Embed Size (px)
Citation preview
MULTIDISCIPLINARY APPROACH TO WOUND CARE
WOUND ASSESSMENT AND CLASSIFICATIONJON HOUSEWORTH DPM
GOALS FOR A CLINICALLY RELEVANT DISEASE CLASSIFICATION SYSTEM
1. Risk stratification surrounding the natural history of the disease
2. Stratification should be accurate and well detailed in order to provide proper comparison of different treatment strategies
3. Descriptive and predictive
SHORTCOMINGS OF CLASSIFICATION SYSTEMS PRIOR TO JANUARY 2014
• Limited use in directing clinical decision-making• Narrow focus• TASC I and II, Bollinger, Gaziani only address arterial anatomy, but no wound quantification
or baseline perfusion status• Fontaine and Rutherford are pure ischemic systems, and lack adequate detail• DFU classifications (PEDIS, UT, Wagner) are primarily ulcer systems and fail to provide
sufficient perfusion status and only have minimal or no mention of gangrene• Gangrene increases risk of amputation when compared to ulceration
2014 SOCIETY FOR VASCULAR SURGERY (SVS) LOWER EXTREMITY THREATENED LIMB CLASSIFICATION SYSTEM
• Designed to define disease burden and combine the best of previous systems• analogous to the tumor, node, metastasis (TNM) system for cancer staging
• Grades 3 major factors: Wound, Ischemia, and foot Infection (WIfI)
• SVS WIfI (2014)
TARGET POPULATION FOR SVS WIFI
• Ischemic rest pain with confirmed, objective hemodynamic studies (ABI, TP, TcPO2)
• DFU
• Non healing LE wound longer than 2 weeks duration
• Gangrene to any part of LE
* Excludes pure venous wounds, ischemia due to microemboli, trauma, and non atherosclerotic conditions (Buerger’s, neoplasm)
WOUND GRADES
• Scale: 0-3 based on size, depth, severity, and difficulty achieving healing
• 0- No Wound. No gangrene
• 1- small, shallow, no bone exposed, minor tissue loss, salvageable with digital amputation or skin coverage. No gangrene
• 2- deeper, bone, joint, or tendon exposed, major tissue loss, salvageable with multiple digit amputations or a standard TMA (+/- skin coverage). Gangrene to digits only
• 3- extensive wound(s) with gangrene involving forefoot, midfoot, and/or rearfoot. Salvageable with non-traditional midfoot amputation and/or flap coverage.
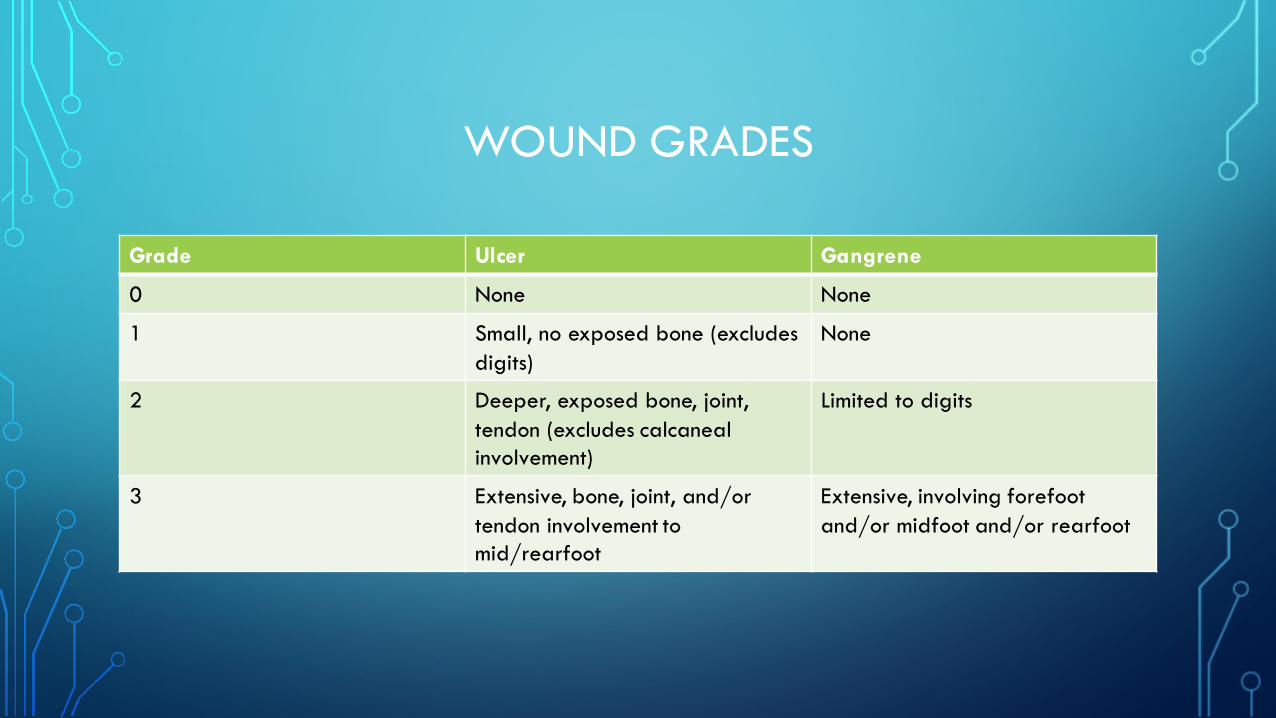
WOUND GRADES
Grade Ulcer Gangrene
0 None None
1 Small, no exposed bone (excludesdigits)
None
2 Deeper, exposed bone, joint, tendon (excludes calcaneal involvement)
Limited to digits
3 Extensive, bone, joint, and/or tendon involvement to mid/rearfoot
Extensive, involving forefoot and/or midfoot and/or rearfoot
ISCHEMIA GRADES
• ABI < 0.8 (no gradient of severity)
• Patients with ABI > 0.8 are low risk for amputation and wound healing is likely to take place without the need for revascularization
• Patients with ABI < 0.4 are high risk for amputation and wound healing is unlikely to take place without revascularization
*If ABI is unreliable (or incompressible), TP (toe pressure) or TcPO2
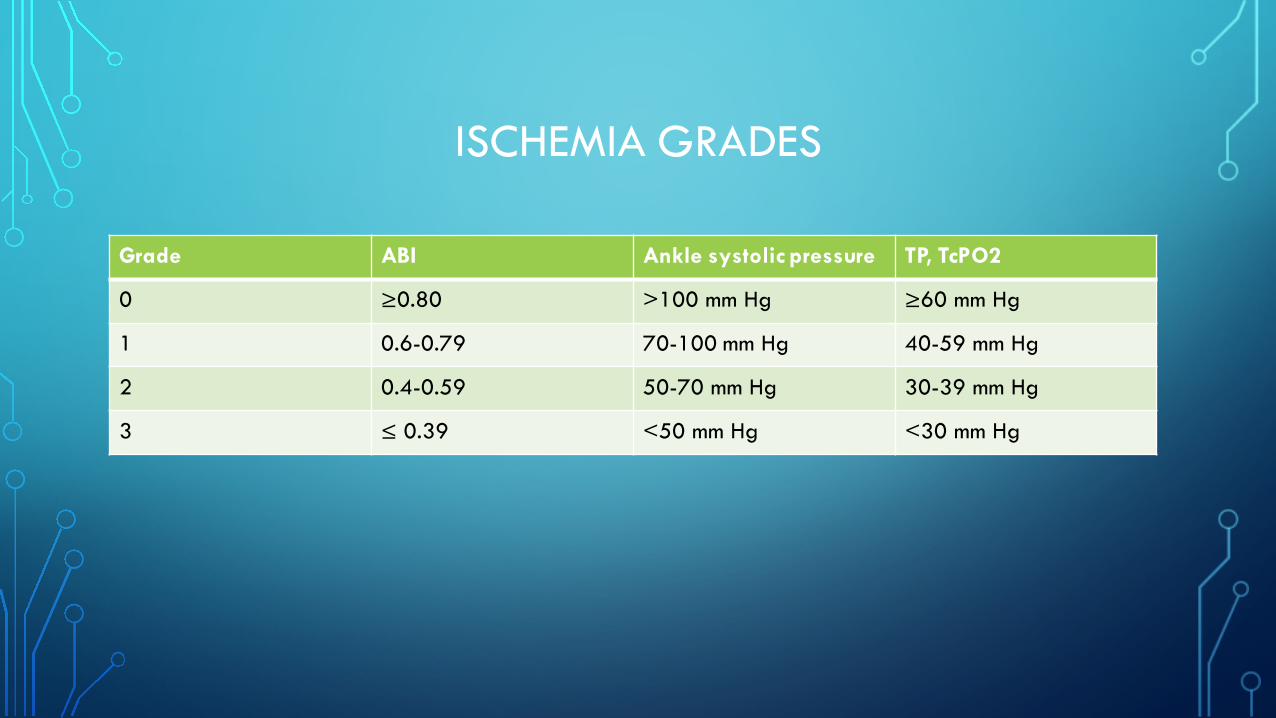
ISCHEMIA GRADES
Grade ABI Ankle systolic pressure TP, TcPO2
0 ≥0.80 >100 mm Hg ≥60 mm Hg
1 0.6-0.79 70-100 mm Hg 40-59 mm Hg
2 0.4-0.59 50-70 mm Hg 30-39 mm Hg
3 ≤ 0.39 <50 mm Hg <30 mm Hg
INFECTION GRADES
• Adopted from the IDSA guidelines- defined as 2 or more clinical signs (swelling, induration, periwound erythema, local pain or tenderness, warmth, purulence)
• Risk of amputation and hospitalization correlates directly with increasing infection severity- IDSA class 2 and 3 50-80% more likely
• Eurodiale study showed patients with wounds and PAD are 3x more likely to remain non-healed than patients with wounds alone
• Infection increases metabolic activity and small vessel thrombosis, ultimately decreasing tissue perfusion
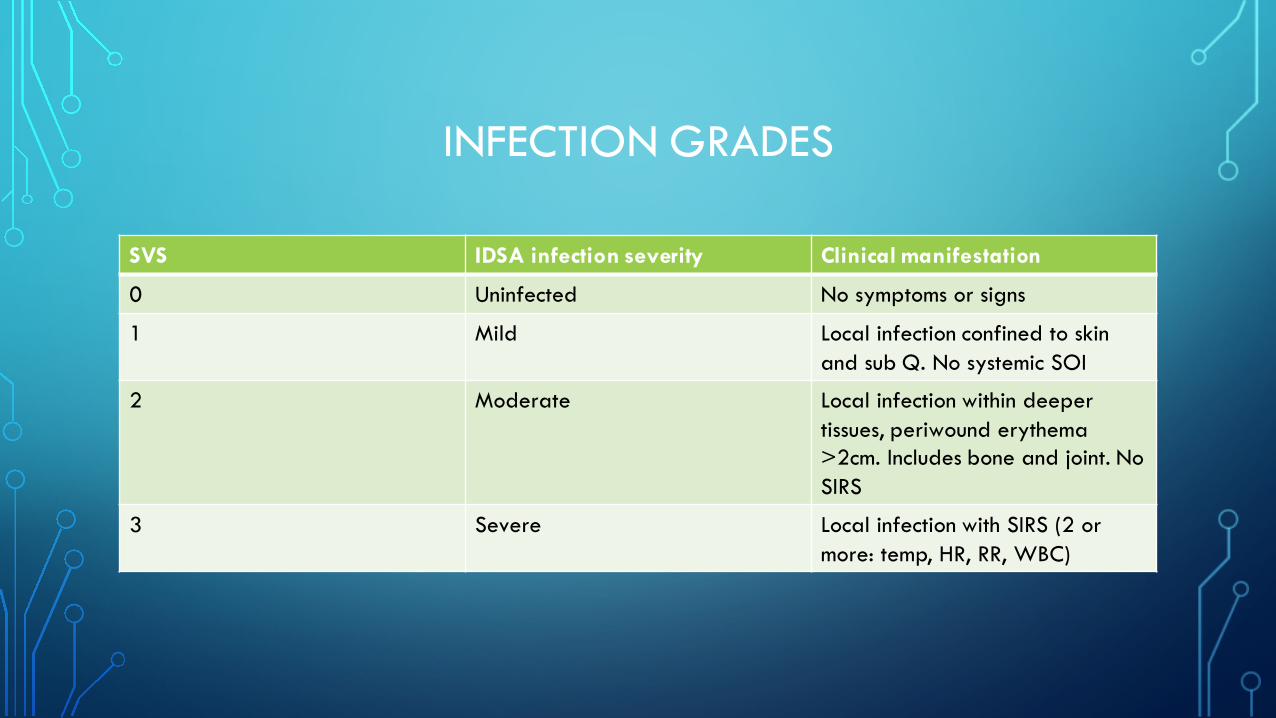
INFECTION GRADES
SVS IDSA infection severity Clinical manifestation
0 Uninfected No symptoms or signs
1 Mild Local infection confined to skin and sub Q. No systemic SOI
2 Moderate Local infection within deeper tissues, periwound erythema >2cm. Includes bone and joint. No SIRS
3 Severe Local infection with SIRS (2 or more: temp, HR, RR, WBC)
DELPHI CONSENSUS GROUP-12 MEMBERS
• Asked to assess all 64 theoretical patient combinations based on the 1 year risk of amputation with medical therapy alone
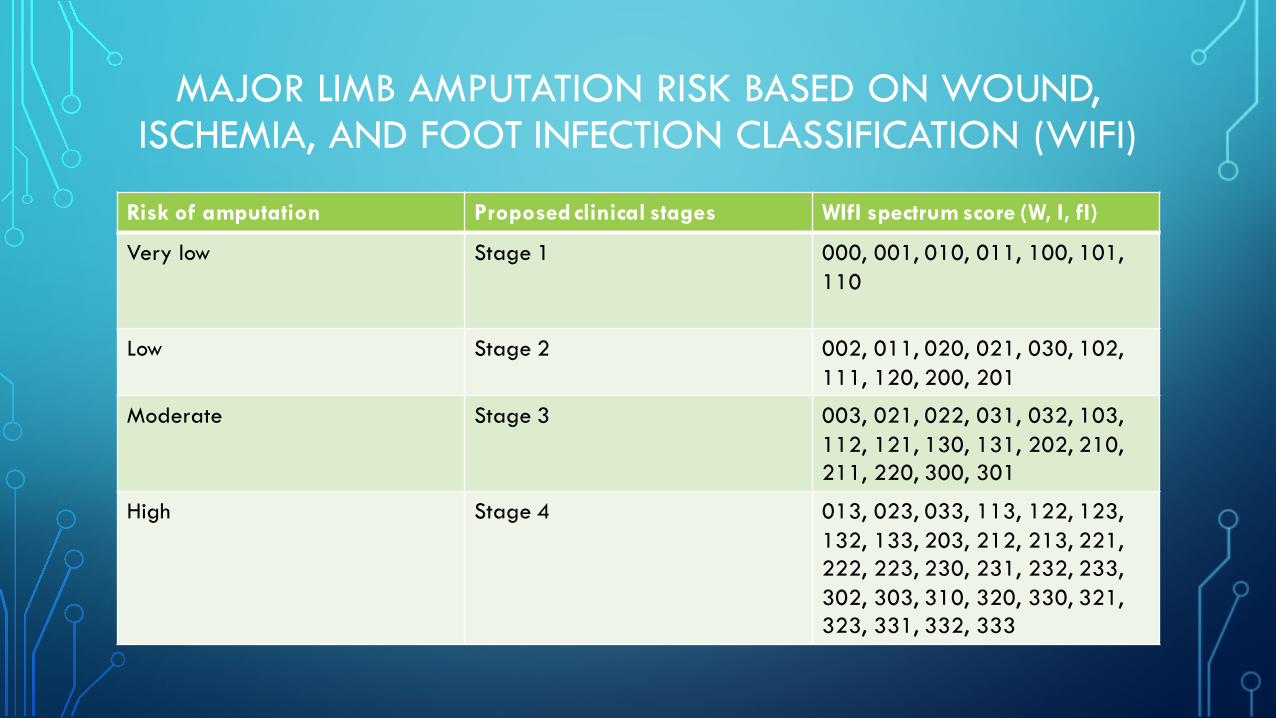
MAJOR LIMB AMPUTATION RISK BASED ON WOUND, ISCHEMIA, AND FOOT INFECTION CLASSIFICATION (WIFI)
Risk of amputation Proposed clinical stages WIfI spectrum score (W, I, fI)
Very low Stage 1 000, 001, 010, 011, 100, 101, 110
Low Stage 2 002, 011, 020, 021, 030, 102, 111, 120, 200, 201
Moderate Stage 3 003, 021, 022, 031, 032, 103, 112, 121, 130, 131, 202, 210,211, 220, 300, 301
High Stage 4 013, 023, 033, 113, 122, 123, 132, 133, 203, 212, 213, 221, 222, 223, 230, 231, 232, 233, 302, 303, 310, 320, 330, 321, 323, 331, 332, 333
EXAMPLES
Pt with ischemic rest pain, ABI 0.35, no wounds , no SOI
Wound grade- 0
Ischemia grade- 3
Infection grade 0
WIfI 030, clinical stage 2- low risk for amputation
EXAMPLES
55M with IDDM, dry gangrene of 4th and 5th digits with <2cm zone of cellulitis at the base of the toes. No systemic SOI. Absent pedal pulses. ABI 1.5. TP is 35mmHg.
Wound 2
Ischemia 2
Infection 1
WIfI 221, clinical stage 4- high risk for amputation
REFERENCES
• Joseph L. Mills Sr., MDcorrespondenceemail, Michael S. Conte, MD, David G. Armstrong, DPM, MD, PhD, Frank B. Pomposelli, MD, Andres Schanzer, MD, Anton N. Sidawy, MD, MPH, George Andros, MD. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: Risk stratification based on Wound, Ischemia, and foot Infection (WIfI).
Society for vascular surgery 2014.
• Bell, P.R.F., Charlesworth, D., DePalma, R.G., Eastcott, H.H.G., Eklöf, B., Jamieson, C.W. et al, The definition of critical ischemia of a limb. Working Party of the International Vascular Symposium. Br J Surg. 1982;69:S2.
• Criqui, M.H. Peripheral arterial disease and subsequent cardiovascular mortality: a strong and consistent association. Circulation. 1990;82:2246–2247.
• Caro, J., Migliaccio-Walle, K., Ishak, K.J., Proskorovsky, I. The morbidity and mortality following a diagnosis of peripheral arterial disease: long-term follow-up of a large database.
BMC Cardiovasc Disord. 2005;5:14.
• rownrigg, J.R.W., Davey, J., Hoilt, P.J., Davis, W.A., Thompson, M.M., Ray, K.K. et al, The association of ulceration of the foot with cardiovascular and all-cause mortality in patients with diabetes: a meta-analysis. Diabetologia. 2012;55:2906–2912.
• Criqui, M.H., Langer, R.D., Fronek, A., Feigelson, H.S., Klauber, M.R., McCann, T.J. et al, Mortality over a period of 10 years in patients with peripheral arterial-disease. N Engl J Med. 1992;326:381–386.
• Rutherford, R.B., Baker, J.D., Ernst, C., Johnston, K.W., Porter, J.M., Ahn, S. et al, Recommended standards for reports dealing with lower extremity ischemia: revised version. J VascSurg. 1997;26:517–538
REFERENCES
• Dormandy, J.A., Rutherford, R.B. Management of peripheral arterial disease (PAD). TASC Working Group: TransAtlantic Inter-Society Consensus (TASC). J Vasc Surg. 2000;31:S1–S296.
• Setacci, C., Ricco, J.B., Apelqvist, J., Becker, F., Cao, P. Management of critical limb ischemia and diabetic foot. Eur J Vas Endovas Surg. 2011;42:S1–90.
• Brass, E.P., Anthony, R., Dormandy, J., Hiatt, W.R., Jiao, J., Nakanishi, A. et al, Parenteral therapy with lipo-ecraprost, a lipid-based formulation of a PGE1 analog, does not alter six-month outcomes in patients with critical leg ischemia. J Vasc Surg. 2006;43:752–759.
• Marston, W.A., Davies, S.W., Armstrong, B., Farber, M.A., Mendes, R.C., Fulton, J.J. et al, Natural history of limbs with arterial insufficiency and chronic ulceration treated without
revascularization. J Vasc Surg. 2006;44:108–114.
• Elgzyri, T., Larsson, J., Thörne, J., Eriksson, K.F., Apelqvist, J. Outcome of ischemic foot ulcer in diabetic patients who had no invasive vascular intervention. Eur J Vasc Endovasc Surg.
2013;46:110–117.
• Fontaine, R., Kim, M., Kieny, R. [Surgical treatment of peripheral circulation disorders]. Helv Chir Acta. 1954;21:499–533.
• Armstrong, D.G., Cohen, K., Courric, S., Bharara, M., Marston, W. Diabetic foot ulcers and vascular insufficiency: our population has changed, but our methods have not. J Diabetes Sci
Technol. 2011;52:1591–1595.