angeles. N Engl J Med 2005; 352:1445.
Modlin RL, Brightbill HD, Godowski PJ. The toll of innate immunity on
microbial pathogens. N Engl J Med 1999; 340:1834-5.
Monnet, X, Rienzo, M, Osman, D, et al.Esophageal Doppler monitoring
predicts fluid responsiveness in critically ill ventilated patients.
Intensive Care Med 2005; 31:1195.
Movat HZ, Cybulsky MI, Colditz IG, et al. Acute inflammation in gram-
negative infection: Endotoxin, interleukin-1, tumor necrosis factor,
and neutrophils. Fed Proc 1987; 46:97.(q up to date 2008)
105

References
Neviere R, Mathieu D, Chagnon JL, et al. Skeletal muscle microvascular
blood flow and oxygen transport in patients with severe sepsis. Am
J Respir Crit Care Med 1996; 153:191. (Q up to date 2008)
Oberholzer A, Oberholzer C, Moldawer LL.Sepsis syndromes: understanding
the role of innate and acquired immunity. Shock 2001; 16:83-96.
Opal SM, Cross AS, Jhung JW, et al. Potential hazards of combination
immunotherapy in the treatment of experimental septic shock. J
Infect Dis 1996; 173:1415-21.
Opal SM, DePalo VA. Anti-inflammatory cytokines. Chest 2000; 117:1162-72.
Opal SM, DePalo VA. Anti-inflammatory cytokines. Chest 2000; 117:1162-72.
Ostermann ME, Keenan SP, Seiferling RA, Sibbald W. Delirium as a
Predictor of Mortality in Mechanically Ventilated Patients in the
Intensive Care Unit. Sedation in the intensive care unit. JAMA.
2000; 283:1451-1459.
Owa T, Hayashi S, Miyoshi M, et al.Successful treatment of necrotizing
fasciitis due to group A streptococcus with impending toxic shock
syndrome. Intern Med 2003; 42:914–5.
Padkin A, Goldfrad C, Brady AR, et al.Epidemiology of severe sepsis
occurring in the first 24 hours in intensive care units in England,
Wales and Northern Ireland. Crit Care Med 2003; 31 (9):2332–8.
Papadopoulos MC, Davies DC, Moss R et al.Pathophysiology of septic
encephalopathy: a review. Crit Care Med. 2000; 28 (8):3019-3024.
Paul M, Benuri-Silbiger I, Soares-Weiser K, Leibovici L. Beta lactam
monotherapy versus beta lactam-aminoglycoside combination
therapy for sepsis in immunocompetent patients: systematic review
and meta-analysis of randomised trials. BMJ 2004; 328:668.
106

References
Paul M, Silbiger I, Grozinsky S, et al. Beta lactam antibiotic monotherapy
versus beta lactam-aminoglycoside antibiotic combination therapy
for sepsis. Cochrane Database Syst Rev 2006; CD003344.
Pellegrini JD, De AK, Kodys K, Puyana JC, Furse RK, Miller-Graziano C.
Relationships between T lymphocyte apoptosis and anergy
following trauma. J Surg Res 2000; 88:200-6.
Piagnerelli M, Boudjeltia KZ, Brohee D, et al. Modifications of red blood cell
shape and glycoproteins membrane content in septic patients. Adv
Exp Med Biol 2003; 510:109. (Q up todate 2008)
Piagnerelli M, Boudjeltia KZ, Vanhaeverbeek M, Vincent JL. Red blood cell
rheology in sepsis. Intensive Care Med 2003; 29:1052.
Pinsky, MR, Matuschak, GM. Multiple organ failure: Failure of host defense
homeostasis. Crit Care Clin 1989; 5:199. (Q up todate 2008)
Poeze M, Solberg BC, Greve JW, Ramsay G. Monitoring global volume-
related hemodynamic or regional variables after initial
resuscitation: What is a better predictor of outcome in critically ill
septic patients?.Crit Care Med 2005; 33:2494.
Price S, Anning PB, Mitchell JA, Evans TW. Myocardial dysfunction in
sepsis: Mechanisms and therapeutic implications. Eur Heart J
1999; 20:715 (Q up to date 2008).
Pugin, J. Recognition of bacteria and bacterial products by host immune cells
in sepsis. In: Yearbook of Intensive Care and Emergency
Medicine, Vincent, JL (Eds), Springer-Verlag, Berlin, 1996; p.11.
(Q up todate 2008)
Quartin AA, Schein RMH, Kett DH, Peduzzi PN. Magnitude and duration of
the effect of sepsis on survival. JAMA 1997; 277:1058-10623
Raad I, Narro J, Khan A, Tarrand J, Vartivarian S, Bodey GP. Serious
complications of vascular catheter-related Staphylococcus aureus
107

References
bacteremia in cancer patients. Eur J Clin Microbiol Infect Dis
1992; 11(8):675-82
Rangel-frausto MS, Pittet D, Costigan M, et al. The natural history of the
systemic inflammatory response syndrome (SIRS) JAMA 1995;
273:117-123
Rangel-Frausto MS, Pittet D, Costigan M, Hwang T, Davis CS, Wenzel RP.
The natural history of the systemic inflammatory response
syndrome (SIRS). A prospective study. JAMA 1995; 273:117-
123 .
Reinhart K, Bloos F, Spies C. Vasoactive drug therapy in sepsis. In: Clinical
Trials for the treatment of sepsis, Sibbald, WJ, Vincent, JL (Eds),
Springer Verlag, Berlin, 1995; P. 207. (Q up to date2008).
Reith HB, Lehmkuhl R, Beier W, et al. Procalcitonin - ein prognostischer
Infektionsparameter bei der Peritonitis. Chir Gastroenterol 1995;
11 (Suppl.2):47-50
Reuter, DA, Bayerlein, J, Goepfert, MS, et al. Influence of tidal volume on left
ventricular stroke volume variation measured by pulse
contouranalysis in mechanically ventilated patients. Intensive Care
Med 2003; 29:476. (Q up to date2008)
Reyes WJ, Brimioulle S, Vincent JL. Septic shock without documented
infection: an uncommon entity with a high mortality. Intensive
Care Med 1999; 25: 1267-1270
Richard, C, Warszawski, J, Anguel, N, et al. Early use of the pulmonary artery
catheter and outcomes in patients with shock and acute respiratory
distress syndrome: a randomized controlled trial. JAMA 2003;
290:2713. (Q up to date2008)
Riedemann NC, Guo RF, Neff TA, et al.Increased C5a receptor expression in
sepsis. J Clin Invest 2002; 110:101. (Q up todate 2008)
108

References
Rivers, E, Nguyen, B, Havstad, S, et al. Early goal-directed therapy in the
treatment of severe sepsis and septic shock. N Engl J Med 2001;
345:1368. (Q up to date2008)
Romanovsky AA, Simons, CT, Szekely, M, Kulchitsky, VA. The vagus nerve
in the thermoregulatory response to systemic inflammation. Am J
Physiol 1997; 273:R407.
Roselle GA, Watanakunakorn C. Polymicrobial bacteremia. JAMA 1979;
242:2411.
Rosser DM, Stidwill RP, Jacobson D, et al. Cardiorespiratory and tissue
oxygen dose response to rat endotoxemia. Am J Physiol 1996;
271H:891. (Q up todate 2008)
Russell JA. Management of sepsis. N Engl J Med. 2006;355:1699-1713.
Sacks-Berg A, Calubiran OV, Cunha BA.Sepsis asociated with transhepatic
cholangiography. J Hosp Infect 1992; 20:43–50.
Safdar N, Handelsman J, Maki DG.Does combination antimicrobial therapy
reduce mortality in Gram-negative bacteraemia? A meta-analysis.
Lancet Infect Dis 2004; 4:519.
Schaff BM, boehmke F, Esnaashari H, et al. pneumococcal septic shock is
associated with the interlukin-10-1082 gene promoter
polymorphism. Am j respire Crit Care Med 2003; 168:476-480
Schramm GE, Johnson JA, Doherty JA, et al. Methicillin-resistant
Staphylococcus aureus sterile-site infection: The importance of
appropriate initial antimicrobial treatment. Crit Care Med 2006;
34:2069.
Schrier RW, Wang W. Acute renal failure and sepsis . N Engl J Med 2004;
351:159-169.
109

References
Segredo V, Caldwell JE Matthay MA, Sharma ML, Gruenke LD, Miller RD.
persistent paralysis in critically ill patients after long-term
administration of vecuronium. N Engl Med 1992; 327:524-528.
Seneff MG,Zimmerman, JE, Knaus, WA, et al. Predicting the duration of
mechanical ventilation. The importance of disease and patient
characteristics. Chest 1996; 110:469. (Up to date 2008)
sepsis rapidly mature but fail to initiate a protective Th1 Stefanie B. Flohé1,
Hemant Agrawal, Daniel Schmitz, Michaela Gertz, Sascha Flohé
and F. Ulrich Schade Dendritic cells during polymicrobial -type
immune response Journal of Leukocyte Biology. 2006; 79:473-
481.
Sessler CN, Perry JC, Varney KL. Management of severe sepsis and septic
shock. Curr Opin Crit Care 2004; 10:354.
Setia U, Gross PA. Bacteremia in a community hospital: spectrum and
mortality. Arch Intern Med 1977; 137:1698.
Sharshar T, Gray F, Lorin de, La Grandmaison G, Hopkinson, NS.
Apoptosis of neurons in cardiovascular autonomic centres
triggered by inducible nitric oxide synthase after death from septic
shock. Lancet 2003; 362:1799 (Q up to date 2008).
Sibbald WJ, Vincent JL. Round table conference on clinical trials for the
treatment of sepsis. Crit Care Med 1995; 23:394.
Siegel JP. Assessing the use of activated protein C in the treatment of severe
sepsis. N Engl J Med 2002; 347:1030-4.
Snell RJ, Parillo JE: Cardiovascular dysfunction in septic shock. Chest 1991;
99:1000–9.
Steinman RM, Nussenzweig MC. Avoiding horror autotoxicus: the importance
of dendritic cells in peripheral T cell tolerance Proc. Natl. Acad.
Sci. USA 2002; 99,351-358.
110

References
Stevens DL. Streptococcal toxic shock syndrome associated with necrotizing
fasciitis. Annu Rev Med 2000; 51:271–88.
Strehlow MC, Emond SD, Shapiro NI, Pelletier AJ, Camargo Jr CA.National
study of emergency department visits for sepsis. Annals of
Emergency Medicine 2006; 48: 326-331.
Sunderram J, Dombrovskiy VY, Martin AA. Rapid increase in hospitalization
and mortality rates for severe sepsis in the United States: A trend
analysis from 1993 to 2003. Crit Care Med 2007; 35:1244-1250)
Szabo G, Kodys K, Miller-Graziano CL.Elevated monocyte interleukin-6 (IL-
6) production in immunosuppressed trauma patients. J Clin
Immunol 1991; 11:326. (Q up todate 2008)
Tang BM, Eslick GD, Craig JC, McLean AS. Accuracy of procalcitonin for
sepsis diagnosis in critically ill patients: systematic review and
meta-analysis. Lancet Infect Dis 2007; 7:210.
Tapper H, Herwald H. Modulation of hemostatic mechanisms in bacterial
infectious diseases. Blood 2000; 96:2329. (Q up todate 2008)
Task Force of the American College of Critical Care Medicine, Society of
Critical Care Medicine. Practice parameters for hemodynamic
support of sepsis in adult patients in sepsis. Crit Care Med 1999;
27:639. (Q up to date2008)
The acute respiratory distress syndrome Network . Ventilation with lower
tidal volumes as compaired with traditional tidal volumes for acute
lung injury and the acute respiratory distress syndrome. N Engl J
Med 2000; 342 (18)1301-1308).
Thiery G, Azoulay E, Darmon M, et al: Outcome of cancer patients considered
for intensive care unit admission: a hospital-wide prospective
study. J Clin Oncol 2005; 23:4406,.
Third European Consensus Conference in Intensive Care Medicine. Tissue
hypoxia: How to detect, how to correct, how to prevent. Societe de
111

References
Reanimation de Langue Francaise. The American Thoracic
Society. European Society of Intensive Care Medicine. Am J
Respir Crit Care Med 1996; 154:1573. (Q up to date2008)
Tinsley KW, Grayson MH, Swanson PE, Drewry AM, Chang KC, Karl IE,
Hotchkiss RS. Sepsis induces apoptosis and profound depletion of
splenic interdigitating and follicular dendritic cells J. Immunol.
2003; 171,909-914
Underhill DM, Ozinsky A. Toll-like receptors: key mediators of microbe
detection. Curr Opin Immunol 2002; 14:103-10.
Upperman JS, Deitch EA, Guo W, et al. Post-hemorrhagic shock mesenteric
lymph is cytotoxic to endothelial cells and activates neutrophils.
Shock 1998; 10:407. (Q up to date 2008)
Van Amersfoort ES, Van Berkel TJ, Kuiper J. Receptors, mediators, and
mechanisms involved in bacterial sepsis and septic shock. Clin
Microbiol Rev 2003;16:379–414.
Van den Berghe G, Wilmer A , Hermans G, et al.Intensive insulin therapy in
the medical ICU. N Engl J Med 2006; 354:449-461.
Van Den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in
the critically ill patients. N Engl J Med. 2001; 345:1359-1367.
Van Der Poll T, Lowry SF. Tumor necrosis factor in sepsis: Mediator of
multiple organ failure or essential part of host defense. Shock
1995; 3:1. (Q up todate 2008)
Vanhorebebeek I, De Vos R, Mesotten D Wouters PJ De Wolf-Peeters C ,
Van den Berghe G. Protection of hepatocyte mitochondrial
ultrastructure and function by strict glucose control with insulin in
critically ill patients. Lancet 2005; 365:53-59.
Vercueil A, Grocott MPW, Mythen MG: Physiology, pharmacology, and
rationale for colloid administration for the maintenance of effective
112

References
hemodynamic stability in critically ill patients. Transfusion Med
Rev 2005; 19:93–109. Vi
Verhoef J, Hustinx WM, Frasa H, Hoepelman AI. Issues in the adjunct
therapy of severe sepsis. J Antimicrob Chemother 1996; 38:167.
(Q up to date 2008).
Villar J, Maca-Meyer N, Perez-Mendez L, Flores C. Bench-to-bedside
review: understanding genetic predisposition to sepsis. Crit Care
2004; 8:180–189.
Vincent JL, Bihari D, Suter PM, et al.The prevalence of nosocmial infection
in intensive care units in Europe .JAMA 1995; 74:639-644
Vincent JL, de Mendonça A, Cantraine F, et al.Use of the SOFA score to
assess the incidence of organ dysfunction/failure in intensive care
units: Results of a multicenter,prospective study. Crit Care Med
1998; 26:1793-1800
Vincent JL. Dear SIRS, I'm sorry to say that I don't like you. Crit Care Med
1997; 25:372-374.
Vincent, JL, Zhang, H, Szabo, C, Preiser, JC. Effects of nitric oxide in septic
shock. Am J Respir Crit Care Med 2000; 161:1781. (Q up to date
2008)
Waghorn DJ. Overwhelming infection in asplenic patients: Current best
practice preventive measures are not being followed. J Clin Pathol
2001;54:214–8.
Walley KR, Lukacs NW, Standiford TJ, Strieter RM, Kunkel SL. Balance of
inflammatory cytokines related to severity and mortality of murine
sepsis Infect. Immun.1996;64,4733-4738.
Walport MJ. Complement. First of two parts. N Engl J Med 2001; 344:1058.
Walport, MJ. Complement. Second of two parts. N Engl J Med 2001;
344:1140. (Q up todate 2008)
113

References
Wang H, Liao H, Ochani M, et al. Cholinergic agonists inhibit HMGB1
release and improve survival in experimental sepsis. Nat Med
2004; 10:1216.
ware LB, Matthay MA, Ware LB et al. the acute respiratory distress syndrome
N Engl J Med.2000; 342(18):1334-1349
Warren HS, Suffredini AF, Eichacker PQ, Munford RS. Risks and benefits
of activated protein C treatment for severe sepsis. N Engl J Med
2002;347:1027-30.
Weinstein Melvin P,L Barth Reller, James R. Murphy,Clinical importance of
polymicrobial Bacteremia, 1986.
Weinstein MP, Murphy JR., Relier LB, Lichtenstein KA. The clinical
significance of positive blood cultures: a comprehensive analysis
of 500 episodes of bacteremia and fungemia in adults. II. Clinical
observations with special reference to factors influencing
prognosis. Rev Infect Dis 1983a; 5:54.
Weinstein MP; Reller LB; Murphy JR Clinical importance of polymicrobial
bacteremia Diagn Microbiol Infect Dis. 1986;5(3):185-96.
Wheeler AP, Bernard GR. Treating patients with severe sepsis. N Engl J Med.
1999;340:207-214.
Wheeler AP, Bernard GR. Treating patients with severe sepsis. N Engl J Med
1999; 340:207. (Q up to date2008)
Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-
management strategies in acute lung injury. N Engl J Med 2006;
354:2564.
Wilkes MM, Navickis RJ. Patient survival after human albumin administration.
A meta-analysis of randomized, controlled trials. Ann Intern Med
2001; 135:149.
114

References
Yiung GB, Bolton CF, Archibald Y et al. the electroencephalogram in sepsis
associated encephalopathy. J Clin Neurophysiol.1992; 9(1):145-
152).
Yoo JH, Choi SM, Lee DG, et al: Prognostic factors influencing infection-
related mortality in patients with acute leukemia in Korea. J
Korean Med Sci 2005; 20:31,.
115

الملخص العربي
الملخص العربى التسمم البكتيرى هى كلمه التينيه بمعنى تعفن وفى الماض;;ى
حيث ق;;امت1992ح;;دث اختالف ح;;ول التعري;;ف ح;;تى ع;;ام الجامعه االمريكية الطباء الصدر فى وضع تعريف موح;;د للتس;;مم
البكتيرى. التسمم البكتيرى ه;;و تحف;;يز للجه;;از المن;;اعى بس;;بب ع;;دوى بكتيرية وع;رض االس;تجابة االلتهابي;;ه الرئس;ية ه;و تحف;يز للجه;از المن;;اعى بغض النظ;;ر عن الس;;بب ح;;رق-ع;;دوى-اص;;ابه التس;;مم البكتيرى الحاد هو تس;مم بكت;;يرى مص;احب بفش;ل بوظيف;;ه اح;د اعض;;اء الجس;;م الص;;دمه البكتيري;;ه هى تس;;مم بكت;;يرى مص;;احب
بهبوط حتد بضغط الدم. التسمم البكتيرى بؤدى الى زيادة الحجز بالرعايه وزيادة مدة البقاء على جهاز التنفس الصناعى مع اخذ مضادات حيوي;;ه غالي;;ه
الثمن مع ارتفاع تكلفة العالج. التسمم البكتيرى مص;;احب بارتف;;اع نس;;بة الوفي;;ات والتط;;ور المرض;;ى لم;;ريض التس;;مم البكت;;يرى يت;;اثر بم;;دى ق;;وة الع;;دوى
والحالة العامة للمريض واستجابة للمريض. فى النص;;;ف الث;;;انى من الق;;;رن العش;;;رين تم اس;;;تخدام المضادات الحيوية لعالج ح;;االت التس;;مم البكت;;يرى مم;;ا ادى الى انخفاض نسبة الوفيات بين هؤالء المرضى .اال ان نس;;بة الوفي;;ات ما بين مرض;;ى التس;;مم البكت;;يرى ال;;ذين يص;;احبهم انخف;;اض فى ضغط الدم او فشل فى وظ;;ائف الكلى اس;;تمرت عالي;;ة وه;;و م;;ا
يسمى بالصدمة البكتيرية. حال;;ة500فى الواليات المتحدة االمريكية هن;;اك على االف;;ل
تسمم بكتيرى سنويا وق;;د ثبت ان نس;بة الوفي;;ات ت;تراوح م;ا بين % بالرغم من اعطائهم مضادات حيوية مع االهتمام50% الى 30
بالتغذية ووجودهم على جهاز التنفس الصناعى. ومن ثم تم البحث عن عق;;اقير اخ;;رى لعالج ح;;االت التس;;مم البكتيرى وخاصة التى يصاحبها انخفاض فى ضغط ال;;دم او فش;;ل فى وظائف الكلى .وجد ان ب;;روتين س;;ى النش;;ط ومع;;اد االتح;;اد وهو مضادات التجلط الطبيعية له دور فى عالج مثل هذة الحاالت .وذل;;ك عن طري;;ق تقلي;;ل الم;;واد ال;;تى تنطل;;ق بع;;د سلس;;له من
1

الملخص العربي
6التفاعالت فى حاالت التس;;مم البكت;;يرى ومن اهمه;;ا ان;;ترلوكين مما يؤدى الى ارتباك نشاط ه;;ذة الم;;واد وع;;دم اكتم;;ال سلس;;لة
التفاعالت التى تحدث فى التسمم البكتيرى.
2

بروتين سي معاد االتحاد
ودوره في عالج حاالت التسمم البكتيري في العناية
المركزةرسالة
للحصول علي درجة الماجستير في طب الحاالتالحرجة
مقدمة من طبيب/ راندة رضا أحمد عبد الحافظ
بكالوريوس الطب والجراحة
تحت إشرافأ.د/ حمدي حسن عليوة
أستاذ التخدير والعناية المركزةكلية الطب - جامعة بنها
د/ أحمد حمدي عبد الرحمنمدرس التخدير والعناية المركزة
كلية الطب - جامعة بنها
كليـــــة الطـــــب

جامعة بنها2015