Embed Size (px)
Citation preview
World Vision Working with
the Global Fund
Annual Report 2013

WV Working with the Global Fund 2013
1 EMPOWER, EQUIP, ADVOCATE
World Vision Working with the Global Fund 2013 Annual Report
1. Introduction
In 2013, World Vision expenditure for health programming from the Global Fund to Fight AIDS, TB and malaria
(the Global Fund) was $37 million.1 This financing institution is among the top three cash grant donors to
World Vision for all sectors and second only to the US government in grants for health. Three grants from
the Global Fund also were among the ten largest grants awarded to World Vision in 2013. Most important,
however, is the increasing number of people in World Vision communities who received life-saving prevention
and treatment for HIV and AIDS, TB and malaria due to our partnership with the Global Fund. These include
nearly 30,000 children who received care and treatment for AIDS in six countries, distribution of more than
3,300,000 insecticide-treated bed nets in three countries, and 34,000 patients enrolled in treatment in 10
countries for tuberculosis.
II. 2013 Global Fund Portfolio Overview
Current Portfolio - At the end of calendar year 2013, WV was implementing 28 grants for malaria, TB or HIV
and AIDS in 22 countries (five countries had multiple grants). These have a multi-year (1 - 3 years) value of
US$111,637,2902 and were leveraged by Support Offices for $4,018,907 in match, for a total current portfolio
value of $115,656 198. See the full list of current grants in Appendix 1.
World Vision Global Fund Portfolio Summary - December 31, 2013
# Awards Grant value
(USD)
Match value
(USD)
Total (USD)
Cumulative Grant Portfolio (total
of current +closed grants) 99 281,702,031 12,515,052 294,217,083
Current Grants (active phases) 28 111,637,290 4,018,907 115,656,198
Closed Grants 71 170,064,741 8,496,145 178,560,885
Pipeline (Additional Board
approved phases 2014-2016) 0 0 0 0
Acquisition
Total New Proposals 7
37,960,157
4,246,171
42,206,328
Newly signed awards (wins) 2
9,831,616
1,429,855
11,261,471
Pending (verbal approval, in negotiation) 1
1,000,000 1,000,000
Proposals (response pending) 1
155,000
27,000
182,000
Losses 3
26,973,541
2,789,316
29,762,857
1 GAM Report Q4 (year-end) FY13 January 2014, Global Field Operations Support Team, WVI
2 All $ values in this report refers to US dollars unless otherwise noted.

WV Working with the Global Fund 2013
2 EMPOWER, EQUIP, ADVOCATE
Acquisitions - During the calendar year there were seven new proposals (Burundi, Malawi, South Africa,
Sudan, Zimbabwe, Zambia and an extension in Papua New Guinea) totaling $37.9 million. Of these, two were
awarded (Zambia and PNG) for $9,831,616 with match from WV SOs of $1,429,855. The Sudan proposal was
verbally approved but is still in negotiation and the Malawi proposal is still pending a response from the donor.
The other three proposals were not approved.
Match - Cost share or match is not required in Global Fund grants, and not every grant has a Support Office to
provide match. Nevertheless, there has been a strong effort by the Global Centre to engage Support Offices to
assist with risk leveling and unallocated support costs. Support Office match was equal to 3.6 percent of the
current 2013 portfolio. In the current portfolio, the average match per grant by region was as follows: LAC
24%, East Asia 1.9%, East Africa 0.9%, Southern Africa 3%, MEER 10.8%, SAP 8.4% and WAR 16.9%.
Trends in Portfolio Growth
The cumulative portfolio value (chart 1) has
leveled out from 2011 and actually declined in 2013
for two main reasons. For three years, the new
awards and extensions have been smaller than the
value of grants ending, resulting in slowed growth.
Also, since 2011 our internal reporting has
improved and as every grant or phase closed we
began reporting the actual final grant value which is
usually less than the originally recorded award value
due to underspending during implementation. The
2013 level is a new, more accurate baseline.
The current portfolio (chart 2) includes multi-year
value of only active grants. The current grant portfolio
value declined steeply in 2011 as older major grants
closed and the Global Fund discontinued global Calls for
Proposals. The current portfolio stabilized somewhat
this year due to the signing of some large phase 2
renewals on top of acquisitions. All current grants with
Board approved five year amounts had signed phase 2
or extension by the end of the year so there are no
Board-approved future phases in the pipeline (chart 3).
Grant closures continued to outpace new grants in
2013 in number and total value (chart 3). From 2011-
2013, there has been very limited new funding for
grants from the Global Fund, which is the reason for
the decline in acquisitions, proposals and pipeline.
This situation is expected to improve in 2014 with the
$ M
$100 M
$200 M
$300 M
$400 M
2008 2009 2010 2011 2012 2013
1. Cumulative Portfolio 2008-2013
match
grant
-40%
-20%
0%
20%
40%
$ M
$50 M
$100 M
$150 M
$200 M
20
09
20
10
20
11
20
12
20
13
2. Current Portfolio 2009-2013
and growth rate
current
growth rate
0
50
100
150
200
250
300
$ M
illio
ns
3. Portfolio Trends-Annual Amount
cumulative
closed
current
pending&pipeline
WV Working with the Global Fund 2013
3 EMPOWER, EQUIP, ADVOCATE
launch of the New Funding Model and a new replenishment.
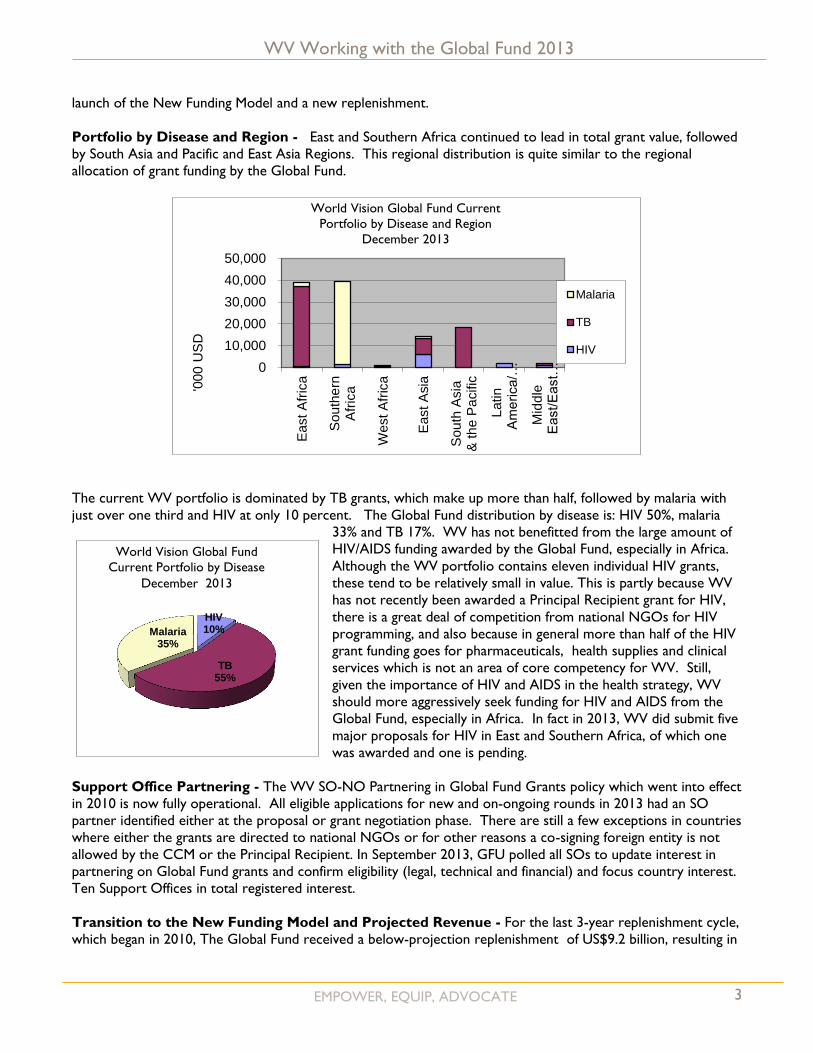
Portfolio by Disease and Region - East and Southern Africa continued to lead in total grant value, followed
by South Asia and Pacific and East Asia Regions. This regional distribution is quite similar to the regional
allocation of grant funding by the Global Fund.
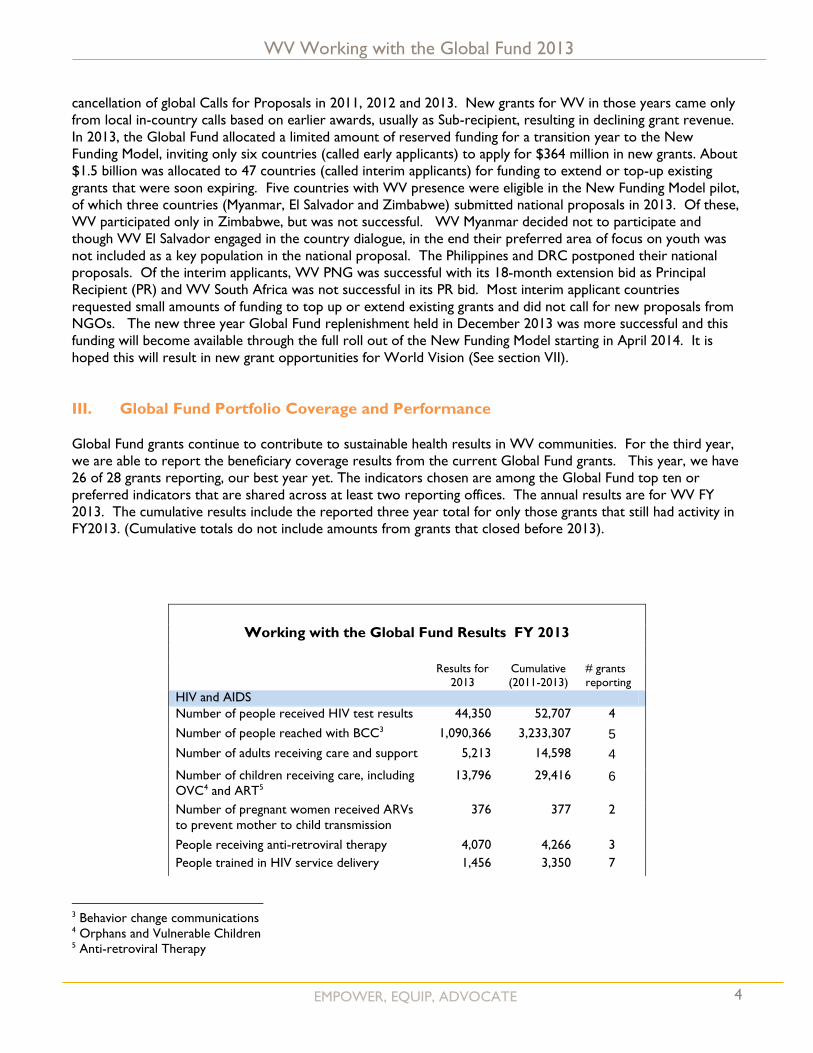
The current WV portfolio is dominated by TB grants, which make up more than half, followed by malaria with
just over one third and HIV at only 10 percent. The Global Fund distribution by disease is: HIV 50%, malaria
33% and TB 17%. WV has not benefitted from the large amount of
HIV/AIDS funding awarded by the Global Fund, especially in Africa.
Although the WV portfolio contains eleven individual HIV grants,
these tend to be relatively small in value. This is partly because WV
has not recently been awarded a Principal Recipient grant for HIV,
there is a great deal of competition from national NGOs for HIV
programming, and also because in general more than half of the HIV
grant funding goes for pharmaceuticals, health supplies and clinical
services which is not an area of core competency for WV. Still,
given the importance of HIV and AIDS in the health strategy, WV
should more aggressively seek funding for HIV and AIDS from the
Global Fund, especially in Africa. In fact in 2013, WV did submit five
major proposals for HIV in East and Southern Africa, of which one
was awarded and one is pending.
Support Office Partnering - The WV SO-NO Partnering in Global Fund Grants policy which went into effect
in 2010 is now fully operational. All eligible applications for new and on-ongoing rounds in 2013 had an SO
partner identified either at the proposal or grant negotiation phase. There are still a few exceptions in countries
where either the grants are directed to national NGOs or for other reasons a co-signing foreign entity is not
allowed by the CCM or the Principal Recipient. In September 2013, GFU polled all SOs to update interest in
partnering on Global Fund grants and confirm eligibility (legal, technical and financial) and focus country interest.
Ten Support Offices in total registered interest.
Transition to the New Funding Model and Projected Revenue - For the last 3-year replenishment cycle,
which began in 2010, The Global Fund received a below-projection replenishment of US$9.2 billion, resulting in
0
10,000
20,000
30,000
40,000
50,000
East
Afr
ica
Sou
the
rnA
fric
a
West A
fric
a
East
Asia
Sou
th A
sia
& th
e P
acific
Latin
America/…
Mid
dle
East/East…
'000 U
SD
World Vision Global Fund Current
Portfolio by Disease and Region
December 2013
Malaria
TB
HIV
HIV 10%
TB 55%
Malaria 35%
World Vision Global Fund
Current Portfolio by Disease
December 2013
WV Working with the Global Fund 2013
4 EMPOWER, EQUIP, ADVOCATE
cancellation of global Calls for Proposals in 2011, 2012 and 2013. New grants for WV in those years came only
from local in-country calls based on earlier awards, usually as Sub-recipient, resulting in declining grant revenue.
In 2013, the Global Fund allocated a limited amount of reserved funding for a transition year to the New
Funding Model, inviting only six countries (called early applicants) to apply for $364 million in new grants. About
$1.5 billion was allocated to 47 countries (called interim applicants) for funding to extend or top-up existing
grants that were soon expiring. Five countries with WV presence were eligible in the New Funding Model pilot,
of which three countries (Myanmar, El Salvador and Zimbabwe) submitted national proposals in 2013. Of these,
WV participated only in Zimbabwe, but was not successful. WV Myanmar decided not to participate and
though WV El Salvador engaged in the country dialogue, in the end their preferred area of focus on youth was
not included as a key population in the national proposal. The Philippines and DRC postponed their national
proposals. Of the interim applicants, WV PNG was successful with its 18-month extension bid as Principal
Recipient (PR) and WV South Africa was not successful in its PR bid. Most interim applicant countries
requested small amounts of funding to top up or extend existing grants and did not call for new proposals from
NGOs. The new three year Global Fund replenishment held in December 2013 was more successful and this
funding will become available through the full roll out of the New Funding Model starting in April 2014. It is
hoped this will result in new grant opportunities for World Vision (See section VII).
III. Global Fund Portfolio Coverage and Performance
Global Fund grants continue to contribute to sustainable health results in WV communities. For the third year,
we are able to report the beneficiary coverage results from the current Global Fund grants. This year, we have
26 of 28 grants reporting, our best year yet. The indicators chosen are among the Global Fund top ten or
preferred indicators that are shared across at least two reporting offices. The annual results are for WV FY
2013. The cumulative results include the reported three year total for only those grants that still had activity in
FY2013. (Cumulative totals do not include amounts from grants that closed before 2013).
Working with the Global Fund Results FY 2013
Results for
2013
Cumulative
(2011-2013)
# grants
reporting
HIV and AIDS
Number of people received HIV test results 44,350 52,707 4
Number of people reached with BCC3 1,090,366 3,233,307 5
Number of adults receiving care and support 5,213 14,598 4
Number of children receiving care, including
OVC4 and ART5
13,796 29,416 6
Number of pregnant women received ARVs
to prevent mother to child transmission
376 377 2
People receiving anti-retroviral therapy 4,070 4,266 3
People trained in HIV service delivery 1,456 3,350 7
3 Behavior change communications 4 Orphans and Vulnerable Children 5 Anti-retroviral Therapy

WV Working with the Global Fund 2013
5 EMPOWER, EQUIP, ADVOCATE
Community groups formed for HIV care and
support
143 279 3
Tuberculosis
Number of new TB patients detected 27,158 54,292 7
Number of patients enrolled in DOTS6 21,710 34,751 10
People trained in improved TB service
delivery
10,834 42,783 10
TB service points supported 184 223 5
Malaria
Number of insecticide treated nets
distributed
1,818,503 3,361,345 3
Number of people trained in malaria service
including CHW7
10,119 20,589 4
Number malaria service delivery points
supported
81 353 3
Number of people with fever receiving
antimalarial treatment according to policy
128,885 130,243 2
IV. Partnership and Advocacy
Inter-Organization Task Team (IOTT) and Civil Society Principal Recipient Network (CSPRN) -
WV was invited to join the IOTT on Community Systems Strengthening (CSS) established by the Global Fund to
provide advice on the CSS investment case. Representing the CSPRN, WV facilitated the review and feedback
on the Investment Guide to Health and Community Systems Strengthening (HCSS) in January 2013. The HCSS
guide was made part of the Global Fund’s Transitional Funding Mechanism guidance package issued in early 2013
and later was made part of the Health System Strengthening (HSS) guidance package. In addition, WV has
facilitated the review and feedback on the CSS Investment Module and the CSS Informational Note in support of
the Global Fund’s New Funding Model.
WV also planned and facilitated a conference call on CSS and civil society engagement with the Global Fund as
part of CSPRN in January 2013. Mauro Guarinieri, from the civil society office of the Global Fund Secretariat,
was the guest speaker at this call. WV also led a core group project to revise the ToR of the CSPRN to focus
more on influencing the Global Fund strategy, reforms and the New Funding Model.
Resources and Advocacy Working Group of Ecumenical Advocacy Alliance (RAWG/EAA) – WV
and six other faith-based NGOs met with the new incoming Executive Director of the Global Fund, Amb. Mark
Dybul, to discuss a more consistent engagement of faith-based organizations (FBOs) in the New Funding Model
(NFM). As a follow up, RAWG/EAA contributed the names of FBOs in the Global Fund NFM countries that
should be invited to the country dialogue including WV national offices. In addition, RAWG/EAA was invited to
submit and WV contributed content about FBO organizational culture and capabilities for a training programme
for the Global Fund portfolio managers. This was in response to evidence that since the 2012 restructuring of
the Global Fund, many new staff do not understand the extensive role of FBOs in health service delivery or their
constraints to participation in Global Fund programs.
The EAA/RAWG also submitted to the Global Fund the report of its survey of FBO participation in Country
Coordinating Mechanisms (CCM) which found that 80 percent of CCM’s have at least one member from an
6 Directly observed treatment short-course 7 Community Health Workers

WV Working with the Global Fund 2013
6 EMPOWER, EQUIP, ADVOCATE
FBO and 70 percent of FBO members of CCMs are satisfied that they have an effective voice on the CCM. Yet
a majority of respondents (86 percent) expressed challenges such as lack of funding for FBOs, a need for skills in
monitoring and evaluation and Global Fund compliance, communications difficulties, weakness in grant
implementation, competency of faith leaders on technical health issues, a gap in collaboration between
government and civil society sectors, funding delays, and the expenses associated with attending CCM meetings.
Respondents expressed a strong interest in establishing network of FBOs engaged in the Global Fund to
strengthen learning, effectiveness and voice. EAA/RAWG is planning how to respond.
V. Global Fund Unit Strategic Support
Capacity Building and Knowledge Management - The Global Fund Unit (GFU) continued to be the
central hub for capacity building and knowledge management related to the Global Fund engagement, acquisition
and compliance, providing the following services:
Orientation conference calls and/or channeled information and resources to EASO, WARO, WVUK,
WV Australia, Ghana, Chad, Zimbabwe, and Uganda.
Direct technical support, advice and review for proposals from Sudan, Malawi, Burundi, Papua New
Guinea, Zimbabwe, and South Africa.
Quarterly webex conferences for information sharing with the ever growing Global Fund Interest
Group (GFIG). Topics focused on the GF’s New Funding Model, major board decisions and lessons
learned from implementing grants. WV Mozambique, Dominican Republic, Myanmar, PNG, Rwanda and
Thailand all contributed to webex calls during the year. The GFIG page on WVcentral was enhanced in
look and content and postings, announcements and emails were used to digest and highlight new
guidance and announcements. The GFIG’s Document Library was used as a model for other IGs.
The GFIG listserv rose from 190 to 336 (45% increase from 2012 and the largest Interest Group after
CHN) as a result of a Health Community of Practice (CoP) survey which assessed the level of interest in
the Interest Group (IG). The GFIG page experienced the highest page hits of all Health CoP IGs (the 7th
highest hits on WVCentral in general) and the member satisfaction survey yielded a score of 3.7 out of
5.0 (second highest of all CoP IGs).
Conducted a Global Fund and European Community Grant Acquisition and Management workshop at
the invitation of SAPO. The five day workshop was conducted in Jakarta for over 30 participants from
NOs in the region interested in acquiring or already implementing Global Fund grants.
Pre-positioning for the New Funding Model
During the first part of 2013, the GFU team focused on disseminating information and guidance about
the Global Fund New Funding Model and details of the transition year which began on 28 February. The
team worked closely with the five WV offices in the early applicant countries and many more in the
interim countries to advise on engagement, decision-making and ultimately with the proposals in three
countries.
In October 2013, the GFU team launched a global pre-positioning campaign to identify the national
offices that plan to prepare for proposals under the New Funding Model in 2014 and to pair them with
Support Offices based on mutual priorities and preferences. This new approach to SO-NO partnering,
permits the earlier involvement of Support Offices in the planning and preparatory stages, early
WV Working with the Global Fund 2013
7 EMPOWER, EQUIP, ADVOCATE
negotiation of partnering terms including match, early technical support from Support Offices, more
efficient technical support and capacity building from GC, and stronger partnerships. Twenty-three
National Offices and seven support offices have indicated their intent to work together to position for
funding in 2014-2015.
Coordination with GFO Grant Acquisition and Management (GAM) - With the establishment of
the WV GAM structure within GFO, GFU began to strategically coordinate with and leverage the new
structure in order to ensure smooth operational cooperation, gain greater visibility and support for the
Global Fund opportunities in World Vision, and to protect the current successful policies and business
process.
GFU coordinated with the GFO financial analyst to improve financial reporting of the Global Fund
portfolio.
GFU began to revise the WV Global Fund Business Process to incorporate the new GAM hubs as
stakeholders in Global Fund grant acquisition and management and to ensure alignment with emerging
GAM policies and procedures.
GFU began to leverage the GAM Community of Practice and GAM hub platform for strategic
communications, joint problem solving related to Global Fund acquisition and management activities.
Research and Resources from the Global Fund Unit - During the year, the team undertook two
research projects:
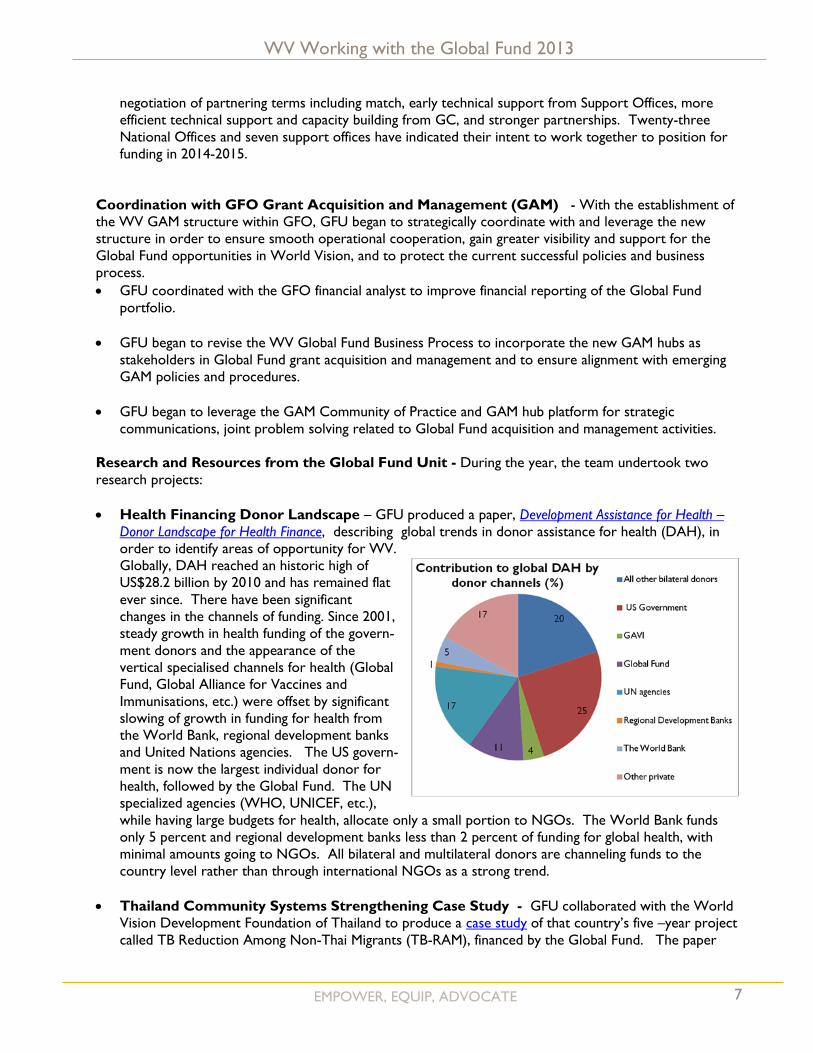
Health Financing Donor Landscape – GFU produced a paper, Development Assistance for Health –
Donor Landscape for Health Finance, describing global trends in donor assistance for health (DAH), in
order to identify areas of opportunity for WV.
Globally, DAH reached an historic high of
US$28.2 billion by 2010 and has remained flat
ever since. There have been significant
changes in the channels of funding. Since 2001,
steady growth in health funding of the govern-
ment donors and the appearance of the
vertical specialised channels for health (Global
Fund, Global Alliance for Vaccines and
Immunisations, etc.) were offset by significant
slowing of growth in funding for health from
the World Bank, regional development banks
and United Nations agencies. The US govern-
ment is now the largest individual donor for
health, followed by the Global Fund. The UN
specialized agencies (WHO, UNICEF, etc.),
while having large budgets for health, allocate only a small portion to NGOs. The World Bank funds
only 5 percent and regional development banks less than 2 percent of funding for global health, with
minimal amounts going to NGOs. All bilateral and multilateral donors are channeling funds to the
country level rather than through international NGOs as a strong trend.
Thailand Community Systems Strengthening Case Study - GFU collaborated with the World
Vision Development Foundation of Thailand to produce a case study of that country’s five –year project
called TB Reduction Among Non-Thai Migrants (TB-RAM), financed by the Global Fund. The paper

WV Working with the Global Fund 2013
8 EMPOWER, EQUIP, ADVOCATE
highlights the community based approaches that contributed to objectives of increased case detection,
referral, treatment and cure. Project activities included community mobilization and systems
strengthening and were carried out by migrant health volunteers and other community volunteers using
community-based health posts as a point of interface with migrants. The project also included elements
of advocacy led by Thai staff who worked to strengthen linkages with the formal health system, local
immigration department, police department, community leaders and business owners to raise awareness
and support for migrant TB patients. The project had an 86 percent treatment success rate for all forms
of TB, which exceeded the target, and also exceeded the national treatment success rate of 79 percent.
VI. Update on the Global Fund
New Leadership - The Global Fund had completed 89 percent of the reforms listed in the
Consolidated Transformation Plan, former General Manager Gabriel Jaramillo said in an outgoing letter
on 18 January 2013 his last day at the Fund. The institution began the year with the appointment of a
new Executive Director, signaling the end of its year of transition and the full implementation of its new
structure, reforms, and vision. The new leader is Ambassador Mark Dybul, who had previously been the
Director of the United States Office of Global AIDS Coordinator (OGAC) which implements PEPFAR.
In his earliest statements, Dr. Dybul described a paradigm shift in the approach to international health
and development: one that views AIDS, TB and malaria as a series of micro –epidemics, requiring
contextualized, evidence-based analysis and response, particularly aimed at most affected communities.
Human rights began taking a front position in the financing institution, with a new focus for including
previously marginalized, highly impacted groups in national dialogue, grant-making, and investment
strategies.
The New Funding Model (NFM) - March 1, 2013 marked the beginning of a transition period for the
NFM with $1.9 billion allocated to 6 “early applicant” countries (defined as those that would apply for
new grants using all the steps of the NFM) and 48 “interim applicants” (countries defined as those that
would apply for extensions to existing grants using some of the steps of the NFM). Early and interim
applicants were selected based on whether disease programmes were currently receiving less than they
would under the NFM’s allocation principles based on disease burden and per-capita income level, or
were at risk of essential service interruptions from 2013 up to the end of September 2014, or were
positioned to achieve rapid impact. All other countries not on the lists of early and interim applicants
were encouraged to take steps to get ready for the full rollout of the NFM in 2014. These include
strengthening their national strategies, strengthening PR capacity and CCM capacity, and starting or
reinforcing the country dialogue process.
The NFM diverges dramatically from the previous acquisition procedures. There will no longer be
annual global Calls for Proposal and a competitive process resulting in winners and losers. The NFM is
designed to permit countries to apply for grants derived from their country health strategy, at a time of
their own choice throughout the year best suited to their specific national planning cycle. Proposals
(now called Concept Notes) are to be prepared as the result of an on-going inclusive country dialogue
and in an iterative consultation with the Global Fund Secretariat, resulting in proposals that are likely to
be approved by the Technical Review Panel (TRP) and the Grant Approval Committee (GAC).
Countries will also know their funding ceiling before preparing the Concept Note, meaning greater
predictability of aid flows. Detailed grant-making that finalizes all the documentation will precede the
Board approval so that disbursements and implementation can begin immediately thereafter, and the
whole process is now expected to take six months to one year, as opposed to the previous one to two
years. For more details on the NFM, as well as the new guidelines, tools and resources see here.
WV Working with the Global Fund 2013
9 EMPOWER, EQUIP, ADVOCATE
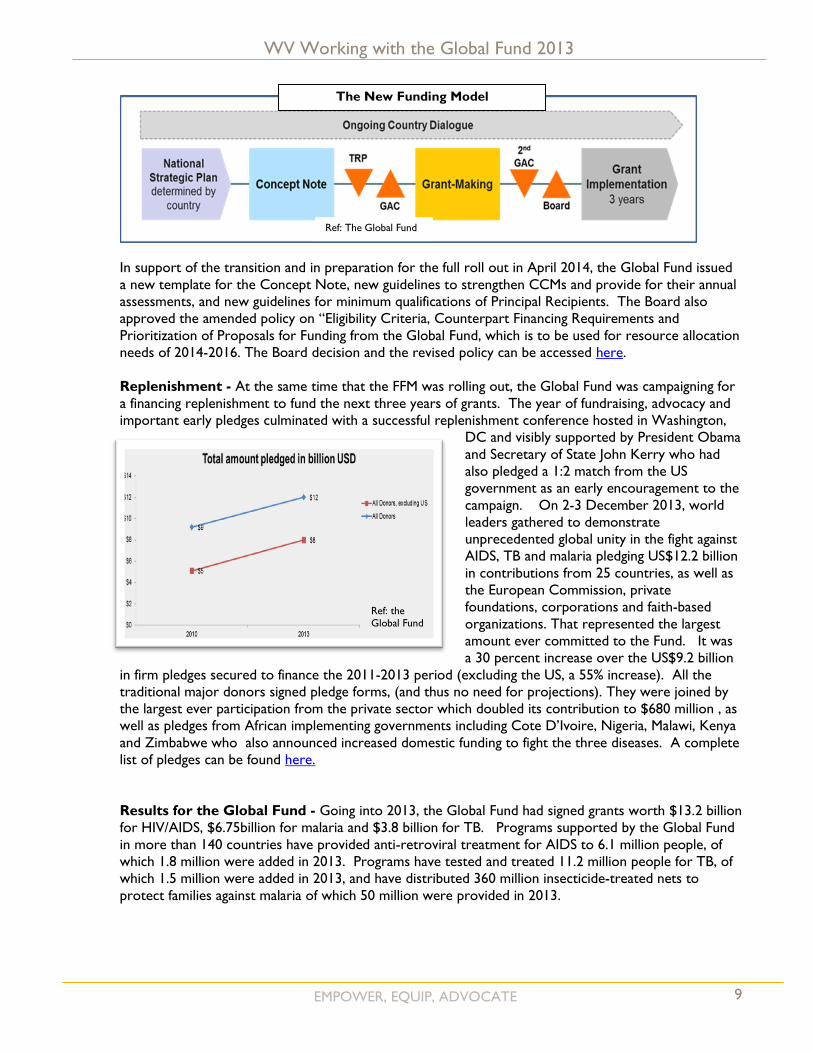
In support of the transition and in preparation for the full roll out in April 2014, the Global Fund issued
a new template for the Concept Note, new guidelines to strengthen CCMs and provide for their annual
assessments, and new guidelines for minimum qualifications of Principal Recipients. The Board also
approved the amended policy on “Eligibility Criteria, Counterpart Financing Requirements and
Prioritization of Proposals for Funding from the Global Fund, which is to be used for resource allocation
needs of 2014-2016. The Board decision and the revised policy can be accessed here.
Replenishment - At the same time that the FFM was rolling out, the Global Fund was campaigning for
a financing replenishment to fund the next three years of grants. The year of fundraising, advocacy and
important early pledges culminated with a successful replenishment conference hosted in Washington,
DC and visibly supported by President Obama
and Secretary of State John Kerry who had
also pledged a 1:2 match from the US
government as an early encouragement to the
campaign. On 2-3 December 2013, world
leaders gathered to demonstrate
unprecedented global unity in the fight against
AIDS, TB and malaria pledging US$12.2 billion
in contributions from 25 countries, as well as
the European Commission, private
foundations, corporations and faith-based
organizations. That represented the largest
amount ever committed to the Fund. It was
a 30 percent increase over the US$9.2 billion
in firm pledges secured to finance the 2011-2013 period (excluding the US, a 55% increase). All the
traditional major donors signed pledge forms, (and thus no need for projections). They were joined by
the largest ever participation from the private sector which doubled its contribution to $680 million , as
well as pledges from African implementing governments including Cote D’Ivoire, Nigeria, Malawi, Kenya
and Zimbabwe who also announced increased domestic funding to fight the three diseases. A complete
list of pledges can be found here.
Results for the Global Fund - Going into 2013, the Global Fund had signed grants worth $13.2 billion
for HIV/AIDS, $6.75billion for malaria and $3.8 billion for TB. Programs supported by the Global Fund
in more than 140 countries have provided anti-retroviral treatment for AIDS to 6.1 million people, of
which 1.8 million were added in 2013. Programs have tested and treated 11.2 million people for TB, of
which 1.5 million were added in 2013, and have distributed 360 million insecticide-treated nets to
protect families against malaria of which 50 million were provided in 2013.
Ref: the Global Fund
The New Funding Model
Ref: The Global Fund
WV Working with the Global Fund 2013
10 EMPOWER, EQUIP, ADVOCATE
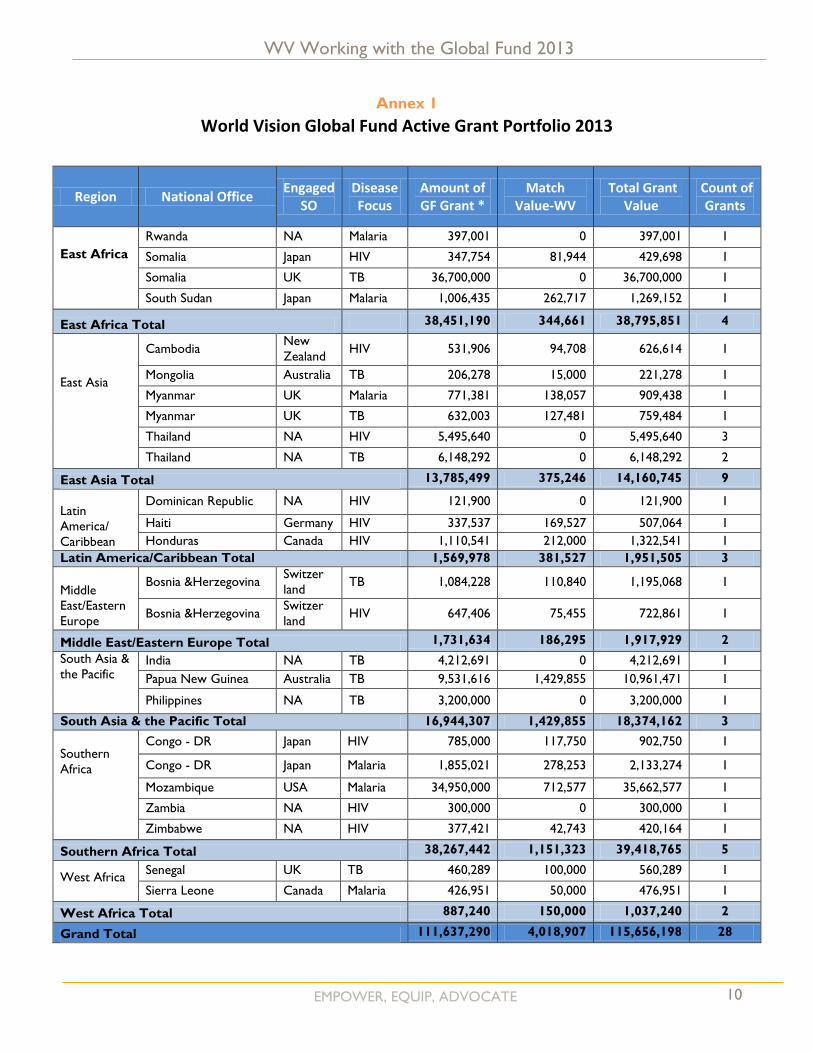
Annex 1
World Vision Global Fund Active Grant Portfolio 2013
Region National Office Engaged
SO Disease Focus
Amount of GF Grant *
Match Value-WV
Total Grant Value
Count of Grants
East Africa
Rwanda NA Malaria 397,001 0 397,001 1
Somalia Japan HIV 347,754 81,944 429,698 1
Somalia UK TB 36,700,000 0 36,700,000 1
South Sudan Japan Malaria 1,006,435 262,717 1,269,152 1
East Africa Total 38,451,190 344,661 38,795,851 4
East Asia
Cambodia New
Zealand HIV 531,906 94,708 626,614 1
Mongolia Australia TB 206,278 15,000 221,278 1
Myanmar UK Malaria 771,381 138,057 909,438 1
Myanmar UK TB 632,003 127,481 759,484 1
Thailand NA HIV 5,495,640 0 5,495,640 3
Thailand NA TB 6,148,292 0 6,148,292 2
East Asia Total 13,785,499 375,246 14,160,745 9
Latin
America/
Caribbean
Dominican Republic NA HIV 121,900 0 121,900 1
Haiti Germany HIV 337,537 169,527 507,064 1
Honduras Canada HIV 1,110,541 212,000 1,322,541 1
Latin America/Caribbean Total 1,569,978 381,527 1,951,505 3
Middle
East/Eastern
Europe
Bosnia &Herzegovina Switzer
land TB 1,084,228 110,840 1,195,068 1
Bosnia &Herzegovina Switzer
land HIV 647,406 75,455 722,861 1
Middle East/Eastern Europe Total 1,731,634 186,295 1,917,929 2
South Asia &
the Pacific
India NA TB 4,212,691 0 4,212,691 1
Papua New Guinea Australia TB 9,531,616 1,429,855 10,961,471 1
Philippines NA TB 3,200,000 0 3,200,000 1
South Asia & the Pacific Total 16,944,307 1,429,855 18,374,162 3
Southern
Africa
Congo - DR Japan HIV 785,000 117,750 902,750 1
Congo - DR Japan Malaria 1,855,021 278,253 2,133,274 1
Mozambique USA Malaria 34,950,000 712,577 35,662,577 1
Zambia NA HIV 300,000 0 300,000 1
Zimbabwe NA HIV 377,421 42,743 420,164 1
Southern Africa Total 38,267,442 1,151,323 39,418,765 5
West Africa
Senegal UK TB 460,289 100,000 560,289 1
Sierra Leone Canada Malaria 426,951 50,000 476,951 1
West Africa Total 887,240 150,000 1,037,240 2
Grand Total 111,637,290 4,018,907 115,656,198 28

WV Working with the Global Fund 2013
11 EMPOWER, EQUIP, ADVOCATE
Annex 2
For any questions regarding this report, please contact Ann Claxton: [email protected]





























