Embed Size (px)
Citation preview
1
LPLP--3M3M--05/0805/08
Wound Care Assessment in Wound Care Assessment in the Home Care Settingthe Home Care Setting
Lynn Peterson, RN, BSN, CWOCNLynn Peterson, RN, BSN, CWOCNTechnical Service SpecialistTechnical Service Specialist
3M Health Care3M Health CareWednesday, May 14, 2008Wednesday, May 14, 2008
LPLP--3M3M--05/0805/08
ObjectivesObjectives
Describe essential elements of a wound Describe essential elements of a wound assessmentassessmentUnderstand the importance of Understand the importance of ““Best Best Practice GuidelinesPractice Guidelines”” in wound carein wound careIdentify how to creatively teach your staff Identify how to creatively teach your staff wound assessmentwound assessmentIdentify how to best utilize a WOCN in the Identify how to best utilize a WOCN in the home care settinghome care setting
LPLP--3M3M--05/0805/08
Why is assessment important?Why is assessment important?
Identify etiology and contribution factorsIdentify etiology and contribution factorsAids in accuracy of MOO questionsAids in accuracy of MOO questionsPrevent inconsistencies in documentationPrevent inconsistencies in documentationDevelopment of a management planDevelopment of a management plan
2
LPLP--3M3M--05/0805/08
Factors to considerFactors to considerSkin and wound assessmentSkin and wound assessmentEtiology of skin damageEtiology of skin damage--pressure, poor pressure, poor perfusion, neuropathyperfusion, neuropathyComorbid ConditionsComorbid ConditionsNutritional/Hydration StatusNutritional/Hydration StatusMobilityMobilityAgeAgeMedicationsMedicationsPsychosocial FactorsPsychosocial Factors
LPLP--3M3M--05/0805/08
Wound Assessment EssentialsWound Assessment EssentialsLocationLocationWound dimensionWound dimension--Size & depthSize & depthCharacteristics of wound baseCharacteristics of wound baseDead spaceDead spaceDrainage (exudate) & OdorDrainage (exudate) & OdorWound EdgesWound EdgesCondition of periwound skinCondition of periwound skinInfectionInfectionPainPainWound EtiologyWound Etiology
LPLP--3M3M--05/0805/08
LocationLocation
Correct identification of anatomic location is Correct identification of anatomic location is criticalcriticalSacral/coccygeal, and Ischial tuberostiy, Sacral/coccygeal, and Ischial tuberostiy, trochanter, heel, Right and left, etctrochanter, heel, Right and left, etc
3
LPLP--3M3M--05/0805/08
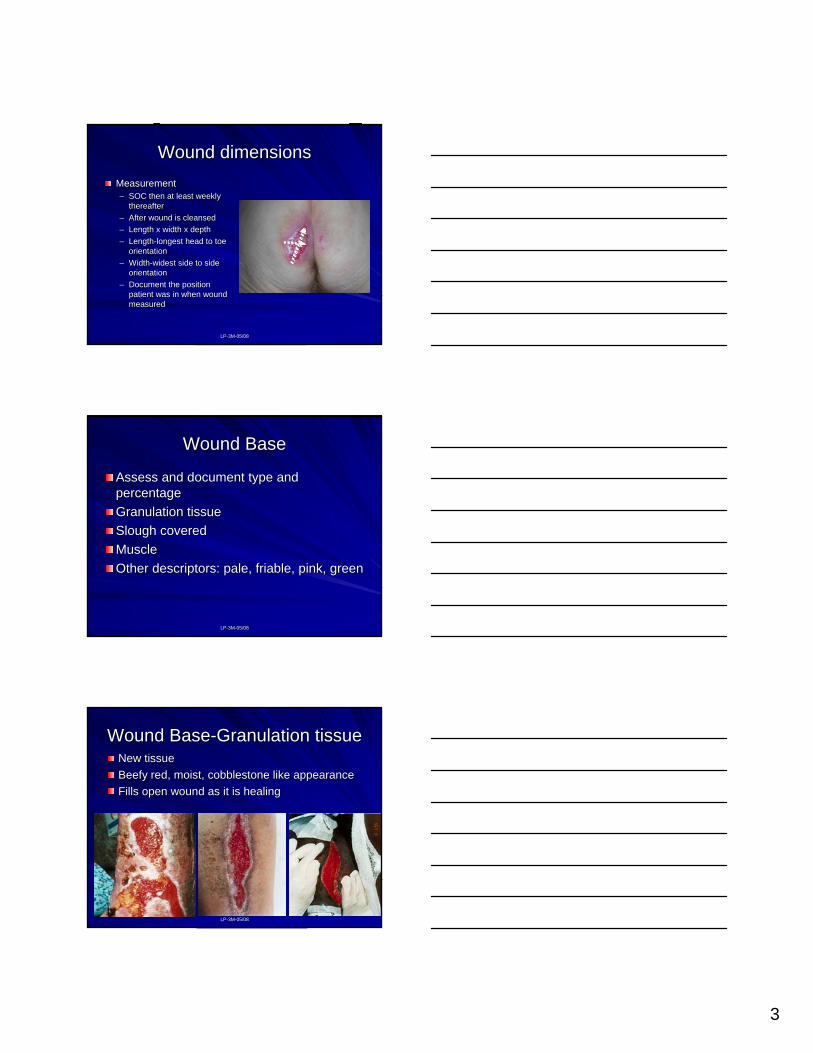
Wound dimensionsWound dimensionsMeasurement Measurement –– SOC then at least weekly SOC then at least weekly
thereafter thereafter –– After wound is cleansedAfter wound is cleansed–– Length x width x depthLength x width x depth–– LengthLength--longest head to toe longest head to toe
orientationorientation–– WidthWidth--widest side to side widest side to side
orientationorientation–– Document the position Document the position
patient was in when wound patient was in when wound measuredmeasured
LPLP--3M3M--05/0805/08
Wound BaseWound Base
Assess and document type and Assess and document type and percentagepercentageGranulation tissueGranulation tissueSlough coveredSlough coveredMuscleMuscleOther descriptors: pale, friable, pink, greenOther descriptors: pale, friable, pink, green
LPLP--3M3M--05/0805/08
Wound BaseWound Base--Granulation tissueGranulation tissueNew tissueNew tissueBeefy red, moist, cobblestone like appearanceBeefy red, moist, cobblestone like appearanceFills open wound as it is healingFills open wound as it is healing
4
LPLP--3M3M--05/0805/08
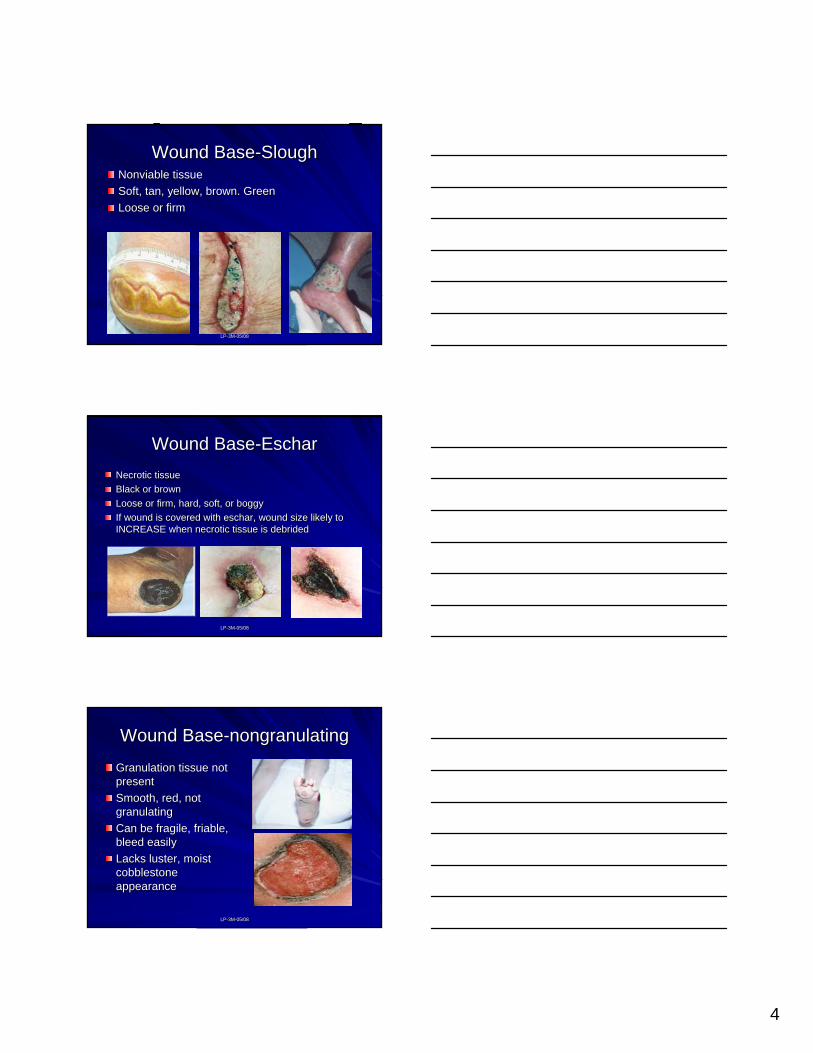
Wound BaseWound Base--SloughSloughNonviable tissueNonviable tissueSoft, tan, yellow, brown. GreenSoft, tan, yellow, brown. GreenLoose or firmLoose or firm
LPLP--3M3M--05/0805/08
Wound BaseWound Base--EscharEscharNecrotic tissueNecrotic tissueBlack or brownBlack or brownLoose or firm, hard, soft, or boggyLoose or firm, hard, soft, or boggyIf wound is covered with eschar, wound size likely to If wound is covered with eschar, wound size likely to INCREASE when necrotic tissue is debridedINCREASE when necrotic tissue is debrided
LPLP--3M3M--05/0805/08
Wound BaseWound Base--nongranulatingnongranulating
Granulation tissue not Granulation tissue not presentpresentSmooth, red, not Smooth, red, not granulatinggranulatingCan be fragile, friable, Can be fragile, friable, bleed easilybleed easilyLacks luster, moist Lacks luster, moist cobblestone cobblestone appearanceappearance
5
LPLP--3M3M--05/0805/08
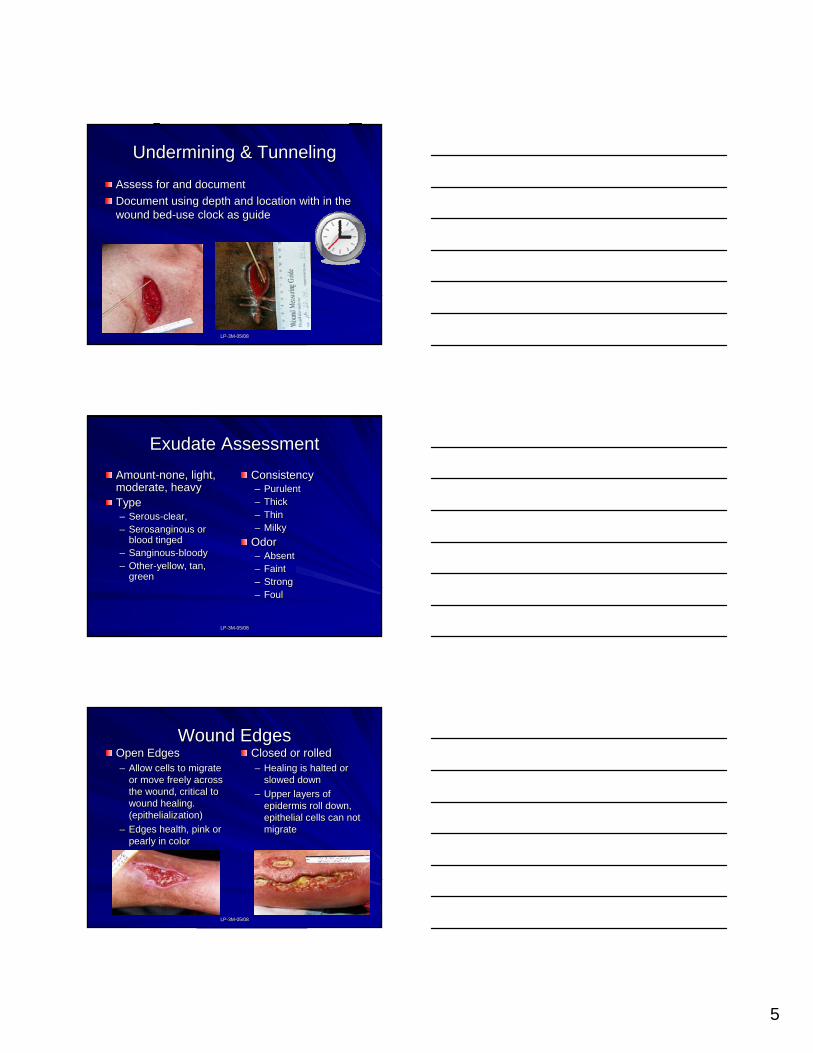
Undermining & TunnelingUndermining & Tunneling
Assess for and documentAssess for and documentDocument using depth and location with in the Document using depth and location with in the wound bedwound bed--use clock as guideuse clock as guide
LPLP--3M3M--05/0805/08
Exudate AssessmentExudate AssessmentAmountAmount--none, light, none, light, moderate, heavymoderate, heavyTypeType–– SerousSerous--clear, clear, –– SerosanginousSerosanginous or or
blood tingedblood tinged–– SanginousSanginous--bloody bloody –– OtherOther--yellow, tan, yellow, tan,
greengreen
ConsistencyConsistency–– PurulentPurulent–– ThickThick–– ThinThin–– MilkyMilky
OdorOdor–– AbsentAbsent–– FaintFaint–– StrongStrong–– FoulFoul
LPLP--3M3M--05/0805/08
Wound EdgesWound EdgesOpen EdgesOpen Edges–– Allow cells to migrate Allow cells to migrate
or move freely across or move freely across the wound, critical to the wound, critical to wound healing. wound healing. (epithelialization)(epithelialization)
–– Edges health, pink or Edges health, pink or pearly in colorpearly in color
Closed or rolled Closed or rolled –– Healing is halted or Healing is halted or
slowed downslowed down–– Upper layers of Upper layers of
epidermis roll down, epidermis roll down, epithelial cells can not epithelial cells can not migratemigrate
6
LPLP--3M3M--05/0805/08
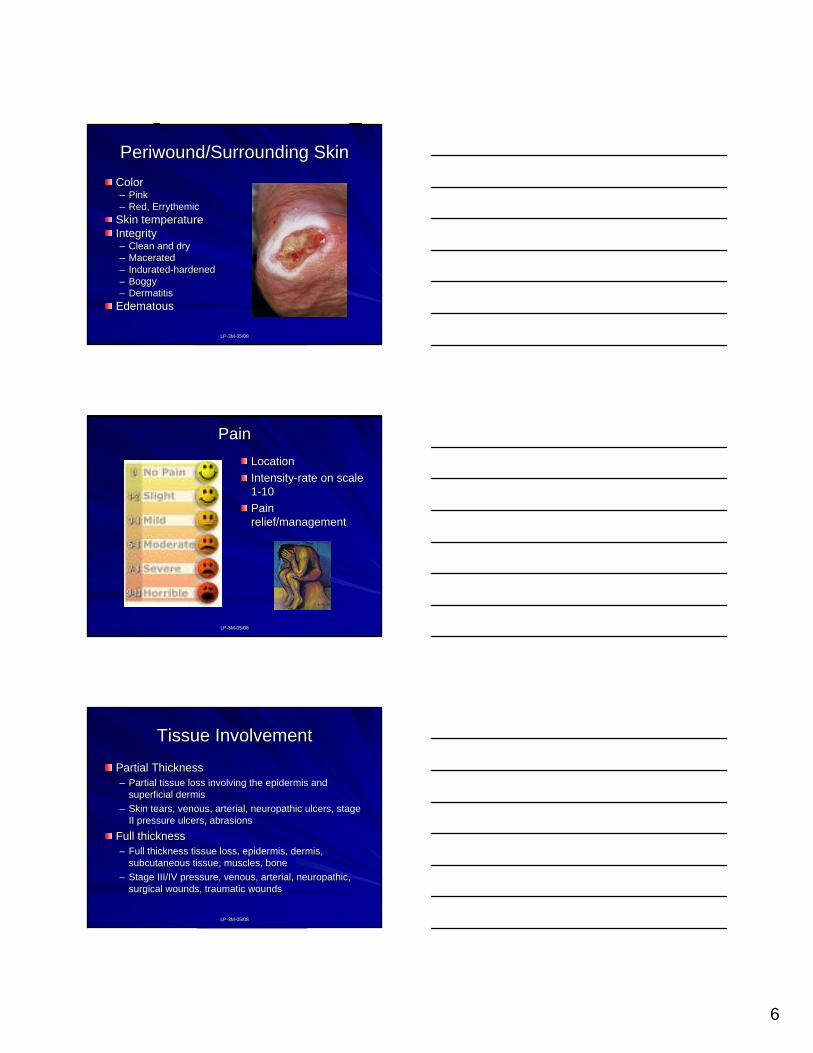
Periwound/Surrounding SkinPeriwound/Surrounding SkinColorColor–– PinkPink–– Red, ErrythemicRed, Errythemic
Skin temperatureSkin temperatureIntegrityIntegrity–– Clean and dryClean and dry–– MaceratedMacerated–– InduratedIndurated--hardenedhardened–– BoggyBoggy–– DermatitisDermatitis
EdematousEdematous
LPLP--3M3M--05/0805/08
PainPainLocationLocationIntensityIntensity--rate on scale rate on scale 11--1010Pain Pain relief/managementrelief/management
LPLP--3M3M--05/0805/08
Tissue InvolvementTissue Involvement
Partial ThicknessPartial Thickness–– Partial tissue loss involving the epidermis and Partial tissue loss involving the epidermis and
superficial dermissuperficial dermis–– Skin tears, venous, arterial, neuropathic ulcers, stage Skin tears, venous, arterial, neuropathic ulcers, stage
II pressure ulcers, abrasionsII pressure ulcers, abrasions
Full thicknessFull thickness–– Full thickness tissue loss, epidermis, dermis, Full thickness tissue loss, epidermis, dermis,
subcutaneous tissue, muscles, bonesubcutaneous tissue, muscles, bone–– Stage III/IV pressure, venous, arterial, neuropathic, Stage III/IV pressure, venous, arterial, neuropathic,
surgical wounds, traumatic woundssurgical wounds, traumatic wounds
7
LPLP--3M3M--05/0805/08
Pressure UlcersPressure Ulcers
Localized injury to skin and/or underling Localized injury to skin and/or underling tissuetissueCause: Pressure over bony prominenceCause: Pressure over bony prominenceFriction, shear, moisture contributing Friction, shear, moisture contributing factorsfactors
LPLP--3M3M--05/0805/08
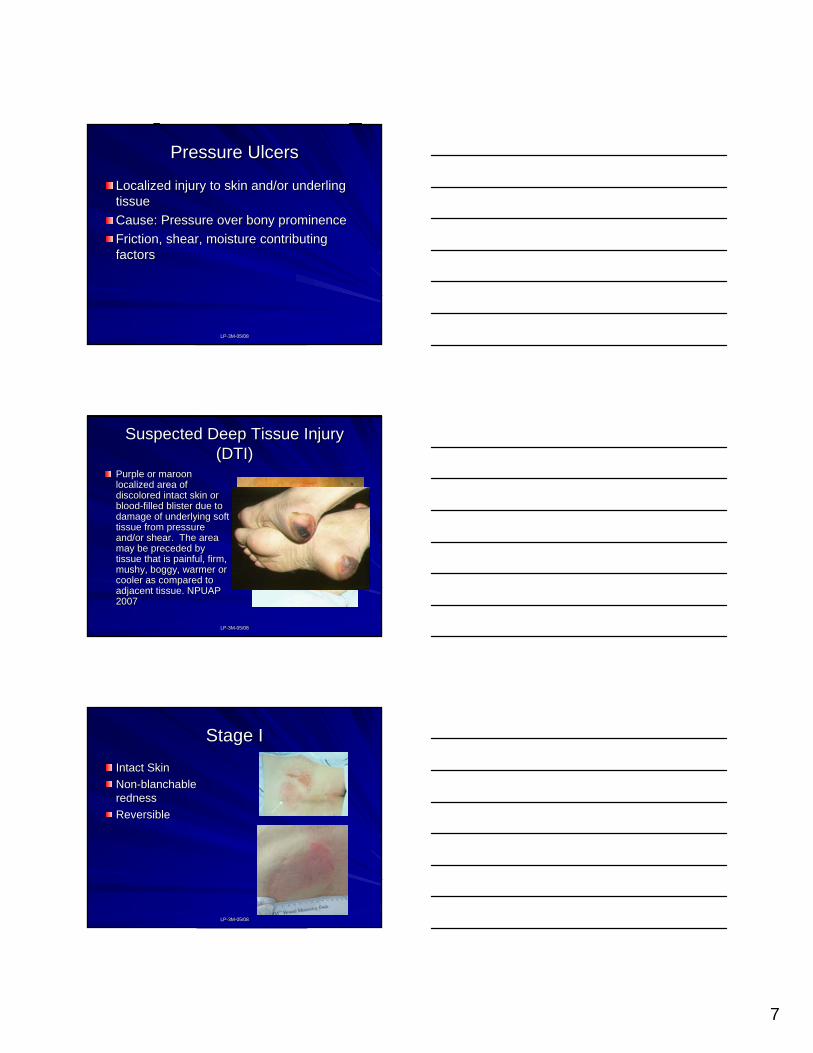
Suspected Deep Tissue Injury Suspected Deep Tissue Injury (DTI)(DTI)
Purple or maroon Purple or maroon localized area of localized area of discolored intact skin or discolored intact skin or bloodblood--filled blister due to filled blister due to damage of underlying soft damage of underlying soft tissue from pressure tissue from pressure and/or shear. The area and/or shear. The area may be preceded by may be preceded by tissue that is painful, firm, tissue that is painful, firm, mushy, boggy, warmer or mushy, boggy, warmer or cooler as compared to cooler as compared to adjacent tissue. NPUAP adjacent tissue. NPUAP 20072007
LPLP--3M3M--05/0805/08
Stage IStage I
Intact SkinIntact SkinNonNon--blanchableblanchablerednessrednessReversibleReversible
8
LPLP--3M3M--05/0805/08
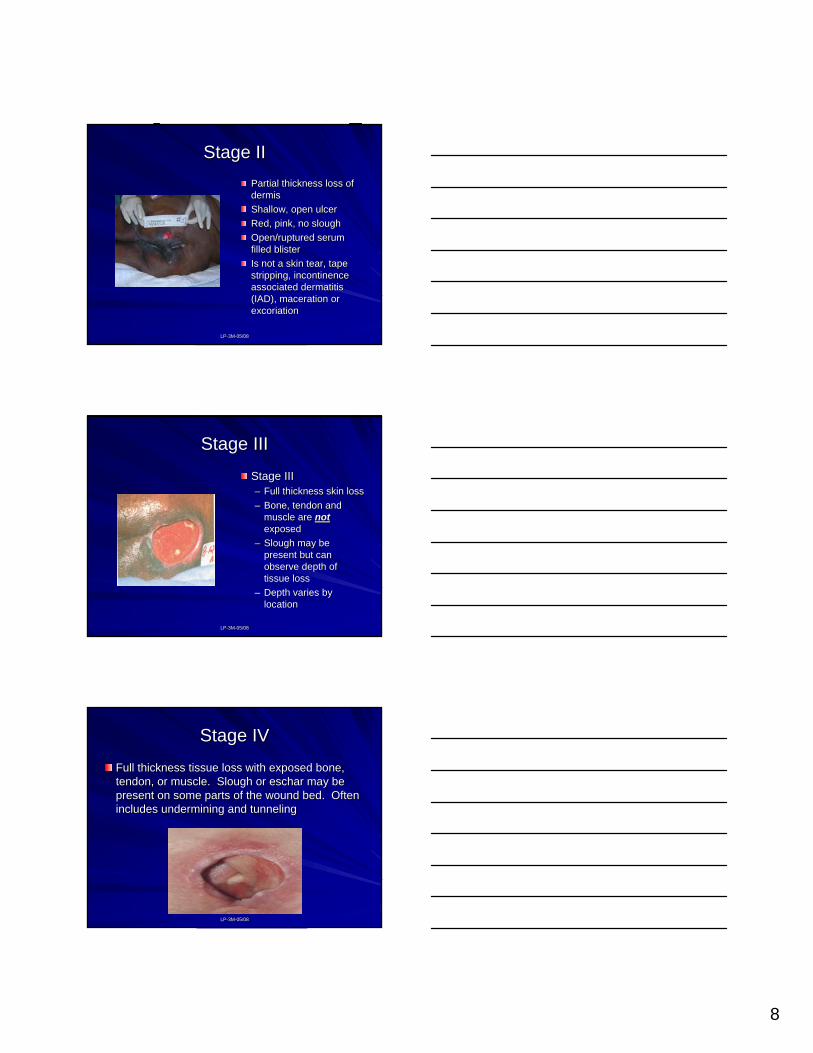
Stage II Stage II Partial thickness loss of Partial thickness loss of dermisdermisShallow, open ulcerShallow, open ulcerRed, pink, no sloughRed, pink, no sloughOpen/ruptured serum Open/ruptured serum filled blisterfilled blisterIs not a skin tear, tape Is not a skin tear, tape stripping, incontinence stripping, incontinence associated dermatitis associated dermatitis (IAD), maceration or (IAD), maceration or excoriationexcoriation
LPLP--3M3M--05/0805/08
Stage IIIStage III
Stage IIIStage III–– Full thickness skin lossFull thickness skin loss–– Bone, tendon and Bone, tendon and
muscle are muscle are not not exposedexposed
–– Slough may be Slough may be present but can present but can observe depth of observe depth of tissue losstissue loss
–– Depth varies by Depth varies by locationlocation
LPLP--3M3M--05/0805/08
Stage IVStage IV
Full thickness tissue loss with exposed bone, Full thickness tissue loss with exposed bone, tendon, or muscle. Slough or eschar may be tendon, or muscle. Slough or eschar may be present on some parts of the wound bed. Often present on some parts of the wound bed. Often includes undermining and tunnelingincludes undermining and tunneling
9
LPLP--3M3M--05/0805/08
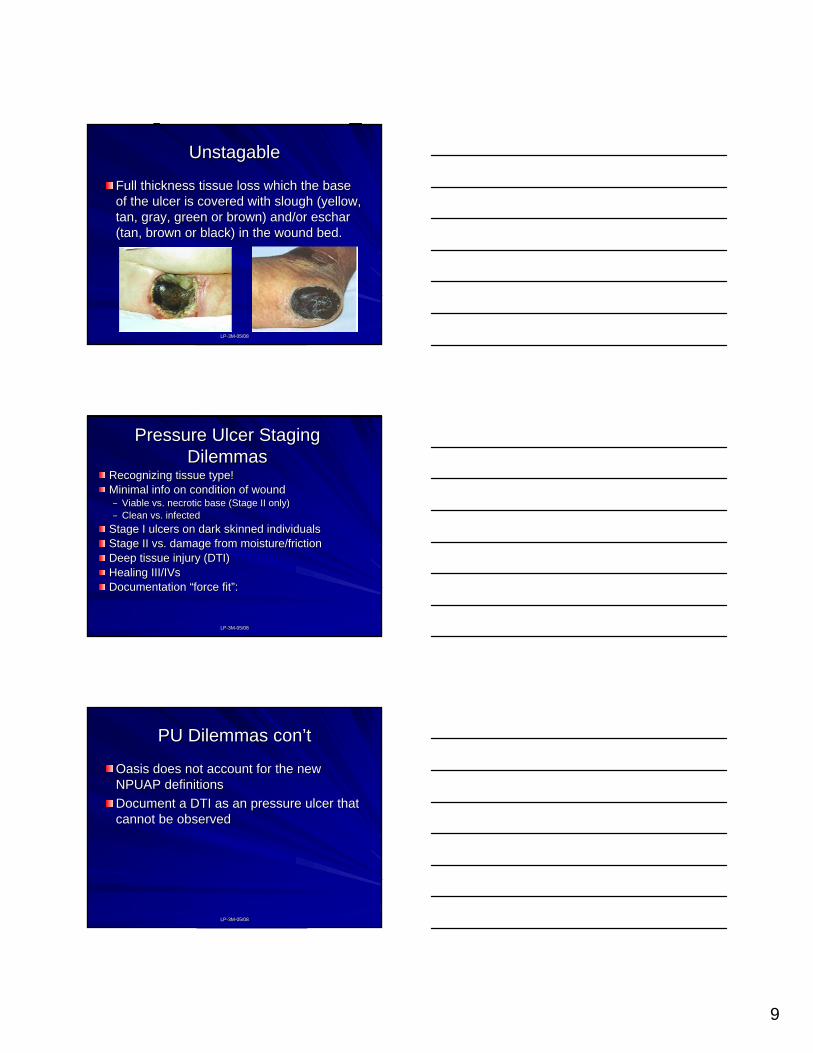
UnstagableUnstagable
Full thickness tissue loss which the base Full thickness tissue loss which the base of the ulcer is covered with slough (yellow, of the ulcer is covered with slough (yellow, tan, gray, green or brown) and/or eschar tan, gray, green or brown) and/or eschar (tan, brown or black) in the wound bed.(tan, brown or black) in the wound bed.
LPLP--3M3M--05/0805/08
Pressure Ulcer Staging Pressure Ulcer Staging DilemmasDilemmas
Recognizing tissue type!Recognizing tissue type!Minimal info on condition of woundMinimal info on condition of wound–– Viable vs. necrotic base (Stage II only)Viable vs. necrotic base (Stage II only)–– Clean vs. infectedClean vs. infected
Stage I ulcers on dark skinned individualsStage I ulcers on dark skinned individualsStage II vs. damage from moisture/frictionStage II vs. damage from moisture/frictionDeep tissue injury (DTI)Deep tissue injury (DTI)Healing III/IVsHealing III/IVsDocumentation Documentation ““force fitforce fit””::
LPLP--3M3M--05/0805/08
PU Dilemmas conPU Dilemmas con’’tt
Oasis does not account for the new Oasis does not account for the new NPUAP definitionsNPUAP definitionsDocument a DTI as an pressure ulcer that Document a DTI as an pressure ulcer that cannot be observedcannot be observed
10
LPLP--3M3M--05/0805/08
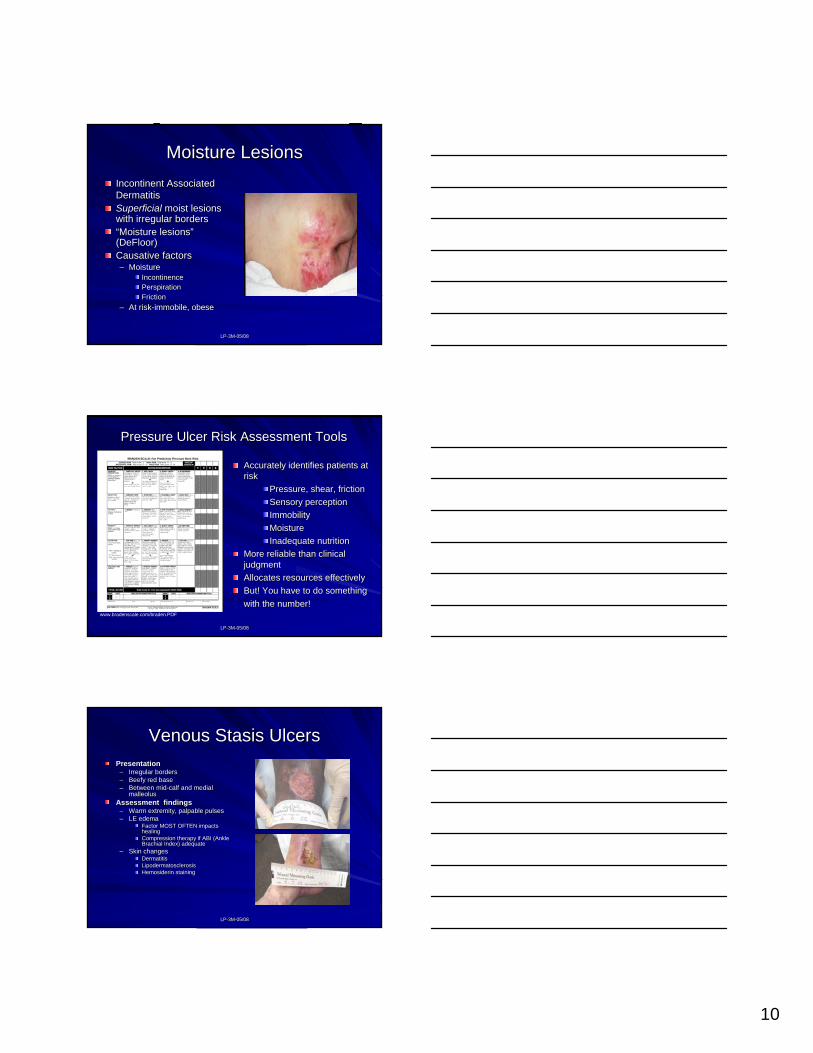
Moisture LesionsMoisture LesionsIncontinent Associated Incontinent Associated DermatitisDermatitisSuperficial Superficial moist lesions moist lesions with irregular borderswith irregular borders““Moisture lesionsMoisture lesions””((DeFloorDeFloor))Causative factorsCausative factors–– MoistureMoisture
IncontinenceIncontinencePerspirationPerspirationFrictionFriction
–– At riskAt risk--immobile, obeseimmobile, obese
LPLP--3M3M--05/0805/08
Pressure Ulcer Risk Assessment ToolsPressure Ulcer Risk Assessment Tools
Accurately identifies patients at Accurately identifies patients at riskrisk
Pressure, shear, frictionPressure, shear, frictionSensory perceptionSensory perceptionImmobilityImmobilityMoistureMoistureInadequate nutritionInadequate nutrition
More reliable than clinical More reliable than clinical judgmentjudgmentAllocates resources effectivelyAllocates resources effectivelyBut! You have to do something But! You have to do something with the number!with the number!
www.bradenscale.com/braden.PDF
LPLP--3M3M--05/0805/08
Venous Stasis UlcersVenous Stasis UlcersPresentationPresentation
–– Irregular bordersIrregular borders–– Beefy red baseBeefy red base–– Between midBetween mid--calf and medial calf and medial
malleolusmalleolusAssessment findingsAssessment findings
–– Warm extremity, palpable pulsesWarm extremity, palpable pulses–– LE edemaLE edema
Factor MOST OFTEN impacts Factor MOST OFTEN impacts healinghealingCompression therapy if ABI (Ankle Compression therapy if ABI (Ankle Brachial Index) adequateBrachial Index) adequate
–– Skin changesSkin changesDermatitisDermatitisLipodermatosclerosisLipodermatosclerosisHemosiderin stainingHemosiderin staining
11
LPLP--3M3M--05/0805/08
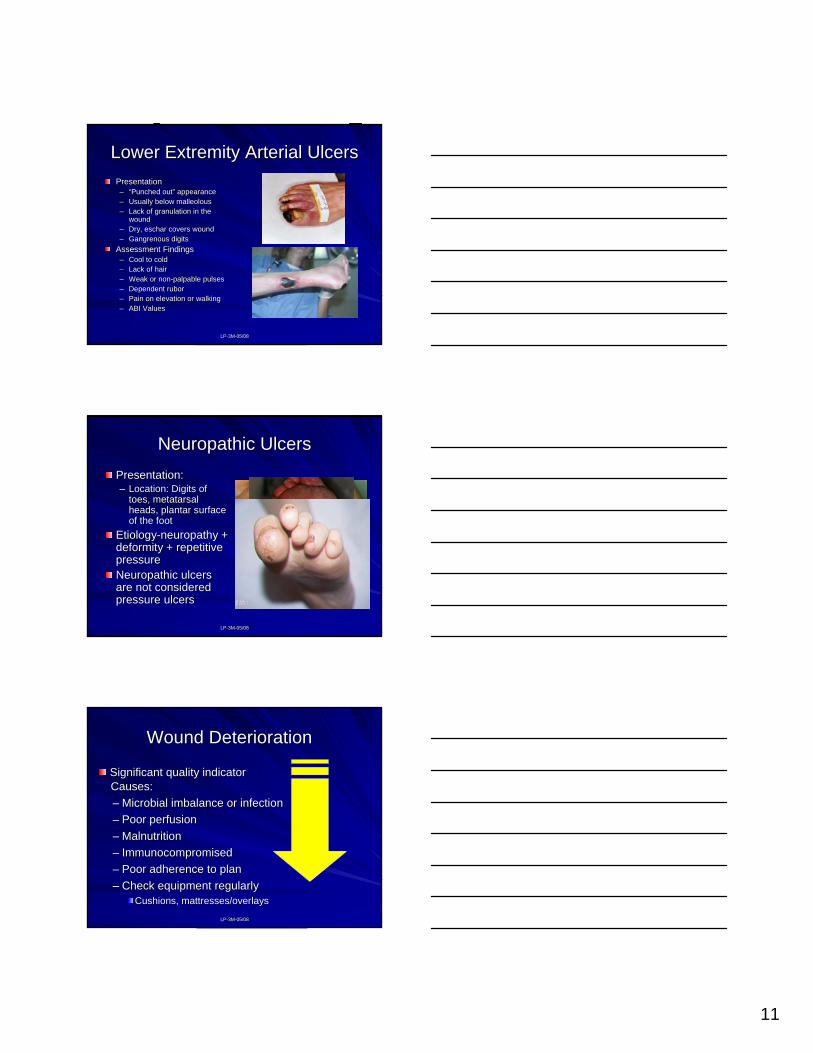
Lower Extremity Arterial UlcersLower Extremity Arterial UlcersPresentationPresentation–– ““Punched outPunched out”” appearanceappearance–– Usually below malleolousUsually below malleolous–– Lack of granulation in the Lack of granulation in the
woundwound–– Dry, eschar covers woundDry, eschar covers wound–– Gangrenous digitsGangrenous digits
Assessment FindingsAssessment Findings–– Cool to coldCool to cold–– Lack of hairLack of hair–– Weak or nonWeak or non--palpable pulsespalpable pulses–– Dependent ruborDependent rubor–– Pain on elevation or walkingPain on elevation or walking–– ABI ValuesABI Values
LPLP--3M3M--05/0805/08
Neuropathic UlcersNeuropathic UlcersPresentation:Presentation:–– Location: Digits of Location: Digits of
toes, metatarsal toes, metatarsal heads, plantar surface heads, plantar surface of the footof the foot
EtiologyEtiology--neuropathy + neuropathy + deformity + repetitive deformity + repetitive pressurepressureNeuropathic ulcers Neuropathic ulcers are not considered are not considered pressure ulcerspressure ulcers
LPLP--3M3M--05/0805/08
Wound DeteriorationWound Deterioration
Significant quality indicatorSignificant quality indicatorCauses:Causes:–– Microbial imbalance or infectionMicrobial imbalance or infection–– Poor perfusionPoor perfusion–– MalnutritionMalnutrition–– ImmunocompromisedImmunocompromised–– Poor adherence to planPoor adherence to plan–– Check equipment regularlyCheck equipment regularly
Cushions, mattresses/overlaysCushions, mattresses/overlays
12
LPLP--3M3M--05/0805/08
Wound DeteriorationWound DeteriorationLocal signsLocal signs–– Pain develops or Pain develops or
increasesincreases–– Edema developsEdema develops–– Poor quality/ color tissue Poor quality/ color tissue
in basein base–– DDrainage rainage
changes/increaseschanges/increases–– FoulFoul odorodor–– Dusky wound edgesDusky wound edges–– Surrounding Surrounding
(advancing!) erythema (advancing!) erythema or indurationor induration
Systemic SymptomsSystemic Symptoms–– FeverFever–– MalaiseMalaise–– Elevated blood Elevated blood
glucose in DMglucose in DM–– FluFlu--like Symptomslike Symptoms–– Change in vital signsChange in vital signs–– Change in orientationChange in orientation
LPLP--3M3M--05/0805/08
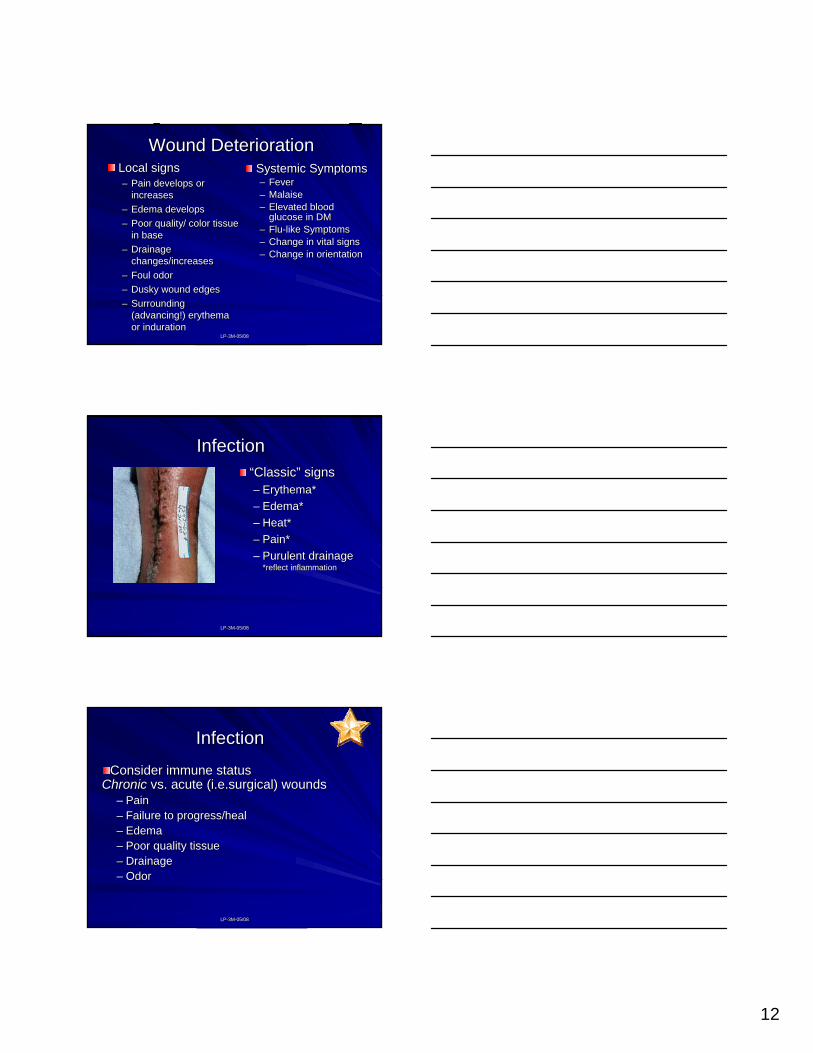
InfectionInfection““ClassicClassic”” signssigns–– Erythema*Erythema*–– Edema*Edema*–– Heat*Heat*–– Pain*Pain*–– Purulent drainagePurulent drainage
*reflect inflammation*reflect inflammation
LPLP--3M3M--05/0805/08
InfectionInfection
Consider immune statusConsider immune statusChronicChronic vs. acute (i.e.surgical) woundsvs. acute (i.e.surgical) wounds
–– PainPain–– Failure to progress/healFailure to progress/heal–– EdemaEdema–– Poor quality tissuePoor quality tissue–– DDrainagerainage–– OOdordor
13
LPLP--3M3M--05/0805/08
Culturing the WoundCulturing the Wound
Method:Method:1.1. Cleanse the woundCleanse the wound2.2. Moisten swab with Moisten swab with
NSNS3.3. Obtain specObtain spec
–– ZZ--strokestroke–– LevineLevine’’s techniques technique
–– DonDon’’t culture necrotic t culture necrotic (non(non--viable) tissue!viable) tissue!
1 cm.
LPLP--3M3M--05/0805/08
EvidenceEvidence--Based PracticeBased Practice
““The integration of best research evidence The integration of best research evidence with clinical expertise and patient values to with clinical expertise and patient values to facilitate clinical decision makingfacilitate clinical decision making””
(Bryant A.R., and Nix, D.P. 2007. Acute & Chronic Wounds, (Bryant A.R., and Nix, D.P. 2007. Acute & Chronic Wounds, Current Management Concepts, Third Edition. St. Louis: Mosby, Current Management Concepts, Third Edition. St. Louis: Mosby, ElservierElservier, p 10), p 10)
LPLP--3M3M--05/0805/08
EvidenceEvidence--Based PracticeBased Practice
Scientific evidenceScientific evidenceGuide clinical decisionsGuide clinical decisionsGuide clinical interventionsGuide clinical interventionsFocus on qualityFocus on qualityHelp reduce health care costsHelp reduce health care costsBest PracticeBest Practice-- Use of evidencedUse of evidenced--based based practice to guide care interventions, practice to guide care interventions, provides for consistency in careprovides for consistency in care
14
LPLP--3M3M--05/0805/08
Guidelines for PracticeGuidelines for Practicewww.guidelines.govwww.guidelines.gov–– National Guideline ClearinghouseNational Guideline Clearinghouse–– Database of evidencedDatabase of evidenced--based clinical practice guidelines and based clinical practice guidelines and
related documentsrelated documents–– Free onFree on--line accessline access–– Agency for Health Resource & QualityAgency for Health Resource & Quality
AHRQ (AHCPR)AHRQ (AHCPR)www.wocn.orgwww.wocn.org -- Wound Ostomy Wound Ostomy Continence Nurses Society Continence Nurses Society
www.whs.orgwww.whs.org -- Wound Healing SocietyWound Healing Society
LPLP--3M3M--05/0805/08
Clinical Staff EducationClinical Staff Education
Quarterly presentation by WOCN / Wound Care Quarterly presentation by WOCN / Wound Care Specialist Specialist –– Wound classificationWound classification–– Assessment parametersAssessment parameters–– Documentation criteriaDocumentation criteria–– Wound bed preparationWound bed preparation–– Evidenced based treatment protocolsEvidenced based treatment protocols–– Nutrition Nutrition –– Support surface criteriaSupport surface criteria–– Supply management / agency formularySupply management / agency formulary
LPLP--3M3M--05/0805/08
Clinical Staff EducationClinical Staff Education
CoCo--visits with case managers/clinical staffvisits with case managers/clinical staffCompetency FairCompetency Fair–– Stations (Pressure Ulcers, Diabetic Ulcers, Stations (Pressure Ulcers, Diabetic Ulcers,
Venous Stasis Ulcers etc)Venous Stasis Ulcers etc)--identify the woundidentify the wound–– Identify appropriate wound treatment planIdentify appropriate wound treatment plan–– Case studiesCase studies--scenarios scenarios
15
LPLP--3M3M--05/0805/08
Utilizing your WOCNUtilizing your WOCN
Promote positive patient outcomesPromote positive patient outcomesDevelop patient care policies and Develop patient care policies and treatment planstreatment plansEstablish standards of care of patientsEstablish standards of care of patients–– Chronic woundsChronic wounds–– OstomiesOstomies–– IncontinenceIncontinence
Provide education to homecare staffProvide education to homecare staff
LPLP--3M3M--05/0805/08
In light of recent OASIS changes:In light of recent OASIS changes:–– Review of OASIS for accuracyReview of OASIS for accuracy–– Assist with supply utilization Assist with supply utilization –– Assist with the involvement of therapy to Assist with the involvement of therapy to
improve patient mobility and independenceimprove patient mobility and independence–– Assist with management of longAssist with management of long--term wound term wound
care patients, cost control and optimal care patients, cost control and optimal outcomesoutcomes
(Peirce, B, Oasis Update, (Peirce, B, Oasis Update, WOCNewsWOCNews, Issue 1 2008. p12, Issue 1 2008. p12--13)13)
LPLP--3M3M--05/0805/08
What Your Peers are Doing!What Your Peers are Doing!The Wound Consultant Model: The Wound Consultant Model:
A New A New ProacativeProacative Position on Wound CarePosition on Wound Care
CWOCN Consultant CWOCN Consultant –– considered expert in the considered expert in the of wound careof wound care1:1 work with clinician1:1 work with clinicianGoal: Improve patient care outcomes and Goal: Improve patient care outcomes and provide higher standard of care to wound, provide higher standard of care to wound, ostomy, and continence patientsostomy, and continence patients
((TedfordTedford, S.T., May/June 2007. Remington Report, Volume 15, Issue 3, p 3, S.T., May/June 2007. Remington Report, Volume 15, Issue 3, p 34, 2364, 236--37.)37.)
16
LPLP--3M3M--05/0805/08
Wound Consultant ModelWound Consultant Model
Consultant Focus:Consultant Focus:–– Verbal referral on every patient with a woundVerbal referral on every patient with a wound–– Review of patient history, etiology, wound assessment, Review of patient history, etiology, wound assessment,
comorbitities, resources, and caregiver availability comorbitities, resources, and caregiver availability –– Digital photography utilized for patients not needing an Digital photography utilized for patients not needing an
inin--home visithome visit–– If visit requested, joint visit madeIf visit requested, joint visit made
CWOCN makes hands on assessment and CWOCN makes hands on assessment and recommendations for care recommendations for care Educational opportunities for CWOCN and clinicianEducational opportunities for CWOCN and clinician
–– Result: Lower utilization of visits and supplies, best Result: Lower utilization of visits and supplies, best treatment initiated during the first visittreatment initiated during the first visit
LPLP--3M3M--05/0805/08
Wound Consultant ModelWound Consultant Model
Focus on Improved OutcomesFocus on Improved Outcomes–– Review of OASIS documentation for accuracyReview of OASIS documentation for accuracy–– Verification of appropriate treatment planVerification of appropriate treatment plan–– Compliance with documentation Compliance with documentation –– Determination of appropriate support surfaceDetermination of appropriate support surface–– Discharge auditsDischarge audits--identified potential OASIS errors, identified potential OASIS errors,
this information used for staff educationthis information used for staff education
LPLP--3M3M--05/0805/08
Wound Consultant ModelWound Consultant Model
Education FocusEducation Focus–– Day long seminars to new clinical staff, basis Day long seminars to new clinical staff, basis
of wound educationof wound educationAnatomy and physiology of skinAnatomy and physiology of skinPressure ulcers, lower extremity woundsPressure ulcers, lower extremity woundsWound assessment and documentationWound assessment and documentationSupport surface criteriaSupport surface criteriaAgency product formulary and supply managementAgency product formulary and supply management
17
LPLP--3M3M--05/0805/08
EducationEducation ((concon’’tt))–– Ongoing staff inOngoing staff in--services services
Focused on chart audit resultsFocused on chart audit resultsResults from consultation visitsResults from consultation visitsResults of documentation complianceResults of documentation compliance
–– Wound rounds at beginning of every Wound rounds at beginning of every multidisciplinary team meetingmultidisciplinary team meeting
LPLP--3M3M--05/0805/08
Wound Consultant ModelWound Consultant ModelResultsResults
–– Confident trusting relationship between CWOCN and Confident trusting relationship between CWOCN and clinical staff clinical staff –– beneficial to patientbeneficial to patient
–– Improvement in pressure ulcers increased by 16%Improvement in pressure ulcers increased by 16%–– Improvement in status of surgical wounds by 16%Improvement in status of surgical wounds by 16%–– Improvement in accuracy and compliance of Improvement in accuracy and compliance of
documentationdocumentation–– Improvement in appropriate wound care choices at Improvement in appropriate wound care choices at
SOCSOC–– Decrease in frequency of visitsDecrease in frequency of visits
LPLP--3M3M--05/0805/08
Questions?Questions?
18
LPLP--3M3M--05/0805/08
ReferencesReferences
BaranoskiBaranoski, S., and , S., and AyelloAyello, E. 2008. Wound Care Essentials, Practice Principles. , E. 2008. Wound Care Essentials, Practice Principles. Second Edition. Philadelphia: Lippincott Williams & WilliamsSecond Edition. Philadelphia: Lippincott Williams & Williams
Bryant A.R., and Nix, D.P. 2007. Acute & Chronic Wounds, CurrentBryant A.R., and Nix, D.P. 2007. Acute & Chronic Wounds, Current Management Management Concepts, Third Edition. St. Louis: Mosby.Concepts, Third Edition. St. Louis: Mosby.
National Pressure Ulcer Advisory National Pressure Ulcer Advisory PanalPanal: : www.npuap.orgwww.npuap.org
Peirce, B. Home Healthcare, OASIS Update, Peirce, B. Home Healthcare, OASIS Update, WOCNewsWOCNews, Issue 1, 2008, p 12, Issue 1, 2008, p 12--1313
TedfordTedford, S.T., May/June 2007. What Your Peers are Doing! The Wound Cons, S.T., May/June 2007. What Your Peers are Doing! The Wound Consultant ultant Model: A New Model: A New ProacativeProacative Position on Wound Care, Remington Report, Volume 15, Position on Wound Care, Remington Report, Volume 15, Issue 3, p 34, 236Issue 3, p 34, 236--37.37.
Waite, R, Killian, P. EvidenceWaite, R, Killian, P. Evidence--Based Practice, Based Practice, www.advanceweb.com/nurseswww.advanceweb.com/nurses, , February 4, 2004February 4, 2004