Embed Size (px)
Citation preview
2011 Volume 47 Number 1
Please tick your box and pass this on:
■ CEO
■ Medical director
■ Nursing director
■ Head of radiology
■ Head of physiotherapy
■ Senior pharmacist
■ Head of IS/IT
■ Laboratory director
■ Head of purchasing
■ Facility manager
Editorial
Management
Hospital demand variations: suggested
instruments for hospital managers
Measuring availability, affordability and
management of essential medicines in public
hospitals of Burkina Faso
SSpecial feattuure: ProcurementInternational overview of hospital procurement
Centralized distribution: reducing ownership
costs by streamlining hospital logistics
The challenges of collaborative procuremement in
the healthcare sector
e-procurement in hospitals
The value of group purchassining organizations in
the United States
Pooling procuremenentt in the Belgian hospital
sector
World Hospitals and Health ServicesThe Official Journal of the International Hospital Federation
www.ihf-fih.org
C
M
Y
CM
MY
CY
CMY
K
00 cover vol47.1.ai 31/3/11 18:00:0400 cover vol47.1.ai 31/3/11 18:00:04
00-01 Contents 46_8:27 4/1/11 13:05 Page 1
World Hospitals and Health Services Vol. 47 No. 1 01
Contents
Contents volume 47 number 1
03 Editorial Eric de Roodenbeke
Management04 Hospital demand variations: suggested instruments for hospital managers
Zoe Boutsioli
08 Measuring availability, affordability and management of essential medicines in public hospitals of Burkina FasoHamado Saouadogo
Special feature: Procurement12 International overview of hospital procurement
Maud Ferrier, David Lariviere, Claire Laurent and Eric Roque
15 Centralized distribution: reducing ownership costs by streamlining hospital logistics Chantal S Laurin
18 The challenges of collaborative procurement in the healthcare sectorGabriella Margherita Racca
21 e-procurement in hospitalsJulio Villalobos Hidalgo, Joan Orrit and D Juan Pablo Villalobos
24 The value of group purchasing organizations in the United StatesCurtis Rooney
27 Pooling procurement in the Belgian hospital sectorGuy Herbert
Reference31 Language abstracts
34 IHF corporate partners
37 Governing Council list
39 Dates for your diary
Editorial StaffExecutive Editor: Eric de Roodenbeke, PhDDesk Editor: Ioana Rusu, MA.
Editorial BoardDr René PetersDutch Hospital Association Norberto LarrocaCamara Argentina de Empresas de SaludDr Harry McConnellGriffith University School of Medicine (Australia)Dr Persephone DoupiSTAKES
Editorial OfficeImmeuble JB SAY,13 Chemin du Levant, 01210 Ferney Voltaire, FranceEmail: [email protected] Internet: www.ihf-fih.org
Subscription OfficeInternational Hospital Federation c/o Fairfax House, 15 Fulwood Place, London WC1V 6AY, UKTelephone: +44 (0) 20 7969 5500;Facsimile: +44 (0) 20 7969 5600
ISSN: 0512-3135
Published by Pro-Brook Publishing Limited for the International Hospital Federation
6 Deben Mill Business CentreWoodbridgeSuffolk IP12 1BLUnited KingdomTel: +44 (0) 1394 446006 Fax: +44 (0) 1473 249034Internet: www.pro-brook.com
For advertising enquiries contact our CommunicationsManager at [email protected]
World Hospitals and Health Services is publishedquarterly. All subscribers automatically receive a copyof the IHF reference books. The annual subscription tonon-members for 2011 costs £175 or US$250.
World Hospitals and Health Services is listed inHospital Literature Index, the single mostcomprehensive index to English language articles onhealthcare policy, planning and administration. The index is produced by the American HospitalAssociation in co-operation with the National Library ofMedicine. Articles published in World Hospitals andHealth Services are selectively indexed in Health CareLiterature Information Network.
The International Hospital Federation (IHF) is anindependent non-political body whose aims are toimprove patient safety and promote health inunderserved communities. The opinions expressed inthis journal are not necessarily those of theInternational Hospital Federation or Pro-BrookPublishing Limited.
00-01 Contents 47_1:27 8/4/11 16:25 Page 1

Editorial
02 World Hospitals and Health Services Vol. 47 No. 1
Editorial
While this editorial is going to print, Japan is facing theworst natural disaster in its history. We want to expressour sympathy to all the people who have suffered and
still have to cope with the consequences of this terrible situation.Since the fifties, the Japan Hospital Association has been a pillarof our organization and in such circumstances, it is normal that theIHF Secretariat calls on other IHF members to offer support in oneform or another.
We would like to thank all those who have respondedimmediately at the request of our colleagues from Japan. Suchsupport expresses the solidarity that exists among us, as we knowthat we may all have to face harsh situations. It also highlights theimportance of international organizations such as IHF that createa venue for healthcare decision-makers to meet. Knowing eachother makes it easier to put in place a solidarity chain. We havehad the need for it in Japan, and we will certainly have similarneeds in the future. Mother Nature will continue to provide us withher beauty, but also reminds us that we are just guests whom shecan treat harshly when she decides to do so.
In a situation like the one in Japan, all those who require carehave to face an additional difficulty due to the conditions in whichthey have to live. Health workers have to face an additionalworkload resulting from the conditions and the casualties fromdisaster. First and foremost, the courage of the Japanese healthworkers has permitted coping with this massive destruction whichhas left so many people homeless. They have been on the frontline, however, it makes a difference for them to know that the restof world is behind them. IHF is not an emergency organization andis not equipped to provide rescue services. However, IHF hasmobilized and encouraged its members to make donations, andto provide in coordination with rescue organizations the criticalmedical consumables. The Japanese disaster has shown that ifresilient health facilities are critical to be able to respondimmediately to post disaster difficulties, there is urgent need formore than the goodwill of the people. Health workers needmedical consumables to deliver care.
In this edition of the World Hospitals and Health Services, we willbe presenting the importance of purchasing strategies for thehealthcare sector. One of the goals of group purchasing is toincrease standardization. Of course, by doing so, it is expected to
ERIC DE ROODENBEKE
CHIEF EXECUTIVE OFFICER, INTERNATIONAL HOSPITAL FEDERATION
have large volume allowing better commercial deals. But whatmay be more important is the standardization of healthcare,making it easier to cope with an unexpected upscaling of activitiesor a need to relocate part of the activities. This example illustrateswell that purchasing is not just about mastering the supply chainand getting best possible prices, but it is also a strategic issue forservice delivery.
IHF believes that purchasing is strategic. For this reason, it hasdecided to put in place a strong partnership with the newlycreated International Association of Group Purchasing (ASSIAPS)as well as to welcome large health care purchasers to become IHFassociate members and to have them create a dedicated chapter.IHF would also like to take this opportunity and thank Ile-de-France Hospital Buyers’ Network (Resah-idf) for its leadership androle in organizing the Purchasing Chapter. Resah-idf groups themajority of the public healthcare institutions in the Ile-de-Francearea. To learn more about the organization, please visithttp://www.resah-idf.com/. Resah-idf was also an active organizerand participant in the 2nd International Symposium on Hospital Procurement which took place last September in Paris (http://www.acheteurs-hospitaliers.com/index.asp). Thissymposium allowed the 400 participants present at the event todiscuss the challenges and prospects of change to procurementwithin the international healthcare sector. Within the PurchasingChapter, IHF will not get involved in the technical aspects relatedto purchasing (ASSIAPS is already doing this), but it will focus onthe policy implications of active purchasing strategies. As aplatform for cross fertilization, IHF is best placed to develop a newdynamic of dialogue between large purchasers from around theworld and large global providers. This may be accelerating theadoption of innovative approaches providing better value formoney.
An international overview of hospital procurement in over 10countries indicates that there is a trend in favour of grouppurchasing. There is, however, still a long way to go as the legalenvironment for procurement, and the differences in the setting ofhospitals does not yet allow full harmonization.
But before getting to harmonization, there is a strong need torely on effective collaboration. First, this collaboration must beinternal to allow all stakeholders within a facility to share the same
02-03 Editorial:29 7/4/11 14:19 Page 2

World Hospitals and Health Services Vol. 47 No. 1 03
Editorial
goals and realize them together with the appropriate inputs.Dialogue also needs to take place across borders to influence theproviders so that they shape their offer to respond to the evolvingdemand.
This effort to harmonize and to foster collaboration does notcome without a cost. The example of the US GPOs which aremore than a hundred year old demonstrates their role to containcost escalation, but also the permanent need to show that thetransaction costs are overridden by the purchasing benefits. Whilea major health reform has been launched in the US for improvingaccess to care, the GPOs will see their role strengthen to avoidthat an increase in demand for care will be fully translated in healthspending.
The Province of Quebec in Canada gives a good example of theimportance of strategic purchasing to curb cost trends in a publicsystem providing free care to all. Whether in public or privatesector and regardless of funding mechanisms, purchasing is nowfully considered an avenue for efficiency improvement.
In addition to implementing strategic purchasing, the e-procurement can allow the hospitals to move a step further. Therecent developments have shown how well designed e-procurement can reduce significantly transaction costs whileallowing better benchmarking of offering in a wider scale.
Group purchasing is often understood as seeking large volumesto get good prices. The example of Belgian hospitals gives anexcellent insight on the concept of the total cost of ownership. Thisconcept is the one guiding all effective purchasing and this is the
reason why dialogue is so important. These various articles on purchasing from both sides of the
Atlantic Ocean and from the largest health care market representa milestone to further invite IHF members to express their interestin this area. With the fast growing development of health caresector in the emerging world, the procurement is going to evolvewith healthcare providers becoming more and more international.The complexity of services offered to hospitals is also a challengethat purchasing organizations have to face.
Mirroring these articles on purchasing, I would you also like todraw your attention to two additional articles in this edition. Theyboth suggest that purchasing is to be related with the full masterof the supply chain in relation with the forecasting of activities.
In low income countries, mastering the supply chain remains thefirst priority. Although group purchasing has allowed reducedprices of essential drugs, it is not enough as the average availabilityof essential drugs remains under 80%. In Burkina Faso, forexample, when drugs are sold to the population, they represent animportant source of revenue, and this may be a challenge foraccessibility by the poor and trigger potential perversemechanisms. On the other hand, having a good forecast ofhospital care demand is not easy, as variation in demand eitherleads to excessive capital investment for avoiding out stocks or toperiodic stock failures as described in the case of Burkina Faso.The work developed in Greece to improve the forecasting ofactivities can allow better mobilization of all inputs and a bettermastering of the supply chain. �
02-03 Editorial:29 7/4/11 14:19 Page 3
Management
4 World Hospitals and Health Services Vol. 47 No. 1
Hospital demand variations: suggestedinstruments for hospital managersi
ABSTRACT: Hospitals worldwide face variations in demand for inpatient care. The accurate forecasting of future demandassists hospitals in programming short-term needs such as staff and supplies, and long-term needs such as beds andbuildings. The existence of the appropriate methodological instruments, applied by hospital managers, could help themsmooth down upcoming patient flows. This work presents two such instruments: first, a univariate autoregressive movingaverage method, and second, a multivariate model. By applying these to the Greek National Health System, we have foundsignificant demand variations. The univariate method provides more accurate forecasting of future unexpected demand.
Hospitals worldwide face considerable demand variations(Smet, 2007; Baker et al., 2004; Hughes & McGuire, 2003;Boutsioli, 2009). Some of these variations are unexpected.
The accurate forecasting of future demand assists hospitals inprogramming short-term needs, such as staff and supplies, andlong-term needs such as beds and buildings. The existence ofappropriate methodological instruments applied by hospitalmanagers could help them smooth down upcoming patient flows.In the literature, two approaches have been mostly used toforecast future hospital demand and particularly the unexpectedpart of demand. The first approach is a univariate autoregressivemoving average (ARMA) model. ARMA is a regression model,where the explanatory variables are lags of the dependentvariable. The model is made of two parts. The first part is theautoregressive part, i.e. hospital daily admissions depend onprevious daily admissions; the second part is the moving averagepart (MA), i.e. an average of all past errors made in predictinghospital admissions. Hospital emergency admissions are used asthe dependent variable to estimate unexpected demand.According to this model, the unexpected demand is based on aresidual estimate of forecasted daily emergency demand. Thus,the level of unexpected demand faced by a hospital is defined asthe difference between realized and forecasted emergencydemand, gained from the ARMA forecasting model (Hughes &McGuire, 2003; Boutsioli, 2010). The second method refers to amultivariate model that unexpected hospital demand is a functionof a number of explanatory variables. The most commonly usedvariables include the day of the week, i.e. the weekend, the “duty”status of the hospital, the summer and the official holiday effects(Hussain et al., 2005; Baker et al., 2004; Fullerton & Crawford,1999; Upshur et al., 2005).
Hospital demand variations in the Athenian hospital context The Greek public hospitals belong to a National Health System
DR ZOE BOUTSIOLI
RESEARCHER, HEALTH RESEARCH UNIT, ATHENS INSTITUTE FOR
EDUCATION AND RESEARCH (ATINER)
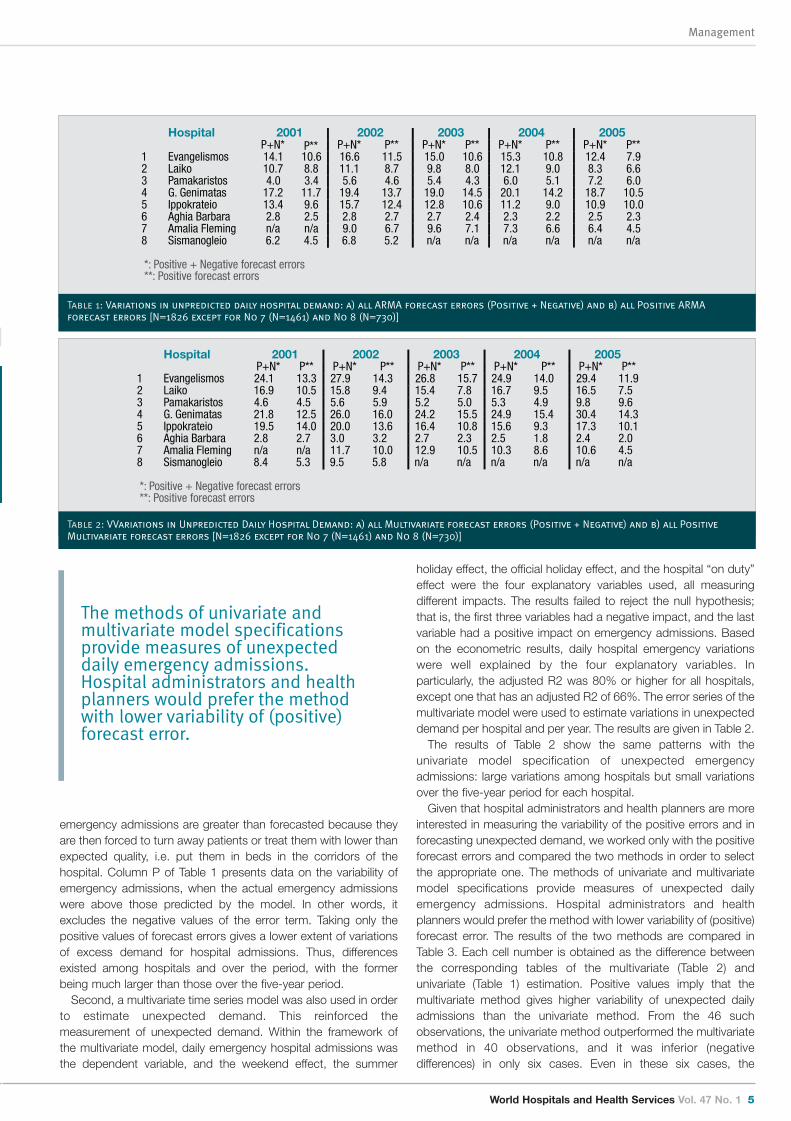
(NHS). We collected daily data of patient emergency admissionsfrom eight Athenian public hospitals from 2001 to 2005. First, weapplied the ARMA method to emergency hospital admissions datato estimate daily measures of unexpected demand. In the test forstationarity of daily emergency admissions, it was found that thenull hypothesis of unit root was rejected at the 1% level ofsignificance, implying that the series are stationary at that level.Based on the criteria proposed by Akaike and Schwarz, weselected the best ARMA model specification. The lower the valuesof the Akaike-Schwartz criterion, the most appropriate the ARMAmodel. Each hospital’s estimation process provides an estimate ofthe residual (_t), which is the unpredicted part of emergency dailyadmissions. These residuals had a zero mean, and their standarddeviation was constant. To estimate the average daily variations ofunexpected demand, we used two ways: a) all the residualsforecasts, both positive and negative, and b) only the positivevalues of forecast errors. These are positive when actual(emergency admissions) are more than the fitted, while they arenegative when the actual are less than the fitted. In case (a), if wesum up the residuals they should be equal to zero, according tothe theory. To overcome this, we have taken the absolute valuesof the negative forecast errors. In case (b), we call this “excessdemand” for unexpected admissions. Table 1 reports measures ofthe standard deviations of unpredicted emergency admissions perhospital per year. The unpredicted part of emergency admissionswas not the same for each hospital, and it also varied over theyears.
The results reported in P+N column of Table 1 treat variations ofdaily emergency admissions as equal around its mean. However,of importance for the hospital manager are the cases that
i This paper is part of my PhD thesis in the University of Kent, UK. I thank very muchfor their support and guidance Professor Ann Netten, University of Kent, UK andProfessor Alastair Gray, University of Oxford, UK.
04-07 Boutsioli:29 31/3/11 18:10 Page 4
World Hospitals and Health Services Vol. 47 No. 1 5
Management
emergency admissions are greater than forecasted because theyare then forced to turn away patients or treat them with lower thanexpected quality, i.e. put them in beds in the corridors of thehospital. Column P of Table 1 presents data on the variability ofemergency admissions, when the actual emergency admissionswere above those predicted by the model. In other words, itexcludes the negative values of the error term. Taking only thepositive values of forecast errors gives a lower extent of variationsof excess demand for hospital admissions. Thus, differencesexisted among hospitals and over the period, with the formerbeing much larger than those over the five-year period.
Second, a multivariate time series model was also used in orderto estimate unexpected demand. This reinforced themeasurement of unexpected demand. Within the framework ofthe multivariate model, daily emergency hospital admissions wasthe dependent variable, and the weekend effect, the summer
holiday effect, the official holiday effect, and the hospital “on duty”effect were the four explanatory variables used, all measuringdifferent impacts. The results failed to reject the null hypothesis;that is, the first three variables had a negative impact, and the lastvariable had a positive impact on emergency admissions. Basedon the econometric results, daily hospital emergency variationswere well explained by the four explanatory variables. Inparticularly, the adjusted R2 was 80% or higher for all hospitals,except one that has an adjusted R2 of 66%. The error series of themultivariate model were used to estimate variations in unexpecteddemand per hospital and per year. The results are given in Table 2.
The results of Table 2 show the same patterns with theunivariate model specification of unexpected emergencyadmissions: large variations among hospitals but small variationsover the five-year period for each hospital.
Given that hospital administrators and health planners are moreinterested in measuring the variability of the positive errors and inforecasting unexpected demand, we worked only with the positiveforecast errors and compared the two methods in order to selectthe appropriate one. The methods of univariate and multivariatemodel specifications provide measures of unexpected dailyemergency admissions. Hospital administrators and healthplanners would prefer the method with lower variability of (positive)forecast error. The results of the two methods are compared inTable 3. Each cell number is obtained as the difference betweenthe corresponding tables of the multivariate (Table 2) andunivariate (Table 1) estimation. Positive values imply that themultivariate method gives higher variability of unexpected dailyadmissions than the univariate method. From the 46 suchobservations, the univariate method outperformed the multivariatemethod in 40 observations, and it was inferior (negativedifferences) in only six cases. Even in these six cases, the
Hospital 2001 2002 2003 2004 2005P+N* P** P+N* P** P+N* P** P+N* P** P+N* P**
1 Evangelismos 14.1 10.6 16.6 11.5 15.0 10.6 15.3 10.8 12.4 7.92 Laiko 10.7 8.8 11.1 8.7 9.8 8.0 12.1 9.0 8.3 6.63 Pamakaristos 4.0 3.4 5.6 4.6 5.4 4.3 6.0 5.1 7.2 6.04 G. Genimatas 17.2 11.7 19.4 13.7 19.0 14.5 20.1 14.2 18.7 10.55 Ippokrateio 13.4 9.6 15.7 12.4 12.8 10.6 11.2 9.0 10.9 10.06 Aghia Barbara 2.8 2.5 2.8 2.7 2.7 2.4 2.3 2.2 2.5 2.37 Amalia Fleming n/a n/a 9.0 6.7 9.6 7.1 7.3 6.6 6.4 4.58 Sismanogleio 6.2 4.5 6.8 5.2 n/a n/a n/a n/a n/a n/a
*: Positive + Negative forecast errors **: Positive forecast errors
Table 1: Variations in unpredicted daily hospital demand: a) all ARMA forecast errors (Positive + Negative) and b) all Positive ARMA
forecast errors [N=1826 except for No 7 (N=1461) and No 8 (N=730)]
Hospital 2001 2002 2003 2004 2005P+N* P** P+N* P** P+N* P** P+N* P** P+N* P**
1 Evangelismos 24.1 13.3 27.9 14.3 26.8 15.7 24.9 14.0 29.4 11.92 Laiko 16.9 10.5 15.8 9.4 15.4 7.8 16.7 9.5 16.5 7.53 Pamakaristos 4.6 4.5 5.6 5.9 5.2 5.0 5.3 4.9 9.8 9.64 G. Genimatas 21.8 12.5 26.0 16.0 24.2 15.5 24.9 15.4 30.4 14.35 Ippokrateio 19.5 14.0 20.0 13.6 16.4 10.8 15.6 9.3 17.3 10.16 Aghia Barbara 2.8 2.7 3.0 3.2 2.7 2.3 2.5 1.8 2.4 2.07 Amalia Fleming n/a n/a 11.7 10.0 12.9 10.5 10.3 8.6 10.6 4.58 Sismanogleio 8.4 5.3 9.5 5.8 n/a n/a n/a n/a n/a n/a
*: Positive + Negative forecast errors **: Positive forecast errors
Table 2: VVariations in Unpredicted Daily Hospital Demand: a) all Multivariate forecast errors (Positive + Negative) and b) all Positive
Multivariate forecast errors [N=1826 except for No 7 (N=1461) and No 8 (N=730)]
The methods of univariate andmultivariate model specificationsprovide measures of unexpecteddaily emergency admissions.Hospital administrators and healthplanners would prefer the methodwith lower variability of (positive)forecast error.
04-07 Boutsioli:29 31/3/11 18:10 Page 5
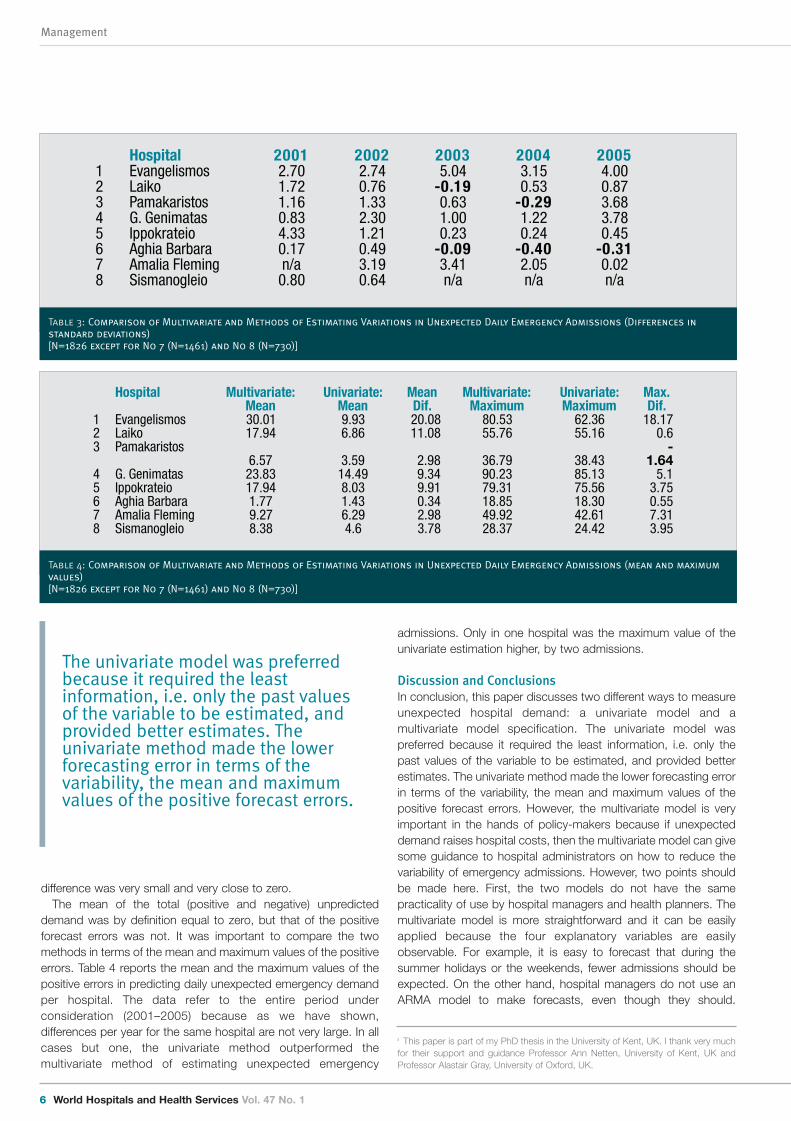
admissions. Only in one hospital was the maximum value of theunivariate estimation higher, by two admissions.
Discussion and ConclusionsIn conclusion, this paper discusses two different ways to measureunexpected hospital demand: a univariate model and amultivariate model specification. The univariate model waspreferred because it required the least information, i.e. only thepast values of the variable to be estimated, and provided betterestimates. The univariate method made the lower forecasting errorin terms of the variability, the mean and maximum values of thepositive forecast errors. However, the multivariate model is veryimportant in the hands of policy-makers because if unexpecteddemand raises hospital costs, then the multivariate model can givesome guidance to hospital administrators on how to reduce thevariability of emergency admissions. However, two points shouldbe made here. First, the two models do not have the samepracticality of use by hospital managers and health planners. Themultivariate model is more straightforward and it can be easilyapplied because the four explanatory variables are easilyobservable. For example, it is easy to forecast that during thesummer holidays or the weekends, fewer admissions should beexpected. On the other hand, hospital managers do not use anARMA model to make forecasts, even though they should.
difference was very small and very close to zero. The mean of the total (positive and negative) unpredicted
demand was by definition equal to zero, but that of the positiveforecast errors was not. It was important to compare the twomethods in terms of the mean and maximum values of the positiveerrors. Table 4 reports the mean and the maximum values of thepositive errors in predicting daily unexpected emergency demandper hospital. The data refer to the entire period underconsideration (2001–2005) because as we have shown,differences per year for the same hospital are not very large. In allcases but one, the univariate method outperformed themultivariate method of estimating unexpected emergency
Management
6 World Hospitals and Health Services Vol. 47 No. 1
Hospital 2001 2002 2003 2004 20051 Evangelismos 2.70 2.74 5.04 3.15 4.002 Laiko 1.72 0.76 -0.19 0.53 0.873 Pamakaristos 1.16 1.33 0.63 -0.29 3.684 G. Genimatas 0.83 2.30 1.00 1.22 3.785 Ippokrateio 4.33 1.21 0.23 0.24 0.456 Aghia Barbara 0.17 0.49 -0.09 -0.40 -0.317 Amalia Fleming n/a 3.19 3.41 2.05 0.028 Sismanogleio 0.80 0.64 n/a n/a n/a
Table 3: Comparison of Multivariate and Methods of Estimating Variations in Unexpected Daily Emergency Admissions (Differences in
standard deviations)
[N=1826 except for No 7 (N=1461) and No 8 (N=730)]
Hospital Multivariate:Mean
Univariate:Mean
Mean Dif.
Multivariate:Maximum
Univariate:Maximum
Max. Dif.
1 Evangelismos 30.01 9.93 20.08 80.53 62.36 18.172 Laiko 17.94 6.86 11.08 55.76 55.16 0.63 Pamakaristos
6.57 3.59 2.98 36.79 38.43-
1.644 G. Genimatas 23.83 14.49 9.34 90.23 85.13 5.15 Ippokrateio 17.94 8.03 9.91 79.31 75.56 3.756 Aghia Barbara 1.77 1.43 0.34 18.85 18.30 0.557 Amalia Fleming 9.27 6.29 2.98 49.92 42.61 7.318 Sismanogleio 8.38 4.6 3.78 28.37 24.42 3.95
Table 4: Comparison of Multivariate and Methods of Estimating Variations in Unexpected Daily Emergency Admissions (mean and maximum
values)
[N=1826 except for No 7 (N=1461) and No 8 (N=730)]
ii This paper is part of my PhD thesis in the University of Kent, UK. I thank very muchfor their support and guidance Professor Ann Netten, University of Kent, UK andProfessor Alastair Gray, University of Oxford, UK.
The univariate model was preferredbecause it required the leastinformation, i.e. only the past valuesof the variable to be estimated, andprovided better estimates. Theunivariate method made the lowerforecasting error in terms of thevariability, the mean and maximumvalues of the positive forecast errors.
04-07 Boutsioli:29 31/3/11 18:10 Page 6

World Hospitals and Health Services Vol. 47 No. 1 7
Management
Second, the better performance of the univariate modelcompared to the multivariate modelii is to a large extent due tovariables omitted from the multivariate model. Unfortunately,important determinants of emergency admissions are not availableon a daily basis, resulting in inferior forecasts by the multivariatemodel. �
Dr Zoe Boutsioli holds a PhD in Social Policy and a MSc inInternational Health Policy. She has published a number of researchpapers on various peer-reviewed journals. Her research interestsfocuses on hospital economics, policy and management.
References1. 1. Baker, L.C., C.S. Phibbs, C. Guarino, D. Supina and J.L. Reynolds (2004). Within-year
Variation in Hospital Utilization and its Implications for Hospital Costs. Journal of HealthEconomics, 23, 191-211.
2. Boutsioli, Z. (2009). Measuring unexpected hospital demand: the application of a univariatemodel to public hopsitals in Greece. Hospital Topics 87(4, Fall): 14-21.
3. Fullerton, K.J. and V.L.S. Crawford (1999). The Winter Bed Crisis – Quantifying SeasonalEffects on Hospital Bed Usage. Quarterly Journal of Medicine: An International Journal ofMedicine, 92(4), 199-206.
4. Hughes, D. and A. McGuire (2003). Stochastic Demand, Production Responses and HospitalCosts. Journal of Health Economics, 22(6), 999-1010.
5. Hussain, S., R. Harrison, J. Ayres, S. Walter, J. Hawker, R. Wilson and G. Shukur (2005).Estimating and Forecasting Hospital Admissions due to Influenza: Planning for WinterPressure – The Case of the West Midlands, UK. Journal of Applied Statistics, 32(3), 191-205.
6. Smet, M. (2007). Measuring Performance in the Presence of Stochastic Demand for HospitalServices: An Analysis of Belgian General Care Hospitals. Journal of Production Annals, 27,13-29.
7. Upshur, R.E.G., R. Moineddin, E. Crighton, L. Kiefer and M. Mamdani (2005). Simplicity withinComplexity: Seasonality and Predictability of Hospital Admissions in the Province of Ontario1988-2001 – A Population-based Analysis. Health Services Research, 5(13)
04-07 Boutsioli:29 31/3/11 18:10 Page 7
Management
8 World Hospitals and Health Services Vol. 47 No. 1
Measuring availability, affordability andmanagement of essential medicines inpublic hospitals of Burkina Faso
ABSTRACT: In Burkina Faso, improving healthcare services and the availability of pharmaceutical productsconstitute a growing concern for the population. This study objective was to evaluate the availability, prices, andsales revenue for a grouping of 50 basic medications in public hospitals from 29 September – 29 December 2009.
The method used to study the prices, availability, affordability and price components from Health ActionInternational (HAI) and the World Health Organization (WHO) has been used to collect and analyze the data.
The results show that the average ratio between the pharmaceutical budget and that of the health centre is16.18. The average rate of availability was 77.69%.
The purchasing price from the hospitals providers is approximately the same as the international referenceprices (1.12). The public hospitals selling price to the public was double the buying price from their provider (2.20).
The total sales revenue from the first three trimesters of 2009 was 708,740,495 FCFA (€1,080,397). This revenueaccounted for roughly 23.02% of the total costs for available pharmaceuticals during the period (3,078,938,053FCFA/€4,693,503).
Faced with a growingdemand to improve themanner of supplying health
services and the place ofmedications and other medicalservices within hospitals, thedevelopment of a central hospitalpharmacy currently presents itselfas an inevitable strategy for theBurkinabé government.
The objective of hospital reformwas to increase the sector’sfunctionality and permit thesector to better place its rights,obligations, and responsibilitiesface-to-face with institutions andpatients. In order to reach thisobjective, each hospital mustassure equal and efficient accessto the health care available.
Pharmaceutical care bringstogether all pharmaceutical acts,from the acquisition to theobservance of treatment, thevigilance and ongoing patient care, and constitutes the centralpillar of healthcare. This care is the heart of each hospital unit andmust be performed with professionalism and dynamism.
Anxious to make public hospitals higher functioning, thegovernment has put in place a legislative framework and
DR HAMADO SAOUADOGO
MINISTRY OF HEALTH, BURKINA FASO
regulations to facilitate a better development of thepharmaceutical hospital sector.
Objective of the studyTo evaluate the availability, prices of a grouping of 50 essential
27
1411
1815
12 12
21
12
0
5
10
15
20
25
30
CHU
YO
CHU
P
CHU
SS
BANF
ORA
DEDO
UGOU
DORI
FADA
GAOU
A
KAYA
KOUD
OUGO
U
OUAH
IGOU
YA
TENK
ODOG
O
Ratio BPP/BT CH
Perc
enta
ge
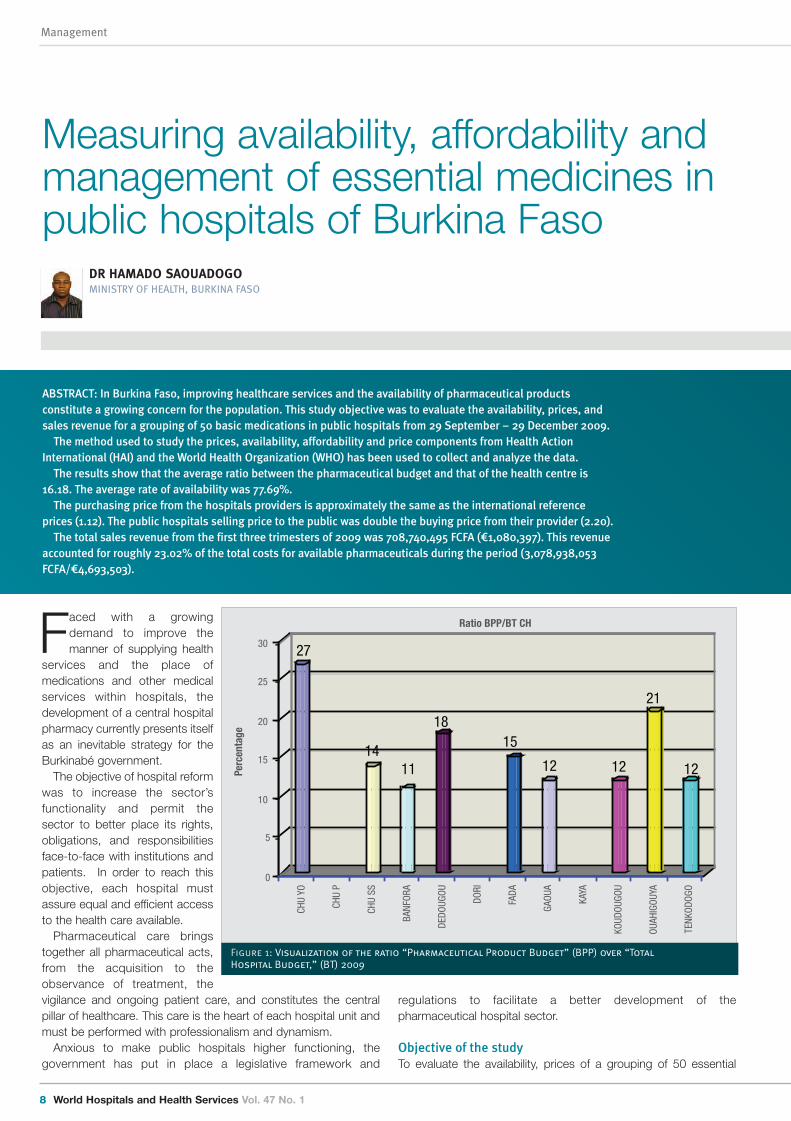
Figure 1: Visualization of the ratio “Pharmaceutical Product Budget” (BPP) over “Total
Hospital Budget,” (BT) 2009
08-11 burkina faso:29 31/3/11 18:13 Page 8
World Hospitals and Health Services Vol. 47 No. 1 9
Management
medications and sales revenue ofmedications in public hospitals fromSeptember 29 to December 29, 2009.MethodsTwo teams of three people, each wereformed to execute data gathering outingsin twelve university (03) and regional (09)hospitals. Four axes were made to takeinto account the geographic situation ofthe hospitals. A data collection formulafor the price and availability of essentialmedications was used. It wasaccompanied by a support and adviceguide in pharmaceutical management.The work started off at the pharmacy, thefinancial administrative offices, theaccounting office, and the generaldirector of each establishment. The datacollected was typed into a standardizedelectronic notebook created by HealthAction International and validated by theWorld Health Organization (HAI/WHO) tomeasure prices, availability, and financialaccessibility of medications. The dataanalysis was performed based on thiselectronic notebook. The ratios andaverage prices were calculated using thesame electronic WHO/HAI tool used inthe execution of this study measuring theprices and availability of medications inBurkina Faso.
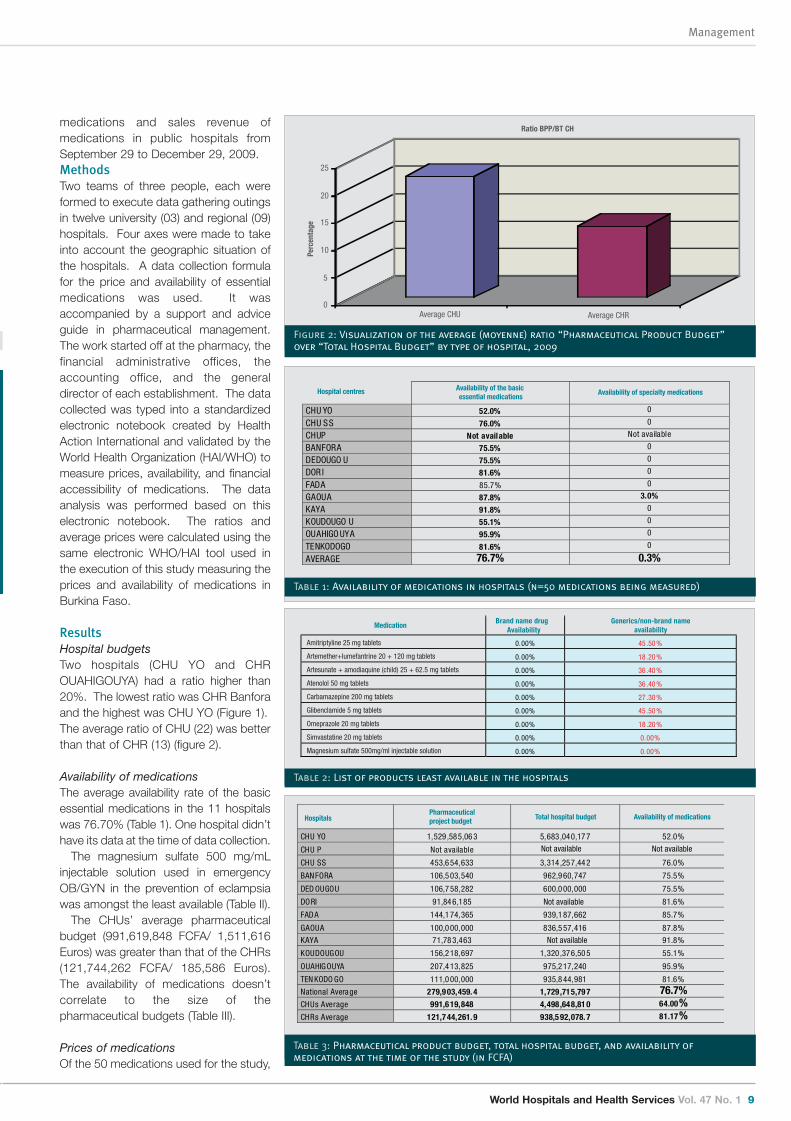
ResultsHospital budgetsTwo hospitals (CHU YO and CHROUAHIGOUYA) had a ratio higher than20%. The lowest ratio was CHR Banforaand the highest was CHU YO (Figure 1).The average ratio of CHU (22) was betterthan that of CHR (13) (figure 2).
Availability of medicationsThe average availability rate of the basicessential medications in the 11 hospitalswas 76.70% (Table 1). One hospital didn’thave its data at the time of data collection.
The magnesium sulfate 500 mg/mLinjectable solution used in emergencyOB/GYN in the prevention of eclampsiawas amongst the least available (Table II).
The CHUs’ average pharmaceuticalbudget (991,619,848 FCFA/ 1,511,616Euros) was greater than that of the CHRs(121,744,262 FCFA/ 185,586 Euros).The availability of medications doesn’tcorrelate to the size of thepharmaceutical budgets (Table III).
Prices of medicationsOf the 50 medications used for the study,
0
5
10
15
20
25
Average CHU Average CHR
Ratio BPP/BT CH
Perc
enta
ge
Figure 2: Visualization of the average (moyenne) ratio “Pharmaceutical Product Budget”
over “Total Hospital Budget” by type of hospital, 2009
CHU YO 52.0% 0
CHU SS 76.0% 0
CHUP Not available Not available
BANFORA 75.5% 0
DEDOUGO U 75.5% 0
DOR I 81.6% 0
FADA 85.7% 0
GAOUA 87.8% 3.0%
KAYA 91.8% 0
KOUDOUGO U 55.1% 0
OUAHIGO UYA 95.9% 0
TENKODOGO 81.6% 0
AVERAGE 76.7% 0.3%
Hospital centres Availability of the basic essential medications
Availability of specialty medications
Table 1: Availability of medications in hospitals (n=50 medications being measured)
MedicationBrand name drug
Availability
0.00% 45 .50%
0.00% 18 .20%
0.00% 36 .40%
0.00% 36 .40%
0.00% 27 .30%
0.00% 45 .50%
0.00% 18 .20%
0.00% 0.00%
0.00% 0.00%
Generics/non-brand nameavailability
Amitriptyline 25 mg tablets
Artemether+lumefantrine 20 + 120 mg tablets
Artesunate + amodiaquine (child) 25 + 62.5 mg tablets
Atenolol 50 mg tablets
Carbamazepine 200 mg tablets
Glibenclamide 5 mg tablets
Omeprazole 20 mg tablets
Simvastatine 20 mg tablets
Magnesium sulfate 500mg/ml injectable solution
Table 2: List of products least available in the hospitals
CHU YO 1,529,585,06 3 5,683,040,17 7 52.0%
CHU P Not available
CHU SS 453,6 54,633 3,314,257,44 2 76.0%
BANFORA 106,5 03,540 962,9 60,747 75.5%
DED OUGOU 106,7 58,282 600,0 00,000 75.5%
DORI 91,84 6,185 Not available 81.6%
FADA 144,1 74,365 939,1 87,662 85.7%
GAOUA 100,0 00,000 836,5 57,416 87.8%
KAYA 71,78 3,463 91.8%
KOUDOUGOU 156,2 18,697 1,320,376,50 5 55.1%
OUAHIGOUYA 207,4 13,825 975,2 17,240 95.9%
TEN KODO GO 111,0 00,000 935,8 44,981 81.6%
National Average 279,9 03,459. 4 1,729,715,79 7 76.7%CHUs Average 991,6 19,848 4,498,648,81 0 64.00%CHRs Average 121,7 44,261. 9 938,5 92,078. 7 81.17%
HospitalsPharmaceuticalproject budget Total hospital budget Availability of medications
Not available
Not available Not available
Table 3: Pharmaceutical product budget, total hospital budget, and availability of
medications at the time of the study (in FCFA)
08-11 burkina faso:29 31/3/11 18:13 Page 9

pharmaceuticals is important to thehospital, the more the medications areavailable.
A study performed in 2008 indicated thatthe absence of financial autonomy inpharmacies played into the quality ofmanagement and availability ofmedications. The absence of frank actionby the General Directors to put in place ahospital pharmacy policy also contributesto the lack of availability of medications.Also the absence of a central pharmacy forall hospitals is a handicap against greatermedication availability in hospitals. Finally,the absence of a health insurance systemdoes not favour the working of a basicpatient care system and plays into thequality of medication management.
The study for measuring medicine prices,availability, affordability and pricescomponents in Burkina Faso at 2009indicated that the existing low householdbuying power was also a negative factoragainst the creation of a good hospital
pharmacy policy. The recourse to social service and non-paymentof bills following un-prepaid urgent care can be seen as proof ofthis (Saouadogo, 2011).
ConclusionThis study allowed for the following of four principle indicators ofquality pharmaceutical management in the hospital setting. Theseindicators are measures of the ratio of the budget forpharmaceutical products over the total hospital budget, of theavailability rate of a grouping of 50 essential medications, of theprice ratio between the public selling price and the buying pricefrom the supplier, and of the financial value of the sales revenue ofthese medications. The results show that the pharmaceuticalmanagement in the hospital setting still needs additionalreinforcement. Also, the difference between the buying price CIFOuagadougou from the suppliers and the public selling price athospitals is 97%. As a result, the sales revenue has been weakerbut the patients are paying double the supply price. Finally, manyfactors affect the composition of the price of medications anddecrease household accessibility despite the introduction of thecommon exterior tariff (TEC) by the West-African Monetary andEconomic Union (UEMOA). This is why solid, rigorously followed,and evaluated hospital pharmacy policy is necessary in the region.
RecommendationsTo improve the following legislation frameworks :� Decree No. 2008-297/PRES/PM/MEF concerning the
accounting and financial Public State Establishments (PSE) ofBurkina Faso.
� Decree No. 2008-173/PRES/PM/MEF concerning generalrules of public functioning and the delegation of public servicesin Burkina Faso.
� Decree No. 2004-191/PRES/PM/MFB concerning the generalstatus of PSE; Decree No. 2006-355/PRES/PM/MS/MESSRS/MFB concerning the particularstatus of CHU; and Decree No. 2006 356/PRES/PM/MS/
41 were found at the bulk dealer and in the hospitals. The ratio ofthe average buying price from the bulk dealer is 1.12. However,the ratio of average selling price to the public is 2.20, producing adifference of 97%. The selling price to the public is double thetotal buying price from the distributor (Table IV).
Sales revenue for medicationsTotal sales of medications during the first three trimesters of 2009in Burkina Faso hospitals during the data collection period were708,740,495 FCFA (1,080,397 Euros). Sales revenue from CHUYO accounted for 31% of total sales, followed by CHU SS(21.94%). Amongst the CHR, Banfora’s sales revenue was thehighest and Dedougou’s was lowest (Table V).
DiscussionAccording to the WHO, a hospital’s pharmaceutical productsbudget must be between 20 and 40% of the hospital’s totalbudget. In Burkina Faso, the CHU YO has a ratio of 27, but theavailability of essential pharmaceutical products was only 52% andone of the lowest of all the hospitals. The average availability ratewas 64% in the CHUs and 81.2% in the CHRs, indicating that apatient has more ease of access to these essential medications ina CHR than in a CHU during the period we conducted our study.During the same period, amongst Burkina Faso’s hospitals, theCHR of Ouahigouya presented the greatest availability of studiedmedications. In most cases, the more budget put aside for
Management
10 World Hospitals and Health Services Vol. 47 No. 1
According to the WHO, ahospital’s pharmaceuticalproducts budget must bebetween 20 and 40% of thehospital’s total budget
Buying from bulkvendor
(n=1 sale )
Hospitals’ se llingprice to the public(n=11 hospitals)
Number ofmedications
found
% difference between hospitals’ PSP and the initial cost from
the bulk vendor
GenericMedications
1.12 2.20 41 96.8%
Table 4: Comparison of the average public selling prices (PSP) and the buying price from
the bulk vendor of generic medications found in hospitals (n=41 medications of the 50
being studied)
Hospitals Percent
CHU Y O 218,3 94,166 30.81
CHU SS 155,4 99,310 21.94
BANFORA 51,78 9,700 7.31
DEDOUGOU 38,81 5,440 5.48
DORI 44,94 5,431 6.34
FA DA 50,56 5,815 7.14
GAOUA 51,52 3,925 7.27
KAYA 49,30 4,423 6.96
KOUDOUGOU 47,90 2,285 6.76
Total 708,7 40,495 100
Sales revenue from medications sold in the first three trimesters of 2009
Table 5: Visualization of the sales revenue of medications during the first three
trimesters of 2009 in public hospitals
08-11 burkina faso:29 31/3/11 18:13 Page 10
World Hospitals and Health Services Vol. 47 No. 1 11
Management
MESSRS/MFB concerning the particular status of CHR.� Decree No. 2006- 463/PRES/PM/MFPRE/MS/MFB
concerning the organization of specific jobs from the Ministerof Health which define the attributes of a Pharmacist.
To use the following legislation for promoting hospital pharmacydevelopment:� Decree No. 2008-328/PRES/PM/MEF concerning the
organization and functioning of the rules for revenue and rulesof state and other public organization advancement.
� Decree No. 2003-372 PRES/PM/MFB concerning theconditions and modalities of the creation, management, andreduction of State run public establishments.
� Decree No. 2009-104/PRES/PM/MS concerning theorganization of the Ministry of Health.
� Decree No. 2009-108/PRES/PM/MATD/MS/MEF/MFPREconcerning the transfer of competencies and resources fromthe State to the communes in the field of health.
� Decree No. 2000-008/PRES/PM/MS from 26/01/00concerning the organization of the Hospital Pharmacy.
� To have specific essential medicine list in each hospital.� To collecte and analyze pharmaceutical data in each the
hospital every quater.� To improve pharmaceutical gouvernance, management and
policy in each hospital. �
Dr Hamado Saouadogo Pharm D, MPH and “Strategies againstemerging and infectious diseases”. He has many certificates. He isworking with the ministry of health in Burkina Faso. He is alsointernational consultant. He worked with the USA Peace Corps inBurkina Faso as Health Technical coordinator and trainer.
References
Decree No. 2008-297/PRES/PM/MEF concerning the financial and accountable program ofPublic State Establishments (PSE) in Burkina Faso
Decree No. 2008-173/PRES/PM/MEF concerning general regulation of public works anddelegations of public service in Burkina Faso
Decree No. 2004-191/PRES/PM/MFB concerning the general status of the PSEDecree No. 2006-355/PRES/PM/MS/MESSRS/MFB concerning particular status of CHUsDecree No. 2006-356/PRES/PM/MS/MESSRS/MFB concerning particular status of CHRsDecree No. 2006- 463/PRES/PM/MFPRE/MS/MFB concerning the organization of specific jobs
under the Ministry of Health and defining the attributes of PharmacistDecree No. 2008-328/PRES/PM/MEF concerning the organization and functioning of revenue
rules and rules governing State and other public organization advancementDecree No. 2003-372 PRES/PM/MFB concerning conditions and modalities of creation,
management, and reduction of State run public establishmentsDecree No. 2009-104/PRES/PM/MS concerning the organization of the Ministry of HealthDecree No. 2009-108/PRES/PM/MATD/MS/MEF/MFPRE concerning the transfer of State
competencies and resources to communes in the field of healthDecree No. 2000-008/PRES/PM/MS from 26/01/00 concerning the organization of the Hospital
PharmacySaouadogo H, Compaore M. Essential medicines access survey in public hospitals of Burkina
Faso. African Journal of Pharmacy and Pharmacology Vol.4 (6), pp.373-380, 2010Saouadogo H. Measuring medicine prices, availability, affordability and price components in
Burkina Faso. HAI/WHO. Ouagadougou, 2010WHO. Indicateurs pour le suivi de la mise en œuvre des politiquespharmaceutiques nationales. Guide pratique. WHO/DAP/94.12 : P19-30
08-11 burkina faso:29 31/3/11 18:13 Page 11
Procurement
12 World Hospitals and Health Services Vol. 47 No. 1
International overview of hospitalprocurement
ABSTRACT: This article was written by four French hospital director students at the Ecole des Hautes Etudes en SantéPublique (EHESP – School of Public Health) from a study conducted jointly with students at the Grenoble School ofManagement to present an international overview of hospital procurement methods in ten countries. An analysis of thesemethods showed that there was a general trend towards group purchasing, with some common aims in terms of costs andperformance and some differences in legislation (competition), size of the public sector and centralization ordecentralization.
In hospitals, procurement practices can reduce costs andimprove performance, releasing funds for investing in hospitalcare for the future.A study was carried out by French hospital director students at
the Ecole des Hautes Etudes en Santé Publique (EHESP – Schoolof Public Health) and students at the Grenoble School ofManagement to present an international overview of hospitalprocurement methods1 in ten countries (France, Italy, Belgium,Germany, United Kingdom, the Netherlands, Sweden, Quebec,the United States and Brazil)2.
An analysis of these methods showed that there was a generaltrend towards group purchasing, with some common aims interms of costs and performance and some differences inlegislation (competition), size of the public sector andcentralization or decentralization.
This article classifies the forms of group purchasing in thecountries studied and describes their advantages anddisadvantages for procurement practices and performance.
Classification of group purchasing The group purchasing forms were classified according to twocriteria. The first concerned the involvement of hospitals in thecreation and operation of the group purchasing organization(whether it was an independent organization supplying hospitalsor an organization set up by the hospitals it supplied). The secondcriterion was the function of the group purchasing organization(purchasing, supplier accreditation and consultancy). Theclassification shows the group purchasing forms used in thevarious countries.
Independent organizations providing services to hospitalsThis type of group purchasing organization is an independent legalentity, state-owned or not, which provides various common
MAUD FERRIER, DAVID LARIVIERE,
CLAIRE LAURENT AND ERIC ROQUE
STUDENT HOSPITAL DIRECTORS
EHESP SCHOOL OF PUBLIC HEALTH, FRANCE
services to hospitals and may involve hospitals in its management.
Independent legal entities purchasing on behalf of hospitalsThese mainly purchase goods and sell them on to the hospitals.They negotiate contracts with suppliers and make purchases onbehalf of the hospitals, taking advantage of volume pricing madepossible by grouping purchases.
In France, the Union des Groupements d’Achats Publics (UGAP– Union of Public Procurement Groups) acts for the whole of thepublic sector, enabling state-owned hospitals to purchasesupplies without requesting competitive quotations.
This form of group purchasing with state-owned nationwideorganizations also exists in Italy (CONSIP), Brazil (Federal stateprocurement services for medicaments) and England (NHS SupplyChain). In Sweden, the state procurement network,Landstingsnätverket för Upphandling (Lfu), covers the eightregions which send representatives to a national assembly. TheLfu has a complementary advisory mission, producing standardsand supplier codes of conduct. The regional procurement servicesare commissioned by the hospitals. The hospitals also have theirown procurement services.
The group purchasing corporations in Québec are owned by thehospitals which have representatives on the Board of Governorsand appoint a General Director responsible for the policy of thegroup purchasing organization. By grouping customers’purchases, they save about 30% on high value added products.The regional corporations combine to purchase medicalequipment and supplies in bulk.
There are also private purchasing organisations: in theNetherlands, the NIC (Nederlands Inkoop Centrum) is a large,highly skilled consultancy body. It acts mainly for the public sectorand has more than 150 consultants responsible for findingsolutions to procurement problems in a wide range of fields
12-14 International overview of hospital procurement - EHESP copy:29 31/3/11 19:19 Page 12

World Hospitals and Health Services Vol. 47 No. 1 13
Procurement
(equipment, information technology, energy).
Purchasing organizations providing supplier accreditationThese legally independent organisations group the purchasevolumes of their members and negotiate prices. However, thehospitals themselves make the purchases under the conditionsdefined in their contracts.
In the United States, Group Purchasing Organizations (GPO)cover most hospital requirements: pharmaceuticals, surgicalinstruments, capital equipment and office supplies. They provide arange of services: benchmarking, marketing, training programmesand insurance. The hospitals have great freedom – they can makepurchases outside the contracts, join other GPOs at any time –and are able to take part in the decisions made by the GPO(product selection). However, certain obligations may be imposedon members (minimum purchases). Most GPOs are financed bythe volume related administrative fees paid by the suppliers, whichare usually 2 to 3% of sales (the hospitals do not have to pay anymanagement fees).
Key figures on the GPOs� The number of GPOs has increased from 40 in 1974 to
900.� GPO contracts account for 70% of hospital purchases,
i.e. 150 billion dollars.� About 96% of hospitals belong to at least one GPO.� 6 GPOs are responsible for purchasing around 90% of all
contracts: Novation, Premier, HealthTrust, MedAssets,Broadlane Group and Amerinet.
In France, independent organisations – CAHPP, Helpévia andCACIC – provide supplier accreditations mainly for privatehospitals. These try to capture a share of state-owned hospitalpurchasing by grouping, drawing up requests for quotation andprocessing quotations, in accordance with the GovernmentContract Code, although currently little used.
Purchasing organizations providing consultancy and supportfunctionsThese are legally and strategically independent entities providingconsultancy for hospitals and encouraging the sharing ofexperience and methods. In the United Kingdom, Commercial
Support Units are responsible locally for the NHS procurementpolicy, pooling the members purchasing skills.
Organizations created by hospitals with a common policySome hospitals have created joint ventures to optimiseprocurement. The statutes of the organizations depend on thefounder members and may take the following forms.
Groups of hospitals making purchases on behalf of membersthrough an organization that may or may not have its own legalstatus The hospitals determine their own requirements, the grouppurchasing organisation manages the procurement procedure andproducts are delivered directly to the hospitals. There is no legalobligation for the hospitals to use the group purchasingorganisation.
This is used in Germany (purchasing cooperatives), in Belgium(IRIS-Achat) and in France (purchasing GIEs).
Supplier accreditation organisationsThe aim of this method is to source products in a way similar toGPOs, the difference being that the organization does not have aparticular legal status. The organization negotiates group pricesand the hospital members then undertake the procurementprocedures themselves.
In Brazil, the Pró-Saúde online marketplace tradesmedicaments, equipment and medical equipment by Internet onbehalf of 24 establishments. An agreement is signed between Pró-Saúde ABASH (the facilitator) and the supplier who then becomesaccredited for the marketplace. The hospital selects its suppliersand makes its purchases, which enables it to retain controlthroughout the order process.
Organisations with a common policy providing consultancy forpurchasersThese organisations have a pool of consultants and sharepractices, experience and procurement methods.
In the French public, not for profit health sector, organisationssuch as the RESHA-IDF Groupement d’Intérêt Public (GIE – PublicInterest Group) (121 members), the UNI-HA Groupement deCoopération Sanitaire (GCS – health cooperation Group) (54members) and the Consortium Achats Groupement d’IntérêtÉconomique (20 members) support collective procurementprocedures by providing technical advice and make it possible to
Function
Purchasing Supplier accreditation Consultancy and common purchasing policy
- France : UGAP - France: CACIC, CAHPP, Helpévia - United Kingdom: CSU- United Kingdom: NHS Supply Chain - USA : GPO- Italy: CONSIP - Netherlands: NIC- Brazil: Grupo des Compras Hospitalares- Sweden: Lfu
- Germany: purchasing cooperatives - USA: IHN - France: UNI-HA, RESAH IDF, Purchasing consortium- Belgium: IRIS-Achats - Brazil: Pró-Saúde - Cross-border cooperation agreement- Quebec: group purchasing corporations online marketplace
Independent organization
providing services to hospitals
Group purchasing for
several hospitals with a common
purchasing policy
Type
of o
rgan
izat
ion
Table 1: Types of organizations and their functions
12-14 International overview of hospital procurement - EHESP copy:29 31/3/11 19:19 Page 13

Conclusion Group purchasing organizations are becoming more common,even though there is no dominant type and several different formsmay exist within a country.
The new French plan focusing on hospital procurementperformance will certainly provide the opportunity for drawing onthe experience of other countries to improve national hospitalprocurement methods and continue to improve practices,perhaps by allowing the emergence of new players within thesupply chain process. �
exchange experience through secure online communities.
Group procurement methods improve performance and savemoney but they also have disadvantages Group purchasing improve performance of organizations andsave moneyGroup purchasing can save money, reducing costs by 10%–15%,depending on the country3.
In Québec, the group purchasing corporations have obtained areduction in equipment maintenance costs of 35% to 80%. InBrazil, using the BIONEXO online marketplace, five state hospitalsin São Paulo state that they save 20% on the group purchase of30 medicaments.
Group purchasing improves quality by standardising products,equipments and medical practices. The exchange of informationand experience via a working network stimulates innovation,harmonisation of practices and therapeutic treatment. In Brazil,group purchasing improves product security by preventing thepurchase of counterfeit medicaments.
Group purchasing is said to strengthen purchase managementwhile reducing the work load (simplifying procedures) and costs.Continuous contact with the suppliers promotes commitment andlong-term collaboration (confidence = quality + savings).
This is the justification in particular for group purchasing inGermany and Sweden where hospital procurement evaluationmodels (quality, price), standards and codes of conduct (humanrights, sustainable development) have been set up.
Group purchasing also improves the performance oforganisations by using skilled buyers. The hospitals share skills,practices and methods and increase “know-how”.
Group purchasing is confronted with barriers which hospitalsmust take into account when drawing up their procurementpoliciesGroup purchasing may skew the hospital market given the scopeand significant financial risks (high market concentration,monopolies or oligopolies).
In the United States, the GPOs are sometimes accused offavouring suppliers who pay high administrative fees. Certaincontractual practices of the GPOs (in particular single sourcecontracts, bundled discounts) favour major suppliers, excludingproducts from more innovative SMEs.
There seems to be a lack of competence and specialist trainingin hospital procurement, despite the increase in purchasingtraining. Purchasing is still often a secondary function, carried outmechanically. In Québec, there is a lack of skilled buyers (buyersare being recruited from abroad). In France, hospitals are startingto recruit purchasing directors and specialist buyers.
Doctors are usually opposed to the standardisation ofpurchasing, claiming that purchases must be made to suit specificlocal requirements.
The degree of group purchasing varies according to the politicalorganisation. In Italy, group purchasing is often at infra-regionallevel. In Sweden, group purchasing is at local level, depending onpolitical organisation. In these countries, group purchasing couldbe done at national level.
Group purchasing organisations can also collapse, for examplethe Dutch purchasing cooperative in Brabant, BKI – BrabantKoopt, which was created in 2008, went out of business in 2010.
Procurement
14 World Hospitals and Health Services Vol. 47 No. 1
References1. Health expenditure accounts for 16% of GDP in the United States, 11.2% in France, 10.5%
in Germany, 9.4% in Sweden and 8.7% in the United Kingdom (Source: OECD)2. Study presented at the Second International Symposium on Hospital Procurement in
September 20103. Conclusion of the Second International Public and Private Health Buyers Symposium, Issy-
les-Moulineaux, 20104. Fehosp- Federação das Santas Casas e Hospitais Beneficentes do Estado de São Paulo
12-14 International overview of hospital procurement - EHESP copy:29 31/3/11 19:19 Page 14
World Hospitals and Health Services Vol. 47 No. 1 15
Procurement
Centralized distribution: reducingownership costs by streamlininghospital logistics
ABSTRACT: All Quebecers have access to a public health system that enables them to receive high-qualityhealthcare, regardless of their individual ability to pay. With the aim of improving effectiveness and efficiencyand achieving cost savings in managing public funds allotted to the healthcare network, SigmaSanté intendsimplementing a central distribution of medical supplies needed by healthcare facilities in Montréal and Laval,Québec, as has been done in many other jurisdictions for numerous years.
It is fortunate that in the Province of Québec, all residents haveaccess to a public healthcare system that allows them to receivehigh-quality healthcare, regardless of financial status. We must,
however, bear in mind that taxpayers indirectly pay for theseservices, and that effective and efficient management of publicfunds financing the healthcare system is crucial.
In this context, SigmaSanté, a not-for-profit organization, offersa group purchase negotiation service for healthcare and socialservice centres in Montréal and Laval, which alone represent25,000 short- and long-term beds. In Québec, group purchasingin the healthcare field has existed for 50 years. Several companiessuch as SigmaSanté provide services of this nature to theprovince’s health centres.
In addition to negotiation of product prices and terms ofpurchase, a significant concern of SigmaSanté is total cost ofownership. SigmaSanté strives to reduce expenditures associatedwith purchasing logistics. It is with that aim that centralizeddistribution comes into focus.
Centralized drug distribution: a tried and proven modelCentralized distribution of drugs purchased by healthcare centresis a model in Québec that has, for several years, proven it’s worthand reliability. Indeed, since 1994, a group of pharmacists aimingto reduce the workload related to purchasing logistics introducedmeasures implementing centralized drug distribution.
Before this initiative, all drugs negotiated by SigmaSanté ordirectly by a healthcare centre were distributed by theirmanufacturers, resulting in numerous orders from severalmanufacturers and as many deliveries and invoices to process.Pharmacists thus decided to assess the impact of centralizeddistribution on their internal logistics; this study showed thatimplementation of this type of distribution could potentiallydecrease drug order processing time by 65%, generating
CHANTAL S LAURIN
CHIEF EXECUTIVE OFFICER, SIGMASANTÉ
significant annual savings in hospital logistics costs. This led to thecreation of the Québec centralized drug distribution model. Today,all healthcare centres enjoy the benefits of this approach.
Currently, SigmaSanté negotiates 88% of drugs purchased byits client institutions, representing more than 66 differentagreements with various manufacturers. The 73 memberinstitutions of SigmaSanté place their orders with a singledistributor who processes the order, ensures delivery to, andinvoices the healthcare centre. All drugs covered by theseagreements are sold at the pre-agreed price to which is added thepre-agreed distribution fee.
Manufacturers deliver their products to a single location, andhealthcare centres receive all the drugs they require by placing asingle order. Products are thus purchased at wholesale prices;logistics are simplified for all involved and environmental impactrelated to transportation, greatly reduced.
Rethinking medical supply distributionIn 2008, SigmaSanté launched a study aimed at improving itsservice package in the field of medical supplies. Collected dataanalysis indicated that expenditures of its members for purchaseof medical supplies had, over five years, increased by more than55%. This study also showed how current financial pressures hadmade institutional managers acutely aware of the importance ofefficiency in the supply chain, which requires multiple humaninterventions to ensure timely availability of supplies at the rightplace.
Beyond supply price management, several healthcare centreswished to reduce purchasing costs whilst improving quality ofservices offered to their in house customers. The centralizeddistribution model then appeared as a highly appealing solution,since it makes it possible to obtain products from multiplesuppliers whilst placing a single order to a single location, to group
15-17 Centralized distribution – lauren:29 31/3/11 19:18 Page 15
Procurement
16 World Hospitals and Health Services Vol. 47 No. 1
products in a single shipment and pay one invoice per order. Thisgain in efficiency is important to healthcare centres, who can thendevote resources to more strategic activities and better serve inhouse customers.
The chosen model The sought distribution model was developed in consultation withpurchasing and finance managers from various types of healthcarecentres. They opted for the model used for drugs distribution,where SigmaSanté acts as an agent for healthcare centres,negotiating purchase terms and product prices. However,submitted prices must be what are called “distributor prices”,which exclude order receiving, processing and delivery costs toand from each healthcare centre. According to this model,manufacturers receive a single order from the distributor, to whomthe entire order is delivered. Responsibilities are shared betweenvarious parties involved as follows:
The distributor must also be able to offer personalized servicesmeeting specific needs of certain healthcare centres as requested,i.e.:� assembly of supplies in containers or carts;� transhipment of direct purchases to consolidate deliveries;� management of private procurement agreements.
Simplified processBy entrusting supply distribution to a single party rather than to amultitude of manufacturers and distributors currently involved inthe model we are attempting to change, centralized distributionwill make it possible to limit the number of middlemen in thedistribution chain. Healthcare centres will continue to pay fordistribution services, but will be able to manage this expenditureand specify required services since the distributor, throughSigmaSanté, will be bound by contract with them.
Gradual phasing inImplementation will be spread over three years, i.e. as existingagreements between SigmaSanté and supply manufacturerscome up for renewal. The distributor will thus be able to adapt andinvest gradually, according to needs of healthcare centres. Such aphasing in greatly reduces the financial risk of the distributor, whichwill have to be taken into account by bidders in their submissions.
As in the drug sector, success of implementation rests with theapplication of rigorous management and performance monitoring
mechanisms with the Monitoring and Development Committee.The agreement provides for the creation of a Monitoring andDevelopment Standing Committee and the appointment of aproject manager for the phasing in period. Gradual implementationwill allow for adjustments as need be, without causing significantoperational problems.
A long-term perspectiveTo obtain competitive prices and make it possible for thedistributor to amortize his investment, healthcare centres mustimperatively make a long-term commitment. As the distributor willnot make significant profits in the first three years, whilstSigmaSanté renegotiates the various contracts withmanufacturers, the intended term for the distribution contract is 12years (a 7-year firm contract followed by one 3-year and one 2-year extension options). As the objective is to create a win-winbusiness partnership, the term of the contract must be reasonableboth for the healthcare centres and the distributor.
Logistic savings firstAbove all, the main objective of centralized distribution is notreduction of distribution expenses, but increased awareness andcontrol over these expenses, currently unknown as they areincluded in product prices. Targeted savings pertain to purchasinglogistics costs, which are unavoidable, even though they differfrom one healthcare centre to the other: � reducing administrative costs resulting from high transaction
volumes: erroneous orders, back orders, incomplete deliveries,high inventory levels, outdated goods, invoice discrepancies,invoicing volumes;
� promoting e-business development, allowing for acceleratedtransaction processing and ensuring information quality, by
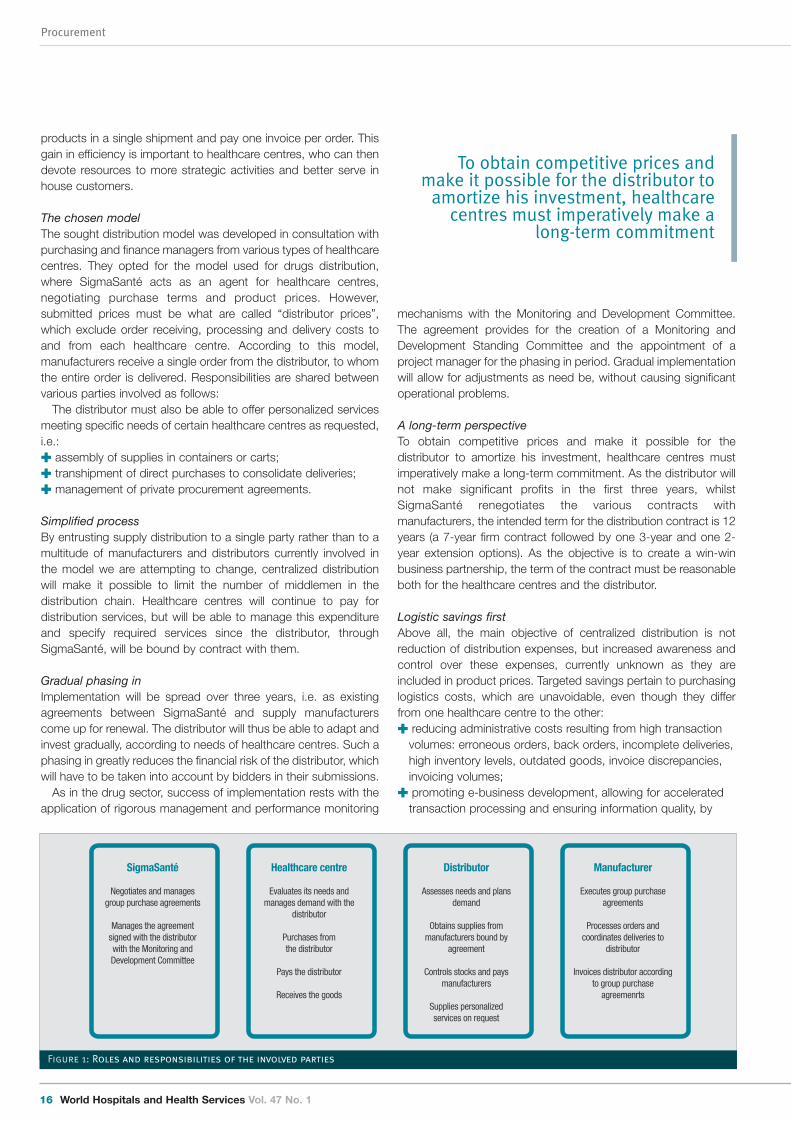
Distributor
Assesses needs and plans demand
Obtains supplies from manufacturers bound by
agreement
Controls stocks and pays manufacturers
Supplies personalized services on request
Healthcare centre
Evaluates its needs and manages demand with the
distributor
Purchases from the distributor
Pays the distributor
Receives the goods
Manufacturer
Executes group purchase agreements
Processes orders and coordinates deliveries to
distributor
Invoices distributor according to group purchase
agreemenrts
SigmaSanté
Negotiates and manages group purchase agreements
Manages the agreement signed with the distributor with the Monitoring and Development Committee
Figure 1: Roles and responsibilities of the involved parties
To obtain competitive prices andmake it possible for the distributor to
amortize his investment, healthcarecentres must imperatively make a
long-term commitment
15-17 Centralized distribution – lauren:29 31/3/11 19:18 Page 16
World Hospitals and Health Services Vol. 47 No. 1 17
Procurement
months. We rely on the competitive factor, the term of the contractand the extraordinary opportunity afforded by implementation ofsuch a service for a party specialized in the distribution sector, toobtain fair and equitable prices for all parties involved.
Obviously, creation of such a distribution model will offendcurrent practices; this will cause fears to healthcare centres,industry manufacturers and distributors. At the time ofestablishment of centralized drug distribution, several key successfactors made it possible to counter these obstacles and ensuresuccess of the project: � a drug management committee made up of determined and
concerned pharmacists;� leadership of the committee’s chairman;� team spirit of institutional pharmacists vis-à-vis industry
pressures;� well-defined practice sector;� one spokesperson per healthcare centre.
In the case of medical supplies, the situation is somewhatdifferent. Because of the large variety of products, manystakeholders with different areas of specialization are affected bythe impact of the model, which makes team spirit and unanimitymore difficult to attain. Thus, industry pressures have a largerimpact, which has to be counterbalanced to allay fears anduncertainties.
In January 2011, SigmaSanté formally asked all institutionalleaders to grant it a clear mandate to allow it to proceed with thisproject with proper authority.
Positive responses will decide whether implementation of thismodel can be applied to the medical supply sector. �
Chantal S Laurin is Chief Executive Officer of SigmaSanté, a jointprocurement corporation that acts as broker for several Québechealthcare facilities, and whose annual transactions exceeds c$800million. Mrs Laurin has previously held the position of ChiefExecutive Officer of Montréal International Airport, as well asvarious key positions with Hydro-Québec and Transport Canada.
reducing human intervention;� savings resulting from the use of best practices: off-peak
deliveries, consolidation of volumes, use of e-business, promptpayment, etc.;
� subcontracting for occasional needs and low value-addedservices.
Centralized distribution also makes it possible for suppliers toachieve savings: � by filling a single order for all healthcare centres, they avoid
delivering at multiple addresses, reducing mileage, shorteningdelivery times and reducing environmental impact;
� decreasing the number of invoices to be processed savesvaluable time.
Better procurement practices and efficient logistics are the bestmeans of guaranteeing fair costs.
Competitiveness for a fair priceThe contract will be awarded to the lowest qualified bidder. Thequalification process has been well planned with representativesfrom various healthcare centres, and criteria are clearly defined.We rely on the competitive factor and the interest for the projectamong distributors (specialized in this sector or not) to obtain a fairand equitable contract price.
Countering resistance As no initial investment is necessary on the part of healthcarecentres, risk is kept to a minimum. The selected distributor willinvest funds gradually, over three years, as contracts come up forrenewal. Naturally, healthcare centres are anxious to know thecost of distribution expenses, which will be disclosed only at thetime of the bids. We will also know, as agreements are beingrenewed, the amount of price reductions which will allow us to freeup funds which will be used to pay our distributor.
The cost of the distributor’s services will become known as partof the tendering process which we plan to initiate in the upcoming
15-17 Centralized distribution – lauren:29 31/3/11 19:18 Page 17

Procurement
18 World Hospitals and Health Services Vol. 47 No. 1
The challenges of collaborativeprocurement in the healthcare sector
ABSTRACT: The article points out the new challenges of collaborative procurement in the healthcare sector.The research focuses on the optimization of healthcare purchasing through the reduction of costs withoutany prejudice to the quality of healthcare performances, but also assuring rationalization and innovation.Moreover, the importance of collaborative procurement is particularly evident considering the ensuingvalorization of the diverse professional skills and their use of strategic purchasing power in theirrelationships with economic operators.
Purchasing aggregation and the professionalization in thepublic procurement field have become two of the mostimportant challenges for public purchasers and for
procuring authorities in general and particularly in the healthcaresector1.
The importance of the public procurement is indeed evident to-date. It is worth mentioning that the procurement market canreach approximately 15% of EU’s GDP and account up to 20% ofdeveloping countries’ GDP2. Such considerable percentagedetermines a strong purchasing power that can be driven towardsinnovation and the creation of value.
Nonetheless, an overall vision of public organization strategicpower is still missing, probably as a widespread fragmentation ofprocuring entities is still present. This is often an obstacle to acomplete and comprehensive vision of the possible strategies ofpublic procuring policies. Thus, the promotion of every form ofcollaborative procurement so as to obtain instruments to steer theuses of such considerable resources is of the utmost importance3.
In general terms, every government, local authority and publicorganisation, utility and agency at any level is endowed withcontractual autonomy and can purchase according tointernational, European and national rules depending on the case,pursuing the goal of obtaining the best value for money4. However,the demand of reducing public expenditure, even as a result of theeconomic crisis, as well as the goal of the European Union toincrease competition in the public market can improve the value ofany form of collaborative procurement and of professionalization,thus achieving a wider and more comprehensive vision of thedifferent market conditions and characteristics.
Nevertheless, in order to create an internal market, theEuropean legislator set common rules for the Member Statesreferring to the principles and procedures of public contractsawarding5. An effective internal market in the supply and services
GABRIELLA MARGHERITA RACCA
FULL PROFESSOR OF ADMINISTRATIVE LAW, DEPARTMENT OF LAW FOR
ECONOMICS, UNIVERSITY OF TURIN (ITALY)
sectors has to be accomplished yet, in the healthcare sector too.Healthcare purchasing is surely a strategic sector in the area ofpublic procurement. The reduction of resources seems to requirethe development of public procurement policies in order tomaintain a high level of protection (as to the healthcareperformances), taking into account the new costs associated tothe evolution of medical science, too. In fact, collaborativeprocurement optimizes public purchasing, especially, but not only,thanks to the economy of scale it achieves.
Purchasing aggregation entails reduction of costs andconsequently may facilitate the achievement of such goalsbecoming creator of value. These costs concern on the one handthe prices of goods and services – for each unit – and, on theother hand, the awarding phase of public procurement (includinghuman resources savings, both in terms of time and money). Thelarge volumes purchased determine a higher purchasing power byassuring the effectiveness of the public action and by acquiringhealthcare products (drugs, equipments, medical devices) andservices at better market conditions and at the best value formoney. Furthermore, public bodies may enjoy the benefits arisingfrom the reduction of costs and time related to autonomous awardprocedures (according to a rough calculation the cost of anautonomous award procedure can reach €20,000). Moreover,purchases aggregation entails the reduction of human resourcesinvolved in the award procedures thus allowing – with a view toimproving the control of the performance phase – theirassignment to the task of monitoring contracts performance andpossible infringements6.
Purchases aggregation is not only an instrument to reducecosts, as it can drive innovation, by promoting competitionbetween economic operators. Indeed, collaborative procurementdoes not harm the development of competition, as it has beenclaimed, rather being an instrument that helps to improve its value
18-20 collaborative procurement - racca:29 31/3/11 18:56 Page 18

World Hospitals and Health Services Vol. 47 No. 1 19
Procurement
ensuring a competitive quality level. Regulatory rules at Europeanlevel have been introduced in 2004, so as to rationalize publicprocurement, providing a European definition of CentralPurchasing Bodies7. In fact, it has been considered that thosetechniques can help increase competition and streamline publicpurchasing in view of the large volumes purchased by theseorganizations. Obviously, collaborative procurement affects therole played by the contracting authorities, as long as anaggregated awarded procedure differs greatly from anautonomous one. In other words, the purchaser is not a personacting individually anymore, since, to the contrary, he is part of ateam of several people with different professional skills (technical,methodological, economic, legal, engineering etc.). Those skillsare often out of reach for most contracting authorities within thehealthcare sector and require the implementation of forms ofaggregation8.
In this context, an organization such as a central purchasingbody can enhance these skills and implement some newpurchasing techniques such as those defined by the 2004European Directives (framework agreements9, electronic auctions,dynamic purchasing systems), with the aim of managing better thecoordination of public demand, by referring to more complexaward procedures.
Moreover, in the most evolved legal systems, central purchasingbodies conduct extensive studies in the relevant markets that thepurchasers cannot carry out on their own. The knowledge of themarket structure enables the outlining of suitable procurementprocedures, in order to fill the gap of common standards to ensurethe monitoring of the exact performances, to define more preciselythe sum of lots included in the procuring procedures or to identifythe best moment to launch a new award procedure or aframework agreement10. This seems to ensure the expansion andthe strengthening of competition and it helps promote the entry ofnew firms (new economic operators) on the market (also SMEs).With regard to this latter aspect, we may recall that the “SmallBusiness Act Europe” improves the activity of SMEs in accordancewith the principle “Think Small First”11. This does not mean that theaward procedures should remain below the European threshold,but, on the contrary, it entails the creation of award procedureswith lots that are territorially and quantitatively adapted to thesystem of the providers, by identifying the territorial level that isoptimal for the aggregation and by ensuring the participation ofmore innovative SMEs, even from abroad12.
The optimal level for collaborative procurement in the healthcaresector is normally identified by the kind of goods and servicesneeded. Therefore it may be at a local, regional, national level and,under a more innovative perspective, at a European level. Indeed,geographic regroupings can be identified aiming at federatinghospitals that operate on the same territory, as well as regroupingsset by nature of the organization (because of the homogeneous
characteristics they present). This does not exclude forms ofcentralization based on the creation of networks in which eachorganization can specialize itself in order to purchase certaincategories of specific goods and services, even on behalf of others(one for drugs, the others for consumable medical devices).
The implementation of policies of collaborative procurement cannot only contribute to the increase of the purchasing power ofpublic bodies, but also to the improvement of the quality of publicexpenditure. More specifically, the proper use of the publicdemand can drive the relevant market to a change in order topositively orient the choices of the enterprises, thus rising socialand environmental standards and achieving a better and moresustainable quality of life for citizens13.
However, it can be pointed out, that, on one hand, thepercentages of aggregated purchases are different from State toState and, on the other hand, that physicians' preferences can -attimes- make such aggregation more difficult, especially withregard to those operator-dependent products (i.e. any kind ofmedical device)14. Nevertheless, even the latter hypothesis doesnot exclude centralization, as the possibility of collecting data andcataloguing suppliers, also by means of more complex frameworkagreements with more economic operators can be considered, byinvolving doctors too in the definition of the technicalspecifications.
The prospect aimed at pooling public purchases could bedeveloped through the creation of a network of Europeanpurchasers, composed by Central Purchasing Bodies orProfessional Buying Organizations. Thus, the evaluation ofbenchmarks comparing the prices of equivalent products (orservices) becomes a foreseeable possibility, in order to set sharedcontractual terms designed for the promotion of a true Europeancompetition.
Indeed, if the European Union pursues the goal of theachievement of a internal market, it should be noticed that thepublic demand still results highly fragmented compared to theoffer of companies, which seems to be more structured. Forexample, referring to the health products market sometimes andfor certain categories of products only few suppliers (even on aworldwide level), who organized themselves by creating supplychains in order to meet the public demand, can be identified.Moreover, in a few years the computerization (and the data filingsystem) of these complex procedures will be complete. It willradically change the possibilities of comparing services and pricesobtained, as well as the possibility to set benchmarks. To-date forexample, in Italy, the costs of medical devices are extremelydifferent depending on the hospital, even in the same area. Thus,the Ministry of Health encouraged centralization of purchases bymeans of a government bill aimed at creating a database ofmedical devices, in order to control consumption and expenditure
The implementation of policies ofcollaborative procurement can not
only contribute to the increase of thepurchasing power of public bodies,but also to the improvement of the
quality of public expenditure
Purchases aggregation is not onlyan instrument to reduce costs, asit can drive innovation, bypromoting competition betweeneconomic operators
18-20 collaborative procurement - racca:29 31/3/11 18:56 Page 19

of products.Computerization seems to ensure transparency and controls on
the quality of goods and services15. This control will not only beperformed on the award procedure. Its scope will include thecontrol of the quality of healthcare provided by doctors in relationto quality and the quantity of devices and treatments provided. Inthis context, the role of central purchasing bodies could reallybecome strategic since the exchange of information – supportedby electronic tools – seems to allow for a coordination to developcommon contract terms which may, in turn, lead to a truly internalmarket in which the best hospital purchasing practices could beidentified and innovative solutions could be developed16.
The development of standard contract models (with reference todifferent categories of purchase), and of uniform contract termsincluding reference to the execution phase of contracts andpayments can promote the participation of a higher number ofcompanies.
By way of example, in Italy it was noted that the payment termsfor health providers can reach almost 800 days. This situationsurely discourages participation in public procurement. From thisperspective it would be, in the European area, take the forms ofexperimentation and fruitful cooperation with a view to comparingcontractual conditions, achieving coordination of procedures,defining models of typical contracts, and perhaps, initiating jointaward procedures17. This cooperation could achieve the definitionof a draft European Directive proposed by public purchasers (notby the high European institutions) who can define models ofuniform contracts, defining all aspects, from award procedures tothe execution of the contract. This perspective seems tocontribute to the development of an effective competition amongEuropean suppliers. Such competition should improve the qualityof healthcare performances in the public interest and collaborativeprocurement could really become creator of value18. �
Gabriella Margherita Racca, PhD, is Full Professor of AdministrativeLaw, Department of Law for Economics, University of Turin (Italy).Her teaching and research interest are in public procurement,environmental law, healthcare organizations, public authorities’ andcivil servants’ liability, judicial review.
Procurement
20 World Hospitals and Health Services Vol. 47 No. 1
References1. Racca, G. M., (2008). Le modalità organizzative e le strutture contrattuali delle aziende
sanitarie, in Pioggia, A. – Dugato, M. – Racca, G. M. – Civitarese Matteucci, S. (eds.), Oltrel’aziendalizzazione del servizio sanitario, Milano: Franco Angeli (pp. 264-297), that is theoutcome of the project which the Unit of the University of Turin (Head of research Prof.Gabriella M. Racca: [email protected]) is developing as regards "Contractualautonomy of health authorities: object limits, organizational structures and cost efficiency",as part of the Research Program of Relevant National Interest (PRIN) on "Health serviceorganization in a comparative perspective: the Italian model of Health Agencies’ structure incomparison with other organizational models" together with the research Units of theUniversity of Perugia, University IUAV of Venice and University “G. d’Annunzio” of Chieti-Pescara; see also: Racca G. M., (2010). Collaborative procurement and contractperformance in the Italian healthcare sector: illustration of a common problem in Europeanprocurement, Public Procurement Law Review. (pp.119 e ss.).
2. Commission (Ec) - Internal Market, Public procurement indicators 2008, April 28, 2010.3. Racca, G. M., (2010). Professional buying organisations, sustainability and competition in
public procurement performance, proceeding for 4th International Public ProcurementConference (IPPC 2010) – Seoul (Korea); Schneller, E. S., Role of Group Purchasing in theUS, proceeding at 2ème symposium International, Paris 8 and 9 September 2010; Rooney,C., Pooling Hospital Procurement through Group Purchasing Organizations (GPOs): The U.S.Experience, proceeding at 2ème symposium International, Paris 8 and 9 September 2010.See also: Schneller, E. S., Smeltzer, L. R., (2006) Strategic management of the Health CareSupply Chain, Jossey-Bass, San Francisco; Schneller, E., (2009). The value of Group
Purchasing – 2009: Meeting the Needs for Strategic Savings, in Health care SectorAdvances.
4. Racca, G. M., (2010). La professionalità nei contratti pubblici della sanità: centrali dicommittenza e accordi quadro, in Foro amm. - C.d.S. (pp. 1727 ss).
5. European Parliament and of the Council Directive 18/2004 of 31 March 2004 on thecoordination of procedures for the award of public works contracts, public supply contractsand public service contracts [2004] O.J. L134/114. See also: Commission (EC), DGEnterprise and Industry, The lead market initiative (2009).
6. Cavallo Perin, R., Racca, G. M., Albano, G. L., (2010) The safeguard of competition in theexecution phase of public procurement, Quaderni Consip, VI.
7. See art. 11 (2) of European Parliament and of the Council Directive 18/2004 of 31 March2004 on the coordination of procedures for the award of public works contracts, publicsupply contracts and public service contracts [2004] O.J. L134/114: “Contracting authoritieswhich purchase works, supplies and/or services from or through a central purchasing bodyin the cases set out in Article 1(10) shall be deemed to have complied with this Directiveinsofar as the central purchasing body has complied with it”.
8. Legouge, D., (2010). Secteur hospitalier et médico-social public: vers de nouvelles stratégiesd’achat de groupe, in Contrats Publics, July - August. (pp. 43 ss.); Cormier, M., (2006).Mutations et enjeux des coopérations hospitalières, Actualité Juridique Droit administratif.(pp. 416 ss.).
9. Pongérard-Payet, H., Bangui, T., (2007). La procédure de l'accord-cadre : un nouvelinstrument du droit de la commande publique, Actualité Juridique Droit administratif. (pp.1055); De Géry, P., Schmidt, P., (2007). Les accords cadres, édition du Moniteur, Paris. (pp.117 ss.).
10. Arrowsmith, S., (1999). Framework Purchasing and Qualification Lists under the EuropeanProcurement Directives, Public Procurement Law Review. (pp. 115-146 and 168-186);Arrowsmith, S., (2005). The Law of Public and Utilities Procurement (2nd ed) London: Sweet& Maxwell; Arrowsmith, S., (2006). The Past and Future Evolution of EC Procurement Law:From Framework to Common Code?, Public Contract Law Journal. (pp. 337 ss.); Arrowsmith,S., (2009). Reform of the UNCITRAL Model Law on Procurement: Procurement Regulation forthe 21st Century, Eagan:West; Arrowsmith, S., Kunzlik, P., (2009). Social and EnvironmentalPolicies in EC Procurement Law: New Directives and New Directions, Cambridge: CambridgeUniversity Press; Bovis, C. H., (2008). EU Public Procurement Law, Cheltenam: Edward ElgarPublishing Limited; Chard, J., Duhs, G., Houlden, J., (2008). Body beautiful or vile bodies?Central purchasing in the UK, Public Procurement Law Review. (NA26); Edler, J., Georghiou,L., (2007). Public procurement and innovation – Resurrecting the demand side, Researchpolicy (pp. 949-963); Garcia, R. H., (2009). International public procurement: a guide to bestpractice, London: Globe Law and Business; Yukins, C. R., (2009). Use and Regulation ofElectronic Reverse Auctions in the United States, in Arrowsmith, S. (eds.), Reform of theUNCITRAL model law on procurement: Procurement regulation for the 21st century,Danvers: Thomson Reuters/West. (pp. 469-489); Yukins, C., (2008) Are IDIQs inefficient?sharing lessons with European framework contracting, Public Contract Law Journal. (pp.546 ss.); Bowsher, M., John, L. E., (2009). The use (and abuse?) of framework agreementsin the United Kingdom, in García, R.H. (ed.) International Public Procurement, (pp. 356 ss.);OGC, Framework Agreements: OGC Guidance on Framework Agreements in the newProcurement Regulations (January 2006)¸Commission (Ec), Explanatory Note – FrameworkAgreements – Classic Directive, 14 July 2005; Arrowsmith, S., (2006). Implementation of thenew EC procurement directives and the Alcatel ruling in England and Wales and NorthernIreland: a review of the new legislation and guidance, Public Procurement Law Review (pp.96-97).
11. Commission (Ec), “Think Small First” - A “Small Business Act” for Europe, COM(2008) 394Final, June 25, 2008.
12. Commission (Ec), European code of best practices facilitating access by SMEs to publicprocurement contracts, SEC(2008) 2193, June 25, 2008.
13. Racca, G. M., (2010). Aggregate models of public procurements and secondaryconsiderations, in The Law of Green and Social Procurement in Europe, Caranta, R. e Trybus,M. (eds.), Copenhagen. (165 ss.); McCrudden C., (2007). Buying Social Justice: Equality,Government Procurement, & Legal Change, Oxford. (114 e ss.); Commission (Ec), Publicprocurement for a better environment, COM(2008) 400 Final, July 16, 2008.
14. Montgomery, K. and Schneller, E. S., (2007). Hospitals’ Strategies for Orchestrating Selectionof Physician Preference Items, The Milbank Quarterly, Vol. 85, No. 2. (pp. 307–335).
15. Commission (EC), Green paper on expanding the use of e-Procurement in the EU, October18, 2010. Commission (EC) - Internal Market, Study on the evaluation of the Action Plan forthe implementation of the legal framework for electronic procurement - Analysis,assessment and recommendations, July 9, 2010.
16. Mourier A., (2010). Compétences managériales et modernisation de la fonction achat dansles hôpitaux public français, in Techniques hospitalières, July - August. (pp. 29 ss.); Baily P.,Farmer D., Jessop D., Jones D., Purchasing Principles and Management, London, PitmanPublishing, 1994.
17. Racca, G. M., (2008). Le modalità organizzative e le strutture contrattuali delle aziendesanitarie, in Pioggia A. – Dugato, M. – Racca, G. M. – Civitarese Matteucci, S. (eds.), Oltrel’aziendalizzazione del servizio sanitario, Milano: Franco Angeli (pp. 264-297).
18. Legouge, D., (2010). Fonction achat: une créatrice de valeur pour l’hôpital et le secteurmédico-social, in Revue hospitalière de France, July - August. (pp. 28 ss.).
18-20 collaborative procurement - racca:29 31/3/11 18:56 Page 20

World Hospitals and Health Services Vol. 47 No. 1 21
Procurement
e-procurement in hospitals
ABSTRACT: This article describes the history, current status, advantages of and oppositionto the implementation of e-procurement in hospitals and examines the results of itsimplementation in a psychiatric hospital.
Portals, market places and electronic purchasing – some ofthe names by which we know e-procurement – came intobeing with the internet boom at the turn of the millennium.
Today it is possible to identify the real potential of e-procurementcompared to its imagined applications at a time when neither thewidespread use of the internet nor the organisations wanting toimplement it were sufficiently advanced.
Over the years, electronic commerce has become widespread,and there are now sectors that could not exist without the use ofthis technology. The health sector, due to its complexity,idiosyncrasies and perhaps its own inertia, took longer than othermore enterprising sectors to incorporate information technologyinto its business. But we believe that due to the advances ininternet usage as well as in e-procurement software – though bothat different speeds – the health sector is now ready to efficientlyincorporate this technology into its hospitals.
Purchasing in hospitalsBuying all the goods a hospital needs to provide its services in anefficient manner is a complex process. As outlined in the figurebelow, the process includes selecting the appropriate products torequest from the suppliers, negotiating, storage, distribution,correct usage to meet patient needs and evaluation of the results,which should influence the selection of new products andsubsequent purchases1.
In Spain, total healthcare spending in 2008, according to themost recent consolidated data, was €82,064 million (M), 8.2% ofGDP. Spending on goods and services, 25%, reached €20,516 Mof which 70% was on medical and non-medical goods, €14,361M. Considering pharmaceutical products, which should beincluded in hospital spending, the figure rose to €20,000 M. Theseare impressive figures and any improvement in the quality of whatwe buy, how we buy, from whom we buy and at what price we buyis fundamental to both financial results and hospital efficiency.
Hospitals are complex organisations not only because of theparticular processes that occur there and the low efficiency ofthese processes in most of them, but also the conditions in which
DR JULIO VILLALOBOS HIDALGO
ASSOCIATE PROFESSOR, HEALTH SCIENCE STUDIES,
INTERNATIONAL POSTGRADUATE INSTITUTE
UNIVERSIDAD ABIERTA DE CATALUÑA (UOC) (OPEN UNIVERSITY
OF CATALONIA)
DR JOAN ORRIT
MANAGING DIRECTOR, BENITO MENNI HOSPITAL
D JUAN PABLO VILLALOBOS
OPERATIONS DIRECTOR, BIONEXO IBÉRICA SA
they are produced2: � Hospitals are businesses, which in most cases provide
services 24 hours a day, 365 days a year.� They often have a high number of references in their
catalogues, between 5,000 and 10,000 per hospital. � They usually have a large number of suppliers. � They have limited supplier selection and prioritisation criteria� Most of the time the staff in the purchasing department are
expected to process the orders. � They have little information on the market and suppliers. � Purchasing plans are based on the annual volumes of
previous policies.� They have little IT support. � They do not thoroughly track purchases. � They often have multiple and generally poorly designed
warehouses.� They have high stock levels.� Internal distribution is slow. � They produce a large number of urgent requests.� There is poor coordination with medical and paramedical staff
concerning the selection of materials. � There is great variability and little standardisation of materials. � They often have little information on usage and costs.
In the EU-10 countries, 98% of hospitals have access to theinternet and 78% to broadband. Some 75% of medium-sizedhospitals use e-procurement services, but only 27% of them usethis system for over 25% of their orders3.
We believe that both internet usage and organisationaladvances in our hospitals permit the efficient use of e-procurement in these establishments. The current economicpressure on increasing efficiency provides a great opportunity forhospitals to start making their purchases electronically.
Benito Menni hospital – a successful caseBenito Menni Hospital is a psychiatric hospital belonging to theCongregation of the Sisters Hospitallers of the Sacred Heart of
21-23 eProcurement - Villlalobis:29 31/3/11 19:17 Page 21
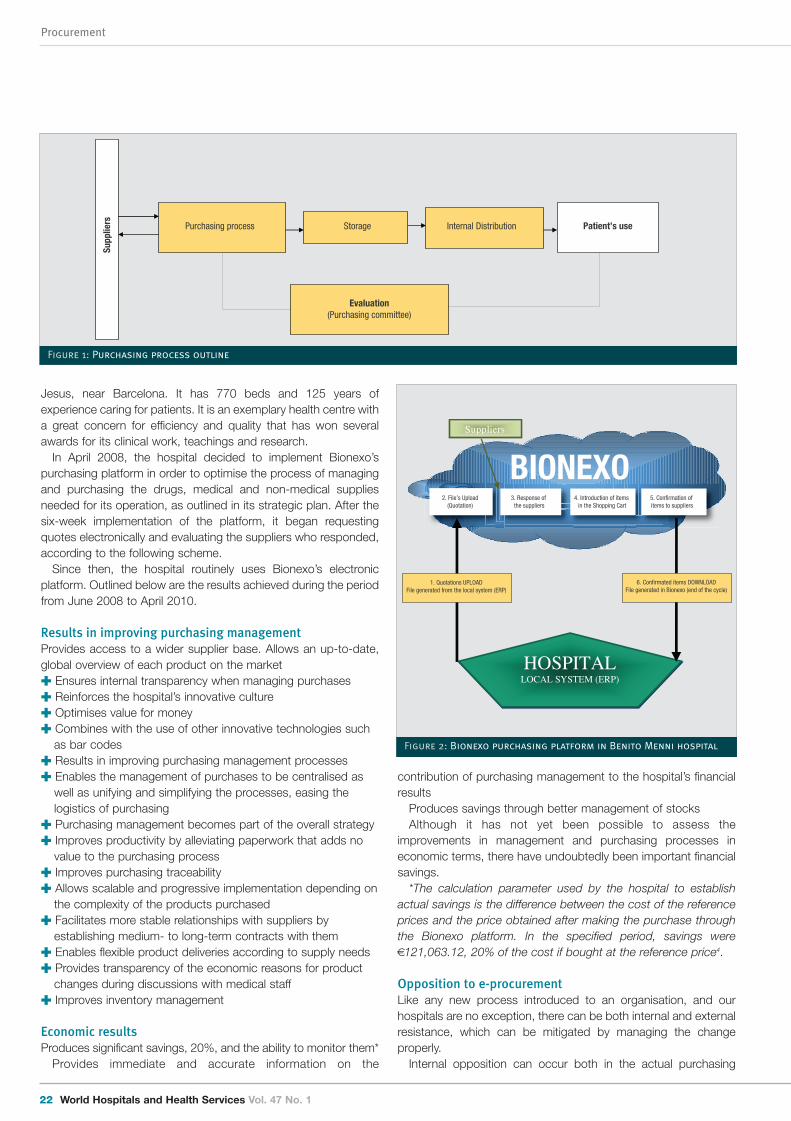
Procurement
22 World Hospitals and Health Services Vol. 47 No. 1
Jesus, near Barcelona. It has 770 beds and 125 years ofexperience caring for patients. It is an exemplary health centre witha great concern for efficiency and quality that has won severalawards for its clinical work, teachings and research.
In April 2008, the hospital decided to implement Bionexo’spurchasing platform in order to optimise the process of managingand purchasing the drugs, medical and non-medical suppliesneeded for its operation, as outlined in its strategic plan. After thesix-week implementation of the platform, it began requestingquotes electronically and evaluating the suppliers who responded,according to the following scheme.
Since then, the hospital routinely uses Bionexo’s electronicplatform. Outlined below are the results achieved during the periodfrom June 2008 to April 2010.
Results in improving purchasing management Provides access to a wider supplier base. Allows an up-to-date,global overview of each product on the market � Ensures internal transparency when managing purchases� Reinforces the hospital’s innovative culture � Optimises value for money � Combines with the use of other innovative technologies such
as bar codes � Results in improving purchasing management processes � Enables the management of purchases to be centralised as
well as unifying and simplifying the processes, easing thelogistics of purchasing
� Purchasing management becomes part of the overall strategy � Improves productivity by alleviating paperwork that adds no
value to the purchasing process � Improves purchasing traceability� Allows scalable and progressive implementation depending on
the complexity of the products purchased� Facilitates more stable relationships with suppliers by
establishing medium- to long-term contracts with them� Enables flexible product deliveries according to supply needs� Provides transparency of the economic reasons for product
changes during discussions with medical staff � Improves inventory management
Economic results Produces significant savings, 20%, and the ability to monitor them*
Provides immediate and accurate information on the
contribution of purchasing management to the hospital’s financialresults
Produces savings through better management of stocksAlthough it has not yet been possible to assess the
improvements in management and purchasing processes ineconomic terms, there have undoubtedly been important financialsavings.
*The calculation parameter used by the hospital to establishactual savings is the difference between the cost of the referenceprices and the price obtained after making the purchase throughthe Bionexo platform. In the specified period, savings were€121,063.12, 20% of the cost if bought at the reference price4.
Opposition to e-procurementLike any new process introduced to an organisation, and ourhospitals are no exception, there can be both internal and externalresistance, which can be mitigated by managing the changeproperly.
Internal opposition can occur both in the actual purchasing
Purchasing process Storage Internal Distribution
Evaluation(Purchasing committee)
Supp
liers Patient’s use
Figure 1: Purchasing process outline
BIONEXO
Suppliers
HOSPITALLOCAL SYSTEM (ERP)
1. Quotations UPLOADFile generated from the local system (ERP)
6. Confirmated ítems DOWNLOADFile generated in Bionexo (end of the cycle)
2. File’s Upload(Quotation)
3. Response of the suppliers
4. Introduction of items in the Shopping Cart
5. Confirmation of items to suppliers
Figure 2: Bionexo purchasing platform in Benito Menni hospital
21-23 eProcurement - Villlalobis:29 31/3/11 19:17 Page 22

World Hospitals and Health Services Vol. 47 No. 1 23
Procurement
Dr Julio Villalobos Hidalgo Academic Director and AssociateProfessor of Health Science Studies at the Open University ofCatalonia and Managing Partner of Bionexo Ibérica S.A. Doctor inMedicine and Industrial Engineering. Specialist in Intensive Care.Diploma in Hospital Management. General Manager of public andprivate hospitals. Advisor and consultant to national andinternational companies. Director of the journal for La SociedadEspañola de Directivos de la Salud [The Spanish Society of HealthExecutives].
Dr Joan Orrit Clotet Managing Director of Benito Menni MentalHealthcare Institute, Sant Boi de Llobregat (Sisters Hospitallers). Chairman of the Mental Health Council for the Unió Catalanad’Hospitals. Academic Contributor ESADE (Barcelona) in the areasof Accounting and Entrepreneurship. Doctor in Medicine. MBAfrom ESADE. PDG [General Manager Programme] from IESE.Masters in Public Health from the Universidad Autónoma deBarcelona.
Juan Pablo Villalobos Operations Director of Bionexo Ibérica S.A.Degree in Marketing and Administration. Has carried out numerousmarket research studies for a variety of companies, particularly inthe fields of new technology, pharmaceuticals and the healthcaresector.
department as well as among the health professionals who areinvolved in the selection of materials.
In the first instance, this comes from a natural resistance to anychange and to the incorporation of new technology, which can beperceived as a threat to their jobs. In general, after a period oftraining, most people adapt and become the strongest advocatesof the new system, as it frees them from repetitive, bureaucratictasks and allows them to focus on more valuable assignmentssuch as negotiating the purchasing process.
In the second instance, health professionals may see thechanges as a loss of control to those in the purchasingdepartment. The latter benefit from more information about theproducts and can therefore expand on their arguments,sometimes with little consideration for scientific evidence, andintroduce cost as a definitive variable in the final selection. After aperiod in which medical staff are given further information, theyoften become, despite exceptions, among the strongestadvocates of the new system, which allows them to use betterproducts while making significant savings.
External opposition comes from the suppliers, because theincrease in and availability of knowledge at the hospital producesgreater competitiveness – and a better prepared institution isharder to negotiate with. Adequately managing the change isimportant in the case of suppliers and should be based onpresenting the technology as a profitable transition for all parties.Although the suppliers will face increased competition, they willalso have more clients to whom they can offer their products,without any additional financial cost, and will no longer have to limittheir sales to a specific time or place due to access to the internet.Moreover, as with the hospital, they can reduce transaction costs,alleviate paperwork and improve efficiency of their sales process.The uptake of e-procurement in other sectors renders invalid anyarguments against the technology being too new, unsafe orunreliable.
The Benito Menni Hospital has successfully managed thetransition as both professionals and suppliers now view theplatform as a tool that enables them to improve their workefficiency; platform implementation is viewed very positively, asdiscussed in the attained results.
Looking aheadWe believe that the implementation of information technology andparticularly online procurement is inevitable, as is occurring inother sectors providing services to citizens.
The advantages of implementation mean hospitals not onlyimprove efficiency in the purchasing process, by improving qualityand reducing costs, but also gain transparency, on-going auditingand increased knowledge, allowing health professionals toparticipate more fully and collectively in selecting the materials forpurchase.
The initial opposition that can arise from suppliers will, webelieve, lessen once the procedure becomes more widespread:their clients, the health institutions, increase in number and theiroperational costs diminish.
The decision to introduce e-procurement in hospitals is astrategic decision and should therefore be taken at managementlevel in the institution, by involving senior management, in additionto members of the purchasing department, who should clearlyunderstand the aims of implementation. �
References1. Villalobos H.J. Las compras electrónicas en las instituciones para la atención de la salud [E-
procurement in health care institutions]. Agathos magazine. Social healthcare and socialwelfare. Year 8, No 2, June 2008; 22-27
2. Soto José. Módulo Gestión de la Logística [Logistics Management Module]. Masters inSenior Health Management. 2004.
3. European Commission. ICT and e-Business in Hospital Activities 2006. E-Business Watch. 4. Hospital Benito Menni. Bionexo Ibérica. First edition of La Unió prize for management
innovation 2010.
21-23 eProcurement - Villlalobis:29 31/3/11 19:17 Page 23
Procurement
24 World Hospitals and Health Services Vol. 47 No. 1
The value of group purchasingorganizations in the United States
ABSTRACT: This article examines the valuable role of group purchasing organizations (GPOs) in hospital purchasing in theUnited States. For over 100 years old GPOs have helped hospitals and other health care providers realize savings and createcontracting efficiencies by aggregating purchasing volume to negotiate discounts with manufacturers, distributors and othervendors. The US has recently enacted a series of healthcare reforms to correct some of the historical concerns regarding cost,quality and access. GPOs are expected to continue to play a critical role in the business of hospital purchasing and maypotential export that other countries may wish to examine.
The rising cost of healthcare goods and services in the UnitedStates is an issue with enormous consequences forpolicymakers and patients alike. For example, the US
federal government spends approximately 25% of its annualbudget on health care matters. This figure is only expected togrow in the future due to the increasing costs associated withmedical technology and an aging population. These factorscombined likely ensure that cost containment will become andremain a key policy objective for both public and private sectorhealth care supply chains. This article will examine one aspect ofthis enormously important and complicated issue: the valuablerole of group purchasing organizations (GPOs) in the hospitalpurchasing supply chain in the United States.
BackgroundIn the US, GPOs have long helped hospitals (and other healthcareproviders including nursing homes, ambulatory care facilities, etc.)realize savings and create contracting efficiencies by aggregatingpurchasing volume and using that leverage to negotiate discountswith manufacturers, distributors and other vendors. The US GPOindustry is over 100 years old. The first GPO was created in 1910by the Hospital Bureau of New York and consisted mostly oflaundry and other shared services. The use of GPO contracts hasgrown and accounts for approximately 73% of non-labourpurchases a hospital makes1. A survey by Burns and Lee (2008)revealed that nearly 85% of US hospitals route 50% or more oftheir commodity-item spending, and 80% route 50% or more oftheir pharmaceutical spending through GPOs2.
The US has approximately 5000 hospitals. Most of theseinstitutions are not-for-profit. A smaller number of hospitals andhealth systems are investor-owned, while still fewer are publicfacilities run by either state or local government. The physiciansthat provide medical services are either employed by the hospital
CURTIS ROONEY
PRESIDENT OF THE HEALTH INDUSTRY GROUP PURCHASING
ASSOCIATION (HIGPA)
or have “privileges” to see patients in that facility. The number ofphysicians in “private practice” is expected to continue to declinewith declining reimbursement rates. US healthcare expenditurestotaled over US$2.3 trillion (approximately 17% of GDP) in 20073.Medicare and Medicaid spending was US$749.8B in Fiscal Year(FY) (October) 2009 compared to US$333.9 billion in federalhealthcare spending in FY 20024.
There are two basic types of healthcare GPOs5. The first iscomprised of an existing network of healthcare providers oftencalled an “Integrated Delivery/Health Network,” which centralizesits purchasing activities into one place. The other type of GPO,which is more prevalent, is the “voluntary GPO,” whose membersparticipate in the benefits of leverage contracting but often buy“off-contract” (i.e., negotiating with and buying directly frommanufacturers or distributors). Buying “off contract” is especiallycommon in connection with “physician preference items” such asimplantable medical devices and specialty pharmacy drugs6.
Voluntary GPOs do not guarantee specific purchase volumes toa manufacturer. The extent to which a given hospital buys “on-contract” (i.e., completes purchases under terms negotiated by itsGPO) is called “compliance” or “participation.” The compliance orparticipation level of a GPO’s members is an importantdeterminant of the GPO’s power in negotiating prices for itsprovider-members. The key reason hospitals join a GPO is that itwill incur a lower total purchasing cost. The voluntary GPO modelis so common that approximately 90 to 96% of all US hospitalsbelong to 1 or more GPOs in the US7. In fact, hospitals use anaverage of 1.6-2.6 GPOs per facility to achieve their purchasinggoals8.
GPOs do not purchase supplies, member hospitals do, underthe terms of GPO-negotiated contracts. To choose the mostappropriate products, GPOs create value analysis teams ofclinicians and experts from member institutions that evaluate,
24-26 Purchasing Organizations in US - rooney:29 31/3/11 18:34 Page 24
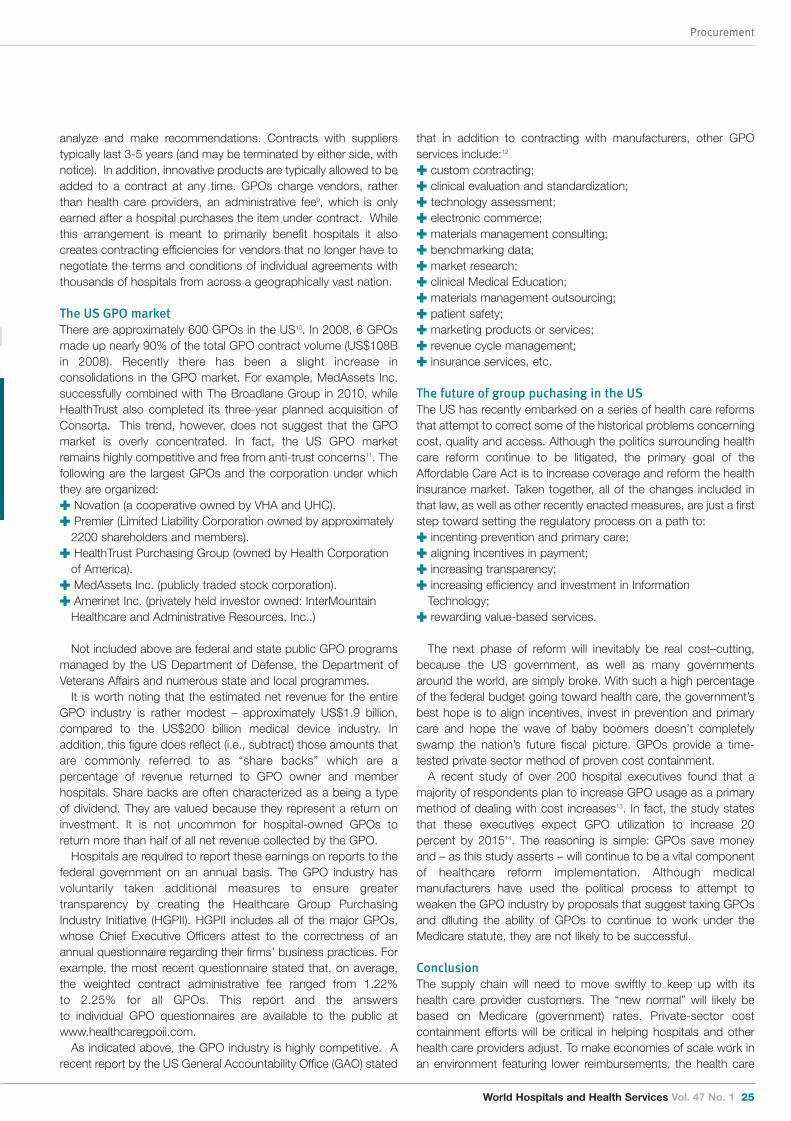
World Hospitals and Health Services Vol. 47 No. 1 25
Procurement
analyze and make recommendations. Contracts with supplierstypically last 3-5 years (and may be terminated by either side, withnotice). In addition, innovative products are typically allowed to beadded to a contract at any time. GPOs charge vendors, ratherthan health care providers, an administrative fee9, which is onlyearned after a hospital purchases the item under contract. Whilethis arrangement is meant to primarily benefit hospitals it alsocreates contracting efficiencies for vendors that no longer have tonegotiate the terms and conditions of individual agreements withthousands of hospitals from across a geographically vast nation.
The US GPO marketThere are approximately 600 GPOs in the US10. In 2008, 6 GPOsmade up nearly 90% of the total GPO contract volume (US$108Bin 2008). Recently there has been a slight increase inconsolidations in the GPO market. For example, MedAssets Inc.successfully combined with The Broadlane Group in 2010, whileHealthTrust also completed its three-year planned acquisition ofConsorta. This trend, however, does not suggest that the GPOmarket is overly concentrated. In fact, the US GPO marketremains highly competitive and free from anti-trust concerns11. Thefollowing are the largest GPOs and the corporation under whichthey are organized:� Novation (a cooperative owned by VHA and UHC). � Premier (Limited Liability Corporation owned by approximately
2200 shareholders and members).� HealthTrust Purchasing Group (owned by Health Corporation
of America). � MedAssets Inc. (publicly traded stock corporation).� Amerinet Inc. (privately held investor owned: InterMountain
Healthcare and Administrative Resources, Inc..)
Not included above are federal and state public GPO programsmanaged by the US Department of Defense, the Department ofVeterans Affairs and numerous state and local programmes.
It is worth noting that the estimated net revenue for the entireGPO industry is rather modest – approximately US$1.9 billion,compared to the US$200 billion medical device industry. Inaddition, this figure does reflect (i.e., subtract) those amounts thatare commonly referred to as “share backs” which are apercentage of revenue returned to GPO owner and memberhospitals. Share backs are often characterized as a being a typeof dividend. They are valued because they represent a return oninvestment. It is not uncommon for hospital-owned GPOs toreturn more than half of all net revenue collected by the GPO.
Hospitals are required to report these earnings on reports to thefederal government on an annual basis. The GPO industry hasvoluntarily taken additional measures to ensure greatertransparency by creating the Healthcare Group PurchasingIndustry Initiative (HGPII). HGPII includes all of the major GPOs,whose Chief Executive Officers attest to the correctness of anannual questionnaire regarding their firms’ business practices. Forexample, the most recent questionnaire stated that, on average,the weighted contract administrative fee ranged from 1.22% to 2.25% for all GPOs. This report and the answers to individual GPO questionnaires are available to the public atwww.healthcaregpoii.com.
As indicated above, the GPO industry is highly competitive. Arecent report by the US General Accountability Office (GAO) stated
that in addition to contracting with manufacturers, other GPOservices include:12
� custom contracting;� clinical evaluation and standardization;� technology assessment;� electronic commerce;� materials management consulting;� benchmarking data;� market research;� clinical Medical Education;� materials management outsourcing;� patient safety;� marketing products or services;� revenue cycle management;� insurance services, etc.
The future of group puchasing in the USThe US has recently embarked on a series of health care reformsthat attempt to correct some of the historical problems concerningcost, quality and access. Although the politics surrounding healthcare reform continue to be litigated, the primary goal of theAffordable Care Act is to increase coverage and reform the healthinsurance market. Taken together, all of the changes included inthat law, as well as other recently enacted measures, are just a firststep toward setting the regulatory process on a path to:� incenting prevention and primary care;� aligning incentives in payment;� increasing transparency;� increasing efficiency and investment in Information
Technology; � rewarding value-based services.
The next phase of reform will inevitably be real cost–cutting,because the US government, as well as many governmentsaround the world, are simply broke. With such a high percentageof the federal budget going toward health care, the government’sbest hope is to align incentives, invest in prevention and primarycare and hope the wave of baby boomers doesn’t completelyswamp the nation’s future fiscal picture. GPOs provide a time-tested private sector method of proven cost containment.
A recent study of over 200 hospital executives found that amajority of respondents plan to increase GPO usage as a primarymethod of dealing with cost increases13. In fact, the study statesthat these executives expect GPO utilization to increase 20percent by 201514. The reasoning is simple: GPOs save moneyand – as this study asserts – will continue to be a vital component of healthcare reform implementation. Although medicalmanufacturers have used the political process to attempt toweaken the GPO industry by proposals that suggest taxing GPOsand diluting the ability of GPOs to continue to work under theMedicare statute, they are not likely to be successful.
ConclusionThe supply chain will need to move swiftly to keep up with itshealth care provider customers. The “new normal” will likely bebased on Medicare (government) rates. Private-sector costcontainment efforts will be critical in helping hospitals and otherhealth care providers adjust. To make economies of scale work inan environment featuring lower reimbursements, the health care
24-26 Purchasing Organizations in US - rooney:29 31/3/11 18:35 Page 25

supply chain will include further consolidations at every level. Inaddition, vendors will need to rethink how their products fit into thenew processes being developed for disease management andcare coordination. GPOs will need to marry their data services toreal-time clinical and quality situations for their hospital customers.Wholesaler/distributors will need to harness their existing data tonew clinical requirements as well. Survivors of consolidation will bebigger, more efficient, leaner, meaner and data-driven. GPOs areexpected to continue to play a critical role in the business ofhospital purchasing. In fact, the US GPO model may be anexciting export that other countries may wish to examine in thefuture. �
Curtis Rooney is President of the Health Industry Group PurchasingAssociation (HIGPA), the leading organization that advocates onbehalf of healthcare group purchasing organizations (GPOs) inWashington, DC. He is responsible for the association’s strategicefforts to advance the healthcare GPO industry.
Prior to becoming President of HIGPA, Mr Rooney was theSenior Associate Director and Counsel, Federal Relations, for theAmerican Hospital Association (AHA) from 1999 to 2006. He wasresponsible for a number of issues including disasterpreparedness, Medicare payment issues, medical liability reform,mental health services, telemedicine and ERISA.
Mr Rooney was an attorney with the law firm of Arent Fox KintnerPlotkin & Kahn, practicing in the Health Law Group in Washington,DC. He has also been Washington Counsel to the AmericanMedical Association (AMA) in the Division of Legislative Counseland Counsel to the Association of Private Pension and WelfarePlans (APPWP) (now the American Benefits Council).
Mr Rooney has written and spoken extensively on politics,Medicare, telemedicine, ERISA and health care reform. He sits ona number of boards including the Healthcare Industry Supply ChainInstitute. He is Chairman of the Children of Kibera Foundationwhich creates educational opportunities for underprivilegedchildren in Nairobi’s (Kenya) largest slum. He received a Bachelorof Arts from The George Washington University and Juris Doctorfrom The Catholic University, JD. He is married and has twochildren.
Procurement
26 World Hospitals and Health Services Vol. 47 No. 1
References1. David E. Goldenberg, Ph.D. and Roland “Guy” King, F.S.A., M.A.A.A. “A 2008 Update of Cost
Savings and a Marketplace Analysis of the Health Care Group Purchasing Industry”, July2008 at p.2.
2. L.R. Burns and J.A. Lee. “Hospitals purchasing alliances: Utilization, Services andPerformance.” Health Care Management Review, July-September, 33: 203-215, 2008.
3. David E. Goldenberg, Ph.D. and Roland “Guy” King, F.S.A., M.A.A.A. “A 2008 Update of CostSavings and a Marketplace Analysis of the Health Care Group Purchasing Industry”, July2008 at p. 2.
4. Id.5. R.E. Bloch, S.P. Perlman, and J.S. Brown. “An Analysis of Group Purchasing Organizations’
Contracting Practices Under the Antitrust Laws: Myth and Reality.” White Paper. Mayer,Brown, Rowe & Maw, 2006.
6. Eugene Schneller, “The Value of Group Purchasing – 2009: Meeting the Need for StrategicSourcing.” Health Sector Advances Inc., April 2009 at 8.
7. See Burns and Lee at p.204.8. See Burns and Lee at p.204.9. The “Medicare and Medicaid Patient Protection Act of 1987” created GPO “Safe
Harbor”which requires: 10. The GPO must have a written agreement with each hospital or healthcare provider, that
provides for either of the following agreements: (a) The vendor from which the hospital or healthcare provider will purchase goods orservices will pay a fee to the GPO of 3% or less of the purchase price of the goods orservices provided by that vendor, and (b) In the event the fee paid to the GPO is not fixed at 3% or less of the purchase price ofthe goods or services, the agreement specifies the exact percentage or amount of the fee. 2) The GPO must disclose in writing to the hospital or healthcare provider at least annually,the amount received from each vendor with respect to purchases made by or on behalf ofthe hospital or healthcare provider. See, 42 U.S.C. § 1320a-7b(b)(3)(C)(i); 42 C.F.R. §1001.952(j) (2009).
11. Report to the Ranking Member, Committee on Finance, U.S. Senate, United StatesGovernment Accountability Office. “GROUP PURCHASING ORGANIZATIONS: Services Providedto Customers and Initiatives Regarding Their Business Practices (GAO-10-738)” at p.4,September 2010.
12. William Kolasky, “Group Purchasing Organization (GPO): Contracting Practices and AntitrustLaw.” White Paper, Wilmer Cutler Pickering Hale and Dorr LLP, November 2009.
13. See GAO-10-738 at p.9.14. Stuart Jackson and Bob Lavoie. “Healthcare Reform Shifts Hospital Priorities, Creates New
Opportunities for MedTech Companies”, L.E.K. Consulting, Volume XIII, Issue 4, February,2011.
15. Id at p. 4.
24-26 Purchasing Organizations in US - rooney:29 31/3/11 18:35 Page 26

World Hospitals and Health Services Vol. 47 No. 1 27
Procurement sepcial feature
Pooling procurement in the Belgianhospital sector
ABSTRACT: The Belgian hospital sector is following the example of a number of other European countries and for more than ten years now, has been striving to pool its medical supplies and equipment purchases in a bid to reduce costs.
The various experiments of which we are aware come under both opportunist purchases and initiatives which aredesigned to encourage local-regional contracts. These attempts have now all come to nothing or are struggling in theabsence of a structured and professional approach.
In 2005, the Saint Luc University Clinic in Brussels decided to set up a high-performance purchasing department, the aim being to centre its initiatives around TCO or Total Cost of Ownership.
Following an analysis of the various experiments into pooling procurement in hospitals in Europe, the Saint Luc UniversityClinic decided on a central procurement agency model, in accordance with new legislation on public procurement.
This article seeks to highlight the prerequisites which are vital for a procurement pooling initiative, withoutunderestimating the risks and limitations of implementing such a change in procurement practices.
The Mercure central procurement agency is now the largest interhospital purchasing structure in Belgium.
The Belgian hospital sector is following the example of a numberof other European countries and for more than ten years now,has been striving to pool its medical supplies and equipment
purchases in a bid to reduce costs.The various experiments of which we are aware come under
both opportunist purchases and initiatives which are designed toencourage local-regional contracts. These attempts have now allcome to nothing or are struggling in the absence of a structuredand professional approach.
In 2005, the Saint Luc University Clinic in Brussels decided to setup a high-performance purchasing department, the aim being tocentre its initiatives around TCO or Total Cost of Ownership.
This purchasing department implements and manages a cross-functional process which uses the estimate of a functionalrequirement as its basis for coordinating the various activitiesinvolved in acquiring goods or securing outside services. It sets outto provide a high-performance service in terms of quality andreliability that best meets the specific aspects of the definedrequirement, at the best cost of ownership and within thescheduled time frame.
Consequently, it is interdependent of all the other departments inthe healthcare centre, tasked with implementing a clearly definedpurchasing process that involves consolidating demand,broadening the range of potential suppliers, overseeing andcoordinating the negotiation process and tracking and complyingwith agreements.
The Belgian hospital sector is following the example of a numberof other European countries and for more than ten years now, hasbeen striving to pool its medical supplies and equipment purchases
GUY HEBERT
HEAD OF PURCHASESAND LOGISTICS – SAINT LUC UNIVERSITY CLINIC,
BRUSSELS, CHAIRMAN OF THE MERCURY CENTRAL PROCUREMENT AGENCY
in a bid to reduce costs.The various experiments of which we are aware come under
both opportunist purchases and initiatives which are designed toencourage local-regional contracts. These attempts have now allcome to nothing or are struggling in the absence of a structuredand professional approach.
In 2005, the Saint Luc University Clinic in Brussels decided to setup a high-performance purchasing department, the aim being tocentre its initiatives around TCO or Total Cost of Ownership.
This purchasing department implements and manages a cross-functional process which uses the estimate of a functionalrequirement as its basis for coordinating the various activitiesinvolved in acquiring goods or securing outside services. It sets outto provide a high-performance service in terms of quality andreliability that best meets the specific aspects of the definedrequirement, at the best cost of ownership and within thescheduled time frame.
Consequently, it is interdependent of all the other departments inthe healthcare centre, tasked with implementing a clearly definedpurchasing process that involves consolidating demand,broadening the range of potential suppliers, overseeing andcoordinating the negotiation process and tracking and complyingwith agreements.
This matrix approach proved decisive in all decision-makingprocesses, mainly in restructuring the team of purchasers and inestablishing new relations between internal clients and purchasers.
After a year of restructuring, the situation looked very promising.The cost of operating supplies, for example, fell by more than 10%,while the cost of medical equipment fell by more than 20%.
27-30 Belgian hospital sector - herbert NEW:29 31/3/11 18:33 Page 27
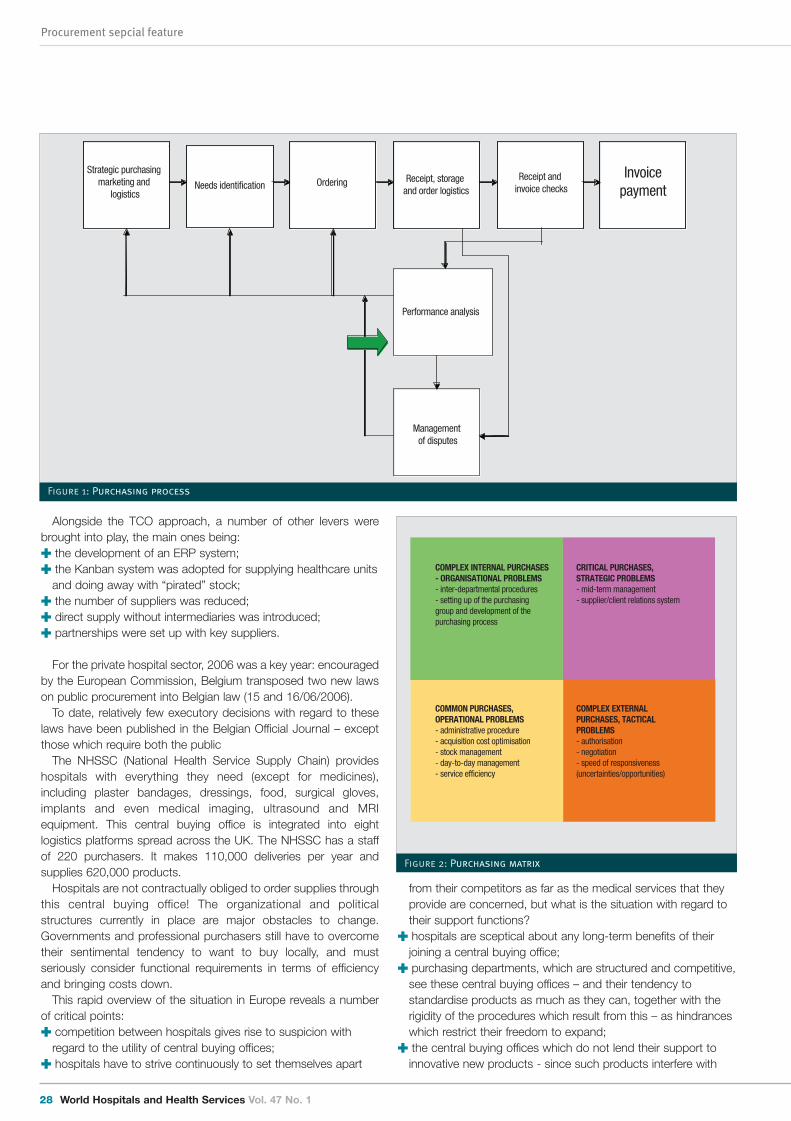
Procurement sepcial feature
28 World Hospitals and Health Services Vol. 47 No. 1
Alongside the TCO approach, a number of other levers werebrought into play, the main ones being:� the development of an ERP system;� the Kanban system was adopted for supplying healthcare units
and doing away with “pirated” stock;� the number of suppliers was reduced;� direct supply without intermediaries was introduced;� partnerships were set up with key suppliers.
For the private hospital sector, 2006 was a key year: encouragedby the European Commission, Belgium transposed two new lawson public procurement into Belgian law (15 and 16/06/2006).
To date, relatively few executory decisions with regard to theselaws have been published in the Belgian Official Journal – exceptthose which require both the public
The NHSSC (National Health Service Supply Chain) provideshospitals with everything they need (except for medicines),including plaster bandages, dressings, food, surgical gloves,implants and even medical imaging, ultrasound and MRIequipment. This central buying office is integrated into eightlogistics platforms spread across the UK. The NHSSC has a staffof 220 purchasers. It makes 110,000 deliveries per year andsupplies 620,000 products.
Hospitals are not contractually obliged to order supplies throughthis central buying office! The organizational and politicalstructures currently in place are major obstacles to change.Governments and professional purchasers still have to overcometheir sentimental tendency to want to buy locally, and mustseriously consider functional requirements in terms of efficiencyand bringing costs down.
This rapid overview of the situation in Europe reveals a numberof critical points:� competition between hospitals gives rise to suspicion with
regard to the utility of central buying offices;� hospitals have to strive continuously to set themselves apart
from their competitors as far as the medical services that theyprovide are concerned, but what is the situation with regard totheir support functions?
� hospitals are sceptical about any long-term benefits of theirjoining a central buying office;
� purchasing departments, which are structured and competitive,see these central buying offices – and their tendency tostandardise products as much as they can, together with therigidity of the procedures which result from this – as hindranceswhich restrict their freedom to expand;
� the central buying offices which do not lend their support toinnovative new products - since such products interfere with
Management of disputes
Strategic purchasing marketing and
logisticsNeeds identification Ordering Receipt, storage
and order logisticsReceipt and
invoice checks
Invoicepayment
Performance analysis
Figure 1: Purchasing process
COMPLEX INTERNAL PURCHASES - ORGANISATIONAL PROBLEMS- inter-departmental procedures- setting up of the purchasing group and development of the purchasing process
COMMON PURCHASES, OPERATIONAL PROBLEMS- administrative procedure- acquisition cost optimisation- stock management- day-to-day management- service efficiency
CRITICAL PURCHASES, STRATEGIC PROBLEMS- mid-term management- supplier/client relations system
COMPLEX EXTERNAL PURCHASES, TACTICAL PROBLEMS- authorisation- negotiation- speed of responsiveness (uncertainties/opportunities)
Figure 2: Purchasing matrix
27-30 Belgian hospital sector - herbert NEW:29 31/3/11 18:33 Page 28
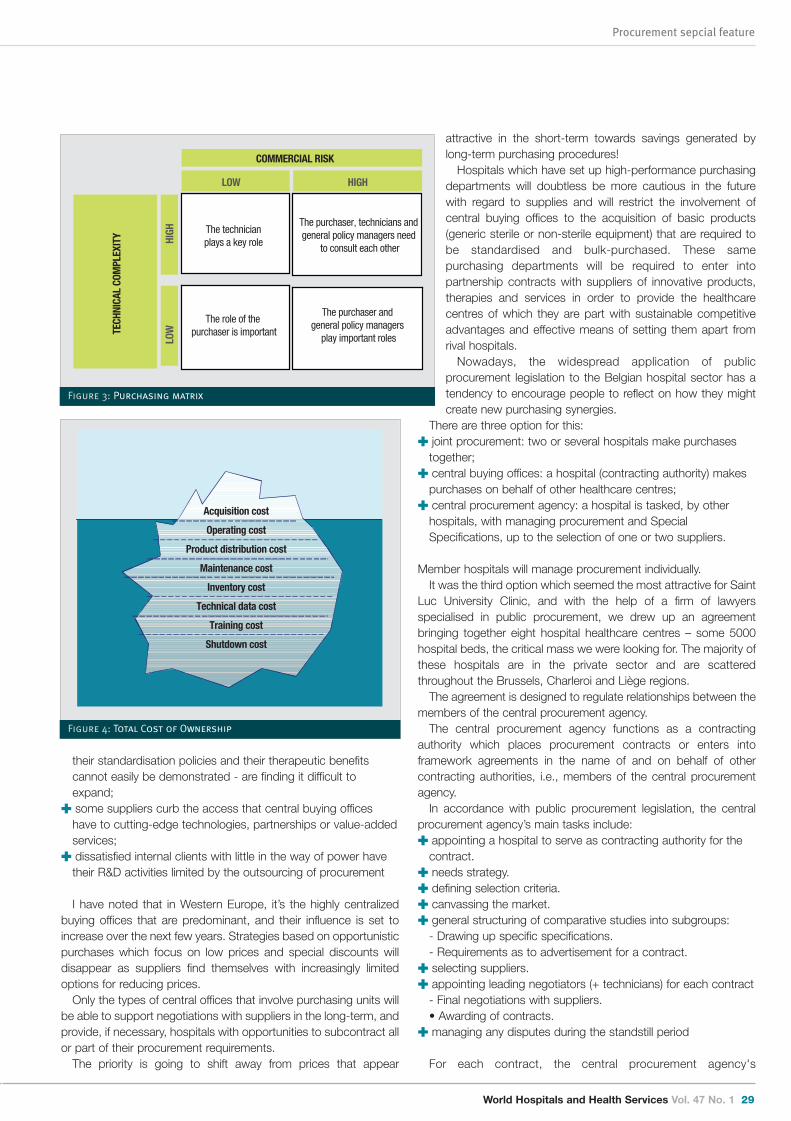
World Hospitals and Health Services Vol. 47 No. 1 29
Procurement sepcial feature
attractive in the short-term towards savings generated bylong-term purchasing procedures!
Hospitals which have set up high-performance purchasingdepartments will doubtless be more cautious in the futurewith regard to supplies and will restrict the involvement ofcentral buying offices to the acquisition of basic products(generic sterile or non-sterile equipment) that are required tobe standardised and bulk-purchased. These samepurchasing departments will be required to enter intopartnership contracts with suppliers of innovative products,therapies and services in order to provide the healthcarecentres of which they are part with sustainable competitiveadvantages and effective means of setting them apart fromrival hospitals.
Nowadays, the widespread application of publicprocurement legislation to the Belgian hospital sector has atendency to encourage people to reflect on how they mightcreate new purchasing synergies.
There are three option for this:� joint procurement: two or several hospitals make purchases
together;� central buying offices: a hospital (contracting authority) makes
purchases on behalf of other healthcare centres;� central procurement agency: a hospital is tasked, by other
hospitals, with managing procurement and SpecialSpecifications, up to the selection of one or two suppliers.
Member hospitals will manage procurement individually.It was the third option which seemed the most attractive for Saint
Luc University Clinic, and with the help of a firm of lawyersspecialised in public procurement, we drew up an agreementbringing together eight hospital healthcare centres – some 5000hospital beds, the critical mass we were looking for. The majority ofthese hospitals are in the private sector and are scatteredthroughout the Brussels, Charleroi and Liège regions.
The agreement is designed to regulate relationships between themembers of the central procurement agency.
The central procurement agency functions as a contractingauthority which places procurement contracts or enters intoframework agreements in the name of and on behalf of othercontracting authorities, i.e., members of the central procurementagency.
In accordance with public procurement legislation, the centralprocurement agency’s main tasks include:� appointing a hospital to serve as contracting authority for the
contract. � needs strategy.� defining selection criteria.� canvassing the market.� general structuring of comparative studies into subgroups:
- Drawing up specific specifications.- Requirements as to advertisement for a contract.
� selecting suppliers.� appointing leading negotiators (+ technicians) for each contract
- Final negotiations with suppliers.• Awarding of contracts.
� managing any disputes during the standstill period
For each contract, the central procurement agency's
their standardisation policies and their therapeutic benefitscannot easily be demonstrated - are finding it difficult toexpand;
� some suppliers curb the access that central buying officeshave to cutting-edge technologies, partnerships or value-addedservices;
� dissatisfied internal clients with little in the way of power havetheir R&D activities limited by the outsourcing of procurement
I have noted that in Western Europe, it’s the highly centralizedbuying offices that are predominant, and their influence is set toincrease over the next few years. Strategies based on opportunisticpurchases which focus on low prices and special discounts willdisappear as suppliers find themselves with increasingly limitedoptions for reducing prices.
Only the types of central offices that involve purchasing units willbe able to support negotiations with suppliers in the long-term, andprovide, if necessary, hospitals with opportunities to subcontract allor part of their procurement requirements.
The priority is going to shift away from prices that appear
The purchaser, technicians and general policy managers need
to consult each other
COMMERCIAL RISK
TECH
NICA
L CO
MPL
EXIT
Y
LOW HIGHLO
W
H
IGH The technician
plays a key role
The role of the purchaser is important
The purchaser and general policy managers
play important roles
Figure 3: Purchasing matrix
Acquisition cost
Operating cost
Product distribution cost
Maintenance cost
Inventory cost
Technical data cost
Training cost
Shutdown cost
Figure 4: Total Cost of Ownership
27-30 Belgian hospital sector - herbert NEW:29 31/3/11 18:33 Page 29
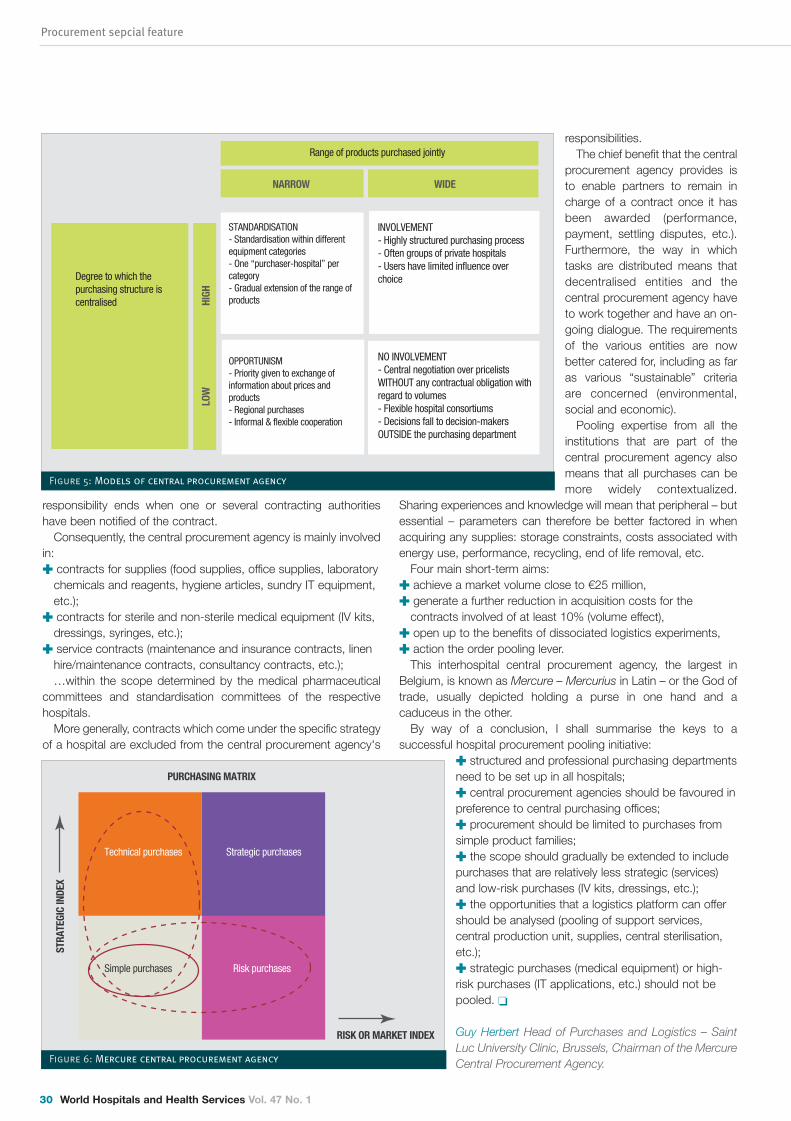
Procurement sepcial feature
30 World Hospitals and Health Services Vol. 47 No. 1
responsibility ends when one or several contracting authoritieshave been notified of the contract.
Consequently, the central procurement agency is mainly involvedin:� contracts for supplies (food supplies, office supplies, laboratory
chemicals and reagents, hygiene articles, sundry IT equipment,etc.);
� contracts for sterile and non-sterile medical equipment (IV kits,dressings, syringes, etc.);
� service contracts (maintenance and insurance contracts, linenhire/maintenance contracts, consultancy contracts, etc.); …within the scope determined by the medical pharmaceutical
committees and standardisation committees of the respectivehospitals.
More generally, contracts which come under the specific strategyof a hospital are excluded from the central procurement agency's
responsibilities.The chief benefit that the central
procurement agency provides isto enable partners to remain incharge of a contract once it hasbeen awarded (performance,payment, settling disputes, etc.).Furthermore, the way in whichtasks are distributed means thatdecentralised entities and thecentral procurement agency haveto work together and have an on-going dialogue. The requirementsof the various entities are nowbetter catered for, including as faras various “sustainable” criteriaare concerned (environmental,social and economic).
Pooling expertise from all theinstitutions that are part of thecentral procurement agency alsomeans that all purchases can bemore widely contextualized.
Sharing experiences and knowledge will mean that peripheral – butessential – parameters can therefore be better factored in whenacquiring any supplies: storage constraints, costs associated withenergy use, performance, recycling, end of life removal, etc.
Four main short-term aims:� achieve a market volume close to €25 million,� generate a further reduction in acquisition costs for the
contracts involved of at least 10% (volume effect),� open up to the benefits of dissociated logistics experiments,� action the order pooling lever.
This interhospital central procurement agency, the largest inBelgium, is known as Mercure – Mercurius in Latin – or the God oftrade, usually depicted holding a purse in one hand and acaduceus in the other.
By way of a conclusion, I shall summarise the keys to asuccessful hospital procurement pooling initiative:
� structured and professional purchasing departmentsneed to be set up in all hospitals;� central procurement agencies should be favoured inpreference to central purchasing offices;� procurement should be limited to purchases fromsimple product families;� the scope should gradually be extended to includepurchases that are relatively less strategic (services)and low-risk purchases (IV kits, dressings, etc.);� the opportunities that a logistics platform can offershould be analysed (pooling of support services,central production unit, supplies, central sterilisation,etc.);� strategic purchases (medical equipment) or high-risk purchases (IT applications, etc.) should not bepooled. �
Guy Herbert Head of Purchases and Logistics – SaintLuc University Clinic, Brussels, Chairman of the MercureCentral Procurement Agency.
NARROW WIDE
Range of products purchased jointly
Degree to which the purchasing structure is centralised
LOW
HIG
H
STANDARDISATION- Standardisation within different equipment categories- One “purchaser-hospital” per category- Gradual extension of the range of products
OPPORTUNISM- Priority given to exchange of information about prices and products- Regional purchases- Informal & flexible cooperation
INVOLVEMENT- Highly structured purchasing process- Often groups of private hospitals- Users have limited influence over choice
NO INVOLVEMENT- Central negotiation over pricelists WITHOUT any contractual obligation with regard to volumes- Flexible hospital consortiums- Decisions fall to decision-makers OUTSIDE the purchasing department
Figure 5: Models of central procurement agency
Technical purchases Strategic purchases
Simple purchases Risk purchases
STRA
TEGI
C IN
DEX
PURCHASING MATRIX
RISK OR MARKET INDEX
Figure 6: Mercure central procurement agency
27-30 Belgian hospital sector - herbert NEW:29 31/3/11 18:33 Page 30
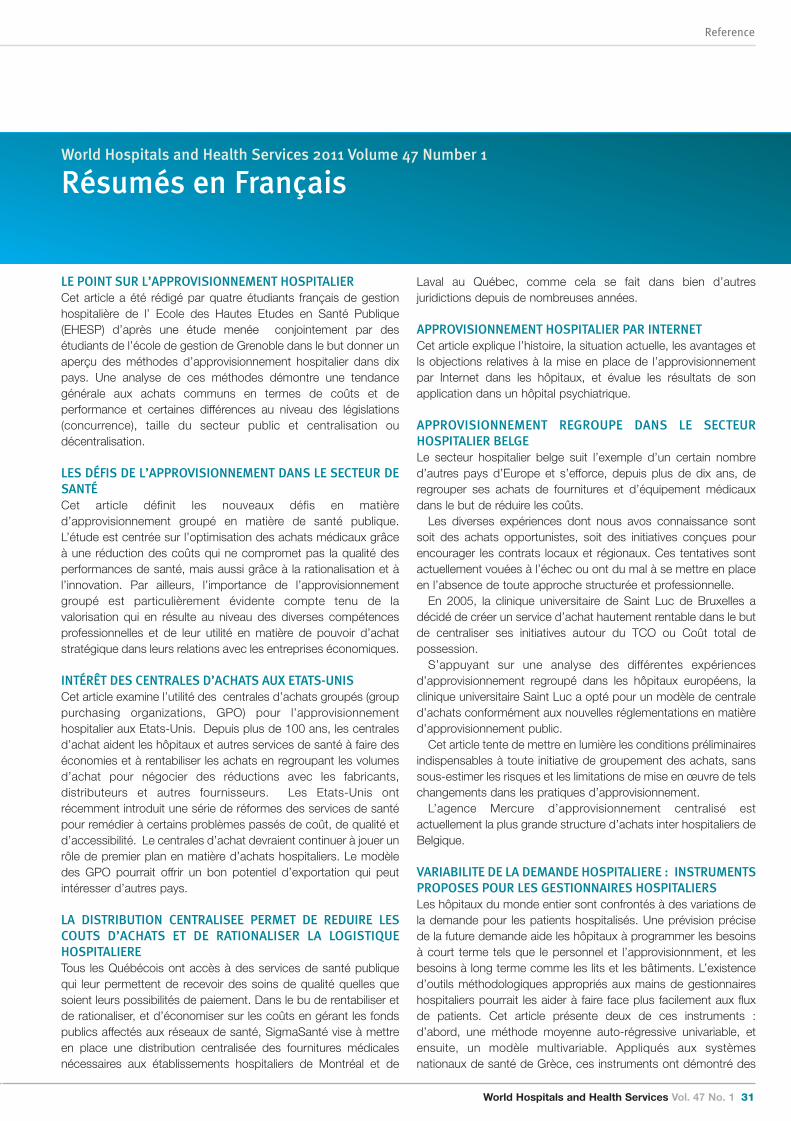
World Hospitals and Health Services Vol. 47 No. 1 31
Reference
World Hospitals and Health Services 2011 Volume 47 Number 1
Résumés en Français
LE POINT SUR L’APPROVISIONNEMENT HOSPITALIERCet article a été rédigé par quatre étudiants français de gestionhospitalière de l’ Ecole des Hautes Etudes en Santé Publique(EHESP) d’après une étude menée conjointement par desétudiants de l’école de gestion de Grenoble dans le but donner unaperçu des méthodes d’approvisionnement hospitalier dans dixpays. Une analyse de ces méthodes démontre une tendancegénérale aux achats communs en termes de coûts et deperformance et certaines différences au niveau des législations(concurrence), taille du secteur public et centralisation oudécentralisation.
LES DÉFIS DE L’APPROVISIONNEMENT DANS LE SECTEUR DESANTÉCet article définit les nouveaux défis en matièred’approvisionnement groupé en matière de santé publique.L’étude est centrée sur l’optimisation des achats médicaux grâceà une réduction des coûts qui ne compromet pas la qualité desperformances de santé, mais aussi grâce à la rationalisation et àl’innovation. Par ailleurs, l’importance de l’approvisionnementgroupé est particulièrement évidente compte tenu de lavalorisation qui en résulte au niveau des diverses compétencesprofessionnelles et de leur utilité en matière de pouvoir d’achatstratégique dans leurs relations avec les entreprises économiques.
INTÉRÊT DES CENTRALES D’ACHATS AUX ETATS-UNISCet article examine l’utilité des centrales d’achats groupés (grouppurchasing organizations, GPO) pour l’approvisionnementhospitalier aux Etats-Unis. Depuis plus de 100 ans, les centralesd’achat aident les hôpitaux et autres services de santé à faire deséconomies et à rentabiliser les achats en regroupant les volumesd’achat pour négocier des réductions avec les fabricants,distributeurs et autres fournisseurs. Les Etats-Unis ontrécemment introduit une série de réformes des services de santépour remédier à certains problèmes passés de coût, de qualité etd’accessibilité. Le centrales d’achat devraient continuer à jouer unrôle de premier plan en matière d’achats hospitaliers. Le modèledes GPO pourrait offrir un bon potentiel d’exportation qui peutintéresser d’autres pays.
LA DISTRIBUTION CENTRALISEE PERMET DE REDUIRE LESCOUTS D’ACHATS ET DE RATIONALISER LA LOGISTIQUEHOSPITALIERE Tous les Québécois ont accès à des services de santé publiquequi leur permettent de recevoir des soins de qualité quelles quesoient leurs possibilités de paiement. Dans le bu de rentabiliser etde rationaliser, et d’économiser sur les coûts en gérant les fondspublics affectés aux réseaux de santé, SigmaSanté vise à mettreen place une distribution centralisée des fournitures médicalesnécessaires aux établissements hospitaliers de Montréal et de
Laval au Québec, comme cela se fait dans bien d’autresjuridictions depuis de nombreuses années.
APPROVISIONNEMENT HOSPITALIER PAR INTERNET Cet article explique l’histoire, la situation actuelle, les avantages etls objections relatives à la mise en place de l’approvisionnementpar Internet dans les hôpitaux, et évalue les résultats de sonapplication dans un hôpital psychiatrique.
APPROVISIONNEMENT REGROUPE DANS LE SECTEURHOSPITALIER BELGELe secteur hospitalier belge suit l’exemple d’un certain nombred’autres pays d’Europe et s’efforce, depuis plus de dix ans, deregrouper ses achats de fournitures et d’équipement médicauxdans le but de réduire les coûts.
Les diverses expériences dont nous avos connaissance sontsoit des achats opportunistes, soit des initiatives conçues pourencourager les contrats locaux et régionaux. Ces tentatives sontactuellement vouées à l’échec ou ont du mal à se mettre en placeen l’absence de toute approche structurée et professionnelle.
En 2005, la clinique universitaire de Saint Luc de Bruxelles adécidé de créer un service d’achat hautement rentable dans le butde centraliser ses initiatives autour du TCO ou Coût total depossession.
S’appuyant sur une analyse des différentes expériencesd’approvisionnement regroupé dans les hôpitaux européens, laclinique universitaire Saint Luc a opté pour un modèle de centraled’achats conformément aux nouvelles réglementations en matièred’approvisionnement public.
Cet article tente de mettre en lumière les conditions préliminairesindispensables à toute initiative de groupement des achats, sanssous-estimer les risques et les limitations de mise en œuvre de telschangements dans les pratiques d’approvisionnement.
L’agence Mercure d’approvisionnement centralisé estactuellement la plus grande structure d’achats inter hospitaliers deBelgique.
VARIABILITE DE LA DEMANDE HOSPITALIERE : INSTRUMENTSPROPOSES POUR LES GESTIONNAIRES HOSPITALIERSLes hôpitaux du monde entier sont confrontés à des variations dela demande pour les patients hospitalisés. Une prévision précisede la future demande aide les hôpitaux à programmer les besoinsà court terme tels que le personnel et l’approvisionnment, et lesbesoins à long terme comme les lits et les bâtiments. L’existenced’outils méthodologiques appropriés aux mains de gestionnaireshospitaliers pourrait les aider à faire face plus facilement aux fluxde patients. Cet article présente deux de ces instruments :d’abord, une méthode moyenne auto-régressive univariable, etensuite, un modèle multivariable. Appliqués aux systèmesnationaux de santé de Grèce, ces instruments ont démontré des
31-33 Translations 29:38 31/3/11 19:20 Page 31
Reference
32 World Hospitals and Health Services Vol. 47 No. 1
VISTA GENERAL DEL PROCEDIMIENTO DE COMPRAS DE LOSHOSPITALES A NIVEL INTERNACIONALEste artículo lo han redactado cuatro estudiantes de direcciónhospitalaria de Francia de la Escuela de Salud Pública (EHESP)como resultado de un estudio realizado conjuntamente conestudiantes de la Escuela de Dirección de Grenoble, con el fin deofrecer una vista general de los métodos de compras de loshospitales en diez países distintos. En un análisis de estosmétodos se demostró que hay una tendencia general hacia lascompras en grupo, con algunos objetivos comunes, como porejemplo los costes y el funcionamiento y algunas diferencias encuanto a la legislación (competencia), la magnitud del sectorpúblico y la centralización o descentralización.
LAS DIFICULTADES DEL MÉTODO DE COMPRAS COLECTIVASDEL SECTOR SANITARIOEste artículo explica las dificultades recientes del método decompras colectivas en el sector sanitario. La investigación secentra en la optimización de las compras del sector sanitariomediante la reducción de costos sin que perjudique para nada lacalidad del rendimiento de los cuidados de salud, a la vez quegarantice la racionalización y la innovación. Lo que es más, laimportancia de las compras en grupo se pone especialmente enevidencia si tenemos en cuenta la consiguiente valorización de losdistintos conocimientos prácticos profesionales y su utilización delpoder adquisitivo estratégico en sus relaciones con los agenteseconómicos.
LA IMPORTANCIA DE LAS ORGANIZACIONES DE COMPRASCOLECTIVAS EN LOS ESTADOS UNIDOSEste artículo examina el papel tan valioso que desempeñan lasorganizaciones de compras colectivas (en inglés GPOS) en los
Estados Unidos. Durante más de cien años estas organizacioneshan ayudado a los hospitales y a otros proveedores de losservicios sanitarios a economizar y firmar contratos favorablesgracias a un incremento en el volumen de compras con el fin denegociar un descuento con los fabricantes, los distribuidores ydemás vendedores. Los Estados Unidos han promulgadorecientemente una serie de reformas sanitarias destinadas acorregir algunas de las preocupaciones iniciales en lo que respectaal coste, la calidad y el acceso. Se espera que las organizacionesde compras colectivas continúen desempeñando un papel crucialen el sector de las compras hospitalarias y quizás un interesantecomercio de exportaciones que otros países podrían estardispuestos a llevar a cabo en el futuro.
APROVISIONAMIENTO ELECTRÓNICO EN LOS HOSPITALESEste articulo describe los antecedentes, la situación actual, lasventajas y la resistencia a la puesta en práctica delaprovisionamiento electrónico en los hospitales y estudia losresultados de su adopción en un hospital psiquiátrico.
DISTRIBUCIÓN CENTRALIZADA. REDUCCIÓN DE LOS GASTOSDEL CAPITAL SOCIAL MEDIANTE LA RACIONALIZACIÓN DELOGÍSTICA DE LOS HOSPITALESTodos los ciudadanos de Quebec tienen acceso a un sistema desalud pública que les permite recibir unos cuidados de salud dealta calidad, independientemente de su capacidad de pagopersonal. Con el fin de mejorar la eficiencia y eficacia y conseguiruna reducción de los costos en la administración de los fondospúblicos asignados al sistema de prestación de servicios de salud,SigmaSanté tiene el proyecto de poner en práctica la distribucióncentral de los suministros médicos que necesiten losestablecimientos sanitarios de Montreal y Laval, Quebec, como se
World Hospitals and Health Services 2011 Volume 47 Number 1
Resumen en Espanol
variations significatives de la demande. La méthode univariablefournit les prévisions les plus précises de future demandeinattendue.
COMMENT MESURER LA DISPONIBILITE, LES PRIX ET LAGESTION DES MEDICAMENTS ESSENTIELS DANS LESHOPITAUX PUBLICS DU BURKINA FASO
Au Burkina Faso, améliorer les services de santé et l’accessibilitédes produits pharmaceutiques est une préoccupation majeurepour la population. L’objectif de cette étude était d’évaluer lesdisponibilités, les prix et les revenus de vente d’un groupement de50 médicamentsessentiels dans des hôpitaux publics du 29septembre au 29 décembre 2009. Une méthode appliquée pour étudier les prix, la disponibilité,
l’abordabilité et les composantes de prix de Health ActionInternational (HAI) de l’Organisation mondiale de la santé (OMS) aété utilisée pour réunir et analyser les données.Les résultats montrent que le taux moyen entre le budgetpharmaceutique et celui du centre médical est de 16.18. Le tauxmoyen de disponibilité était de 77.69%. Le prix d’achat auprès des fournisseurs de l’hôpital était à peuprès le même que les prix de référence internationaux (1.12). Lesprix de vente de l’hôpital public au public étaient le double du prixd’achat à leur fournisseur (2.20). Les revenus totaux de vente pour les trois premiers trimestres de2009 étaient de 708, 740, 495 FCFA (1.080,397 Euros). Ce revenureprésente environ 23,02% des coûts totaux de produitspharmaceutiques disponibles durant cette période (3,078,938,053FCFA/ 4,693,503 Euros).
31-33 Translations 29:38 31/3/11 19:20 Page 32
World Hospitals and Health Services Vol. 47 No. 1 33
Reference
de camas e instalaciones. La existencia de instrumentosmetodológicos adecuados y su aplicación por parte de ladirección hospitalaria, podría ayudar a ésta a allanar dificultadespor el flujo de pacientes en el futuro. Este artículo presenta dosinstrumentos diferentes: en primer lugar, un método auto-regresivo a una variable del promedio móvil y en segundo lugar, unmodelo con múltiples variables. Al aplicar estos métodos alSistema Nacional de Salud de Grecia se han encontrado unasvariaciones muy considerables en la demanda. El método a unavariable ofrece una previsión más correcta de la demandaimprevista en el futuro.
EVALUACION DE LA DISPONIBILIDAD, CAPACIDAD DE PAGO YADMINISTRACION DE FÁRMACOS ESENCIALES EN LOSHOSPITALES PUBLICOS DE BURKINA FASOPara la población de Burkina Faso la mejora de los servicios desalud y la disponibilidad de los productos farmacéuticosconstituyen una preocupación cada vez mayor. El objetivo de esteestudio consistió en evaluar la disponibilidad, los precios y losingresos de ventas de un grupo de 50 fármacos esenciales en loshospitales públicos desde el 29 de septiembre hasta el 29 dediciembre de 2009. El método empleado para estudiar losprecios, la disponibilidad, la capacidad de pago y el componentede precios de Health Action International (HAI) y la OrganizaciónMundial de la Salud (OMS) se ha utilizado para recopilar y analizarlos datos.
Los resultados muestran que la relación media entre elpresupuesto farmacéutico y el centro de salud es 16.18. El índicemedio de disponibilidad es del 77.69%. El precio de compra delos proveedores hospitalarios es aproximadamente el mismo queel precio internacional de referencia (1.12). El precio de venta delhospital público al paciente es el doble del precio de compra delproveedor (2.20).
El total de ingresos de las ventas para los tres primerostrimestres de 2009 es 708,740, 495 FCFA (1.080.397 Euros).Estos ingresos representan aproximadamente el 23.02% delcoste total de los productos farmacéuticos disponibles durante elperiodo (3.078.938.053 Francos CFA/4.693.503 Euros).
viene haciendo en numerosas otras jurisdicciones hace años.
ASOCIACION DE COMPRAS EN EL SECTOR HOSPITALARIOBELGAEl sector hospitalario belga está siguiendo el ejemplo denumerosos países europeos y lleva más de diez añosesforzándose por constituir un fondo para la adquisición deequipamiento y suministros médicos con el fin de reducir costos.Los diversos experimentos que conocemos van desde lascompras oportunistas hasta las iniciativas encaminadas afomentar los contratos locales y regionales. Estos intentos hanfracasado o bien avanzan con dificultad por falta de un modo deenfocarlos de una manera estructurada y profesional.
En 2005, la Clínica Universitaria Saint Luc de Bruselas decidióinstaurar un departamento de alto rendimiento, con el objetivo decentrar sus iniciativas en el TCO, es decir el Total Cost ofOwnership, o Coste Total de la Propiedad.
Tras un análisis de los distintos experimentos sobre laasociación de compras hospitalarias en Europa, la ClínicaHospitalaria Saint Luc decidió adoptar el ejemplo de losorganismos centrales de compras, conforme a la nuevalegislación de las adquisiciones públicas.
Este artículo tiene por objetivo poner de relieve los requisitosprevios de importancia primordial para poner en marcha unaasociación de compras sin menospreciar los riesgos yrestricciones de instaurar esta reforma en las prácticas delaprovisionamiento.
Hoy en día, la empresa central de compras Mercure es el mayororganismo de compras entre hospitales de Bélgica.
VARIACIONES EN LA DEMANDA HOSPITALARIA: POSIBLESINSTRUMENTOS A DISPOSICION DE LA DIRECCIONHOSPITALARIAHay una diferencia enorme en la demanda de los servicios dehospitalización entre los hospitales del mundo. Una previsióncorrecta de la demana futura ayuda a los hospitales a programarsus necesidades a corto plazo en términos de personal ysuministros médicos y a largo plazo en lo que respecta al número
31-33 Translations 29:38 31/3/11 19:20 Page 33

IHF corporate partners
34 World Hospitals and Health Services Vol. 47 No. 1
Company profiles
is a global leader in professional services, providing award-winning food services, management of facilities, assets, and clinicaltechnology, and uniform/career apparel to health care institutions and other businesses. In FORTUNE magazine's 2010 list of "World'sMost Admired Companies," ARAMARK ranks number one in its industry, consistently ranking since 1998 as one of the top three mostadmired companies in its industry. ARAMARK seeks to responsibly address key issues by focusing on employee advocacy,environmental stewardship, health and wellness, and community involvement. Headquartered in Philadelphia, Pennsylvania (USA),ARAMARK’s 255,000 employees serve clients in 22 countries.Visit www.aramark.com
is the centre of a community comprised of over 15,000 players of the hospital business. Through our web platform, we integratehospitals throughout the supply chain sector, focusing on business development and relationships. Established in 2000, in just 10years, Bionexo was structured in Brazil, becoming the largest marketplace reference to the hospital industry and contributingsignificantly to the professionalization of the purchasing sector and growth of the healthcare market.The success of this innovative business model has led to Bionexo for Latin America and Europe, where also attained leadership inaddition to export technology and implement a new concept in commercial transactions of organizations. Everything happened in ashort time, just like businesses are made between the companies that integrate our platforms. This makes Bionexo the largest core ofthe hospital sector in Brazil. Pioneering and innovation, helping thousands of companies and hospitals.www.bionexo.com.br
is the world leader in GIS technology. On any given day, more than one million people around the world use ESRI geographicinformation system (GIS) software to improve the way their organizations conduct business. ESRI GIS solutions are becoming anintegral component of health organizations in addition to nearly every other type of business and government service.By adding a geographic component to data and analysis, ESRI software promotes exploring, analyzing and visualizing massive amountsof information according to spatial relationships. Since most health and human service problems facing the world today exist in alocation-based context, geography can play a major role in helping health professionals understand health dynamics and the spread ofdisease. Health surveillance systems are used to gather, integrate and analyze health data; interpret disease transmission and spread;and monitor the capabilities of health systems. GIS is the enabling technology to spatially relate much of the information, making it apowerful tool for identifying, tracking and responding to disease patterns and health service needs.
ESRI software is extensively used by health organizations throughout the world, including the US Centers for Disease Control andPrevention (CDC), the World Health Organization (WHO), 112 national health ministries, and over 500 hospitals.www.esri.com/health
34-37 Company profiles:28 1/4/11 08:52 Page 34

World Hospitals and Health Services Vol. 47 No. 1 35
IHF corporate partners
owns the Capital’s six leading private hospitals all based in central London and each with an international reputation for the higheststandards of care. They are: The Wellington – the largest private hospital in Europe, The London Bridge Hospital, The Harley StreetClinic, The Portland Hospital for Women and Children, The Lister Hospital and The Princess Grace Hospital. HCA also has four outpatientand diagnostic centres – soon to be six – a blood and bone cancer treatment joint venture with the NHS at University College Hospital,The London Gamma Knife Centre, another joint venture with the NHS at St Bartholomew’s Hospital and Harley Street at Queen’s, aprivate patient cancer centre at the NHS Queen’s Hospital in Romford.
The six HCA hospitals treat around 300,000 patients per year. They also specialise in the most complex medical procedures includingcardiac care, liver transplantation, inter cranial surgery and complex cancer care. The HCA CancerCare network, for example, is thelargest provider of cancer care in the UK outside the NHS. Uniquely, HCA has its own clinical trials unit based in Harley Street in centralLondon. Medical teams in HCA are involved in research programmes aimed at finding new treatments in areas such as heart diseaseand cancer. In recent years HCA has invested around £250 million in capital expenditure including new diagnostic and treatmenttechnology. As an example, HCA has recently installed at The Harley Street Clinic, the revolutionary CyberKnife robotic radiotherapymachine, which is able to target previously untreatable tumours. It is the first machine of its kind in the UK.www.hcainternational.com
uses its 125 years of experience to help healthcare organizations create comfortable, safe and sustainable healing environments whileproviding measurable results. By utilizing our expertise in energy and sustainability, facilities, building and technology infrastructure,healthcare organizations can improve their financial results, the environment of care and their standing in the community. JohnsonControls provides design assist and construction management, funding solutions, network integration solutions for clinical and non-clinical systems, energy management and central utility plants, operations support and best practices, systems maintenance andfacility management services. Johnson Controls helps healthcare organizations create comfortable, safe and sustainable healingenvironments while providing measurable results.www.johnsoncontrols.com
a business of Ingersoll Rand – the world leader in creating and sustaining safe, comfortable and energy efficient environments –creates ideal environments of care for healthcare organizations all over the globe. Our products, services and solutions optimizethe link between the physical environment to patient outcomes, staff satisfaction/productivity and the bottom line.
Trane/Ingersoll Rand solutions optimize healing environments with a broad portfolio of energy efficient heating, ventilating andair conditioning systems, building and contracting services, parts support and advanced controls for healthcare buildings. Ourmarket-leading products also include electronic and biometric access control systems; time and attendance and personnelscheduling systems; mechanical locks and portable security, door closers and exit devices, steel doors and frames, architecturalhardware and technologies and services for global healthcare markets.www.Trane.com and www.ingersollrand.com
34-37 Company profiles:28 31/3/11 19:22 Page 35
IHF corporate partners
36 World Hospitals and Health Services Vol. 47 No. 1
ROYAL PHILIPS ELECTRONICS OF THE NETHERLANDS (NYSE: PHG, AEX: PHI) is a diversified health and well-being company, focused onimproving people’s lives through timely innovations. As a world leader in healthcare, lifestyle and lighting, Philips integratestechnologies and design into people-centric solutions, based on fundamental customer insights and the brand promise of “sense andsimplicity”. Headquartered in the Netherlands, Philips employs 119,000 employees in more than 60 countries worldwide. With sales ofEUR 25.4 billion in 2010, the company is a market leader in cardiac care, acute care and home healthcare, energy efficient lightingsolutions and new lighting applications, as well as lifestyle products for personal well-being and pleasure with strong leadershippositions in flat TV, male shaving and grooming, portable entertainment and oral healthcare. News from Philips is located atwww.philips.com/newscenter.
GE Healthcare's Performance Solutions business partners with hospitals and health systems across the globe to help improve theiroverall performance. The business provides knowledge solutions to reduce unnecessary waste - which comes in three forms (1)underutilization of resources (2) unintended clinical variation (3) and fragmented care delivery - and create safer more efficient patientcare. Performance Solutions leverages GE's operational improvement tools and advisory capabilities with GE Healthcare's clinical andtechnological capabilities, providing a unique combination of advisory, technology and healthcare expertise. The business splits itsglobal headquarters between Barrington, United States and Buc, France. Visit www.gehealthcare.com to learn more.
34-37 Company profiles:28 31/3/11 19:22 Page 36

00-01 Contents 47_1:27 31/3/11 18:09 Page 1
Reference
38 World Hospitals and Health Services Vol. 47 No. 1
IHF Governing Council 2009-2011
PresidentDr JOSE CARLOS DE SOUZAABRAHAOPresidentCONFEDERACAO NACIONALDE SAUDE (CNS)SRTVIS Quadra 701,Conjunto EEdificio Palacio do Radio 1Brasilia DF, CEP 70340-906BRAZIL
President-DesignateMr THOMAS C DOLANCEOAMERICAN COLLEGE OF HEALTHCARE EXECUTIVESOne North Franklin StreetSuite 1700Chicago, Illinois 60606-3491UNITED STATES OFAMERICA
Immediate Past PresidentsDr IBRAHIM A ALABDULHADIAssistant Undersecretaryfor Health Insurance AffairsMINISTRY OF HEALTHState of Kuwait PO Box 5, PIN Code 13001 KUWAIT
Mr GERARD VINCENTDélégué GénéralFEDERATION HOSPITALIEREDE FRANCE1 bis Rue Cabanis75014 ParisFRANCE
TreasurerDr LEKE PITANFormer Commissioner forHealth – Lagos StateHouse G40C, Road 2Victoria Garden City, LagosNIGERIA
Dr JUAN CARLOS LINARES DirectorCAMARA ARGENTINA DE EMPRESAS DE SALUD (CAES)Tucuman 1668, 2 PisoBuenos Aires C.P. 1050 ARGENTINA
Prof HELEN LAPSLEYResearch ProfessorCENTRE OF NATIONAL RESEARCH ON DISABILITY &REHABILITATION MEDICINEUniversity of Queensland3 Keston AvenueMosman, Sydney NSW 2088AUSTRALIA
Prof GUY DURANTAdministrateur généralCLINIQUES UNIVERSITAIRES SAINT-LUCAvenue Hippocrate 10B – 1200 BruxellesBELGIUM
Dr GEORG BAUMChief ExecutiveGERMAN HOSPITAL FEDERATIONWegelystrasse 310623 BerlinGERMANY
Dr LAWRENCE LAISenior AdvisorHONG KONG HOSPITAL AUTHORITY Room 1003, Administration BlockQueen Mary Hospital 102 Pokfulam Road HONG KONG (SAR)
Dr MUKI REKSOPRODJOInternational Relations INDONESIAN HOSPITAL ASSOCIATION (IHA) - PERHIMPUNAN RUMAH SAKIT SELURUH INDONESIA(PERSI)c/o Jl.H.R.Rasuna Said Kav.C-21 Kuningan JakartaSelatan 12940 INDONESIA
Dr TSUNEO SAKAIPresidentJAPAN HOSPITAL ASSOCIATION13-3 Ichibancho, Chiyodaku, TokyoJAPAN
Dr TAI-CHUN YOOPresident KOREAN HOSPITAL ASSOCIATION35-1, Mapo-Dong, Mapo-Gu, SeoulKOREA
Dr ERIK KREYBERG NORMANNProject DirectorDepartment of Hospital Services NORWEGIAN DIRECTORATE OF HEALTHP.O.Box 7000 St. Olavs plass, N-0130 OSLO, NORWAY
Prof CARLOS PEREIRA ALVESVice ChairASSOCIACAO PORTUGUESA PARA ODESENVOLVIMENTO HOSPITALAR(Portuguese Association for the Hospital Development)Av. António Augusto de Aguiar, 32-4º1050-016 LisboaPORTUGAL
Dr THABO LEKALAKALADirector - Hospital Management and Planning DEPARTMENT OF HEALTHStreet Hallmark Building 231 Proes Street001 PretoriaSOUTH AFRICA
Dr DELON WUPresidentTAIWAN HOSPITAL ASSOCIATION25F, No29-5Sec. 2, Jung jeng E. RoadDanshuei Township, Taipei CountyTAIWAN
Mrs ALISON KANTARAMAPresident UGANDA NATIONAL ASSOCIATION OF HOSPITALADMINISTRATORS (UNAHA)Mulago HospitalPO Box 7051, KampalaUGANDA
Mr ABDUL SALAM AL-MADANIPresident INDEX HOLDING Dubai Healthcare CityBlock B, Offices 203 – 303P.O.Box 13636, Dubai UNITED ARAB EMIRATES
SIR KEITH PEARSON ChairmanNHS CONFEDERATION29, Bressenden PlaceLondon SW1E 5DDUNITED KINGDOM
THE EXECUTIVE COMMITTEE
38-40 Governing council-diary:29 7/4/11 14:24 Page 38

Reference
World Hospitals and Health Services Vol. 47 No. 1 39
2011 Events
IHF
37th World Hospital Congress8-10 November 2011, Dubai, United Arab Emirates Theme: “Healthcare in a Changing World: Overcoming the Challenges” Email: [email protected]; [email protected] Website: http://www.ihfdubai.ae
MEMBERS
CANADA
2011 National Healthcare Leadership ConferenceJune 6-7, 2011 at the Whistler Conference Centre in beautiful Whistler, British Columbia, Canada. The theme will be "Rising to the Challenge: Resources, Realities and Relationships". For more information: http://www.healthcareleadershipconference.ca/
FRANCE
Federation Hospitaliere de France: Geront-expo / Handicap-expo May 17-19, 2011 For more information: http://www.gerontexpo.com/default.asp
36ème Congrès de la FEHAP October 5, 6 and 7, 2011, la Cité des Congrès de Lyon, LyonFor more information: http://congres.fehap.fr/
HONG KONG
2011 Hong Kong Hospital Association Annual Convention7-8 June 2011, Hong Kong
HUNGARY
The Hungarian Hospital Association XXIII CongressApril 13-15, 2011. For more information: http://www.mkszkongresszus.hu/altalanos_informaciok
SWITZERLAND
2011 National Healthcare Leadership ConferenceJune 6-7, 2011 at the Whistler Conference Centre in beautiful Whistler, British Columbia, Canada. The theme will be "Rising to the Challenge: Resources, Realities and Relationships". For more information:http://www.healthcareleadershipconference.ca/
USA
2011 Congress on Healthcare Leadership, March 21-24, 2011, Chicago, Illinois, Hilton Chicago and Palmer HouseHilton. Beginning on March 21, approximately 4,500 healthcare leaders from more than 20 countries will gather in Chicago for four days ofeducational seminars, lectures, networking opportunities and other special events. During the meeting, seminar presenters will discussemerging trends in the field of healthcare management, including topics such as patient safety and quality, environmental sustainability,innovative technologies, financial challenges, leadership strategies and more.
Future Congress on Healthcare LeadershipMarch 19-22, 2012, in Chicago, Illinois, Hyatt Regency Chicago. For more information on 2011 Congress, visit: ache.org/Congress
38-40 Governing council-diary:29 31/3/11 19:23 Page 39

American Hospital Association: AHA Annual Membership Meeting Theme – Pursuing Excellence. One Vision, OneVoiceApril 10-13, 2011 Hilton Hotel, Washington DC.
COLLABORATIVE
SINGAPORE
Hospital Management Asia 2011 (HMA2011) 7 & 8 September 2011, SingaporeFor more information: http://hospitalmanagementasia.com/
GERMANY
8th MCC Congress, Strategic Options for the Hospital Market, collaborative event with IHFSeptember 22-23, 2011, Berlin, Germany. For more information: www.hospitalworld.info
2012MEMBERS
USA
Congress on Healthcare Leadership 19-22 March 2012, Hyatt Regency Chicago, Chicago, Illinois For more information: http://ache.org/Congress
2013IHF
38th World Hospital Congress 18-20 June, Oslo, NorwayEmail: [email protected]
Reference
40 World Hospitals and Health Services Vol. 47 No. 1
38-40 Governing council-diary:29 7/4/11 14:32 Page 40

34-37 Company profiles:28 1/4/11 08:52 Page 38
00-01 Contents 46_8:27 4/1/11 13:05 Page 1