Embed Size (px)
Citation preview
AD-A221 395
INSTITUTE REPORT NO. 447 OTIC
Wound Ballistics Research of the PastTwenty Years: A Giant Step Backwards
Martin L. Facihier
D~Sh~ T~M
7ie- ONlfl~rd~e
Division of Military Trauma -R arch
Januaary 1990
LETTERMAK ARMY INSTITUTE OF RESEARCH PRESID40 OF SAN FRANCISCO CALIFORNIA 94129
o5A 0508 lap
iI
Woun Ballistics Reseaicht of the Past Twenty Years: A Giant Step Backwards(MilitAry Triaima Report 447.) -- ML Fackler
Reproiluction of this documeitt in whole or in part is prohibited except with the permissionof the Commander, Letterman Army Institute of Research, Presidio of San Francisco,California 94129-6800. However, the Defense Technical Information Center is authorized toreproduce the document for United States Government purposes.
Deatrvy this report when it is no longer needed. Do- not rvturn to the originator
Cittw of, trade names in this report does not constitate an official endorsement or approvalof the thze of such items.
This material has been revit.wed by Leterman Army Institute of Research and thereis no objection to its presentation and/or publication. The opinions or assertionscontained herein are the private views of the author(s) and are not to be construed asofficial or as reflecting the views of the Department of the Army or the Departmentof Defense. (AR 360-5)
Commanding
This document has 'been approved for public release and- %ale; its, distribution is unlimited.
TTMT"T, C, ,, T -- T-T)SECURITY CLASSIFICATION OF THIS PAGE -
OUM ATO PForm Approved
REPORT DOCUMENTATION PAGE OMSNO. 0704-0 Ise
Ia. REPORT SECURITY CLASSIFICATION Ilb. RESTRICTIVE MARK:NGS
UNCLASSIFIED I2a. SECURITY CLASSIFICATION AUTHORITY 3. OISTRIBUTiON IAVAILABILITY OF REPORT
This document has been approved for2b. DECLASSiFICATIONIDOWNGRAoIr. SCHEDULE public release and sale. Unlimited
4. PERFORMING ORGANIZATION REPORT NUMBER(S) j5.MONITOP!N G ORGANIZATION REPORT NUMBER(S)
Institute Report No. 447
6a. NAME OF PERFORMING ORGANIZATION 6b. OFFiCe SYMBOL I 7a. NAME OF MONITORING ORGANIZATIONLetterman Army Institute (If applicable) I U.S. Army Medical Research and Deve:of Research I SGRD-ULT-M " ment 'Commahd
6c. ADDRESS (City, State, and ZIP Code) 7b. ADDRESS (Cir/, State. and ZIP Code)
Division of Military Trauma Research, Fort Detrick, Frederick, MD 21701LAIRPSF. CA 94129-6800 :
3a. NAME OF FUNDING/SPONSORING I8b. OFF.CE SYMBOL 9. PROCUREMENT NSTRUMENT :DENTIF:CA7CN NUMBERORGANIZATIONj (If applicable)
ac. ADDRESS (City, State, and ZIP Coae) t0. SOURCE CF FUNDING NUMBERS
PROGRAM I ?.OJEcT I TASK IWCRK UNIT
ELEME NT NO. jS62771 NO. ACCzSS;ON N,
62"772-A 2A8741 10
11. TITLE (include Security Classificarion)
(UNCLASSIFIED) Wound Ballistics of the Past Twenty Years: A Giant Step Backwards.
12. PERSONAL AUTHOR(S)
'Packler, Martin L.' OF REPORT 13b. TIME COVERED 114. DATE OF REPORT (Year, Month, Day) lS. PAGE COUNT
TUTE I FROM 1,qRi,_TO _0a 1990, January, 16 15-MENTARY NOTATION
17. ._4TI CODES 18. SUBJECT7 TERMS (Continue on reverse if necessary and identify by block numcer)
FIELD GROUP SUB-GROUP Wond ballisticsI I
19. ABSTRACT (Continue on reverse if necesary and idirtify by block number)
Wound ballistics research is supposed to aid the surgeon inproviding optimal care for the wounded, but recent trends inballistics reserach have not provided the surgeon withobjectively determined information. Twenty years ago, woundsfrom penetrating projectiles were likely to be treated in arational and effective manner; today many surgeons are prone toremove excessive amounts of tissue when treating wounds caused bywhat they assume to be "high-velocity" projectiles.
(Continued on Reverse)
20. DISTRIBUTION/AVAILABIU'TY OF ABSTRACT -21. ABSTRACT SECURITY CLASSIFICATION
13 UNCLASSIFIEDIUNUMITED 0I SA~ME AS RPr. 03 OTIC USERS UNCLASSIFIED -
22a. NAME OF RESPONSIBLE INDIVIDUAL 22b. TELEPHONE (Include Area Code) j 22c. OFFICE SYMBOLDonald G. Corbv COL, MC J (415) 561-4982 j SGRD-ULZ
DO Form 1473, JUN 86 Previous editions are obsolete. SECURITY CLASSIFICATION OF 1HIS PAGE
UNCLASSIFIED
'19)The most common battlefield wound has a simple punctate entrance with tissuedisruption limited to a diameter no larger than the wounding projectile. Therifle wound of the extremitywhere the bullet has not yet yawed, and virtuallyall individual wounds from explosive device fragments fall into this category.
Historically, chis type of wound has healed well, despite little or no treat-ment -- even in preantibiotic days.
Since the Vietnam era, the bulk of wound ballistics "research" has beenpolitically motivated. This research has employed flawed methods to exaggeratewounding effects, seriously confusing current wound treatment doctrine. Thebattlefield surgeon determines treatment according to the amount, type andlocation'of disruption, rather than the supposed velocity of the projectile.
ABSTRACT
Wound ballistics research is supposed to aid the surgeon inproviding optimal care for the wounded, but recent trends inballistics research have not provided the surgeon withobjectively determined information. Twenty years ago, woundsfrom penetrating projectiles were likely to be treated in arational and effective manner; today many surgeons are prone toremove excessive amounts of tissue when treating wounds caused bywhat they assume to be "high-velocity" projectiles.
The most common battlefield wound has a simple punctate entrancewith tissue disruption limited to a diameter no larger than thewounding projectile. The rifle wound of the extremity, where thebullet has not yet yawed, and virtually all individual woundsfrom explosive device fragments fall into this category.
Historically, this type of wound has healed well, despite littleor no treatment -- even in preantibiotic days.
Since the Vietnam era, the bulk of wound ballistics "research"has been politically motivated., Tis research has employedflawed methods to exaggerate wounding X cts, seriouslyconfusing current wound treatment doctrine he battlefieldsurgeon determines treatment according to the amount, type, andlocation of tissue disruption, rather than the supposed velocityof the projectile. (1T7) --
ccesiot For\ ;i7OTIS CRA&I
11-DTIC TAB IUnannounced 0Justification
.istribution I
Availebity Codes
i Avail and I or01st I Special
i
WOUND BALLISTICS RESEARCH OF THE PAST TWENTY YEARS: A
GIANT STEP BACKWARDS
INTRODUCTION
The widespread misconception that "high-velocity"or "high-energy" projectiles invariably cause extensivedamage (1,2) has been addressed recently (3,4). In thepast, critical reviews questioning this concept havegone relatively unheeded (5,6). Interestingly, thosewho have questioned the "high-velocity/high-energy"concept of wounding (Lindsey, Hampton, Fackler) haveall had extensive combat surgery experience.
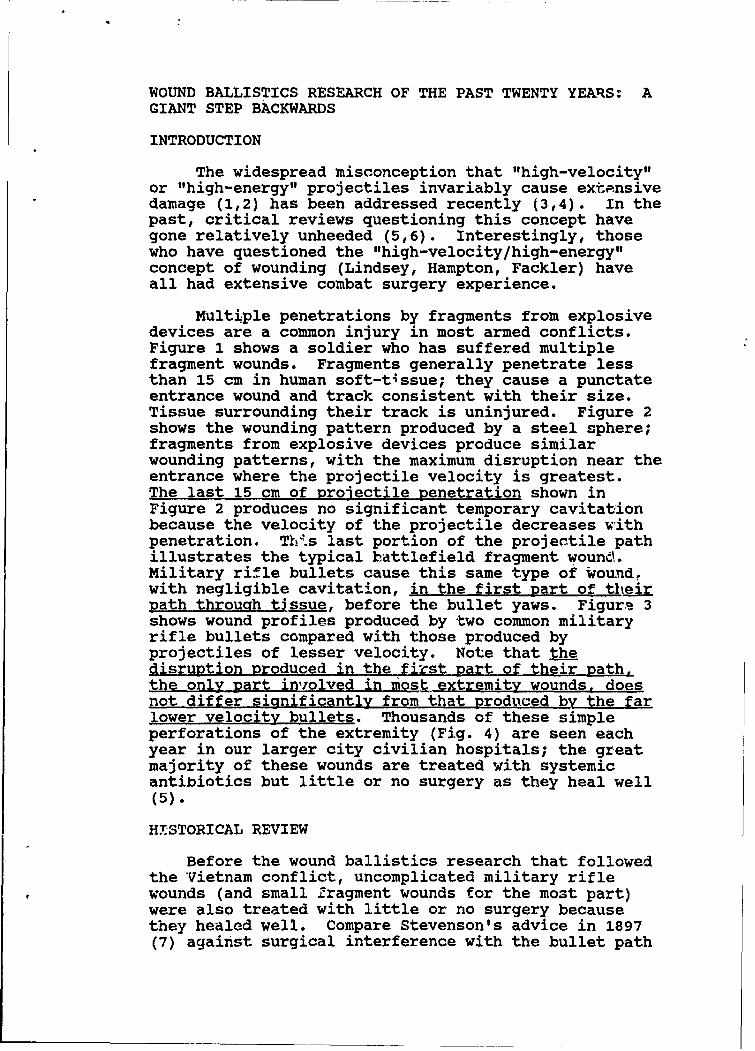
Multiple penetrations by fragments from explosivedevices are a common injury in most armed conflicts.Figure 1 shows a soldier who has suffered multiplefragment wounds. Fragments generally penetrate lessthan 15 cm in human soft-tissue; they cause a punctateentrance wound and track consistent with their size.Tissue surrounding their track is uninjured. Figure 2shows the wounding pattern produced by a steel sphere;fragments from explosive devices produce similarwounding patterns, with the maximum disruption near theentrance where the projectile velocity is greatest.The last 15 cm of projectile penetration shown inFigure 2 produces no significant temporary cavitationbecause the velocity of the projectile decreases vithpenetration. This last portion of the projectile pathillustrates the typical battlefield fragment wound.Military rifle bullets cause this same type of wound,with negligible cavitation, in the first part of theirpath through tissue, before the bullet yaws. Figurs 3shows wound profiles produced by two common militaryrifle bullets compared with those produced byprojectiles of lesser velocity. Note that thedisruption produced in the first part of their path.the only part involved in most extremity wounds, doesnot differ significantly from that produced by the farlower velocity bullets. Thousands of these simpleperforations of the extremity (Fig. 4) are seen eachyear in our larger city civilian hospitals; the greatmajority of these wounds are treated with systemicantibiotics but little or no surgery as they heal well(5).
HMSTORICAL REVIEW
Before the wound ballistics research that followedthe Vietnam conflict, uncomplicated military riflewounds (and small Zragment wounds for the most part)were also treated with little or no surgery becausethey healed well. Compare Stevenson's advice in 1897(7) against surgical interference with the bullet path
BALLISTICS RESEARCH -- FACKLER -- 2
in rifle wounds, with Theodor Kocher's observationsfrom World War I (8), that the minimal damage producedby the rifle bullet allowed the wounds ("...wieVerletzungen ohne hautwunde ausheilten.") to heal sowell that it appeared as if they had no skin wounds.
Jolly, in 1941 (9), noted,
Many high-velocity bullet wounds of softparts have small punctured wounds of entranceand exit. Often such wounds do not requireoperation; and if operation is performed,nothing more than excision of the orifices ofthe track to provide better drainage need beundertaken. Such wounds usually healspontaneously within ten days. The highvelocity bullet, unlike other projectiles,does not usually carry foreign matter intothe tissues and tends to leave an aseptictrack.
Bailey, in 1942 (10), advised that the "...setonwound is innocuous, it should be left alone." Fergusonet al. (11), Slesinger (12), Crile (13), and Cope (14)made similar observations, and Ogilvie (15), consultanturgeon to British forces in World War II, listed as
his first "sin" of war surgery tne unnecessaryoperations on through and through bullet wounds of thesoft parts. He wrote, "The majority of these with restand sulfonamide heal rapidly and leave no disability;operation means loss of time and loss of function."
King (16), reporting on war wounds from SouthVietnam, wrote that "Unconplicated perforating soft-tissue wounds were the most common bullet wounds of theextremities. They showed small entry and exit woundsand a clean soft-tissue track with little or nodevitalization of tissue. They usually healed if leftalone."
The author of this paper served in one of thebusiest hospitals in South Vietnam (US Naval SupportActivity Hospital, DaNang) during the most activeperiod of t%-,, Vitn74 -- P1 .. n.a 01+ -v -
I=L.L V .=%.AACAU %OOAA % " - -k-
December 1968). Immediately thereafte.r he served threeyears at the US Naval Hospital, Yokosuka, Japan, caringfor the combat casualties from South Vietnam who weretransported there by air soon after initial surgery.He was also a delegate at the last two Tri-Service WarSurgery Conferences (1970, 1971) (17). The author andhis colleagues determine the treatment of penetrating
BALLISTICS RESEARCH -- FACKLER -- 3
war wounds by assessing the amount, type, and locationof tissue disruption, evidenced by physical examinationand appropriate x-ray studies (17).
ORIGINS OF CURRENT MISCONCEPTIONS
If we had no trouble treating the gunshot woundsof the Vietnam War, why has this field regressed sobadly since then? 'n 1967, one small series of woundscaused by the then new M-16 assault rifle was reported(18,19). These wounds were described using suchemotionally charged terms such as "massivelydestructive" (18) and "devastating woundingpower... tremendous wounding and killing power" (19)rather than reporting wound dimensions and/or includingmeasuring scales on photographs to give the reader anobjective means of comparing these wounds with thosecaused by other weapons.
Remembering the political climate of that time, andthe fact that the Swedish government, as a part of itsanti-war stance, was actively encouraging desertion byAmerican soldiers and providing them refuge, it is notsurprising that Swedish interests saw an opportunity tobe exploited in these reports. They began a program todeclare the M-16 "inhumane" and to be outlawed byinternational convention. The "research" performed tosupport this program used methods of easilymisinterpreted to make wounding effects of by the M-16bullet appear worse than those of other small-armsprojectiles. For example, shoccing projectiles throughsmall (14 cm) blocks of tissue simulant or the legs of20 kg pigs in which the tissue path is even shorter,can provide results which are misleading. The photosin Berlin, et al. (20) show a 15 cm stellate exit woundcaused by a 5.56 mm bullet compared to an exit wound ofonly about 1 cm caused by a 7.62 mm bullet, therebymaking the smaller bullet appear to have a far greaterwounding capacity.
Military bullets begin their tissue path travelingpoint forward. They yaw (turn sideways in relation totheir line of flight) at a penetration depth under 10cm to over 20 cw, depending upon th " bullt. Even ingroups of shots using the same type of bullet,variations in the penetration depth at which the bulletyaws can easily vary 25% from the average (2.). Thismeans that in any group of shots with a given bulletthere are likely to be some that yaw within these smalltargets; these will show large exit wounds. There willbe others that have not yet yawed; these will show
BALLISTICS RESEARCH -- FACKLER -- 4
minimal wounds. Individuals with an interest in"proving" one bullet less "humane" than another needonly to photograph the appropriate exit wound. Thisvariation in yawing distance also explains apparentinconsistencies in bullet effects. Nordstrand, et al.(22), showed comparative microsecond x-ray picturescomparing the same type bullets (5.56 and 7.62) forwhich Berlir et al. (20) had indicated an apparentlyfar greater wounding effect for the 5.56 mm bullet. Inthe Nordstrand study (22), both bullets yawed and brokeapart at the same depth of penetration in a soap block.and the 7..62 mm bullet's disruptive effects were fargreater.
By using enough tissue/tissue simulant to catch theentire projectile path, the entire potential of theprojectile can be determined (23); nothing is hidden.Only presentation of the projectile's disruptionpattern along its entire tissue path allows meaningfulcomparison of wounding potential among variousprojectiles.
Apparently overzealous in his attempt to justifythe Swedish efforts, Berlin wrote, "During the 1960'sinjuries of much greater severity were reported due toa new generation of small firearms." (24). Those whowish to check will find that only two of the sevencitations Berlin gives to support that statement do, infact, support it; these two are by the same author(18). In fact, it appears that all the furor over theM-16, repeated and amplified in many papers, originatedfrom this one source (18).
OBJECTIVE OBSERVERS SAW NO MORE SEVERE WOUNDS FROM THEM-16 THAN FROM OTHER SMALL-ARMS
The five Tri-Service Vietnam war surgeryconferences did not identify any special problemsassociated with "high-velocity" projectile wounds. Thelast conference (17) listed "Topics suggested forfurther study," but no need to study penetratingprojectiles (wound ballistics) was mentioned.
Scott (25), in a superbly comprehensive study whichcombined an outstanding historical review, comparativeshots into tissue simulant and live animals at rangesup to 600 m, as well as case reports of 70 shootingswith the new 5.56 mm caliber, concluded, "Theexperimental observations which I have made underwidely varying circumstances do not indicate that lightweight rifle bullets inflict more severe wounds than
BALLISTICS RESEARCH -- FACKLER -- 5
those caused by rifles in use since the early part ofthis century. My experience in the field supports thisconclusion."
Albreht et al. (26) did an extensive study shootingvarious military rifle bullets through the tied-together thighs of 59-66 kg swine to study bulleteffects in a more realistic tissue thickness (25 cm)than was used in the Swedish studies. Their findingswere clear; the 7.62 NATO bullet caused more damagethan the 5.56 mm M-16 bullet.
Bellamy (27) recently reviewed the informationcollected on approximately 1400 gunshot woundcasualties by the Wound Data and MunitionsEffectiveness Team (WDMET) in Vietnam. Wounds causedby the M-16 rifle comprised about one fourth of thesecases and Bellamy states unequivocally that they dianot cause more severe wounding than other small armsused in this conflict.
SCOPE OF THE MISINFORMATION
Five International Wound Ballistics Symposia havebeen sponsored by the Swedish research group. Theproceedings of these symposia have been published, andmany readers assume that the information is validscientific literature, selected by peer review. It isnot. Papers submitted to these symposia are acceptedand published without critical review. The majoremphasis appears to be on attracting participation andinterest in the symposia; this has resulted in greatlyincreasing the vcltue of data with no regard for theaualitv of this data. Serious contradictions in thiswork have gone unaddressed, e.g., two papers by Swedishresearchers concluded that the amount of nonviabletissue around a projectile wound increases with time(28,29). Three papers from other countries (30-32)reported contradictory findings.
The degree of exaggeration is well illustrated byrecommendations given by Rybeck (33). He wrote that"...the clinical experience [is) that tissues whichhave been subjected to the formation of the temporarycavity after a high velocity missile will notsurvive.", and "...the temporary cavity, especiallyafter missiles travelling at high velocities, is verylarge (30 times the diameter of the projectile)...".Using Rybeck's conclusion to calculate extent of thetissue excision recommended for the wound shown inFigure 4, for example (5.56 mm M-16 bullet diameter,
BALLISTICS RESEARCH -- FACKLER -- 6
multiplied by 30), we find a diameter of 16.68 cm (over6 inches). Compare this with the experience of King,cited above (16), that this type of wound "...usuallyhealed if left alone." The reader can judge forhimself which treatment recommendation appears to bethe more reasonable.
Rather than striving for a rational synthesis,correcting and striving to replace flawed data withmore valid work, those in control of the symposia he,attempted to suppress contrary information. Forexample, the printed Proceedings of the 5th Symposium(they did not appear until 1988 although the symposiumwas held in 1985) omitted a panel discussion in whichdata very critical of Swedish research methods waspresented. Additionally, the printed Proceedingscontained none of the comments made from the floor onthe papers presented (many of these comments werecritical of methods, conclusions, etc.) (34).
CONCLUSION
Scientific work demands hard choices, separatingthe valid from the unsound, the significant from thetrivial, and the common from the rare. When this isnot done the flawed works pile up, greatly outnumberingthe valid; repetition compounds the problem and manyare misled. The sad legacy of the misguided studies ofthe past twenty years can be found in the faultyunderstanding of wounding mechanisms and irrationaltreatment recommendations in recent surgical textbooks(35-38). The detrimental effects are clear. Mostwounds seen on the battlefield are simple and have beentreated by simple means with good results for the pastone hundred years (5, 7-17). Since it has resulted inrecommendations for unnecessarily radical explorationsand excision of tissue for all "high-velocity"'projectile wounds, and assumptions that all battlefieldwounds fall into this category, the overall effect ofthe past twenty years of wound ballistics research canonly be considered a giant step backwards. It is hopedthat this documentation of the problem will stimulatecorrective measures.
BALLISTICS RESEARCH -- FACKLER -- 7
REFERENCES
1. C7:en-Smith MS. Wounds caused by the weapo.- ofwar. In: Westaby S, ed. Wound Care. London:Heinemann Medical Books, 1985;112.
2. Pilcher DB, Davis JH. Aorta and peripheralarteries. In: Davis JH, Drucker WR, Foster RS Jr.et al. eds. Clinical Surgery. St. Louis: Mosby,1987;2117.
3. Fackler ML. What's wrong with the wound ballisticsliterature, and why. Presidio of San Francisco,California: Letterman Army Institute of Research,1987; Institute Report No.239.
4. Fackler ML. Wound ballistics: A review of commonmisconceptions. JAMA 1988;259:2730-2736.
5. Hampton OP Jr. The indications for debridement ofgunshot (bullet) wounds of the extremities incivilian practice. J Trauma 1961;1:368-372.
6. Lindsey D. The idolatry of velocity, or lies, damnlies, and ballistics. J Trauma 1980;20:1068-1069.
7. Stevenson WF. Wounds in War. London, LongmansGreen & Company. 1897:107.
8. Kocher T. Eindrucke aus Deutchen kriegslazaretten.Correspondenz-blatt 'uer Schweitzer aerzte.1915;45:449-479.
9. Jolly DW. Field Surgery in Total War. New York,Hoeber. 1941:68.
10. Bailey H. eds. Surgery of Modern Warfare. 2nd ed,Vol I. Baltimore: Williams & Wilkins, 1942:16.
11. Ferguson LK, Brown RB, Nicholson JT, et al.Observations on the treatment of battle woundsaboard a hospital ship. US Nav Med Bull1943;41:299-305.
BALLISTICS RESEARCH -- FACKLER -- 8
12. Slesinger EG. The treatment of flesh wounds. In:Maingot R, Slesinger EG, Fletcher E eds. WarWounds and Injuries, 2nd ed. Baltimore: Williamsand Wilkins. 1943:22.
13. Crile G Jr. Experiences of the surgical service ofthe USNH, Aukland, NZ with casualties from theinitial Solomon Island engagement. US Nay Med Bull1943;41:306-324.
14. Cope Z. ed. Surgery. London: Her Majesty'sStationery Office, 1953:29.
15. Ogilvie WH. Cardinal sins of war surgery. Bull USA my Med Dept 1944;76:35-';6.
16. King KF. Orthopaedic aspects of war wounds inSouth Vietnam. J Bone & Joint Surg 1969;51B:112-117.
17. Commander in Chief Pacific (CINCPAC). War Surgery.In: Proceedings of the Commander in Chief PacificFifth Conference on War Surgery, 29 March - 2April 1971, Tokyo, Japan. 1971:33. (Available fromCINCPAC, Attn: Surgeon, FPO San Francisco,California 96610).
18. Rich NM, Johnson EV, Dimond, FC Jr. Wounding powerof missiles used in the Republic of Vietnam. JAMA1967;199:157-161,168.
19. Dimond FC Jr, Rich NM. M-16 rifle wounds inVietnam. J Trauma 1967;7:619-625.
20. Berlin R, Gelin LE, Janzon B, et al. Local effectsof assault rifle bullets in live tissues. ActaChir Scand; Suppl 1979;459.
21. Fackler ML. Wounding pattern of military riflebullets. Int Def Rev Jan 1989;59-64.
22. Nordstrand I, Janzon B, Rybeck, B. Break-upbehaviour of some smail calibre projectiles when
1979;489:81-90.
23. Fackler ML, Malinowski JA. The wound profile: avisual method for quantifying gunshot woundcomponents. J Trauma 1985;25:522-529.
BALLISTICS RESEARCH -- FACKLER -- 9
24. Berlin R. Energy transfer and regional blood flowchanges following missile trauma, J Trauma1979;19:170-176.
25. Scott R. Projectile Trauma: an Enquiry into BulletWounds. Oxford: University College;1976.
26. Albreht M, Scepanovic D, Ceramilac A, et al.Experimental soft tissue wounds caused by standardmilitary rifles. Acta Chir Scand; Suppl1979;489:185-198.
27. Bellamy RF. Personal communication 1988.
28. Dahlgren B, Berlin R, Janzon B, et al. The extentof muscle tissue damage following missile traumaone, six and twelve hours after the infliction oftrauma, studied by the current method ofdebridement. Acta Chir Scand; Suppl 1979;489:137-144.
29. Rockert H, Berlin R, Dahlgren B, et al. Celldamage at different distances from wound channelscaused by spherical missiles with high impactvelocity 1-12 hours after injury. Acta Chir Scand;Suppl 1979;489:151-158.
30. Wang ZG, Qian CW, Zhan DC, et al. Patholcicalchanges of gunshot wounds at various intervalsafter wounding. Acta Chir Scand; Suppl1982;508:197-210.
31. Zhang D, Qian C, Liu Y, et al. Morphologicobservations on high-velocity steel bullet woundsat various intervals after wounding. J Trauma;Suppl 1988;28:$98-SI04.
32. Ziervogel JF. A study of the muscle damage causedby the 7.62 NATO rifle. Acta Chir Scand; Suppl1979;489:131-135.
33. Rybeck B. Missile wounding and hemodynamic effectsof energy absorption. Acta Chir Scand; Suppl1974;450:5-32.
34. Proceedings of the 5th International Symposium onWound Ballistics. Gothenburg, Sweden, June 11-14,1985. J Trauma 28, Suppl, 1988.
35. Davis JH, Drucker WR, Foster RS, et al. ClinicalSurgery. St. Louis: Mosby, 1987:2117, 2337.
BALLISTICS RESEARCH -- FACKLER -- 10
36. Owen-Smith MS. Wounds caused by the weapons ofwar. In: Westaby S, ed. Wound Care, London:Heinemann Medical Books, 1985:110, 112, 114.
37. Dufour D, Kroman Jensen S, Owen-Smith M, et al.Surgery for victims of War. Geneva: InternationalCommittee of the Red Cross, 1988; 7, 11, 13e14,43.
38. Sedwitz MM, Shackford SR. Vascular trauma, In:Cuschieri A, Giles GR, Moossa AR, eds. EssentialSurgical Practice. 2nd ed, London: Wright,1988:305.
--FACING PAGE--
Fig. 1. All of the fragments that caused theseentrance wounds remained in the body, as isthe case almost without exception. Thisindicates that the striking velocity wasprobably not over 1000 ft/s (305 m/s).
BALLISTICS RESEARCH -- FACKLER -- 11
~0.
~4~
.. ~
~$~I-44'h Ut.
~~
trvt"
4zt. ~
"I'.
- 'U -
'-'CI -''
~ ~.ft ~
1'
4$4
A
* 'J,4
/- * -,
J5
BALLISTICS RESEARCH -- FACKLER -- 12
0
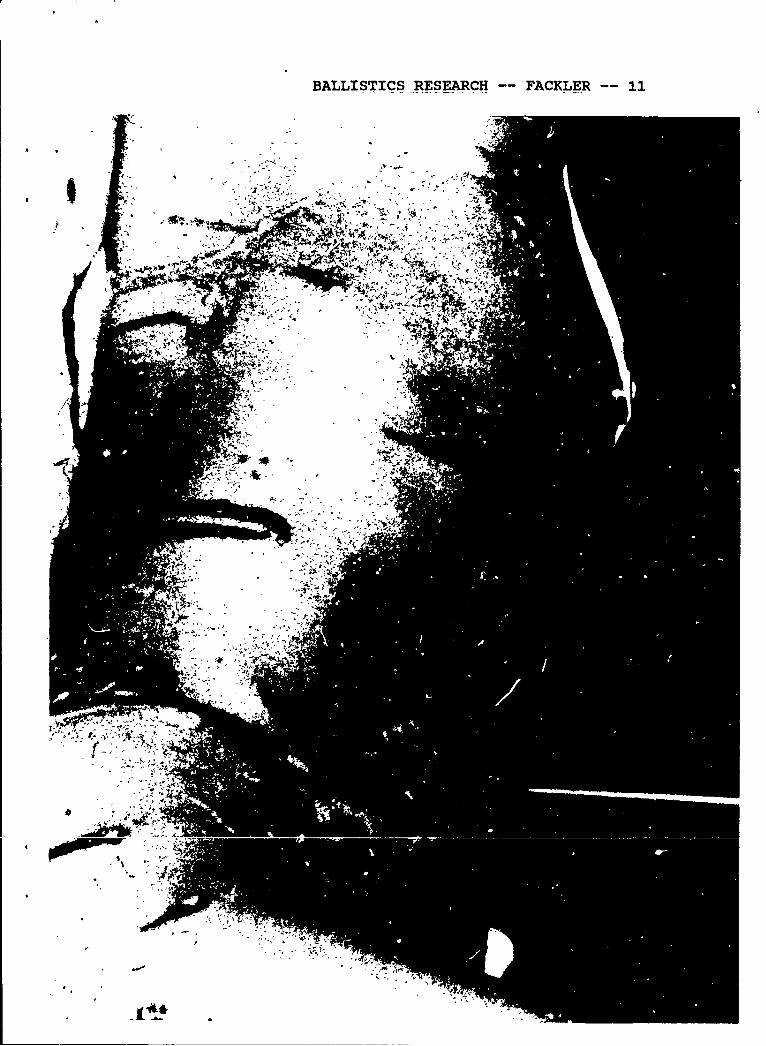
6 mm Steei SphereVel-3382 f/s (1031 mis)Wt- 13.6 gr (0.9gm)
Temporary Cavity
Permanent Cavity
0 i,. 1 .- - t T
... .. .. -. ". -
OC 5 10 15 20 25 30 315 4'0 43
Fig. 2. Wound profile produced by a steel sphere.Observe that little or no cavitation occursin the last 15 cm of penetration. This lastpart of the sphere's path corresponds to thatobserved in battlefield casualty, yet mostwound ballistics researchers who use thisprojectile concentrate exclusively on theinitial part of the path. The cavitationeffects of the first part of the projectilepath A-,e not en n frgment wounds of thewounded combat casualty and the cavitationeffects produced by rifle bullets occur at adeeper penetration. Although the sphere doesproduce easily repeatable results, theseresults unfortunatly do not reproducebattlefield type wounds.
BALLISTICS RESEARCH -- FACKLER *-13
~- 4 *.111
~~is
.-. i C."
[7 :7=~
IIA.
m-tag 1240- )UU
-, ."* 4..II,)P
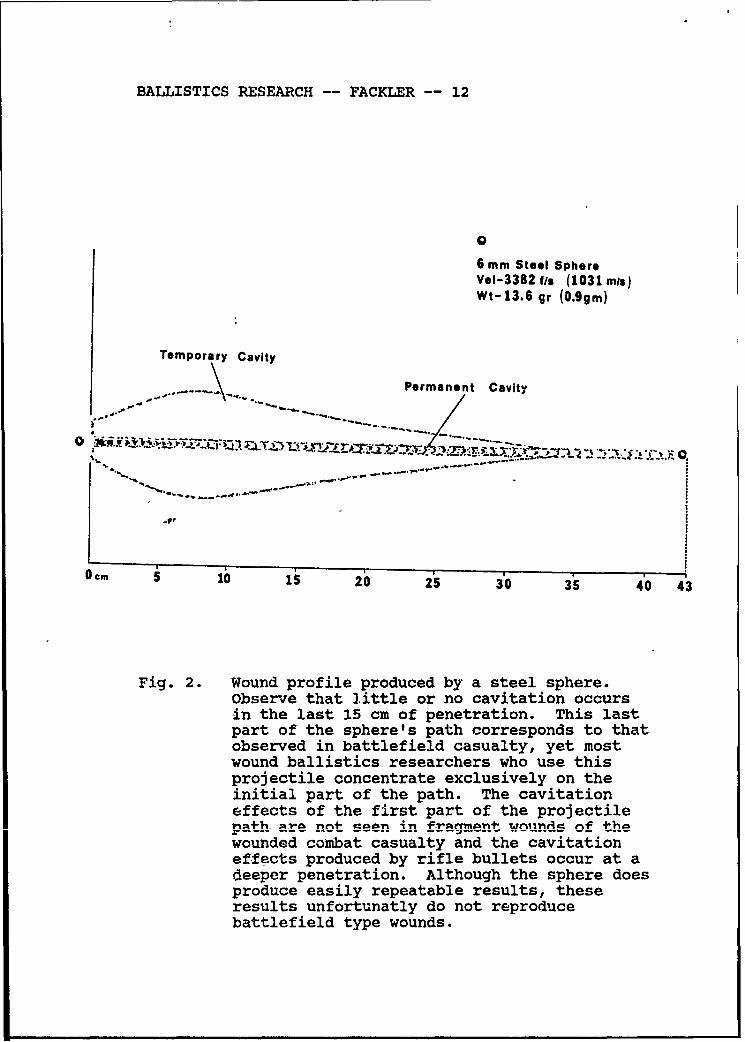
0-1 6 S i o is6 s9X3zrz Con ca rf 4-h-
D"60------66-v ---- ---
veloiy rife bulet ma3 enomr
edirupetive pth mny shipe extrmit wroundes
caused by lowest velocity handgun bullet.
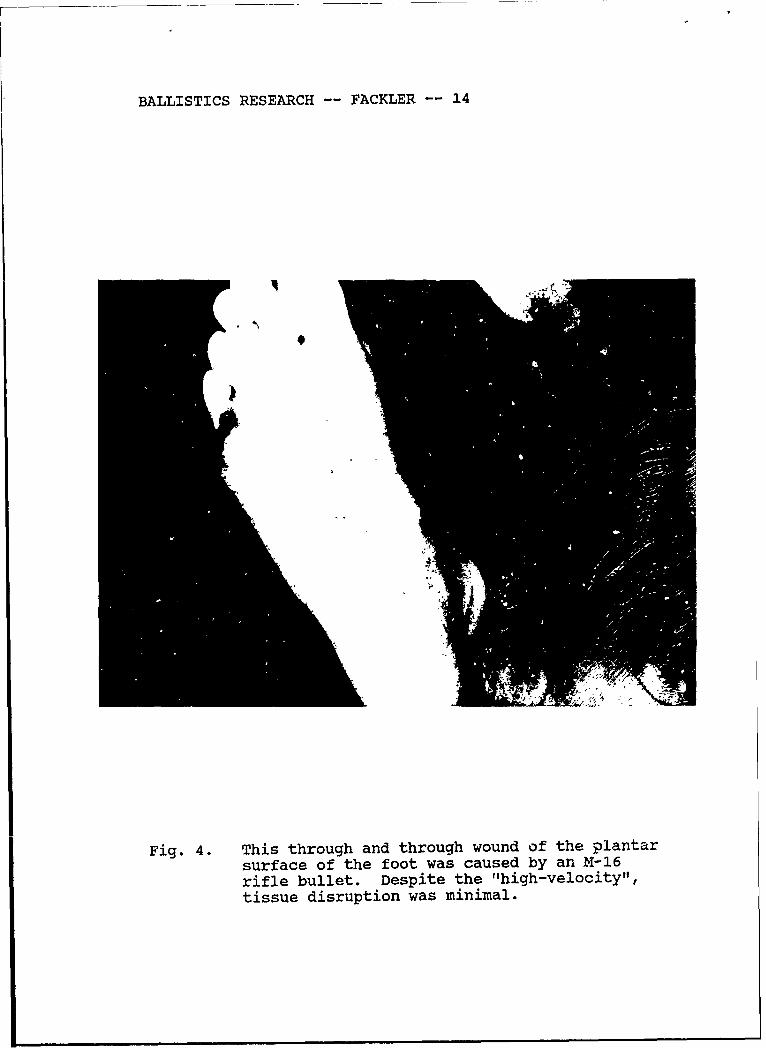
BALLISTICS RESEARCH -- FACKLER -- 14
Fig. 4. This through and through wound of the plantarsurface of the foot was caused by an M-16rifle bullet. Despite the "high-velocity",tissue disruption was minimal.
BALLISTICS RESEARCH FACKLER -- 15
OFFICIAL DISTRIBUTION LIST
Commander CommanderUS Army Medical Research US Army Medical Materiel Development
& Development Command ActivityATTN: SGRD-RMS/Mrs. Madigan Fort Detrick, Bldg T622Fort Detrick, MD 21701-5012 Frederick, MD 21701-5009
Defense Technical Information Center Commande:ATTN: -DTIC/DDAB (2 copies) US Army Biomedical Research andCameron Station Development LaboratoryAlexandria, VA 22304-6145 ATTi14: Library
Fort Detrick, Bldg 568Office of Under Secretary of Defense Frederick, MD 21701-5010
Research and EngineeringATTN: R&AT (E&LS)," Room 3D129 CommanderThe Pentagon US Ar.my Research Institute ofWashington, DC 20301-3080 Environmental Medicine
ATMN: SGRD.UE-RSADASG-AAF.JML Kansas StreetArmy/Air Force Joint Medical Library Natick, MA 01760-5007Offices of the Surgeon: General5109 Leesburg Pike, Room 670 CommanderFalls Church, VA 22041-3258 US Army Institute of Surgical Research
Fort Sam Houston, TX 78234-6200HQ DA (DASG-ZXA)WASH DC 20310-2300 Commander
US Army Medical Rearch Institute ofCommandant Chemical DefenseAcademy of Health Sciences ATTN: SGRD-UV-4JUS Army Aberdeen Proving Ground, MD 21010-5425ATMN: HSH!A-CDMFort Sam Houston, TX 78234-6100 Commander
US Army Aeromedical ResearchUniformed Services University of Laboratory
Health Sciences Fort Rucker, AL 36362-5000Office of Grants Management4301 Jones Bridge Road AIR FORCE Office of ScientificBethesda, MD 20814-4799 Research (NL)
Building 410, Room A217US Army Research Office Boiling Air Force Base, DC 20332-6448ATTN: Chemical and Bio, 3gical
Sciences Division USAF School of Aerospace MedicineP0 Box 12211 Document SectionResearch Triangle Park, NC 27709-2211 USAFSAM/TSKD
Brooks Air Forc, Base, TX 78235-5301DirectorWalter Reed Army Institute of Research Head, Biological Sciences DivisionATTN: SGRD-UWZ-L OFFICE OF NAVAL RESEARCHWashington, DC. 20307-5100 800 North Quincy Street
xlIn,, ... A 22217-5000CommanderUS Army Medical Research Institute
of Infectious DiseasesATMN: SGRD-ULZ-AFort Detrick, MD 21701-5011
4/88



![2019-04-27 OnTarget First Aid Training Flyer [print]...Gun Range/Gunshot Wound Basic First Aid* Topics Covered: Gunshot Wound Basics: Tactical Treatment Ballistics and the Effects](https://img.pdfslide.us/doc/110x75/5f4849042f6f1a4a393115fb/2019-04-27-ontarget-first-aid-training-flyer-print-gun-rangegunshot-wound.jpg)