Embed Size (px)
Citation preview
WOUND CARE AND REPAIR
FARAS ABUZEYAD, MD.
Epidemiology:
In USA > 10,000,000 annual ER visitsAverage cost of $200 per patient
Hollander et al: Wound Registry: Development and Validation. Ann Emerg Med, May 1995.
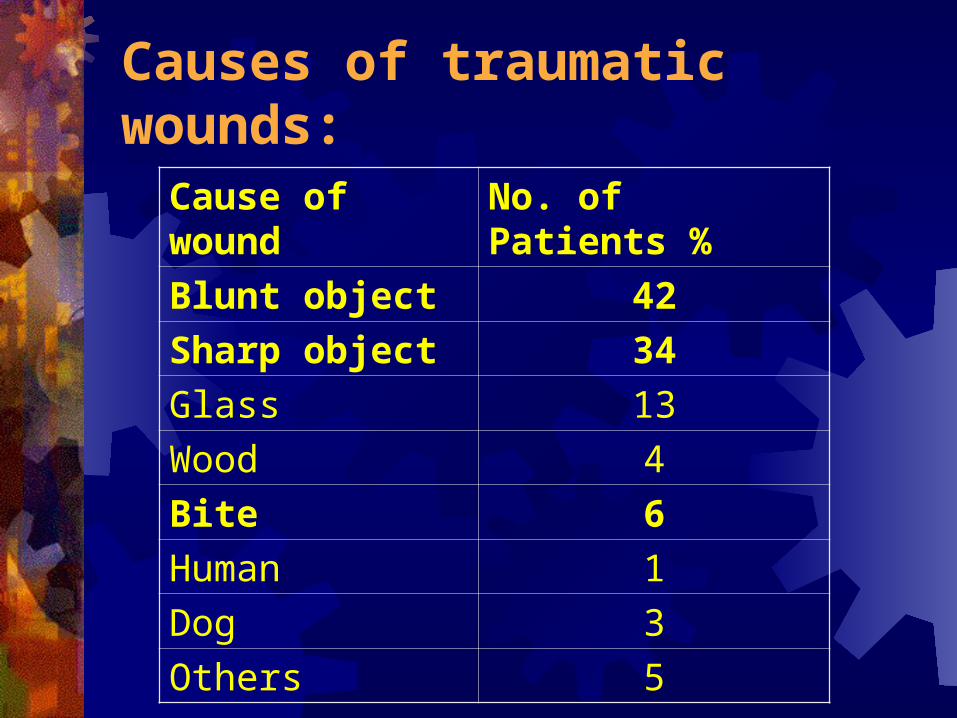
Causes of traumatic wounds:
Cause of wound No. of Patients %
Blunt object 42
Sharp object 34
Glass 13
Wood 4
Bite 6
Human 1
Dog 3
Others 5
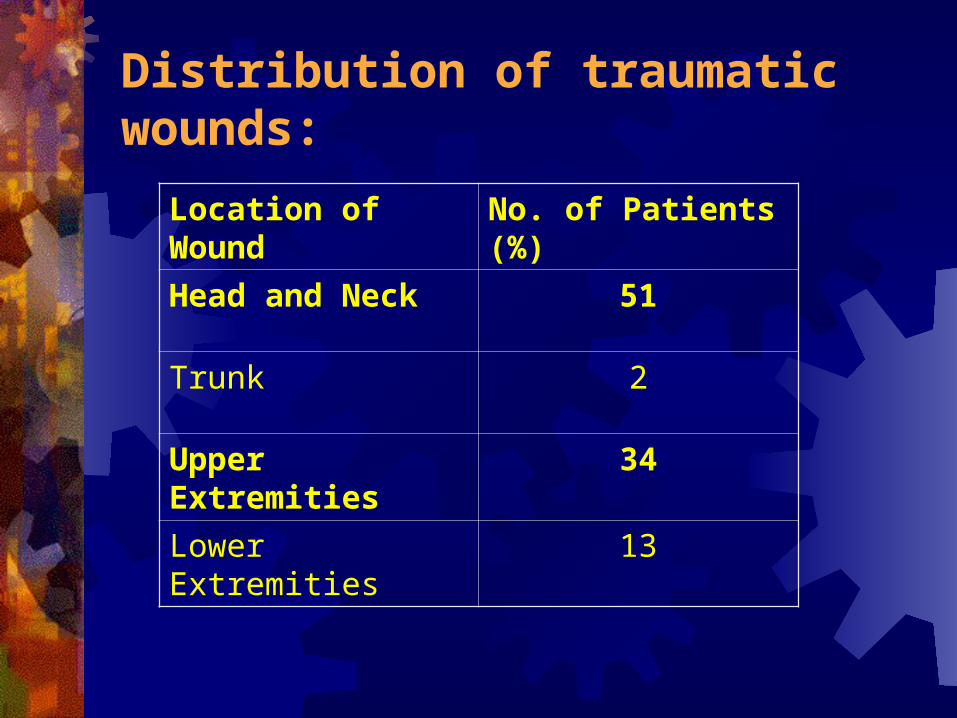
Distribution of traumatic wounds:
Location of Wound No. of Patients (%)
Head and Neck 51
Trunk 2
Upper Extremities 34
Lower Extremities 13
Malpractice: Karcz: Malpractice claims against emergency physicians
in Massachusetts; 1975-1993. Am J Emerg Med 1996. wounds claims 19.85%, and 3.15% total expenses
($1,235,597) American College of Emergency Physicians. Foresight
Issue 49, September 2000: Laceration mismanagement & failure to diagnose a retained foreign body is the 2nd most common malpractice claims against emergency physician
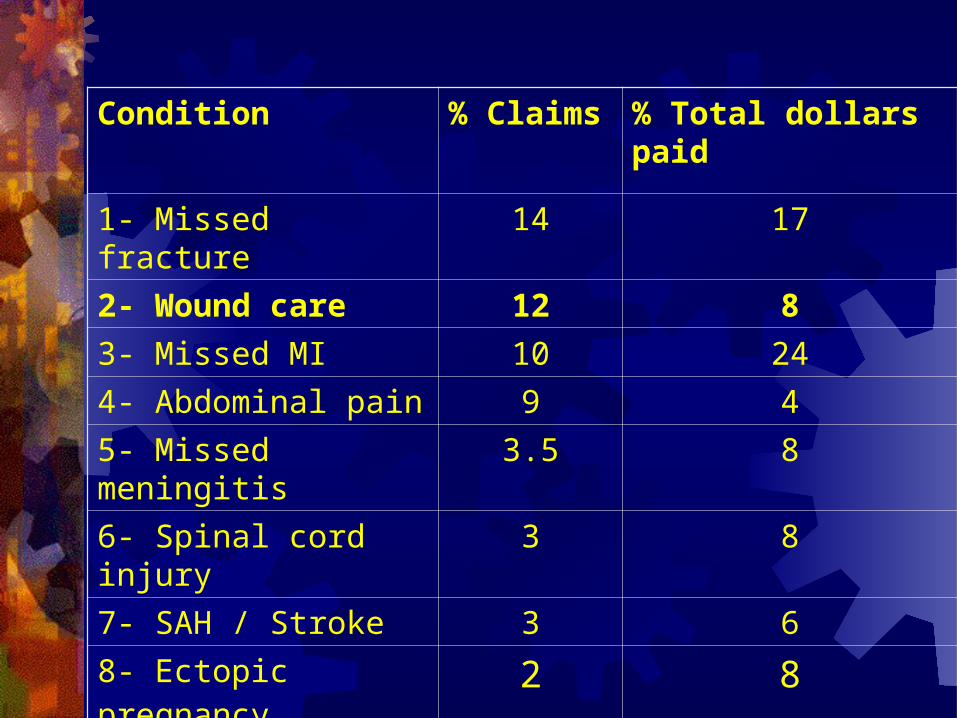
Condition % Claims % Total dollars paid
1- Missed fracture 14 17
2- Wound care 12 8
3- Missed MI 10 24
4- Abdominal pain 9 4
5- Missed meningitis 3.5 8
6- Spinal cord injury 3 8
7- SAH / Stroke 3 6
8- Ectopic pregnancy 2 8
What patients want? Adam: Patient Priorities With Traumatic
Lacerations. Am J Emerg Med, October 2000.
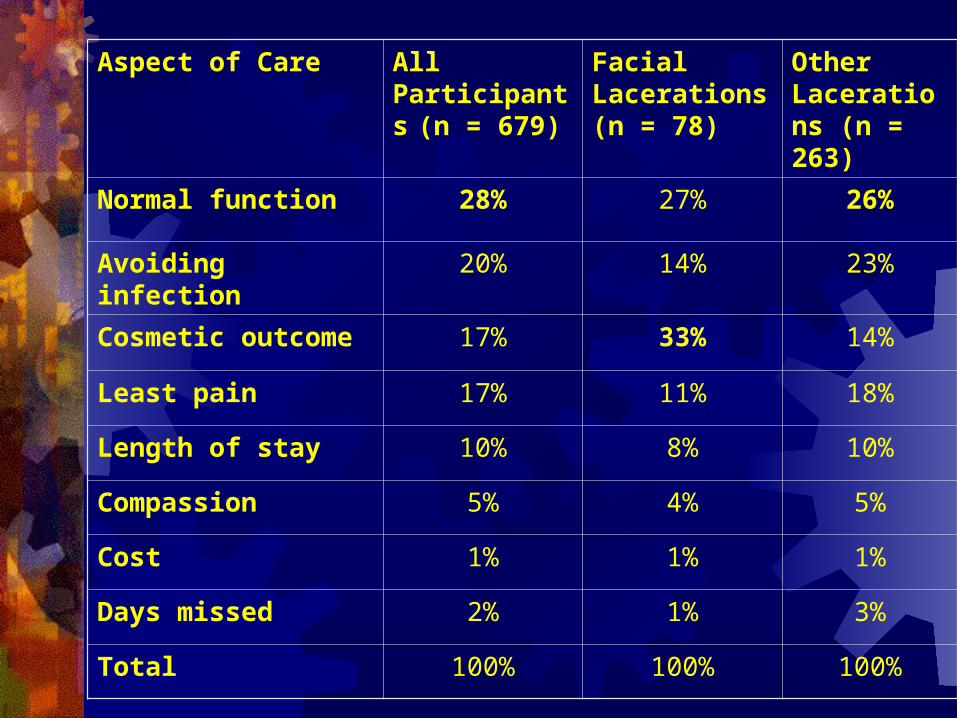
Aspect of Care All Participants
(n = 679) Facial Lacerations (n = 78)
Other Lacerations (n = 263)
Normal function 28% 27% 26%
Avoiding infection 20% 14% 23%
Cosmetic outcome 17% 33% 14%
Least pain 17% 11% 18%
Length of stay 10% 8% 10%
Compassion 5% 4% 5%
Cost 1% 1% 1%
Days missed 2% 1% 3%
Total 100% 100% 100%
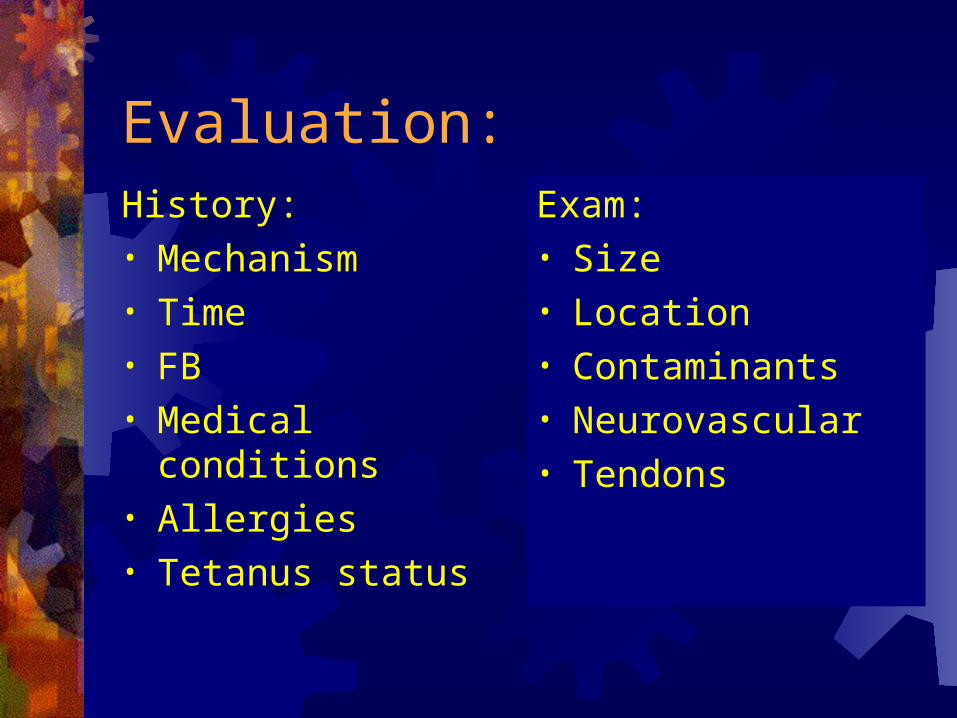
Evaluation:History:• Mechanism• Time• FB• Medical conditions• Allergies• Tetanus status
Exam:• Size• Location• Contaminants • Neurovascular• Tendons
Universal Precautions:
CDC published guidelines on use of universal precautions.
Use of protective barriers:
eg. Gloves/ gowns/ masks/ eyewear
Will decrease exposure to infective material.
Gloves: Use latex free gloves Since March 1999, FDA reported:
2,330 latex allergic reactions
including 21 deaths
Bodiwala: Surgical gloves during wound repair in the accident and emergency department. Lancet 1982.
randomized 337 patients to ‘gloves’ or ‘careful hand-washing, no gloves’:
INFECTION GLOVES NO GLOVES
None 167 (82.7%) 170 (82.5%) ‘Mild’ 27 (13.4%) 27 (13.1%) ‘Severe’ 8 (4.0%) 9 (4.4%)
Caliendo: Surgical masks during laceration repair. J Am Coll Emerg Phys 1976.
Alternated face mask / no mask for 99 wound repairs:
Mask: 1 / 47 infectedNo mask: 0 / 42 infected
Local Anesthesia: 2 main groups
1- Esters: Cocaine Procaine (Novocain) Benzocaine
(Cetacaine) Tetracaine
(Pontocaine) Chloroprocaine
(Nesacaine)
2- Amides: Lidocaine (Xylocaine) Mepivacaine (Polocaine,
Carbocaine) Bupivacaine (Marcaine) Etidocaine (Duranest) Prilocaine
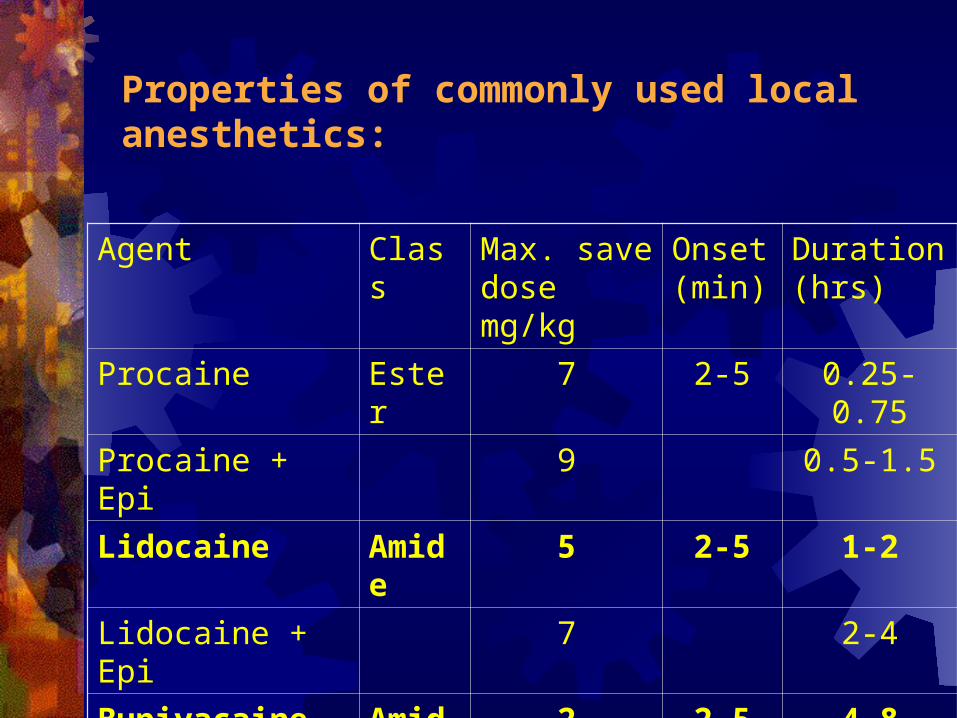
Properties of commonly used local anesthetics:
Agent Class Max. save dose mg/kg
Onset (min)
Duration (hrs)
Procaine Ester 7 2-5 0.25-0.75
Procaine + Epi 9 0.5-1.5
Lidocaine Amide 5 2-5 1-2
Lidocaine + Epi 7 2-4
Bupivacaine Amide 2 2-5 4-8
Bupivacaine + Epi 3 8-16
Why Lidocaine? Less painfulRapid onsetLess cardiotoxicLess expensive
Morris: Comparison of pain associated with intradermal and subcutaneous infiltration with various local anesthetic solutions. Anesth Analg 1987.
24 volunteers each injected with 5 anesthetic agents and NS visual analog pain scale Etidocaine> Bupivacaine> Mepivacaine> NS>
Chloroprocaine> Lidocaine (least painful)
Methods to reduce pain of Lidocaine local infiltration:
1-Small-bore needles 2-Buffered solutions 3-Warmed solutions 4-Slow rates of injection 5-Injection through wound edges 6-Subcutaneous rather than intradermal
injection 7- Pretreatment with topical anesthetics
1-Small-bore needles: Edlich, 1988:30-gauge hurts less than a 27-gauge27-gauge hurts less than a 25-gauge, etc.
2-Buffered solutions: with sodium bicarbonate at a ratio of 1:10 change in the pH of the anesthetic solution does
not increase wound infection rates No compromise to anesthesia effect
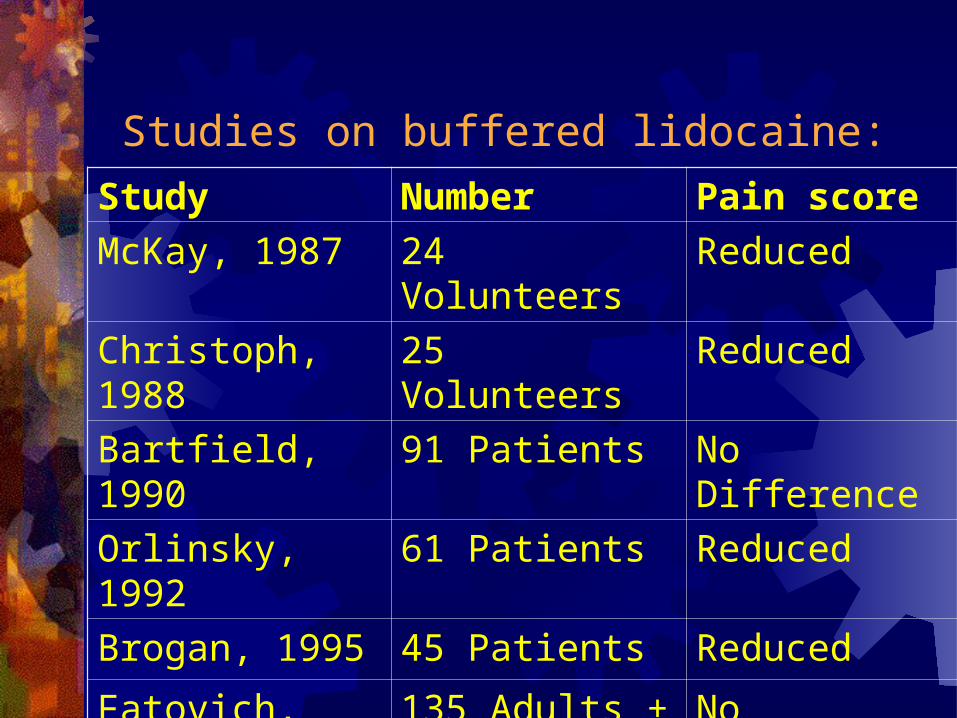
Studies on buffered lidocaine:
Study Number Pain score
McKay, 1987 24 Volunteers Reduced
Christoph, 1988 25 Volunteers Reduced
Bartfield, 1990 91 Patients No Difference
Orlinsky, 1992 61 Patients Reduced
Brogan, 1995 45 Patients Reduced
Fatovich, 1999 135 Adults + 136 children
No Difference
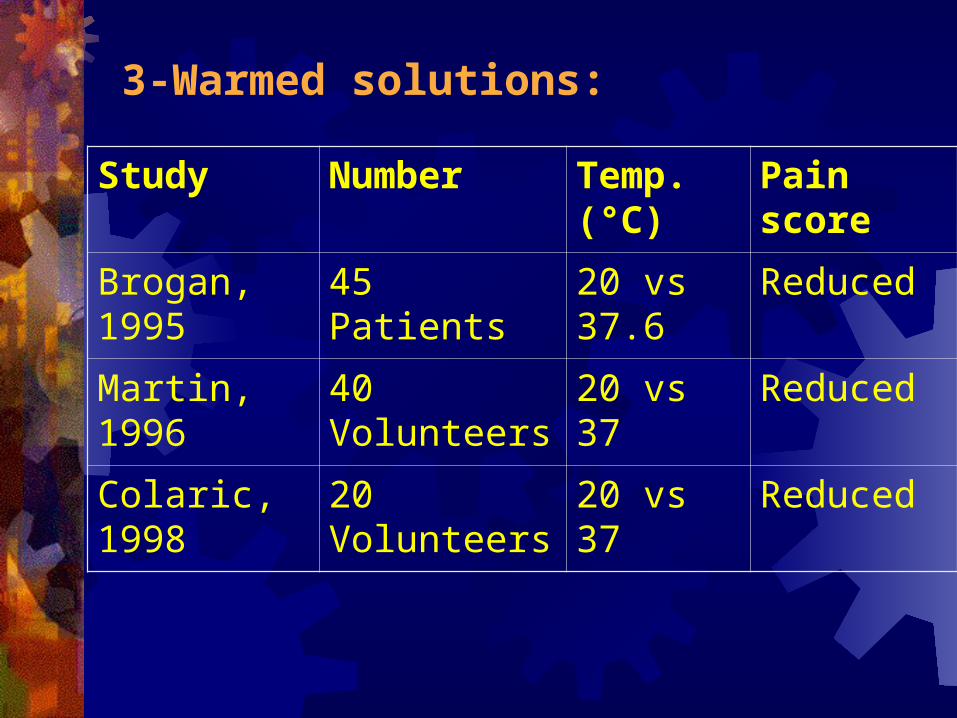
3-Warmed solutions:
Study Number Temp. (°C)
Pain score
Brogan, 1995 45 Patients 20 vs 37.6 Reduced
Martin, 1996 40 Volunteers 20 vs 37 Reduced
Colaric, 1998 20 Volunteers 20 vs 37 Reduced
Warming and Buffering have synergistic effect:
Mader, 1994 and Bartfield, 1995: Effect of warming and buffering on pain of Lidocaine infiltration.
Warming and Buffering have synergistic effect in reducing pain
Temp. used 40 and 38.9 °C vs room temp.
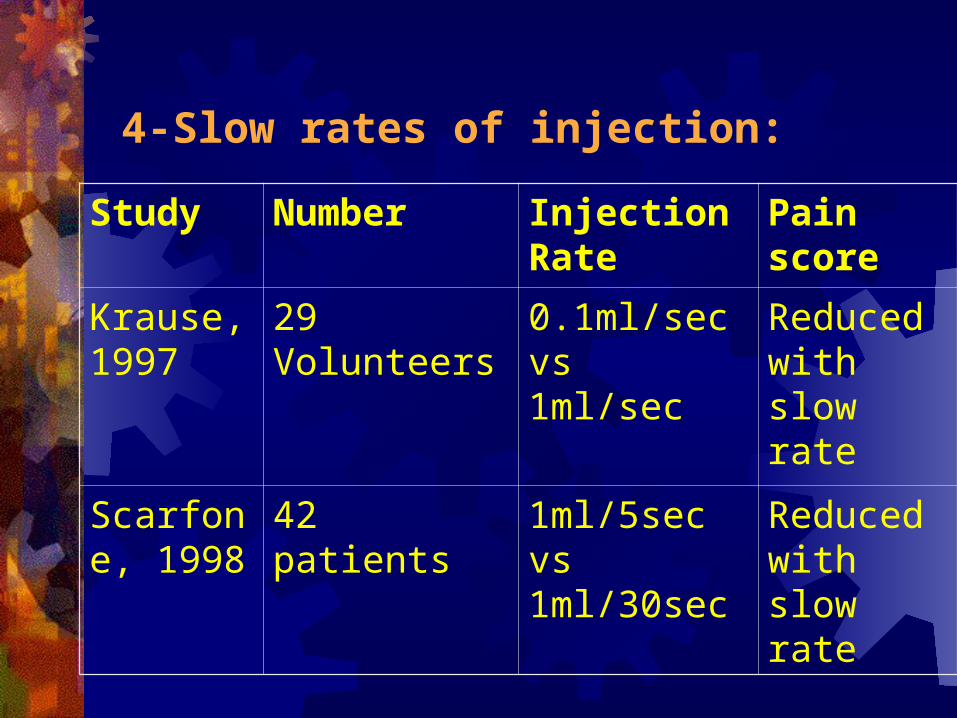
4-Slow rates of injection:
Study Number Injection Rate
Pain score
Krause, 1997
29 Volunteers 0.1ml/sec vs 1ml/sec
Reduced with slow rate
Scarfone, 1998
42 patients 1ml/5sec vs 1ml/30sec
Reduced with slow rate
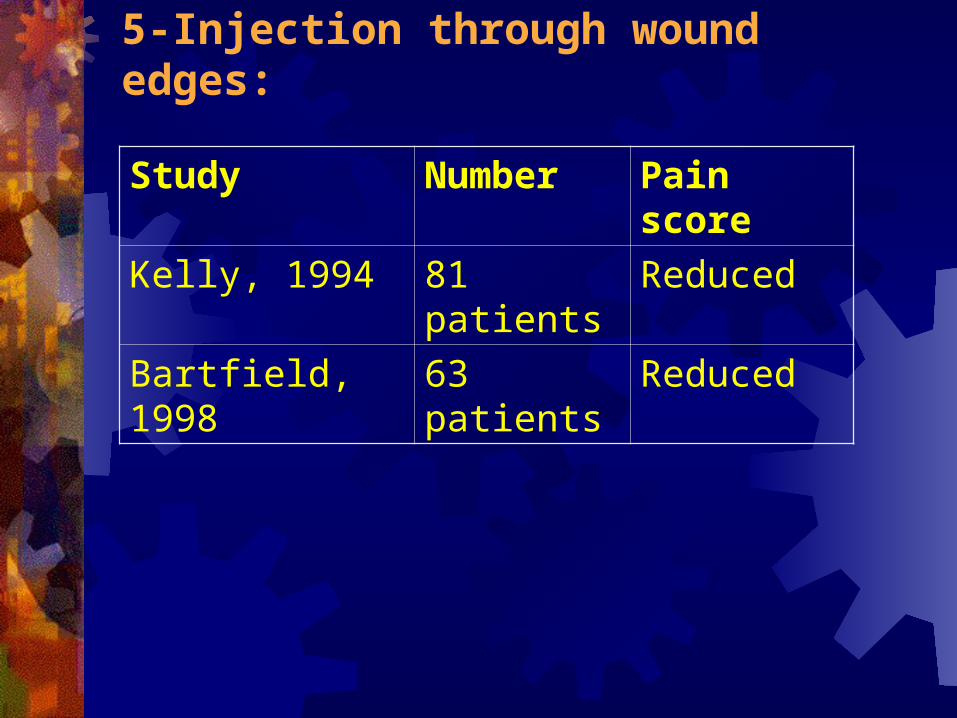
5-Injection through wound edges:
Study Number Pain score
Kelly, 1994 81 patients Reduced
Bartfield, 1998 63 patients Reduced
6-Subcutaneous rather than intradermal
injection:
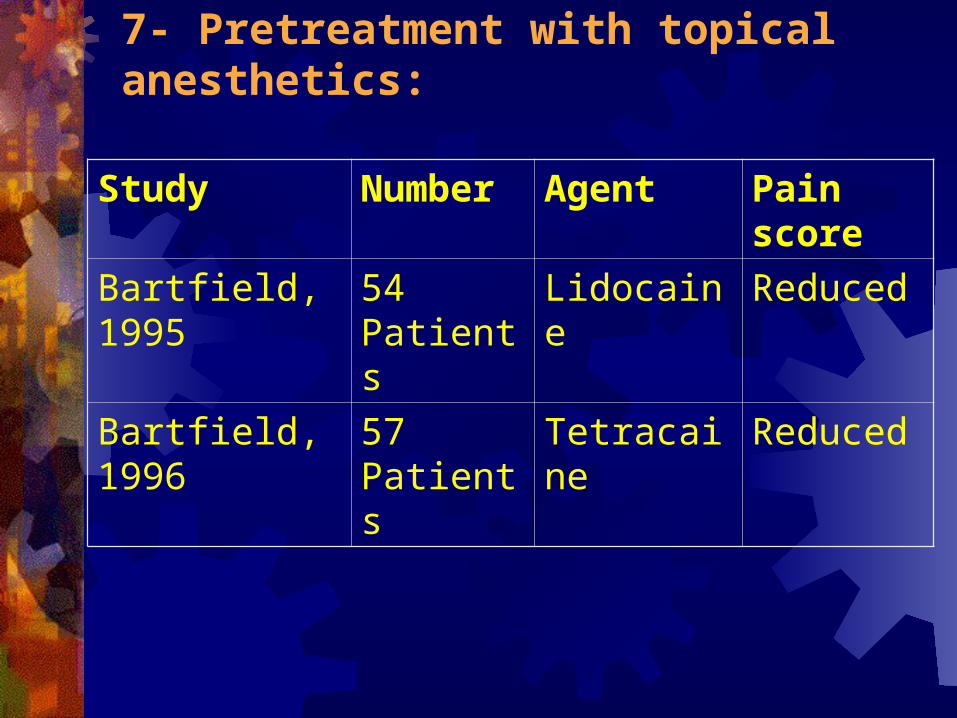
7- Pretreatment with topical anesthetics:
Study Number Agent Pain score
Bartfield, 1995 54 Patients Lidocaine Reduced
Bartfield, 1996 57 Patients Tetracaine Reduced
8- Digital / Regional nerve block: A critical skill for all ED physicians Save time Decrease possibility of systemic toxicity Less painful than local infiltration Do not cause the volume-related tissue distortion
Topical Anesthetic instead of local:
TAC: Tetracaine – 25 cc of 2% solution Adrenalin – 50 cc of a 1:1000 solution Cocaine – 11.8 gm Pryor, 1980 and Hegenbarth, 1990: topical TAC vs lidocaine infiltration, in laceration
repair No significant difference in anesthetic efficacy
TAC: Down sides are: Not reliable when used below the head Tissue toxic, Case reports of death and seizures Corneal damage Intense vasoconstriction avoid in digits, nose,
pinna and penis Must be mixed by hospital pharmacist Not approved by FDA Expensive – up to $35 / dose
LAT, LET, or XAP:
Lidocaine – 15cc of 2% viscous Adrenaline – 7.5cc of 1:1000 topical Tetracaine – 7.5cc of 2% topical Ernst-1995, Blackburn-1995, Ernst-1997: showed
effective anesthesia if left in place for 15 to 20 minutes Schilling-1995 and Amy-1995: As efficacious as TAC $5 / dose Much less potential for significant toxicity
Lidocaine with Epinepkrine:
In animal models, there is theoretic concern for increased risk of wound infection
Tissue ischemia and necrosis if injected in digits
Skin and Wound preparation: 1- Hair removal 2- Disinfecting the skin 3- Debridement 4-Wound Cleansing and Irrigation 5-Soaking
1- Hair removal:To shave or not to shave!
Seropian, 1971: 406 clean surgical wounds If shaved pre-op, 3.1% infection rate If depilated, 0.6% infection rate Howell, 1988: 68 scalp lacerations repaired without hair removal
(93% within 3 hours of injury), no infection at 5-day follow-up
2- Disinfecting the skin:
An ‘ideal agent’ does not exist – either tissue toxic or poorly bacteriostatic
Simple scrub water around wound should be sufficient
No studies have demonstrated the impact of cleaning intact skin on infection rate, however it is important to decrease bacterial load to minimize ongoing wound contamination.
Avoid mechanical scrubbing unless heavily contaminated (increase inflammation in animal data)
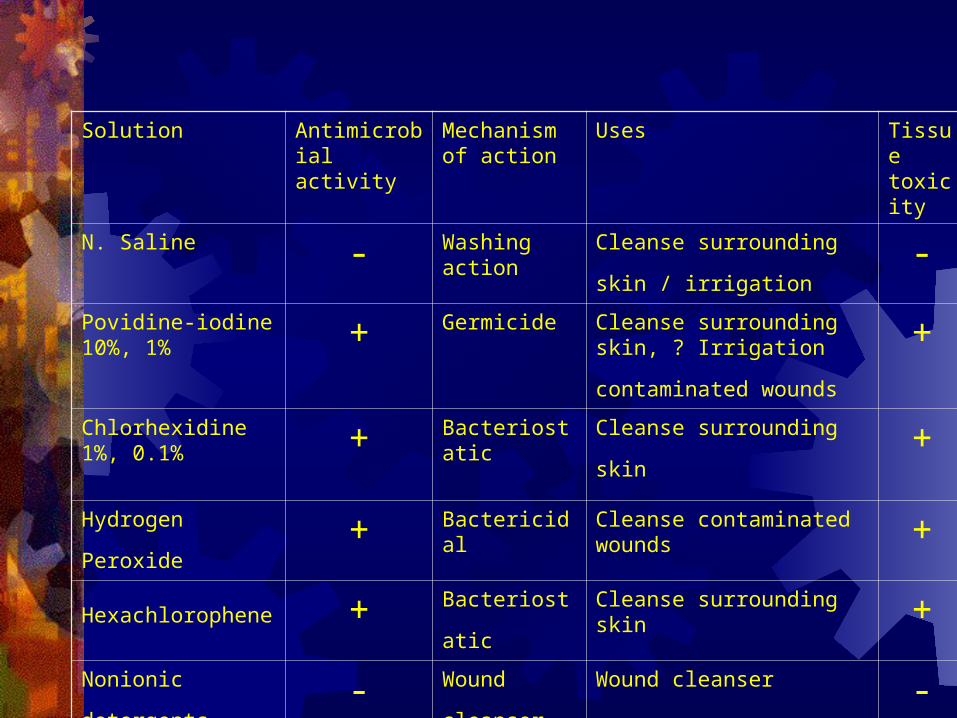
Solution Antimicrobial activity
Mechanism of action
Uses Tissue toxicity
N. Saline - Washing action Cleanse surrounding skin /
irrigation -
Povidine-iodine 10%, 1% + Germicide Cleanse surrounding skin, ?
Irrigation contaminated wounds +
Chlorhexidine 1%, 0.1% + Bacteriostatic
Cleanse surrounding skin +
Hydrogen Peroxide + Bactericidal Cleanse contaminated wounds +
Hexachlorophene + Bacteriostatic Cleanse surrounding skin +
Nonionic detergents - Wound
cleanser Wound cleanser -
3- Debridement: Devitalized soft tissue acts as a culture medium
promoting bacterial growth Inhibits leukocyte phagocytosis of bacteria and
subsequent kill Anaerobic environment within the devitalized
tissue may also limit leukocyte function
Dhingra V: Periphral Dissemination of Bacteria in Contaminated Wounds: Role of Devitalized tissue: Evaluation of Therapeutic Measures. Surgery, 1976.
Animal study, devitalized wounds contaminated with 3 Bacteria, treated with NS jet irrigation or debridement at 2, 4, 6 hr
Debridement more effective in reducing bacteria count and infection rate
4-Wound Cleansing and Irrigation: Decreasing wound contamination and hence
infection, "the solution to pollution is dilution." Indications Methods Pressure Solution Volume Side effects
1- Indications: Any contaminated or bite wounds Animal and human studies demonstrate irrigation lowers
infection rates in contaminated wounds Hollander JE et al: Irrigation in facial and scalp lacerations:
Does it alter outcome? Ann Emerg Med 1998. 1,923 patients 1,090 patients received saline irrigation, and 833
patients did not Nonbite, noncontaminated facial skin or scalp lacerations who
presented less than 6 hours No difference in wound infection rate or cosmetic appearance
2- Methods:
• Bulb syringe• IV bag +/- pressure cuff• Syringe and needle• Jet lavage
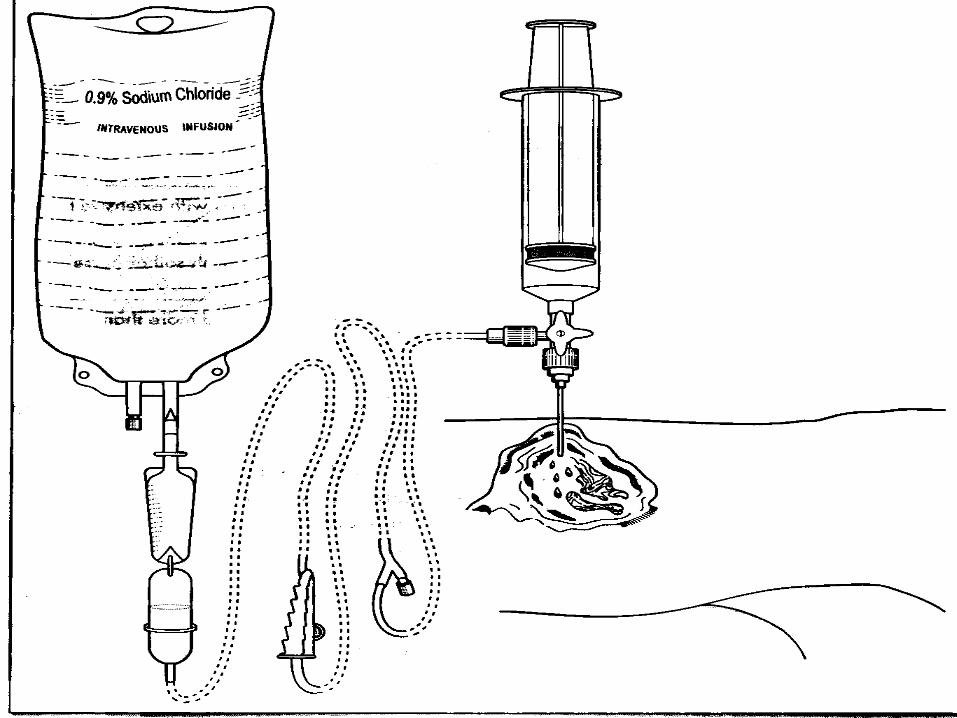
3- Pressure: lack of clinical studies recommend irrigation pressures in the range of 5
to 8 psi High-pressure irrigation is defined as more than 8
psi (use of a 30- to 60-mL syringe and a 18-20 gauge needle)
Animal studies: Rodeheaver, 1975 & Stevenson, 1976, high-pressure irrigation reduce both bacterial wound counts and wound infection rates
4- Solution: Ideal solution must be: Not toxic to tissues Does not increase rate of infection Does not delay healing Does not reduce tensile strength of wound healing Inexpensive
Dire DJ: A comparison of wound irrigation solutions used in the emergency department. Ann Emerg Med 1990.
531 patients were randomized into 3 groups, and irrigated with:
NS, 1% PI, or pluronic F-68No difference in wound infection rate NS has the lowest cost
Lineaweaver: Cellular and bacterial toxicities of topical antimicrobials. Plast Reconstr Surg, 1985.
1% povidone-iodine 3% hydrogen peroxide 0.25% acetic acid 0.5% sodium hypochlorite assayed in vitro using cultures of human fibroblasts
and Staphylococcus aureus All agents tested killed 100 percent of exposed
fibroblasts
Then he looked at different dilutions… …povidone-iodine 0.01, 0.001, 0.0001% …sodium hypochlorite 0.05, 0.005, 0.0005% …hydrogen peroxide 3.0, 0.3, 0.03, 0.003% …acetic acid 0.25, 0.025, 0.0025% ONLY antiseptic not harmful to fibroblasts yet
still bacteriostatic was Povidone iodine 0.001%
Moscati: Comparison of normal saline with tap water for wound irrigation. Am J Emerg Med 1998.
lacerations were made on each animal and inoculated with standardized concentrations of Staph. aureus
irrigation with 250 cc of either NS from a sterile syringe or water from a tap
no difference in bacterial count in 2 groups
Lammers:Bacterial counts in experimental, contaminated crush wounds irrigated with various concentrations of cefazolin and penicillin. Richard Lammers, American Journal of Emergency Medicine, January 2001.
An animal bite wound model was created inoculated with 0.4 mL of a standard bacterial solution each wound was scrubbed for 30 seconds with 20%
poloxamer 188 and then irrigated with 100 mL of one of 4 solutions: NS(control); cefazolin + penicillin G (LD); CZ + PCN (ID); and CZ + PCN (HD)
No differences in the bacterial counts or infection rates
Kaczmarek, 1982: Cultured open bottles of saline irrigating solution
36/169 1000cc bottles were contaminated 16/105 500cc bottles were contaminated
Brown, 1985: Approximately one in five of the opened bottles use for irrigation were contaminated
4- Volume:
Irrigation volume not studied use 50 mL to 100 mL of irrigant per cm of
laceration
5- Side effects:
Increase tissue inflammation (very high pressure irrigation), but benefit outweigh risk
Splatter (use your hand or plastic shield)
5- Soaking: Lammers: Effect of povidone-iodine and saline soaking
on bacterial counts in acute, traumatic contaminated wounds. Ann Emerg Med, 1990.
Contaminated traumatic wounds within 12 hours of injury 33 wounds randomized into: soaking in either 1% PI, NS, or covered with dry gauze
(control) for 10 min. Bacterial counts not changed in PI + control groups, but
increased in NS group Infection rate: PI=12.5% (1/8), control= 12.5% (1/8),
NS=71% (5/7)
Foreign Bodies:
Glass, metal, and gravel are Radiopaque Wooden objects and some aluminum products are
radiolucent Glass is accurately visualized on 2-view
radiographs if it is 2 mm or larger and gravel if it is 1 mm or larger
Wound Closure: Time Delayed primary closure Options Suturing method
Time:
The Golden Period: the time interval from injury to laceration closure and the risk of subsequent infection, (is highly variable)
Morgan WJ: The delayed treatment of wounds of the hand and forearm under antibiotic cover. Br J Surg 1980.
300 hand and forearm lacerations closed < 4hr had infection rate 7% closed > 4hr had infection rate 21%
Berk WA: Evaluation of the "golden period" for wound repair: 204 Cases from a third world emergency department. Ann Emerg Med 1988.
evaluation in a third-world country - 204 patients <19 hours to repair 92% satisfactory healing >19 hours to repair 77% satisfactory healing Exception: head and face lacerations had 95.5%
satisfactory healing, regardless of time
Baker: The management and outcome of lacerations in urban children. Ann Emerg Med 1990.
2,834 pediatric patients No difference in infection rate for lacerations
closed less than or more than 6hrs
Delayed primary wound closure: High risk wounds that are contaminated or contain
devitalized tissue Wound is initially cleansed and debrided Covered with gauze and left undisturbed for 4 to 5
days If the wound is uninfected at the end of the
waiting period, it is closed with sutures or skin tapes
Dimick, 1988: Delayed Primary Closure
Wound left open for 4 or 5 days until edema subsides, no sign of infection, and all debris and exudates removed
>90% success rate in closure without infection Final scar as same as primary closure
Options:
Nonabsobable suture Absorbable suture Tissue adhesive Adhesive tapes Staples

Nonabsobable suture:
Material Knot Security
Wound Tensile Strength
Tissue Reactivity
Workability
Nylon (Ethilon)
Good Good Minimal Good
Polypropylene (Prolene)
Least Best Least Fair
Silk Best Least Most Best
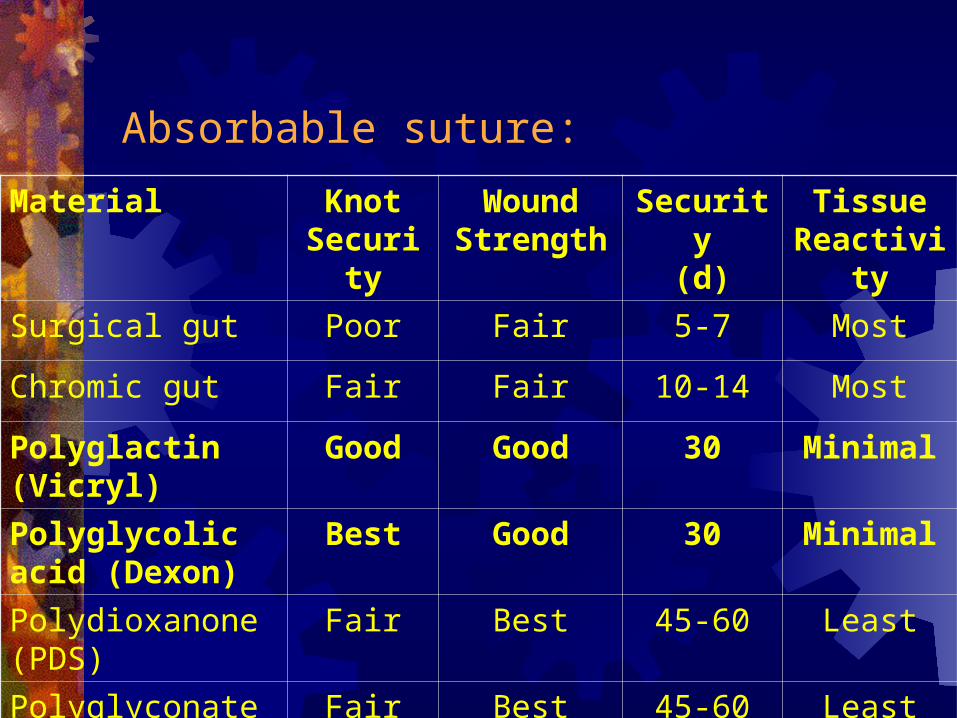
Absorbable suture:
Material Knot Security
Wound Strength
Security(d)
Tissue Reactivity
Surgical gut Poor Fair 5-7 Most
Chromic gut Fair Fair 10-14 Most
Polyglactin (Vicryl) Good Good 30 Minimal
Polyglycolic acid (Dexon)
Best Good 30 Minimal
Polydioxanone (PDS)
Fair Best 45-60 Least
Polyglyconate (Maxon)
Fair Best 45-60 Least
Tissue adhesive: N-butyl-2-cyanoacrylate, Histoacryl blue (HAB),
GluStitch First described in 1949 and first used medically in
1959 Antibacterial effect Cost $5 per single-use ampule Reduction in cost (Canadian $) per patient of
switching from nondissolving sutures $49.60
S. Mizrahi: Use of Tissue Adhesives in the Repair of Lacerations in Children. Journal of Pediatric Surgery,April, 1988.
1500 pediatric patients with simple laceration in ED, closed with HAB
Infection 1.8% Dehiscence 0.6%
Tissue adhesive:
Octylcyanoacrylate (OCA), or Dermabond Approved by FDA in 1998 Antibacterial effect Cost $25 per single-use ampule Greater strength than HAB
Which laceration?
Short (< 6-8 cm) Low tension (< 0.5 cm gap) Clean edged Straight to curvilinear wounds that do not cross
joints or creases
Contraindications: Jagged or stellate lacerations Bites, punctures or crush wounds Contaminated wounds Mucosal surfaces Axillae and perineum (high-moisture areas) Hands, feet and joints (unless kept dry and
immobilized)
Advantages of Adhesive vs Sutures: Faster repair time Less painful Eliminate the risk for needle sticks Antibacterial effect Does not require removal of sutures
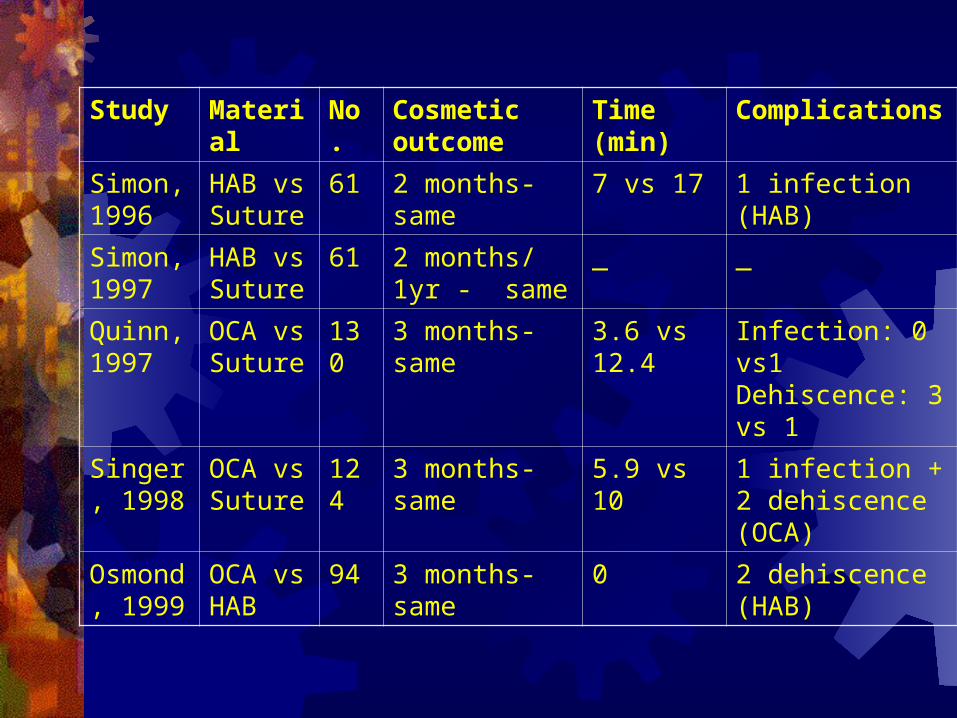
Study Material No. Cosmetic outcome
Time (min)
Complications
Simon, 1996
HAB vs Suture
61 2 months- same 7 vs 17 1 infection (HAB)
Simon, 1997
HAB vs Suture
61 2 months/ 1yr - same
_ _
Quinn, 1997
OCA vs Suture
130 3 months- same 3.6 vs 12.4 Infection: 0 vs1 Dehiscence: 3 vs 1
Singer, 1998
OCA vs Suture
124 3 months- same 5.9 vs 10 1 infection + 2 dehiscence (OCA)
Osmond, 1999
OCA vs HAB
94 3 months- same 0 2 dehiscence (HAB)
Adhesive tapes:
Seldom recommended for wound closure in the ED
Require the use of adhesive adjuncts (eg, tincture of benzoin)
May be used with tissue adhesive or after suture removal to decrease tension
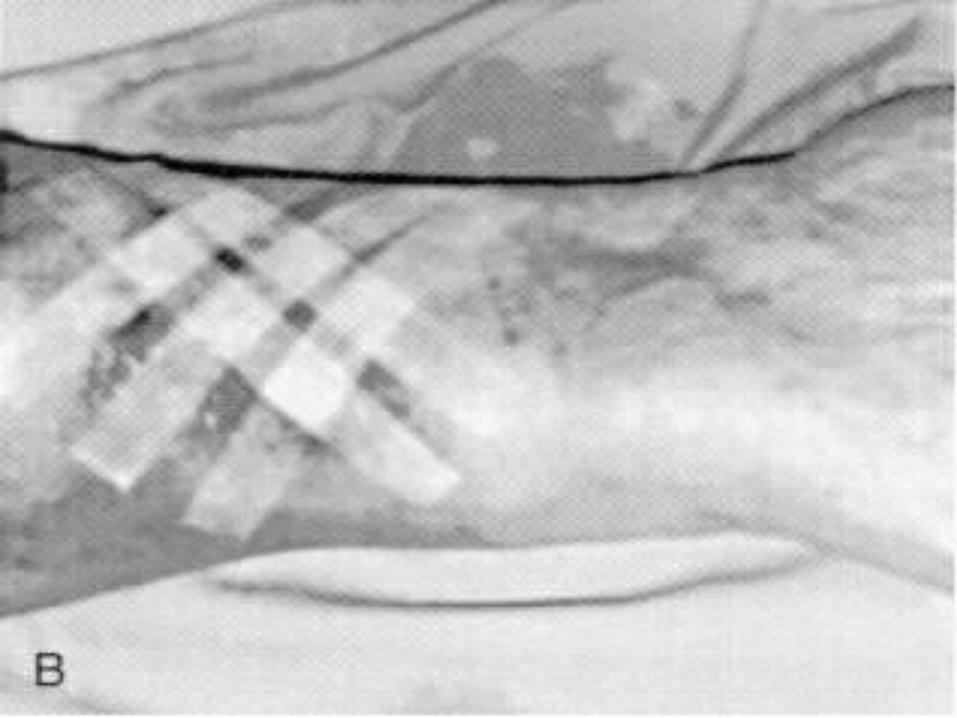
Staples: Consider staples for linear lacerations not involving the face or
other cosmetically sensitive areas Frequently used for scalp, trunk, or extrimities lacerations. Optimally, two operators perform this procedure
Brickman KR: Evaluation of skin stapling for wound closure in the emergency department. Ann Emerg Med 1989;18:1122-1125.
87 ER patients with 87 lacerations (2/3 scalp, trunk, and extremities)
65% closed in 30 seconds using staples No infections
John T. Kanegaye: 88 child with scalp lacerations, nonabsorbable
suture vs staples Shorter overall times for wound care and closure:
395 vs 752 sec Total cost based on equipment and physician time:
$23.55 vs $38.51 F/U rate 91%, with no cosmetic or infectious
complications in either group
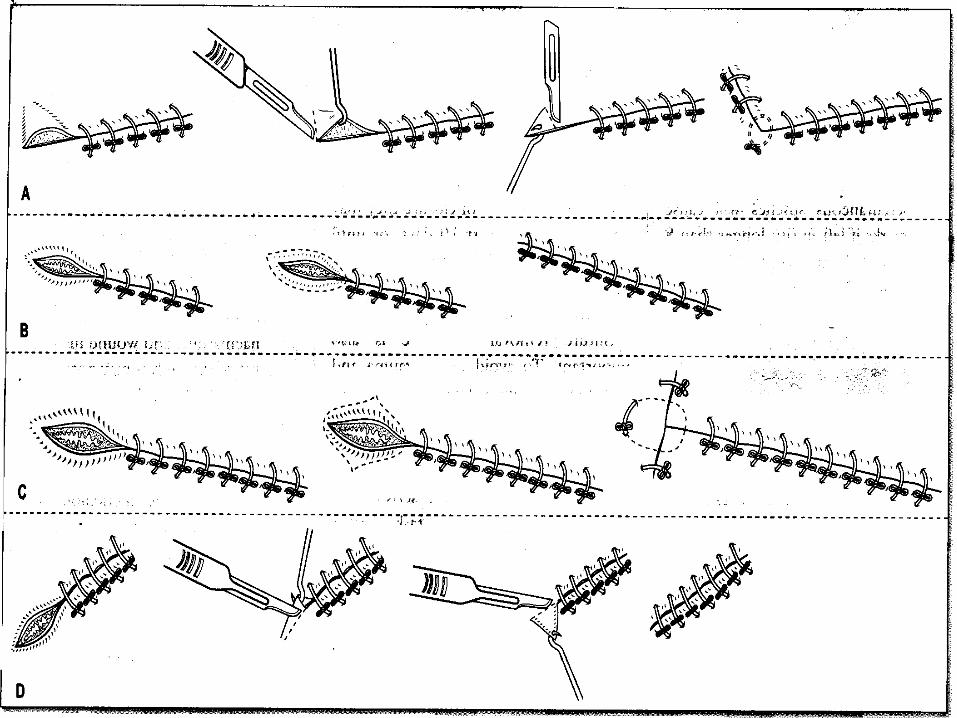
Suturing methods:
Simple interrupted Simple running Horizontal mattress Vertical mattress Running subcuticular (intradermal)
Simple Interrupted:
Most common Easy to master Can adjust tension with each suture Stellate, multiple components, or directions
wound
Simple Running:
Minimize time of suture repair Even distribution of tension Low-tension, simple linear wounds Removed within 7 days to avoid suture marks Optimal suture material is nonabsorbable
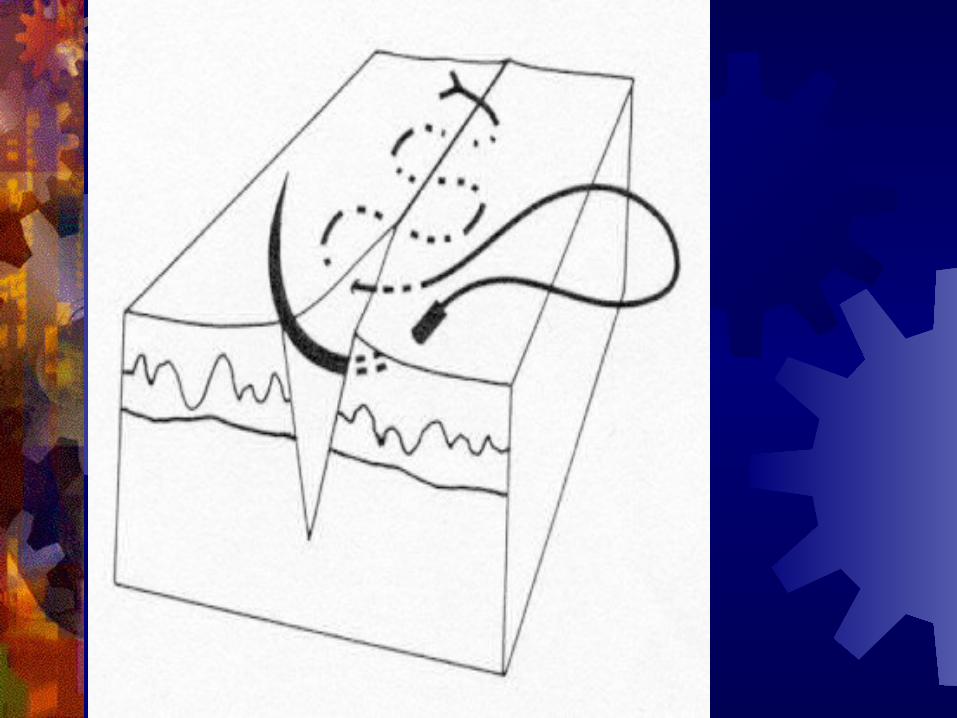
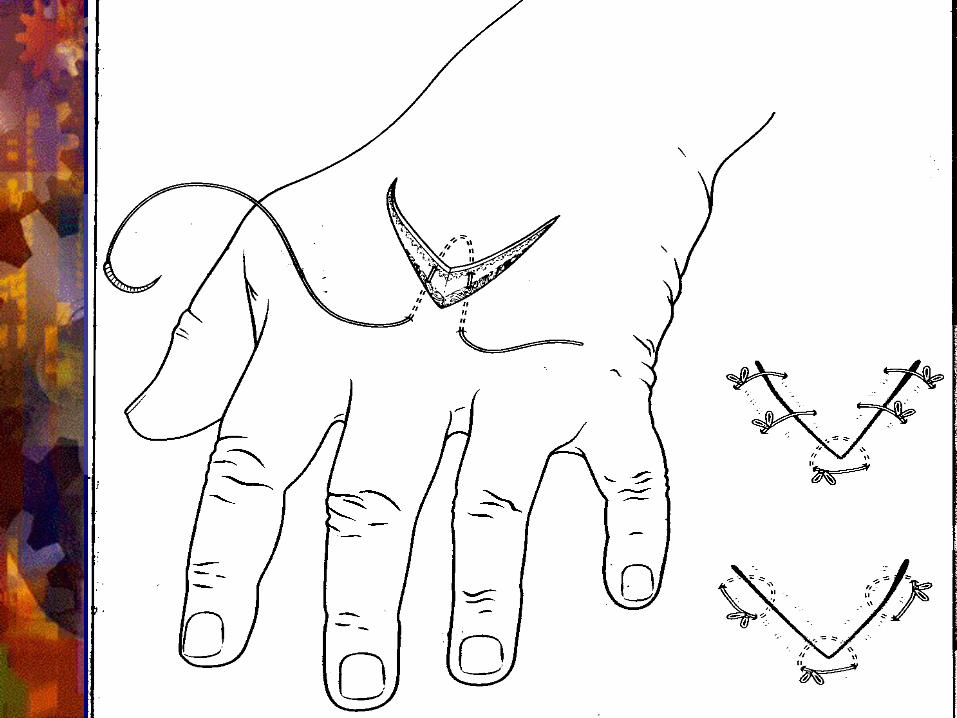
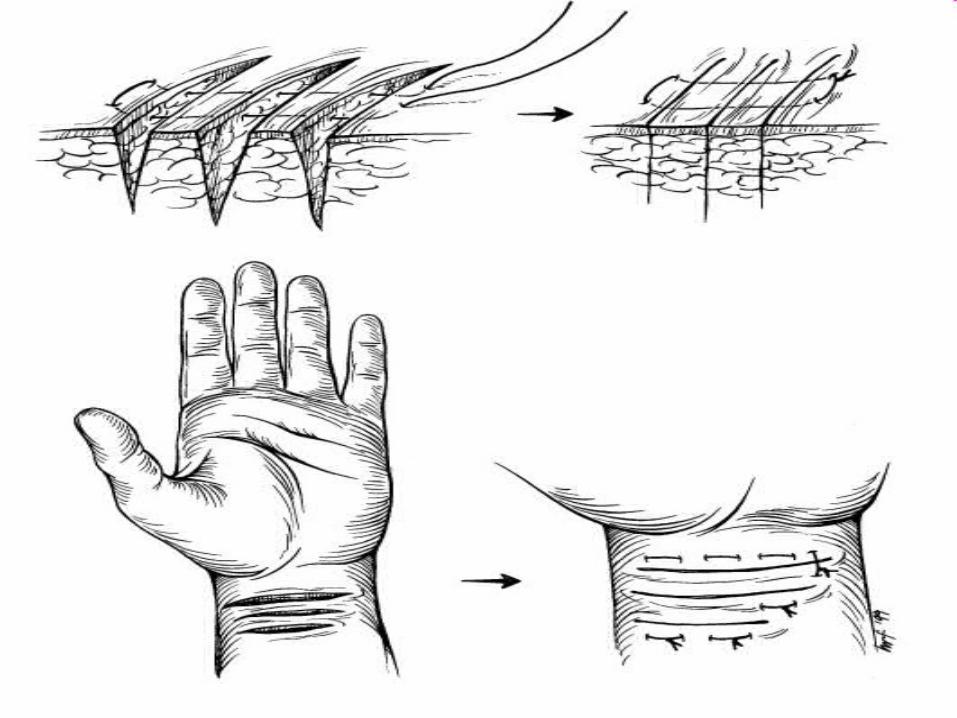
Horizontal Mattress:
Cause wound edges eversion Single layer closure with significant tension Decrease repair time, less knots required Need delayed suture removal, so risk of suture
marks
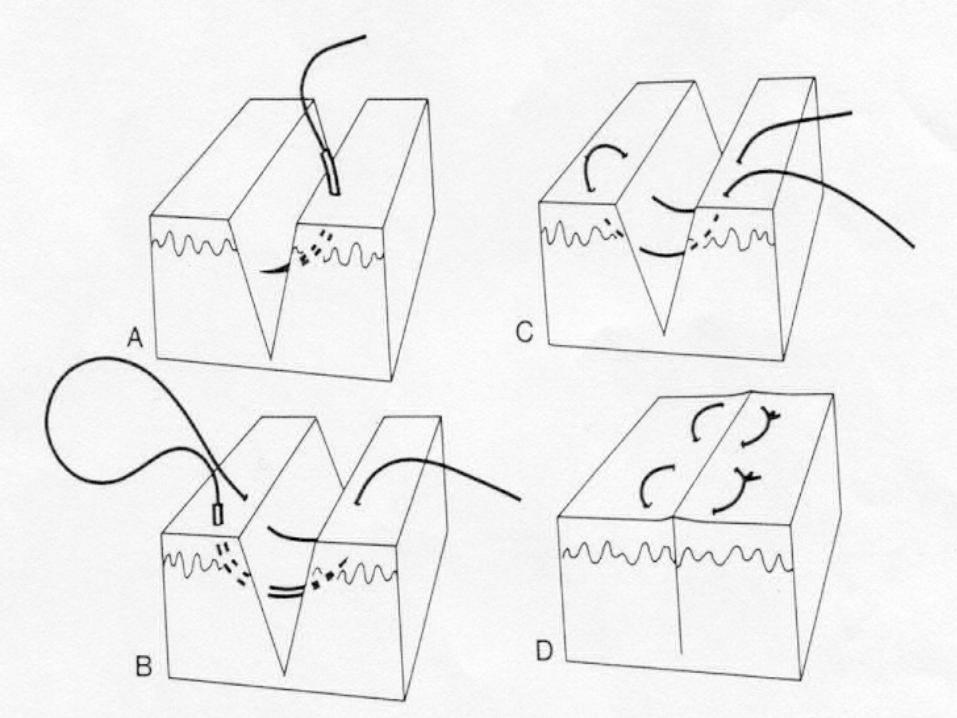
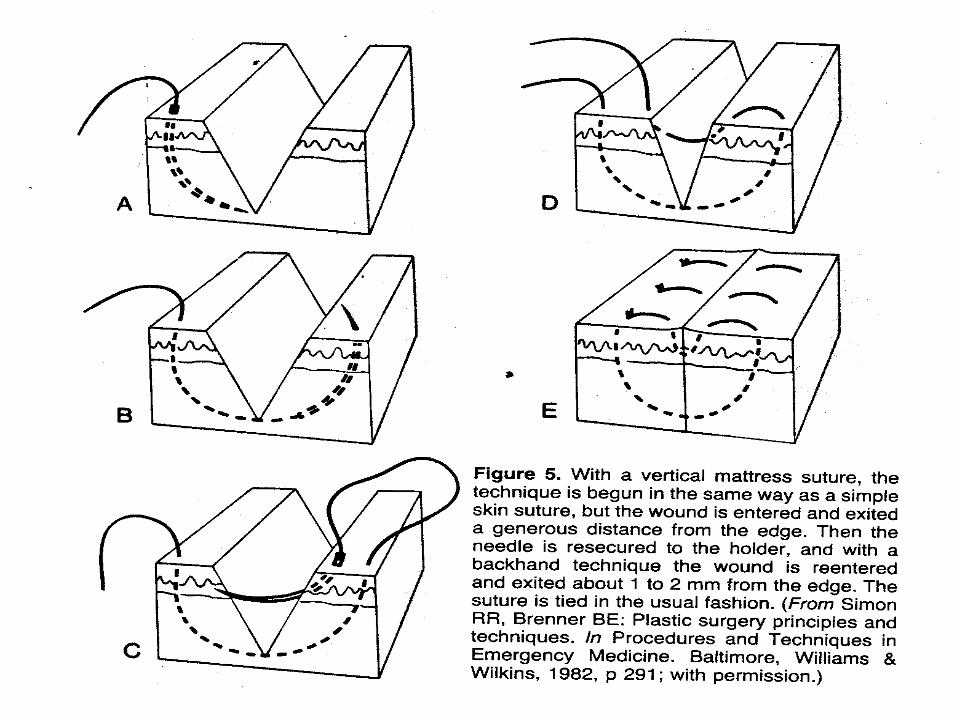
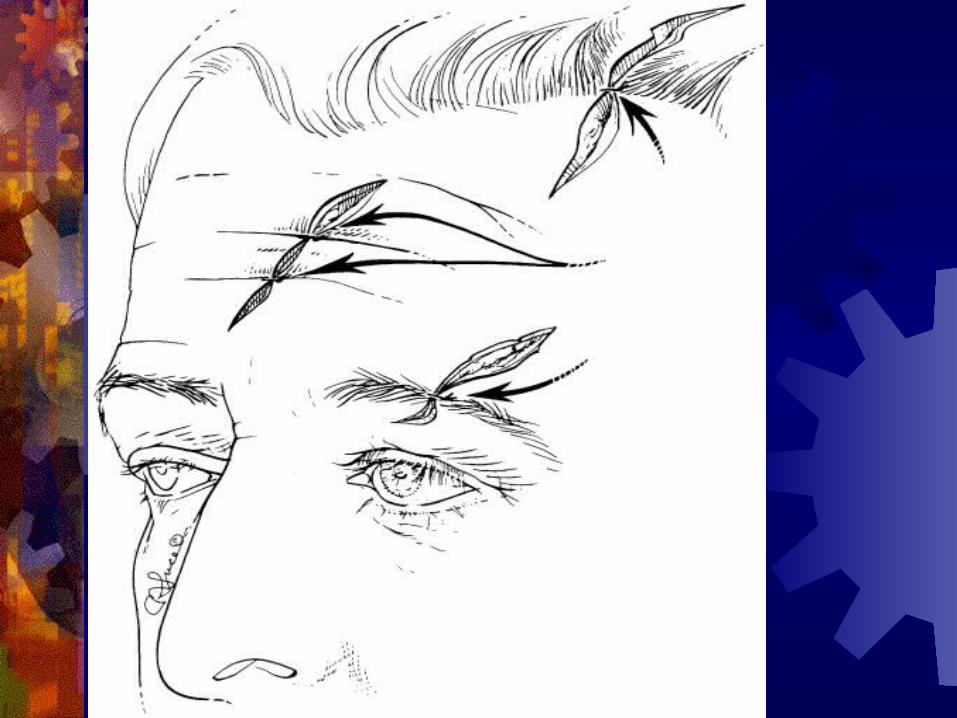
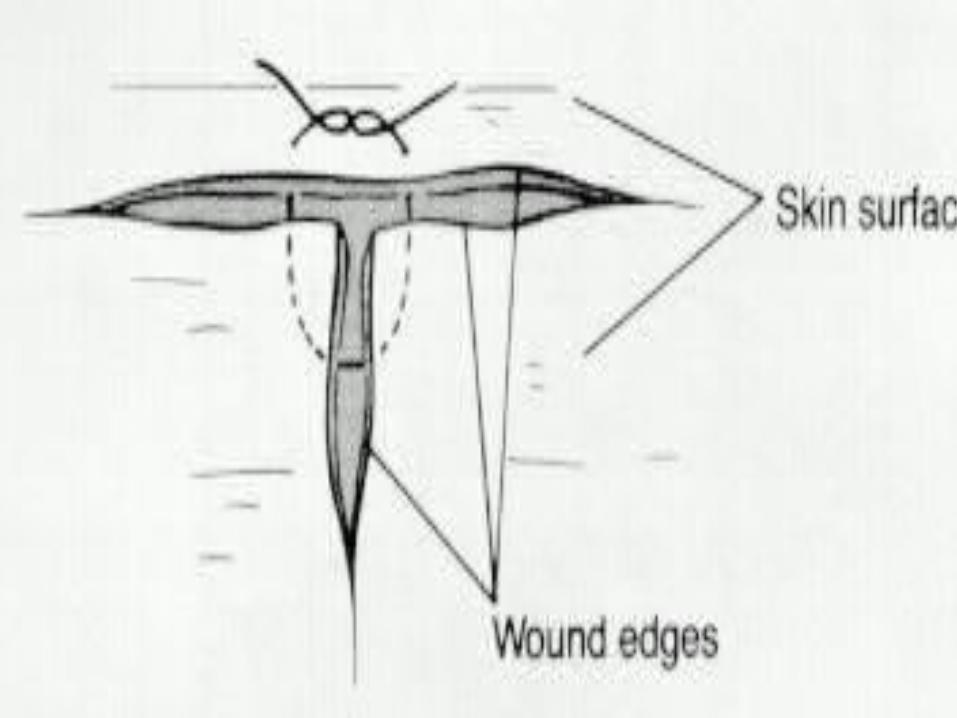
Vertical Mattress:
High-tension wounds Prone to skin suture marks if left in too long
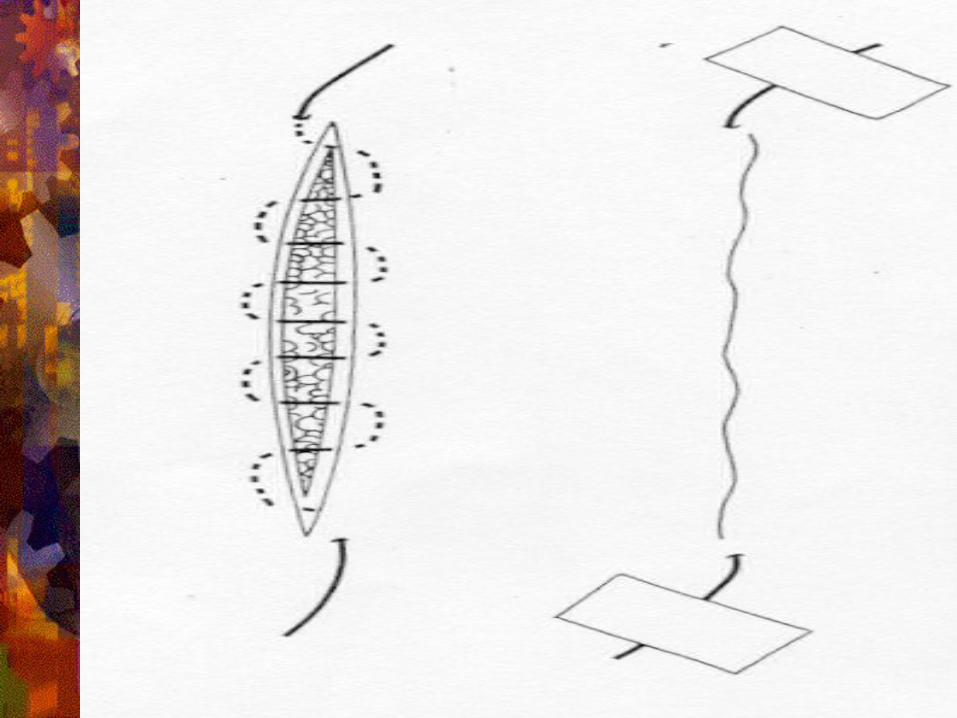
Running Subcuticular (Intradermal):
Best for areas where cosmetic result is of utmost importance
Time-consuming Difficult to master Low tension wounds Absorbable suture
McLean, 1980: 51 patients with continuous, running 54 patients with interrupted stitch Two infections in each group
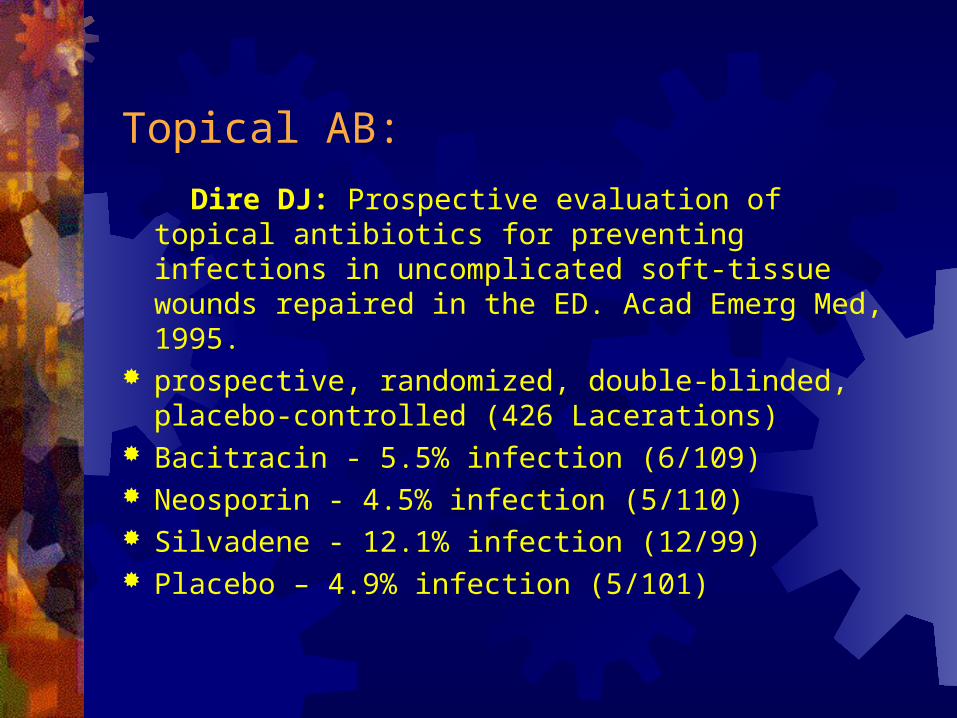
Topical AB: Dire DJ: Prospective evaluation of topical antibiotics for
preventing infections in uncomplicated soft-tissue wounds repaired in the ED. Acad Emerg Med, 1995.
prospective, randomized, double-blinded, placebo-controlled (426 Lacerations)
Bacitracin - 5.5% infection (6/109) Neosporin - 4.5% infection (5/110) Silvadene - 12.1% infection (12/99) Placebo – 4.9% infection (5/101)
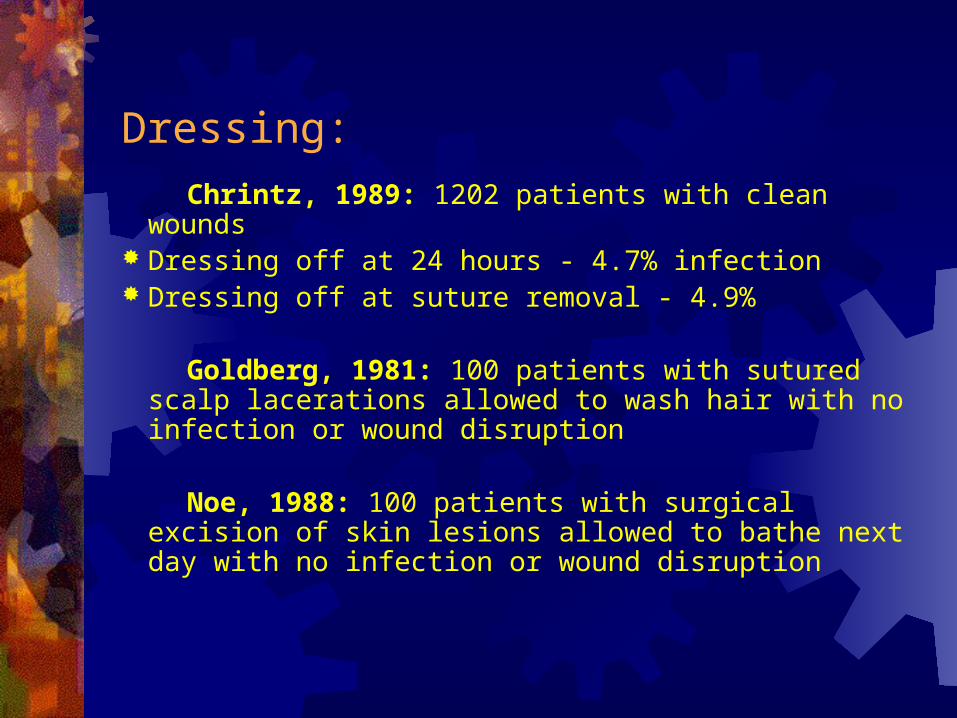
Dressing: Chrintz, 1989: 1202 patients with clean wounds Dressing off at 24 hours - 4.7% infection Dressing off at suture removal - 4.9%
Goldberg, 1981: 100 patients with sutured scalp lacerations allowed to wash hair with no infection or wound disruption
Noe, 1988: 100 patients with surgical excision of skin
lesions allowed to bathe next day with no infection or wound disruption
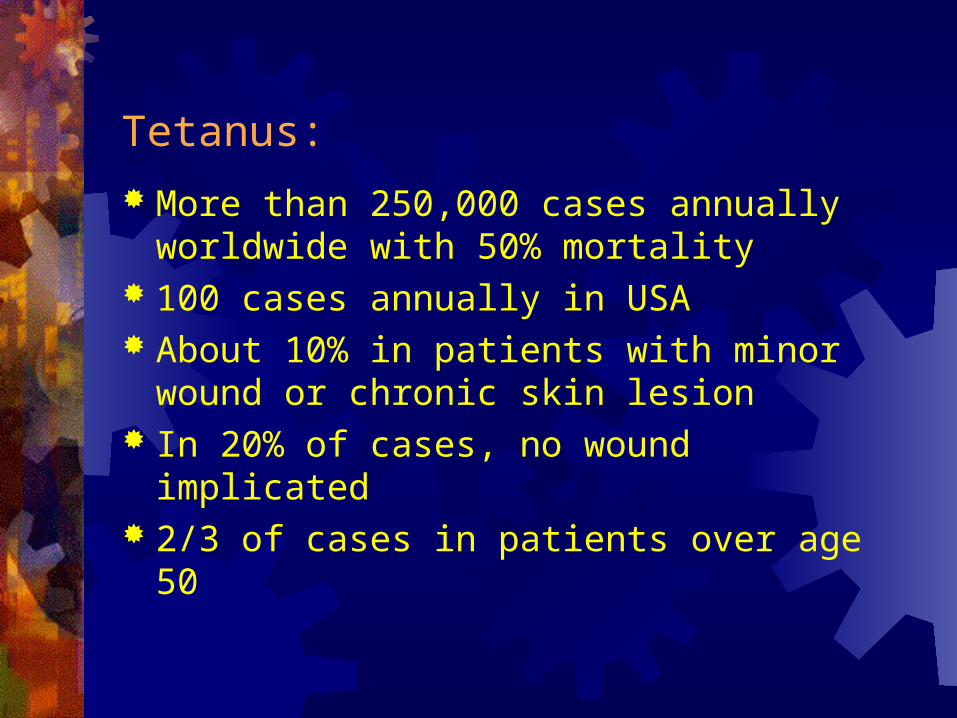
Tetanus:
More than 250,000 cases annually worldwide with 50% mortality
100 cases annually in USA About 10% in patients with minor wound or
chronic skin lesion In 20% of cases, no wound implicated 2/3 of cases in patients over age 50
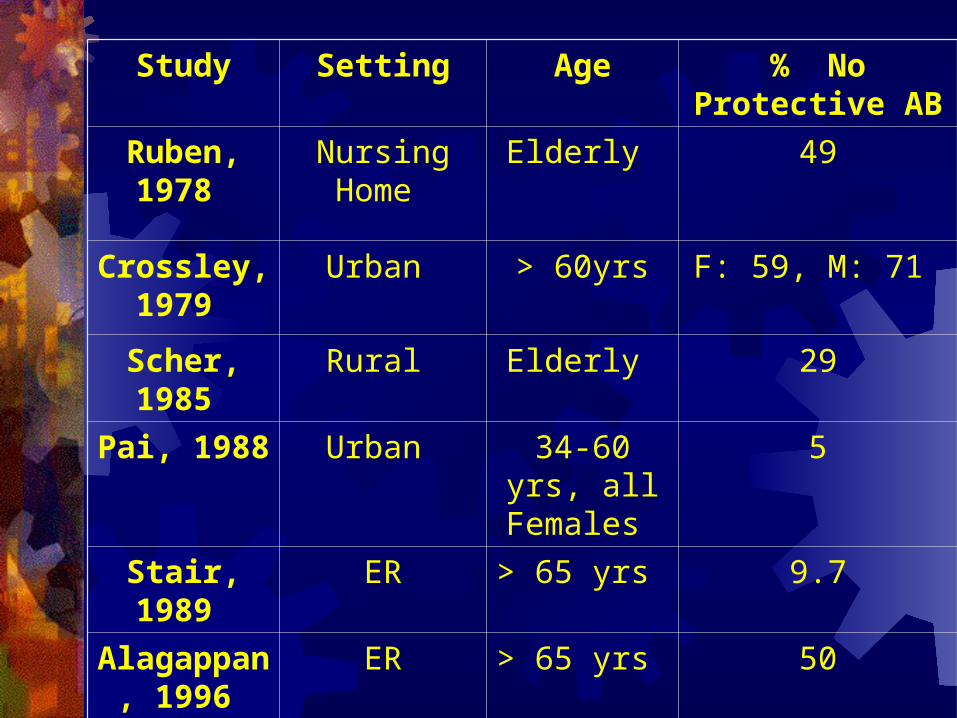
Study Setting Age % No Protective AB
Ruben, 1978 Nursing Home
Elderly 49
Crossley, 1979
Urban > 60yrs F: 59, M: 71
Scher, 1985 Rural Elderly 29
Pai, 1988 Urban 34-60 yrs, all Females
5
Stair, 1989 ER > 65 yrs 9.7
Alagappan, 1996
ER > 65 yrs 50
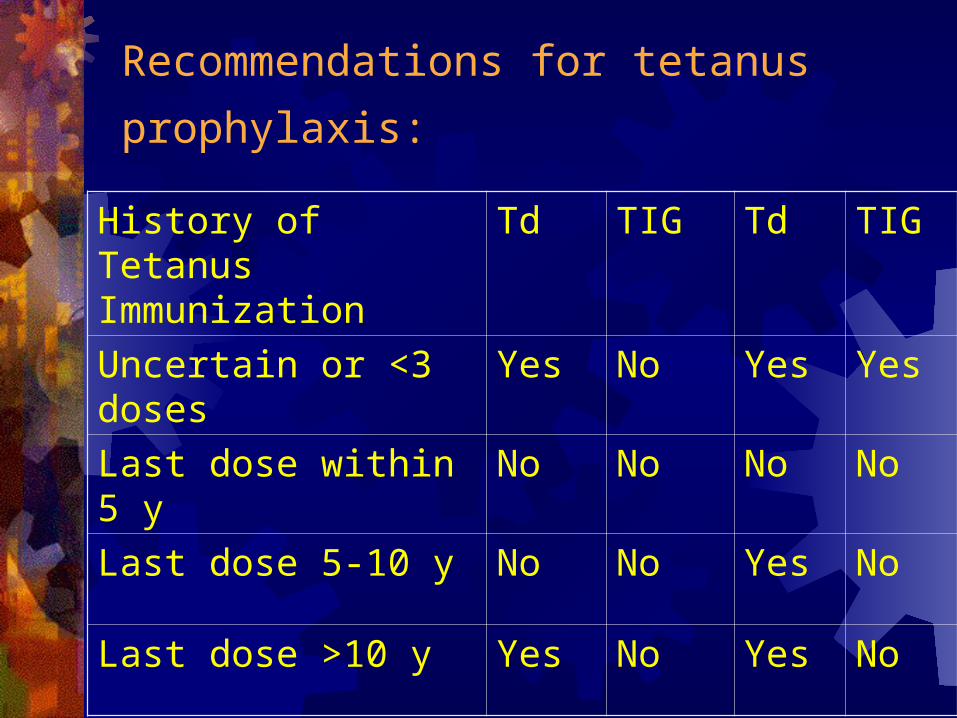
Recommendations for tetanus prophylaxis:
History of Tetanus Immunization
Td TIG Td TIG
Uncertain or <3 doses Yes No Yes Yes
Last dose within 5 y No No No No
Last dose 5-10 y No No Yes No
Last dose >10 y Yes No Yes No
3 doses
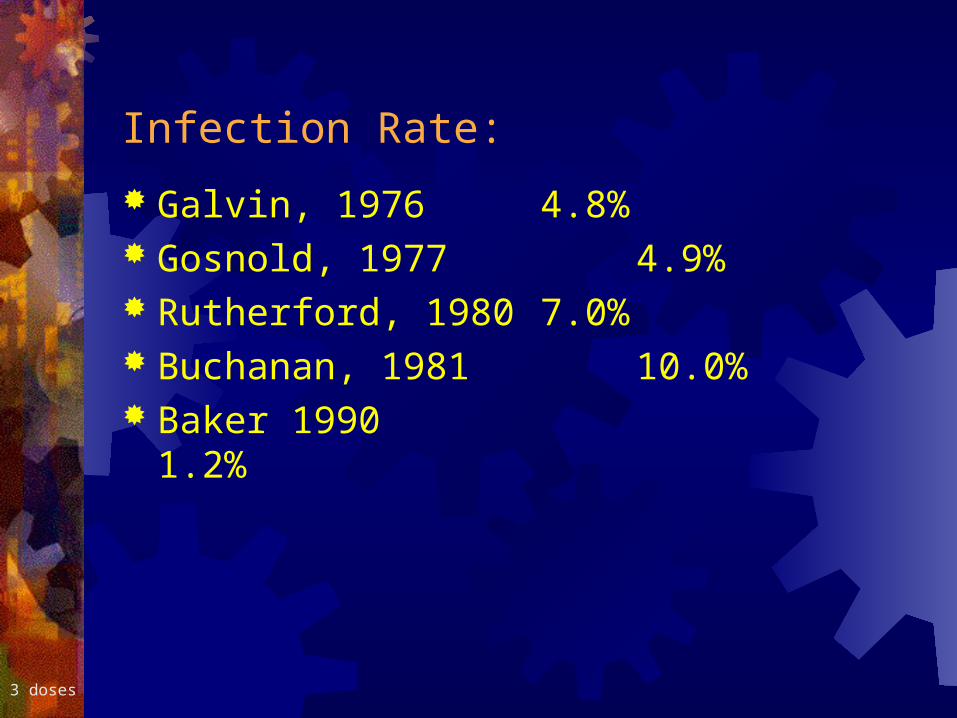
Infection Rate: Galvin, 1976 4.8% Gosnold, 1977 4.9% Rutherford, 1980 7.0% Buchanan, 1981 10.0% Baker 1990 1.2%
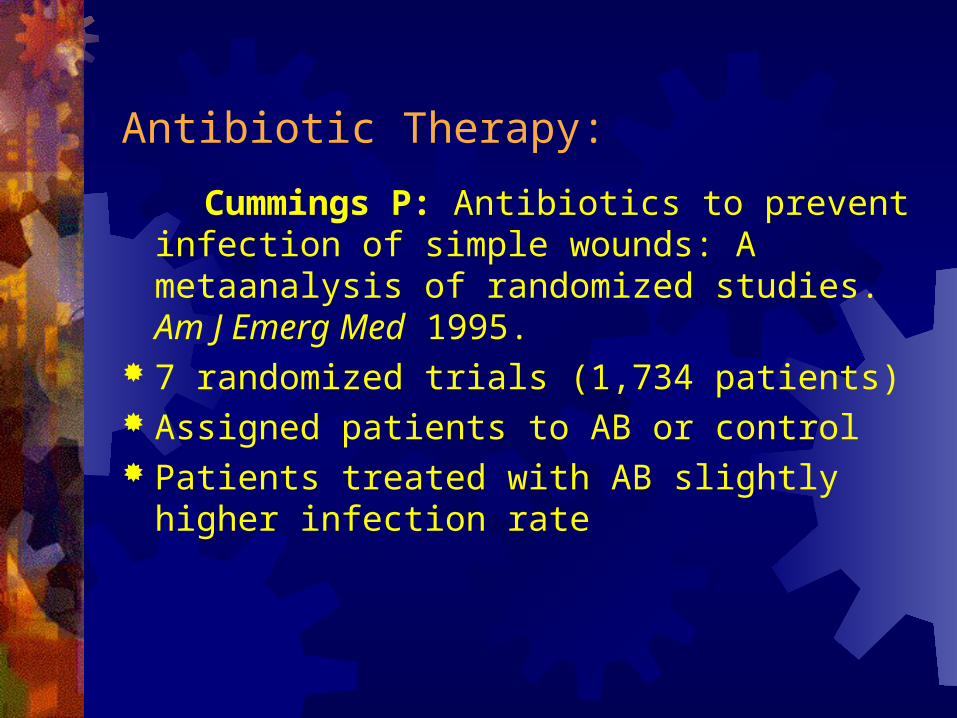
Antibiotic Therapy: Cummings P: Antibiotics to prevent infection of
simple wounds: A metaanalysis of randomized studies. Am J Emerg Med 1995.
7 randomized trials (1,734 patients) Assigned patients to AB or control Patients treated with AB slightly higher infection
rate
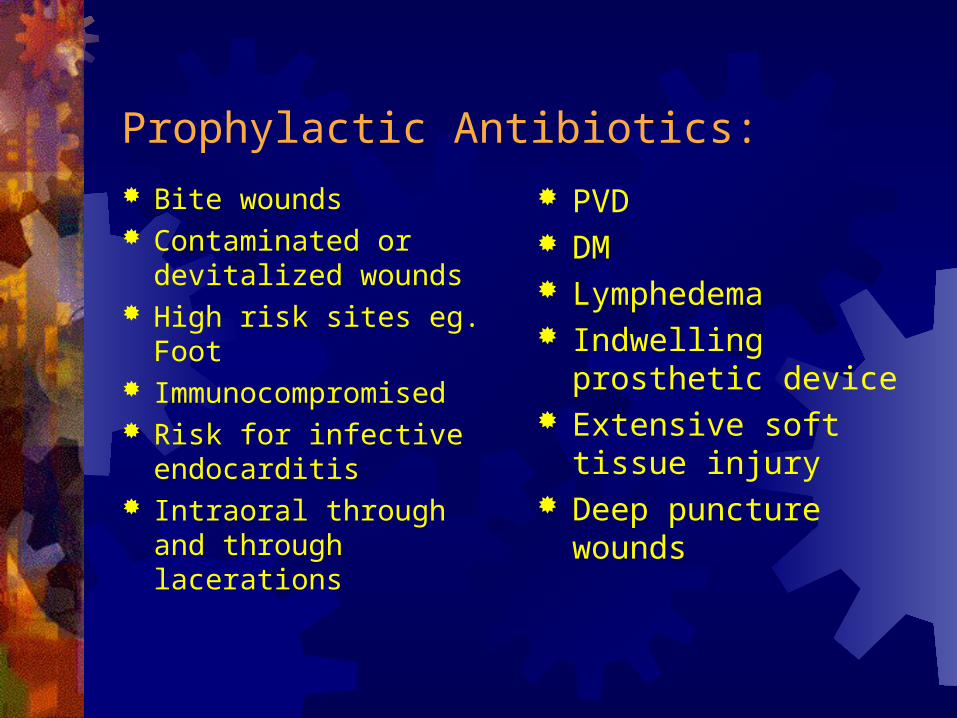
Prophylactic Antibiotics: Bite wounds Contaminated or
devitalized wounds High risk sites eg. Foot Immunocompromised Risk for infective
endocarditis Intraoral through and
through lacerations
PVD DM Lymphedema Indwelling prosthetic
device Extensive soft tissue
injury Deep puncture wounds
Prophylactic Antibiotics:
Amoxicillin, Clavulin Keflex Erythromycin recommended course is 3 to 5 days

Level of Training and Rate of Infection:
Adam: Level of Training, Wound Care Practices, and Infection Rates, American J Emerg. Med, May 1995.
Wounds were evaluated in 1,163 patients Medical students 0/60 (0%); All resident 17/547 (3.1%) Physician assistants 11/305 (3.6%) Attending physicians 14/251 (5.6%)
Level of Training and Cosmetic outcome:
Adam: Association of Training level and Short-term Cosmetic Apperance of Repaired Lacerations, Academic Emerg. Med, April 1996.
Retrospective study, 552 patients % achieving optimal cosmetic score Medical student 50% R1 54% R2 66% R3 68% Physician assistance 70% Attending physician 66%
Points to Take Home:
Laceration mismanagement & failure to Dx. FB is 2nd most common malpractice
Be aware of different methods to reduce pain from Lidocaine infiltration
In contaminated wounds with devitalized tissues debride and irrigate
You have a wide options for wound closure Always check tetanus status AB only for high risk wounds