Embed Size (px)
Citation preview

KimKaim 8/19/2016 Page1of31
Wound Assessment
www.woundcareresource.com
Assessment..................................................................................................................................................2History......................................................................................................................................................................2Examination............................................................................................................................................................3Measurethewound.............................................................................................................................................................4WoundLocation....................................................................................................................................................................6UsingTIMEtoassessthewound....................................................................................................................................7TisforTISSUE........................................................................................................................................................................7IisforINFECTION/INFLAMMATION.......................................................................................................................10MisforMOISTURE.............................................................................................................................................................13EisforEDGES.......................................................................................................................................................................15
Investigation........................................................................................................................................................16Diagnosis...............................................................................................................................................................16Implementation..................................................................................................................................................17Collaboration........................................................................................................................................................................18
Assessmenttoolsusedinwoundmanagement............................................................................18Thedigitalage.....................................................................................................................................................21
AppendixA–StudentAssessmentTool...........................................................................................22AppendixB–STARSkinTearClassification...................................................................................24AppendixC–PressureInjuryClassifications................................................................................26References.................................................................................................................................................29

KimKaim 8/19/2016 Page2of31
Assessment Yearsago,clevererpeoplethanIcouldseepatternsemergingwhereifcertainthingsweredonetherewouldbebetterwoundhealingoutcomes.Theypulledalltheseideastogetherandwrappedmnemonicsaroundthemtomakethemeasiertoremember.TwomnemonicsthatworkwelltogetherareHEIDIandTIME.ThesestandforHistory,Examination,Investigation,DiagnosisandImplementation(HEIDI)andTissue,Inflammation,MoistureandEdges(TIME).TohelpremembertheseIhaveincludedadatacollectiontoolyoucanuse,seeAppendixA.NowwewillgointoALOTmoredetailabouteachofthese.
History ItisimportantthatyourassessmentconsiderstheWHOLEpatient,notjusttheHOLEinthepatient(1).Startbyconsideringwhatsystemicfactorsmightimpactonwoundhealingorimpactonyourplan.
o Systemic§ Diseaseprocesses§ Behavioral§ Social
ThisiscertainlyNOTcomprehensive,buttogiveyouanideaofwhatsomeofthesethingsmightlooklike:
Systemic Impactonabilitytoheal plan
Medical Poorcirculation–howwillthenutrientsgettotheskin,howwillwaste/oedemabetakenaway?Pooroxygenation–howmuchoxygenismakingittotheskin?Metabolic–whatimpactdoesdiabeteshaveonwoundhealing?Auto-immune–forreasonsnotyetfullyunderstoodthebodyattacksit’sownorgans,includingtheskinandsupportingstructures.
immunecompromised-willnotshowtypicalsignsofinfection,doyouwatchforothersignsoruseatopicalantimicrobialprophylactically?impairedsensation–cannotfeelifcompressionistootight.

KimKaim 8/19/2016 Page3of31
Systemic Impactonabilitytoheal plan
Surgical/Iatrogenic
AlterationtolymphsystemsuchasinlymphnoderemovalforCancer–canleadtooedemaPreviousscartissue–suchasfromradiationorburns–structureisdifferenttonormalskinandslowertoheal,canbethesourceofmalignancyGatechanges–amputationwillchangegate,causingabnormalpressuresinotherareasofthefoot,potentialforfurtherulcerationinthosenewareas.
workingaroundsurgicalsites–applyingaVACaroundex-fixpinsmanagingexudatefromastomaorfistula
Nutrition Noteatingwell–oftenrelatedtoageVegetarian
expectdelay–higherproteinandcaloricintakeisrequiredforwoundhealing
Social Notmobile–pressurerelatedtissuedamage,poorcalfmusclepumpPoorhousingorincome–poorenvironmentalcontrolscanimpactonhealingSmoking–reducedoxygentoskin
onfeetallday–off-loading?Venousreturn?cost-cannotafforddressings
Medications CorticosteroidsAnti-inflammatoriesAnti-coagulents
Warfarin–wouldyoudebride?
Allergies AdhesivesIodineChlorhexadine
Theinformationwegetfromthepatient’shistorygivesusalistofitemsthatmayresultinimpairedhealingorthepotentialforskinbreakdown.Weneedtoplantomitigatetheimpactofasmanyaswecan;ieeducationonquittingsmoking,refertospecialist,orchoosingmoreaffordabledressingsaswellasanyhomesupporttheymighthaveorneed.
Examination Thisiswherewestarttogetourhandsonthepatient.So,continuingonfromabove,wenowneedtoassessregionalsymptomsthatwillneedtobemanagedtoimprovewoundhealing.
o Regionalexamples§ Circulation§ Infection§ Oedema

KimKaim 8/19/2016 Page4of31
Regional Impactonabilitytoheal plan
Oedema oedemamakesitdifficultforadequatedistributionofnutrientstofeedtheskin
Canitbemanaged?
Pulses indicatesabilityofnutrientstogettothearea
Present?Notpresent?Doyouneedtocollaborate?
Atrophy,nohair,thinshineyskin
Oftenassociatedwithlackofpulses,mayindicatepoorarterialsupply,possibleclaudicationpain
RequirescollaborationwithVascularasaminimum–donotdebride
Haemosiderinstaining,varicoseveins,ankleflair,etc…
Oftenassociatedwithoedemaoraninvertedchampagnebottleappearance,mayindicatepoorvenousreturn
ReferraltoVeinspecialist,ABPIrequired,assessmentforcompressionsuitability
Drycrackedskin Lessresilient,increasesriskofinfection
non-soapcleaning,waterintake?,humidity(airconditioning),moisturize
Charcotdeformity Changestogate,potentialforulceration
Requirescollaborationwithpodiatryasaminimum
Contractures Maybeputtingconstantpressureontocertainareasorincreasingbuildupofmoistureincreases.
Redistributepressureasable.Managemoisture.Collaboratewithoccupationaltherapistand/orphysiotherapist
Again,notfullycomprehensivebutastart;seeifyoucancomeupwithmore!NOW!!Thisiswherewestarttolookatthewound(finally!).
Measure the wound Weneedtorecordthesizeandlocationofthewound.Serialsizemeasurementsneedtoberecordedastheyindicatewhetherornotawoundishealing;onesourcerecommendsthatawoundshouldbeatleast30%smaller(surfacearea)byweek4(2)tobeconsideredonahealingtrajectory.Measurementofthewoundcanbedoneinseveralways:
• Ruler• Acetate/Grid• Visitrak(planimetry)• Digitalphotoandwoundtracingsoftware(digitalplanimetry)• Specialisedphotographicdevice
Priortomeasuringthewound,cleanthewound.Ifplanningtodebride,conductmeasurementsafterdebriding.Positionthepatientinacomfortablepositionkeepingmindthatpositioning,bodycurvature,ortaperingofthelimbswillimpactontheaccuracyofthevarioustechniques(3).Alsoensurethatallmeasurementsaretakenofthewoundbase,correctidentificationofwoundmarginshasalargeimpactonwoundsizeaccuracy(4).

KimKaim 8/19/2016 Page5of31
Whenusingaruler,measurementsaretakenofthegreatestwidestandthegreatestlengthperpendiculartothegreatestwidth(5).Thisisaquickmethodandworksbestwithregularlyshaped,smalltomediumsizedwoundsliketheoneinthephotoontheright(3,4).Multiplylengthxwidthtoconverttoanareameasurement.Inirregularlyshapedwounds,itismoreaccuratetotracethewoundontoacetateandmeasuretheareabyplacingthetracingongridpaperandaddingupthenumberofsquarescontainedwithinthemarginoftheoutlineofthewound.Whilethisisconsideredmoreaccurateforirregularlyshapedwounds,errorcomesintoplaywhentryingtodeterminehowtoincludepartiallycoveredsquares(3,4).Considerthewoundontherightandaskyourselfhowwouldyougomeasuringthiswound?Wouldyouusearuleroracetate?VisitrakisadevicethatwascreatedbySmithandNephewforwoundmeasurement.Ithadasterileacetatesheetwithdisposablebackingfortracingthewoundonto.Youthenlaidthetracingontothedeviceandre-traceditwiththedevice’sstylus.Whilethiswasverygoodforinfectioncontrolandcouldquicklyreportheight,width,areaandcircumference,therewerepotentialforerrorsinaccuracyrelatedtoretracingandalsothesizeofthedevicelimitedthesizeofthewoundyoucoulduseiton(4,5).ThereissoftwareavailableforpurchasesuchasMOWA,whichallowstheusertotakeaphotographwiththeircamera,tracethewoundedgesinthephoto,anditproduceswounddimensionsandrecommendstissuetypebasedoncolour.TherearealsofreeprogramssuchasImageJ,whichcanbeloadedontoacomputerandalsoallowstheusertotracethewoundedgesanditproducesthedimensions.Theaccuracyofbothofthesemethodswillbeaffectedbythecurvatureofthesurfaceandtheabilityoftheusertotracethewoundedgeaccurately.Anumberofspecializedphotographicdevicesareonthemarkettoday.TheSilhouetteStarisacamerawhichuseslasertechnologytomeasurewounddepthanddigitalplanimetry(wheretheusertracesthewoundedgeinthephoto)tomeasurearea.Themanufacturerclaimsahighdegreeofaccuracyandeaseofuse.YouneedtohaveacomputerortabletwiththeSilhouettesoftwareattachedtothecamera.WhiletheSilhouetteStardoeshaveamethodforcalculatingdepth,inallotherinstancestheuserwillneedtodothismanually.Also,evenwhenusingtheSilhouetteStar,underminingisnotdetectedand,again,willneedtobemeasuredmanuallywithasterileprobe.Thereareanumberofdevicesthatcanbeusedincludingcotton-tippedswabsandsterileplasticstickswithmeasurementgraduationsonthem.ThedepthgaugethatwassoldtoaccompanytheVisitraksystemwasathinplasticstickwithmeasurementgraduationsandafoamtip.Thiswasthinandflexibleenoughtomeasuremostundermining/sinuseswithoutfearofdamagingsurroundtissueorleavingfibresbehind.Youwillneedtoprobearoundthewoundtofindthegreatestdepthtorecord.Also,wherethereisasinusorundermining,youwillwanttorecordthegreatestdepthandalsothelocationatthewoundedge.Thisisdonebyimaginingaclockfaceoverthe

KimKaim 8/19/2016 Page6of31
woundwith12o’clockbeingatthehead.Therefore,inthepictureontherightyouwoulddescribetheunderminingasbeingXcmextendingfrom6O’clockto9O’clock.
Wound Location Thelocationofthewoundwillalsoimpactondeterminingadiagnosisandcontributetotheplan(3).Belowisatableshowinglocationsandtheirlikelycorrelationstowoundtype.However,thisisjustaguideandnotadiagnosis.
Siteofwound&typeofulcerSite TypeofulcerLowerthirdoflegbelowknee VenousulcerBonyprominencese.g.heels,coccyx,sacrum,hips)
Pressureulcer
Topoffoot,bonyprominences ArterialulcersAnkles Venous,arterialorpressureulcerSoleoffoot&toes DiabeticfootulcersSunexposedareas Skincancers

KimKaim 8/19/2016 Page7of31
Using TIME to assess the wound
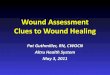
T is for TISSUE Epithelial Granulating Slough Necrotic
Theimageaboveistryingtoconveythatifthewoundisgreaterthan50%granulatingandepithelial,considerprotectionasyouraim.Ifitfallstothesloughandnecroticsidethenconsiderdebridement.Tissuetypestendtobedescribedbycolour.Pinkisforepithelial,redforgranulating,yellowforsloughandblackforeschar.Alsoconsiderotherdescriptorsthatmaybehelpful,thesefouralonedonotalwaysgiveyouagoodpictureofwhat’shappeninginthewound.Thewoundinthephotoontherightcouldbedescribedas90%escharand10%granulationtissue.Butthatcouldalsopertaintoacrustydryscab,andthisisreallywet;it’sactuallycoagulatedbloodfromunderabloodblister.Somayberatherthansayingescharitcouldberecordedaswetescharorevenclottedbloodfirmlyadheredtothewoundbed.Photosareagreatwaytorecordawound,butevenwithaphotoagooddescriptioncanbeveryhelpful.Theepithelialandgranulatingtissuetypesareconsideredviable.Thesearealiveanddoingwell.Sloughandeschararenotviable,theydonothaveabloodsupplytosupporthealingandtheyarenotalive.Itisdeadmaterialanditneedstogo.Thepresenceofnon-viabletissueanddebris(foreignbodies/olddressingproduct/sutures)(6):
• providesafocusforinfection• prolongstheinflammatoryphase• mechanicallyobstructscontraction• impedesre-epithelialization• masksunderlyingfluidcollectionsor
abscesses• makesitdifficulttoevaluatewound depth
NonViable
Viable
Epithelial
Granulating
Slough
Necrotic
Debride
Protect

KimKaim 8/19/2016 Page8of31
Debridementistheactofremovingdevitalizedtissuesfromthewoundbed.Theactofdebridingthewoundbednotonlyimprovesthetissueinthewoundbedbutitalsohasapositiveimpactoninflammation(restoresfunctionalextracellularmatrixproteins),moisture(reducesexudate)andedges(encouragesmigration)–theotherthreecomponentsofTIME.Anumberofthingsneedtobeconsideredbeforedebriding(7):
• Patientpreference-includingpaintolerance(plustheymightnotlikemaggots)• SkilloftheclinicianandScopeofPractice–Getotherswiththeexperienceandclinical
skillsinvolvedifneeded• Riskmanagement–isthereachanceyoucoulddomoreharmthangood,isthere
trainingyoucandotoimproveyourskills,andagain,istheresomeonewhocanassistyou?
• Environmentalfactors–thingslikelighting,posture,PPEandriskforcontaminationoftheenvironmentorfurthercontaminationofthewound
• Resources-makesureyouhaveeverythingyouneedbeforeyougetstarted.Insomeareasyoumaybelimitedinyouroptions.
• Contraindications-theseincludepropensitytobleed,presenceofunderlyingstructuresandlackofadequatebloodsupply.
Ifdebridementisrequiredyouneedtodeterminethebestmethod.MostoftenasNurseswemakeuseofautolyticandmechanicaldebridement(thevigoroususeofasurgispongeisconsideredmechanicaldebridement).Butyouneedtobesurethatdebridement–whateverthechosenmethod–issafe.WhennottoDebrideDebridementisnotalwaysthepreferredoptionforallwounds.Inthecaseofthenecroticheelortoeinthepatientwithpoorarterialflow.Iftheareaisdry,leaveit.Itwilleventuallymummifyandauto-amputate.Tryingtomoistenorremovethetissueisonlylikelytointroducenewwaysformicrobialinvasionthatthebodyisnotabletofight(8).Also,forthepalliativepatientwherecareissupportive,againifitisdryandnotcausinganypain,leaveit(9).Fungatingwoundsarechallenginginthattheyproducecopiousamountsofexudateandodourbutarehighlyvascular.Attemptstodebridemaycausecatastrophicbleeding,howeverleavingitcausesfurtherdamagetothesurroundingskinfrommacerationandstresstothepatientfromtheodour(10).CleaningwithsomethinglikeProntosanhelpstoreducethebioburden,whichinturnreducestheexudateandtheodour(11).

KimKaim 8/19/2016 Page9of31
Table 1: Debridement methods Type Mechanisms of action Advantages Disadvantages Who/where
Autolytic
Uses the body’s own enzymes and moisture to rehydrate, soften and liquefy hard eschar and slough using occlusive or semi-occlusive dressings and/or antimicrobial products to create a balanced moist wound environment either by donating or absorbing moisture
Can be used for pre-debridement, when there is a small amount of non-viable tissue �Also suitable for wounds where other forms of debridement are inappropriate
Can be used for maintenance debridement
The process is slow, increasing potential for infection �and maceration
Can be done by both generalist and specialist
Biosurgical
Larvae of the green bottle fly are used to remove necrotic and devitalised tissue from the wound. Larvae are also able to ingest pathogenic organisms in the wound.
Highly selective and rapid
Costs are higher than autolytic debridement, but treatment is short once in place �Not suitable for all patients or wounds
Can be applied by generalist or specialist practitioner with training. Closed bag method reduces skill level required and can be left for 4-5 days
Hydrosurgical Removal of dead tissue using a high energy saline beam as a cutting implement
Short treatment time and selective. Capable of removing most if not all devitalised tissue from the �wound bed
Requires specialist equipment. There is potential for aerosol spread and it is associated with higher costs
Must be carried out by a specialist practitioner with relevant training. Can be used in a variety of settings
Mechanical
Traditional method involves using wet to dry gauze that dries and adheres to the top layer of the wound bed, which is �‘pulled’ away when the dressing is removed
Newer methods are more selective, faster and relatively pain-free �
Non-selective and traditional methods are potentially harmful Requires frequent dressing changes and can be very painful for the patient
Can be done by both generalist and specialist
Sharp
Removal of dead or devitalised tissue using a scalpel, scissors and/or forceps to just above the viable tissue level. This does not result in total debridement of all non-viable tissue and can be undertaken in conjunction with other therapies (eg autolysis)
Selective and quick. No analgesia is required normally
Clinicians need to be able to distinguish tissue types and understand anatomy as the procedure carries the risk of damage to blood vessels, nerves and tendons
Can be done at the patient’s bedside or in clinic by a skilled practitioner with specialist training
Surgical
Excision or wider resection of non-viable tissue, including the removal of healthy tissue from the wound margins, until a healthy bleeding wound bed is achieved
Selective and is best used on large areas where rapid removal is required
It can be painful for the patient and anaesthetic is normally required �It can be associated with higher costs
Must be performed in the operating theatre by a surgeon, podiatrist or specialist nurses following training
Ultrasonic
Devices deliver ultrasound either in direct contact with the wound bed or via an atomised solution (mist). Most devices include a built-in irrigation system and are supplied with a variety of probes for different wound types
Immediate and selective. It can be used for excisional debridement and/or maintenance debridement over several sessions
Availability issues due to higher costs and requirement for specialist equipment �Requires longer set up and clean up time (involving sterilisation of hand pieces) than sharp debridement.
Must be carried out by competent practitioner with specialist training in a variety of settings
TablecopiedfromDebridementMadeEasy(12)

KimKaim 8/19/2016 Page10of31
I is for INFECTION / INFLAMMATION
Thisimageshowstheprogressionfromnormalinflammation(wherethewoundiscontaminatedwithopportunisticandtransientpathogens)tosystemicinfection.Beloweachphasearetheactionsyoucanconsiderforeachphase.Theyarecumulative:soforawoundthatappearscriticallycolonizedyouwouldwanttoclean,debrideanduseatopicalantimicrobial.Infectionistheoutcomeofthedynamicinteractionsthattakeplacebetweenahostandapotentialpathogenwherethehostdefensestrategiesaresuccessfullyevadedandthereisanegativeimpactonthehost(13).Complexinteractionsleadingtoinfectionarenotyetcompletelyunderstoodbuthavebeengroupedinto3broadareas:Contamination
• Allwoundswillhaveatransientcollectionofmicro-organisms.Whenthehost’sdefensesareadequateandtheconditionsarenotinfavourofthemicro-organism,theywillnotmultiplyandwoundhealingisnotdelayed.
Colonisation
• Microbialspeciesareabletosuccessfullygrowandreplicatebutdonotprogressfurthertodamagethehost.Woundhealingmaybedelayed.
Infection
• Thelevelofmicrobialgrowthandreplicationoverwhelmsthehost’sdefensesleadingtocellularinjuryandhostimmunologicalreactions.Woundmaydeteriorate.
Theimageshownabove,theinfectioncontinuumarrow,isamodifiedversionoftheonein“TheMicrobiologyofWounds”byPercival&Dowd(14).Theyexpandthisspreadfromcolonizationtoinfectioninto6stages:
Clean
Debride
TopicalAntimicrobial
SystemicMedications

KimKaim 8/19/2016 Page11of31
Table 2: Stages of microbial invasion ContaminationorTransientStage
Thisiswherebacteriaareenteringanareaandassessingitssuitabilityforcolonization.Theymayhavecomefromsurroundingareasonthepatient(endogenous)orfromtheenvironmentorhealthcareworker(exogenous).Thesebacteriaarestillinafreefloatingor‘planktonic’stageandarevulnerabletoeradication.
ColonizationStage1—ReversibleAdhesion
Ifthebacteriadecidethatthisisasuitablelocationtogrowitwillstarttoattachitselftothehostcellsusingwhateveradhesionoptionsithas.Thisiscalledreversibleadhesionbecauseitisstillpossibletoremovethesebacteriawithlowlevelsofsheerforce(egsalinerinses)andtheyarealsostillverysusceptibletoantimicrobialagentsandhostdefenses.Astimegoesontheadhesionforcesbecomestrongerandthebacteriastarttoproduceextracellularsubstancestomaketheareamoresuitable,thusstartingthedevelopmentofthebiofilm.EarlycolonizingbacteriaaretypicallyStaphylococcusandbetahemolyticStreptococci.
ColonizationStage2—IrreversibleAdhesion
Atthispointthebiofilmisnowstartingtoaltertheconditionsinthewound,makingitmoredifficultforthehostdefensesandantibioticstogettothebacteriahidinginit.Itisstillpossibletoremovebutwithagreateramountofforcerequired.Thisnewbiofilmencouragesotherbacteriatojointhecommunity.Asthecommunitygrowsandnumbersofbacteriaincreasemicro-coloniesformandareasofthebiofilmbecomehypoxic,thuscreatingasuitableenvironmentforanaerobicbacteriaaswell.
CriticalColonizationStage—ClimaxCommunityor“Biofilm”
Fromaclinicalperspective,thisiswherethewoundissufficientlycolonizedtoexertit’seffectsonthewoundandpreventhealing.Fromamicrobiologicalpointofviewitisthecriticalmassofbacteriathathasformedaviablecolonybuthasnotyetobtainedhighenoughnumberstoinvadesurroundingtissues(causeinfection).Thereisnosetnumberasdifferentcombinationsofpathogensandhostdefensesmeanthisthresholdwillvary.
LocalInfectionStage
Oncethecolonyismature,growthwillcontinueexponentiallyandbacteriawillbeabletousethissafecolonyasastagingareatoinvadelocaltissues.Alocalwoundinfectionwillpresentclinicallywithredness(erythema),excessivepain,swelling,heatgeneration,woundbreakdownandincreasedlocaltemperature.Othermoresubtleclinicalsignsofinfectionhaveincludedalterationinexudate,friablegranulationtissuethatbleedseasily,malodor,anddiscoloredgranulationtissue.Reportedgranulationtissuediscolourationhasincludedyellow,green,orbluewhenbacteriasuchasPseudomonasaeruginosa,Streptococci,andBacteroidesfragilishavebeencultured.
SystemicInfectionStage
Ifthebiofilmisnotdisturbedwithappropriatewoundbedpreparationtechniques,appropriatedressingmanagementandtheuseoftopicalantimicrobialsthecolonywillcontinuetoproduceinvadingbacteriawhichcanleadtobacteriagettingintothebloodstream(bacteremia)leadingtosepsisorsepticemia(multiplicationofbacteriainthebloodandtoxinproduction),potentialorganfailure,andinextremecases,death.
Cleaning,debridingandappropriateuseofantimicrobialdressingsallhelptoreducebioburdenandreducetheestablishmentofabiofilm.Researchersarestillunclearhowlongittakesabiofilmtoform.Therearemanyvariablesincludingstrainofbacteriaandit’s

KimKaim 8/19/2016 Page12of31
adhesionmethods,hostdefensesandtypeofmaterialbeingadheredto(ieskinvsimplant).Therearein-vitrostudies(controlledenvironment,inalab/notonalivesubject)thatindicateStaphylococcusaureuscancreateabiofilmwithin2-3hoursandotherstudiesonpigmodelsthathaveestablishedbiofilmswithin48hours(15,16).Thetheoriesbehindwhythesebacteriaformbiofilmsarealsovaried(17).Biofilmsmaybecreatedforprotectionfromhostdefenses,colonizationofanutrient-richareaand/orutilizationofthecooperativebenefitsofacommunity(17).Thebiofilmisknowntoenhancecommunalprotectionfromphagocytosisbypolymorphonuclearleukocytes(PMNs).Thismeansthatoncethehardierspecieshavestartedtoestablishabiofilmthemoresensitivespecieswillhaveasafeplacetoattachandgrow.Itmayevenmakethesesensitivespeciesappeartobe‘resistant’.Oncetheoxygenstartstobedepletedtheanaerobescanalsojointhecommunity.Thissynergybetweenaerobicandanaerobicbacteriahasbeendocumentedtoincreasetheseverityofaninfection(18,19).Thesitethebacteriachoosetocolonizemaybenutrientrich,butthebacteriastillneedtobeabletounlockthosenutrientsincludingglycoproteins,sugars,andproteins.Inordertodothisnumerousenzymesarerequired,rangingfromproteasestoglycosidases.Havingacommunityofbacteriawitharangeofdifferentenzymaticpropertiesmeansthatmorenutrientscanbe‘unlocked’whichwouldbenefitthecommunityasawhole(14).Bycreatingcommunitieswheredifferentbacteriainhabitnichemicro-habitatsbestsuitedfortheirsurvival,andwherethebacteriacooperatetomeettheircollectivemetabolicrequirements,thebiofilmismorelikelytosucceed.Ifwedonotremovethebiofilm,thenthewoundislesslikelytoheal(14,20).Howdoweknowit’sinfected?Identifyingthedifferencebetweeninflammationandinfectioncanbetricky.Generallyspeaking,erythema,warmth,exudateandpaincanbeassociatedwithboth.Inapersonwhoisimmunocompromisedorhasareducedimmuneresponseforanotherreason(suchasinthefeetofpeoplewithdiabetes)theremaybenolocalsignthatinfectionispresent;thefirstsignscouldberigorsorpainatregionallymphnodes(21,22).Chronicandacutewoundsarealsoassesseddifferentlybecauseinacutewoundswehavethewindowofthefirst48hourswherewehaveanexpectationofwhatthe‘normal’woundhealingwilllooklike.Weexpectthatfortheacutewound,after48hoursthereshouldbeareductioninerythema,warmth,exudateandpainandifthesedonotreduce,oriftheygetworse,theremaybealocalinfection.ForchronicwoundsSibbaldetal(23)recommendtwomnemonicstohelprememberwhattolookforandtoalsodifferentiatebetweensuperficialanddeepbacterialburden.Thedifferencebeingthatsuperficialbacterialburdenmayrespondtotopicalantimicrobialswhereasdeepinfectionsusuallyrequiretheuseofsystemicmedications.
Forsuperficialinfection,thinkofNERDS
Fordeepinfection,thinkofSTONES
NonhealingwoundsExudativewounds
Redandbleedinggranulationtissue(friable)Debris(yelloworblacknecrotictissue)
Smellorunpleasantodourfromthewound
SizeisbiggerTemperatureincreased
Os[probetoorexposedbone]Neworsatelliteareasofbreakdown
Exudate,erythema,edemaSmell

KimKaim 8/19/2016 Page13of31
M is for MOISTURE
Animbalanceinmoistureresultsin:
• Desiccation-slowsepithelialcellmigration• Maceration–damagetowoundmargin
Theaimistorestoreepithelialcellmigrationthroughthemanagementofexudateanditsunderlyingcauses(24).Attheedgesofthewoundkeratinocytesproliferateandproducedaughtercellstomigrateintothewoundbed.Ifascabispresentproteaseshavetobreakdownandclearapathforthekeratinocytestoburrowunderneaththescab.Butinamoistenvironment,withoutascab,themigrationiseasierandhealingisaccelerated.Thisdiscoveryledtodevelopmentoftheconceptofmoistwoundhealing(25).Whilethisnewlayerofcellsisdelicate,mostmodernwounddressingsdonotremovethemwhenthedressingischanged.However,ifadressingisallowedtodryoutoradheretothewound,traumaticremovalofthedressingmayharmthedelicatenewepitheliallayer(26).Moistureinawoundcanbemodifieddirectlyorindirectly(27):
• Directo Theuseofabsorbentormoisture-balancingdressingso Theuseofcompressionand/orelevationtoeliminatefluidfromthewoundsiteo TheuseofTopicalNegativePressure(TNP)withdevisessuchastheVAC-
VacuumAssistedClosure• Indirect
o Controlofinfectionorbacterialloado Controlofoedemabysystemictherapysuchasthetreatmentofheartfailureo Useofimmunosuppressionorsteroidstocontrolinflammatoryexudatefrom
woundssuchaspyodermagangrenousum,vasculiticorrheumatoidulcersGeneralobservationsaboutdressings:
• DressingthatcontributetowoundmoistureincludeTenderWet,hydrogels,Honey,IodosorbPasteandother“Wet”dressings.
• Dressingsthatconservemoisture(stopiffromevaporatingawayand/orhandleasmallamountofexudate)includefilmsandhydrocolloids.
TooDry:Presenceofeschar,slower‘2-stage’healing
TooWet:Macerationandexcoriationdamagesperiwoundskinandslowshealing
Justright:Warm,moistwoundhealing
Absorb/ManageMoisture
Contribute/ConserveMoisture

KimKaim 8/19/2016 Page14of31
• Moderateamountsofexudatecanbemanagedbyhydrofibres,alginates,foams,simpledressings(likemelolinifchangedfrequently)anddressingswhichcontaintheseitemsasoneofitscomponents.AnexampleofacombinationdressingistheAquacelSurgical,whichhasahydrofibreinterfaceandahydrocolloidadhesivebacking.
• Highamountsofexudateneedeithermuchmorefrequentchangesofsimplerdressings(suchascombine)oruseofhighabsorbencydressingssuchasZetuvitorDrymax.Alternativelyincontinenceaids(withtheelastictrimmedoff)canbesecuredtotheexudingarea.Productslikeblueys/pinkiesandimproperlysecuredincontinenceaidscanbetriphazardssoshouldnotbeusedonmobile,orpotentiallymobile,patients.
• Otheroptions.Therearesomedressingswhichwillallowtheexudatetopassthroughtoasecondarydressingssothattheprimarydressingdoesnothavetogetchangedasoftenasthecheapersecondarydressingbutstillprovidethebenefitsofthelongerweartimefortheprimarydressing(examplesaremepilextransfer,aquacel,tullegras,andsiliconeinterfacedressings).Exudatemanagementsystemsinvolvinghydrocolloidsealsandplasticbagsarealsoanoption.Topicalnegativepressuretherapycanalsobeconsidered.

KimKaim 8/19/2016 Page15of31
E is for EDGES
Woundedgesthatare:• rolled• atadifferentleveltothewoundbed• undermined
donotallowforthemigrationofkeratinocytesacrossthewoundbed.Addressingtheunderlyingcauseshouldbetheanswer,butdebridementortheuseofadjunctivetherapiesmayneedtobeconsidered.Theaimistoencouragekeratinocytemigrationandwoundcontraction;thiswillbeseenasanadvancingwoundedgeandreductioninwoundbedsize(6).TheedgesreallyarethefinalindicatortoletyouknowthateverythingelseyoudidwithT,I,andMisworkingornot.Also,theedgescangiveusinformationtohelpdiagnosethetypeofwound.Belowisatableshowingedgecharacteristicsandtheirlikelycorrelationstowoundtype.However,thisisjustaguideandnotadiagnosisbyitself.
WoundedgecharacteristicsEdges TypeofwoundSloping VenousulcerPunchedout ArterialulcerRolled BasalcellcarcinomaRaised SquamouscellcarcinomaUndermining PressureulcerCalloused DiabeticfootulcerPurple Vasculitic
Theotherthingtorememberisthattheseedges,andtheperiwoundskin,needtobeprotectedduringthecourseofthewoundtreatment.Thingslikeexcessmoistureandincreasedbioburdenlevelscanaffecttheperiwoundskin.Theuseofadhesivescancausedamagefromtheirfrequentremovalormaytriggeranallergicresponse.Productsusedtodebridenecrotictissuecanbejustasreadytobreakdownthehealthytissuesocaremustbetaken.Theuseofmoisturizers/emollientsandanadequateintakeofwater,daily,helptogivetheskinresilience(28).Simpleperiwoundskinprotectioncanbeobtainedbyusingbarrierwipes,creamsorsprays(11).Insomecases,exudatemanagementbags,hydrocolloiddressingsandpastesneedtobeusedtoensureadequateprotection.Totryandsimplifyallofthisinformation,achartthatplotstissuetype,exudatelevelsandthepresences/absenceofinfectioncanbeusedtohelpsummarizeoptions.Butremember,everypersonisdifferent,everywoundisdifferent,sousethisasaguideonly.Andifawounddoes

KimKaim 8/19/2016 Page16of31
notshowimprovementwithin2-4weeksofoptimumcare,doafullpatientre-assessmentandconsiderfurthercollaborationwithothers.
Investigation Dowehaveenoughinformationtounderstandtheunderlyingproblem(diagnosis)andcreateacomprehensivemanagementplan,ordoweneedmore?Examplesofinvestigationswecandoatthebesidearethingslikecheckingforthepresenceofpulsesandsensation.Getintothepractice(onhealthypatients)offindingbrachial,dorsalispedis,posteriortibialandpoplitealpulses.Wedon’ttendtousetheseoftensodon’tgetmuchpractice.Also,having,andknowinghowtouse,amonofilamentpenortuningforktodeterminesensationperceptionisveryuseful.Otherinvestigationsundertakenbythedoctorsincludepathologyandmedicalimaging.Youcanalwaysrecommendinvestigationsbedonewhendiscussingyourpatientwiththedoctor.Forexample,inawoundwithboneonview,itisreasonabletorecommendimagingforosteomyelitis.Inlegswithsignsofarterialorvenousdisease,itisreasonabletorecommendanABPI.Forthewoundbedthatisfriable,hasanoddorpearlytexture,especiallywherethepatienthasahistoryofskincancers,itisreasonabletorecommendabiopsy.Thedoctormayormaynotwishtoincludethisintheirplan,butatleastyouhavebroughtattentiontoapotentialproblem.RemembertouseyourSBARcommunicationskillswhenmakingtheserecommendations.
Diagnosis Weunderstandadiagnosistobetheidentificationofadiseaseormedicalconditionbyexaminationofthesigns,symptomsandanytestsperformed(29).Somediagnosesareobvious,likewhenthepatienthitstheirarmontherollatorandgetsaskintear.Thisisaskintear(withappropriateSTARcategory)secondarytotrauma.Wecanusuallyputadiagnosistotheacutewoundsandsomechronicwoundslikepressureinjuries.However,otherchronicwoundsthatarenothealingwithoptimumtreatmentmayeitherhavenodiagnosis,orthewrongone.Let’shaveanotherlookatthewomanwhohitherarmontherollator.Thewoundiscleaned,edgesre-apposed,anddressingwithcompressionapplied.Afterafewmonthsthewomanisseenagain,shestillhasasmallareathatappearstoheal,thengetsabitcrustyandstartsbleedingagain.Theareaisslightlyraisedcomparedtothesurroundingskin.Isthediagnosisofskintearstillappropriate?Orshouldtherebefurtherinvestigationstodeterminewhatishappeningatthecellularleveltostopthiswoundcompletelyhealing?Thisiswhereweneedtocollectasmuchinformationanddiscusstheneedforfurtherinvestigationsandpossiblyreferralwiththetreatingteam.Someexamplesofwounddiagnosesare:
• SkinTear(category1a,1b,2a,2bor3aspertheSTARclassificationsystem–seeAppendixB)
• PressureInjury(stageI,II,III,IV,mucosal,unstageable,orsuspecteddeeptissueinjuryaspertheNPUAPclassificationsystem–seeAppendixC)
• Surgical• DiabeticFootUlcer

KimKaim 8/19/2016 Page17of31
• VenousUlcer• ArterialUlcer• MixedVenous/ArterialUlcer• Cancer(SCC,BCC,solarkeratosis,melanoma,andmanyothers)• Vasculitis• PyodermaGangrenosum• Toomanydermatologicalconditionstomention!
Theimportantthingtorememberisthatweneedtoknowwhatitistobeabletocreatethemostappropriatecareplan.Failuretocorrectlydiagnoseawoundtypemayresultinfailedmanagementandwastedresources.Interventionsbasedonaccuratediagnosisdeliversbenefitstopatients,healthcaresystemsandsociety(30).Let’slookatthepersonwithchestpainthatwesenthome.What’sgoingtohappen?Isthepaingoingtocomeback?Getworse?Thispatientislikelytore-presenttohospitaltimeandtimeagainwiththesamesymptoms,orworse.Theunderlyingcondition(whateveriscausingtheinfarct)isnotlikelytoimprovebyitselfandwillgenerallyfollowadeterioratingcourse.Sonowlet’slookatapersonwithaninfectedulcer.It’sbeenthereawhile,theantibioticsreducetherednessandswellingandthewoundappearstostarthealing,butithasdonethisbefore,andwilldoitagain.Why?Wehavenodiagnosissowedon’tknowwhy.Becausewehavenottreatedthecausewehavewastedtimeandresourcesandthepersonwiththewoundhastocontinuetolivewithitandbearthecosts,everyday.Whatifthediagnosisofthewoundisasquamouscellcarcinomaorperipheralvenousdisease?Weneedadiagnosistoensurethewoundisadequatelymanagedandallcontributoryfactorsareaddressed(29,31).Asoursocietycontinuestoage,andlifestylediseasescontinuetoincrease,theproblemofpressureinjuriesanddiabeticulcersisgrowing.Theseandothercommontypesofchronicwoundswillrequireaccurateandconcisediagnosisandappropriatetreatmentaspartofholisticcare(2).
Implementation Onceyouhavecollectedyourhistory,doneyourexamination,completedanyotherinvestigationsanddeterminedthewounddiagnosis,youwillbereadytoputtogetheryourcomprehensivewoundcareplan.Inallofthesepreviousstepsyouwillhaveidentifiedriskstohealingorotherthingsthatwillimpactonhealingoryourcareplan.Forexample:History • Smoking
• HeartFailurewithFluidoverload
• Lossof10kginthelast2months
• Educationtoquitsmoking• Thetreatingteamwillbemanagingthefluidoverload,buttheconditionwillimpactonanyplansforcompression:compressionshiftsthefluidfromthelegsbackintocirculation,whichwillexacerbatethefluidoverloadproblem.
• Refertodieticianfornutritionalsupportinlightoftheextrarequirementsneededforwoundhealing
Examination >50%sloughHighexudateOedemaVaricoseveins,ankleflair,haemosiderinstainingPalpabledorsalispedis,warmfeet.
• debride• Managemoisture,preventperiwoundmaceration• Manageoedema
Investigation ABPI:Leftleg1,Rightleg1.1Longdurationofulcer(6years)and‘lumpy’tissueinpartofthewoundbase
• Legswilltoleratecompressionbutthereisstilltheproblemoffluidshifts.
• DiscusswiththetreatingteamtheneedtoruleoutMarjolin’sulcerviabiospy.
Diagnosis ?VenousLegUlcer Discusswiththetreatingteamtheneedforadiagnosisandplanforcompression.

KimKaim 8/19/2016 Page18of31
Collaboration Communication and collaboration inwound care is essential. Gottrup(32) refers to a studydoneinonehospitalinCopenhagenwheretheyfoundinthemajorityofcasesthat:
• Chronicwoundswerenothavingdiagnosticexaminations• Venouslegulcerswerenotreceivingcompressiontherapy• PatientswithfootulcerswerenotbeingassessedforDiabetesMellitus• Patientswithpressureulcerswerenothavingoff-loadingtreatment
Why?Didtheynothaveadiagnosisorwerethepeoplelookingafterthesepatientsmissingthenecessaryskills?Gottrupproposesthattoremedythisandprovideoptimumcareforthecomplexwoundcarepatient,careneedstobedeliveredbyteams,andnotindividuals.Whoare the collaborators thatmakeup these teams? Wementioned thepatient’s treatingteam,specialistsandalliedhealthabove. Whataboutthepatientandtheirfamily/carersorother support in thehome? Are they in anursinghome?For the complex, chronicwound,evidence tells us that we need a coordinated, multidisciplinary care team, includingparticipation fromat-home caregivers and thepatient, foroptimumresults. Specialist-leadadvancedcareisneededwhenthereisevidenceofischemia,inabilitytocomplywithwound-care regimens, suspected malignancy, and peripheral arterial disease(33). This is bestsupplemented with a member of the allied health care team (for example, occupationaltherapist,physicaltherapist,podiatrist,dietitian,socialworkerandsoon)(2).Howdoyouknowwhentorefer?Wheneveryouareindoubtregardingetiology,suspectedmalignancy,evidenceof ischemiaorwoundsthatdonotdemonstrateanadequateresponsetotreatment(33).Bygettingtherightpeopleinvolvedwecanallowforearlierdiagnosis,bettermanagement,andmayreducethecostoftreatingwounds(33).Withthelevelofcomplexityinthe patients we see, accurate wound diagnosis and development of successful treatmentsplanscanbequitechallenging(2).Butitcanbeequallyrewarding.
Assessment tools used in wound management Since1970wehaveknownthatastandardizedmethodformeasuringwoundhealingisneeded(34).Regularassessment,documentingprogressandassessingtheeffectivenessoftreatmentmaximizeshealingrates(35).Forchronicwounds,thosewoundswhichdonothealinatimelymanner,thebenefitsofusingastandardizedassessmenttoolcanbesignificant(36).Therearemanyfactors,systemic,regional,localandenvironmental,thatcanimpairwoundhealingandincreasetheriskofanacutewoundbecomingachronicwound(1).Thesystematicassessmentandcollectionofdataminimisesthisrisk(37).Whereassessmentsarenotperformedcorrectlythereistheriskofdelayedhealingandthepotentialforseriouscomplicationsassociatedwithlivingwithawoundforaprolongedperiodoftime(37).Notonlyarethererisksassociatedwithreducedskinbarrierfunction,suchasinfection,butthereisoftenpain,socialisolation,andpoorerqualityoflife(38,39).Delayedwoundhealingrequiresadditionalnursingandmedicalresources,highercostsofconsumablesinwoundcare,andpotentiallyhighercostsofhospitallengthsofstaytotreatcomplications(37).Theever-expandingmarketofdressingproductsonlyaddstoworsenthesituationwhenyoucombineapoorassessmentwithaninappropriateandexpensivedressingselection(34).Conversely,whereskilledcliniciansuseastandardizedframeworkwhichclearlyguidesNursesfromassessmentthroughtoimplementingandmonitoringwoundcareplansthatcorrectlyaddressthefactorsimpactingonwoundhealing,healingtimesarereduced,patientsufferingisreducedandtheoveralleconomicburdenisreduced(36-38).Byaddressingthesystemiccausesofwoundsandimpairedhealing,suchasreferralstovascularordermatologicalspecialists,

KimKaim 8/19/2016 Page19of31
thereisalsothepotentialforreducingtheriskoffuturewoundsoccurringorreducingtheirduration(40,41).Theidealwoundassessmenttool(WAT)willleadcliniciansfromassessmentanddiagnosisthroughtosettingclearhealingobjectivesandwoundcareplans.Itwillbegroundedinresearchandevidence,andfasttouseforcliniciansofallknowledgelevels(42-45).AWMAhascreatedasetofstandardsforwoundmanagement(46)inwhichtheyincluderecommendationsforassessment,planninganddocumentation.TheirrecommendationsaresummarizedinTable1.TherecommendationsfromtheAWMAstandardsadheretothisidealandcanbegroupedasinitialassessment(patienthistoryandsystemicobservations),optionalassessment(regionalobservationsandinvestigationsrelevanttowoundlocationandaetiology),ongoingassessment(woundbedandlocalarea)andcareplanning(managementplan,collaboration,documentationandevaluation)(46).TheserecommendationsareverybroadandAWMAdoesnotprovidespecificsonhowthisshouldbedone.TheserecommendationswerethebasisforaliteraturereviewinvestigatinganumberofwoundassessmenttoolsandhowtheycomparedtotheAWMAstandard.Youcanreadthisreviewinfullonmywebsite(http://woundcareresource.com/downloads/litreview-wat.pdf).ThereviewshowsthatnosingletoolencompassedallrecommendationsfromtheAWMAstandards,howevertheGCUHWCPcoveredmoreitemsthanthecomparisontools.ThiswasstilllessthanhalfofAWMA’stotalrecommendations.Whileallthereviewarticlesagreedthatcomprehensivewoundassessmentisneeded,suchacomprehensivetoolasoutlinedbyAWMAwouldnotbepractical,andwouldnotbeusedbyNurses.ThiswasreflectedintheauditoftheGCUHWCPwhere(onaverage)halfoftheitemsonthetoolwerenotcompleted.NursesmainlyusedtheWCPonlyasameanstorecordwhatdressingswereappliedtothewound.Arguably,thegreaternumberofassessmentitemsmeansthegreatertheabilitytodetectvariation(47)butalsothemoretimeconsumingtoadministerandthereforemorecostly(48).Themoderncareenvironmentisonewherenursesfindtheyhavemoreresponsibilities,lesstimeandhighstaffturnoverrates;allofwhicharebarrierstoensuringconsistentuseofaWAT(38,45,49).However,itisimportanttorememberthatcorrectcompletionoftheWATshowingevidencebaseddecisionmakingprocesseswhichareclear,consistent,andcoherentwillreducetheriskofpoorpracticeand,subsequently,theriskoflitigation(50).

KimKaim 8/19/2016 Page20of31
Table1Recommendationsforinclusioninawoundtool,modifiedfromAWMAstandardsInitialAssessment OngoingAssessment OptionalAssessment
whenindicatedCarePlanning
ReasonforPresentation
Woundtype/Aetiology Riskassessments(falls,skinintegrity)
Shortandlongtermgoals
HealthHistory Duration Vascularassessment ManagementPlantooptimizewoundhealingpotential
Age Location Sensoryassessment Individualandcarerpreference,abilityandwillingnesstoparticipate
Previouswoundhistoryandoutcome
Dimensions Nutritionalassessment Evidenceofinter-professionalcommunicationandcare
Medicationhistory Woundbedcharacteristics(tissuetypeandforeignbodies)
Psychologicalassessment
Comprehensiveandchronologicaldocumentation
Psychosocialimplicationsresultingfromwounding
Woundedgesappearance Medicalimaging Effectiveness
Nutritionalstatus Peri-woundappearance Pathology Increaseawarenessofhealthylifestylechoices
Sensitivitiesandallergies Exudate PromoteactivityandmobilityactivitiesRelevantdiagnosticsandinvestigations
Odour
Painassessment Inflammation/Infection Vitalsigns WoundPain Individual’sperceptionsofwoundhealinggoals

KimKaim 8/19/2016 Page21of31
The digital age Collectionofinformationinthedigitalagehasallowedustoaccessthedataeasier,toquicklydeterminetrendsinhealing,ortousetheinformationforresearch(forexample,assessingindicatorsofpotentialvenuslegulcerrecurrence(51)).Theinternetprovidesuswithawealthofwoundmanagementinformation,someexcellent(WoundsInternational,WorldWideWounds)andsomewhichare,welllet’ssay,notpeerreviewed…WithinourhealthcaresettingsthemajorityofourWATsarestillpaper-basedandwecontinuetomeasurewithdisposablerulers.However,thedigitalageisencroachingonwoundcare.Inmyopinion,themostsignificantofthesehasbeentheintroductionofthedigitalcamera.Beingabletoquickly,easilyandaccuratelyrecordtheprogressofawoundthroughtheseimageshasbeenincrediblyhelpful,increasingobjectivityintemporalassessment.Woundmeasurementisalsoahotlydebatedtopicas,overtheyears,eachnewtechnologyhaspromisedtobecomethegoldstandardforwoundmeasurement(um,no,westilldon’thaveone).Theproblembeing,itisquickandeasytomeasureawoundwitharulerortraceitonaruledpieceofacetateandcountthesquares.Thesetoolsarecheapandeasytohavehandy.3Dcamerasandthesoftwaretorunthem,digitalplanimetrydevicesandtheirconsumables,allhavehighcostsandtaketimetolearn.Whilestudieshaveshownthattheaccuracyofthesemoreexpensivedevicesisgreaterthanthatofthestandardrulermeasurements(52),thequestionis–howaccuratedoyouneedthemeasurementtobe?Inter-raterandintra-raterreliabilityhasregularlybeenshowntobehighforsimplemeasurementssuchasthosewitharuler.Howevertherulermeasurementitselfhasbeenproventoconsistentlyover-estimatethewoundsize(53).Sodoesitmatterifthesizeisconsistentlyover-estimatedintheclinicalsetting?Itwillstillshowatrend,whichiswhatisrequiredtoassistinclinicaldecision-making.Butnowwecometothepointintimewhereeveryonehasacamera,andthesoftwarethatcanbeusedtocalculatethewoundsizeiseitherverycheap(MOWA)orfree(ImageJ).Whilesomeofthepitfallsofwoundphotographywillbementionedshortly,Ithinkthatitissafetosaythatwiththeaccuracyandnon-contactnatureoftakingthephoto(4),theminimalexpenserequired,thetech-savvynatureofnursesandspeedofmeasurement,thistypeofwoundmeasurementwillincreaseinclinicaluse.

KimKaim 8/19/2016 Page22of31
Appendix A – Student Assessment Tool History
• What is the complaint?
• How long has it existed?
• What has been done about the complaint so far?
• Medical History
• Surgical History
• Medications
• Social History
• Ever Smoked
• Alcohol Intake
• Mobility
• Allergies
• Diet
Examination
• Systemic
• Regional
• Local Location
Size
o Tissue
o Inflammation
o Moisture
o Edges

KimKaim 8/19/2016 Page23of31
Investigations
Diagnosis
Intervention
Cleansing
Emollient/Barrier
Primary Dressing
Secondary Dressing
Retention/Compression
Dressing change frequency
Review:

KimKaim 8/19/2016 Page24of31
Appendix B –STAR Skin Tear Classification

KimKaim 8/19/2016 Page25of31

KimKaim 8/19/2016 Page26of31
Appendix C – Pressure Injury Classifications
Category/StageI:Non-blanchablerednessofintactskinIntactskinwithnon-blanchableerythemaofalocalizedareausuallyoverabonyprominence.Discolorationoftheskin,warmth,edema,hardnessorpainmayalsobepresent.Darklypigmentedskinmaynothavevisibleblanching.Furtherdescription:Theareamaybepainful,firm,soft,warmerorcoolerascomparedtoadjacenttissue.Category/StageImaybedifficulttodetectinindividualswithdarkskintones.Mayindicate“atrisk”persons.
Category/StageII:PartialthicknessskinlossorblisterPartialthicknesslossofdermispresentingasashallowopenulcerwitharedpinkwoundbed,withoutslough.Mayalsopresentasanintactoropen/rupturedserum-filledorsero-sanginousfilledblister.Furtherdescription:Presentsasashinyordryshallowulcerwithoutsloughorbruising.Thiscategory/stageshouldnotbeusedtodescribeskintears,tapeburns,incontinenceassociateddermatitis,macerationorexcoriation.

KimKaim 8/19/2016 Page27of31
Category/StageIII:Fullthicknessskinloss(fatvisible)Fullthicknesstissueloss.Subcutaneousfatmaybevisiblebutbone,tendonormusclearenotexposed.Somesloughmaybepresent.Mayincludeunderminingandtunneling.Furtherdescription:ThedepthofaCategory/StageIIIpressureulcervariesbyanatomicallocation.Thebridgeofthenose,ear,occiputandmalleolusdonothave(adipose)subcutaneoustissueandCategory/StageIIIulcerscanbeshallow.Incontrast,areasofsignificantadipositycandevelopextremelydeepCategory/StageIIIpressureulcers.Bone/tendonisnotvisibleordirectlypalpable.
Category/StageIV:Fullthicknesstissueloss(muscle/bonevisible)Fullthicknesstissuelosswithexposedbone,tendonormuscle.Sloughorescharmaybepresent.Oftenincludeunderminingandtunneling.Furtherdescription:ThedepthofaCategory/StageIVpressureulcervariesbyanatomicallocation.Thebridgeofthenose,ear,occiputandmalleolusdonothave(adipose)subcutaneoustissueandtheseulcerscanbeshallow.Category/StageIVulcerscanextendintomuscleand/orsupportingstructures(e.g.,fascia,tendonorjointcapsule)makingosteomyelitisorosteitislikelytooccur.Exposedbone/muscleisvisibleordirectlypalpable.

KimKaim 8/19/2016 Page28of31
Unstageable/Unclassified:Fullthicknessskinortissueloss–depthunknownFullthicknesstissuelossinwhichactualdepthoftheulceriscompletelyobscuredbyslough(yellow,tan,gray,greenorbrown)and/oreschar(tan,brownorblack)inthewoundbed.Furtherdescription:Untilenoughsloughand/orescharareremovedtoexposethebaseofthewound,thetruedepthcannotbedetermined;butitwillbeeitheraCategory/StageIIIorIV.Stable(dry,adherent,intactwithouterythemaorfluctuance)escharontheheelsservesas“thebody’snatural(biological)cover”andshouldnotberemoved.
SuspectedDeepTissueInjury-depthunknownPurpleormaroonlocalizedareaofdiscoloredintactskinorblood-filledblisterduetodamageofunderlyingsofttissuefrompressureand/orshear.Furtherdescription:Theareamaybeprecededbytissuethatispainful,firm,mushy,boggy,warmerorcoolerascomparedtoadjacenttissue.Deeptissueinjurymaybedifficulttodetectinindividualswithdarkskintones.Evolutionmayincludeathinblisteroveradarkwoundbed.Thewoundmayfurtherevolveandbecomecoveredbythineschar.Evolutionmayberapidexposingadditionallayersoftissueevenwithtreatment.InformationfromTheAustralianWoundManagementAssociation(AWMA)PanPacificGuidelineDevelopmentSteeringCommitteeandtheEuropeanPressureUlcerAdvisoryPanel/NationalPressureUlcerAdvisoryPanel.(54,55)

KimKaim 8/19/2016 Page29of31
References 1. Harding,K.,etal.,EvolutionorRevolution?Adaptingtocomplexityinwound
management.InternationalWoundJournal,2007.4Suppl.2(2):p.1-12.2. Sibbald,R.G.,etal.,Specialconsiderationsinwoundbedpreparation2011:anupdate.
WorldCouncilofEnterostomalTherapistsJournal,2012.32(2):p.10-30.3. Grey,J.E.,S.Enoch,andK.Harding,ABCofWoundHealing:WoundAssessment.British
MedicalJournal,2006.332:p.285-288.4. Chang,A.C.,B.Dearman,andJ.E.Greenwood,Acomparisonofwoundareameasurement
techniques:Visitrackversusphotography.ePlasty,2011.11:p.158-166.5. Bilgin,M.andÜ.Y.Güneş,AComparisonof3WoundMeasurementTechniques.Journalof
Wound,Ostomy&ContinenceNursing,2013.40(6):p.590-593.6. Dowsett,C.andE.Ayello,TIMEprinciplesofchronicwoundbedpreparationand
treatment.BritishJournalofNursing,2004.13(15):p.S16.7. O'Brien,M.,Debridement:ethical,legalandpracticalconsiderations.WoundCare,2003.
March:p.23-25.8. unkown,Debridementinwoundcare.WoundEssentials,2011.6:p.88-89.9. Anderson,I.,Debridementmethodsinwoundcare.NursingStandard,2006.20(24):p.
65-72.10. Benbow,M.,Fungatingmalignantwoundsandtheirmanagement.Journalof
CommunityNursing,2009.23(11):p.12.11. Bradbury,S.andJ.Fletcher,Prontosanmadeeasy.WoundsInternational,2011.2(2):p.
s25-s30.12. Vowden,K.andP.Vowden,Debridementmadeeasy.WoundsUK,2011.7(4):p.1-4.13. Cooper,R.A.,UnderstandingWoundInfection,inEuropeanWoundManagement
Association(EWMA)PositionDocument:IdentifiyingCriteriaforWoundInfection,S.Caine,etal.,Editors.2005,MEPLtd:London.
14. Percival,S.L.andS.E.Dowd,Chapter6.TheMicrobiologyofWounds,inMicrobiologyofWounds,S.PercivalandK.Cutting,Editors.2010,CRCPress:BocaRaton,Fla.
15. LiesseIyamba,J.M.,etal.,StudyoftheformationofabiofilmbyclinicalstrainsofStaphylococcusaureus.Biofouling,2011.27(8):p.811-821.
16. Davis,S.C.,etal.,Microscopicandphysiologicevidenceforbiofilm-associatedwoundcolonizationinvivo.WoundRepairAndRegeneration,2008.16(1):p.23-29.
17. Jefferson,K.K.,Whatdrivesbacteriatoproduceabiofilm?FEMSMicrobiologyLetters,2004.236(2):p.163-173.
18. Mastropaolo,M.D.,etal.,Synergyinpolymicrobialinfectionsinamousemodeloftype2diabetes.InfectionAndImmunity,2005.73(9):p.6055-6063.
19. Pollock,A.V.,Woundinfection:synergybetweenaerobicandanaerobicbacteria.AnnalsOfTheRoyalCollegeOfSurgeonsOfEngland,1980.62(3):p.243-244.
20. Fazli,M.,etal.,NonrandomdistributionofPseudomonasaeruginosaandStaphylococcusaureusinchronicwounds.JournalOfClinicalMicrobiology,2009.47(12):p.4084-4089.
21. Richard,J.-L.,J.-P.Lavigne,andA.Sotto,Diabetesandfootinfection:morethandoubletrouble.Diabetes/MetabolismResearchandReviews,2012.28:p.46-53.
22. Edmonds,M.,A.V.M.Foster,andP.Vowden,Woundbedpreparationfordiabeticfootulcers,inEuropeanWoundManagementAssociation(EWMA)PositionDocument:WoundBedPreparationinPractice2004,MEPLtd:London.
23. Sibbald,R.G.,K.Woo,andE.A.Ayello,Increasedbacterialburdenandinfection:thestoryofNERDSandSTONES.AdvancesinSkin&WoundCare,2006.19(8):p.447-461.
24. Dowsett,C.,Moistureinwoundhealing:exudatemanagement.BritishJournalofCommunityNursing,2011:p.S6-s12.

KimKaim 8/19/2016 Page30of31
25. Moore,K.,CellBiologyofNormalandImpairedHealing,inMicrobiologyofWounds,S.PercivalandK.Cutting,Editors.2010,CRCPress:BocaRaton,Fla.p.151-186.
26. Strecker-McGraw,M.K.,T.R.Jones,andD.G.Baer,Softtissuewoundsandprinciplesofhealing.EmergencymedicineclinicsofNorthAmerica,2007.25(1):p.1-22.
27. Vowden,K.andP.Vowden.WoundBedPreparation.2002;Availablefrom:http://www.worldwidewounds.com/2002/april/Vowden/Wound-Bed-Preparation.html.
28. Carville,K.,WoundCareManual.5thed2007,OsbornPark,WA:SilverChainNursingAssociation.
29. WorldUnionofWoundHealingSocieties(WUWHS),Principlesofbestpractice:Diagnosticsandwounds.Aconsensusdocument.2008,London:MEPLtd.
30. Inernationalconsensus,Makingthecaseforcosteffectivewoundmanagement.WoundsInternational,2013.
31. Casey,G.,Chronicwoundhealing:Legulcers.KaiTiakiNursingNewZealand,2011.17(11):p.24-29.
32. Gottrup,F.,Aspecialisedwoundcareconcept:Themulti-disciplinaryapproach.TheChronical,2009.26(Spring2009):p.5-6.
33. OptimalCareofChronic,Non-Healing,LowerExtremityWounds:AReviewofClinicalEvidenceandGuidelines,2013,CanadianAgencyforDrugsandTechnologiesinHealth.
34. Cooper,D.M.,Humanwoundassessment:statusreportandimplicationsforclinicians.AACNClinicalIssuesinCriticalCareNursing,1990.1(3):p.553-565.
35. Ferrell,B.A.,TheSessingScaleformeasurementofpressureulcerhealing.AdvancesInWoundCare:TheJournalForPreventionAndHealing,1997.10(5):p.78-80.
36. Fletcher,J.,WoundassessmentandtheTIMEframework.BritishJournalofNursing,2007.16(8):p.462-4.
37. Greatrex-White,S.andH.Moxey,Woundassessmenttoolsandnurses'needs:anevaluationstudy.InternationalWoundJournal,2013.
38. Cook,L.,Woundassessment:exploringcompetencyandcurrentpractice.BritishJournalofCommunityNursing,2011:p.S34-40.
39. Moffatt,C.,etal.,Psychosocialfactorsanddelayedhealing,inPositionDocument:Hard-to-healwounds:aholisticapproach,EuropeanWoundManagementAssociation,Editor2008,MEPLtd:London.p.10-14.
40. Martin,F.andA.Duffy,Assessingandmanagingvenouslegulcersinthecommunity:areview.BritishJournalofCommunityNursing,2011:p.S6-s14.
41. Muir,C.andL.Watret,Managingwoundsusingastructuredassessmenttool.JournalofCommunityNursing,2006.20(1):p.10.
42. Kennedy,C.andD.Arundel,Districtnurses'knowledgeandpracticeofwoundassessment:2.BritishJournalOfNursing(MarkAllenPublishing),1998.7(8):p.481-486.
43. Hess,C.T.,Theartofskinandwoundcaredocumentation.AdvancesinSkin&WoundCare,2005.18(1):p.43-55.
44. Gray,D.,etal.,Usingthewoundhealingcontinuumtoidentifytreatmentobjectives,inAppliedwoundmanagmentsupplement.Part2Implementation,D.Gray,R.White,andP.Cooper,Editors.2005,Wounds-UK:Aberdeen.
45. BestPracticeStatement:Optimisingwoundcare.WoundsUK,2008.46. AustralianWoundMangementAssociation,StandardsforWoundManagement.2nd
ed2010:AustralianWoundMangementAssociation.31.47. Matsui,Y.,etal.,DevelopmentoftheDESIGN-Rwithanobservationalstudy:Anabsolute
evaluationtoolformonitoringpressureulcerwoundhealing.WoundRepair&Regeneration,2011.19(3):p.309-315.

KimKaim 8/19/2016 Page31of31
48. Barber,S.,Aclinicallyrelevantwoundassessmentmethodtomonitorhealingprogression.Ostomy/WoundManagement,2008.54(3):p.42-49.
49. Maklebust,J.,PUSHtoolrealitycheck:audienceresponse...proceedingsoftheNationalPressureUlcerAdvisoryPanel,FifthNationalConference,"MonitoringPressureUlcerHealing:anAlternativetoReverseStaging".AdvancesinWoundCare,1997.10(5):p.102-106.
50. Gray,D.,etal.,Appliedwoundmanagement,inAppliedwoundmanagementsupplement,D.Gray,Editor2004,Wounds-UK:Aberdeen.
51. Finlayson,K.,H.Edwards,andM.Courtney,Relationshipsbetweenpreventiveactivities,psychosocialfactorsandrecurrenceofvenouslegulcers:aprospectivestudy.JournalofAdvancedNursing,2011.67(10):p.2180-2190.
52. Fette,A.M.Aclinimetricanalysisofwoundmeasurementtools.WorldWideWounds,2006.
53. Brown,D.,Comparingdifferentulcermeasurementtechniques:apilotstudy.PrimaryIntention,2003.11(3):p.125-134.
54. TheAustralianWoundManagementAssociation(AWMA)PanPacificGuidelineDevelopmentSteeringCommittee,PanPacificClinicalPracticeGuidelineforthePreventionandManagementofPressureInjury.2012,OsbornePark,WA:CambridgeMedia.
55. EuropeanPressureUlcerAdvisoryPanelandNationalPressureUlcerAdvisoryPanel,Treatmentofpressureulcers:QuickReferenceGuide2009,WashingtonDC:NationalPressureUlcerAdvisoryPanel.