Embed Size (px)
Citation preview
Wrist and Forearm Injuries
Rebecca Burton-MacLeod
R2, Emergency Medicine
July 29, 2004

Anatomy of the wrist
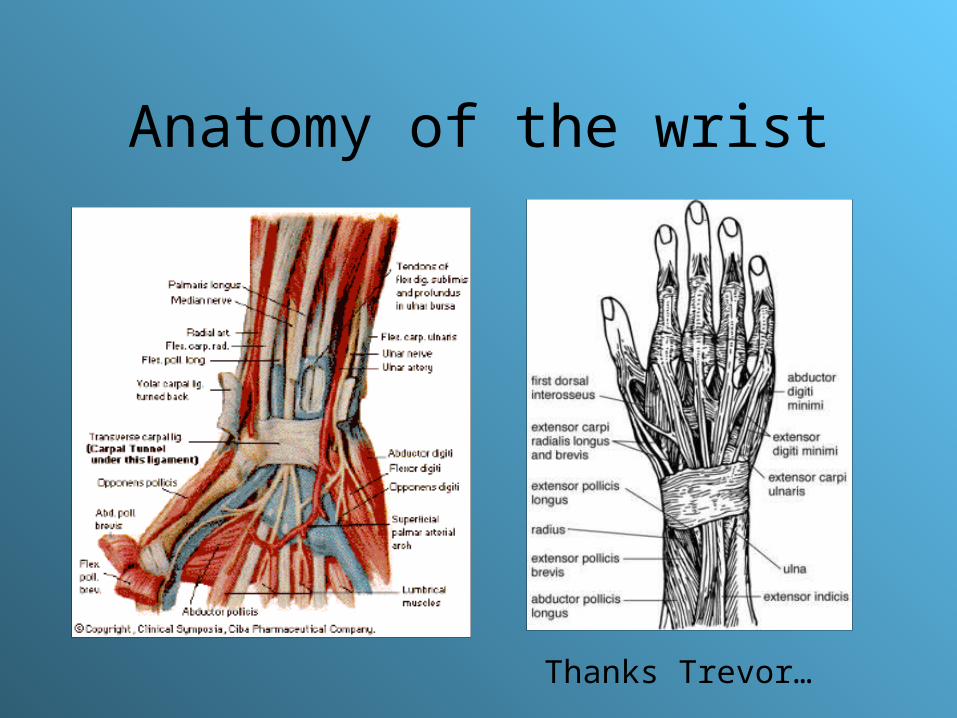
Anatomy of the wrist
Thanks Trevor…

Anatomy of the forearm
• Volar compartment:– Flexors
– pronators
•Dorsal compartment:
–Extensor muscles

History and physical
• History– Mechanism
– Point of maximal pain
• Physical– Inspection
– Palpation (Lister’s tubercle, snuffbox, ulnar styloid)
– ROM
– Neurovascular (document presence of radial/ulnar/brachial pulses and radial/median/ulnar nerves)

Case
• 19y.o. male presents to ED after partying all night. Fell down stairs, can’t quite remember how he landed. But c/o pain “in the wrist”. O/E right wrist is swollen and diffusely tender over dorsum distal radius and lunate. Otherwise normal exam. – You decide to order xrays and xray tech wants
to know what views you want?

Xrays
• 3 main views:– PA– Lateral– Oblique
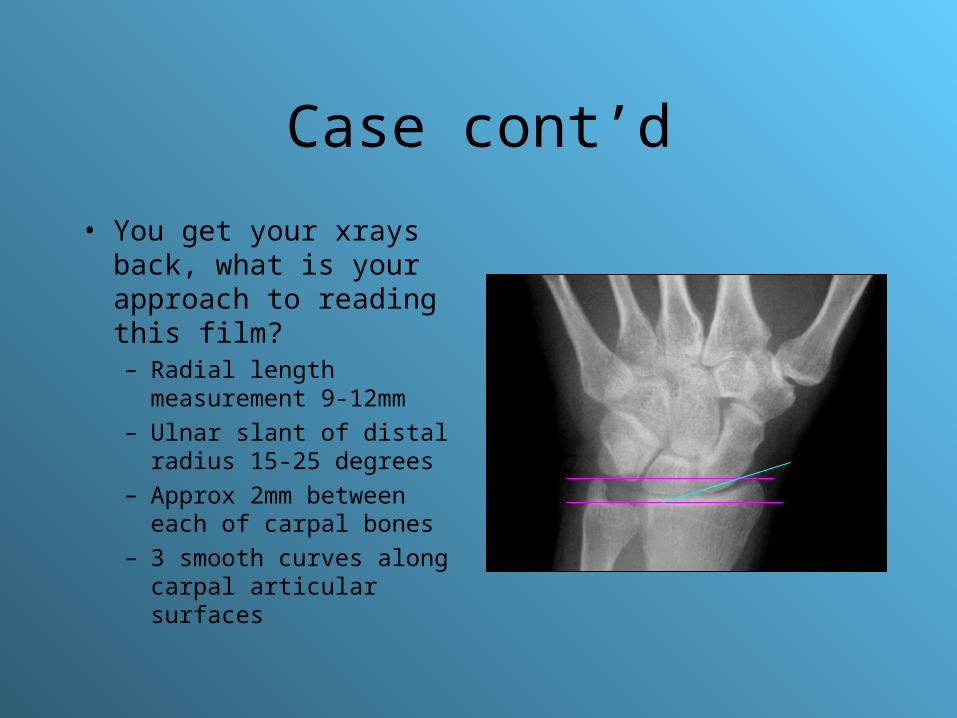
Case cont’d
• You get your xrays back, what is your approach to reading this film?– Radial length measurement
9-12mm
– Ulnar slant of distal radius 15-25 degrees
– Approx 2mm between each of carpal bones
– 3 smooth curves along carpal articular surfaces
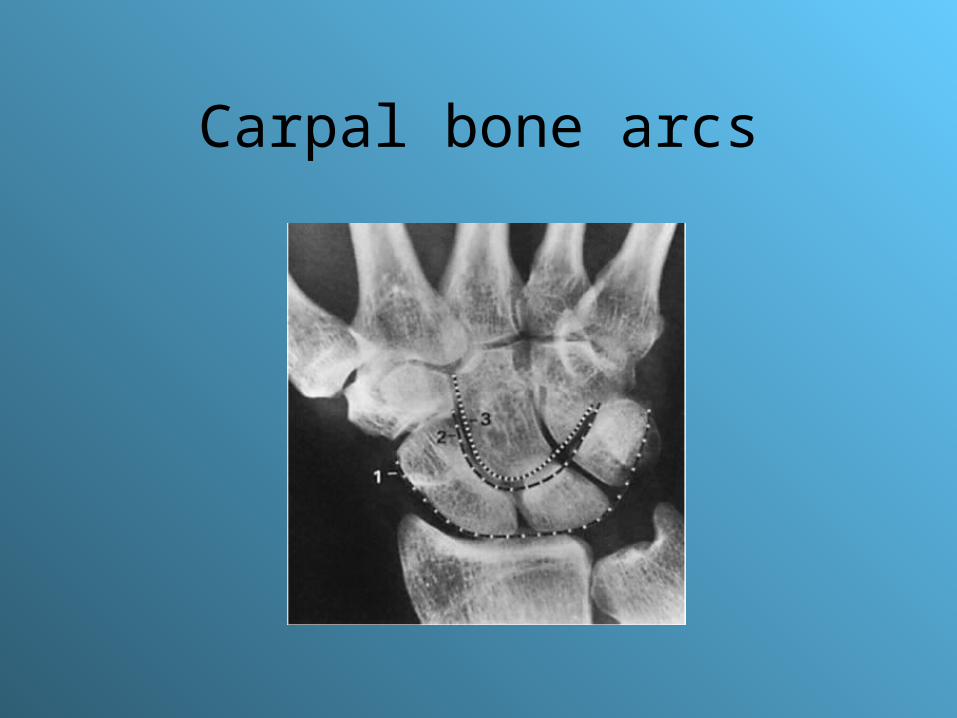
Carpal bone arcs
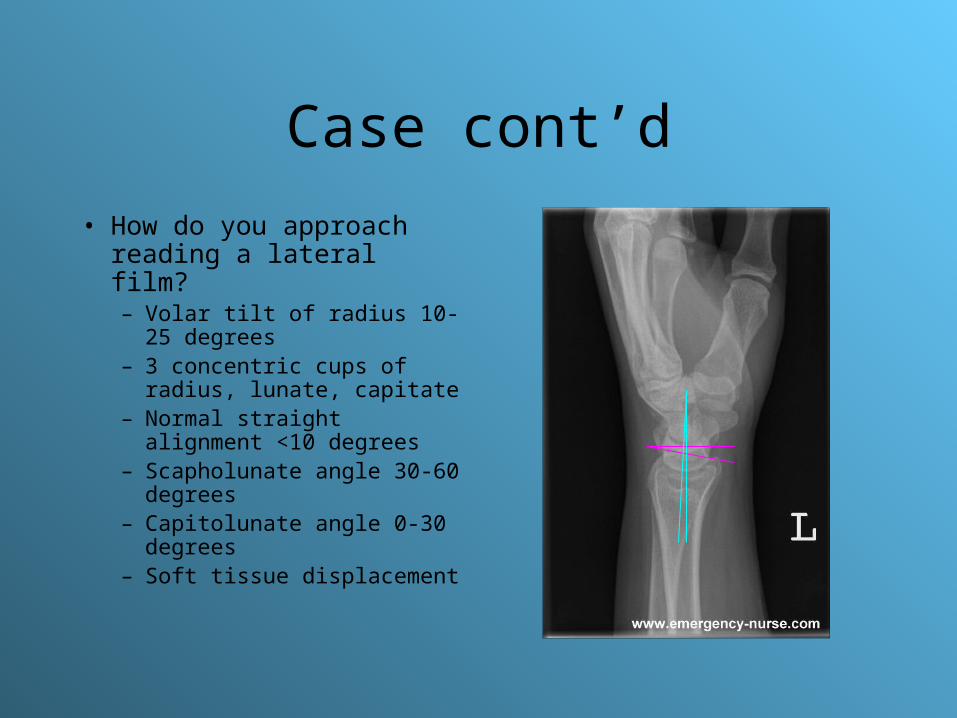
Case cont’d
• How do you approach reading a lateral film?– Volar tilt of radius 10-25
degrees– 3 concentric cups of radius,
lunate, capitate– Normal straight alignment
<10 degrees– Scapholunate angle 30-60
degrees– Capitolunate angle 0-30
degrees– Soft tissue displacement

Case
• 27y.o. M was hit with hockey stick across right arm and has swollen mid forearm. Tender over entire length of ulna.
• What views do you want?– AP and lat
• Anything else you want to make sure is included in xrays?– Joint above and below #

Case cont’d
• How would you determine if proximal radius is appropriately aligned?– Line through prox
radial shaft and head should intersect capitellum

Carpal injuries

Scaphoid #
• Makes up 60% of carpal bone #
• MoI: FOOSH
• # through waist of scaphoid most common
• Risks of AVN due to distal source of blood supply (3%)
• 17% of pts have associated # in wrist/forearm

Scaphoid complications

Scaphoid complications
• Nonunion, arthritis, AVN, collapse of pole, settling of capitate into proximal row
• Post-surgical proximal carpectomy
Case
• 27y.o. M presents to ED after falling off mountain bike. Swelling and pain in left wrist. On exam, how would you identify scaphoid #?– Tenderness over snuffbox, tenderness over
scaphoid tubercle, pain with axial compression of MC jt, pain with resisted supination

Case cont’d
• Anything noticeable on xray?
Case cont’d
• What if xray were completely normal, but worrisome exam?– 15% of scaphoid # do not show up on xray– If clinically suspicious then cast immobilization
and rpt xray in 10-14 days– If rpt xray still negative but suspicious exam,
then CT may show #
Scaphoid #
• What type of cast:
• Acute nondisplaced stable scaphoid #?– Below elbow thumb spica cast x 12 wks
• Delayed nondisplaced stable scaphoid #?– Long arm thumb spica cast x 6 wks, then short
arm thumb spica cast for remainder (time to union is 3 mos faster)

Case
• 42y.o. F sustained FOOSH to right hand. O/E tender over dorsal aspect of wrist distal to ulnar styloid, decreased wrist ROM.– What xrays do you want to order?

Case cont’d
• Interpretation of xray?– Small dorsal chip
fragment
– Triquetral #

Case cont’d
• Management of triquetral #?– Immobilize in short arm cast x 4-6 wks
• Similar treatment recommended for pisiform #, trapezium #, capitate #, trapezoid #

Case
• Xray interpretation?– Trapezium #

Case
• What type of xray is this?– Carpal tunnel view
• What bones are fractured?– Trapezium and hamate

Hamate #
• Hook of hamate is most common site of #
• Treatment is immobilization in short arm cast, with ortho f/u in 1-2wks
• Complications:– Ulnar nerve injury– nonunion
• May require surgical excision of hook

Case
• 35y.o. M who is right-handed and presents with remote hx of being hit in dorsiflexed right hand with jack hammer while at work 2 yrs ago. Since c/o gradually worsening tender wrist. No other recent trauma
• You do xrays and see…

Case cont’d
• Interpretation?– Sclerotic lunate
fragment
• What is the name of this condition?– Kienbock’s disease
– AVN of lunate following traumatic #
– Treatment--ortho
Lunate #
• Because of risk of Kienbock’s disease, all suspected lunate # should be immobilized in short arm cast
• Should receive ortho f/u in 1-2wks

Carpal # general rules
• All displaced carpal bone #, carpal dislocation, or # involving carpal-metacarpal jt should be referred to ortho for ORIF

Carpal instability
• Stage 1—scapholunate failure
• Stage 2—capitolunate failure
• Stage 3—triquetrolunate failure
• Stage 4—lunate dislocation

Carpal instability
• Stage 1:– Fall on extended wrist is usual cause– Frequently c/o pain in wrist with activity followed by
aching– Scaphoid test and catch-up clunk
• 4 fingers on dorsum or radius and thumb over scaphoid tuberosity, move hand from ulnar deviation to radial deviation and apply pressure with thumb—pain as scaphoid is moved dorsally if unstable
• Move wrist from radial to ulnar deviation and will hear clunk as lunate catches up with alignment of scaphoid
Carpal instability
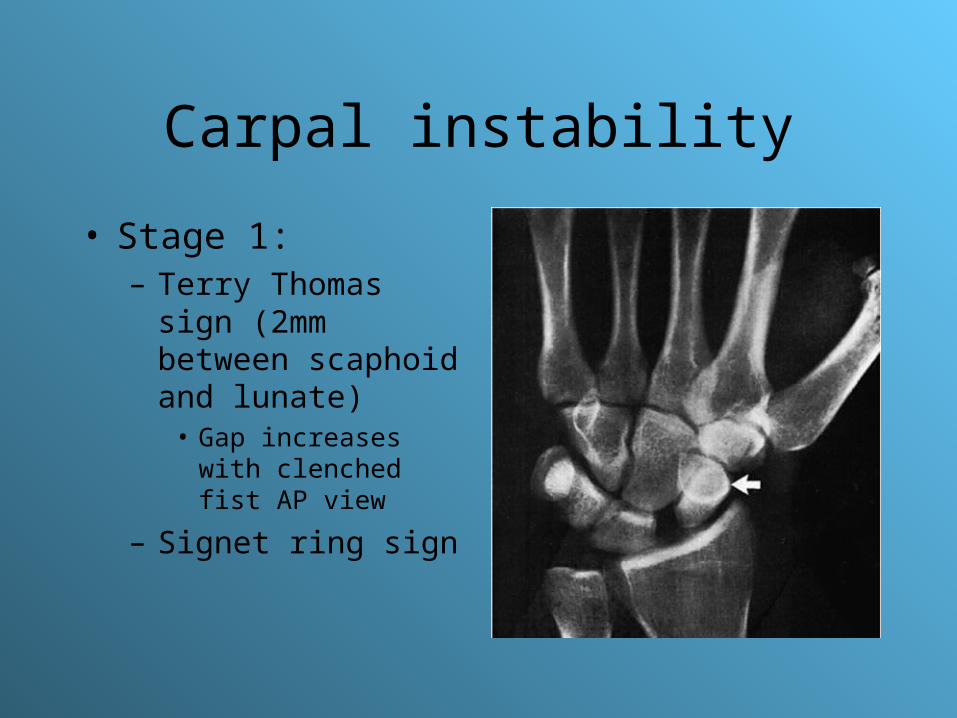
• Stage 1:– Terry Thomas sign
(2mm between scaphoid and lunate)
• Gap increases with clenched fist AP view
– Signet ring sign

Carpal instability
• Stage 2:– Fall on extended wrist

Carpal instability
• Stage 2:– Best seen on lat view
– Capitate is dorsally dislocated
– Lunate in normal position

Carpal instability
• Stage 3:– Axial loading on hyperextended pronated wrist– Pain and laxity on ulnar side of wrist– Xray show triquetrum displaced proximally on
AP view; may be exaggerated with ulnar deviation

Carpal instability
• Stage 4:– Major complication is
acute compression of median nerve
– xray shows triangular lunate, and on lat view spilled teacup and dorsal displacement of capitate

Carpal instability
• All carpal dislocation injuries need ortho referral for reduction/stabilization
• Complications include median nerve palsy, chronic carpal instability, degenerative arthritis
Distal radius / ulna injuries

Quiz
• What # is associated with “dinner fork” deformity?– Colles #
• What is the other name for a “reverse Colles #”?– Smith’s #
• Which type of # gives classical “chauffeurs #”?– Hutchinson #
Case
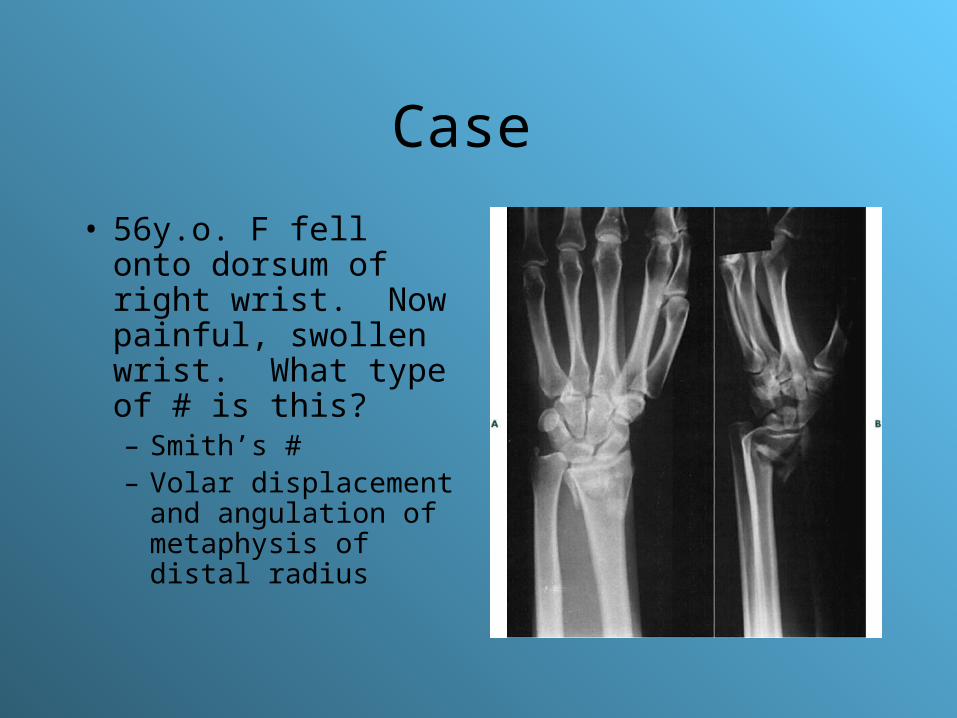
• 56y.o. F fell onto dorsum of right wrist. Now painful, swollen wrist. What type of # is this?– Smith’s #– Volar displacement
and angulation of metaphysis of distal radius
Case cont’d
• What would your management be of this #?– Attempt closed reduction, if unsuccessful then
ORIF necessary– Cast x 6-8 wks
Colles’ #
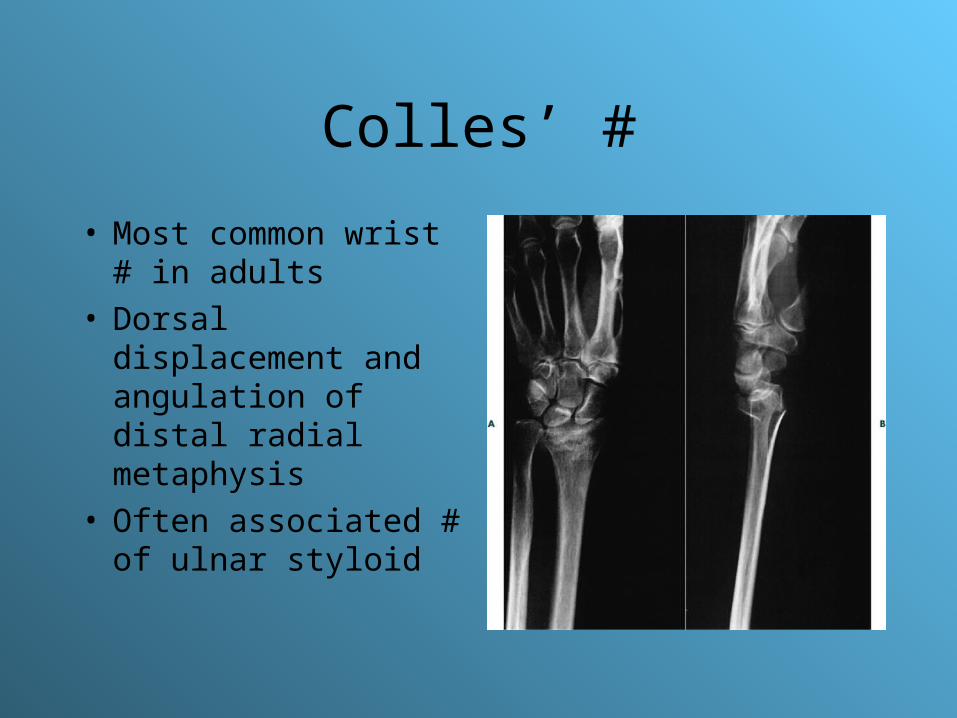
• Most common wrist # in adults
• Dorsal displacement and angulation of distal radial metaphysis
• Often associated # of ulnar styloid
Colles’ #
• Management:– Prompt closed reduction– If marked dorsal comminution, intraarticular
extension of #, displacement >20 degrees dorsal angulation, then require ortho f/u
– If open #, neurovasc compromise, or failed attempt at reduction then immediate ortho referral

Acceptable measurements for healing of distal radius #
• Xray criteria:• Radiulnar length
• Radial inclination• Radial tilt
• Articular incongruity
• Measurements:• <5mm radial
shortening• >= 15 degrees• 15 degree dorsal tilt
and 30 degree volar• <= 2mm at radiocarpal
joint

Case
• 33y.o. M construction worker was tightening a crank pulley when he lost grip and crank hit him in back of right wrist.
• Xray interpretation?– Transverse # of radial
metaphysis with extension into radiocarpal joint
• Type of #?– Hutchinson #
Case cont’d
• Management of nondisplaced #?– Short arm cast x 4-6 wks
• Management of displaced #?– ORIF
Barton’s #
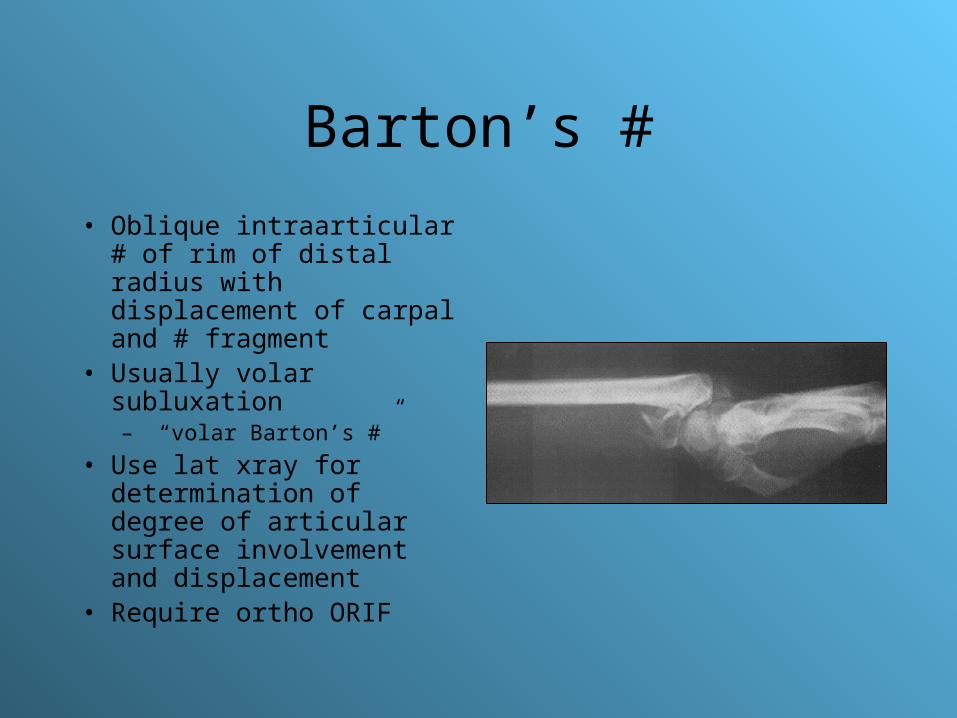
• Oblique intraarticular # of rim of distal radius with displacement of carpal and # fragment
• Usually volar subluxation– “volar Barton’s #”
• Use lat xray for determination of degree of articular surface involvement and displacement
• Require ortho ORIF

DRUJ
• Dislocation of radioulnar joint• Often associated with distal radius or Galeazzi’s #• Clinical high suspicion for diagnosis• May either be dorsal or volar dislocation of ulna• Disruption of triangular fibrocartilage complex,
avulsion # of ulna styloid common

DRUJ
• With dorsal dislocation:– Prominent ulnar styloid– Pain and limitation with supination
• With volar dislocation:– Loss of normal ulnar styloid prominence– Pain and limitation with pronation
DRUJ
• Xrays may be normal
• If DRUJ suspected, CT is recommended of the wrist
• Require ortho consult for reduction/stabilization
• Long arm cast x 6 wks

Forearm injuries

Case
• 41y.o. M minding his own business when assaulted near Cecil Hotel. Hit on left forearm with baseball bat.
• Describe the xray• Any other xray images
you want?

Case cont’d
• Management of this #?– Short arm cast x 6-8 wks
• If the # were in mid or proximal third of ulna, what would your management be?– Long arm cast– Q1wk f/u to ensure no displacement

When to refer…
• If >10 degrees of angulation
• # with >50% displacement of diameter of ulna

Interventions for isolated diaphyseal fractures of ulna in adults.
Handoll, HH. Cochrane Database. Jan 2004.
• 3 articles about management of isolated ulnar #• Short arm prefabricated braces with long arm casts
—no difference in # healing, pts were more functional and “happier” with braces
• Wrap bandages, short arm casts, and long arm casts—pts with wrap bandages had more pain
• 2 types of plates—no significant difference in # healing (doesn’t matter to us!)
• Overall—not great trials, need better data to indicate appropriate method of treatment

Radius and ulna shaft #
• Usually requires significant force so often displacement as well
• As you can see….
ORIF required for displacement
If undisplaced then long arm cast x 8 wks (ortho f/u in 1wk to ensure no displacement)

Which one is which?
Galeazzi’s # Monteggia’s #
Monteggia’s #
• # of proximal ulna and dislocation of radial head• Delayed diagnosis of radial head dislocation in ¼
of cases• MoI: forced pronation of forearm during FOOSH• Often damage to deep branch of radial nerve
(wkness or paralysis on extension of fingers and thumb)
• Requires immediate ortho referral for ORIF

Monteggia’s #

Monteggia’s #
• Type 1—ant dislocation and angulation
• Type 2—post dislocation and angulation
• Type 3—lat dislocation and angulation
• Type 4—# of radial and ulna shafts with radial head dislocation

Galeazzi’s #
• 3-7% of all forearm # seen• Distal radius # and
dislocation of DRUJ• MoI: wrist in extension,
forearm pronated, and FOOSH
• “fracture of necessity”…I.e. surgery is necessity for good outcome!
• Require ortho referral as unstable # for ORIF
Pediatric injuries

Pediatric injuries
• Or as I like to call it…is anything wrong with this arm?

Pediatric fractures
• 3 main types:– Buckle—treat in short arm cast and ortho f/u– Greenstick– complete

Xray…
• What type of # is this?– buckle

Greenstick #
• By definition, they are displaced #
• Thus, require long-arm cast x 6-8 wks and ortho f/u to ensure no further displacement
• When to reduce (I.e. how much displacement is too much? ) ?– Angulation >10 degrees

Xray…

Complete #
• Complete # through both cortices of radius, often associated ulna # as well
• Require reduction
• If reduction not adequate, then possible ORIF
• Long arm cast x 7-8wks

Reduction versus remodelling in pediatric distal forearm fractures: a preliminary cost
analysis.Do, TT. J Ped Ortho. Mar 2003.
• N=34 pts with wrist metaphyseal fractures who were reduced and lost reduction on f/u
• Pts with <15 degrees angulation, <1cm shortening, open physis—heal within cast in 6wks; remodel in 7.5 months
• Pts with no reduction—saved 2h ED time, saved 50% of costs (US$270 vs. US$536)
• No significant clinical deformities or residual functional deficits
Position of immobilization for pediatric forearm fractures.
Boyer, BA. J Ped Ortho. Mar 2002. • N=99; distal-third forearm fractures• Closed reduction and casting in neutral,
pronated or supinated positions• Initial angulation—20 degrees; post-
reduction angulation—3 degrees; angulation at union—7 degrees
• No significant difference between casting positions with regards to forearm angulation

Growth plate #
• Usually Salter I or II of distal radius
• Salter I—treat with short arm cast/splint, with ortho f/u
• Salter II—if displaced, require ortho for reduction; immobilize in long-arm cast, with ortho f/u

Plastic deformation
• Unique to children• Bowing of bone without
obvious #• May be associated with #
in other forearm bone…so be careful not to miss it!
• Contralateral arm xrays may be useful
• Refer to ortho for reduction and long arm cast and f/u

References
• Rosen’s• Canale: Campbell’s Operative Orthopedics. 10th ed. Mosby , Inc. 2003• Perron, AD. Evaluation and management of high-risk orthopedic
emergencies. Emerg Med Clin NA. Feb 2003. 21(1):159-204.• Overly, F. Common pediatric fractures and dislocations. CPEM. June
2002. 3:106-117.• Do, TT. Reduction versus remodeling in pediatric distal forearm
fractures: a preliminary cost analysis. J Ped Ortho B. Mar 2003. 12(2):109-115.
• Handall, HH. Interventions for isolated diaphyseal fractures of ulna in adults. Cochrane database. Jan 2004.
• Boyer, BA. Position of immobilization for pediatric forearm fractures. J Ped Ortho. Mar 2002. 22(2):185-187.

Questions ?