8/2/2019 Wright Kurin SAA 2012 Final
1/1
A Possible Case of Cancer in the Late Prehispanic Peruvian
Andes
1. Introduction
This cranium, MCH1.2, was excavated from Pukamachay Cave, at the
site of Cachi in Andahuaylas, Peru . Theremains pertain to the
Chanka culture and date to the early Late Intermediate Period (A.D.
1000-1250). Becausethe cave was badly looted, no post-cranial
elements could be associated with the MCH1.2 cranium, and no
otherbones exhibited lytic lesions.
The Chanka culture, which emerged following the collapse of the
Wari Empire ca. AD 1000, was a society thatwitnessed high levels of
endemic violence, as well as a higher frequency of pathological
lesions indicative ofdisease than earlier imperial era populations.
Medico-cultural interventions, such as amputation
throughdismemberment and trepanation were likely enacted by the
Chanka society to cope with novel challenges in theaftermath of
collapse and suggest a nuanced, emic understanding of health and
disease (Kurin 2012).
Katherine Wright and Danielle S. Kurin
4. Conclusions
While the absence of postcranial elements makes an absolute
diagnosis difficult, the nature of thelesions in MCH1.2 can rule
out most of the previously detailed conditions.
Tuberculosis can be ruled out as a cause of the cranial lesions
in MCH1.2. First, cranial lesionsusually present in younger
individuals, and MCH1.2 is an adult. Furthermore, the lesions
present moreextensive resorbtion of the diploe and the outer tables
rather than the inner table. The lesions arelarger than 2mm, and do
not cross suture lines.
Langerhans Cell Histiocytosis can also be disregarded, mainly
due to its early age of onset. Even so,
the lesions seen in MCH1.2 are not punched out, and show some
signs of reactive bone formationon the margins.
Multiple myeloma seems a less likely diagnosis than metastatic
carcinoma for MCH1.2. All of thelesions seem too large, too varied
in size, and not numerous enough to be caused by multiple
myeloma. The edges are not as sharp and punched out as they
would be with a multiple myelomadiagnosis, and there are signs of
osteoblastic boney reaction along the m argins.
Secondary metastatic carcinoma seems to be the most likely cause
of the lesions, but is not a definitediagnosis. The largest lesion
has an irregular, sharp, lacy margin with osteoblastic activity and
exhibitsthe most destruction in the diploe. The other lesions seem
to be varied in size and stage. Althoughfurther research and
radiographic analysis are needed to make a certain diagnosis, the
characteristicsof the lesions and the age of the individual suggest
a most probable diagnosis of secondarymetastatic carcinoma in
MCH1.2.
References:Assis, S.C., 2010. Metastatic carcinoma in a
14th-19th century skeleton from Constancia.International Journal of
Osteoarchaeology, 20(5), pp.603-620.Buikstra, J.E. and Ubelaker,
D.H., 1994. Standards for data collection from human skeletal
remains: Proceedings of a seminar at the Field Museum of Natural
History.Arkansas Archeological Survey Research Series, 44.Kurin,
D., 2012.The bioarchaeology of collapse: Ethnogenesis and ethnocide
in post-imperial Andahuaylas Peru. Unpub. PhD. Vanderbilt
University.Marks, M.K. and Hamilton, M.D., 2007.Metastatic
carcinoma: Palaeopathology and differential diagnosis.International
Journal of Osteoarchaeology,17, pp.217-234.Ortner, D.J.,
2003.Identification of pathological conditions in human skeletal
remains. San Diego: Academic Press.Rothschild, B.M., Hershkovitz,
I. and Dutour, O., 1998.Clues potentially distinguishing lytic
lesions of multiple myeloma from those of metastatic carcinoma.
American Journal of Physical Anthropology, 105, pp.241-250.Smith,
M.O., 2002. A probable case of metastatic carcinoma from the Late
Prehistoric Eastern Tennessee River Valley.International Journal of
Osteoarchaeology, 12, pp.235-247.
Acknowledgements: This project was supported by Fulbright-Hays
and Vanderbilt University. Special thanks to the
ProyectoBioarqueologico Andahuaylas crew including Enmanuel Gomez,
Edison Mendoza Martinez, Anna Schneider, Kirsten Green,
KirstenDelay, and Jasmine Kelly. Thanks also to Dr. Rebecca Gowland
of Durham University and Dr. Don Brothwell of the University of
York.
2. Materials and Methods
The sex and age of the individual were estimated using standards
outlined by Buikstra and Ubelaker (1994).Dental eruption, dental
wear, and cranial suture closure indicate the individual was
between 35 and 40 at thetime of death. Sex was determined as male
based on the rugosity of the mastoid process, nuchal
crest,supraorbital margin, and glabella.
The largest lesion is located superior to and intersecting the
right supraorbital margin. The lesion penetrates theinner table,
diploe, and outer table of the skull. Destruction is the most
extensive in the diploe, and more
extensive in the outer table than the inner. table Two other
lytic foci are evident: a smaller depressed area25.4mmabove the
left suprarobital margin with a pinprick hole in the center, and a
larger depressed area on theright parietal. Both these lesions
present as depressions in the cranium, and the most extensive
osteoclasticactivity in the largest lesion is present in the
diploe, suggesting the cause of the lesions originated within
thediploe. There is new woven bone on the outer margins of the
lesion.
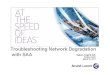
Fig.3:Second lesion on the left frontal bone showing new
bonegrowth and a pinprick hole perforating the outer table.
Wright,2011
Wright,2011
Wright,2011
Department of Archaeology, Durham University; Department of
Anthropology, Vanderbilt University
77th Annual Meeting ofthe
Societyfor AmericanArchaeology
April 18-22, 2012
Memphis, TN
Fig. 1: Map of Peru showing the location of the Cachi site.
Fig.4:Active lytic lesion on the right frontal bone of MCH1.2
showing extensive damage to thediploe and reactive bone formation
along the margins.
Fig.5:Pathological cranial lesions present in among Chanka
populations in Andahuaylas. From left to right: porotic
hyperostosis, periosteal reaction from a healingtrepanation,
degraded unhealed trepanation, healing trauma, and the lytic lesion
from MCH1.2
Fig.10:Right lateral view of MCH1.2
Fig.2:Third lesion on the right parietal demonstratingnew bone
growth and a pinprick hole perforating the
outer table.
TuberculosisTuberculosis is an infectious disease caused by the
mycobacterium tuberculosiscomplex. Once the body detects the
bacterias presence, it initiates an aggressiveimmune response that
could affect nearby organ tissues. Pathognomic changes
oftuberculosis are most commonly seen in the vertebral column, but
associated lesionscan also be seen in the skull. Cranial lesions
are most commonly seen in subadults
younger than 10, and are characterized by a round lytic focus of
no more than 2 cm in
diameter, perforation of both inner and outer tables, and
commonly crossing suturelines. When seen in adults, cranial lesions
usually have more extensive resorption ofthe inner table than the
outer and the formation of a sequestrum (Ortner, 2003).
Langerhans Cell HistiocytosisLangerhans Cell Histiocytosis (LCH)
is a disease in which a proliferation ofLangerhans cells (immune
cells called histiocytes) leads to increased phagocyticactivity,
which can cause lytic lesions if the bone tissues are affected. LCH
is most
frequently seen in the skull, and generally affects subadults
between the ages of 0and 15. Lesions in the bone are usually lytic,
without reactive bone formation, smalland round, and may coalesce
to create a geographic border (Ortner, 2003). Theedges of LCH
lesions are usually punched out, meaning sharply defined
andcircular, with scalloped edges (Marks and H amilton, 2007;
Rothschild et al., 1998).
Multiple MyelomaMultiple myeloma is a type of cancer in which
plasma cells undergo malignanttransformation and growth. The
malignant plasma cells secrete a substance thattriggers
osteoclastic activity and inhibits osteoblastic activity
(Rothschild et al., 1998;Marks and Hamilton, 2007). Therefore,
reactive bone growth is not typically seen incases of multiple
myeloma. Lesions typically appear as sharply defined,
multiple,spherical, small (3-10mm), consistently sized, punchedout
holes that penetrate allcranial tables and rarely show remodeled
margins. The prevalence of multiple
myeloma increases with age and is generally seen in older
adults.
Secondary Metastatic CarcinomaThe most common cause of tumors
affecting the skeleton is metastasis from other organs(Ortner,
2003). In secondary metastatic carcinoma, expanding blood-borne
tumorous cells
can grow and displace cancellous bone, eventually piercing the
cortex and exposing thediploe (Assis, 2010; Smith, 2002). Secondary
metastatic carcinoma is most commonlyseen in adults and the
elderly. Metastatic tumors to bone are most commonly osteolytic,
butmay also be osteoblastic or a mix of both. Lesions tend to be
well-defined, and spherical inshape with an ellipsoid component or
geographic (irregular) boundary. Lesions vary in
size, and sometimes have raised margins (Ortner, 2003;
Rothschild et al., 1998, p.244).
3. Differential Diagnosis
Fig. 7:Multiple punched out lesions
of multiple myeloma.
Fig. 9:Osteolytic lesion of secondarymetastatic carcinoma with
reactivebone and raising on the margins.
Fig. 8:LCH lesions showing geographicshape and little reactive
bone formation.
Fig. 6:Lesion of tuberculosis showingpenetration of both tables
and formation of
a sequestrum .
Marksand Hamilton,2007
Images below fromOrtner,2003
Abstract
The cranium of a 35-40 year old adult male from the Chanka
culture (AD 1000-1400) was excavated from the site of Cachi in
Andahuaylas, Peru. The cranium presents lesions on the frontal and
parietal bones. The osteolytic nature ofthree of the lesions
suggested they may be the effect of a treponemal or neoplastic
disease. Based on the shape and nature of the lesions, the age and
sex of the individual, and the number of lesions, a differential
diagnosis is presentedthat includes tuberculosis, Langerhans Cell
Histiocytosis, multiple myeloma, and metastatic carcinoma.
Ultimately, the lesions seen in MCH1.2 seem most likely to be
caused by secondary metastatic carcinoma.