Embed Size (px)
Citation preview

Double Directional Persuasion
Fan Wu, Jie Zheng∗
First Version September 23, 2018; Updated June 2nd, 2019
Abstract
We study a double directional persuasion game between two players: a doctor and
a patient. The health condition of the patient, either severely ill or mildly ill, is known
to the doctor but not to the patient, while the type of valuation (or willingness to
pay) for the treatment, either high or low, is the patient’s private information. The
doctor’s payoff is merely the price she charges, while the patient’s payoff depends on
his health condition, his type, and the price charged by the doctor. This sequential
game consists of two stages: the ex ante design stage and the ex post implementation
stage. We consider all reasonable orders of play and fully characterize the equilib-
rium in each situation whenever an equilibrium exists. Our results imply that when
design is sequential, an equilibrium always exists and being the first mover at the de-
sign stage is weakly dominated by being the second mover, regardless who is the first
mover. In contrast, when design is simultaneous, there may not exist an equilibrium
under some parameter environment, and the equilibrium when the doctor sends signal
first is the equilibrium when the patient sends signal first and also coincides with the
equilibrium when design is sequential and the doctor designs (and sends signal) first.
Furthermore, comparing the situations where the patient sends signal first, we show
that the equilibrium under sequential design payoff dominates the one under simul-
taneous design, whenever an equilibrium exist. Our work applies to other scenarios
when sellers have professional knowledge regarding customers’ needs. The finding is
consistent with many real world observations and provides a better understanding of
the situations where persuasion can be sequential and double directional.
Keywords. Bayesian Persuasion, Sequential Persuasion, Two-sided Asymmetric Infor-
mation, Information Design
JEL Codes. C72, C73, D82, D83
∗Fan Wu: PBC School of Finance, Tsinghua University(email: [email protected]); Jie Zheng: School
of Economics and Management, Tsinghua University (email: [email protected]). For helpful comments and
insights, we thank Zhuoqiong Chen, Hong Feng, Matthew Gentzkow, Xiangting Hu, Xiaoxi Li, Xiang Sun, Jean Tirole,
Ruixin Wang, Mu Zhang, Mofei Zhao, and seminar participants at Harbin Institute of Technology (Shenzhen) and
Wuhan University. This research is funded by National Natural Science Foundation of China (Projects No.61661136002
and No.71873074), and Tsinghua University Initiative Scientific Research Grant (Project No.20151080397). All errors
are our own.
1

1 Introduction
Suppose two types of patients (H or L) with different willingness to pay under the
same health condition go to see the doctor (she). The doctor provides treatment and
charges a price. For the doctor, she always wishes to extract the full surplus from
the patient, which is the first best outcome for her. On the other hand, the patient
(he) of type H might try to convince the doctor that he is type-L in order to pay a
lower price. However, he cannot indulge his desire to lie. In other words, there is a
constraint that he cannot do so to pass the threshold when the doctor is indifferent
between two valuations (as the extremal market in Bergemann, Brooks and Morris
(2015)). The optimal way to persuade is Bayesian persuasion.
Now consider a different scenario. Suppose only one type of patients but with
different health conditions (S or M) go to see the doctor. After diagnosis, the doctor
would disclose his health condition and provide treatment accordingly. In addition,
the treatment for condition S is more advanced and thus more expensive. As a result,
the doctor always has the incentive to convince the patient that he is under condition
S which requires superior treatment. Therefore, she might benefit from Bayesian
persuasion due to her information superiority, i.e., professional knowledge.
What if we combine these two forces at play under one setup? That is to say, the
patient might be under condition S or M which the doctor knows, being type H or L
which is his private information. On the one hand, the H type patient might resort to
persuasion to mimic type L patient. On the other hand, the doctor might persuade the
patient regarding his health condition. As a whole, these two forces might interact
with each other. In this paper, we fully characterize the equilibrium for such a
double directional persuasion game whenever an equilibrium exists, by considering
different orders of play. Depending on whether the design stage is sequential move
or simultaneous move and which player sends the signal first at the implementation
stage, there are in total 4 sensible orders of play: (a) doctor being the first mover both
at the design stage and the implementation stage; (b) patient being the first mover
both at the design stage and the implementation stage; (c) simultaneous design with
doctor being the first mover at the implementation stage; (d) simultaneous design
with patient being the first mover at the implementation stage.
The first set of our results relates to the existence of equilibrium. For the two
setups with sequential design an equilibrium always exists, while for the two setups
with simultaneous design an equilibrium may not always exist and the space of pa-
rameter values under which equilibrium exists for the setup where the doctor sends
2

the signal first is a subset of that for the setup where the patient sends the signal
first.
The second set of our results relates to the welfare comparison for players. Our
Theorem 1 shows that being the first mover at the design stage (and the implementa-
tion stage) is weakly dominated by being the second mover, regardless of the identity
of the first mover. In contrast, Theorem 2 states that the equilibrium with simultane-
ous design and the doctor being the first signal sender is the same as the equilibrium
with simultaneous design and the patient being the first signal sender whenever the
equilibrium exists. The comparison of equilibria between the setup of simultaneous
design with the doctor being the first signal sender and the setup of sequential design
with the doctor being the first signal designer (and signal sender) yields a similar
result (Theorem 3). Finally, if we compare the setups of patient being the first sig-
nal sender, the equilibrium under sequential design payoff dominates the one under
simultaneous design, whenever an equilibrium exists (Theorem 4).
Our work belongs to the rising literature on Bayesian persuasion, following the
seminal work by Kamanica and Gentzkow (Kamenica and Gentzkow (2011)). Since in
the game we consider, more than one player sends the signal and more than one player
receives the signal, our work is related to both the studies on Bayesian persuasion
with multiple senders (Li and Norman (2017), Gentzkow and Kamenica (2017a),
Gentzkow and Kamenica (2017b)) and those on Bayesian persuasion with multiple
receivers (Alonso and Camara (2016a), Alonso and Camara (2016b), Bardhi and Guo
(2018), Chan et al. (2019), Wang (2015), Marie and Ludovic (2016)). However, the
key distinction between our work and those mentioned above is that in our setup the
receivers of some message are indeed the senders of a different message which means
the information transmission is double directional. Since both players have private
information in our setup, our work is also related to studies on Bayesian persuasion
of a privately informed receiver (for example, Kolotilin et al. (2017)), while we differ
from that literature by providing the privately informed receiver an opportunity to
persuade the sender.
The outline of this paper is as follows. In Section 2 we setup the model. In Sections
3 and 4, we analyze the setup of sequential design and consider the case where the
doctor moves first and the case where the patient moves first, respectively. Sections
5 and 6 consider the setup of simultaneous design where the doctor sends the signal
first and that where the patient sends the signal first, respectively. In Section 7, we
conduct welfare comparisons between different setups and deliver the main results.
Section 8 concludes.
3

2 The model
We consider a double directional sequential persuasion problem with double-sided
information asymmetry, between a doctor and a patient. The health condition of
the patient, either severely ill (j = S) or mildly ill (j = M), is known to the doctor
but not to the patient, while the type of valuation (or willingness to pay) for the
treatment, either high (i = H) or low (i = L), is the patient’s private information.
This sequential game consists of two stages: the ex ante signal design stage and the
ex post singal implementation stage. The players become privately informed between
these two stages, that is, after players design their persuasion strategies and before
they implement their persuasion strategies, nature draws patient’s type i ∈ {H,L}(high or low) and his health condition j ∈ {S,M}. Patient becomes aware of his
type while his condition is revealed to the doctor (she). Both players are assumed to
commit to their designed strategy when implementing their strategy at the second
stage. The information structure, the order of play, and the commitment assumption
are all common knowledge.
In the information design stage, we consider both sequential and simultaneous
commitment. For the information realization stage, the patient sends signal i while
the doctor sends signal j. In addition, we endogenize the timing of their commit-
ments (if sequential) and their reports. After reporting, the doctor would charge a
corresponding price P (i, j) for the treatment of his disease depending on the reported
type and condition. The information reported from both sides is unverifiable.
The value vij of the treatment to the patient is given by
vij H L
S xa a
M xb b
where a ≥ b is dictated by the definition of j while the patient’s type implies x ≥ 1.
We further assume that xb ≥ a to guarantee that the willingness to pay for type H
is always higher than type L, i.e., there is no price inversion under any parameter
settings represented by the following matrix which is the distribution of the patient’s
type and health condition:
Nij H L
S qn n
M pm m
where Nij indicates the relative amount of type i patients under condition j. There is
4

an alternative interpretation that this matrix provides the probability of the patient
being type i under condition j once you normalize them.
Preferences: The patient’s utility ui (where i ∈ {H,L}) relies on his type, his
condition reported j, and the price P (i, j) charged by the doctor
ui(i, j) =∑j
π(j|j) · vij − P (i, j)
with the outside option ui = 0 if he rejects the treatment. The doctor’s utility Ud
depends on the price P (i, j) of the treatment given the patient’s acceptance of the
treatment. Here we normalize the cost of this treatment to zero (or we could interpret
that P denotes the profit of the treatment after taking the cost into consideration).
Ud =∑i,j,i,j
Nij (i, j) · 1ui (i,j)≥0 · P (i, j)
where Nij (i, j) denote the number of type i, j patients under signal realization i, j.
The first best outcome for the doctor is
Ud0 =
∑i,j
Nijvij
which extracts the full surplus from the patient. We use Ud0 as a benchmark to
characterize the doctor’s relative welfare loss
U ≜ Ud − Ud0 .
Persuasion: The doctor’s persuasion signal is denoted by j. An arbitrary signal
j would take the form of
π(j = S|j = S) = t π(j = S|j = M) = r
π(j = M |j = S) = 1− t π(j = M |j = M) = 1− r
where 0 ≤ t ≤ 1, 0 ≤ r ≤ 1.
Similarly, an arbitrary signal i of the patient would be
π(i = H|i = H) = T π(i = H|i = L) = R
π(i = L|i = H) = 1− T π(i = L|i = L) = 1−R
where 0 ≤ T ≤ 1, 0 ≤ R ≤ 1.
5

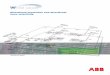
Figure 1: Sequential commitment-Doctor moves first
0 1 2 3
Doctor
commits
Patient
commits
Doctor sends signal,
then patient sends
signal
Doctor charges
price P, then
patient chooses
to accept or not
We shall define two persuasion thresholds πm and πs which would prove to be
useful later.
πm =1
(x− 1)p
πs =1
(x− 1)q.
Solution concept: We focus on subgame perfect equilibria. To simplify the anal-
ysis without loss of generality, we restrict our attention to the straightforward signal
under persuasion, which indicates the same meaning as Kamenica and Gentzkow
(2011).
3 Sequential Commitment-Doctor Moves First
In this section, the doctor takes the lead and the patient acts subsequently (both in
information design stage and information realization stage). In the information de-
sign stage, she is free to commit to any straightforward signal to send to the patient
regarding his condition in the first period. Notice that her commitment is indepen-
dent on the patient’s type, since she is unaware of that information at this point.
Then, with the doctor’s commitment in mind, the patient will choose his commit-
ment concerning his type. His strategy hinges upon both his type and the doctor’s
incoming signal j.
In the information generalization stage, the doctor sends her signal first. In the
second period, the patient sends his signal. In the third period, the doctor arrives
at the optimal P price to charge given patient’s report and her persuasion strategy.
Equilibrium is achieved when the doctor chooses the commitment to maximize her
utility given the anticipated commitment of the patient while the patient chooses the
optimal commitment strategy given the doctor’s commitment.
6

We characterize the equilibrium by backward induction. First, we address the
case where only one condition exists to see how the patient would act accordingly.
Second, we relax this assumption to analyze both player’s actions.
First, suppose only one condition exists, which implies that the doctor does not
need to diagnose. The patient has the incentive to convince her that his type is L
to reveal a lower willingness to pay. Thus, for type L patient, he would report so
with probability 1. However, type H patient might mimic type L where his uniquely
optimal strategy is a binary signal under which the doctor is indifferent between
charging vH and vL if she receives signal L. Therefore, we immediately obtain the
following lemma.
Lemma 1. If the market contains two types (H or L) of customers whose relative
amount N and willingness to pay v are represented by
H L
N NH NL
v vH vL,
the optimal persuasion strategy for the customer would be
π(i = L|i = H) = min[1
NH
NL(vHvL
− 1), 1] (1)
π(i = L|i = L) = 1 (2)
and the seller’s best response is
P =
vH , if i = H,
vL, if i = L.
The economic intuition is simple. Type L patient has no incentive to misreport
his type. However, type H patient could mimic type L patient to lower his payment.
But he could not indulge himself for doing so. Otherwise, the doctor may charge vH if
the market with i = L is mostly filled with type H patient. The threshold is reached
when the doctor is exactly indifferent between charging vH and vL. On the other
hand, the doctor’s best response to his action is to charge the price corresponding to
his report.
By Lemma 1, if j = S is truthfully revealed to the patient, his optimal signal i
for persuasion is
π(i = L|i = L) = 1
7

π(i = L|i = H) =
1(x−1)q
= πs, if πs ≤ 1,
1, o.w.
and the doctor’s best response is
P =
vHS, if i = H,
vLS, if i = L.
On the other hand, if j = M is truthfully revealed to the patient, his optimal signal
for persuasion is
π(i = L|i = L) = 1
π(i = L|i = H) =
1(x−1)p
= πm, if πm ≤ 1,
1, o.w.
and the doctor’s best response is
P =
vHM , if i = H,
vLM , if i = L.
From here we can see that (1) and (2) fully characterize patient’s best response,
which means that the doctor would lead the patient to react accordingly. What’s left
is the doctor’s persuasion strategy.
From Lemma 1, it is clear that if the patient’s type is H, he always attempts to
persuade the doctor. However, there is a natural constraint that
π(i = L|i = H) ≤ 1.
Suppose the doctor reveals the truth. We call the case where πs>1 as full persuasion
under condition S, since this constraint is binding and π(L|H) = 1. Otherwise,
π(L|H) = πs ≤ 1, which we refer to as partial persuasion. The same goes for
the patient under condition M where πm>1 is called full persuasion while partial
persuasion indicates π(L|H) = πm ≤ 1. As a result, we will address the issue case by
case: double partial persuasion, double full persuasion, single full persuasion.
Now we allow the doctor to persuade as well. Under an arbitrary persuasion
strategy by the doctor
π(j = S|j = S) = t π(j = S|j = M) = r,
8

the patient would be divided into two markets (or groups) j ∈ {S,M} where the first
one j = S is described by:
H L
N tqn+ rpm tn+ rm
v x tqna+rpmbtqn+rpm
tna+rmbtn+rm
(3)
Define
NH(t, r) ≜ tqn+ rpm
NL(t, r) ≜ tn+ rm
vH(t, r) ≜ xtqna+ rpmb
tqn+ rpm
vL(t, r) ≜tna+ rmb
tn+ rm
∆v(t, r) ≜ vH(t, r)− vL(t, r).
v relies on the persuasion because the patient would take the doctor’s persuasion
strategy into account and adjust his willingness to pay. It turns out that either one
of these two sub-market admits the following property.
Define
π(t, r) ≜ 1NH(t,r)NL(t,r)
(vH(t,r)vL(t,r)
− 1).
Lemma 2.
min[πs, πm] ≤ π(t, r) ≤ max[πs, πm]
always holds for any j.
That is to say, the persuasion threshold for either one is bounded between two
original thresholds.
3.1 Double Partial Persuasion
In this case, we have
πm ≤ 1
πs ≤ 1.
If the doctor reveals j truthfully,
U = −qnπs(xa− a)− pmπm(xb− b)
= −qn1
(x− 1)q(xa− a)− pm
1
(x− 1)p(xb− b)
= −na−mb.
9

However, it turns out that this result not only holds if the doctor is telling the truth,
but for all possible scenarios as well.
Lemma 3. If πs ≤ 1 and πm ≤ 1, the doctor’s welfare loss is
U = −na−mb
regardless of her own persuasion strategy.
This lemma directly leads us to the following proposition.
Proposition 1. Given doctor moves first, if πm ≤ 1 and πs ≤ 1,
1. the doctor is indifferent with any of her persuasion strategy.
2. the patient’s persuasion follows (1) and (2) under j = S and j = M , respec-
tively.
This proposition is easy to interpret. Since it is partial persuasion (interior so-
lution) under both conditions, it remains so for any reported condition j. Recall
that if it is interior persuasion, the doctor will suffer a loss which is equivalent to
the surplus of the L type patient. Combining both reported conditions together, her
welfare loss is equal to the result from lemma 3, which is a constant independent on
her persuasion strategy.
3.2 Double Full Persuasion
In this case, we have
πm>1
πs>1.
By Lemma 2,
π(t, r) ≥ min[πs, πm]>1,
π(1− t, 1− r) ≥ min[πs, πm]>1.
Thus, for both group of patients, they will employ full persuasion again
π(i = L|i = H) = 1
which leads to the following proposition.
10

Proposition 2. If πm>1 and πs>1, the doctor will always befully uninformative (t = r = 1), if p ≥ q,
fully informative (t = 1, r = 0), o.w.
and the patient’s best response is π(L|H) = 1.
From our previous case in double partial persuasion, we see that the persuasion
from the doctor’s side is ineffective to improve her utility. However, it is a different
story under double full persuasion case. Here, the patient will employ full persuasion
regardless of the doctor’s persuasion. If the doctor indeed bunch patients under
two conditions together, these patients would harbor the same willingness to pay.
Therefore, we could intuitively interpret this proposition. If p = q, the doctor’s
utility would remain the same, since now the willingness to pay for type H would be
x times of type L, which is the same as vHS
vLSand vHM
vLM. Nevertheless, if p>q, the ratio
of vH(1,1)vL(1,1)
would be smaller, hence a smaller price gap between type H and L, which
implies a lower welfare loss for the doctor (recall that her welfare loss derives from
and only from the price gap under double full persuasion).
3.3 Single Full Persuasion
Single full persuasion implies
min[πm, πs] ≤ 1<max[πm, πs].
Since it is either p<q or q<p, we will address them case by case.
Case 1: p<q
In this case,
πs ≤ 1<πm.
Proposition 3. If πs ≤ 1<πm, the doctor will always tell the truth and the patient’s
best response is
π(L|H) =
1, if j = M,
πs, o.w.
The intuition comes from two observations. A. It is not optimal to bunch patients
under two conditions into an interior solution π(t, r) ≤ 1. Otherwise, it would waste
the corner solution condition πm>1 where the patient is unable to tap into the full
potential of his persuasion. B. It is not a good choice to bunch patients together into
11

a corner solution, either. To see this, we could view such a bunching process as two
steps. 1. Bunching to the point where π(t, r) just hits the corner solution π(t, r) = 1.
2. Bunching further to pass the corner point. It is obvious that the first step will
take a toll on her (see point A). The doctor will suffer a loss in second step as well
(see Proposition 2). Therefore, she is better off revealing the truth when p<q.
Case 2: q<p
In this case,
πm ≤ 1<πs.
Define π1 and π0 as
(a− b)(p− q) = (m+ n
n)2b[p(x− 1)− 1
π1
] (4)
(a− b)(p− q) = b[p(x− 1)− 1
π0
] (5)
By their definitions, π1<π0 is self-obvious. If you plug π1 = πm into the RHS of (4),
LHS>0 = RHS
which implies πm<π1. If you plug π0 = πs into the RHS of (5),
LHS = (a− b)(p− q) ≤ b(x− 1)(p− q) = RHS
due to a ≤ xb. Therefore, π0 ≤ πs. Thus,
πm<π1<π0 ≤ πs. (6)
Proposition 4. If πm ≤ 1<πs, the doctor’s optimal strategy is
t = 1
r =
0, if π0 ≤ 1,
1, if π1 ≥ 1,
nm{√
(a−b)(p−q)b[p(x−1)−1]
− 1}, o.w.
and the patient’s best response is
π(L|H) =
1, if j = S,
πm, o.w.
12

Figure 2: Sequential commitment-Patient moves first
0 1 2 3
Patient
commits
Doctor
commits
Patient sends signal,
then doctor sends
signal
Patient charges
price P, then
doctor chooses
to accept or not
To understand this proposition, it is crucial to recall two observations. First, if
r is too large, it might render an interior solution π(L|H)<1, which is not desirable
because it allows the patient to exploit the full potential of his persuasion. Second, in
Proposition 2, it is optimal to bunch different types altogether since q<p. Therefore,
the doctor’s final utility hinges upon the trade-off between those two forces. In
addition, we have a natural constraint that 0 ≤ r ≤ 1, which leads to our proposition
above.
4 Sequential Commitment-Patient Moves First
For now we consider the case where the patient makes the first move. For the infor-
mation design stage, the patient commits first and the doctor commits afterwards.
For the information generalization stage, the patient sends signal first and the doctor
sends second. Then, the doctor is going to charge the patient for the treatment.
Equilibrium is achieved when the patient chooses the optimal commitment strategy
given the doctor’s following commitment strategy while the doctor chooses to commit
to maximize her utility given the patient’s commitment.
If the patient always reveals his type truthfully to the doctor, the doctor would
be able to obtain the first best outcome which is the full surplus from the market.
In addition, every type H patient has the incentive to convince the doctor that he is
type L in order to show a lower willingness to pay. However, he cannot indulge his
desire to lie to the doctor without any kind of restraint because the doctor is aware
of this fact and might charge vH as she sees fit. Besides, the patient is unaware of
his condition when he commits first. Thus, his commitment strategy is independent
on his condition. In this setup, it is the game between the doctor and the H type
patient. L type patient has no incentive to convince the doctor that his type is H.
Nor does he have any bargaining power in group i = L because he either needs to
13

offer his full willingness to pay or leave when vH is charged. It is the same even if
doctor would misreport. In this sense, L type patient is at the mercy of the doctor
and type H patient and always obtains zero surplus.
π(i = L|i = L) = 1
Therefore, there is only one variable in the strategy of type H patient we need to pin
down, π(i = L|i = H) which we will refer to as π(L|H). Under π(L|H), the doctor
is going to face two markets where the first one i = H is represented by
Nij H L
S [1− π(L|H)]qn 0
M [1− π(L|H)]pm 0
while the second one i = L is mixing
Nij H L
S π(L|H)qn n
M π(L|H)pm m.
Now we introduce the following lemma to pinpoint the sub-range which the opti-
mal π(L|H) belongs to.
Lemma 4. If the patient moves first,
1. The patient’s utility is monotonically increasing with π(L|H) over the sub-range
π(L|H) ∈ [0,min[πm, πs]] given any persuasion strategy of the doctor.
2. The patient’s persuasion strategy π(L|H) ∈ (0,min[πm, πs]] would strictly dom-
inate persuasion design where π(L|H)>max[πm, πs], if max[πm, πs]<1.
This lemma is easy to interpret. In the sub-range π(L|H) ∈ [0,min[πm, πs]], since
it has not reached the threshold yet, he could improve his persuasion power through
increasing π(L|H). However, in the sub-range π(L|H)>max[πm, πs], type H patient
would end up with zero surplus, since the doctor is going to charge vH regardless of
her persuasion design. Thus, π(L|H)>max[πm, πs] is always dominated by a small
value of π(L|H).
By the second part of this lemma, π(L|H)>max[πm, πs] is ruled out because it
is inferior to the choice 0<π(L|H) ≤ min[πm, πs]. Besides, π(L|H) = min[πm, πs]
dominates all the other solutions π(L|H) ∈ [0,min[πm, πs]]. Thus, optimal π(L|H)
satisfies
min(πm, πs) ≤ π(L|H) ≤ max(πm, πs) (7)
14

if max(πm, πs) ≤ 1.
To mirror our analysis in the previous section, we will continue to address this
issue case by case with the same method to categorize them. That is, if doctor reveals
his condition truthfully first, the patient under S and M would resort to: double full
persuasion, double partial persuasion, single full persuasion (notice this is only to
facilitate categorizing different parameter settings).
Before coming to our discussion, we need to point out that this section is closely
related to the previous one by the following lemma, which implies that some conclu-
sions in Section 3 could greatly simplify our upcoming analysis.
Lemma 5. Surplus loss equivalence: If the market contains two types (H or L) of
customers whose relative amount N and willingness to pay v are represented by
H L
N NH NL
v vH vL,
the producer’s surplus loss would be equivalent in two setups: 1. Directly charge a
single optimal price. 2. Let the patient persuade first and then decide the optimal
prices to charge separately.
The doctor is going to face market i = L
Nij H L
S π(L|H)qn n
M π(L|H)pm m
after the patient’s persuasion. Suppose there are two scenarios. In the first one,
the doctor employs persuasion and then charge prices directly. For another one,
the doctor employs persuasion and then let the patient persuade. Afterwards, she
charges prices based on the patient’s signal. By Lemma 5, the doctor’s payoff would
be identical in those two scenarios. That is to say, we could borrow the results from
Section 3 if we replace the p and q with π(L|H)p and π(L|H)q, respectively, to analyze
the doctor’s best response.
4.1 Double Partial Persuasion
In this case,
πm ≤ 1,
15

πs ≤ 1.
Case 1: p ≤ q (πs ≤ πm ≤ 1)
Proposition 5. If the patient moves first and πs ≤ πm ≤ 1, the patient’s optimal
action is
π(L|H) =
πs, if πs
πm>1− na
mb,
πm, o.w.
and the doctor will always reveal the truth (t = 1, r = 0).
By Lemma 4, the patient’s persuasion should satisfy π(L|H) ≤ max(πs, πm), which
would fall into our previous discussions in Proposition 1 and Proposition 3. Thus,
the doctor will always reveal the truth. The patient needs to consider the relative
probability of his health condition. Intuitively speaking, if condition S is highly
possible, he should bet on that result to choose π(L|H) = πs and vice versa.
Case 2: p>q (πm<πs ≤ 1)
Proposition 6. If the patient moves first and πm<πs ≤ 1, there exists a cutoff π∗
that the patient’s optimal
π(L|H) =
π1, if π1 ≥ π∗,
πs, o.w.
while the doctor’s best response is t = 1,
r =
1, if π(L|H) = π1,
0, if π(L|H) = πs.
In this case, the patient’s payoff is convex in sub-range [π1, πs], which leads to
corner solution. If the probability for him being under condition S is sufficiently
high, he should choose πs and abandon his persuasion benefit under condition M . If
q is relatively small compared to p, he should pick π1, which partially gives up his
persuasion potential under condition S.
4.2 Double Full Persuasion
In this case,
πm>1
πs>1.
16

Previously in Section 3.2 where doctor moves first, patient will always employ full
persuasion, i.e.,
π(L|H) = 1.
Notice that in that setup, doctor has already taken the patient’s action into account.
Therefore, if the patient does so beforehand, her action would remain the same as
Section 3.2.
As for the patient, by Lemma 4 his utility is monotonically increasing with π(L|H)
over the sub-range
π(L|H) ∈ [0,min(πm, πs)].
Since
min(πm, πs)>1,
he would choose π(L|H) = 1.
To sum up, the equilibrium is exactly the same as Section 3.2, which is character-
ized by Proposition 2.
4.3 Single Full Persuasion
Single full persuasion implies
min[πm, πs] ≤ 1<max[πm, πs].
Case 1: p<q (πs ≤ 1<πm)
Proposition 7. If patient moves first and πs ≤ 1<πm, patient’s optimal action is
π(L|H) =
πs, if 1−πs
πm≤ na
mb,
1, o.w.
and the doctor will always reveal the truth.
The intuition for this proposition is almost the same as Proposition 5. If the
probability of condition S is sufficiently large, the patient should pick π(L|H) = πs.
Otherwise, π(L|H) = 1.
Case 2: p>q (πm ≤ 1<πs)
Proposition 8. Given patient moving first and πm ≤ 1<πs, the optimal strategy of
the players is as follows:
1. If π1 ≥ 1, the patient would choose π(L|H) = 1 and the doctor chooses t = r =
1.
17

Figure 3: Simultaneous commitment-Doctor sends signal first
0 1 2 3
Simultaneous
commitment
Doctor sends
signal
Patient sends
signal
Patient charges
price P, then
doctor chooses
to accept or not
2. If π1<1<π0, there exists a cutoff π∗∗ that the patient would choose
π(L|H) =
π1, if π1 ≥ π∗∗,
1, o.w.
The doctor’s best response is t = 1,
r =
1, if π(L|H) = π1,
nm{√
(a−b)(p−q)b[p(x−1)−1]
− 1}, if π(L|H) = 1.
3. If π0 ≤ 1, the patient would choose
π(L|H) =
π1, if π1 ≥ π∗
πs,
1, o.w.
The doctor’s best response is t = 1,
r =
1, if π(L|H) = π1,
0, if π(L|H) = 1.
π1 and π0 are defined in (4) and (5).
The intuition of this proposition derives from Section 4.2 and Proposition 6. Since
the patient always choose corner solution to maximize his utility, the doctor only needs
to respond accordingly.
5 Simultaneous Commitment-Doctor sends signal
First
5.1 Double Partial Persuasion
Proposition 9. Under simultaneous commitment with doctor sending her signal first,
given πm ≤ 1 and πs ≤ 1,
18

1. if p = q, there is no equilibrium.
2. if p = q, equilibria exist with only this form such that the patient chooses
π(L|H) = πs(= πm) while the doctor is indifferent with her persuasion strategy.
With simultaneous commitment, the existence of equilibrium is more delicate.
That is to say, equilibrium may not exist under some parameter settings. Proposition
9 is easy to interpret. The case for p = q is self-obvious and we shall illustrate the
case for p = q (πs = πm). Given any commitment of the doctor, the patient is always
able to achieve his first-best outcome as in Lemma 3, which is the worse case scenario
for the doctor. However, now the doctor would always deviate to improve her welfare,
i.e., to switch two groups when t = r or to fully separate the patient (reveal the truth)
when t = r. That is to say, both players desire to obtain the second-mover advantage,
which makes it impossible to reach an equilibrium under simultaneous setup.
5.2 Double Full Persuasion
By Proposition 2, although the doctor would lead the patient’s commitment, she is
already fully aware of the patient’s action, i.e., π(L|H) = 1. Thus, under simultaneous
commitment setup, this is the unique equilibrium.
Proposition 10. Under simultaneous commitment with doctor sending her signal
first, given πm>1 and πs>1, the doctor will always the doctor will always befully uninformative (t = r = 1), if p ≥ q,
fully informative (t = 1, r = 0), o.w.
and the patient’s best response is π(L|H) = 1.
Proof of Proposition 10. The proof follows directly from previous discussions.
5.3 Single Full Persuasion
Proposition 11. Under simultaneous commitment with doctor sending her signal
first, if πs ≤ 1<πm, there is no equilibrium.
The economic intuition is similar to Proposition 9. No equilibrium exists due to the
fact that both players desires to play wait and see to gain the second-mover advantage.
To be more specific, given any doctor’s commitment strategy, the best response of
the patient would cause the doctor to deviate from her original commitment.
19

Proposition 12. Under simultaneous commitment with doctor sending her signal
first, given πm ≤ 1<πs,
1. If π1 ≥ 1, equilibrium exists: the doctor would pool the patient into one group
(t = r = 1) while the patient chooses π(L|H) = 1.
2. Otherwise, no equilibrium.
We could compare this proposition with Proposition 4 to facilitate our under-
standing. If π1 ≥ 1, equilibrium remains exactly the same as sequential commitment.
(Actually, it is essentially the same as the case in Proposition 10.) Otherwise, equi-
librium does not exist due to the second-mover advantage for both players.
πm
πs
1
10
π1 = 1
Figure 4: Simultaneous Commitment Doctor First
Before concluding this section, we combines all possible parameter settings into
figure 4. The shaded area identifies the parameter values where the equilibrium does
not exist. The curve represents π1 = 1.
6 Simultaneous Commitment-Patient sends signal
First
6.1 Double Partial Persuasion
Case 1: p ≤ q (πs ≤ πm ≤ 1)
Recall Proposition 5. Given the patient’s persuasion
min(πm, πs) ≤ π(L|H) ≤ max(πm, πs)
20

Figure 5: Simultaneous commitment-Patient sends signal first
0 1 2 3
Simultaneous
commitment
Patient sends
signal
Doctor sends
signal
Patient charges
price P, then
doctor chooses
to accept or not
by Lemma 4, fully separating the patient would become the dominant strategy for
the doctor by the proof of Proposition 5. Meanwhile, the patient’s choice is the
best response given the doctor’s strategy. Thus, under simultaneous commitment
with patient sending his signal first, the unique equilibrium remains the same as
Proposition 5.
Proposition 13. Under simultaneous commitment with patient sending his signal
first, given πs ≤ πm ≤ 1, the patient’s optimal action is
π(L|H) =
πs, if πs
πm>1− na
mb,
πm, o.w.
and the doctor will always reveal the truth (t = 1, r = 0).
Proof of Proposition 13. The proof follows directly from previous discussions.
Case 2: p>q (πm<πs ≤ 1)
Proposition 14. Under simultaneous commitment with patient sending his signal
first, given πm<πs ≤ 1, the unique equilibrium exists if and only if
πm
πs
≤ 1− mb
na
Under this equilibrium, the patient’s optimal action is π(L|H) = πs and the doctor
will reveal the truth (t = 1, r = 0).
The economic intuition is as follows. Since the patient sends signal first, his
commitment is independent on the doctor’s signal j. That is to say, he commits a
single π(L|H) for both j = S and j = M . To maximize his utility, he either chooses
π(t, r) or π(1 − t, 1 − r). If he chooses the smaller one, the doctor would deviate
to pooling all patients together in the commitment stage. If he chooses the larger
21

one ( = πs), the doctor would deviate to fully separate all patients (reveal the truth).
Therefore, the only possible equilibrium exists when the doctor reveals the truth and
the patient chooses π(L|H) = πs. The condition for the existence of such equilibrium
dictates that the patient would prefer πs over πm.
Notice in this equilibrium, type L patient under condition M is crowded out of
the market, since price vHM is charged. Thus, social welfare is not optimal and there
is some welfare losses due to transaction failure.
6.2 Double Full Persuasion
In this case, the equilibrium is exactly the same as Proposition 10.
Under simultaneous commitment with doctor sending her signal first, given πm>1
and πs>1, the doctor will always befully uninformative (t = r = 1), if p ≥ q,
fully informative (t = 1, r = 0), o.w.
and the patient’s best response is π(L|H) = 1.
6.3 Single Full Persuasion
Case 1: πs ≤ 1<πm
Recall Proposition 7. Once more, fully separating the patient would become
the dominant strategy for the doctor by the proof of Proposition 7. Meanwhile,
the patient’s choice is the best response given the doctor’s strategy. Thus, under
simultaneous commitment with patient sending his signal first, the unique equilibrium
remains the same as Proposition 7.
Proposition 15. Under simultaneous commitment with patient sending his signal
first, given πs ≤ 1<πm, the patient’s optimal action is
π(L|H) =
πs, if 1−πs
πm≤ na
mb,
1, o.w.
and the doctor will always reveal the truth (t = 1, r = 0).
Proof of Proposition 15. The proof follows directly from previous discussions.
Case 2: πm ≤ 1<πs
22

Proposition 16. Under simultaneous commitment with patient sending his signal
first, given πm ≤ 1<πs,
1. If π1 ≥ 1, the unique equilibrium is such that the patient would choose π(L|H) =
1 and the doctor chooses t = r = 1.
2. If π1<1<π0, there exists a cutoff Π∗ that the unique equilibrium exists if and
only if
πm ≤ Π∗.
Under this equilibrium, the patient would choose
π(L|H) = 1.
The doctor’s best response is t = 1,
r =n
m{
√(a− b)(p− q)
b[p(x− 1)− 1]− 1}.
3. If π0 ≤ 1, the unique equilibrium exists if and only if
1− πm
πs
≥ mb
na.
Under this equilibrium, the patient would choose
π(L|H) = 1.
The doctor’s best response is
t = 1, r = 0.
The readers could turn back to Proposition 8 to gain more insight into this propo-
sition. Equilibrium exists only if π(L|H) = 1. Recall that the patient either chooses
π(t, r) or π(1 − t, 1 − r) in equilibrium. If π(L|H) = 1, the doctor would deviate to
reveal the truth (bunch all the patients together) when he chooses the larger (smaller)
one of π(t, r) and π(1− t, 1− r). The condition in the Proposition 16 is to guarantee
that the patient would not deviate from commitment π(L|H) = 1.
In figure 6, the shaded area identifies the parameter values where the equilibrium
does not exist. Two curves represent π1 = 1 and π0 = 1, respectively.
7 Comparison and Result
7.1 Comparison between Sequential Games
In this section, we are ready to draw a comparison between two setups in Section 3
and Section 4. That is, how would the patient and the doctor choose between those
23

πm
πs
1
10
1− mbna
π1 = 1
π0 = 1
Figure 6: Simultaneous Commitment Patient First
two setups? Would they choose to move first to gain some first-mover advantages?
Or they prefer to wait and observe to obtain second-mover advantage? With the
following theorem, we shall illustrate that if the doctor plays wait and see, her utility
is weakly better than the case where she takes the first move. What’s more, the same
goes for the patient. In other words, for both players, the strategy to wait always
dominates moving first.
Theorem 1. Both parties weakly prefer to play wait and see, i.e., choosing to let the
other one move first always weakly dominates taking the first move.
The readers should be familiar with both players’ utilities by now and the intuition
is simple. If there is only one possible type of patient (H or L), the doctor’s persuasion
would serve no purposes because the patient would take her action into consideration
and adjust his willingness to pay accordingly. Therefore, she would end up with the
same surplus which is her first best outcome. By contrast, the patient’s persuasion
is indeed effective, since the type H patient could disguise themselves as type L and
thereby lower the payment. Thus, in this double directional game, if the doctor is
strictly better off with her persuasion, this improvement must derive from type H
patient. To be more specific, her persuasion could mitigate her surplus loss caused
by the patient’s persuasion. In other words, her persuasion is able to keep type H
patient’s persuasion in check.
If the patient moves first, without knowing which group j he will end up being, he
needs to take both possibilities into account. However, the maximum π(L|H) allowed
by the doctor varies with j. By the proof of Theorem 1, the patient’s utility function
is convex over π(L|H) ∈ [π1, π0]. Thus, he will choose corner solution as a result.
24

If it is the smaller corner solution, compared to the situation where patient moves
second, the doctor is better off while type H patient is worse off, since his persuasion
power does not reach its full potential, relatively speaking. Type L patient remains
the same. If it is the larger corner solution, compared to the situation where patient
moves second, type H patient is worse off because some of them end up paying H
price while crowding out corresponding type L patient. The doctor remains the same.
7.2 Comparison between Simultaneous Games
Theorem 2. Under simultaneous commitment, if equilibrium exists under both regimes
(doctor sending first versus patient first), then equilibrium for two regimes remains
the same.
Comparing two setups under simultaneous commitment, it is clear that the space
of parameter values under which equilibrium exists when doctor sends signal first is a
subset of that when patient sends signal first. (In this subset, the equilibrium under
two regimes are identical.) That is to say, it is more difficult to reach an equilibrium
when doctor sends signal first. A closer look at Proposition 9 and Proposition 13
would shed light on this issue. Recall that when doctor sends signal first, the patient’s
commitment is more intricate. His commitment is contingent on the signal j he will
receive. In other words, he is at the liberty to commit to different π(L|H) for j = S
and j = M , respectively, which provides him with more commitment power. However,
is this a blessing? The answer is negative. From the doctor’s perspective, she could
use it to her advantage to improve her welfare. In Proposition 9, she could deviate
to switch j = S and j = M to obtain a positive gain relative to full loss. However,
when the patient sends signal first (forgoes such conditional commitment), the doctor
finds it more difficult to deviate to profit. Binding the hands the patient nullifies the
doctor’s incentive to deviate, which renders it easier to reach an equilibrium.
7.3 Comparison between Simultaneous and Sequential Com-
mitment
Theorem 3. If equilibrium exists under both regimes (simultaneous commitment and
sequential commitment) where doctor moves first, the equilibrium in those two regimes
are the same.
Once again, the space of parameter values under which equilibrium exists under
simultaneous commitment is a subset of that under sequential commitment. (In this
25

subset, the equilibrium under two regimes are identical.) This result is easy to in-
terpret. For sequential commitment, equilibrium always exists that the doctor would
lead the patient to respond (commit). That is to say, regardless of the doctor’s strat-
egy, the patient’s best response always exists. So does the equilibrium. Nevertheless,
under simultaneous commitment, given the patient’s best response, we need to check
whether the doctor would deviate or not, which kicks in one more necessary condition
for the equilibrium to hold and shrinks the parameter space befitting the equilibrium.
Theorem 4. If equilibrium exists under both regimes (simultaneous commitment and
sequential commitment) where the patient moves first, the sequential-commitment
setup Pareto dominates the simultaneous-commitment one.
If equilibrium exists, we could focus on the case πm<πs, since otherwise equilibria
remain the same under two regimes. For the sequential-commitment regime, the pa-
tient leads the doctor to respond and chooses between two corner solutions of π(L|H).
If he prefers the larger one, the equilibrium is identical to that of simultaneous-
commitment setup. On the other hand, if he prefers the smaller corner solution, both
players are better off. For the patient, this is due to his larger choice set. For the
doctor, her utility is monotonically decreasing in π(L|H) (see the proof of Theorem
1). As a result, sequential-commitment regime Pareto dominates the simultaneous-
commitment one. How does the social welfare improve in this game? The answer
lies within the participation of type L patient. If he faces an over-charged price, he
would forgo the transaction and leave, which could only be caused by the persuasion
strategy of type H patient. However, this is not ideal in terms of social welfare, since
the positive gain of trade vLS or vLM is lost. Taking the smaller corner solution of
π(L|H) means to bring the type L patient into the game and let them participate in
the transaction. Their participation provides cover for the type H patient in a sense
that type H patient could more easily disguise themselves as type L and thus lower
their payment. However, for type H patient, in this generous strategy, there is one
drawback that sometimes the persuasion does not reach its full potential, since it is
the smaller corner solution by design. Therefore, whether both players are strictly
better off hinges upon the tension between those two forces.
8 Conclusion
In this paper, we study the double directional Bayesian persuasion in a setting of
two-sided asymmetric information where both players are rational Bayesian updaters
26

and can commit to their persuasion strategies designed before the private information
is received. As far as we know, this is the first work on sequential persuasion with
different directions, and the first work incorporating the order of play into the design
stage (and the implementation stage) of the persuasion strategies.
Depending on whether the design stage is sequential move or simultaneous move
and which player sends the signal first at the implementation stage, we consider in
total four reasonable orders of play and fully characterize the equilibrium in each
setup whenever an equilibrium exists. For the two setups with sequential design we
show the existence of equilibrium, while for the two setups with simultaneous design
an equilibrium may not always exist and the space of parameter values under which
equilibrium exists for the setup where the doctor sends the signal first is a subset of
that for the setup where the patient sends the signal first.
By comparing the equilibria between different setups, we show that being the
first mover at the design stage (and the implementation stage) is weakly dominated
by being the second mover, regardless who is the first mover. By contrast, under
simultaneous design, the equilibrium for the doctor being the first signal sender is the
same as the equilibrium with the patient being the first signal sender whenever the
equilibrium exists. The comparison of equilibria between the setup of simultaneous
design with the doctor being the first signal sender and the setup of sequential design
with the doctor being the first signal designer (and signal sender) yields a similar
result. Finally, if we compare the setups of patient being the first signal sender,
the equilibrium under sequential design payoff dominates the one under simultaneous
design, whenever an equilibrium exists.
Our analysis for the doctor-patient interaction could easily extend to other sce-
narios where the seller has professional knowledge regarding the customer’s needs.
On the one hand, the customer desires to signal a lower willingness to pay in order
to lower the payment. On the other hand, the seller wishes to sell the customer a
more advanced (fancier) product in order to earn a higher profit. Both phenomena
coincide with real life experiences that customers like to haggle and might end up
buying something flashier (more expensive) than previously expected. Within both
processes, Bayesian persuasion could serve as a useful tool.
Notice that we assume commitment for both players in our study, which is a very
strong assumption. Alternative setups to analyze such a double directional persuasion
game may either have both players cheap talk or let one player cheap talk while the
other employ a committed strategy. As another direction for future study, we may
consider how our result is related to the bargaining literature where two privately
27

informed players interact via sequential bargaining.
28

References
Alonso, Ricardo, and Odilon Camara. 2016a. “Bayesian Persuasion with Het-
erogeneous Priors.” Journal of Economic Theory, 165: 672–706.
Alonso, Ricardo, and Odilon Camara. 2016b. “Persuading Voters.” American
Economic Review, 106(11): 3590–3605.
Bardhi, Arjada, and Yingni Guo. 2018. “Modes of Persuasion Toward Unanimous
Consent.” Theoretical Economics, 13(3): 1111–1150.
Bergemann, Dirk, Benjamin Brooks, and Stephen Morris. 2015. “The Limits
of Price Discrimination.” American Economic Review, 105(3): 921–957.
Chan, Jimmy, Seher Gupta, Fei Li, and Yun Wang. 2019. “Pivotal Persua-
sion.” Journal of Economic Theory, 180: 178–202.
Gentzkow, Matthew, and Emir Kamenica. 2017a. “Bayesian Persuasion with
Multiple Senders and Rich Signal Spaces.” Games & Economic Behavior, 104.
Gentzkow, Matthew, and Emir Kamenica. 2017b. “Competition in Persuasion.”
Review of Economic Studies, 84: 300–322.
Kamenica, E., and M. Gentzkow. 2011. “Bayesian Persuasion.” American Eco-
nomic Review, 101(6): 2590–2615.
Kolotilin, Anton, Tymofiy Mylovanov, Andriy Zapechelnyuk, and Li Ming.
2017. “Persuasion of a Privately Informed Receiver.” Econometrica, 85(6): 1949–
1964.
Li, Fei, and Peter Norman. 2017. “Sequential Persuasion.” Working Paper.
Marie, Laclau, and Renou Ludovic. 2016. “Public Persuasion.” Working Paper.
Wang, Yun. 2015. “Bayesian Persuasion with Multiple Receivers.” Working Paper.
29

A Omitted Proofs in Section 3
Proof of Lemma 1. We only need to prove i is the patient’s best response, since the
rest is obvious. For the producer to be indifferent between charging vH and vL if
i = L.
π(i = H |i = L)NHvH = [π(i = H |i = L)NH +NL]vL
π(i = H |i = L) =1
NH
NL(vHvL
− 1),
if 1NHNL
(vHvL
−1)≤ 1. Otherwise,
π(i = H |i = L) = 1.
Proof of Lemma 2. It suffices to prove
min[(x− 1)q, (x− 1)p] ≤ 1
π(t, r)≤ max[(x− 1)q, (x− 1)p]. (8)
1
π(t, r)=tqn+ rpm
tn+ rm(x
tqna+ rpmb
tqn+ rpm
tn+ rm
tna+ rmb− 1)
=xtqna+ rpmb
tna+ rmb− tqn+ rpm
tn+ rm
=xp− p+ (q − p)tn[xa
tna+ rmb− 1
tn+ rm]
=xq − q + (p− q)rm[xb
tna+ rmb− 1
tn+ rm]
To prove (8), it suffices to prove
xa
tna+ rmb− 1
tn+ rm≥ 0 (9)
xb
tna+ rmb− 1
tn+ rm≥ 0. (10)
Notice that (9) is already guaranteed by a ≥ b and x ≥ 1 while (10) is equivalent to
x ≥ tna+ rmb
tnb+ rmb
which is assured by xb ≥ a.
The proof for the other group of patient under j = M is almost the same if you
replace t and r with 1− t and 1− r, respectively.
30

Proof of Lemma 3. For j = S, by (1)
π(i = L|i = H) = min[π(t, r), 1].
From Lemma 2
π(t, r) ≤ max[1
(x− 1)q,
1
(x− 1)p] ≤ 1
Therefore, the doctor’s welfare loss for the group of patients under j = S would be
Uj=S = −NH(t, r)π(i = L|i = H)∆v(t, r)
= −NH(t, r)1
NH(t,r)NL(t,r)
(vH(t,r)vL(t,r)
− 1)(vH(t, r)− vL(t, r))
= −tna− rmb.
The same logic goes for market 2 where j = M ,
Uj=M = −(1− t)na− (1− r)mb.
Thus, we obtain the total welfare loss
U = Uj=S + Uj=M = −na−mb.
Lemma 6. If 0 ≤ r ≤ 1 and 0 ≤ t ≤ 1,
1
m+ n=
rt
rm+ tn+
(1− r)(1− t)
(1− r)m+ (1− t)n+
mn(t− r)2
(m+ n)(rm+ tn)[(1− r)m+ (1− t)n].
Proof of Proposition 2. If the doctor reveals the truth, her welfare loss is
U = −qn(x− 1)a− pm(x− 1)b.
If she chooses t = r = 1, by Lemma 2,
π(1, 1) ≥ min[πs, πm]>1
U ′ = −(qn+ pm)∆v(1, 1).
The difference between these two strategies is denoted by ∆U
∆U = U ′ − U
= qn[(x− 1)a−∆v(1, 1)] + pm[(x− 1)b−∆v(1, 1)]
= qn[b− a
m+ nm− x
b− a
qn+ pmpm] + pm[
a− b
m+ nn− x
a− b
qn+ pmqn]
=mn
m+ n(a− b)(p− q)
31

Under persuasion strategy t, r by the doctor, the difference between doctor’s persua-
sion and her revealing the truth would be
∆U = (a− b)(p− q)[rmtn
rm+ tn+
(1− r)m(1− t)n
(1− r)m+ (1− t)n].
If p<q, ∆U<0. Thus, her best strategy would be revealing the truth.
If p ≥ q, ∆U ≥ 0. Besides, by Lemma 6
(a− b)(p− q)[rmtn
rm+ tn+
(1− r)m(1− t)n
(1− r)m+ (1− t)n] ≤ (a− b)(p− q)
mn
m+ n.
Therefore, her optimal choice is to group them together by always reporting only one
condition (t = r = 1).
Lemma 7. In the case of single full persuasion, if doctor persuades the patients under
under j = S and j = M to form a group where
π(t, r) ≤ 1,
from this group she will sustain a strict loss compared to revealing the truth.
Proof of Lemma 7. We shall only prove the case where p<q because the proof for the
scenario p>q is the same.
Suppose p<q. Since patient will employ single full persuasion if doctor reveals the
truth, we have1
(x− 1)q≤ 1<
1
(x− 1)p.
Suppose π(t, r) ≤ 1. Under persuasion,
U ′ = −NH(t, r)π(t, r)∆v(t, r)
= −NL(t, r)vL(t, r)
= −tna− rmb
Without doctor’s persuasion, her welfare loss from this group of patients is
U =− rpm(x− 1)b− tqnπs(x− 1)a
>− rmp1
(x− 1)p(x− 1)b− tqn
1
(x− 1)q(x− 1)a
=− tna− rmb
=U ′
where the inequality holds since 1(x−1)p
>1.
If this group is j = M , the proof is quite similar where you only need to replace
r and t with 1− r and 1− t.
32

Proof of Proposition 3. Under persuasion strategy t, r by the doctor, if
π(t, r) ≤ 1,
doctor would sustain a strict loss from this group by Lemma 7. If it is the case for
both groups j = S and j = M , the doctor’s persuasion would take a toll on her.
Otherwise, there is at least one group where
π(t, r)>1
or π(1− t, 1− r)>1. Suppose it is group j = S.
U ′ = −(prm+ qtn)∆v(t, r).
For 1(x−1)q
≤ 1< 1(x−1)p
, if doctor reveals condition truthfully, her welfare loss from this
group would be
U = −prm(x− 1)b− tna.
The difference between persuading them together and telling the truth is
∆U =U ′ − U
=prm[(x− 1)b−∆v(t, r)] + tn[a− q∆v(t, r)]
=prm[a− b
rm+ tntn− x
a− b
qtn+ prmqtn] + tnq[
a
q− (x− 1)a+ rm
b− a
rm+ tn− x
b− a
qtn+ prmprm]
=− tna[(x− 1)q − 1] +rmtn
rm+ tn(a− b)(p− q)
<0
where the inequality holds since p<q and (x− 1)q ≥ 1.
If this group is j = M , the proof is quite similar where you only need to replace
r and t with 1− r and 1− t.
Lemma 8. If πm ≤ 1<πs and t = 1, the doctor’s optimal strategy is
r =
0, if π0 ≤ 1,
1, if π1 ≥ 1,
nm{√
(a−b)(p−q)b[p(x−1)−1]
− 1}, o.w.
Proof of Lemma 8. If t = 1, there is only one variable r left for the doctor to maximize
her utility. If doctor reveals the truth,
U = −qn(x− 1)a−mb (11)
33

If she resorts to persuasion π(j = S|j = M) = r, for group j = S we have
H L
Ni qn+ rpm n+ rm
vi x qna+rpmbqn+rpm
na+rmbn+rm
By Lemma 7,
r<r∗ (12)
where r∗ is defined by
π(1, r∗) = 1. (13)
Otherwise, the doctor would be better off refraining from persuasion. Thus, her utility
would be
U ′ = −(qn+ rpm)∆v(1, r)− (1− r)mb (14)
The difference between persuasion and telling the truth is
∆U = U ′ − U
= qn[(x− 1)a−∆v(1, r)] + rm[b− p∆v(1, r)]
= qn[b− a
rm+ nmr − x
b− a
qn+ pmrpmr] + rmp[
b
p− (x− 1)b− xqn
a− b
qn+ pmr+ n
a− b
rm+ n]
= −rmb[p(x− 1)− 1] +mrn
rm+ n(a− b)(p− q)
∆U = m{−rb[p(x− 1)− 1] +rn
rm+ n(a− b)(p− q)} (15)
∂∆U
∂r= m{−b[p(x− 1)− 1] + (a− b)(p− q)
n2
(n+ rm)2} (16)
∂2∆U
∂r2<0
Therefore, there is a unique maximizer in the sub-range r ∈ [0, 1].
If (a− b)(p− q) ≤ b[p(x− 1)− 1],
∂∆U
∂r≤ 0.
Thus, ∆u reaches its maximum when r = 0.
If b[p(x− 1)− 1]<(a− b)(p− q)<(m+nn
)2b[p(x− 1)− 1], ∆u reaches its maximum
when
b[p(x− 1)− 1] = (a− b)(p− q)n2
(n+ rm)2.
34

If (a− b)(p− q) ≥ (m+nn
)2b[p(x− 1)− 1],
∂∆U
∂r≥ 0, 0 ≤ r ≤ 1
Thus, ∆U reaches its maximum when r = 1.
Notice that for the optimal r, by (15)
m{−rb[p(x− 1)− 1] +rn
rm+ n(a− b)(p− q)} ≥ 0.
Now we come back to illustrate that the optimal r already satisfies the constraint
r<r∗. Suppose r ≥ r∗, we arrive at
π(1, r) ≤ 1.
By Lemma 2. Thus,
U ′ = −(qn+ rpm)π(1, r)(vH − vL)− (1− r)mb ≥ −(qn+ rpm)(vH − vL)− (1− r)mb
Therefore, by (15)
∆U = U ′ − U ≥ m{−rb[p(x− 1)− 1] +rn
rm+ n(a− b)(p− q)}
However, by Lemma 7,
∆U<0
m{−rb[p(x− 1)− 1] +rn
rm+ n(a− b)(p− q)} ≤ ∆U<0,
a contradiction.
Lemma 9. If 1(x−1)p
≤ 1< 1(x−1)q
, the doctor’s persuasion strategy
π(j = S|j = S) = 1
r =
0, if (a− b)(p− q) ≤ b[p(x− 1)− 1],
1, if (a− b)(p− q) ≥ (m+nn
)2b[p(x− 1)− 1],
nm{√
(a−b)(p−q)b[p(x−1)−1]
− 1}, o.w.
will always dominate the strategy to pool all patient together
t = r
Proof of Lemma 9. Doctor’s strategy to bunch the patient together is same as r = 1
in Lemma 8. However, the optimal r in Lemma 8 maximize her utility over the
sub-range r ∈ [0, 1] which contains the case r = 1.
35

Proof of Proposition 4. We are about to prove that the doctor’s strategy in the propo-
sition dominates an arbitrary persuasion strategy
π(j = S|j = S) = t π(j = S|j = M) = r (17)
π(j = M |j = S) = 1− t π(j = M |j = M) = 1− r. (18)
If the doctor is able to divide the patient into two markets where the first one is
represented by:
Nij H L
S qtn tn
M prm rm
while second one isNij H L
S q(1− t)n (1− t)n
M p(1− r)m (1− r)m.
Furthermore, if she is able to independently employ persuasion in those two markets.
By Lemma 9, the strategy to dictate t1,r1 in market 1 and t2, r2 in market 2 where
t1 = 1
r1 =
0, if (a− b)(p− q) ≤ b[p(x− 1)− 1],
1, if (a− b)(p− q) ≥ ( rm+tntn
)2b[p(x− 1)− 1],
tnrm
{√
(a−b)(p−q)b[p(x−1)−1]
− 1}, o.w.
t2 = 1
r2 =
0, if (a− b)(p− q) ≤ b[p(x− 1)− 1],
1, if (a− b)(p− q) ≥ ( (1−r)m+(1−t)n(1−t)n
)2b[p(x− 1)− 1],
(1−t)n(1−r)m
{√
(a−b)(p−q)b[p(x−1)−1]
− 1}, o.w.
would dominate the original persuasion strategy indicated by (17) and (18). There-
fore, it suffices to prove that the persuasion strategy
t = 1
r =
0, if (a− b)(p− q) ≤ b[p(x− 1)− 1],
1, if (a− b)(p− q) ≥ (m+nn
)2b[p(x− 1)− 1],
nm{√
(a−b)(p−q)b[p(x−1)−1]
− 1}, o.w.
36

in the whole market weakly dominates persuading the patient by t1,r1 in market 1
and t2, r2 in market 2, respectively. Without loss of generality, we assume t ≥ r
(Otherwise, you could switch t and r).
r1 ≥ r ≥ r2
Case 1: (a− b)(p− q) ≤ b[p(x− 1)− 1]
In this case,
r1 = r2 = r = 0.
Thus, the doctor will always reveal the truth in market 1, 2 and the whole market.
Whether the segmentation of the whole market exists or not does not matter and we
are done here.
Case 2: b[p(x− 1)− 1]<(a− b)(p− q)<(m+nn
)2b[p(x− 1)− 1]
In this case,
0<r<1.
Suppose r and t are such that r1<1. Let ∆U1, ∆U2 and ∆U denote the benefit
of doctor’s persuasion in market 1, market 2, and the whole market, respectively. By
(15),
∆U = −rmb[p(x− 1)− 1] +rmn
rm+ n(a− b)(p− q)
Define C1 as
C1 = {
√(a− b)(p− q)
b[p(x− 1)− 1]− 1}.
r =n
mC1
Define C2 as
C2 = −C1b[p(x− 1)− 1] +C1
C1 + 1(a− b)(p− q)
∆U =− C1nb[p(x− 1)− 1] +C1n
2
C1n+ n(a− b)(p− q)
=− C1nb[p(x− 1)− 1] +C1n
C1 + 1(a− b)(p− q)
=n{−C1b[p(x− 1)− 1] +C1
C1 + 1(a− b)(p− q)}
=C2n
To derive ∆U1 from ∆U , we only need to replace n, m, r with tn, rm, r1 in (15).
∆U1 = C2tn
37

∆U2 = C2(1− t)n
∆U = ∆U1 +∆U2
Thus, we would be done here.
Otherwise, r1 = 1. Define r′1 as
r′1 =t
rr.
r′1 ≥ 1
By (16), ∆U1 reaches its unique maximum at r1 = r′1,
∆U1
∣∣∣∣r1=r′1
≥ ∆U1
∣∣∣∣r1=1
= ∆U1
Since
∆U = C2n = ∆U1
∣∣∣∣r1=r′1
+∆U2,
∆U ≥ ∆U1 +∆U2
which concludes the discussion for this case.
Case 3: (a− b)(p− q) ≥ (m+nn
)2b[p(x− 1)− 1]
In this case,
r1 = r = 1.
By (15),
∆U = m{−rb[p(x− 1)− 1] +rn
rm+ n(a− b)(p− q)}
= −b[p(x− 1)− 1]m+nm
m+ n(a− b)(p− q)
Define C3 = b[p(x− 1)− 1], C4 = (a− b)(p− q) where
C4>0.
∆U = −C3m+ C4nm
m+ n
∆U1 = −C3rm+ C4rmtn
rm+ tn
Suppose r and t are such that r2 has reached corner solution r2 = 1.
∆U2 = −C3(1− r)m+ C4(1− r)m(1− t)n
(1− r)m+ (1− t)n
38

By Lemma 6,
∆U1+∆U2 = −C3m+C4[rmtn
rm+ tn+
(1− r)m(1− t)n
(1− r)m+ (1− t)n] ≤ −C3m+C4
nm
m+ n= ∆U
Otherwise, r2<1.
∆U2 = C2(1− t)n
∂U2
∂r= 0
Since r1 = 1, by (15)
∆U1 = −rmb[p(x− 1)− 1] +rmtn
rm+ tn(a− b)(p− q)
∂∆U1
∂r= −mb[p(x− 1)− 1] + (
tn
rm+ tn)2m(a− b)(p− q)
By the definition of r1 = 1,
(a− b)(p− q) ≥ (rm+ tn
tn)2b[p(x− 1)− 1]
(tn
tn+ rm)2(a− b)(p− q) ≥ b[p(x− 1)− 1]
Thus,∂∆U1
∂r≥ 0
∂∆U1 +∆U2
∂r≥ 0
As a result, the doctor would be better off increasing r for a given t. Since
r2 =(1− t)n
(1− r)mC1,
this process would increase r2 to the point where r2 = 1, which has been addressed
earlier.
B Omitted Proofs in Section 4
Lemma 10. If the market contains two types (H or L) of customers whose relative
amount N and willingness to pay v are represented by
H L
N NH NL
v vH vL,
39

and they all claim to be type L, the optimal price to charge would be
P =
vL, if 1
NHNL
(vHvL
−1)≥ 1,
vH , o.w.
Proof of Lemma 10. Charging vL is optimal if and only if
vL(NH +NL) ≥ NHvH
NLvL ≥ NH(vH − vL)
1 ≥ NH
NL
(vHvL
− 1)
1NH
NL(vHvL
− 1)≥ 1
Proof of Lemma 4. 1. Suppose π(L|H) ∈ [0,min[πm, πs]].
In market i = H (market 1),
Nij H L
S [1− π(L|H)]qn 0
M [1− π(L|H)]pm 0
where the doctor would easily extract the full surplus from him. For instance, the
doctor could reveal the truth and charge vHS and vHM accordingly. Or she could
persuade them together by always reporting j = S (or M) and charge vH = x qna+pmbqn+pm
.
That is to say, the patient would end up with zero utility if he reports H.
In market i = L (market 2) where
Nij H L
S π(L|H)qn n
M π(L|H)pm m.
Under an arbitrary persuasion strategy of the doctor, this market would be divided
into two groups j ∈ {S,M}. For j = S,
H L
Ni (tqn+ rpm)π(L|H) tn+ rm
vi x tqna+rpmbtqn+rpm
tna+rmbtn+rm
40

Thus,
NH(t, r) = (tqn+ rpm)π(L|H)
By the proof of Lemma 2,
min[πs, πm]
π(L|H)≤ π(t, r) ≤ max[πs, πm]
π(L|H)
(Notice here the setup is slightly different where NH is π(L|H) times what it used to
be in Lemma 2.) Since π(L|H) ≤ min[πm, πs],
π(t, r) ≥ min[πs, πm]
π(L|H)≥ 1.
By Lemma 10, the doctor would always charge vL. Due to
min(xa, xb) ≥ xb ≥ a ≥ tna+ rmb
tn+ rm= vL,
the type H patient’s willingness to pay is always above the price charged. The proof
for another group j = M is almost the same where you need to replace r and t with
1 − r and 1 − t. Thus, he will always obtain a positive surplus in market i = L. As
a result, end up being in market i = L (market 2) is always preferred over market
i = H (market 1), which means the patient’s utility is monotonically increasing in
π(L|H).
2. Suppose π(L|H)>max(πm, πs). By the proof of Lemma 2,
min[πs, πm]
π(L|H)≤ π(t, r) ≤ max[πs, πm]
π(L|H)<1.
By Lemma 10, the doctor would charge vH in market 2 (i = L) leaving zero surplus
for type H patient. He would thereby be wiser to choose 0<π(L|H) ≤ min(πm, πs)
so that she would charge vL in market i = L where he would fare better.
Proof of Lemma 5. Case 1: 1NHNL
(vHvL
−1)≥ 1
If the producer directly charge a single optimal price, she would charge vL by
Lemma 10. Thus, the surplus loss would be
U = −NH(vH − vL).
If we let the customer to persuade first,
π(L|H) = min[1
NH
NL(vHvL
− 1), 1] = 1
41

which indicates the same surplus loss for the producer because she would still charge
vL and we are done here.
Case 2: 1NHNL
(vHvL
−1)<1
If the producer directly charge a single optimal price, she would charge vH by
Lemma 10. Thus, the surplus loss would be
U = −NLvL.
If we let the customer to persuade first,
π(L|H) = min[1
NH
NL(vHvL
− 1), 1] =
1NH
NL(vHvL
− 1).
The doctor would charge vL and her surplus loss is
U = −NH1
NH
NL(vHvL
− 1)(vH − vL) = −NLvL.
Proof of Proposition 5. The doctor is going to face market i = L
Nij H L
S π(L|H)qn n
M π(L|H)pm m
to decide whether to persuade or not. We need to point out that this structure bears
quite the resemblance with what we encounter in Section 3, except that we need to
replace q and p in Section 3 with π(L|H)p and π(L|H)q. Furthermore, under any
persuasion strategy adopted by the doctor, Lemma 5 holds for any j (S or M). That
is to say, we could rely on propositions in Section 3 to analyze her strategy if we take
the nuance, π(L|H), into account.
Since the optimal π(L|H) satisfy (7)
πs ≤ π(L|H) ≤ πm
due to πs ≤ πm ≤ 1, for group j = S we have
1NHS
NLS(vHS
vLS− 1)
=1
(x− 1)π(L|H)q=
πs
π(L|H)≤ 1
while for group j = M we have
1NHM
NLM(vHM
vLM− 1)
=1
(x− 1)π(L|H)p=
πm
π(L|H)≥ 1.
42

πs
π(L|H)≤ 1 ≤ πm
π(L|H)
We shall first prove that the doctor will always tell the truth and then analyze
the patient’s choice.
Case 1: πm
π(L|H)= 1
In this case,πs
π(L|H)≤ πm
π(L|H)= 1.
By Lemma 5, we could rely on Proposition 1 which indicates that the doctor is
indifferent with any of her persuasion strategy. Thus, revealing the truth is obviously
one of her best response.
Case 2: πm
π(L|H)>1
In this case,πs
π(L|H)≤ 1<
πm
π(L|H).
By Lemma 5 and Proposition 3, the doctor strictly prefer to reveal the truth.
Given telling the truth as the doctor’s best response, if
πs<π(L|H) ≤ πm,
by Lemma 10 the doctor is going to charge vHS for patients under j = S in market
i = L because
1NHS
NLS(vHS
vLS− 1)
=1
(x− 1)π(L|H)q=
πs
π(L|H)<1.
But the doctor will charge vLM for patients under j = M in market i = L because
1NHM
NLM(vHM
vLM− 1)
=1
(x− 1)π(L|H)p=
πm
π(L|H)≥ 1.
If type H patient is in market i = H (see proof of Lemma 4) or stays in market i = L
under condition j = S, he will end up with zero surplus. However, he will fare better
if he end up being in market i = L under condition j = M . Therefore, the patient’s
utility is monotonically increasing with π(L|H) over the sub-range (πs, πm]. Thus,
π(L|H) = πm
dominates all the other choice of π(L|H) where π(L|H) ∈ (πs, πm]. Consequently,
only two choices left: π(L|H) = πm or π(L|H) = πs.
If the patient chooses π(L|H) = πs,
pm(πm − πs)(x− 1)b ≤ na
43

mb(1− πs
πm
) ≤ na
πs
πm
≥ 1− na
mb
Therefore, the patient’s optimal action would be
π(L|H) =
πs, if πs
πm≥ 1− na
mb,
πm, o.w.
Proof of Proposition 6. By (7), optimal π(L|H) satisfies
πm ≤ π(L|H) ≤ πs.
For group j = S we have
1NHS
NLS(vHS
vLS− 1)
=1
(x− 1)π(L|H)q=
πs
π(L|H)≥ 1
while for group j = M we have
1NHM
NLM(vHM
vLM− 1)
=1
(x− 1)π(L|H)p=
πm
π(L|H)≤ 1.
πm
π(L|H)≤ 1 ≤ πs
π(L|H)
As we mentioned earlier in Proposition 5, we could use the results in Section 3 to an-
alyze the doctor’s response once we replace their p and q with π(L|H)p and π(L|H)q,
which is assured by Lemma 5.
If πs
π(L|H)= 1,
πm
π(L|H)≤ πs
π(L|H)= 1
where we could rely on Proposition 1 which indicates that revealing the truth is
obviously one of her best response.
If πs
π(L|H)>1,
πm
π(L|H)≤ 1<
πs
π(L|H)
implying that we could use the result of Proposition 4 which illustrates the doctor’s
best response as
t = 1
44

r =
0, if (a− b)(p− q) ≤ b[p(x− 1)− 1
π(L|H)], (19)
1, if (a− b)(p− q) ≥ (m+ n
n)2b[p(x− 1)− 1
π(L|H)], (20)
n
m{√
(a− b)(p− q)
b[p(x− 1)− 1π(L|H)
]− 1}, o.w. (21)
which concludes the discussion for the doctor’s best response. Next, we analyze the
patient’s action.
First, we point out that the patient’s utility is monotonically increasing with
π(L|H) over the sub-range [πm, π1]. Suppose π(L|H) ∈ [πm, π1]. By the definition of
π1 in (4),
(a− b)(p− q) ≥ (m+ n
n)2b[p(x− 1)− 1
π(L|H)]
which indicates the doctor’s response is
r = 1
by (20). Therefore, market i = L becomes one group
H L
Ni π(L|H)(pm+ qn) n+m
vi xpmb+qnapm+qn
mb+nam+n
.
By the definition of r∗ in (12) and (13), we have
π(t, r)>1.
By Lemma 10, the doctor is about to charge vL. Since
xb ≥ a>mb+ na
m+ n= vL,
the patient always prefer market i = L over market i = H where he end up with zero
surplus (see proof of Lemma 4). Thus, his utility is monotonically increasing with
π(L|H) over the sub-range [πm, π1].
Second, we shall prove that the patient’s utility is monotonically increasing with
π(L|H) over the sub-range [π0, πs]. Suppose π(L|H) ∈ [π0, πs]. By the definition of
π0 in (5),
(a− b)(p− q) ≤ b[p(x− 1)− 1
π(L|H)]
which indicates the doctor’s response is
r = 0
45

by (19). Therefore, she will always reveal the truth and the market i = L is thereby
separate between two conditions. For group j = S, we have
1NHS
NLS(vHS
vLS− 1)
=1
(x− 1)π(L|H)q=
πs
π(L|H)≥ 1
where she charges vLS by Lemma 10. For group j = M , we have
1NHM
NLM(vHM
vLM− 1)
=1
(x− 1)π(L|H)p=
πm
π(L|H)<1,
since πm<π0 ≤ π(L|H) which is guaranteed by (6). Thus, she charges vHM . If the
patient stays in market i = H (see proof of Lemma 4), he will return home with zero
surplus. By contrast, if he is in market i = L, he might obtain positive surplus, since
he could be under condition S. Thus, his utility is monotonically increasing over the
sub-range [π0, πs].
Third, we shall prove that the patient’s utility is convex over sub-range π(L|H) ∈[π1, π0]. Suppose π(L|H) ∈ [π1, π0]. By (21), we have
(a− b)(p− q)(n
n+ rm)2 = b[p(x− 1)− 1
π(L|H)] (22)
(n+ rm)2[p(x− 1)− 1
π(L|H)]− a− b
b(p− q)n2 = 0
Define G(r, π(L|H)) as
G = (n+ rm)2[p(x− 1)− 1
π(L|H)]− a− b
b(p− q)n2
∂G
∂r= 2m(n+ rm)[p(x− 1)− 1
π(L|H)]
∂G
∂π(L|H)= [
n+ rm
π(L|H)]2
By implicit function theorem,
dr
dπ(L|H)= −
∂G∂π(L|H)
∂G∂r
= − 1
[π(L|H)p(x− 1)− 1]
n+ rm
2mπ(L|H)<0 (23)
where the inequality is due to π(L|H) ≥ π1>πm. Now we characterize the patient’s
gain uH from persuasion. Recall that only by staying in market 2 under j = S could
46

he obtain a positive gain. Define β = pq.
uH =π(L|H)qn+ pmr
qn+ pm(x
qna+ rpmb
qn+ rpm− na+ rmb
n+ rm)
=π(L|H)
qn+ pm[xqna+ xrpmb− na+ rmb
n+ rm(qn+ pmr)]
=π(L|H)
qn+ pm[xqna+ xrpmb− qnb− rpmb− n
a− b
n+ rm(qn+ pmr)]
=qπ(L|H)
qn+ pm[xna+ xrβmb− nb− rβmb− n
a− b
n+ rm(n+ βmr)]
=π(L|H)
n+mβ[xna− nb+ (x− 1)rβmb− βn(a− b) + n2 a− b
n+ rm(β − 1)]
Define Z(r) as
Z(r) = xna− nb+ (x− 1)rβmb− βn(a− b) + n2 a− b
n+ rm(β − 1). (24)
Thus,
uH =π(L|H)
n+mβZ(r). (25)
By (22),dZ(r)
dr= (x− 1)βmb−mn2 a− b
(n+ rm)2(β − 1) =
bm
π(L|H)q.
dZ(r)
dπ(L|H)=dZ(r)
dr
dr
dπ(L|H)
=bm
π(L|H)q
dr
dπ(L|H)
=− bm
q
1
[π(L|H)p(x− 1)− 1]
n+ rm
2mπ2(L|H)
=− b(n+ rm)
2π2(L|H)q
1
[π(L|H)p(x− 1)− 1]
=− b(n+ rm)
2π2(L|H)q
b(n+ rm)2
π(L|H)(a− b)(p− q)n2
=− b2
2n2q(a− b)(p− q)
(n+ rm)3
π3(L|H)
where the third equality is due to (23) while the fifth one derives from (22).
duH
dπ(L|H)=
1
n+ βm{Z(r) + π(L|H)
dZ(r)
dπ(L|H)}
=1
n+ βm{Z(r)− b2
2n2q(a− b)(p− q)
(n+ rm)3
π2(L|H)}
47

d2uH
dπ2(L|H)=
1
n+ βm{ dZ(r)
dπ(L|H)− b2
2n2q(a− b)(p− q)
d (n+rm)3
π2(L|H)
dπ(L|H)}
=1
n+ βm{− b2
2n2q(a− b)(p− q)
(n+ rm)3
π3(L|H)− b2
2n2q(a− b)(p− q)
d (n+rm)3
π2(L|H)
dπ(L|H)}
=1
n+ βm
b2
2n2q(a− b)(p− q){−(n+ rm)3
π3(L|H)−
d (n+rm)3
π2(L|H)
dπ(L|H)}
=1
n+ βm
b2
2n2q(a− b)(p− q){−(n+ rm)3
π3(L|H)+ 2
(n+ rm)3
π3(L|H)− 1
π2(L|H)
d(n+ rm)3
dπ(L|H)}
=1
n+ βm
b2
2n2q(a− b)(p− q){(n+ rm)3
π3(L|H)− 1
π2(L|H)
d(n+ rm)3
dπ(L|H)}
>0
where the second equality utilize the result from dZ(r)dπ(L|H)
while the inequality is guar-
anteed by (23). That is to say, patient’s utility is convex over sub-range π(L|H) ∈[π1, π0], which means his optimal choice over this sub-range is either π(L|H) = π1 or
π(L|H) = π0.
To sum up, the first, second and the third part indicates π(L|H) = π1, π(L|H) =
π1 orπ0, π(L|H) = πs as the optimal solution over the sub-range [πm, π1], [π1, π0],
[π0, πs], respectively. The best choice for him over the entire range [πm, πs] would be
either π(L|H) = π1 or π(L|H) = πs. If π(L|H) = π1,
uH =q
qn+ pmπ1Z(1)
by (25). If π(L|H) = πs,
uH =qn
qn+ pmπs(x− 1)a =
n
qn+ pma.
Thus, the optimal strategy for the patient would be
π(L|H) =
π1, if π1 ≥ naqZ(1)
≜ π∗,
πs, o.w.
where Z(r) is defined by (24). The best response of the doctor is t = 1,
r =
1, if π(L|H) = π1,
0, if π(L|H) = πs.
48

Proof of Proposition 7. Here, we have πs ≤ 1<πm. Besides,since the optimal π(L|H)
satisfy (7),
πs ≤ π(L|H) ≤ 1<πm.
πs
π(L|H)≤ 1<
πm
π(L|H).
As we discussed in the proof of Proposition 5, the doctor strictly prefer to reveal the
truth by Lemma 5 and Proposition 3. Since the patient’s utility is monotonically
increasing with π(L|H) over the sub-range (πs, 1]. Thus,
π(L|H) = 1
dominates all the other choice of π(L|H) where π(L|H) ∈ (πs, 1]. Consequently, only
two choices left: π(L|H) = πs or π(L|H) = 1.
If the patient chooses π(L|H) = πs,
pm(1− πs)(x− 1)b ≤ na
1− πs
πm
≤ na
mb
Therefore, the patient’s optimal action would be
π(L|H) =
πs, if 1−πs
πm≤ na
mb,
1, o.w.
Proof of Proposition 8. In the proof of Proposition 6, the patient’s utility is mono-
tonically increasing over the sub-range [πs, π1] and [π0, 1]. In addition, his utility is
convex over the sub-range [π1, π0]. We can directly borrow these results to simplify
our analysis here. The only difference is that in this case πs ≤ 1<πm which indicates
that the relative order of π1, π0 and 1 is undetermined and we shall address it case
by case.
Case 1: π1 ≥ 1
As in the proof of Proposition 6, the patient’s utility is increasing over π(L|H) ∈[πs, π1], which results in π(L|H) = 1 as the patient’s optimal choice. By the definition
of π1 in (4), π1 ≥ 1 indicates (a− b)(p− q) ≥ (m+nn
)2b[p(x− 1)− 1]. Since π(L|H) ≤1 ≤ π1, by (20) we have
t = r = 1
as the doctor’s best response.
49

Case 2: π1<1<π0
By the definition of π1 and π0 in (4) and (5), π1<1<π0 indicates b[p(x− 1)− 1] ≤(a− b)(p− q)<(m+n
n)2b[p(x− 1)− 1]. As in the proof of Proposition 6, the patient’s
utility is convex over the sub-range π(L|H) ∈ [π1, π0]. Thus, the patient would choose
either π(L|H) = π1 or π(L|H) = 1 as the optimal choice.
By (25), if π(L|H) = π1,
uH =q
qn+ pmπ1Z(1).
If π(L|H) = 1,
uH =q
qn+ pmZ(
n
m{
√(a− b)(p− q)
b[p(x− 1)− 1]− 1}).
Thus, the optimal strategy for the patient would be
π(L|H) =
π1, if π1 ≥Z( n
m{√
(a−b)(p−q)b[p(x−1)−1]
−1})Z|r=1
≜ π∗∗,
1, o.w.
where Z(r) is defined by (24).
By (20) and (21), the doctor’s best response is t = 1,
r =
1, if π(L|H) = π1,
nm{√
(a−b)(p−q)b[p(x−1)−1]
− 1}, if π(L|H) = 1.
Case 3: π0 ≤ 1
By the definition of π0 in (5), π0 ≤ 1 indicates (a − b)(p − q)<b[p(x − 1) − 1].
As in the proof of Proposition 6, the patient would choose either π(L|H) = π1 or
π(L|H) = 1 as the optimal choice.
By (25), if π(L|H) = π1,
uH =q
qn+ pmπ1Z(1).
If π(L|H) = 1,
uH =qn
qn+ pm(x− 1)a.
Thus, the optimal strategy for the patient would be
π(L|H) =
π1, if π1 ≥ π∗
πs,
1, o.w.
50

By (19) and (20), the doctor’s best response is t = 1,
r =
1, if π(L|H) = π1,
0, if π(L|H) = 1.
C Omitted Proofs in Section 7.1
Lemma 11. Given patient moves (π(L|H)) first, if p>q and π1<1, the doctor’s gain
from her persuasion strategy is monotonically decreasing with π(L|H) over the sub-
range [π1,min(π0, 1)].
Proof of Lemma 11. Suppose π(L|H) ∈ [π1,min(π0, 1)]. The doctor’s gain from her
persuasion is delivered by (15). If the patient’s first move π(L|H) is taken into account
in market i = L (we need to replace p and q with π(L|H)p and π(L|H)q),
∆U = −rmb[π(L|H)p(x− 1)− 1] +rmn
rm+ n(a− b)(p− q)π(L|H).
Since r(π(L|H)) is the unique maximizer given π(L|H), by envelope theorem
d∆U
dπ(L|H)=
∂∆U
∂π(L|H)
∣∣∣∣r=r(π(L|H))
=− rmbp(x− 1) +rmn
rm+ n(a− b)(p− q)
=rm[−bp(x− 1) +n
rm+ n(a− b)(p− q)]
By (22),
n
n+ rm=
√b[p(x− 1)− 1
π(L|H)]
(a− b)(p− q)
d∆U
dπ(L|H)= rm[−bp(x− 1) +
√b[p(x− 1)− 1
π(L|H)](a− b)(p− q)] (26)
b[p(x− 1)− 1
π(L|H)](a− b)(p− q)<bp(x− 1)(a− b)(p− q)
≤bp(x− 1)(xb− b)(p− q)
<b2p2(x− 1)2
where the first inequality derives from π(L|H)>πm and the second one is due to
xb ≥ a. Thus, √b[p(x− 1)− 1
π(L|H)](a− b)(p− q)<bp(x− 1)
51

By (26),d∆U
dπ(L|H)<0.
Lemma 12. Given doctor moves first, if p>q and π1<1, the doctor’s gain from her
persuasion strategy is equivalent to the type H patient’s loss incurred by the doctor’s
persuasion.
Proof of Lemma 12. Suppose doctor moves first. By Lemma 1, the optimal persua-
sion strategy for the customer would be
π(L|H) = min[π(t, r), 1].
We need to point out that the type H patient’s gain by his persuasion strategy derives
from the doctor. Recall that if doctor moves first, the L type patient will always accept
the deal with zero surplus left. That is to say, their situation will remain the same
with or without type H patient’s persuasion. However, type H patient will always
accept the deal as well. If he gains some surplus by his persuasion, this gain must
derives from the doctor. By the proof of Lemma 3, the doctor’s loss is
U = −NH(t, r)π(L|H)∆v(t, r)
which is exactly the type H patient’s gain ∆uH by his persuasion
∆uH = NH(t, r)π(L|H)∆v(t, r).
Thus, if the doctor would somehow benefit from her persuasion, her gain must comes
from the type H patient. To be more specific, she gains some surplus by reducing
her loss which is caused by the patient’s action. By the proof of Lemma 8, if doctor
reveals the truth,
U = −qn(x− 1)a−mb.
If she optimally persuades,
U ′ = −(qn+ rpm)∆v(1, r)− (1− r)mb
Therefore, her gain from persuasion U ′ − U is the type H patient’s loss
U ′ − U = −(∆uH ′ −∆uH)>0.
52

Lemma 13. Suppose p>q, π1<1. If we switch the setup from the doctor first to
patient first,
1. the type H patient is strictly worse off.
2. the doctor is at least as good as before.
Proof of Lemma 13. In this proof, we shall construct a new model which acts as a
bridge between two setups. Since this lemma is critical for the proof of the next
theorem, we will elaborate this one here in detail.
The Model
There are two types of patients H or L on the market.
N i = i = H i = H, i = L i = i = L
j = S [1− π(L|H)]qn π(L|H)qn n
j = M [1− π(L|H)]pm π(L|H)pm m.
In the first period, the patient reports his type through i by Bayesian persuasion. In
the second period, the doctor persuades i = L patient. (There is no need to persuade
the i = H patient, since she could easily extract the full surplus by the proof of
Lemma 4). In the third period, type i = H, i = L patient could choose to turn
back to i = i = H (to eat their words) with some positive probability to guarantee
that vL(t, r) (vL(1− t, 1− r)) will be charged instead of vH(t, r) (vH(1− t, 1− r)) in
the corresponding sub-market. In the fourth period, the doctor chooses an optimal
price to charge in sub-markets i = L, j = S and i = L, j = M , which concludes our
fictitious model.
Our first setup where the doctor moves first is equivalent to this fictitious model
where π(L|H) = 1. Suppose π(L|H) = 1. The doctor is going to face
Nij H L
S qn n
M pm m
and persuades them. Then what happens in the third period in our fictitious model
is the patient’s persuasion at work.
On the other hand, our second setup is the same as our fictitious model if we
restrain type i = H, i = L patient from his action in the third period. That is, he has
no right to turn back on his words and the doctor is going to charge immediately.
Now we analyze our fictitious model. Let uHk and Uk denote the type H patient
and the doctor’s utility in the following step k. Notice they are functions of π(L|H).
We focus our attention on the sub-range π(L|H) ∈ [π1, 1].
53

In step 1, suppose we restrict the doctor from persuasion in the second period. If
so, uH1 is strictly increasing with π(L|H) over the sub-range [0,min(πs, 1)] and remains
a constant over [min(πs, 1), 1]. The logic is straightforward. If π(L|H) ∈ [0, πm], he
strictly benefits from π(L|H) regardless of his condition. If π(L|H) ∈ [πm,min(πs, 1)],
he would be strictly better off under condition S. Otherwise, π(L|H) ∈ [min(πs, 1), 1],
increasing π(L|H) is futile, since either π(L|H) = 1 ≤ πs reaches its corner solution or
πs<1 implies that all the increment over πs needs to be offset in the third period due
to π(L|H) ≥ πs>πm. On the other hand, U1 is strictly decreasing over [0,min(πs, 1)]
and remains a constant over [min(πs, 1), 1].
In step 2, we relax the restriction and allow the doctor to persuade in the second
period. Notice that this would make a difference only over [π1,min(π0, 1)] where the
doctor does persuade by (19), (20), (21) and the definition of π1 and π0 in (4), (5).
By Lemma 11, the doctor’s gain from her persuasion ∆U is strictly decreasing over
the sub-range [π1,min(π0, 1)] and becomes zero over [min(π0, 1), 1]. Thus,
U2 = U1 +∆U
is strictly decreasing over [π1,min(πs, 1)] and remains a constant over [min(πs, 1), 1]
due to πm<π1<π0 ≤ πs. On the other hand, the type H patient’s loss incurred by
her persuasion is the same as ∆U by Lemma 12, which means
uH2 = uH
1 −∆U
is strictly increasing over [π1,min(πs, 1)] and remains a constant over [min(πs, 1), 1].
In step 3, we restrain the patient from turning back to i = i = H (eating his
words) in period 3 to mirror our second setup. If so, this would have no effects on
the doctor’s utility over the sub-range [π1, 1] by Lemma 5. Thus,
U3 = U2.
By contrast, this would have a significant impact on the patient side. By (21), the
doctor would persuade the patient with π(S|M) = r over π(L|H) ∈ [π1,min(π0, 1)].
For those who left in j = M , she will charge vHM due to π(L|H)>πm by Lemma 10.
Therefore, it would incur welfare loss (1− r)mb for the type H patient by Lemma 1.
For π(L|H) ∈ [π0, 1] if π0<1, his welfare loss is mb with r = 0.
uH3 = uH
2 − (1− r)mb
.
54

Since it must be one of π1<1 ≤ πs, πs<1, we shall compare both players’ welfare
under two setups case by case.
Case 1: π1<1 ≤ πs
In this case, the type H patient will choose either π1 or 1 when he moves first.
If he chooses π1 under the second setup, then his welfare is strictly getting worse
than the first setup (doctor first), since
uH3 (π1) = uH
2 (π1)<uH2 (1)
while type L patient remains the same. In addition, the doctor is strictly better than
when she moves first
U3(π1) = U2(π1)>U2(1)
If he chooses 1 under the second setup, then his welfare is strictly getting worse
than the first setup (doctor first), since
uH3 (1) = uH
2 (1)− (1− r)mb<uH2 (1)
while type L patient under j = M gives up the transaction. In addition, the doctor’s
welfare remains the same
U3(1) = U2(1)
Case 2: πs<1
In this case, the type H patient will choose either π1 or πs when he moves first.
If he chooses π1 under the second setup, then his welfare is strictly getting worse
than the first setup (doctor first), since
uH3 (π1) = uH
2 (π1)<uH2 (1)
while type L patient remains the same. In addition, the doctor is strictly better than
when she moves first
U3(π1) = U2(π1)>U2(1)
If he chooses πs under the second setup, then his welfare is strictly getting worse
than the first setup (doctor first), since
uH3 (πs) = uH
2 (πs)−mb = uH2 (1)−mb<uH
2 (1)
while type LM patient gives up the transaction due to r = 0. In addition, the doctor’s
welfare remains the same
U3(πs) = U2(πs) = U2(1)
55

Proof of Theorem 1. We shall address this issue case by case, including double full
persuasion, double partial persuasion, single full persuasion. In the Section 4.2, we
have seen that there is no difference between those two setups under double full
persuasion (πm>1, πs>1). For the following part, we shall address another two cases.
We shall go through this proof by switching from the first setup where doctor moves
first to the second setup to see how the welfare of both parties change accordingly.
Case 1: Double Partial Persuasion p ≤ q
In this case, πs ≤ πm ≤ 1. First, suppose doctor moves first. By Lemma 3, her
utility is
U = −na−mb.
By proposition 5, if we switch to the second setup, the doctor will always prefer to
reveal the truth and the patient shall choose either π(L|H) = πs or π(L|H) = πm.
If he chooses π(L|H) = πs (see the proof of Proposition 5 for the condition under
which he does so), the doctor would charge vLS and vLM for those under condition S
and M , respectively, by Lemma 10. Thus, her utility is higher
U = −na− pmπs(x− 1) ≥ −na−mb,
since πs ≤ πm ≤ 1. Meanwhile, type H patient’s utility is lower and type L patient
remains the same.
If he chooses π(L|H) = πm (see the proof of Proposition 5 for the condition under
which he does so), the doctor would charge vHS and vLM for those under condition
S and M , respectively, by Lemma 10. Thus, her utility is the same as before
U = −na−mb,
since πs ≤ πm ≤ 1. Meanwhile, type LS patient gives up the transaction and type LM
patient remains the same. The type H patient is strictly worse than before because
the doctor’s income does not change and some type L patients quit the transaction.
Case 2: Double Partial Persuasion p>q
In this case, πm<πs ≤ 1. Since π1<πs ≤ 1, by Lemma 13, the type H patient is
strictly worse off and the doctor is weakly better than setup 1.
Case 3: Single Full Persuasion p ≤ q
In this case, πs ≤ 1<πm. This case is quite similar to the case 1. First, suppose
doctor moves first. By proof of Lemma 1, her utility is
U = −na− pm(x− 1)b.
56

By proposition 7, if we switch to the second setup, the doctor will always prefer
to reveal the truth and the patient shall choose either π(L|H) = πs or π(L|H) = 1.
If he chooses π(L|H) = πs (see the proof of Proposition 7 for the condition under
which he does so), the doctor would charge vLS and vLM for those under condition S
and M , respectively, by Lemma 10. Thus, her utility is higher
U = −na− pmπs(x− 1)b ≥ −na− pm(x− 1)b,
since πs ≤ 1<πm. Meanwhile, type H patient’s utility is lower and type L patient
remains the same.
If he chooses π(L|H) = 1 (see the proof of Proposition 7 for the condition under
which he does so), the doctor would charge vHS and vLM for those under condition
S and M , respectively, by Lemma 10. Thus, her utility is the same as before
U = −na− pm(x− 1)b,
since πs ≤ 1<πm. Meanwhile, type LS patient gives up the transaction and type LM
patient remains the same. The type H patient is strictly worse than before because
the doctor’s income does not change and some type L patients quit the transaction.
Case 4: Single Full Persuasion p>q
In this case, πm ≤ 1<πs.
If π1 ≥ 1 which indicates (a− b)(p− q) ≥ (m+nn
)2b[p(x− 1)− 1], those two setups
are exactly the same. By Proposition 4, if doctor moves first, r = 1 and π(L|H) = 1.
By the proof of Proposition 6, if patient moves first, his utility is strictly increasing
with π(L|H) over the sub-range [πm, π1], which implies π(L|H) = 1, r = 1.
Otherwise, π1<1. By Lemma 13, the type H patient is strictly worse off and the
doctor is weakly better than before.
D Omitted Proofs in Section 5
Let π(t, r) denote 1NH (t,r)
NL(t,r)(vH (t,r)
vL(t,r)−1)
in those two groups created by the doctor’s signal.
π(t, r) =1
x tqna+rpmbtqn+rpm
tn+rmtna+rmb
− 1· tn+ rm
tqn+ rpm(27)
π(t, r) only relies on tr. Therefore, we take the limit and define
π(0, 0) = π(1, 1).
57

The intuition is simple. For strategy t = r = 1, it is exactly the same as t = r = 0.3
that pooling into one group is the same as pooling into one and further divide to two
homogenous groups.
Proof of Proposition 9. Since the patient sends his signal after the doctor’s signal,
his best response for commitment is just π(t, r) and π(1 − t, 1 − r) for those two
realizations of j, respectively. If p = q, it degenerates to a trivial case and the result
is obvious. Now we focus on p = q.
First, suppose π(t, r) = π(1−t, 1−r). Without loss of generality, let π(t, r)>π(1−t, 1 − r). Given the patient’s best response, the doctor would sustain full loss by
Lemma 3 and always has incentive to switch t and r with 1− t and 1− r, i.e., swap
those two groups. After swapping, patient only commit π(1− t, 1− r) in group t, r.
Since
π(1− t, 1− r)<π(t, r),
it would generate a strict positive gain for the doctor relative to full loss
∆U = (tqn+ rpm)[π(t, r)− π(1− t, 1− r)]∆v(t, r).
In another group, doctor’s surplus remains the same. Thus, she would deviate to
profit.
Second, suppose π(t, r) = π(1 − t, 1 − r). This case is identical to the situation
where the doctor would pool all the patient together. Given the patient’s best re-
sponse, the doctor would deviate to fully separating strategy. After that, patient only
commit π(t, r) in group S and group M . Since
π(t, r)<max(πs, πm),
the logic is the same and she would deviate to fully separate the patient to profit.
Proof of Proposition 11. First, suppose π(t, r) = π(1 − t, 1 − r). Without loss of
generality, let π(t, r)>π(1− t, 1− r). If π(1− t, 1− r)<1, the doctor will always have
incentive to swap two groups, since she will gain a strict positive surplus
∆U = (tqn+ rpm)[min[1, π(t, r)]− π(1− t, 1− r)]∆v(t, r).
If π(1− t, 1− r) ≥ 1, the patient would choose π(L|H) = 1. Given π(L|H) = 1, the
doctor would choose to reveal the truth (fully separate patients). To see this, notice
in Proposition 3, patient’s strategy is
π(L|H) =
1, if j = M,
πs, o.w.
58

However, for the doctor, this is identical to
π(L|H) =
1, if j = M,
1, o.w.
Therefore, by Proposition 3, the doctor would choose to reveal the truth. Conse-
quently, t = 0 and r = 1 would render π(1− t, 1− r)<1, a contradiction.
Second, suppose π(t, r) = π(1 − t, 1 − r). If π(1, 1)<1, π(L|H) = π(t, r) =
π(1, 1)<1. Given π(L|H)<1, the doctor would sustain full loss and would deviate to
fully separating the patient. By doing so, she could gain
∆U = pm(πm − π(1, 1))∆v(0, 1)
relative to full loss. If π(1, 1) ≥ 1, π(L|H) = 1. Given π(L|H) = 1, the doctor would
choose to reveal the truth, a deviation from π(t, r) = π(1− t, 1− r).
Proof of Proposition 12. First, suppose π(t, r) = π(1 − t, 1 − r). Without loss of
generality, let π(t, r)>π(1− t, 1− r). If π(1− t, 1− r)<1, by the proof of Proposition
11, the doctor would deviate to swap two groups. If π(1 − t, 1 − r) ≥ 1, the patient
would choose π(L|H) = 1. Given π(L|H) = 1, the doctor would choose
r =
0, if (a− b)(p− q) ≤ b[p(x− 1)− 1],
1, if (a− b)(p− q) ≥ (m+nn
)2b[p(x− 1)− 1],
nm{√
(a−b)(p−q)b[p(x−1)−1]
− 1}, o.w.
by Proposition 4. However, all these cases would violate either π(t, r) = π(1−t, 1−r)
or π(1− t, 1− r) ≥ 1. Thus, no equilibrium.
Second, suppose π(t, r) = π(1 − t, 1 − r). If π(t, r) = π(1, 1)<1, π(L|H) =
π(t, r)<1. Given π(L|H)<1, the doctor would deviate to fully separating the patient
by the proof of Proposition 11. If π(1, 1) ≥ 1, π(L|H) = 1. Given π(L|H) = 1,
equilibrium exists if and only if the doctor chooses r = 1. Therefore, by Proposition
4, the unique equilibrium only exists under condition (a− b)(p− q) ≥ (m+nn
)2b[p(x−1)− 1].
Proof of Proposition 14. First, suppose π(t, r) = π(1 − t, 1 − r). Under t = r, the
patient would choose π(L|H) = π(t, r) = π(1, 1). Given π(L|H) = π(1, 1), the doctor
would deviate to fully separating strategy to obtain a strictly positive gain
∆U = qn[πs − π(1, 1)]∆v(1, 0)
59

relative to full loss. Thus, she will deviate to profit.
Second, suppose π(t, r) = π(1−t, 1−r). Without loss of generality, let π(t, r)>π(1−t, 1− r) (i.e., t>r). Facing this, the patient would choose either π(L|H) = π(t, r) or
π(L|H) = π(1− t, 1− r). We shall address this issue case by case.
Case 1: π(L|H) = π(1− t, 1− r)
In this case, the doctor would deviate to pooling the patient into one group if and
only if
(tqn+rpm)[π(t, r)−π(1−t, 1−r)]∆v(t, r)<(qn+pm)[π(1, 1)−π(1−t, 1−r)]∆v(1, 1)
(tna+ rmb)[1− π(1− t, 1− r)
π(t, r)]<(na+mb)[1− π(1− t, 1− r)
π(1, 1)]
na+mb
π(1, 1)<tna+ rmb
π(t, r)+
(1− t)na+ (1− r)mb
π(1− t, 1− r)
By (27),
(na+mb)[xqna+ pmb
na+mb− qn+ pm
n+m]<(tna+ rmb)[x
tqna+ rpmb
tna+ rmb− tqn+ rpm
tn+ rm]
+(t′na+ r′mb)[xt′qna+ r′pmb
t′na+ r′mb− t′qn+ r′pm
t′n+ r′m]
where we use t′ and r′ to denote 1− t and 1− r.
(na+mb)qn+ pm
n+m>(tna+ rmb)
tqn+ rpm
tn+ rm+ (t′na+ r′mb)
t′qn+ r′pm
t′n+ r′m
By Lemma 6,
(na+mb)(qn+ pm)mn(t− r)2
n+m>(t′n+ r′m)[qnna(t− r)t+ pmmb(r − t)r]
+(tn+ rm)[qnna(t′ − r′)t′ + pmmb(r′ − t′)r′]
(na+mb)(qn+ pm)mn(t− r)
n+m>(t′n+ r′m)[qnnat− pmmbr]
+(tn+ rm)[−qnnat′ + pmmbr′]
(na+mb)(qn+ pm)mn(t− r)
n+m>naqmn(tr′ − t′r) +mbpmn(tr′ − rt′)
(na+mb)(qn+ pm)
n+m>naq +mbp
mnap+mnbq>mnaq +mnbp
ap− aq>bp− bq
a>b
60

which is satisfied trivially. Therefore, the doctor would deviate to pooling the patient
together. No equilibrium under this case.
Case 2: π(L|H) = π(t, r)
If π(t, r)<πs, the doctor would deviate to fully separating the patient, since she
would obtain a strictly positive gain
∆U = qn[πs − π(t, r)]∆v(1, 0).
With π(t, r) = πs (i.e., t = 1, r = 0), the doctor would have no incentive to deviate.
We need to check if π(L|H) = πs is indeed the patient’s best response given t = 1, r =
0.
The patient would choose π(L|H) = πs if and only if
qn[πs − πm](x− 1)a ≥ mb
na(1− πm
πs
) ≥ mb
πm
πs
≤ 1− mb
na
Proof of Proposition 16. First, suppose π(t, r) = π(1 − t, 1 − r). Under t = r, the
patient would choose π(L|H) = min[1, π(t, r)]. If π(t, r)<1, given π(L|H) = π(t, r),
the doctor would sustain full loss and have incentive to deviate to fully separating
strategy (t = 1, r = 0) to obtain a strictly positive gain
∆U = qn[πs − π(t, r)]∆v(1, 0)
relative to full loss. Thus, she will deviate to profit. If π(t, r) ≥ 1, given π(L|H) = 1,
the doctor’s best response is characterized in Proposition 8. Thus, only if π1 ≥ 1 that
equilibrium would exist in this case. Otherwise, the doctor would deviate to r<1, a
deviation for t = r. Under π1 ≥ 1, unique equilibrium exists such that π(L|H) = 1
and t = r = 1.
Second, suppose π(t, r) = π(1−t, 1−r). Without loss of generality, let π(t, r)>π(1−t, 1 − r) (i.e., t>r). Facing this, the patient would choose π(L|H) = π(t, r) or
π(L|H) = π(1− t, 1− r) or π(L|H) = 1. We shall address this issue case by case.
Case 1: π(L|H) = π(1− t, 1− r)<1
If π(t, r) ≤ 1, the doctor would deviate to fully pooling strategy by the proof of
Proposition 14.
61

Besides, if π(t, r)>1 or π(1, 1)>1, the same logic still holds and the corner solution
does not bite our previous proof in Proposition 14 whatsoever. The reason is that we
only consider the doctor’s surplus relative to full loss. Thus, the doctor would deviate
to fully pooling strategy (t = r) no matter what. No equilibrium as a result.
Case 2: π(L|H) = π(t, r)<1
Facing π(L|H) = π(t, r)<1, the doctor would sustain full loss and have incentive
to deviate to fully separating strategy t = 1, r = 0 to gain a strictly positive gain
∆U = qn[πs − π(t, r)]∆v(1, 0).
No equilibrium as a result.
Case 3: π(L|H) = 1
Facing π(L|H) = 1, the doctor’s best response is characterized in Proposition 8.
The equilibrium exists if and only if π(L|H) = 1 is indeed the patient’s best response.
If π1<1<π0, the patient would choose π(L|H) = 1 instead of π(L|H) = πm if and
only if1− πm
n+mβ· Z(r) ≥ pm(1− r)
pm+ qnπm(x− 1)b
by (11).
(1− πm)Z(r) ≥mb(1− r)
q
πm ≤ 1− mb(1− r)
qZ(r)≜ Π∗
If π0 ≤ 1, the patient would choose π(L|H) = 1 instead of π(L|H) = πm if and
only if
qn(1− πm)(x− 1)a ≥ mb
1− πm
πs
≥ mb
na
E Omitted Proofs in Section 7.2
Proof of Theorem 2. From Section 5, equilibrium exists only under three cases. Case
1. πs = πm ≤ 1. Case 2. πs>1, πm>1. Case 3. πs>1, πm ≤ 1, π1 ≥ 1.
By Proposition 9 and Proposition 13, if p = q, for two setups equilibrium re-
mains the same where π(L|H) = πs(= πm) and the doctor is indifferent between her
persuasion strategy.
62

By Proposition 10 (Proposition 12) and Section 6.2 (Proposition 16), it is clear
that for two setups equilibrium (if exists) remains the same where t = r = 1 and
π(L|H) = 1.
F Omitted Proofs in Section 7.3
Proof of Theorem 3. The proof follows directly from the comparison between Propo-
sition 2 and Proposition 10; Proposition 4 and Proposition 12; Proposition 1 and
Proposition 9.
Proof of Theorem 4. By the comparison between Proposition 5 and Proposition 13,
Proposition 7 and Proposition 15, Section 4.2 and Section 6.2, the equilibrium remains
the same for those two setups. Only two cases left: 1. πm<πs ≤ 1. 2. πm ≤1<πs, π1<1.
Case 1: πm<πs ≤ 1
By the proof of Proposition 6, the patient would choose between two corner so-
lutions π(L|H) = π1 or π(L|H) = πs in sequential-commitment game. However, by
Proposition 14, equilibrium only exists for π(L|H) = πs in simultaneous-commitment
game.
If the patient chooses π(L|H) = π1 in sequential-commitment game, his utility
would be at least as good as choosing π(L|H) = πs which is the action he takes
in simultaneous-commitment game. Otherwise, his utility is the same for those two
setups. Therefore, the patient weakly prefers sequential game where his choice set is
larger.
If the patient chooses π(L|H) = π1 instead of π(L|H) = πs in sequential-commitment
game, the doctor’s surplus will increase as well due to the monotonicity of U3 (see the
Proof of Lemma 13). That is to say, the doctor also weakly prefers sequential setup.
Case 2: πm ≤ 1<πs, π1<1
The logic is the same as Case 1 that the patient would choose between two corner
solutions of π(L|H) under sequential-commitment setup. If he chooses the smaller
one, both players’ payoff would be higher in sequential-commitment game than in the
simultaneous-commitment one.
63