Embed Size (px)
Citation preview
World Health Organization Recommendations on Caregiving Interventions to
Support Early Child Development in the First Three Years of Life:
Report of the systematic review of evidence
Joshua Jeong PhD, Emily Franchett MSc, Aisha K. Yousafzai PhD
Department of Global Health and Population
Harvard T.H. Chan School of Public Health
12 November 2018
(finalized 08 Feb 2020)
Contact information:
Aisha K. Yousafzai, PhD
Associate Professor
Department of Global Health and Population
Harvard T.H. Chan School of Public Health
665 Huntington Avenue, Boston, MA 02115, USA
Email: [email protected]

2 | P a g e
Executive summary
An estimated 250 million children are at risk of not achieving their developmental
potential in the first 5 years of life. Policies and programmes that enable caregivers to support
young children’s development are critical. Evidence in the series Early childhood development:
from science to scale published in the Lancet in 2017 highlighted the importance of nurturing
care comprising caregivers’ practices with respect to health, nutrition, safety and security,
responsive caregiving, and early learning opportunities that support children’s healthy
development. The health sector plays a critical role in delivering key nurturing care
interventions, and there is opportunity to strengthen the nurturing care approach in health
services and in partnership with other sectors. In order to guide the health sector, the World
Health Organization (WHO) intends to develop evidence-based guidelines for approaches to
improve early childhood development (ECD) enabling Member States to make informed
decisions about a range of policy and programme actions in their efforts to achieve targets in the
Sustainable Development Goals pertaining to health, learning and behaviour for human
development. These guidelines will complement and support existing WHO guidelines and tools
relevant to nurturing care.
A Guideline Development Group (GDG) comprising experts in the field of ECD and
health proposed four1 key research questions for review of evidence to inform recommendations
relating to early learning and responsive care.
1. What is the effectiveness of responsive caregiving on ECD in the first 3 years of life?
2. What is the effectiveness of caregiving interventions that promote early learning on ECD
in the first 3 years of life?
3. What is the effectiveness of caregiving to support healthy child socioemotional and
behavioural development on ECD in the first 3 years of life?
4. What are the effects of combined caregiving and nutrition programmes on ECD and child
growth outcomes in the first 3 years of life?
In many interventions, strategies to promote early learning and responsive caregiving were
combined; therefore, it was agreed to carry out additional analysis related to the first two
questions:
2.1 What is the effectiveness of caregiving interventions that combine both responsive
caregiving and the promotion of early learning on ECD in the first 3 years of life?
1 A fifth question was addressed in a separate review.

3 | P a g e
2.2. What is the effectiveness of any caregiving interventions (responsive caregiving, promotion
of early learning, or combined responsive caregiving and the promotion of early learning) on
ECD in the first 3 years of life.
This report is a synthesis of the evidence undertaken by a systematic review team at the
Harvard T.H. Chan School of Public Health. In total, across the four original questions we report
on 67 studies (77 records): question 1 (n = 17 studies, 19 records), question 2 (n = 22 studies, 22
records), question 3 (n = 10 studies, 11 records), and question 4 (n = 18 studies, 25 records),
were identified for review. Outcomes assessed included ECD, attachment, child behaviour, child
growth, child health and nutrition, caregiving knowledge, caregiving practices, caregiver-child
interactions, and caregivers’ mental health. Quality of evidence was assessed using the Grading
of Recommendations Assessment, Development and Evaluation (GRADE) approach. The final
recommendations based on the quality of the evidence will be determined by the GDG informed
by evidence-to-decision making tables for the key research questions.
4 | P a g e
Acknowledgments
We are grateful to the members of the systematic review team at the Harvard T.H. Chan
School of Public Health for their contributions to reviewing studies and synthesizing evidence
for analysis: Alastair Fung, Raghbir Kaur, Helen Pitchik, Vijayaragavan Prabakaran, Clariana
Vitória Ramos, Mathilda Regan, Katharine Robb, Rucha Shelgikar, and Yu-Cheng Tsai. We
thank Carol Mita, librarian at the Francis A. Countway Library of Medicine, Harvard Medical
School and Boston Medical Library, for her assistance in the literature search. We also thank the
GDG chaired by Jane Fisher, Monash University, for its contributions to the process of the
review of evidence. The support and guidance of the WHO team, including Bernadette
Daelmans, Tarun Dua and Nigel Rollins, is gratefully acknowledged.
5 | P a g e
Table of contents
Executive summary ......................................................................................................................... 2
Acknowledgments........................................................................................................................... 4
Introduction and scope of the review .............................................................................................. 7
Methods......................................................................................................................................... 12
Evidence and recommendations for responsive caregiving interventions (PICO 1) .................... 22
Evidence and recommendations for caregiving interventions that promote early learning (PICO
2) ................................................................................................................................................... 26
Evidence and recommendations for caregiving interventions that combine responsive caregiving
and promotion of early learning: additional analysis 2.1 .............................................................. 31
Evidence and recommendations for all caregiving interventions that deliver responsive
caregiving, promotion of early learning, or combined responsive caregiving and promotion of
early learning: Additional analysis 2.2 ......................................................................................... 36
Evidence and recommendations for caregiving interventions to support healthy child
socioemotional and behavioural development (PICO 3) .............................................................. 39
Evidence and recommendations for combined caregiving and nutrition interventions (PICO 4) 44
Research gaps................................................................................................................................ 58
References ..................................................................................................................................... 59
Appendix A: Glossary................................................................................................................... 69
Appendix B: List of Guideline Development Group Members .................................................... 74
Appendix C: Summary of interventions for all included studies in the systematic reviews ........ 75
Appendix D: GRADE tables and analysis for responsive caregiving interventions (n=17) ........ 76
Appendix E: GRADE tables and analysis for caregiving interventions to support early learning
opportunities (n=22) ..................................................................................................................... 85
Appendix F: GRADE tables and analysis for combined responsive caregiving and the promotion
of early learning interventions (n=42) .......................................................................................... 94
Appendix G: GRADE tables and analysis for caregiving interventions for responsive caregiving,
early learning, or a combined responsive caregiving and promotion of early learning intervention
(n=81) .......................................................................................................................................... 103
Appendix H: GRADE tables and analysis for caregiving interventions to support healthy child
socioemotional and behavioural development (n=10) ................................................................ 112
Appendix I: GRADE tables and analysis for integrated caregiving and nutrition interventions
(n=18) .......................................................................................................................................... 117
6 | P a g e
Abbreviations and acronyms2
BSID Bayley Scale of Infant and Toddler Development
CBCL Child Behavior Check List
CES-D Center for Epidemiological Studies Depression Scale
CI Confidence interval
c-RCT Cluster randomized controlled trial
ECD Early childhood development
ES Effect size
GDG Guideline Development Group
GRADE Grading of Recommendations Assessment, Development and Evaluation
HAZ Height-for-age Z-score
HIC High-income country
HOME Home Observation for Measurement of the Environment
ITSEA Infant-Toddler Social Emotional Assessment
LMIC Low- and middle-income country
NCAST Nursing Child Assessment Satellite Teaching
PICO Population/Problem, Intervention, Comparison/Control, Outcome
PROSPERO Prospectively registered systematic reviews in health and social care, welfare,
public health, education, crime, justice, and international development
RCT Randomized controlled trial
SDQ Strengths and Difficulties Questionnaire
WAZ Weight-for-age Z-score
WHO World Health Organization
WHZ Weight-for-height Z-score
2 See Appendix A for Glossary of terms.

7 | P a g e
Introduction and scope of the review
An estimated 250 million children are at risk of not achieving their developmental
potential in the first 5 years of life (Lu et al., 2016). Policies and programmes that enable
caregivers to support young children’s development are critical. Evidence in the series Early
childhood development: from science to scale published in the Lancet highlighted the importance
of nurturing care comprising caregiver and family practices in health, nutrition, safety and
security, responsive caregiving, and early learning opportunities that support children’s healthy
development (Figure 1) (Black et al., 2017; Britto et al., 2017; Richter et al., 2017). A central
tenant of the nurturing care concept is the process of care encompassing caregiving practices
such as caregiver sensitivity to children’s physical and emotional needs, protection from harm,
provision of opportunities for exploration and learning, and interactions with young children that
are responsive, emotionally supportive, and cognitively stimulating.
Figure 1. Domains of nurturing care (Black et al., 2017).
While all sectors have roles and responsibilities in promoting policies and programmes
for nurturing care, the health sector plays a particularly important role during the first 3 years of
life (from conception to 2 years of age). Firstly, the health sector can reach the youngest
children and their caregivers in the first 3 years of life to promote protective care and mitigate
risk factors in an especially important and sensitive period of brain development (Nelson, 2000).
Secondly, health services commonly implement components of nurturing care (e.g. breastfeeding
promotion or the Integrated Management of Childhood Illness) that reduce risks for childhood
mortality and morbidity as well as support early development but could potentially be
strengthened with a holistic approach to the provision of nurturing care (Aboud & Yousafzai,
8 | P a g e
2016; Britto et al., 2017). Thirdly, the health sector can play a strong role in leveraging
partnerships across sectors that enable the coordination of services for young children (Richter et
al., 2017).
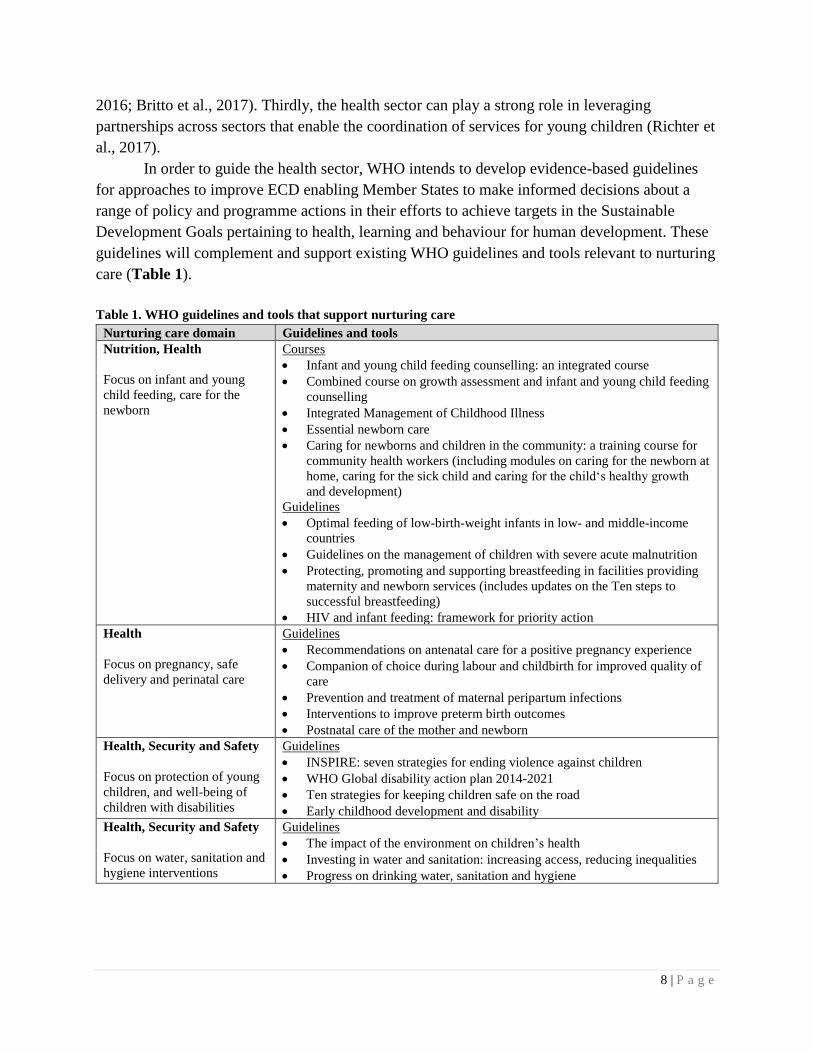
In order to guide the health sector, WHO intends to develop evidence-based guidelines
for approaches to improve ECD enabling Member States to make informed decisions about a
range of policy and programme actions in their efforts to achieve targets in the Sustainable
Development Goals pertaining to health, learning and behaviour for human development. These
guidelines will complement and support existing WHO guidelines and tools relevant to nurturing
care (Table 1).
Table 1. WHO guidelines and tools that support nurturing care
Nurturing care domain Guidelines and tools
Nutrition, Health
Focus on infant and young
child feeding, care for the
newborn
Courses
• Infant and young child feeding counselling: an integrated course
• Combined course on growth assessment and infant and young child feeding
counselling
• Integrated Management of Childhood Illness
• Essential newborn care
• Caring for newborns and children in the community: a training course for
community health workers (including modules on caring for the newborn at
home, caring for the sick child and caring for the child‘s healthy growth
and development)
Guidelines
• Optimal feeding of low-birth-weight infants in low- and middle-income
countries
• Guidelines on the management of children with severe acute malnutrition
• Protecting, promoting and supporting breastfeeding in facilities providing
maternity and newborn services (includes updates on the Ten steps to
successful breastfeeding)
• HIV and infant feeding: framework for priority action
Health
Focus on pregnancy, safe
delivery and perinatal care
Guidelines
• Recommendations on antenatal care for a positive pregnancy experience
• Companion of choice during labour and childbirth for improved quality of
care
• Prevention and treatment of maternal peripartum infections
• Interventions to improve preterm birth outcomes
• Postnatal care of the mother and newborn
Health, Security and Safety
Focus on protection of young
children, and well-being of
children with disabilities
Guidelines
• INSPIRE: seven strategies for ending violence against children
• WHO Global disability action plan 2014-2021
• Ten strategies for keeping children safe on the road
• Early childhood development and disability
Health, Security and Safety
Focus on water, sanitation and
hygiene interventions
Guidelines
• The impact of the environment on children’s health
• Investing in water and sanitation: increasing access, reducing inequalities
• Progress on drinking water, sanitation and hygiene
9 | P a g e
While these guidelines and tools support ECD and highlight the importance of the nurturing care
domains of responsive caregiving and early learning, there is a need to develop focused
guidelines to better integrate a range of caregiving interventions in health and other services.
Aims and objectives of the guideline
The aim of the guideline is to improve ECD. The three objectives of are to:
1. identify ECD-specific interventions that are effective in improving developmental
outcomes in children;
2. identify effective, feasible approaches to deliver interventions to improve ECD outcomes;
3. consolidate in one guideline WHO-recommended interventions that promote ECD.
The target audience for the guideline includes district and sub-national health managers, health
workers, development agencies and implementing partners, nongovernmental organizations and
policy-makers working in the area of maternal and child health.
The guideline will be developed following the process outlined in the WH O Handbook
for guideline development, second edition. The Departments of Maternal, Newborn, Child and
Adolescent Health and Mental Health and Substance Abuse have identified experts for the GDG.
A scoping meeting was convened in September 2017 to formulate questions to be addressed in
systematic reviews to inform the recommendations of the GDG (see Appendix B for list of GDG
members).
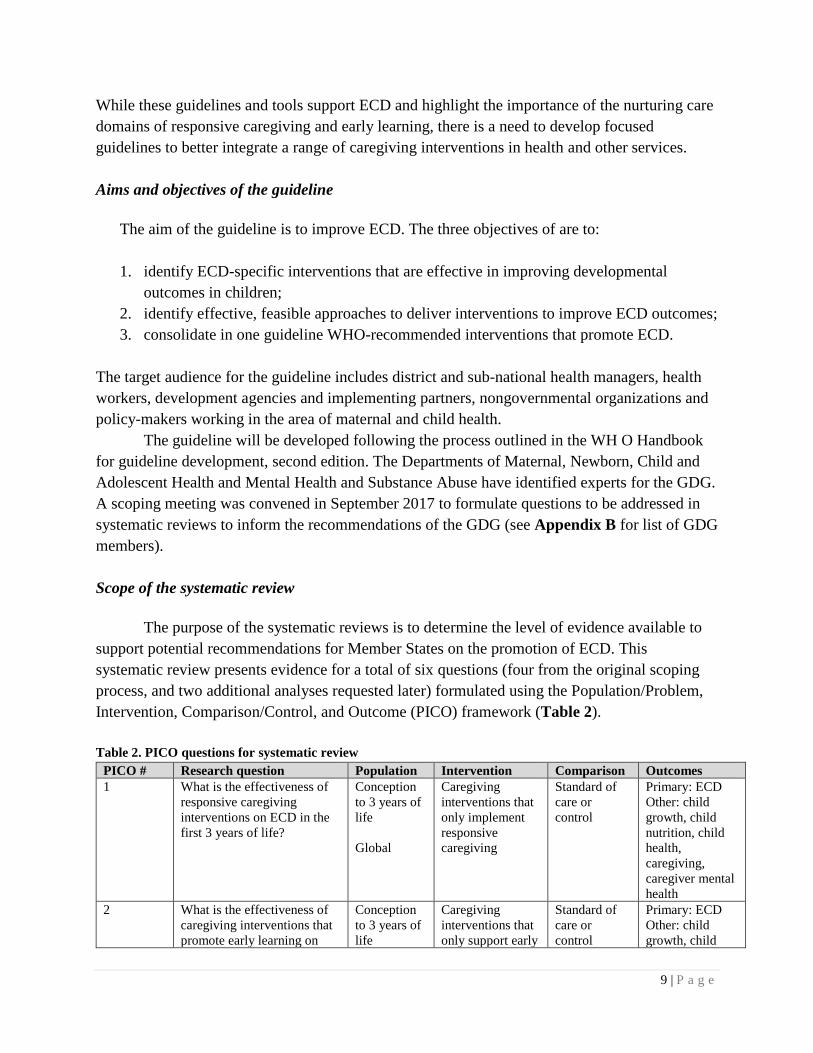
Scope of the systematic review
The purpose of the systematic reviews is to determine the level of evidence available to
support potential recommendations for Member States on the promotion of ECD. This
systematic review presents evidence for a total of six questions (four from the original scoping
process, and two additional analyses requested later) formulated using the Population/Problem,
Intervention, Comparison/Control, and Outcome (PICO) framework (Table 2).
Table 2. PICO questions for systematic review
PICO # Research question Population Intervention Comparison Outcomes
1 What is the effectiveness of
responsive caregiving
interventions on ECD in the
first 3 years of life?
Conception
to 3 years of
life
Global
Caregiving
interventions that
only implement
responsive
caregiving
Standard of
care or
control
Primary: ECD
Other: child
growth, child
nutrition, child
health,
caregiving,
caregiver mental
health
2 What is the effectiveness of
caregiving interventions that
promote early learning on
Conception
to 3 years of
life
Caregiving
interventions that
only support early
Standard of
care or
control
Primary: ECD
Other: child
growth, child

10 | P a g e
PICO # Research question Population Intervention Comparison Outcomes
ECD in the first 3 years of
life?
Global
learning and
development
nutrition, child
health,
caregiving,
caregiver mental
health
2.1
(additional
analysis)
What is the effectiveness of
caregiving interventions that
combine both responsive
caregiving and the promotion
of early learning on ECD in
the first 3 years of life?
Conception
to 3 years of
life
Global
Caregiving
interventions with
components of
both responsive
caregiving and the
promotion of
early learning
Standard of
care or
control
Primary: ECD
Other: child
attachment, child
growth, child
nutrition, child
health,
caregiving,
caregiver mental
health
2.2
(additional
analysis)
What is the effectiveness of
any caregiving interventions
(responsive caregiving,
promotion of early learning,
or combined responsive
caregiving and the promotion
of early learning) on ECD in
the first 3 years of life?
Conception
to 3 years of
life
Global
All interventions
from PICOs 1, 2,
and 2.1 are
included
Standard of
care or
control
Primary: ECD
Other: child
attachment, child
growth, child
nutrition, child
health,
caregiving,
caregiver mental
health
3 What is the effectiveness of
caregiving to support healthy
child socioemotional and
behavioural development on
ECD in the first 3 years of
life?
Conception
to 3 years of
life
Global
Caregiving to
support healthy
socioemotional
and behavioural
development
Standard of
care or
control
Primary: ECD
Other: child
growth, child
nutrition, child
health,
caregiving,
caregiver mental
health
4 What are the effects of
combined caregiving and
nutrition programmes on
ECD and child growth
outcomes in the first 3 years
of life?
• What are the
independent and additive
effects of caregiving and
nutrition interventions on
ECD and child growth
outcomes in the first 3
years of life?
• Do the effects on ECD
and child growth
outcomes differ between
programmes that are
targeted for young
children with moderate
to severe malnutrition
compared to general
programmes?
Conception
to 3 years of
life
Global
Combined
caregiving and
nutrition
interventions
Standard of
care or
control
Primary: ECD,
child growth
Other: child
attachment, child
nutrition, child
health,
caregiving,
caregiver mental
health

11 | P a g e
The components of nurturing care interventions addressed in this review are responsive
caregiving and support for early learning and development. We organized the analysis by
whether the intervention focuses only on one component or whether it combines both
components (i.e. responsive caregiving and support for early learning and development), which
we reference as PICO questions 1, 2 and additional analysis 2.1 and 2.2 respectively.
A challenge in the literature is the wide application of definitions of the nurturing care
components (responsive caregiving and support for early learning and development), which are
not consistently operationalized in the studies. Therefore, a central aspect to the review process
was to establish a clear definition for each nurturing care component, which iteratively evolved
over the first weeks of the data extraction process as the team reviewed and discussed each
intervention. This categorization is broad and is based on often limited descriptions reported
about the interventions in the published studies; however, a degree of delineation was feasible.
The purpose of the additional analysis (2.2) which includes all the caregiving interventions
together by merging intervention studies under PICO 1, 2 and 2.1 was to acknowledge that broad
categorization and the potential for overlap across intervention strategies. A general conclusion
may be drawn about the effect of general caregiving interventions to support ECD from the
additional analysis.
However, the PICO questions were not framed to ask whether a specific caregiving
component had greater or lesser effects on ECD than another, and studies have not been designed
to address this question. Thus, the purpose of the additional analysis was not to compare the
different components (i.e. support for early learning and responsive caregiving). It is
recommended that any comparisons of caregiving components are interpreted with caution given
the wide range of applications of these concepts, the diverse approaches to combining these
concepts and the variation in the implementation characteristics for the interventions.
12 | P a g e
Methods
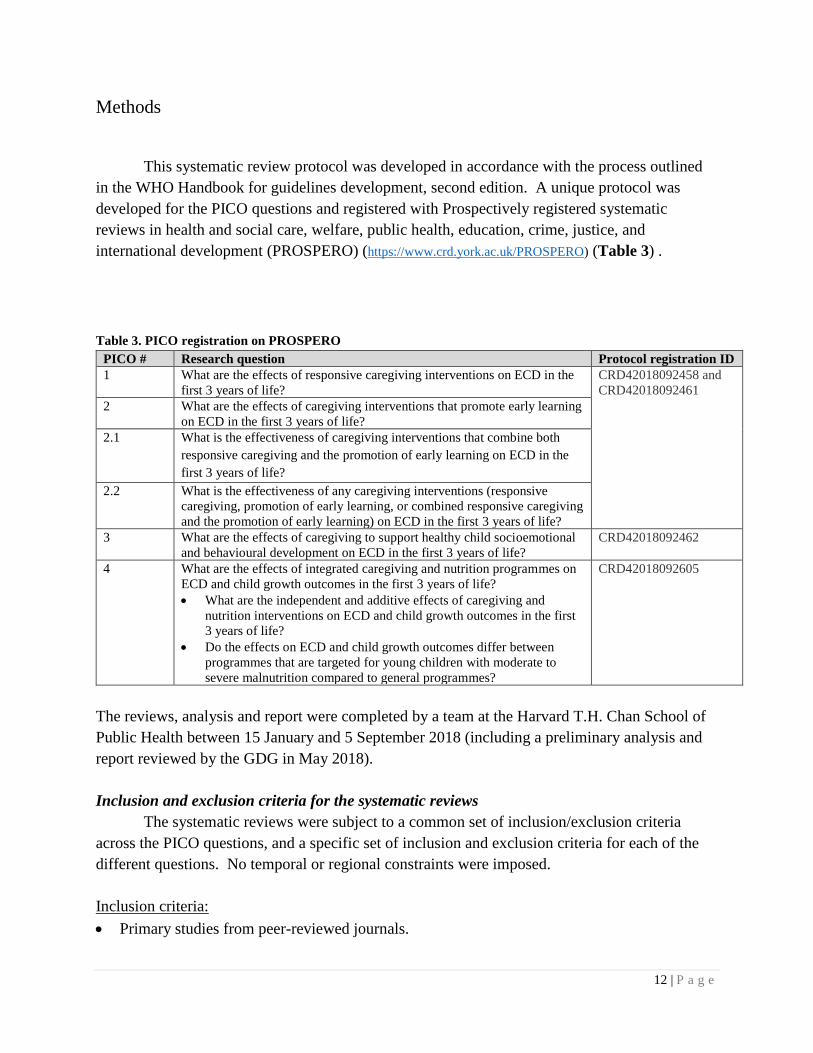
This systematic review protocol was developed in accordance with the process outlined
in the WHO Handbook for guidelines development, second edition. A unique protocol was
developed for the PICO questions and registered with Prospectively registered systematic
reviews in health and social care, welfare, public health, education, crime, justice, and
international development (PROSPERO) (https://www.crd.york.ac.uk/PROSPERO) (Table 3) .
Table 3. PICO registration on PROSPERO
PICO # Research question Protocol registration ID
1 What are the effects of responsive caregiving interventions on ECD in the
first 3 years of life?
CRD42018092458 and
CRD42018092461
2 What are the effects of caregiving interventions that promote early learning
on ECD in the first 3 years of life?
2.1 What is the effectiveness of caregiving interventions that combine both
responsive caregiving and the promotion of early learning on ECD in the
first 3 years of life?
2.2 What is the effectiveness of any caregiving interventions (responsive
caregiving, promotion of early learning, or combined responsive caregiving
and the promotion of early learning) on ECD in the first 3 years of life?
3 What are the effects of caregiving to support healthy child socioemotional
and behavioural development on ECD in the first 3 years of life?
CRD42018092462
4 What are the effects of integrated caregiving and nutrition programmes on
ECD and child growth outcomes in the first 3 years of life?
• What are the independent and additive effects of caregiving and
nutrition interventions on ECD and child growth outcomes in the first
3 years of life?
• Do the effects on ECD and child growth outcomes differ between
programmes that are targeted for young children with moderate to
severe malnutrition compared to general programmes?
CRD42018092605
The reviews, analysis and report were completed by a team at the Harvard T.H. Chan School of
Public Health between 15 January and 5 September 2018 (including a preliminary analysis and
report reviewed by the GDG in May 2018).
Inclusion and exclusion criteria for the systematic reviews
The systematic reviews were subject to a common set of inclusion/exclusion criteria
across the PICO questions, and a specific set of inclusion and exclusion criteria for each of the
different questions. No temporal or regional constraints were imposed.
Inclusion criteria:
• Primary studies from peer-reviewed journals.
13 | P a g e
• Interventions targeted toward caregivers, which we define using a modified operational
definition of a caregiving programme from UNICEF as one that incorporates “activities,
programmes, services or interventions, for caregivers, aimed at improving caregiver
interaction, behaviors, knowledge, beliefs, attitudes and practices” (Britto et al., 2015).
Caregivers were defined as the legal guardian, biological parent, or adult responsible for the
well-being of the child.
• Interventions that were evaluated using a randomized controlled study design with at least
one control group and one intervention group.
• Interventions that targeted children and their caregivers in the early life course (pregnancy
through the first 3 years of life).
• Interventions that assessed at least one measure of ECD (cognition, language, motor,
socioemotional development) or behaviour as a primary outcome.
• Evaluations that assessed outcomes immediately after the completion of the intervention (or
shortly thereafter).
Exclusion criteria:
• Interventions that targeted children who were preterm or who have a chronic illness, very
low birth weight, or disability.3
• Interventions conducted with caregivers who have an illness or disability.
• Interventions that were not evaluated using a randomized controlled study design.
• Interventions that were not relevant to caregiving.
• Interventions that did not assess at least one ECD outcome.
• Interventions that enrolled children older than 3 years of age (on average).
Literature search and screening
The research team worked closely with a research librarian with expertise in
comprehensive bibliographic database searching. Intervention studies were searched across five
electronic bibliographic databases: EMBASE, PubMed, PsycINFO, Cochrane Central Register of
Controlled Trials (CENTRAL), and ERIC. Search strategies were developed in accordance with
each database. A string of keywords was determined to capture four broad categories: (1)
caregiving interventions, (2) targeting children aged from pregnancy through 3 years, (3) that
were evaluated using a randomized controlled study design, and (4) assessed an ECD outcome.
Keywords were informed by search terms and keywords used in prior systematic reviews related
to caregiving interventions (Aboud & Yousafzai, 2015; Britto et al., 2017; Eshel et al., 2006;
Mol et al., 2008), as well as through consultations with the research librarian to select relevant
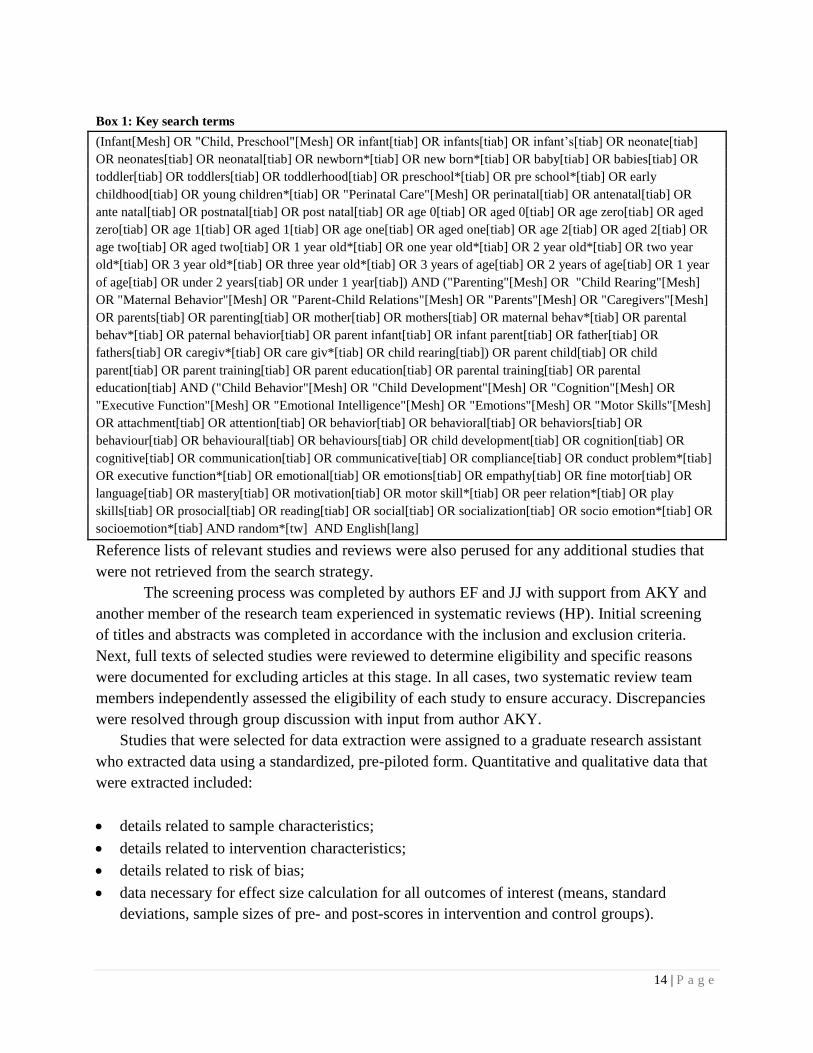
MESH terms and search filters. The full list of key search terms is shown in Box 1.
3 Interventions targeting children with low birth weight (< 2500g) were included and interventions targeting children
with very low birth weight alone excluded (< 1500g).
14 | P a g e
Box 1: Key search terms
(Infant[Mesh] OR "Child, Preschool"[Mesh] OR infant[tiab] OR infants[tiab] OR infant’s[tiab] OR neonate[tiab]
OR neonates[tiab] OR neonatal[tiab] OR newborn*[tiab] OR new born*[tiab] OR baby[tiab] OR babies[tiab] OR
toddler[tiab] OR toddlers[tiab] OR toddlerhood[tiab] OR preschool*[tiab] OR pre school*[tiab] OR early
childhood[tiab] OR young children*[tiab] OR "Perinatal Care"[Mesh] OR perinatal[tiab] OR antenatal[tiab] OR
ante natal[tiab] OR postnatal[tiab] OR post natal[tiab] OR age 0[tiab] OR aged 0[tiab] OR age zero[tiab] OR aged
zero[tiab] OR age 1[tiab] OR aged 1[tiab] OR age one[tiab] OR aged one[tiab] OR age 2[tiab] OR aged 2[tiab] OR
age two[tiab] OR aged two[tiab] OR 1 year old*[tiab] OR one year old*[tiab] OR 2 year old*[tiab] OR two year
old*[tiab] OR 3 year old*[tiab] OR three year old*[tiab] OR 3 years of age[tiab] OR 2 years of age[tiab] OR 1 year
of age[tiab] OR under 2 years[tiab] OR under 1 year[tiab]) AND ("Parenting"[Mesh] OR "Child Rearing"[Mesh]
OR "Maternal Behavior"[Mesh] OR "Parent-Child Relations"[Mesh] OR "Parents"[Mesh] OR "Caregivers"[Mesh]
OR parents[tiab] OR parenting[tiab] OR mother[tiab] OR mothers[tiab] OR maternal behav*[tiab] OR parental
behav*[tiab] OR paternal behavior[tiab] OR parent infant[tiab] OR infant parent[tiab] OR father[tiab] OR
fathers[tiab] OR caregiv*[tiab] OR care giv*[tiab] OR child rearing[tiab]) OR parent child[tiab] OR child
parent[tiab] OR parent training[tiab] OR parent education[tiab] OR parental training[tiab] OR parental
education[tiab] AND ("Child Behavior"[Mesh] OR "Child Development"[Mesh] OR "Cognition"[Mesh] OR
"Executive Function"[Mesh] OR "Emotional Intelligence"[Mesh] OR "Emotions"[Mesh] OR "Motor Skills"[Mesh]
OR attachment[tiab] OR attention[tiab] OR behavior[tiab] OR behavioral[tiab] OR behaviors[tiab] OR
behaviour[tiab] OR behavioural[tiab] OR behaviours[tiab] OR child development[tiab] OR cognition[tiab] OR
cognitive[tiab] OR communication[tiab] OR communicative[tiab] OR compliance[tiab] OR conduct problem*[tiab]
OR executive function*[tiab] OR emotional[tiab] OR emotions[tiab] OR empathy[tiab] OR fine motor[tiab] OR
language[tiab] OR mastery[tiab] OR motivation[tiab] OR motor skill*[tiab] OR peer relation*[tiab] OR play
skills[tiab] OR prosocial[tiab] OR reading[tiab] OR social[tiab] OR socialization[tiab] OR socio emotion*[tiab] OR
socioemotion*[tiab] AND random*[tw] AND English[lang]
Reference lists of relevant studies and reviews were also perused for any additional studies that
were not retrieved from the search strategy.
The screening process was completed by authors EF and JJ with support from AKY and
another member of the research team experienced in systematic reviews (HP). Initial screening
of titles and abstracts was completed in accordance with the inclusion and exclusion criteria.
Next, full texts of selected studies were reviewed to determine eligibility and specific reasons
were documented for excluding articles at this stage. In all cases, two systematic review team
members independently assessed the eligibility of each study to ensure accuracy. Discrepancies
were resolved through group discussion with input from author AKY.
Studies that were selected for data extraction were assigned to a graduate research assistant
who extracted data using a standardized, pre-piloted form. Quantitative and qualitative data that
were extracted included:
• details related to sample characteristics;
• details related to intervention characteristics;
• details related to risk of bias;
• data necessary for effect size calculation for all outcomes of interest (means, standard
deviations, sample sizes of pre- and post-scores in intervention and control groups).

15 | P a g e
All data extraction team members were trained to use the data extraction sheet and received a
detailed standard operating protocol that included a set of standardized definitions for
intervention characteristics. EF held weekly in-person meetings with all data extractors to
monitor team progress and address any discrepancies that arose in the data extraction process.
All data extraction forms were reviewed by EF and JJ on a weekly basis. For additional quality
assurance, 50% of included articles were subsampled for quality assurance by either EF or JJ
during the first three weeks of data extraction while research assistants were familiarizing
themselves with the process. During the remaining weeks of the data extraction process, 20% of
studies were subsampled for quality assurance by EF, JJ or AKY.4 The flow of articles from the
original search through the final selected studies is shown using the Preferred Reporting Items
for Systematic Reviews and Meta-Analyses flow diagram (Figure 2).
The review was submitted mid-April 2018. Following a review of the preliminary analysis by the
GDG in May 2018, all excluded articles were rescreened by EF, JJ and AKY, and any additional
data extraction was managed by EF and JJ. This was to include interventions targeting children
with low birth weight and to include studies with a sample size smaller than 85 that had been
excluded in the original analysis. Responses to GDG reviews were submitted on Sept 5th 2018
following the May 2018 GDG meeting.
4Data extraction between June and August 2018.

16 | P a g e
Figure 2. Data screening and selection process5
5 A second search without English language restrictions was completed. This generated 439 unique studies which we
did not review due to resource limitations.
9,579 unique records identified
from search of 5 databases
11 additional records identified
from other sources
9,590 titles of records screened
923 records excluded
259 full-texts of records assessed for
eligibility 159 records excluded•62 - no ECD outcome
assessed
•41 – children are older than
age-3 years
•21 – not a caregiving
intervention
•18 – longer term follow-
up/secondary analysis of a
program
•17 - clinically targeted
population
•10 – not an RCT90 records included in systematic review
and meta-analysis
1,182 abstracts of records screened
8,408 records excluded
19 records in PICO 1
(n=17 studies)
22 records in PICO 2
(n=22 studies)
49 records in PICO 3
(n=42 studies)
25 records in PICO 4
(n=18 studies)
17 | P a g e
Assessment of risk of bias of individual studies
Each individual study selected for the review was assessed for risk of bias using the
criteria outlined by the Cochrane risk of bias assessment tool for randomized controlled trials
recommended by the Cochrane Handbook version 5.1.0. The risk of bias in the included studies
was assessed alongside the data extraction process by considering the following characteristics:
(1) randomization sequence generation; (2) concealment of allocation to treatment group; (3)
blinding of participants and investigators; (4) reporting of data on all study participants (taking
into account attrition and exclusions); (5) complete reporting of all study outcomes that were
specified a priori; (6) other sources of bias (including considerations around measurement
reliability and validity). Disagreements between the team members over the risk of bias
inparticular studies were resolved by group discussion with involvement of AKY where
necessary.
Synthesis, analysis, and reporting
A challenge in the literature is the wide application of definitions for caregiving (or
parenting) interventions, which are not consistently defined in the literature. Therefore, a central
aspect to the review process was to establish a clear definition for each type of intervention,
which iteratively evolved over the first weeks of the data extraction process as the team reviewed
and discussed each intervention (see Table 4 describing how each intervention was defined for
analysis).
A meta-analysis was conducted for each of the following outcomes: ECD, child
behaviour, child attachment, child growth, child nutrition, child health, caregiving (practices,
knowledge, and caregiver-child interactions), and caregiver mental health if the number of
available studies for the specific outcome was sufficient.
• Standardized tools were selected over non-standardized tools or study-specific tools.
• Comprehensive assessments were selected over screens or single items.
A predetermined decision-making matrix was developed for situations where a study reported
more than one result for a specific outcome of interest. This was considered the most
parsimonious approach as recommended by statistical advisors. The decision-making matrix was
informed by the developmental theory for language and motor development. Across the pool of
80 studies from which data were extracted, this applied to five studies reporting language
development and two studies reporting motor development. Given the small number of studies
dispersed across the PICO questions and the underlying theoretical rationale, a sensitivity
analysis was not conducted.
18 | P a g e
• For child language, receptive language was selected over expressive language (if a
combined score was not possible to ascertain due to the assessment tool used, the degree
of adaptation/modification to any tool or limitations in the data reported). Children
typically develop receptive language skills first, and this is especially important in the age
group of interest (i.e. 0-3 years) in this meta-analysis.
• For child motor development, fine motor was selected over gross motor (if a combined
score was not possible to ascertain due to the assessment tool used, the degree of
adaptation/modification to any tool or limitations in the data reported). There is evidence
in the literature indicating an association between the development of fine motor skills in
early life with subsequent learning and development.
For child behavioural problems, separate analyses were undertaken for internalizing and
externalizing problem behaviours. If multiple behavioural scores were reported in either category
which could not be separated using developmental theory, then the protocol adopted by Tanner-
Smith and Tipton (2014) was followed. The robust variance estimation allows adjustment for
correlated effect sizes between the different outcomes from the same study for a given domain.
In each PICO question, a sub-analysis was also conducted by regional context: globally,
high-income countries (HICs), and low- and middle-income countries (LMICs). PICOs 1 and 2
were predominantly studies from HICs, 2.1 and 2.2 were a mixture of both HICs and LMICs,
and PICOs 3 and 4 comprised studies only from HICs.
Quantitative data synthesis was conducted with either fixed or random effects meta-
analysis based on a test of heterogeneity. Heterogeneity was evaluated using Cochran's Q test of
heterogeneity and the I² statistic. Subgroup analyses were conducted to identify potential sources
of heterogeneity using random-effect meta-analysis methods to estimate the average effect across
groupings of studies. Results from the meta-analyses are presented with a forest plot. The Egger
regression asymmetry test for publication bias will be calculated for the outcomes to assess the
possibility of publication bias.
Additionally, EF, JJ and AKY summarized the quality of the body of evidence for each
outcome of interest listed in the questions, in accordance with the GRADE approach. GRADE
evidence profiles, containing the assessment of the quality of the evidence and a summary of
findings across studies for each important or critical outcome were created. The quality of the
body of evidence for each outcome was categorized as high, moderate, low or very low (see
Appendix C for a summary of each intervention study and Appendices D-I for GRADE profiles
for each question). In summary, across the questions we report on 81 studies: question 1 (n=17),
question 2 (n=22), additional analysis 2.1 (n=42), additional analysis 2.2 (81) question 3 (n=10)
and question 4 (n=18), were identified for review.

19 | P a g e
Table 4. Intervention definitions for PICO questions
Intervention Focus Description and Type of Interventions Types of Interventions
Excluded
Interventions that
only implement
responsive
caregiving
Responsive caregiving interventions target the
caregiver-child dyad to promote responsive
caregiver-child interactions and strengthen the
parent-child relationship. These interventions
encourage and support sensitivity and responsiveness
(care that is prompt, consistent, contingent, and
appropriate to the child’s cues, signals, behaviours
and needs) or secure attachment. Interventions that
improve caregivers’ abilities to incorporate the
child’s signals and perspective can be undertaken in
the context of, but not limited to, play and
communication or feeding. They include, but are not
limited to, facilitating the caregiver to be attuned to
and identify the child’s needs and wants, to follow
the child’s lead, help the child to focus, support the
child’s exploration and scaffold development
• Interventions that relate to
caregiving more generally,
but without a primary focus
on promoting positive
caregiver-child interactions.
• Interventions that focus on
infant and young child
feeding or exclusive
breastfeeding, without an
emphasis on responsiveness
between caregiver and
child.
• Interventions that
exclusively target caregivers
(e.g. through provision of
information or education),
rather than targeting the
caregiver-child dyad to
facilitate and encourage
quality caregiver-child
interactions.
• Interventions that focus
exclusively on the child.
Interventions that
only implement early
learning and
development
Interventions that enhance caregivers’ access,
knowledge, attitudes, practices, or skills with respect
to supporting early learning and development for
young children. These interventions may either: a)
directly support caregivers in providing new early
learning opportunities for their children; or b) build
caregiver capacities more generally, providing
information and guidance around healthy
newborn/child development or a range of nurturing
care topics. Interventions may incorporate aspects of
responsive caregiving or behaviour management, but
the overall goals and activities of interventions to
support early learning are broader in scope.
Interventions may be supplemented by messages
about a variety of different caregiving topics but
must include messaging around early learning and
development. Intervention goals that relate to
caregiving, but are not clearly specified, will be also
categorized as general caregiving interventions.
Specific examples of caregiving interventions to
support early learning may include:
• Interventions to promote dialogic caregiver-child
book readings or book sharing.
• Interventions that provide learning and play
materials, such as book gifting or
developmentally-appropriate toys, to increase
opportunities for early learning.
• Interventions that promote general caregiving
• Interventions that focus on
supporting the needs of
caregivers and families, but
do not include a specific
objective to support
caregiving skills for
promoting early learning
and child development.
• Interventions that focus on
reproductive, maternal,
newborn and child health,
but do not include a specific
objective to support
caregiving skills for
promoting child
development.
• Interventions that are
specifically focused on
particular aspects of
caregiving (e.g. only
behaviour management,
only responsive caregiving)

20 | P a g e
Intervention Focus Description and Type of Interventions Types of Interventions
Excluded
competencies to support early learning and
development in young children. These
interventions primarily focus on and support
caregivers themselves, as opposed to enhancing
the caregiver-child relationship. Examples
include caregiver group meetings to share
information and discuss caregiving issues;
home-visiting programmes to improve caregiver
knowledge of ECD and caregiving skills; or
informational sessions providing general advice
on caregiving covering discipline, routines,
feeding, and child health and development.
Interventions that
promote both
responsive
caregiving and the
promotion of early
learning/development
Caregiving interventions that combine
features/components of responsive caregiving and the
promotion of early learning (as defined above).
All caregiving
interventions
categorized above
Recognizing the variation of caregiving intervention
descriptions, this category captures all interventions
together categorized as either responsive caregiving,
early learning promotion, or a combination of
responsive caregiving and the promotion of early
learning.
Caregiving to
support healthy
socioemotional and
behavioural
development
Interventions that support caregivers in promoting
healthy socioemotional and behavioural development
for young children and preventing child behaviour
problems or child maltreatment. This includes
encouraging caregivers to use appropriate and
desirable practices, including sensitive discipline and
limit-setting; reduce inappropriate behaviour
management practices, such as harsh discipline and
coercion; or some combination. Positive parenting
and behaviour management interventions encourage
stable and healthy family relationships and provide
for the physical and emotional safety of the child to
promote positive behavioural development outcomes
for young children. Examples of interventions for
caregiving to support healthy child socioemotional
and behavioral development include:
• Interventions promoting positive behaviour
management techniques, such as establishing
daily routines, praise and appropriate discipline.
• Interventions reducing child maltreatment and
associated factors, such as harsh punishment.
• Interventions that relate to
caregiving more generally,
in which behaviour
management or child
behavioural development is
not the primary focus.
• Interventions intended to
promote early learning
opportunities.
• Interventions where the
primary goal is secure
attachment and supportive,
sensitive and responsive
interactions between
caregivers and children
more broadly.
Combined caregiving
and nutrition
interventions
Interventions that combine a caregiving component
with a nutrition component such as:
• Caregiving component: interventions that
enhance caregivers’ access, knowledge,
attitudes, practices, or skills with respect to
supporting caregiving (responsive caregiving,
caregiving to support early learning, healthy
socioemotional and behavioural development for
• Interventions that contain
only caregiving components
or only nutrition
components.
• Interventions that do not
assess a child development
outcome.
21 | P a g e
Intervention Focus Description and Type of Interventions Types of Interventions
Excluded
young children).
• Nutrition component: may include breast
feeding promotion, agricultural or nutrition
education or provision of a macronutrient or
micronutrient supplement.
• Interventions that promote
nutrition through agriculture
only (e.g. livestock, crops).
• Interventions that promote
water, sanitation and
hygiene only.

22 | P a g e
Evidence and recommendations for responsive caregiving interventions (PICO 1)
Review question
What are the effects of responsive caregiving interventions on ECD in the first 3 years of life?
P – Caregivers and their children in the first 3 years of life
I – Responsive caregiving interventions [alone]
C – Standard of care or comparison groups without responsive caregiving interventions
O – ECD (primary), child attachment, child growth, child health and nutrition, caregiving
knowledge, caregiving practices, caregiver-child interactions, and caregivers’ mental health.
Summary of evidence
The GRADE table and forest plots for the meta-analyses are shown in Appendix D. We
identified 17 responsive caregiving programmes for caregivers and their children during the first
3 years of life. The majority (n=13) of programmes were conducted in HICs, specifically
Australia (Wake et al., 2011), Canada (Barrera et al., 1986), Japan (Cheng et al., 2007), the
Netherlands (Juffer et al., 1997; Van Zeijl et al., 2006; Velderman et al., 2006), the United
Kingdom (McGillion et al., 2017), and the United States (Dozier et al., 2009; Guttentag et al.,
2014; Kochanska et al., 2013; Mendelsohn et al., 2007; Spieker et al., 2012; Weisleder et al.,
2016). The four remaining programmes were conducted in Bangladesh (Frongillo et al., 2017),
Chile (Santelices et al., 2011), Lithuania (Kalinauskiene et al., 2009), and South Africa (Cooper
et al., 2009; Murray et al., 2016).
Three programmes used a cluster randomized control trial (c-RCT) study design, and 14
used a randomized control trial (RCT) design with randomization at the individual or household
level. Studies ranged in publication date from 1986 to 2017. The programmes evaluated between
43 (Barrera et al., 1986) and 4365 individuals (Frongillo et al., 2017). They varied in the
populations that they targeted at enrollment. Three programmes enrolled expectant mothers
(Cooper et al., 2009; Guttentag et al., 2014; Santelices et al., 2010), three targeted caregivers and
their newborn infants during the first 3 months of life (Weisleder et al., 2016; Juffer et al., 1997;
Mendelsohn et al., 2007), five focused on infants during the first year of life (Barrera et al., 1986;
Kalinauskiene et al., 2009; McGillion et al., 2017; Velderman et al., 2006; Cheng et al., 2007),
and six were conducted with a broader age range of children, from birth to 4 years old (Frongillo
et al., 2017; Spieker et al., 2012; Kochanska et al., 2013; Van Zeijl et al., 2006; Wake et al.,
2011; Dozier et al., 2009). All programmes focused on engaging mothers and their children.
The programmes also varied in terms of implementation. Dosage and duration ranged from
a shorter intervention delivered in weekly sessions over 2.5 months (Spieker et al., 2012) to a
longer intervention delivered over three years (Weisleder et al., 2016). Twelve programmes were
delivered through individualized home visits, two were delivered through individualized sessions
at a research center or clinic, one was delivered through caregiver groups, and two used a
combination of both individualized visits and caregiver groups.
23 | P a g e
Early child outcomes:
The effects of responsive caregiving interventions on early child outcomes are categorized and
presented in terms of the following outcome domains: cognitive development, language
development, motor development, socioemotional development, attachment, height-for-age
(HAZ), and weight-for-age (WAZ).
Cognitive development: Three studies assessed programme impact on cognitive development.
All three of these used the Bayley Scale of Infant Development (BSID) (Murray et al., 2016;
Mendelsohn et al., 2007; Barrera et al., 1986). Only Mendelsohn and colleagues (2007)
presented the unadjusted means and standard deviations which could be extracted for this
analysis. Results from this study indicated that the impact on cognitive development was null
(SMD = 0.26, 95% CI: -0.14, 0.66; n = 1). The overall quality of evidence was graded as low.
Language development: Five programmes evaluated intervention impact on language
development. Two evaluations used the Landry Parent-Child Interaction Scales and Preschool
Language Scale (Guttentag et al., 2014; Mendelsohn et al., 2007), one used a measure developed
by the investigators (Frongillo et al., 2017), and two used a version of the MacArthur-Bates
Communicative Development Inventory (McGillion et al., 2017; Wake et al., 2011). The pooled
results showed no significant impacts on language development (SMD = 0.08, 95% CI: -0.07,
0.23; n = 5). The overall quality of evidence was graded as moderate.
Motor development: Two programmes evaluated the impact on motor development. One study
used the BSID (Barrera et al., 1992), and the other used a caregiver-reported motor milestone
checklist previously adapted by the authors (Frongillo et al., 2017). Frongillo and colleagues
(2017), was the only study to present unadjusted means and standard deviations to calculate the
effect size, and the results indicated a significant improvement in motor development (SMD =
0.19, 95% CI: 0.12, 0.26; n = 1). The overall quality of evidence was graded as moderate.
Socioemotional development: Four programmes evaluated the impact on socioemotional
development -- measured using the Infant–Toddler Social and Emotional Assessment (ITSEA)
(Guttentag et al., 2014; Kochanska et al., 2013; and Spieker et al., 2012) and the Behavior
Assessment System for Children (Weisleder et al., 2016). The pooled results showed no
significant effect on improving socioemotional development (SMD = 0.14, 95% CI: -0.03, 0.30;
n = 4). The overall quality of evidence was graded as low.
Behaviour problems: Seven programmes evaluated the impact on behaviour problems measured
using the Child Behavior Checklist (CBCL) (Cheng et al., 2007; Mendelsohn et al., 2007;
Spieker et al., 2014; Van Zeijl et al., 2006; Wake et al., 2011), the ITSEA (Guttentag et al.,
2014), and the BASC (Weisleder et al., 2016). The pooled results showed no significant effect on
reducing behaviour problems (SMD = -0.14, 95% CI: -0.29, 0.002; n = 7). The overall quality of
evidence was graded as low.
Attachment: Seven studies evaluated the impact of responsive caregiving interventions on
attachment outcomes. The measure that was most commonly used to assess attachment outcomes
was the Ainsworth Strange Situation procedure (Santelices et al., 2010; Juffer et al., 1997;

24 | P a g e
Velderman et al., 2006). Pooled results indicated no impacts on attachment outcomes (SMD =
0.13, 95% CI: -0.11, 0.37; n = 3). Three studies which could not be included in the pooled results
similarly reported null effects; one reported significant improvements in attachment outcomes
(Cooper et al., 2009). The overall quality of evidence was graded as low.
HAZ and WAZ: One programme evaluated the impact on HAZ and WAZ (Frongillo et al., 2017).
This study found a positive effect on improving HAZ (SMD = 0.10, 95% CI: 0.03, 0.16; n = 1).
The overall quality of evidence on HAZ was graded as moderate. This study found no significant
effect on improving WAZ (SMD = 0.03, 95% CI: -0.04, 0.10; n = 1). The overall quality of
evidence on WAZ was graded as moderate.
Caregiving outcomes:
The effects of responsive caregiving interventions on caregiving/parenting outcomes are
categorized and presented in terms of the following aspects of parenting: caregiving knowledge,
caregiving practices, caregiver-child interactions, and caregivers’ mental health.
Caregiving knowledge: One programme evaluated the impacts on caregiving knowledge
(Spieker et al., 2012). This study used Raising a Baby (RAB), a measure of caregiver knowledge
of infant and toddler socioemotional needs and developmentally-appropriate expectations. The
results showed no impact on caregiving knowledge (SMD = 0.29, 95% CI: -0.01, 0.58; n=1). The
overall quality of evidence was graded as low.
Caregiving practices: Three programmes evaluated the impacts on caregiving practices. One
evaluation measured caregiving practices using Home Observation for Measurement of the
Environment (HOME) (Barrera et al., 1986), one used a coded video observation measure
(Murray et al., 2016), and one study assessed parenting practices using the StimQ. The pooled
results showed no impacts on caregiving practices (SMD = 0.53, 95% CI: -0.10, 1.17; n = 2).
The overall quality of evidence was graded as low.
Caregiver-child interactions: Eight programmes evaluated impacts on caregiver-child
interactions. Caregiver-child interactions were observed and coded using measures including the
Landry Parent-Child Interaction Scales (Guttentag et al., 2014), the Nursing Child Assessment
Teaching Scale (Spieker et al., 2012), the Ainsworth Scales (Kalinauskiene et al., 2009;
Velderman et al., 2006; Juffer et al., 1997), and the Parent/Caregiver Involvement Scale (Cooper
et al., 2009). The pooled results showed a significant improvement in the quality of caregiver-
child interactions (SMD = 0.34, 95% CI: 0.15, 0.54; n=6). The overall quality of evidence was
graded as low.
Caregiver depressive symptoms: Three programmes evaluated the impacts on caregiver
depressive symptoms. One study used the Edinburgh Postnatal Depression Scale (Cooper et al.,
2009), one used the Beck Depression Inventory (Kalinauskiene et al., 2009), and the third used
the Center for Epidemiological Studies Depression Scale (CES-D) (Mendelsohn et al., 2007).
The pooled results showed that interventions significantly reduced caregiver depressive

25 | P a g e
symptoms (SMD = -0.21, 95% CI: -0.39, -0.04, n = 3). The overall quality of evidence was
graded as moderate.
Subgroup analyses
Subgroup analyses were conducted to examine possible moderating effects by HIC versus LMIC
for outcomes for which it was feasible. Results are presented in Table 5; it is noteworthy that
only two studies from LMICs had quantitative data available for the analysis.
Table 5. Child and caregiver outcomes for interventions that implement responsive caregiving only, by HICs
versus LMICs
Outcome
HICs LMICs
SMD 95% CI N SMD 95% CI N
Child outcomes
Language development 0.00 -0.15, 0.15 4 0.23 0.16, 0.30 1
Attachment 0.16 -0.10, 0.43 2 0.00 -0.53, 0.53 1
Caregiver outcomes
Caregiving practices 0.21 -0.19, 0.61 1 0.86 0.45, 1.28 1
Caregiver-child interactions 0.32 0.07, 0.58 4 0.46 -0.06, 1.00 2
Caregiver depressive symptoms -0.17 -0.56, 0.23 1 -0.22 -0.42, -0.03 2
Considerations for adverse effects and costs
There were no reported risks of adverse outcomes with responsive caregiving
interventions for ECD or parenting outcomes. None of the studies presented data on costs.
In conclusion, the global evidence suggests that responsive caregiving interventions during the
first 3 years of life are effective in improving early child motor development and caregiving
outcomes, specifically caregiver and child interactions and maternal depressive symptoms. More
studies are required from LMICs.
26 | P a g e
Evidence and recommendations for caregiving interventions that promote early
learning (PICO 2)
Review question
What is the effectiveness of caregiving interventions that promote early learning on ECD in the
first 3 years of life?
P – Caregivers and their children in the first 3 years of life
I – Interventions that promote early learning [alone]
C – Standard of care or comparison groups without caregiving interventions to support early
learning
O – ECD (primary), child attachment, child growth, child health and nutrition, caregiving
knowledge, caregiving practices, caregiver-child interactions, and caregivers’ mental health
Summary of evidence
GRADE table and forest plots for the meta-analyses are shown in Appendix E. The
evidence for caregiving interventions to promote early learning is derived from 22 RCTs. Four
trials were conducted in LMICs, including China, India, Uganda, and Zambia. Eighteen were
conducted in HICs, including Australia, Bermuda, France, Hong Kong, New Zealand, , the
United States and the United Kingdom (see Appendix C for full list of PICO 2 programmes and
characteristics). The majority were RCTs randomized at the individual level (n = 17), and five
studies were c-RCTs. Studies were published between the years 1988 and 2017. The analytic
sample sizes at endline ranged from 48 (Wasik et al., 1990) to 2557 participants (Goodson et al.,
2000).
Seven of the trials targeted women beginning during pregnancy (Goodson et al., 2000;
Guedeney et al., 2013; Jacobs et al., 2016; Love et al., 2005; Norr et al, 2003; Robling et al.,
2016; Walkup et al., 2009); four interventions targeted women immediately following childbirth
(Caughy et al., 2004; Schwarz et al., 2012; Brooks-Gunn et al., 1992; Nair et al., 2009); three
interventions enrolled women and children within the first 3 months of life (Fergusson et al.,
2005; Sawyer et al., 2017; Wasik et al., 1990); four targeted children within the first year of life
(Jin et al., 2007; Wagner et al., 2002; Rockers et al., 2016; Muhoozi et al., 2017); and four
enrolled children within their first 36 months (Hutchings et al., 2016; Leung et al., 2017b; Scarr
& McCartney, 1988; Heubner et al., 2000). Most programmes targeted the mother or other
female primary caregiver.
In terms of delivery, ten of the programmes were delivered to families individually
through home visitations, five were group-based, and seven included a mix of individual and
group-based delivery strategies. Programme duration varied extensively, ranging from 1.5
(Heubner et al., 2000) to 60 months (Goodson et al., 2000).
27 | P a g e
Early child outcomes:
The effects of caregiving interventions to support early learning on early child outcomes
are categorized and presented in terms of the following outcome domains: cognitive
development, language development, motor development, socioemotional development, child
behaviour problems, attachment, HAZ and WAZ.
Cognitive development: Thirteen studies assessed programme impact on cognitive development.
Four of these used the BSID. The remaining ones used a variety of measures, including:
Wechsler Preschool and Primary Scale of Intelligence (Schwarz et al., 2012), Kaufman
Assessment Battery for Children (Goodson et al., 2000), INTERGROWTH-21st NDA tool
(Rockers et al., 2016), Preschool Developmental Assessment Scale (Leung et al., 2017b), an
author-created measure of standardized checklist items (Robling et al., 2016), McCarthy Scales
of Children’s Abilities (Wasik et al., 1990), Schedule of Growing Skills II (SGS-II) (Hutchings
et al., 2016), Stanford-Binet Test of Intelligence (Scarr & McCartney, 1988), and Developmental
Profile II (DPII) (Wagner et al., 2002). The pooled results indicated positive impacts of
caregiving interventions on cognitive development (SMD = 0.20, 95% CI: 0.01, 0.39; n = 8). The
overall quality of evidence was graded as low.
Language development: Impacts on language development were assessed in nine studies. Three
used the Peabody Picture Vocabulary Test-Revised (Goodson et al., 2000; Heubner, 2000; Love
et al., 2005). Other measures included the Gesell Development Schedules (Jin et al., 2007), the
Stanford-Binet Test of Intelligence (Brooks-Gunn et al., 1992), the BSID (Muhoozi et al., 2017),
the Wechsler Preschool and Primary Scale of Intelligence (Schwarz et al., 2012), an Early
Language Milestone measure (Robling et al., 2016), and the Developmental Profile II (Wagner et
al., 2000). Pooled results indicated that interventions had no significant impacts on language
development (SMD = 0.07, 95% CI: -0.11, 0.24; n = 6). The overall quality of the evidence was
graded as low.
Motor development: Seven studies evaluated programme effects on motor development. Three
used the BSID (Muhoozi et al., 2017; Norr et al., 2003; Nair et al., 2009). Two studies used a
caregiver-reported measure (Wagner et al., 2002; Rockers et al., 2016), and two used direct
observation measures (Brooks-Gunn et al., 1992; Jin et al., 2007). The pooled results show
significant positive effects on motor development (SMD = 0.32, 95% CI: 0.12, 0.52; n = 5). The
overall quality of the evidence was graded as low.
Socioemotional development: Nine studies assessed programme impacts on socioemotional
development -- measured using the Ages and Stages Questionnaire (Muhoozi et al., 2017;
Pontoppidan et al., 2016; and Sawyer et al., 2017), the Adaptive Social Behavior Inventory
(Wagner et al., 2002), ITSEA (Barlow et al., 2007; Walkup et al., 2009), the Strengths and
Difficulties Questionnaire (SDQ) (Leung et al., 2017b), the Gesell Development Schedules (Jin
et al., 2007), and a measure from the NICHD Study of Early Child Care (Love et al., 2005).
Pooled results showed positive effects on socioemotional development outcomes (SMD = 0.28,
95% CI: 0.09, 0.48, n = 3). However, there were non-significant differences in five out of the six
other studies that could not be meta-analysed. The overall quality of the evidence was graded as
very low.
28 | P a g e
Behaviour problems: Eight programmes evaluated the impact on behaviour problems - measured
using the ITSEA (Fergusson et al., 2005; Jacobs et al., 2016; Walkup et al., 2009), the CBCL
(Caughy et al., 2004; Goodson et al., 2000; Love et al., 2005), the SDQ (Leung et al., 2017b),
and the PSI-DC (Hutchings et al., 2016). The pooled results showed no significant effect on
reducing behaviour problems (SMD = -0.25, 95% CI: -0.54, 0.04, n = 3). Of the five studies that
could not be meta-analysed, the evidence was mixed: three studies found reductions in children’s
behaviour problems, and two found no significant differences. The overall quality of evidence
was graded as very low.
Attachment outcomes: Two studies assessed programme impacts on attachment outcomes
(Caughy et al., 2004; Guedeney et al., 2013). Only one study (Guedeney et al., 2013) contributed
to the effect size estimate (measured reductions in social withdrawal using the Alarm Distress
Baby Scale; direction of effect size was reversed for analysis). Results indicated significant
positive impacts on attachment outcomes (SMD = 0.30, 95% CI: 0.09, 0.51; n = 1). Caughy and
colleagues (2004), similarly reported significant improvements in secure attachment
relationships for intervention group children (as measured by the Attachment Q-Set). The overall
quality of evidence was graded as low.
HAZ and WAZ: Two studies evaluated impacts on HAZ and WAZ (Muhoozi et al., 2017;
Rockers et al., 2016). The pooled results showed no effects on child HAZ outcomes (SMD = -
0.02, 95% CI: -0.29, 0.24, n = 2). The overall quality of the evidence was graded as moderate.
The pooled results showed no effects on child WAZ outcomes (SMD = 0.05, 95% CI: -0.10,
0.19, n = 2). The overall quality of the evidence was graded as moderate.
Caregiving outcomes
The effects of caregiving interventions to support early learning on caregiving outcomes are
categorized and presented in terms of the following aspects of parenting: caregiving knowledge,
caregiving practices, caregiver-child interactions, and caregivers’ mental health.
Caregiving knowledge: Three studies assessed intervention impacts on caregiving knowledge.
Two studies used questionnaires created by the authors for the purposes of the study (Jin et al.,
2007; Walkup et al., 2009), and one used the Knowledge of Infant Development Inventory
(Wagner et al., 2002). Two of the evaluations reported significant improvements in caregiving
knowledge (Jin et al., 2007; Walkup et al., 2009), while one study found no programme effects
(Wagner et al., 2002). Unadjusted means and standard deviations were not presented in the
papers, and therefore it was not possible to calculate a pooled estimate. The overall quality of the
evidence was graded as low.
Caregiving practices: Programme impacts on caregiving practices were assessed in eight studies.
Only one of the trials found significant improvements in caregiving practices (Love et al., 2005),
while the remaining studies reported null effects (Wasik et al., 1990; Walkup et al., 2009;
Wagner et al., 2002; Norr et al., 2003; Hutchings et al., 2016; Goodson et al., 2000; Caughy et
al., 2004). All of the studies used the HOME. Pooled results indicated no programme impacts on

29 | P a g e
caregiving practices (SMD = 0.05, 95% CI: -0.04, 0.13; n = 2). The overall quality of evidence
was graded as low.
Caregiver-child interactions: Five studies evaluated intervention impacts on caregiver-child
interactions. The majority of studies measured interactions using the Nursing Child Assessment
Satellite Training (NCAST) measure (Caughy et al., 2004; Goodson et al., 2000; Wagner et al.,
2002). Three studies reported positive impacts on caregiver-child interactions (Caughy et al.,
2004; Love et al., 2005; Hutchings et al., 2016), while two studies reported no impacts (Goodson
et al., 2000; Wagner et al., 2002). It was not possible to calculate a pooled estimate as studies did
not present the unadjusted means and standard deviations. Overall quality of evidence was rated
as low.
Caregiver depressive symptoms: Four studies assessed programme impacts on caregiver
depressive symptoms. Two studies used the Beck Depression Inventory (Schwarz et al., 2012;
Hutchings et al., 2016); one study used the WHO Self-Reporting Questionnaire (SRQ) z-score
(Rockers et al., 2016); and the fourth used the CES-D (Walkup et al., 2009). The pooled results
showed no effect on caregiver depressive symptoms (SMD = 0.07, 95% CI: -0.08, 0.22, n = 2).
The overall quality of the evidence was graded as moderate.
Subgroup analyses
Subgroup analyses were conducted to examine possible moderating effects by HICs
versus LMICs. Results are presented in Table 6. The impact on ECD and caregiver mental
health appears greater in LMICs; however, more studies measuring this outcome in both HICs
and LMICs are required, as currently we draw findings from only one study in each context.
Table 6. Child and caregiver outcomes for interventions that promote early learning and development, by
HICs versus LMICs
Outcome HICs LMICs
SMD 95% CI N SMD 95% CI N
Child outcomes
Cognitive development 0.08 -0.02, 0.18 5 0.32 -0.11, 0.75 3
Language development 0.03 -0.09, 0.15 4 0.30 -0.67, 1.27 2
Motor development 0.08 -0.10, 0.26 1 0.39 0.17, 0.60 4
Caregiving outcomes
Caregiver depressive symptoms 0.13 -0.11, 0.37 1 0.03 -0.16, 0.22 1
30 | P a g e
Considerations for adverse effects and costs:
There were no indications of adverse effects caused by caregiving interventions to
support development and early learning. Costing data for these interventions were not readily
available in the literature.
In conclusion, the intervention studies on caregiving to support early learning suggest
these are promising interventions with significant (modest) effects found on child cognition,
motor development and attachment. Evidence for effectiveness on caregiving outcomes was not
observed in the pooled data. However, more studies from LMICs and more data on caregiver-
level outcomes are needed.
31 | P a g e
Evidence and recommendations for caregiving interventions that combine
responsive caregiving and promotion of early learning: additional analysis 2.1
Review Question
What is the effectiveness of caregiving interventions that combine both responsive caregiving
and the promotion of early learning on ECD in the first 3 years of life?
P – Caregivers and their children in the first 3 years of life
I – Caregiving interventions that combine responsive caregiving and the promotion of early
learning
C – Standard of care or comparison groups without caregiving interventions to support
responsive caregiving and the promotion of early learning
O – ECD (primary), child attachment, child growth, child health and nutrition, caregiving
knowledge, caregiving practices, caregiver-child interactions, and caregivers’ mental health
Summary of evidence
The GRADE table and forest plots for the meta-analyses are shown in Appendix F. We
identified 42 caregiving interventions that had components of both responsive caregiving and the
promotion of early learning for caregivers and their children during the first 3 years of life.
Approximately half (n=22 or 52.4%) of these programmes were conducted in LMICs. A total of
14 programmes used a c-RCT study design, and 28 programmes used a RCT design with
randomization at the individual level. Studies ranged in publication date from 1974 (Johnson et
al., 1974) to 2017 (Fernald et al., 2017; Helmizar et al., 2017; Leung et al., 2017a). The
programmes evaluated between 32 (Johnson et al., 1974; Pontoppidan et al., 2016; Whitt &
Casey, 1982) and 1411 individuals (Yousafzai et al., 2014). These programmes varied in targeted
population at enrollment. Seven programmes (16.7%) focused on expectant mothers beginning
during pregnancy, 13 rogrammes (31.0%) targeted caregivers and their newborn infants during
the first 3 months of life, six (14.3%) focused on infants during the first year of life, and the
remaining 16 (38.1%) were conducted either after the first year or among a broader age range of
children from birth to 4 years old. Nearly all programmes (n=38 or 90%) targeted mothers and
their children. Four notable programmes (10%) engaged both mothers and fathers (Johnson et al.,
1974; Kaaresen et al., 2008; Kyno et al., 2012; Singla et al., 2015).
The programmes also varied in terms of implementation. Dosage and duration ranged from
as short as fewer than 10 sessions over two months (Aboud & Ahkter, 2011; Vally et al., 2015;
Murray et al., 2016) to as long as weekly (Kaminski et al., 2013) or biweekly sessions
(Wallander et al., 2014) over three years. A total of 25 (60%) were individualized programmes,
six (14%) were delivered through caregiver groups, and 11 (26%) used a combination of both
home visits and caregiver groups.
32 | P a g e
Early child outcomes:
Cognitive development: Thirty-six studies assessed programme impact on cognitive
development. Twenty-one of these used the BSID. Six studies used the Griffith’s scales of
Mental Development (Waber et al., 1981; Walker et al., 2004; Powell & Grantham-McGregor,
1989; Powell et al., 2004; Gardner et al., 2005; Grantham-McGregor et al., 1991). The remaining
studies utilized a variety of measures, including the Kaufman Assessment Battery for Children
(Drotar et al., 2009), Preschool Developmental Assessment Scale (PDAS) (Leung et al., 2017a),
McCarthy Scales of Children’s abilities (Fernald et al., 2017), a nationally validated author-
created checklist measure (Hartinger et al., 2017), Stanford-Binet Test of Intelligence (Johnson
et al., 1974; Madden et al., 1984), Cattell Scales (Olds et al., 1986), Bracken Basic Concept
Scale (Cronan et al., 1996), and Mullen Scale of Early Learning (Kyno et al., 2012). The pooled
results showed positive impacts of caregiving interventions on cognitive development (SMD =
0.45, 95% CI: 0.25, 0.65; n = 20). The overall quality of evidence was graded as low.
Language development: Seventeen studies assessed the effects on language development. Six
used the BSID. Four used the Griffiths Mental Development Scales (Chang et al., 2015; Gardner
et al., 2005; Grantham-McGregor et al., 1991; Powell et al., 2004). The MacArthur-Bates
Communicative Development Inventory was used in three studies (Vally et al., 2015; Goldfeld et
al., 2011; Cronan et al., 1996). Remaining studies used other measures of direct observation. The
pooled results indicated positive impacts on language outcomes (SMD = 0.38, 95% CI: 0.16,
0.60; n = 14). The overall quality of evidence was graded as low.
Motor development: Eighteen studies assessed programme impacts on motor development.
Twelve measured motor development using the BSID (Attanasio et al., 2014; Field et al., 1982;
Hamadani et al., 2006; Heinicke et al., 1999; Helmizar et al., 2017; Kaaresen et al., 2008; Lozoff
et al., 2010; Nahar et al., 2012a; Tofail et al., 2013; Vazir et al., 2013; Wallander et al., 2014;
Yousafzai et al., 2014). Five studies used the Griffith Mental Development Scale (Chang et al.,
2015; Gardner et al., 2005; Grantham-McGregor et al., 1991; Grantham-McGregor et al., 1989;
Powell et al., 2004), and one study used the Mullen Scales of Early Learning (Kyno et al., 2012).
Pooled results indicated significant positive effects on motor development outcomes (SMD =
0.25, 95% CI: 0.09, 0.40; n = 13). The overall quality of evidence was rated as low.
Socioemotional development: Four studies assessed programme impacts on socioemotional
development -- measured using the ASQ (Kyno et al., 2012), the SDQ (Kaminski et al., 2013),
the Social Skills Rating System (Drotar et al., 2008), and the BSID (Yousafzai et al., 2014).
Pooled results showed null effects on socioemotional development outcomes (SMD= 0.06, 95%
CI: -0.18, 0.28, n=2). The studies that could not be meta-analysed similarly found no statistically
significant differences for socioemotional development. The overall quality of the evidence was
graded as moderate.
Behaviour problems: Seven programmes evaluated the impact on behaviour problems measured
using the CBCL (Constantino et al., 2001; Kaaresen et al., 2008; Kitzman et al., 1997; Kyno et
al., 2012; Olds et al., 2002), the Devereux Early Childhood Assessment (Kaminski et al., 2013),
and the Eyberg Child Behavior Inventory (Leung et al., 2017a). The pooled results showed no
significant effect on reducing behaviour problems (SMD = -0.18, 95% CI: -0.40, 0.04, n = 2). Of

33 | P a g e
the five studies that could not be meta-analysed, four found no significant differences. The
overall quality of evidence was graded as low.
Attachment outcomes: Two studies evaluated programme impacts on attachment outcomes.
Measures included the Ainsworth Strange Situation procedure (Heinicke et al., 1999) and the
Attachment Q-Set (Roggman et al., 2009). Both studies reported significant positive impacts on
attachment outcomes, although a pooled effect size could not be calculated. Overall quality of
evidence was graded as moderate.
HAZ and WAZ: Eight studies evaluated impacts on HAZ and WAZ. Two other studies assessed
height and weight but did not present a z-score; therefore, they were excluded from the meta-
analysis (Attanasio et al., 2014; Nair et al., 2009). The pooled results showed no effects on child
HAZ outcomes (SMD = -0.04, 95% CI: -0.15, 0.07, n = 8). The overall quality of the evidence
was graded as moderate. The pooled results showed no effects on child WAZ outcomes (SMD =
0.02, 95% CI: -0.07, 0.11, n = 6). The overall quality of the evidence was graded as high.
Caregiving outcomes:
Caregiving knowledge: Seven studies examined programme impact on caregiving knowledge.
Four studies used caregiver self-report questionnaires developed by the authors (Hamadani et al.,
2006; Vazir et al., 2013; Powell et al., 2004; Singla et al., 2015). Pooled results indicated that
programmes had a significant positive impact on caregiving knowledge (SMD = 0.73, 95% CI:
0.57, 0.89; n = 6). The overall quality of evidence was rated as low.
Caregiving Practices: Eighteen studies assessed intervention effects on caregiving practices. The
majority of studies used the HOME (Aboud & Akhter, 2011; Aboud et al., 2013; Barlow et al.,
2007; Chang et al., 2015; Heinicke et al., 1999; Helmizar et al., 2017; Johnson et al., 1974;
Kitzman et al., 1997; Nahar et al., 2012b; Singla et al., 2015; Walker et al., 2004; Yousafzai et
al., 2015; Olds et al., 1986; Field et al., 1982). Two studies used the Family Care Indicators
(Attanasio et al., 2014; Tofail et al., 2013). Pooled results indicated that interventions had a
significant positive effect on caregiving practices (SDM = 0.48, 95% CI: 0.20, 0.76; n = 10). The
overall quality of evidence was rated as low.
Caregiver-child interactions: Programme impacts on caregiver-child interactions were assessed
in 12 studies. Measures to assess the quality of mother-child interactions included the NCAST
(Kitzman et al., 1997) and the Observation of Mother and Child Interaction (OMCI) (Yousafzai
et al., 2015). Other measures of caregiver-child interactions included assessments of responsive
talk (Aboud & Akhter, 2011) and reciprocity during book-sharing activities (Murray et al.,
2016). The pooled results indicated that interventions had a significant positive effect on
caregiver-child interactions (SMD = 0.74, 95% CI: 0.39, 1.10; n = 5). Overall quality of evidence
was rated as moderate.
Caregiver depressive symptoms: Nine studies assessed programme impacts on caregiver
depressive symptoms. Six used the CES-D (Chang et al., 2015; Aboud et al., 2013; Singla et al.,
2015; Nahar et al., 2015; Attanasio et al., 2014; Baker-Henningham et al., 2005). Of the
remaining studies, one used the SRQ (Yousafzai et al., 2015), one used the Major Depression
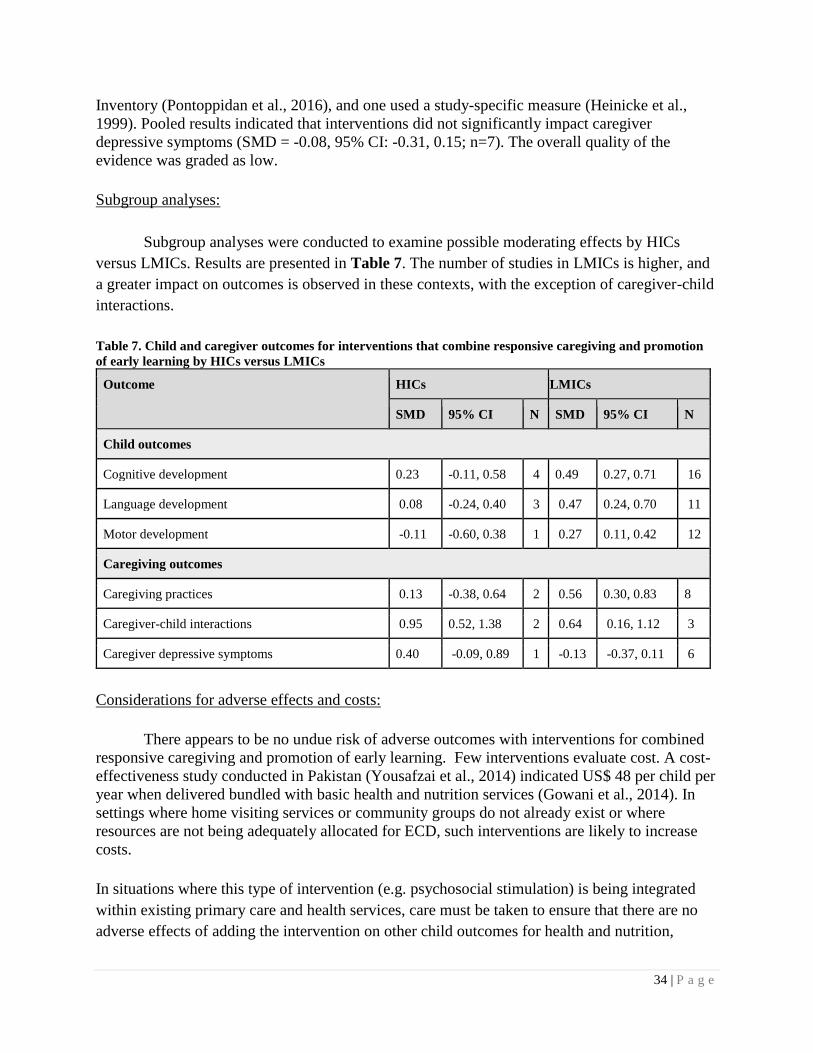
34 | P a g e
Inventory (Pontoppidan et al., 2016), and one used a study-specific measure (Heinicke et al.,
1999). Pooled results indicated that interventions did not significantly impact caregiver
depressive symptoms (SMD = -0.08, 95% CI: -0.31, 0.15; n=7). The overall quality of the
evidence was graded as low.
Subgroup analyses:
Subgroup analyses were conducted to examine possible moderating effects by HICs
versus LMICs. Results are presented in Table 7. The number of studies in LMICs is higher, and
a greater impact on outcomes is observed in these contexts, with the exception of caregiver-child
interactions.
Table 7. Child and caregiver outcomes for interventions that combine responsive caregiving and promotion
of early learning by HICs versus LMICs
Outcome HICs LMICs
SMD 95% CI N SMD 95% CI N
Child outcomes
Cognitive development 0.23 -0.11, 0.58 4 0.49 0.27, 0.71 16
Language development 0.08 -0.24, 0.40 3 0.47 0.24, 0.70 11
Motor development -0.11 -0.60, 0.38 1 0.27 0.11, 0.42 12
Caregiving outcomes
Caregiving practices 0.13 -0.38, 0.64 2 0.56 0.30, 0.83 8
Caregiver-child interactions 0.95 0.52, 1.38 2 0.64 0.16, 1.12 3
Caregiver depressive symptoms 0.40 -0.09, 0.89 1 -0.13 -0.37, 0.11 6
Considerations for adverse effects and costs:
There appears to be no undue risk of adverse outcomes with interventions for combined
responsive caregiving and promotion of early learning. Few interventions evaluate cost. A cost-
effectiveness study conducted in Pakistan (Yousafzai et al., 2014) indicated US$ 48 per child per
year when delivered bundled with basic health and nutrition services (Gowani et al., 2014). In
settings where home visiting services or community groups do not already exist or where
resources are not being adequately allocated for ECD, such interventions are likely to increase
costs.
In situations where this type of intervention (e.g. psychosocial stimulation) is being integrated
within existing primary care and health services, care must be taken to ensure that there are no
adverse effects of adding the intervention on other child outcomes for health and nutrition,
35 | P a g e
particularly in low-resource contexts where health service capacities may be limited. A study
from the Caribbean explored these issues and found no negative impacts of integrating a
psychosocial stimulation intervention within existing health services on child nutrition or
immunization (Chang et al., 2015).
In conclusion, interventions that combine both features of caregiving (i.e., responsive
care and support for early learning) had significant positive effects for cognitive, language and
motor development, as well as caregiving knowledge, caregiver practices, and caregiver-child
interactions. Studies in 2.1 had global representation from both HICs and LMICs.
36 | P a g e
Evidence and recommendations for all caregiving interventions that deliver
responsive caregiving, promotion of early learning, or combined responsive
caregiving and promotion of early learning: additional analysis 2.2
Review question
What is the effectiveness of any caregiving interventions (responsive caregiving, promotion of
early learning, or combined responsive caregiving and the promotion of early learning) on ECD
in the first 3 years of life.
P – Caregivers and their children in the first 3 years of life
I – Any caregiving interventions (responsive caregiving, promotion of early learning or
combined responsive caregiving and the promotion of early learning)
C – Standard of care or comparison groups without caregiving interventions
O – ECD (primary), child attachment, child growth, child health and nutrition, caregiving
knowledge, caregiving practices, caregiver-child interactions, and caregivers’ mental health
Summary of evidence
The GRADE table and forest plots for the meta-analyses are shown in Appendix G. Here
we explore the effectiveness of caregiving interventions included in PICO questions 1, 2 and and
2.1. We describe the effectiveness of any caregiving interventions (responsive caregiving,
promotion of early learning, or combined responsive caregiving and the promotion of early
learning) on ECD in the first 3 years of life.
Early child outcomes:
Cognitive development: Fifty-two studies assessed programme impact on cognitive development.
Over half of these used the BSID. Remaining studies used a variety of measures, the majority of
which were direct observation. The pooled results showed positive impacts of caregiving
interventions on cognitive development (SMD = 0.37, 95% CI: 0.22, 0.52, n = 29). The overall
quality of evidence was graded as low.
Language development: Overall, 31 studies evaluated intervention effects on language
development. The pooled results indicated positive effects of caregiving interventions on
language outcomes (SMD = 0.24, 95% CI: 0.11, 0.36; n = 25). The overall quality of evidence
was graded as low.
37 | P a g e
Motor development: Twenty-seven studies assessed programme impacts on child motor
development outcomes. Pooled results indicated significant positive effects (SMD = 0.27, 95%
CI: 0.17, 0.37; n = 19). The overall quality of evidence was graded as moderate.
Socioemotional development: Seventeen studies assessed programme impacts on socioemotional
development. Pooled results indicated significant positive effects on socioemotional
development outcomes (SMD = 0.15, 95% CI: 0.04, 0.27, n = 9). The overall quality of the
evidence was graded as low.
Behavioural development: Twenty-two studies assessed programme impacts on behavioural
problems. Pooled results indicated significant reductions in behavioural problems (SMD = -0.17,
95% CI: -0.28, -0.06, n = 12). However, the majority of studies that could not be meta-analysed
found non-significant differences in behavioural problems. The overall quality of the evidence
was graded as low.
Attachment outcomes: Eleven studies evaluated the effects of caregiving interventions on
attachment outcomes. Pooled results indicated significant positive impacts of caregiving
interventions on attachment outcomes (SMD = 0.23, 95% CI: 0.07, 0.38; n = 4). The overall
quality of evidence was graded as low.
HAZ and WAZ: Eleven studies evaluated impacts on HAZ and WAZ. The pooled results showed
no effects on child HAZ outcomes (SMD = -0.02, 95% CI: -0.10, 0.07, n = 11). The overall
quality of the evidence was graded as high. The pooled results showed no effects on child WAZ
outcomes (SMD = 0.03, 95% CI: -0.02, 0.08, n = 9). The overall quality of the evidence was
graded as high.
Child health outcomes: Four programmes evaluated the impact on child sickness, as reported by
the child’s primary caregiver. Three studies found no effects on reducing sickness (Aboud et al.,
2013; Menon et al., 2016; Singla et al., 2015), whereas another study found reductions in
diarrhoea and acute respiratory illness (Yousafzai et al., 2014).
Caregiving outcomes:
Caregiving knowledge: Eleven studies measured the impact of interventions on caregiving
knowledge. Over half used a study-specific questionnaire developed by the authors. Pooled
results indicated that interventions had a significant positive effect on caregiving knowledge
(SMD = 0.68, 95% CI: 0.51, 0.85; n = 7). The overall quality of the evidence was graded as low.
Caregiving practices: Overall, 29 studies assessed programme impact on caregiving practices.
The majority of these (n = 23) measured caregiving practices using the HOME. Pooled results
indicated that interventions significantly improved caregiving practices (SMD = 0.44, 95% CI:
0.21, 0.67; n = 14). The overall quality of evidence was graded as low.
Caregiver-child interactions: Across all caregiving interventions, 25 studies assessed the effects
on caregiver-child interactions. All of these used a measure for coding video- or live-
observations of the mother-child dyad. The pooled results for intervention effects on interactions

38 | P a g e
indicated that programmes significantly improved outcomes for caregiver-child interactions
(SMD = 0.54, 95% CI: 0.30, 0.78; n = 11). The overall quality of the evidence was rated as low.
Caregiver depressive symptoms: Sixteen evaluations assessed programme impacts on caregiver
depressive symptoms. The majority of studies used either the CES-D or the Beck Depression
Inventory. The pooled results indicated that interventions did not significantly reduce caregiver
depressive symptoms (SMD = -0.07, 95% CI: -0.22, 0.07; n = 12). The overall quality of
evidence was rated as low.
Subgroup analyses:
Subgroup analyses were conducted to examine possible moderating effects by HICs
versus LMICs. Results are presented in Table 8. In LMICs a greater impact on outcomes is
observed, with the exception of attachment.
Table 8. Child and caregiver outcomes across all included caregiving interventions by HICs versus LMICs
Outcomes HICs LMICs
SMD 95% CI N SMD 95% CI N
Child outcomes
Cognitive development 0.12 0.01, 0.23 10 0.46 0.26, 0.65 19
Language development 0.02 -0.07, 0.11 11 0.42 0.23. 0.61 14
Motor development 0.06 -0.11, 0.23 2 0.29 0.19, 0.40 17
Attachment 0.25 0.08, 0.41 3 0.00 -0.53, 0.53 1
Caregiving outcomes
Caregiver knowledge 0.29 -0.01, 0.58 1 0.73 0.57, 0.89 6
Caregiving practices 0.05 -0.07, 0.17 5 0.59 0.35, 0.84 9
Child-caregiver practices 0.48 0.20, 0.76 6 0.58 0.20, 0.95 5
Caregiver depressive symptoms 0.10 -0.16, 0.37 3 -0.12 -0.29, 0.05 9
In conclusion, benefits of caregiving interventions are observed on multiple outcomes of
ECD (with significant impacts on cognition, language, motor and behavioural development, and
attachment) as well as caregiving knowledge and practices, and caregiver and child interactions.
39 | P a g e
Evidence and recommendations for caregiving interventions to support healthy
child socioemotional and behavioural development (PICO 3)
Review question
What are the effects of caregiving interventions to support child socioemotional and behavioural
development on ECD?
P – Caregivers and their children in the first 3 years of life
I – Caregiving interventions that support socioemotional and behavioural development
C – Standard of care or comparison groups without caregiving interventions to support healthy
child socioemotional and behavioural development
O – ECD (primary), child growth, child health and nutrition, caregiving knowledge, caregiving
practices, caregiver-child interactions, and caregivers’ mental health.
Summary of Evidence6
The GRADE table and forest plots for the meta-analyses are shown in Appendix H. We
identified 10 caregiving studies to support healthy socioemotional development and behaviour
for children during the first 3 years of life. The evidence for the impact of caregiving
interventions to support socioemotional and behavioural development for children under 3 years
of age is derived from 10 RCTs representing 11 interventions. All 10 studies were conducted in
HICs, including Australia (n = 2), the Netherlands (n = 1), New Zealand (n = 1) and the United
States (n = 6). The majority were two-arm RCTs randomized at the individual level (n = 8), with
one two-armed c-RCT (Hiscock et al., 2008) and one three-armed c-RCT (Hiscock et al., 2018).
Studies were published between the years 2005 and 2018. The analytic sample sizes at endline
ranged from 237 (Van Zeijl et al., 2006) to 1353 (Hiscock et al., 2018). The median sample size
across all studies was 388 individuals.
Programmes varied in terms of the targeted caregivers. Most interventions (n = 7)
primarily targeted mothers or the primary caregiver of the child (Caldera et al. 2007; Gross et al.,
2009; Breitenstein et al., 2012; Fergusson et al., 2005; Hiscock et al., 2008; Hiscock et al., 2018;
Dishion et al., 2008). One programme restricted enrollment to children from dual-caregiver
families (i.e., biological mothers and father-figures) (Van Ziejl et al., 2006). Two programmes
specifically targeted adolescent and young mothers (Barlow et al., 2015; Jacobs et al. 2016).
Programmes also differed in the age of the child targeted for enrollment. Three
programmes targeted pregnant mothers, but the window for enrollment varied, through 32-weeks
gestation (Barlow et al., 2015), birth (Caldera et al., 2007), and the child’s first year of life
6 The terms ‘programmes’ and ‘studies’ are used interchangeably. The term ‘programme’ does not refer to routine service delivery in this report.
40 | P a g e
(Jacobs et al., 2016). One programme targeted children aged 0-3 months (Fergusson et al., 2005);
one enrolled children aged 1-3 years (Van Ziejl et al., 2006); one enrolled children aged 2-3
years (Dishion et al., 2008); two targeted caregivers with children aged 2-4 years (Gross et al.,
2009; Breitenstein et al., 2012); and three enrolled infants at their 8-month well-child visits
(Hiscock et al., 2008; Hiscock et al., 2018).
The majority of programmes were home visitation (n = 6) delivered to individual
families. Two studies evaluated group caregiver-training programmes affiliated with day-care
centres (Gross et al., 2009; Breitenstein et al., 2012). Two programmes contained both group and
individualized components, one of which was clinic-based only while the other also incorporated
in-home visitation (Hiscock et al., 2008; Hiscock et al., 2018).
There was a wide range in programme duration and dosage, from two-hour visits over
seven months (Hiscock et al., 2008) to home visiting interventions with up to 40 visits through
the child’s third birthday (Barlow et al., 2015). Median programme duration was 19.35 months.
Early child outcomes:
The effects of interventions to support healthy socioemotional development and
behaviour on early child outcomes are categorized and presented in terms of the following
outcome domains: cognitive development, motor development, socioemotional development,
behavioural problems, and any other child nutrition or health outcome. None of the studies
assessed outcomes for language development or growth outcomes, and therefore these child
outcomes have also been excluded from the meta-analysis.
Cognitive development: Only one study assessed cognitive development. Cognition was
measured using the Mental Development Index score from the BSID. Mean scores for
intervention group children were significantly higher compared to children in the control group
(p<0.05) (Caldera et al., 2007). Unadjusted means and standard deviations were not presented so
the unadjusted effect size could not be calculated, although the authors indicate an adjusted
effect size of 0.29. The overall quality of evidence was graded as very low.
Motor development: One study assessed motor development (Caldera et al., 2007). Motor
development was measured using the Psychomotor Development Index score from the BSID.
Unadjusted effect sizes could not be calculated, but authors presented an adjusted effect size of
0.19, although the difference between groups was not statistically significant (p = 0.16). The
overall quality of evidence was graded as very low.
Socioemotional development: Barlow and colleagues (2015) was the only study to assess
socioemotional development. This was measured using the parental-reported Competence score
from the ITSEA. No significant effects were found (adjusted mean difference in intervention
41 | P a g e
group versus control scores: 0.04; p = 0.09; adjusted ES = 0.14). The overall quality of the
evidence was graded as very low.
Child behaviour problems: All 10 studies evaluated child behaviour problems. The pooled
results showed no effect on reductions in child behaviour problems (SMD = -0.02, 95% CI: -
0.07, 0.02, n = 5). Five studies used the parent-reported CBCL; two studies used the parent-
reported ITSEA (Barlow et al., 2015, Fergusson et al., 2005); one study used the Brief-ITSEA
(Jacobs et al., 2016); and two used the parent-reported Eyberg Child Behavior Inventory,
teacher-reported Caregiver-Teacher Report Form, and direct observation of child behaviour
problems assessed from videotaped play sessions (Gross et al., 2009; Breitenstein et al., 2012).
The overall quality of the evidence was graded as moderate.
Child health: Two studies examined programme impacts on indicators for child health and
medical outcomes. Outcomes were assessed through maternal interviews and review of medical
records. Caldera and colleagues (2007) indicated significant improvements in the number of
families with health care coverage for the child, but no effects on immunizations, receipt of well-
child visits, incidence of injuries requiring medical care, or number of hospitalizations and
emergency department visits. Fergusson and colleagues (2005) found intervention effects on
children being up-to-date on well-child visits, experiencing fewer hospitalizations for accidents
and injuries, and having higher rates of preschool dental services enrollment, but no effects were
observed on immunization rates. Child health outcomes were not commonly or consistently
measured across studies; therefore, child health was not included in the meta-analysis.
Caregiving outcomes:
The effects of interventions to support healthy socioemotional development and
behaviour on caregiving outcomes are categorized and presented in terms of the following
aspects of parenting: caregiving knowledge, caregiving practices, caregiver-child interactions,
child maltreatment, caregivers’ mental health, and caregivers’ self-efficacy.
Caregiving knowledge: Two studies assessed programme impacts on caregiving knowledge.
Caldera and colleagues (2007) assessed maternal knowledge of infant development using the
Knowledge of Infant Development Inventory, and Barlow and colleagues (2015) assessed
caregiving knowledge through an author-designed maternal-reported questionnaire. Caldera and
colleagues (2007) found no significant effects on maternal knowledge, while Barlow and
colleagues (2015) observed significant improvements in caregiving knowledge among
intervention mothers. Unadjusted means and standard deviations were not presented, so pooled
results could not be calculated. The overall quality of evidence was graded as very low.
42 | P a g e
Caregiving practices: Eight evaluations examined programme impacts on caregiving practices.
Two studies used the HOME (Caldera et al., 2007; Barlow et al., 2015). Seven studies examined
parenting discipline strategies, two using the self-reported Parent Questionnaire (Breitenstein et
al., 2012; Gross et al., 2009), two using the self-reported Parent Behavior Checklist (Hiscock et
al., 2008; Hiscock et al., 2018), and three using the self-reported Parent-Child Conflict Tactics
Scale (Jacobs et al. 2016; Fergusson et al., 2005; Caldera et al., 2007). One study additionally
generated two parenting practices scores through factor analysis of the caregiver self-reported
Child Rearing Practices Report and the Adult-Adolescent Parenting Inventory measures
(Fergusson et al., 2005). The pooled results showed no effect on reductions in child behaviour
problems (SMD= 0.01, 95% CI: -0.04, 0.06, n=2). The overall quality of evidence was graded as
low.
Caregiver-child interactions: Five evaluations assessed programme effects on caregiver-child
interactions. One programme used the NCAST scale (Caldera et al., 2007). Two studies assessed
caregiver use of praise and commands during observed play and clean-up sessions, coded with
the Dyadic Parent-Child Interactive Coding System-Revised (Breitenstein et al., 2012; Gross et
al., 2009). Dishion and colleagues (2008) created a composite positive behaviour support score,
drawing items from HOME’s involvement subscale and direct observation measures. Van Ziejl
and colleagues (2006) assessed sensitivity, positive and negative discipline scores through three
direct observation measures during laboratory tasks. The pooled results showed no significant
effect on improving caregiver-child interactions (SMD = 0.14, 95% CI: -0.07, 0.34, n = 1). The
overall quality of evidence was graded as very low.
Child maltreatment: Two studies assessed programme impacts on child maltreatment. One study
examined parental report of contact with the Child, Youth and Family Service for issues relating
to child abuse and neglect (Fergusson et al., 2005) but did not see reductions in agency contacts.
The other (Jacobs et al., 2016) examined records from Child Protective Services to assess
whether substantiated child maltreatment reports had been filed, but also did not observe any
significant effects.
Caregiver mental health: Four studies assessed intervention impacts on caregiver mental health.
Two studies used the maternal self-reported CES-D (Barlow et al., 2015; Shaw et al., 2009) and
two studies used the primary caregiver-reported Depression Anxiety and Stress Scales (Hiscock
et al., 2008; Hiscock et al., 2018). The pooled results showed no effect on reductions in maternal
depressive symptoms (SMD = -0.05, 95% CI: -0.11, 0.01, n = 3). The overall quality of the
evidence was graded as low.
Self-efficacy: Three studies assessed intervention impacts on caregiver self-efficacy. Caldera and
colleagues (2007) measured maternal self-efficacy using the Teti Maternal Self-efficacy scale;
Breitenstein and colleagues (2012) and Gross and colleagues (2009) used the Toddler Care
Questionnaire. Both Caldera and colleagues (2007) and Breitenstein and colleagues (2012) found

43 | P a g e
intervention group mothers to have significantly higher self-reported self-efficacy scores
compared to control groups; however, Gross and colleagues (2009) found no effects. Unadjusted
means and standard deviations were not presented so pooled results could not be calculated. The
overall quality of evidence was graded as low.
Subgroup analyses:
Subgroup analyses were conducted to examine possible moderating effects by intended
programme intensity (infrequent contacts or for less than 3 months versus regular contacts and
longer than 3 months) and programme delivery (individual versus group-based/mixed contacts).
None of the pooled effect sizes on child and caregiver outcomes differed by programme intensity
or programme delivery. It is likely that statistical power to detect differences by subgroup was
limited due to the small number of studies for many of the caregiver and child outcomes.
Considerations for adverse effects and costs:
There were no indications of adverse effects caused by caregiving interventions to
support child socioemotional and behavioural development. Costing data were not readily
available. One study reported data on intervention costs (Hiscock et al., 2018). Mean costs of
this trial intervention programme were AUS$ 218 (AUS$ 208 costs to government and AUS$ 10
costs to family) and AUS$ 682 (AUS$ 516 costs to government and AUS$ 166 costs to family)
per family in the targeted and combined arms of the intervention respectively.
In conclusion, the global evidence on caregiving interventions to support children’s
socioemotional wellbeing and behaviour during the first three years of life is from HICs.
Therefore, these findings cannot be generalized to LMICs.
44 | P a g e
Evidence and recommendations for combined caregiving and nutrition
interventions (PICO 4)
Research questions
What are the effects of combined caregiving and nutrition programmes on ECD and child growth
outcomes in the first 3 years of life?
• What are the independent and additive effects of caregiving and nutrition interventions on
ECD and child growth outcomes in the first 3 years of life?
• Do the effects on ECD and child growth outcomes differ between programmes that are
targeted for young children with moderate to severe malnutrition compared to universal
programmes?
P – Caregivers and their children in the first 3 years of life
I – Combined caregiving (responsive caregiving, early learning promotion, or combined
responsive caregiving and early learning promotion) and nutrition programmes
C – a) standard of care; b) caregiving intervention alone; c) nutrition intervention alone
O – ECD (primary), child attachment, child growth, child health and nutrition, caregiving
knowledge, caregiving practices, caregiver-child interactions, and caregivers’ mental health
Summary of Evidence7
The GRADE table and forest plots for the meta-analyses are shown in Appendix I. We
identified 18 combined caregiving and nutrition interventions delivered to caregivers and their
young children during the first 3 years of life. Table 9 shows all 18 interventions (see Appendix
C for further details of programmes and characteristics). All 18 studies were conducted in
LMICs: Bangladesh (n = 6), Chile (n = 1), Colombia (n = 2), India (n = 1), Indonesia (n = 1),
Jamaica (n = 3), Pakistan (n = 1), Uganda (n = 2) and Zambia (n = 1). The RCTs varied in the
number of trial arms: 2-arms (n = 9), 3-arms (n = 2), 4-arms (n = 5), 5-arms (n = 1) and 6-arms
(n = 1). The majority of studies enrolled children from 6 months of age; however, Waber and
colleagues (1981) recruited caregivers during pregnancy, and Vazir and colleagues (2013) and
Yousafzai and colleagues (2014) enrolled children less than 6 months old.
With respect to the nutrition component of the intervention, nine studies provided
nutrition supplementation, typically with nutrition education, and the remainder focused on
nutrition education alone. Seven studies specifically targeted undernourished children (Gardner
7 The terms ‘programmes’ and ‘studies’ are used interchangeably. The term ‘programme’ does not refer to routine
service delivery in this report.

45 | P a g e
et al., 2005; Grantham-McGregor et al., 1991; Hamadani et al., 2006; Lozoff et al., 2010; Nahar
et al., 2012a; Powell et al., 2004; Tofail et al., 2013). With respect to the studies by Lozoff and
colleagues (2010) and Tofail and colleagues (2013) from Chile and Bangladesh respectively,
only the iron-deficient anemia arms of the trials were analysed. No studies were retrieved
combining caregiving and over-nutrition meeting the specified inclusion criteria in the initial
search.
Most interventions targeted mothers and children, with the exception of Singla and
colleagues (2015) where the targeting of mothers and fathers as caregivers was specified. The
interventions largely employed individual contacts or combined group and individual contacts,
with only two interventions using a group-only contact mode of delivery (Aboud & Akhter,
2011; Muhoozi et al., 2017). The average duration of implementation was 14 months, ranging
from two months (with a booster at six months) (Aboud & Akhter, 2011) to 36 months (Waber et
al., 1981).
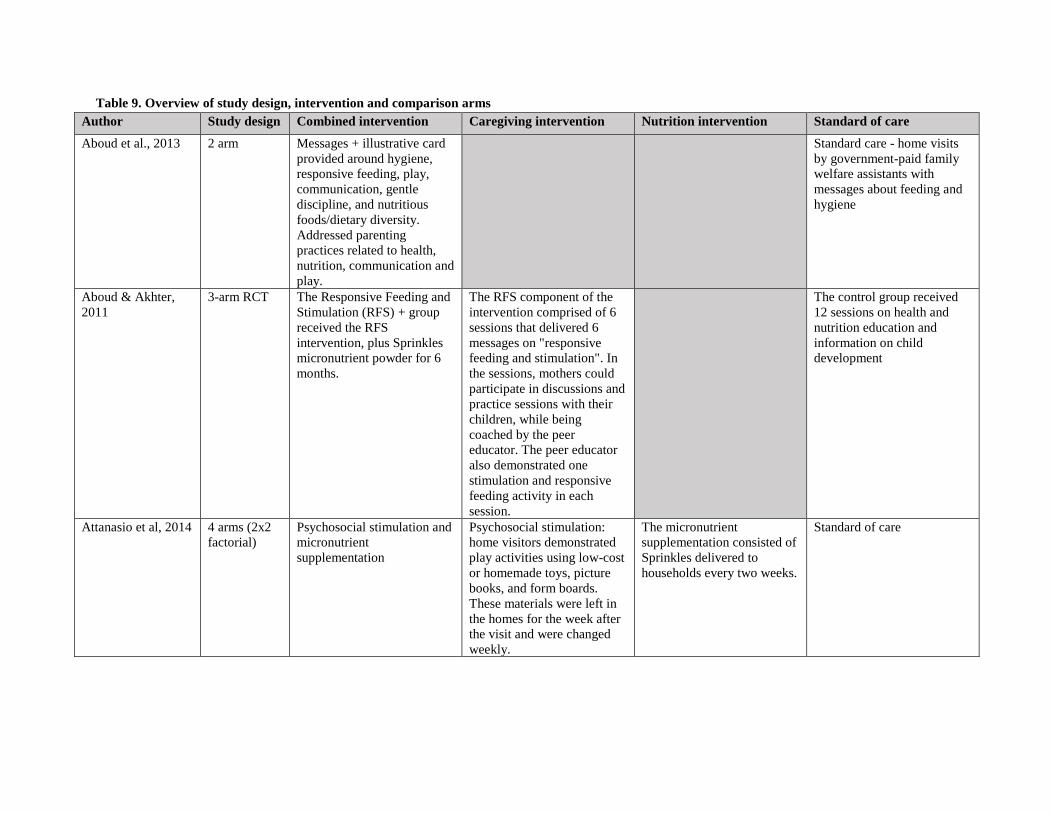
Table 9. Overview of study design, intervention and comparison arms
Author Study design Combined intervention Caregiving intervention Nutrition intervention Standard of care
Aboud et al., 2013 2 arm Messages + illustrative card
provided around hygiene,
responsive feeding, play,
communication, gentle
discipline, and nutritious
foods/dietary diversity.
Addressed parenting
practices related to health,
nutrition, communication and
play.
Standard care - home visits
by government-paid family
welfare assistants with
messages about feeding and
hygiene
Aboud & Akhter,
2011
3-arm RCT The Responsive Feeding and
Stimulation (RFS) + group
received the RFS
intervention, plus Sprinkles
micronutrient powder for 6
months.
The RFS component of the
intervention comprised of 6
sessions that delivered 6
messages on "responsive
feeding and stimulation". In
the sessions, mothers could
participate in discussions and
practice sessions with their
children, while being
coached by the peer
educator. The peer educator
also demonstrated one
stimulation and responsive
feeding activity in each
session.
The control group received
12 sessions on health and
nutrition education and
information on child
development
Attanasio et al, 2014 4 arms (2x2
factorial)
Psychosocial stimulation and
micronutrient
supplementation
Psychosocial stimulation:
home visitors demonstrated
play activities using low-cost
or homemade toys, picture
books, and form boards.
These materials were left in
the homes for the week after
the visit and were changed
weekly.
The micronutrient
supplementation consisted of
Sprinkles delivered to
households every two weeks.
Standard of care

47 | P a g e
Author Study design Combined intervention Caregiving intervention Nutrition intervention Standard of care
Frongillo et al.,
2017
Menon et al., 2016
2 arm Included intensive
interpersonal counselling on
infant and young child
feeding, responsive feeding,
mass media campaign, and
community mobilization
Alive and thrive usual
package (nutrition
counselling and mass media
campaign)
Gardner et al., 2005 4 arm (2X2
factorial
design; plus a
second non-
stunted
control
group, not
included in
this analysis)
Participants in the integrated
group received both
psychosocial stimulation and
zinc supplementation
Weekly, 30-minute
psychosocial stimulation
sessions were conducted by
trained community health
workers and focused on
improving maternal-child
interactions. In these
sessions, mothers learned
about activities to engage
with their child in an age-
appropriate fashion and
received simple toys from
the programme.
The nutrition component of
the intervention comprised
weekly zinc supplementation
The control group received
placebo and routine care but
no stimulation
Grantham-
McGregor et al.,
1991
Walker et al., 1991
4 arm (2X2
factorial
design, plus
non-stunted
control
group)
Participants received both the
supplementation and
stimulation services
In the stimulation component
of the intervention, stunted
children received weekly
hour-long home visits from
community health aides that
focused on play and
stimulation. Mothers in this
group were instructed on
how to play with children
and impact their
development. Toys left
behind after the visit
facilitated mother-child play
and interactions in-between
two visits.
The supplementation
component of the
intervention comprised of
weekly distribution of 1kg of
milk-based formula for the
duration of the intervention.
The participants in the
control group of stunted
children received weekly
health visits from health
workers and free medical
care.
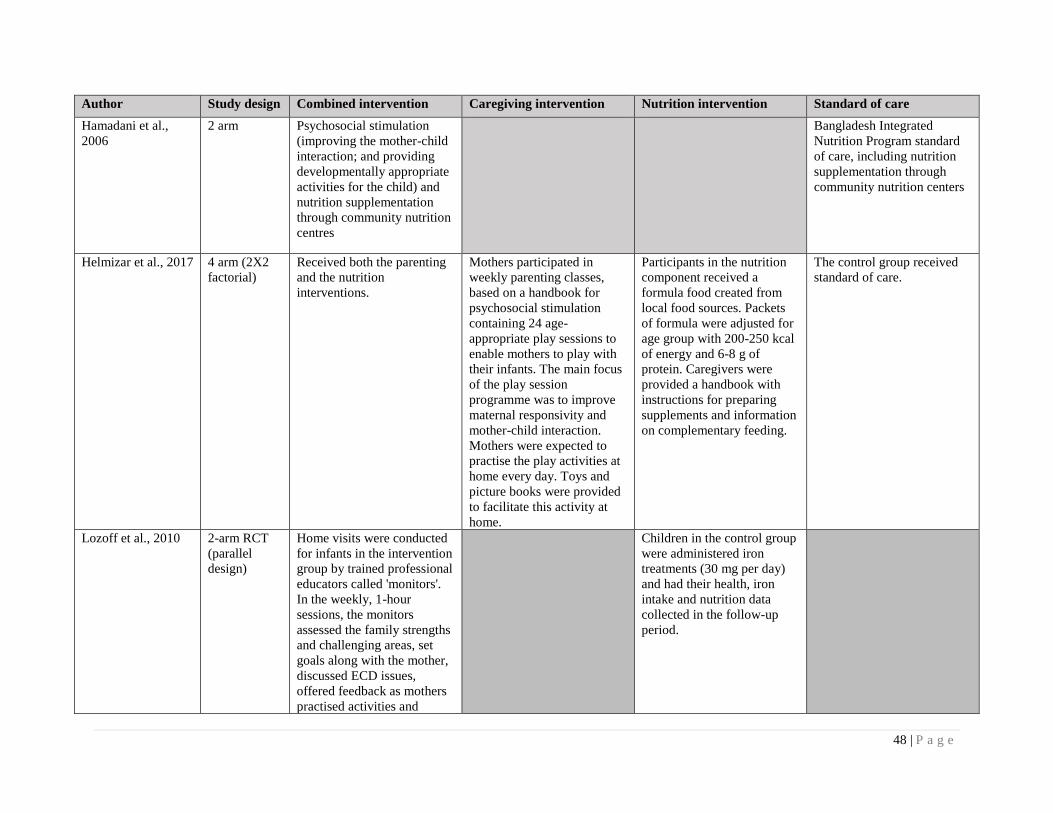
48 | P a g e
Author Study design Combined intervention Caregiving intervention Nutrition intervention Standard of care
Hamadani et al.,
2006
2 arm Psychosocial stimulation
(improving the mother-child
interaction; and providing
developmentally appropriate
activities for the child) and
nutrition supplementation
through community nutrition
centres
Bangladesh Integrated
Nutrition Program standard
of care, including nutrition
supplementation through
community nutrition centers
Helmizar et al., 2017 4 arm (2X2
factorial)
Received both the parenting
and the nutrition
interventions.
Mothers participated in
weekly parenting classes,
based on a handbook for
psychosocial stimulation
containing 24 age-
appropriate play sessions to
enable mothers to play with
their infants. The main focus
of the play session
programme was to improve
maternal responsivity and
mother-child interaction.
Mothers were expected to
practise the play activities at
home every day. Toys and
picture books were provided
to facilitate this activity at
home.
Participants in the nutrition
component received a
formula food created from
local food sources. Packets
of formula were adjusted for
age group with 200-250 kcal
of energy and 6-8 g of
protein. Caregivers were
provided a handbook with
instructions for preparing
supplements and information
on complementary feeding.
The control group received
standard of care.
Lozoff et al., 2010 2-arm RCT
(parallel
design)
Home visits were conducted
for infants in the intervention
group by trained professional
educators called 'monitors'.
In the weekly, 1-hour
sessions, the monitors
assessed the family strengths
and challenging areas, set
goals along with the mother,
discussed ECD issues,
offered feedback as mothers
practised activities and
Children in the control group
were administered iron
treatments (30 mg per day)
and had their health, iron
intake and nutrition data
collected in the follow-up
period.
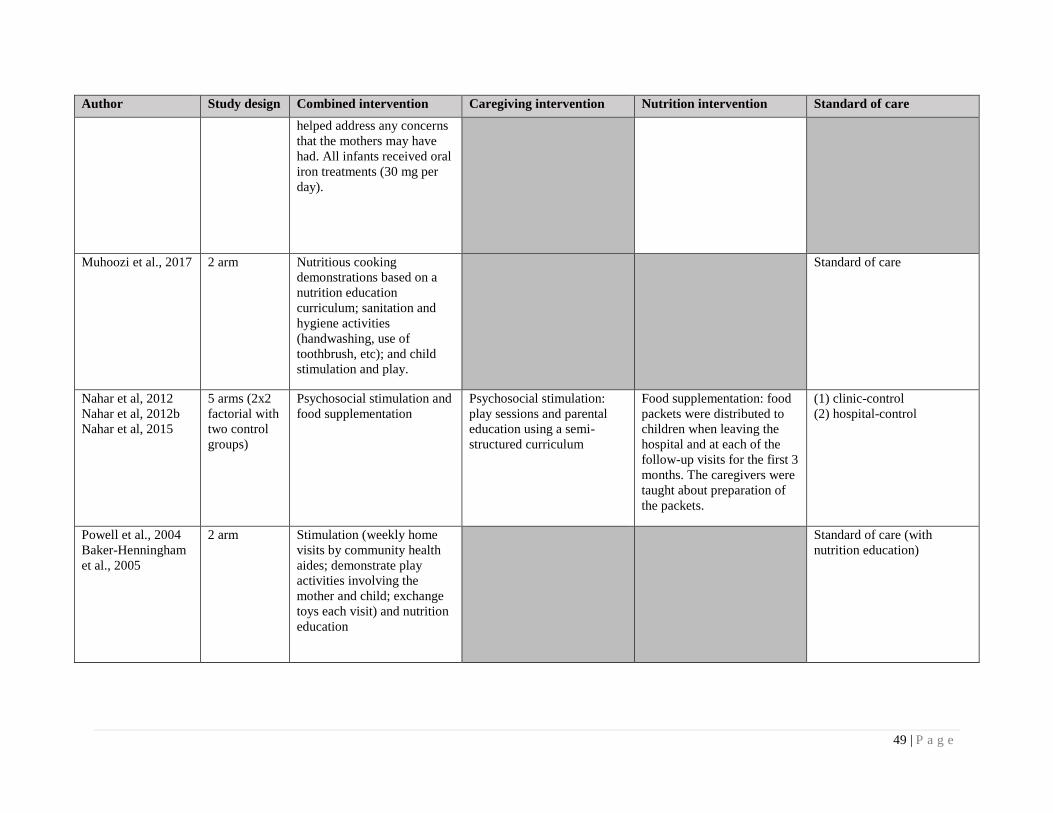
49 | P a g e
Author Study design Combined intervention Caregiving intervention Nutrition intervention Standard of care
helped address any concerns
that the mothers may have
had. All infants received oral
iron treatments (30 mg per
day).
Muhoozi et al., 2017 2 arm Nutritious cooking
demonstrations based on a
nutrition education
curriculum; sanitation and
hygiene activities
(handwashing, use of
toothbrush, etc); and child
stimulation and play.
Standard of care
Nahar et al, 2012
Nahar et al, 2012b
Nahar et al, 2015
5 arms (2x2
factorial with
two control
groups)
Psychosocial stimulation and
food supplementation
Psychosocial stimulation:
play sessions and parental
education using a semi-
structured curriculum
Food supplementation: food
packets were distributed to
children when leaving the
hospital and at each of the
follow-up visits for the first 3
months. The caregivers were
taught about preparation of
the packets.
(1) clinic-control
(2) hospital-control
Powell et al., 2004
Baker-Henningham
et al., 2005
2 arm Stimulation (weekly home
visits by community health
aides; demonstrate play
activities involving the
mother and child; exchange
toys each visit) and nutrition
education
Standard of care (with
nutrition education)

50 | P a g e
Author Study design Combined intervention Caregiving intervention Nutrition intervention Standard of care
Rockers et al., 2016 2 arm (1) Screening and referral for
symptoms of infectious
disease; (2) screening and
referral for acute
malnutrition; (3)
encouragement of the use of
routine health care services
for children; (4) group
meetings addressed different
topics each month, including
parenting skills, child
nutrition and cooking
demonstrations, forms of
play, cognitive stimulation
and language development
activities.
Standard of care
Singla et al., 2015 2 arm 12 60-90 minute-long group
sessions were held that
targeted key messages on
children and maternal well-
being. Topics included use of
play materials, gentle
discipline, consumption of a
diverse diet, hygiene and
sanitation messages. Along
with these discussions, there
were demonstrations for
ways to play and talk to the
child and of food quantities.
Topics for maternal well-
being included strengthening
primary relationships, and
there were sessions for
mothers and fathers,
independently as well as
together.
The waitlist control group
received services from Plan
Uganda as well as nutrition
information around dietary
diversity.
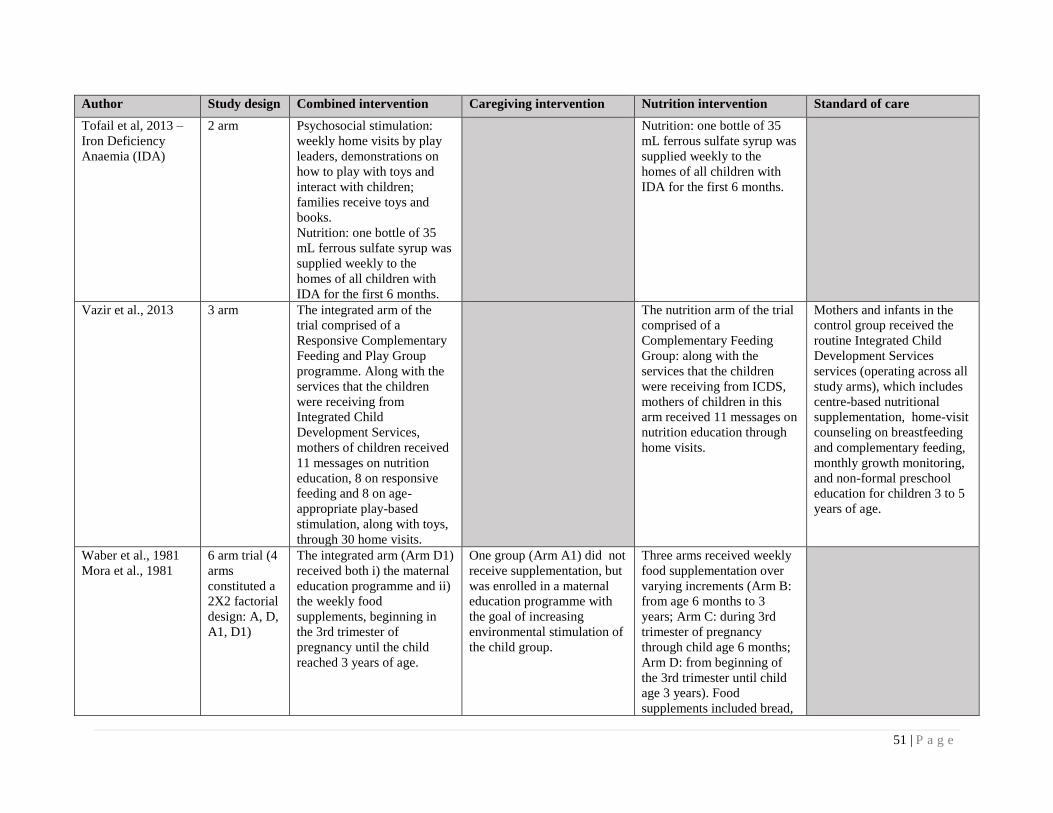
51 | P a g e
Author Study design Combined intervention Caregiving intervention Nutrition intervention Standard of care
Tofail et al, 2013 –
Iron Deficiency
Anaemia (IDA)
2 arm Psychosocial stimulation:
weekly home visits by play
leaders, demonstrations on
how to play with toys and
interact with children;
families receive toys and
books.
Nutrition: one bottle of 35
mL ferrous sulfate syrup was
supplied weekly to the
homes of all children with
IDA for the first 6 months.
Nutrition: one bottle of 35
mL ferrous sulfate syrup was
supplied weekly to the
homes of all children with
IDA for the first 6 months.
Vazir et al., 2013 3 arm The integrated arm of the
trial comprised of a
Responsive Complementary
Feeding and Play Group
programme. Along with the
services that the children
were receiving from
Integrated Child
Development Services,
mothers of children received
11 messages on nutrition
education, 8 on responsive
feeding and 8 on age-
appropriate play-based
stimulation, along with toys,
through 30 home visits.
The nutrition arm of the trial
comprised of a
Complementary Feeding
Group: along with the
services that the children
were receiving from ICDS,
mothers of children in this
arm received 11 messages on
nutrition education through
home visits.
Mothers and infants in the
control group received the
routine Integrated Child
Development Services
services (operating across all
study arms), which includes
centre-based nutritional
supplementation, home-visit
counseling on breastfeeding
and complementary feeding,
monthly growth monitoring,
and non-formal preschool
education for children 3 to 5
years of age.
Waber et al., 1981
Mora et al., 1981
6 arm trial (4
arms
constituted a
2X2 factorial
design: A, D,
A1, D1)
The integrated arm (Arm D1)
received both i) the maternal
education programme and ii)
the weekly food
supplements, beginning in
the 3rd trimester of
pregnancy until the child
reached 3 years of age.
One group (Arm A1) did not
receive supplementation, but
was enrolled in a maternal
education programme with
the goal of increasing
environmental stimulation of
the child group.
Three arms received weekly
food supplementation over
varying increments (Arm B:
from age 6 months to 3
years; Arm C: during 3rd
trimester of pregnancy
through child age 6 months;
Arm D: from beginning of
the 3rd trimester until child
age 3 years). Food
supplements included bread,
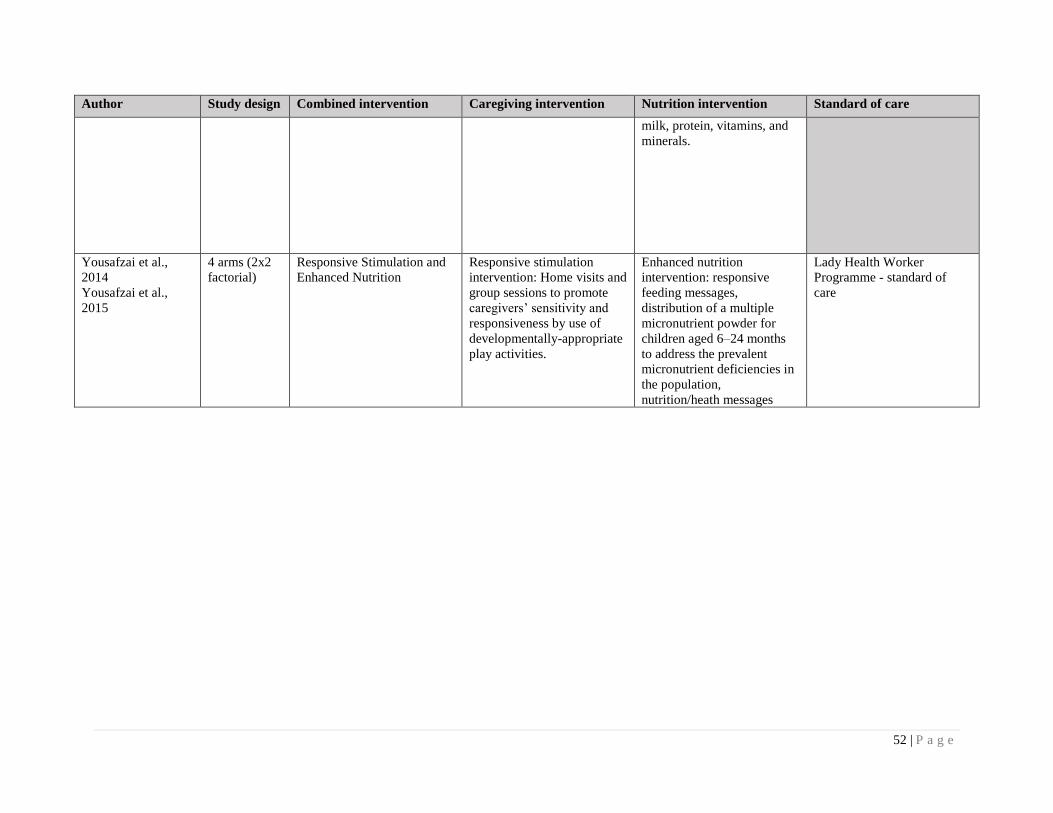
52 | P a g e
Author Study design Combined intervention Caregiving intervention Nutrition intervention Standard of care
milk, protein, vitamins, and
minerals.
Yousafzai et al.,
2014
Yousafzai et al.,
2015
4 arms (2x2
factorial)
Responsive Stimulation and
Enhanced Nutrition
Responsive stimulation
intervention: Home visits and
group sessions to promote
caregivers’ sensitivity and
responsiveness by use of
developmentally-appropriate
play activities.
Enhanced nutrition
intervention: responsive
feeding messages,
distribution of a multiple
micronutrient powder for
children aged 6–24 months
to address the prevalent
micronutrient deficiencies in
the population,
nutrition/heath messages
Lady Health Worker
Programme - standard of
care
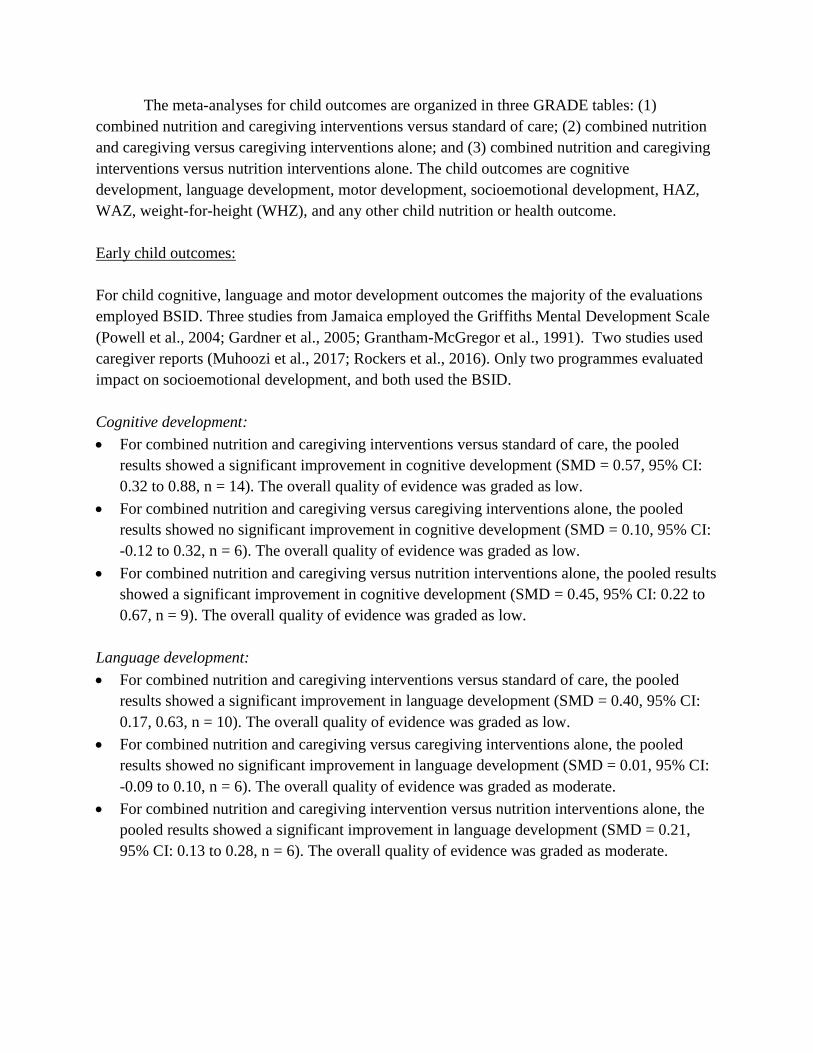
The meta-analyses for child outcomes are organized in three GRADE tables: (1)
combined nutrition and caregiving interventions versus standard of care; (2) combined nutrition
and caregiving versus caregiving interventions alone; and (3) combined nutrition and caregiving
interventions versus nutrition interventions alone. The child outcomes are cognitive
development, language development, motor development, socioemotional development, HAZ,
WAZ, weight-for-height (WHZ), and any other child nutrition or health outcome.
Early child outcomes:
For child cognitive, language and motor development outcomes the majority of the evaluations
employed BSID. Three studies from Jamaica employed the Griffiths Mental Development Scale
(Powell et al., 2004; Gardner et al., 2005; Grantham-McGregor et al., 1991). Two studies used
caregiver reports (Muhoozi et al., 2017; Rockers et al., 2016). Only two programmes evaluated
impact on socioemotional development, and both used the BSID.
Cognitive development:
• For combined nutrition and caregiving interventions versus standard of care, the pooled
results showed a significant improvement in cognitive development (SMD = 0.57, 95% CI:
0.32 to 0.88, n = 14). The overall quality of evidence was graded as low.
• For combined nutrition and caregiving versus caregiving interventions alone, the pooled
results showed no significant improvement in cognitive development (SMD = 0.10, 95% CI:
-0.12 to 0.32, n = 6). The overall quality of evidence was graded as low.
• For combined nutrition and caregiving versus nutrition interventions alone, the pooled results
showed a significant improvement in cognitive development (SMD = 0.45, 95% CI: 0.22 to
0.67, n = 9). The overall quality of evidence was graded as low.
Language development:
• For combined nutrition and caregiving interventions versus standard of care, the pooled
results showed a significant improvement in language development (SMD = 0.40, 95% CI:
0.17, 0.63, n = 10). The overall quality of evidence was graded as low.
• For combined nutrition and caregiving versus caregiving interventions alone, the pooled
results showed no significant improvement in language development (SMD = 0.01, 95% CI:
-0.09 to 0.10, n = 6). The overall quality of evidence was graded as moderate.
• For combined nutrition and caregiving intervention versus nutrition interventions alone, the
pooled results showed a significant improvement in language development (SMD = 0.21,
95% CI: 0.13 to 0.28, n = 6). The overall quality of evidence was graded as moderate.
54 | P a g e
Motor development:
• For combined nutrition and caregiving interventions versus standard of care, the pooled
results showed a significant improvement in motor development (SMD = 0.4, 95% CI: 0.26
to 0.53, n = 10). The overall quality of evidence was graded as low.
• For combined nutrition and caregiving versus caregiving interventions alone, the pooled
results showed no significant improvement in motor development (SMD = 0.18, 95% CI: -
0.06 to 0.42, n = 6). The overall quality of evidence was graded as low.
• For combined nutrition and caregiving interventions versus nutrition interventions alone, the
pooled results showed no significant improvement in motor development (SMD = 0.14, 95%
CI: 0.07 to 0.22, n = 9). The overall quality of evidence was graded as high.
Socioemotional development:
• For combined nutrition and caregiving interventions versus standard of care, the pooled
results showed no significant improvement in socioemotional development (SMD = 0.09,
95% CI: -0.11, 0.30, n = 2). The overall quality of evidence was graded as low.
• For combined nutrition and caregiving versus caregiving interventions alone, Yousafzai and
colleagues (2014) had an effect size of 0.11, 95% CI: -0.04 to 0.26. The overall quality of
evidence was graded as low.
• For combined nutrition and caregiving interventions versus nutrition interventions alone,
Yousafzai and colleagues (2014) had an effect size of -0.09, 95% CI: 0.24 to 0.07. The
overall quality of evidence was graded as low.
Overall, no significant benefits were found on child growth outcomes.
HAZ:
• For combined nutrition and caregiving interventions versus standard of care, the pooled
results showed SMD = -0.13, 95% CI: -0.31 to 0.05, n = 9. The overall quality of evidence
was graded as low.
• For combined nutrition and caregiving versus caregiving interventions alone, the pooled
results showed SMD = -0.21, 95% CI: -0.60 to 0.19, n = 4. The overall quality of evidence
was graded as low.
• For combined nutrition and caregiving interventions versus nutrition interventions alone, the
pooled results showed SMD = -0.42, 95% CI: -0.85 to 0.01, n = 4. The overall quality of
evidence was graded as low.
WAZ:
• For combined nutrition and caregiving interventions versus standard of care, the pooled
results showed SMD = 0.06, 95% CI: -0.02 to 0.13, n = 7. The overall quality of evidence
was graded as high.
55 | P a g e
• For combined nutrition and caregiving versus caregiving interventions alone, the pooled
results showed SMD = 0.07, 95% CI: -0.04 to 0.17, n = 3). The overall quality of evidence
was graded as moderate.
• For combined nutrition and caregiving interventions versus nutrition interventions alone, the
pooled results showed SMD = 0.06, 95% CI: -0.02 to 0.14, n = 4. The overall quality of
evidence was graded as moderate.
WHZ:
• For combined nutrition and caregiving interventions versus standard of care, the pooled
results showed SMD = 0.20, 95% CI: 0.05 to 0.34, n = 6. The overall quality of evidence was
graded as moderate.
• For combined nutrition and caregiving versus caregiving interventions alone, the pooled
results showed SMD = 0.16, 95% CI: 0.03 to 0.29, n = 4. The overall quality of evidence was
graded as moderate.
• For combined nutrition and caregiving interventions versus nutrition interventions alone, the
pooled results showed SMD = 0.17, 95% CI: -0.04 to 0.38, n = 5. The overall quality of
evidence was graded as low.
Impact on other child nutrition and child health outcomes: In general, child nutrition and health
outcomes were not commonly or consistently measured across studies; therefore, these outcomes
were not included in the meta-analysis. Aboud and Akhter (2011) reported significant
improvements in the intervention groups (receiving combined nutrition and caregiving
interventions) on mouthfuls eaten and handwashing practices. Vazir and colleagues (2013) found
children in the nutrition arms (with or without early learning interventions) of the trial
significantly improved dietary intake as a result of nutrition education intervention exposure.
Yousafzai and colleagues (2015) reported children exposed to nutrition interventions (with or
without responsive caregiving and early learning) had significantly improved age-appropriate
breast feeding practices, and children exposed to the caregiving interventions (with or without
the nutrition interventions) had significantly improved minimal acceptable diet and meal
frequency . Three studies found no effects on reducing sickness (Aboud et al., 2013; Menon et
al., 2016; Singla et al., 2015), while another study found reductions in diarrhoea and acute
respiratory illness (with or without responsive caregiving and early learning) (Yousafzai et al.,
2014).
Subgroup analyses
We analysed the interventions by whether they targeted malnourished children compared
with universal implementation (no targeting). The findings are shown in Tables 10-12. In each

56 | P a g e
comparison, we find the effect size for development outcomes are higher for malnourished
children than the universally-implemented studies, with mixed results on growth outcomes.
Table 10. Combined responsive caregiving and early learning versus standard of care
Outcome Overall Targeted: malnourished Universal
SMD 95% CI N SMD 95% CI N SMD 95% CI N
Cognitive
development
0.57 0.32, 0.82 13 0.63 0.34, 0.92 6 0.52 0.15, 0.88 7
Language
development
0.40 0.17, 0.63 10 0.56 0.32, 0.81 3 0.35 0.07, 0.63 7
Motor development 0.40 0.26, 0.53 10 0.38 0.13, 0.64 5 0.41 0.25, 0.58 5
Attachment
Socioemotional
development
0.09 -0.11, 0.30 1
HAZ -0.13 -0.31, 0.05 9 -0.36 -0.88, 0.15 2 -0.07 -0.25, 0.11 7
WAZ 0.06 -0.02, 0.13 7 0.00 -0.14, 0.14 2 0.08 -0.01, 0.17 5
WHZ 0.20 0.05, 0.34 6 0.11 -0.10, 0.31 3 0.25 0.04, 0.46 3
Table 11. Combined responsive caregiving and early learning versus caregiving alone
Outcome Overall Targeted: malnourished Universal
SMD 95% CI N SMD 95% CI N SMD 95% CI N
Cognitive
development
0.10 -0.12, 0.32 6 0.32 -0.03, 0.66 4 -0.13 -0.24, -0.02 2
Language
development
0.01 -0.09, 0.10 6 0.26 -0.12, 0.63 2 -0.01 -0.11, 0.09 4
Motor
development
0.18 -0.06, 0.42 6 0.42 -0.26, 1.09 3 0.06 -0.14, 0.25 3
Attachment
Socioemotional
development
0.11 -0.04, 0.26 1
HAZ -0.21 -0.60, 0.19 4 -0.83 -1.19, -0.46 1 0.00 -0.25, 0.25 3
WAZ 0.07 -0.04, 0.17 3 0.00 -0.15, 0.15 1 0.12 -0.02, 0.27 2
WHZ 0.16 0.03, 0.29 4 0.09 -0.19, 0.38 2 0.18 0.03, 0.32 2
Table 12. Combined responsive caregiving and early learning versus nutrition alone
Outcome Overall Targeted: malnourished Universal
SMD 95% CI N SMD 95% CI N SMD 95% CI N
Cognitive
development
0.45 0.22, 0.67 9 0.61 0.18, 1.05 6 0.23 0.13, 0.33 3
Language
development
0.21 0.13, 0.28 6 0.43 -0.20, 1.07 2 0.21 0.15, 0.27 4
Motor
development
0.14 0.07, 0.22 9 0.07 -0.16, 0.30 4 0.17 0.11, 0.23 6
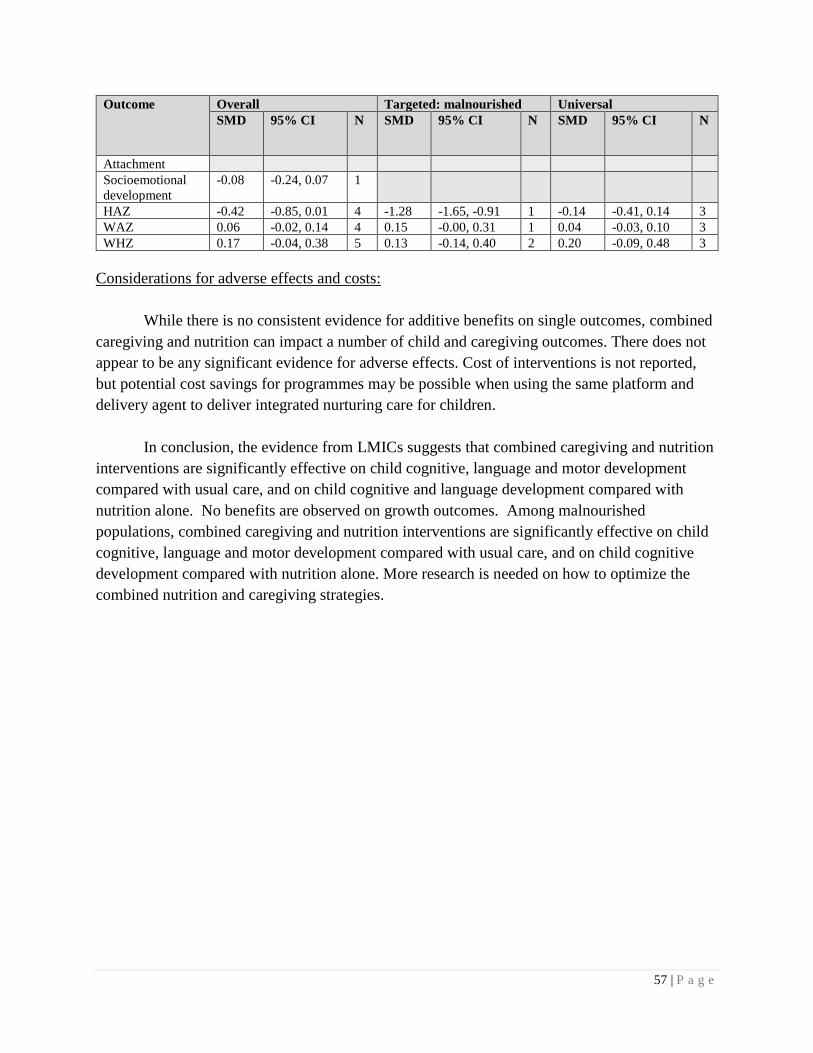
57 | P a g e
Outcome Overall Targeted: malnourished Universal
SMD 95% CI N SMD 95% CI N SMD 95% CI N
Attachment
Socioemotional
development
-0.08 -0.24, 0.07 1
HAZ -0.42 -0.85, 0.01 4 -1.28 -1.65, -0.91 1 -0.14 -0.41, 0.14 3
WAZ 0.06 -0.02, 0.14 4 0.15 -0.00, 0.31 1 0.04 -0.03, 0.10 3
WHZ 0.17 -0.04, 0.38 5 0.13 -0.14, 0.40 2 0.20 -0.09, 0.48 3
Considerations for adverse effects and costs:
While there is no consistent evidence for additive benefits on single outcomes, combined
caregiving and nutrition can impact a number of child and caregiving outcomes. There does not
appear to be any significant evidence for adverse effects. Cost of interventions is not reported,
but potential cost savings for programmes may be possible when using the same platform and
delivery agent to deliver integrated nurturing care for children.
In conclusion, the evidence from LMICs suggests that combined caregiving and nutrition
interventions are significantly effective on child cognitive, language and motor development
compared with usual care, and on child cognitive and language development compared with
nutrition alone. No benefits are observed on growth outcomes. Among malnourished
populations, combined caregiving and nutrition interventions are significantly effective on child
cognitive, language and motor development compared with usual care, and on child cognitive
development compared with nutrition alone. More research is needed on how to optimize the
combined nutrition and caregiving strategies.

Research gaps
In undertaking the systematic reviews, the following research gaps were identified by the
research team.
1. The largest group of studies were for (additional analysis) 2.1 (combined responsive
caregiving and promotion of early learning) with good global representation. However, PICO
1 (responsive caregiving alone) had limited intervention research in LMICs. Similarly, PICO
4 (integrated caregiving and nutrition programmes) was largely focused on undernutrition in
LMICs and did not address the growing challenges in many countries on child overnutrition.
2. Few studies report on caregiving-related outcomes, which are critical for understanding
processes for the effectiveness of caregiving/parenting programmes on child outcomes
(Jeong et al., 2018).
3. Few studies reported adequate information on programme characteristics to enable analysis
on actual implementation processes, rather than intended implementation processes (e.g.
dosage, behaviour change techniques). These data are essential to inform evidence-based
implementation planning of nurturing care programmes.
4. There is little information on caregiving and overnutrition.
5. Few studies reported findings on subgroups to determine whether interventions were more or
less effective for particular groups within the population (e.g. child and caregiver
characteristics).
6. Limited data on cost were reported in relation to the interventions. Policy makers require cost
information to plan programmes, and more research is required on costing of interventions.
7. Many tools employed to assess both child and caregiving outcomes are unstandardized,
making it difficult to assess a specific construct of development. Reporting about the
reliability and validity of adapted tools is limited.
8. Definitions for interventions are variable, making comparisons challenging. The systematic
review team defined common characteristics for interventions categorized as responsive
caregiving, early learning promotion, and support for socioemotional and behavioural
development. Clear intervention reporting guidelines would be helpful for the multi-
disciplinary research community working in the field of ECD.
9. Data from large scale studies are limited.
10. Data that report on caregivers, other than mothers, and measure outcomes on other caregivers
are limited.
59 | P a g e
References
Cited in introduction and methods
Aboud FE, Yousafzai AK. Very early childhood development. Reproductive, Maternal,
Newborn, and Child Health. 2016: 241.
Aboud FE, Yousafzai AK. Global health and development in early childhood. Ann Rev Psychol.
2015; 66:433-57.
Black MM, Walker SP, Fernald LC, et al. Early childhood development coming of age: science
through the life course. Lancet 2017; 389(10064): 77-90.
Britto PR, Lye SJ, Proulx K, et al. Nurturing care: promoting early childhood development.
Lancet. 2017; 389(10064): 91-102.
Britto P, Ponguta L, Reyes C, Karnati R. A systematic review of parenting programmes for
young children in low-and middle-income countries. New York, NY: United Nations Children’s
Fund; 2015.
Eshel N, Daelmans B, Mello MCd, Martines J. Responsive parenting: interventions and
outcomes. Bull World Health Org. 2006; 84(12): 991-8.
Fergusson DM, Grant H, Horwood LJ, Ridder EM. Randomized trial of the Early Start program
of home visitation. Pediatrics. 2005; 116(6): e803-9.
Jeong J, Pitchik HO, Yousafzai AK. Stimulation interventions and parenting in low- and middle-
income countries: a meta-analysis. Pediatrics. 2018; e20173510.
Lu C, Black MM, Richter LM. Risk of poor development in young children in low-income and
middle-income countries: an estimation and analysis at the global, regional, and country level.
Lancet Global Health. 2016; 4(12): e916-e22.
Nelson CA. The neurobiological bases of early intervention. Handbook of early childhood
intervention. 2000; 2: 204-27.
Mol SE, Bus AG, De Jong MT, Smeets DJ. Added value of dialogic parent–child book readings:
a meta-analysis. Early Education and Development. 2008; 19(1): 7-26.
Richter LM, Daelmans B, Lombardi J, et al. Investing in the foundation of sustainable
development: pathways to scale up for early childhood development. Lancet. 2017; 389(10064):
103-18.

60 | P a g e
Tanner‐Smith EE & Tipton E. Robust variance estimation with dependent effect sizes: practical
considerations including a software tutorial in Stata and SPSS. Research Synthesis
Methods. 2014; 5(1): 13-30.
Studies/records included in review
Aboud FE, Akhter S. A cluster-randomized evaluation of a responsive stimulation and feeding
intervention in Bangladesh. Pediatrics. 2011; 127(5): e1191-7.
Aboud FE, Singla DR, Nahil MI, Borisova I. Effectiveness of a parenting program in Bangladesh
to address early childhood health, growth and development. Soc Sci Med. 2013; 97: 250-8.
Attanasio OP, Fernández C, Fitzsimons EO, Grantham-McGregor SM, Meghir C, Rubio-Codina
M. Using the infrastructure of a conditional cash transfer program to deliver a scalable integrated
early child development program in Colombia: cluster randomized controlled trial. BMJ. 2014;
349: g5785.
Baker-Henningham H, Powell C, Walker S, Grantham-McGregor S. The effect of early
stimulation on maternal depression: a cluster randomised controlled trial. Arch Dis Child. 2005;
90(12): 1230-4.
Barlow J., et al. Role of home visiting in improving parenting and health in families at risk of
abuse and neglect: results of a multicentre randomised controlled trial and economic evaluation.
Arch Dis Child. 2007; 92(3): 229-33.
Barlow A, Mullany B, Neault N, et al. Paraprofessional-delivered home-visiting intervention for
American Indian teen mothers and children: 3-year outcomes from a randomized controlled trial.
Am J Psychiatry. 2015; 172(2): 154-62.
Barrera M. E., et al. Early home intervention with low-birth-weight infants and their parents.
Child Dev. 1986; 57(1): 20-33.
Breitenstein SM, Gross D, Fogg L, Ridge A, Garvey C, Julion W et al. The Chicago Parent
Program: comparing 1-year outcomes for African American and Latino parents of young
children. Res Nurs Health. 2012; 35(5): 475-89.
Brooks-Gunn J, et al. Effects of early intervention on cognitive function of low birth weight
preterm infants. Pediatrics. 1992; 120: 350-9.
Caldera D, Burrell L, Rodriguez K, Crowne SS, Rohde C, Duggan A. Impact of a statewide
home visiting program on parenting and on child health and development. Child Abuse Negl.
2007; 31(8): 829-52.
61 | P a g e
Caughy MOB, et al. The effects of the Healthy Steps for Young Children Program: results from
observations of parenting and child development." Early Childhood Research Quarterly. 19(4):
611-30.
Chang SM, Grantham-McGregor SM, Powell CA, et al. Integrating a parenting intervention with
routine primary health care: a cluster randomized trial. Pediatrics. 2015; 136(2): 272-80.
Cheng S, et al. The effectiveness of early intervention and the factors related to child behavioural
problems at age 2: a randomized controlled trial. Early Hum Dev. 2007; 83(10): 683-91.
Constantino JN, et al. Supplementation of urban home visitation with a series of group meetings
for parents and infants: results of a "real-world" randomized, controlled trial. Child Abuse Negl.
25(12): 1571-81.
Cooper PJ, Tomlinson M, Swartz L, et al. Improving quality of mother-infant relationship and
infant attachment in socioeconomically deprived community in South Africa: randomised
controlled trial. BMJ. 2009; 338(7701): 997.
Cronan T A, et al. The effects of a community-based literacy program on young children's
language and conceptual development. Am J Community Psychol. 1996; 24(2): 51-272.
Dishion TJ, Shaw D, Connell A, Gardner F, Weaver C, Wilson M. The family check-up with
high-risk indigent families: preventing problem behavior by increasing parents' positive behavior
support in early childhood. Child Dev. 2008; 79(5): 1395-414.
Dozier M, et al. Effects of a foster parent training program on young children's attachment
behaviors: preliminary evidence from a Randomized Clinical Trial. Child Adolesc Social Work
J. 26(4): 321-32.
Drotar D, Robinson J, Jeavons L, Lester Kirchner H. A randomized, controlled evaluation of
early intervention: the Born to Learn curriculum. Child Care Health Dev. 2009; 35(5): 643-9.
Fergusson DM, Grant H, Horwood J, Ridder EM Randomized trial of the Early Start Program of
Home Visitation. Pediatricts. 2005; 116(6): e803-e809.
Fernald LC, Kagawa R, Knauer HA, Schnaas L, Guerra AG, Neufeld LM. Promoting child
development through group-based parent support within a cash transfer program: experimental
effects on children’s outcomes. Developmental psychology. 2017; 53(2): 222.
Field T, et al. Effects of parent training on teenage mother and their infants. Pediatrics. 69(6):
703-7.
Frongillo EA, Nguyen PH, Saha KK, et al. Large-scale behavior-change initiative for infant and
young child feeding advanced language and motor development in a cluster-randomized program
evaluation in Bangladesh. J Nutr. 2017; 147(2): 256-63.
62 | P a g e
Gardner JM, Powell CA, Baker-Henningham H, Walker SP, Cole TJ, Grantham-McGregor SM.
Zinc supplementation and psychosocial stimulation: effects on the development of
undernourished Jamaican children. Am J Clin Nutr. 2005; 82(2): 399-405.
Goldfeld S, Napiza N, Quach J, Reilly S, Ukoumunne OC, Wake M. Outcomes of a universal
shared reading intervention by 2 years of age: the Let's Read trial. Pediatrics. 2011; 127(3): 445-
53.
Goodson BD, Layzer JI, Pierre RG, Bernstein LS, Lopez M. Effectiveness of a comprehensive,
five-year family support program for low-income children and their families: findings from the
Comprehensive Child Development Program. Early Childhood Research Quarterly. 2000; 15(1):
5-39.
Gowani S, Yousafzai AK, Armstrong R, Bhutta ZA. Cost effectiveness of responsive
stimulation and nutrition interventions on early child development outcomes in Pakistan. Ann N
Y Acad Sci. 2014; 1308: 149-161.
Grantham-McGregor SM, Powell CA, Walker SP, Himes JH. Nutritional supplementation,
psychosocial stimulation, and mental development of stunted children: the Jamaican Study.
Lancet. 1991; 338(8758): 1-5.
Gross D, Garvey C, Julion W, Fogg L, Tucker S, Mokros H. Efficacy of the Chicago parent
program with low-income African American and Latino parents of young children. Prevention
science: the official journal of the Society for Prevention Research. 2009; 10(1): 54-65.
Guedeney A, et al. Impact of a randomized home-visiting trial on infant social withdrawal in the
CAPEDP prevention study. Infant Mental Health Journal. 2013; 34(6): 594-601.
Guttentag CL, Landry SH, Williams JM, et al. "My Baby & Me": effects of an early,
comprehensive parenting intervention on at-risk mothers and their children. Dev Psychol. 2014;
50(5): 1482-96.
Hamadani JD, Huda SN, Khatun F, Grantham-McGregor SM. Psychosocial stimulation
improves the development of undernourished children in rural Bangladesh. J Nutr. 2006;
136(10): 2645-52.
Hartinger SM, Lanata CF, Hattendorf J, et al. Impact of a child stimulation intervention on early
child development in rural Peru: a cluster randomised trial using a reciprocal control design. J
Epidemiol Community Health. 2017; 71(3): 217-24.
Heinicke CM, et al. Relationship-based intervention with at-risk mothers: Outcome in the first
year of life. Infant Mental Health Journal. 1999; 20(4): 349-74.
Helmizar H, Jalal F, Lipoeto NI, Achadi EL. Local food supplementation and psychosocial
stimulation improve linear growth and cognitive development among Indonesian infants aged 6
to 9 months. Asia Pacific Journal of Clinical Nutrition. 2017; 26(1): 97.
63 | P a g e
Heubner CE Promoting toddlers' language development through community-based intervention.
Journal of Applied Developmental Psychology. 21(5): 513-35.
Hiscock H, Bayer JK, Price A, Ukoumunne OC, Rogers S, Wake M. Universal parenting
programme to prevent early childhood behavioural problems: cluster randomised trial. BMJ
2008; 336(7639): 318-21.
Hiscock H, Gulenc A, Ukoumunne OC, et al. Preventing preschool mental health problems:
population-based cluster randomized controlled trial. J Dev Behav Pediatr. 2018; 39(1): 55-65.
Hutchings J, et al. Evaluating the Incredible Years Toddler Parenting Programme with parents of
toddlers in disadvantaged (Flying Start) areas of Wales. Child Care Health Dev. 2016; 43(1):
104-13.
Jacobs F, Easterbrooks MA, Goldberg J, et al. Improving adolescent parenting: results from a
randomized controlled trial of a home visiting program for young families. Am J Public Health.
2016; 106(2): 342-9.
Jin X, et al. "Care for Development" intervention in rural China: a prospective follow-up study. J
Dev Behav Pediatr. 28(3): 213-8.
Johnson DL, et al. TheHouston Parent-childDevelopment Center: a parent education program for
Mexican-American families. Amer J Orthopsychiat. 44(1): 121-8.
Juffer F, et al. Early intervention in adoptive families: supporting maternal sensitive
responsiveness, infant-mother attachment, and infant competence. J Child Psychol Psychiatry.
38(8): 1039-50.
Kaaresen PI, et al. A randomized controlled trial of an early intervention program in low birth
weight children: outcome at 2 years. Early Hum Dev. 2008; 84(3): 201-9.
Kalinauskiene L, et al. Supporting insensitive mothers: the Vilnius randomized control trial of
video-feedback intervention to promote maternal sensitivity and infant attachment security.
Child Care Health Dev.2009; 35(5): 613-23.
Kaminski JW, Perou R, Visser SN, et al. Behavioral and socioemotional outcomes through age 5
years of the legacy for children public health approach to improving developmental outcomes
among children born into poverty. Am J Public Health. 2013; 103(6): 1058-66.
Kitzman H, Olds DL, Henderson CR Jr, et al. Effect of prenatal and infancy home visitation by
nurses on pregnancy outcomes, childhood injuries, and repeated childbearing. A randomized
controlled trial. JAMA . 1997; 278(8): 644-52.
Kochanska G, et al. Promoting toddlers' positive social-emotional outcomes in low-income
families: a play-based experimental study. J Clin Child Adolesc Psychol. 2013; 42(5): 700-12.
64 | P a g e
Kyno NM, et al. Effect of an early intervention programme on development of moderate and
late preterm infants at 36 months: a randomized controlled study. Infant Behav Dev. 2012; 35(4):
916-26.
Leung C, Tsang S, Li B. Efficacy of Fun to Learn for the Young Program: randomized
controlled trial. J Child Fam Stud. 2017a; 26: 2865-78.
Leung C, et al. Evaluation of Parent and Child Enhancement (PACE) program: randomized
controlled trial. Research on Social Work Practice. 2017b; 27(1): 19-35.
Love JM, Kisker EE, Ross C, et al. The effectiveness of early head start for 3-year-old children
and their parents: lessons for policy and programs. Dev Psychol. 2005; 41(6): 885-901.
Lozoff B, Smith JB, Clark KM, Perales CG, Rivera F, Catillo M. Home intervention improves
cognitive and social-emotional scores in iron-deficient anemic infants. Pediatrics. 2010; 126(4):
e884-e894.
Madden J, et al. Home again: effects of the Mother-Child Home Program on mother and child.
Child Dev. 1984; 55(2): 636-47.
McGillion M, et al. A randomised controlled trial to test the effect of promoting caregiver
contingent talk on language development in infants from diverse socioeconomic status
backgrounds. J Child Psychol Psychiatry. 2017; 58(10): 1122-31.
Mendelsohn AL, Valdez P, Flynn V, Foley G, Berkule S, Tomopoulos S, et al. Use of
videotaped interactions during pediatric well-child care: impact at 33 months on parenting and
on child development. Journal of Developmental and Behavioral Pediatrics. 2007; 28:206–12.
Menon P, Nguyen PH, Saha KK, Khaled A, Sanghvi T, Baker J, et al. Combining intensive
counseling by frontline workers with a nationwide mass media campaign has large differential
impacts on complementary feeding practices but not on child growth: results of a cluster-
randomized program evaluation in Bangladesh–3. Journal of Nutrition. 2016; 146(10): 2075-84.
Mora J, Herrera M, Suescun J, De Navarro L, Wagner M. The effects of nutritional
supplementation on physical growth of children at risk of malnutrition. Am J Clinical Nutrition.
1981; 34(9): 1885-92.
Muhoozi GKM, Atukunda P, Diep LM, et al. Nutrition, hygiene, and stimulation education to
improve growth, cognitive, language, and motor development among infants in Uganda: a
cluster-randomized trial. Matern Child Nutr. 2017;
Murray L, De Pascalis L, Tomlinson M, et al. Randomized controlled trial of a book-sharing
intervention in a deprived South African community: effects on carer-infant interactions, and
their relation to infant cognitive and socioemotional outcome. J Child Psychol Psychiatry. 2016;
57(12): 1370-9.
65 | P a g e
Nahar B, Hossain MI, Hamadani JD, et al. Effects of a community-based approach of food and
psychosocial stimulation on growth and development of severely malnourished children in
Bangladesh: a randomised trial. Eur J Clin Nutr. 2012a; 66(6): 701-9.
Nahar B, Hossain MI, Hamadani JD, Ahmed T, Grantham-McGregor S, Persson LA. Effects of
psychosocial stimulation on improving home environment and child-rearing practices: results
from a community-based trial among severely malnourished children in Bangladesh. BMC
Public Health. 2012b; 12: 622.
Nahar B, Hossain I, Hamadani JD, Ahmed T, Grantham‐ McGregor S, Persson LA. Effect of a
food supplementation and psychosocial stimulation trial for severely malnourished children on
the level of maternal depressive symptoms in Bangladesh. Child: care, health and development.
2015; 41(3): 483-93.
Nair MKC, Philip E, Jeyaseelan L, George B, Mathews S, Padma K. Effect of Child
Development Centre Model early stimulation among at-risk babies-a randomized controlled
trial. Indian Pediatrics. 2009; 46: S20-S26.
Norr KF, Crittenden KS, Lehrer EL, et al. Maternal and infant outcomes at one year for a nurse-
health advocate home visiting program serving African Americans and Mexican Americans.
Public Health Nurs. 2003; 20(3): 190-203.
Olds DL, et al. Preventing child abuse and neglect: a randomized trial of nurse home visitation.
Pediatrics. 1986. 78(1): 65-78.
Olds DL, Robinson J, O'Brien R, et al. Home visiting by paraprofessionals and by nurses: a
randomized, controlled trial. Pediatrics. 2002; 110(3): 486-96.
Pontoppidan M, et al. The Incredible Years Parents and Babies Program: a pilot randomized
controlled trial." PLoS One. 2016;11(12): e0167592.
Powell C, Grantham McGregor S. Home visiting of varying frequency and child development.
Pediatrics. 1989; 84(1): 157-64.
Powell C, Baker-Henningham H, Walker S, Gernay J, Grantham-McGregor S. Feasibility of
integrating early stimulation into primary care for undernourished Jamaican children: cluster
randomised controlled trial. BMJ. 2004; 329(7457): 89.
Rauh VA, et al. Minimizing adverse effects of low birthweight: four-year results of an early
intervention program. Child Dev. 1988; 59(3): 544-53.
Robling M, Bekkers MJ, Bell K, et al. Effectiveness of a nurse-led intensive home-visitation
programme for first-time teenage mothers (Building Blocks): a pragmatic randomised controlled
trial. Lancet. 2016; 387(10014): 146-55.
66 | P a g e
Rockers PC, Fink G, Zanolini A, et al. Impact of a community-based package of interventions on
child development in Zambia: a cluster-randomised controlled trial. BMJ Global Health. 2016;
1(3): e000104.
Roggman LA, et al. Keeping kids on track: mpacts of a parenting-focused Early Head Start
program on attachment security and cognitive development. Early Education and Development.
2009; 20(6): 920-41.
Santelices MP, et al. Promoting secure attachment: Evaluation of the effectiveness of an early
intervention pilot programme with mother–infant dyads in Santiago, Chile. Child: Care, Health
and Development. 2011; 37(2): 203-10.
Sawyer MG, Reece CE, Bowering K, et al. Nurse-moderated internet-based support for new
mothers: non-inferiority, randomized controlled trial. J Med Internet Res. 2017; 19(7): e258.
Scarr S, McCartney K. Far from home: an experimental evaluation of the Mother-Child Home
Program in Bermuda. Child Development. 1988; 59(3): 531-43.
Schwarz DF, O'Sullivan AL, Guinn J, et al. Promoting early intervention referral through a
randomized controlled home-visiting program. Journal of Early Intervention. 2012; 34(1): 20-39.
Shaw DS, Connell A, Dishion TJ, Wilson MN, Gardner F. Improvements in maternal depression
as a mediator of intervention effects on early childhood problem behavior. Dev Psychopathol.
2009; 21(2): 417-39.
Singla DR, Kumbakumba E, Aboud FE. Effects of a parenting intervention to address maternal
psychological wellbeing and child development and growth in rural Uganda: a community-
based, cluster randomised trial. Lancet Global Health. 2015; 3(8): e458-e69.
Spieker SJ, Oxford ML, Kelly JF, Nelson EM, Fleming CB. Promoting first relationships:
randomized trial of a relationship-based intervention for toddlers in child welfare. Child
Maltreatment. 2012; 17(4): 271-86.
Tofail F, Hamadani JD, Mehrin F, Ridout DA, Huda SN, Grantham-McGregor SM. Psychosocial
stimulation benefits development in nonanemic children but not in anemic, iron-deficient
children–3. Journal of Nutrition. 2013; 143(6): 885-93.
Vally Z, et al. The impact of dialogic book‐sharing training on infant language and attention: a
randomized controlled trial in a deprived South African community. Journal of Child Psychology
and Psychiatry. 2015;56(8): 865-73.
Van Zeijl J, Mesman J, Van IJzendoorn MH, et al. Attachment-based intervention for enhancing
sensitive discipline in mothers of 1-to 3-year-old children at risk for externalizing behavior
problems: a randomized controlled trial. Journal of Consulting and Clinical Psychology. 2006;
74(6): 994.
67 | P a g e
Vazir S, Engle P, Balakrishna N, et al. Cluster-randomized trial on complementary and
responsive feeding education to caregivers found improved dietary intake, growth and
development among rural Indian toddlers. Matern Child Nutr. 2013; 9(1): 99-117.
Velderman MK, et al. Effects of attachment-based interventions on maternal sensitivity and
infant attachment: differential susceptibility of highly reactive infants. J Fam Psychol. 2006;
20(2): 266-74.
Waber DP, Vuori-Christiansen L, Ortiz N, et al. Nutritional supplementation, maternal
education, and cognitive development of infants at risk of malnutrition. AmJ Clin Nut. 1981;
34(4): 807-13.
Wagner M, et al. The effectiveness of the Parents as Teachers program with low-income parents
and children. Topics in Early Childhood Special Education. 2002; 22(2): 67-81.
Wake M, Tobin S, Girolametto L, et al. Outcomes of population based language promotion for
slow to talk toddlers at ages 2 and 3 years: Let’s Learn Language cluster randomised controlled
trial. BMJ. 2011; 343(7821): 1-10.
Walker SP, Powell CA, Grantham-McGregor SM, Himes JH, Chang SM. Nutritional
supplementation, psychosocial stimulation, and growth of stunted children: the Jamaican study.
Am J Clin Nut. 1991; 54(4): 642-8.
Walker SP, Chang SM, Powell CA, Grantham-McGregor, SM. Psychosocial intervention
improves the development of term low-birth-weight infants. Community and International
Nutrition. 2004; 134(6): 1417-23.
Walkup JT, et al. Randomized controlled trial of a paraprofessional-delivered in-home
intervention for young reservation-based American Indian mothers." J Am Acad Child Adolesc
Psychiatry. 2009;48(6): 591-601.
Wallander JL, Bann CM, Biasini FJ, et al. Development of children at risk for adverse outcomes
participating in early intervention in developing countries: a randomized controlled trial. J Child
Psychol Psychiatry. 2014; 55(11): 1251-9.
Wasik BH et al. A longitudinal study of two early intervention strategies: Project CARE. Child
Dev. 1990; 61(6): 1682-96.
Weisleder A, Cates CB, Dreyer BP, et al. Promotion of positive parenting and prevention of
socioemotional disparities. Pediatrics. 2016; 137(2): e20153239.
Whitt JK, Casey PH. The mother–infant relationship and infant development: the effect of
pediatric intervention. Child Development. 1982; 53(4): 948-56.
Yousafzai AK, Rasheed MA, Rizvi A, Armstrong R, Bhutta ZA. Effect of integrated responsive
stimulation and nutrition interventions in the Lady Health Worker programme in Pakistan on

68 | P a g e
child development, growth, and health outcomes: a cluster-randomised factorial effectiveness
trial. Lancet. 2014; 384(9950): 1282-93.
Yousafzai AK, Rasheed MA, Rizvi A, Armstrong R, Bhutta ZA. Parenting skills and emotional
availability: an RCT. Pediatrics. 2015; 135(5): e1247-57.
69 | P a g e
Appendix A: Glossary
• Attachment: an emotional bond between an infant and one or more adults. The infant will
approach these individuals in times of distress, particularly during the phase of infant
development when the presence of strangers induces anxiety. In addition, the infant is
distressed if separated from attachment figures.1
o Attachment status: a description of an infant’s attachment as being either secure or
insecure.
▪ Secure attachment: a child who is securely attached actively explores the
environment in the presence of the caregiver, is visibly upset by separation,
and greets the mother warmly when they are reunited.
▪ Insecure attachment: attachment that takes one of three forms: avoidant
attachment, anxious-resistant attachment and disorganized/disoriented
attachment.
• Attunement: an empathic responsiveness between two individuals, described by Daniel
Stern as the ‘performance of behaviours that express the quality of feeling of a shared affect
state.’2
• Behaviour problems:
o Externalizing: “behaviour problems that are manifested in children’s outward
behaviour and reflect the child negatively acting on the external environment. Other
terms to describe externalizing behaviour problems include ‘conduct problems,’
‘antisocial,’ and ‘under-controlled.’3
o Internalizing: “behaviour problems such as withdrawn, anxious, inhibited, and
depressed behaviours that more centrally affect the child’s internal psychological
environment rather than the external world.”3
• Bundling: combining two or more services in a single programme, with the goal of
maintaining or enhancing the benefits of existing services and gaining additional benefits
from the new intervention.4
• Developmental potential: ability to think, learn, remember, relate, and articulate ideas
appropriate to age and level of maturity; an estimated 39% of the world’s children under age
five years do not attain this potential.5
1 Richter L. The importance of caregiver-child interactions for the survival and health development of young children: a review. Geneva: World Health Organization; 2004. 2 Stern DN. The interpersonal world of the infant: a view from psychoanalysis and developmental psychology. New York: Basic Books; 1985, p.
142; cited in Richter L. 2004. 3 Liu J. Childhood externalizing behavior: theory and implications. Journal of Child and Adolescent Psychiatric Nursing. 2004;17(3): 93–103. 4 Alderman H. Early childhood development: does bundling services for young children and their families reduce costs? Brookings: Education
Plus Development; 2015. 5 Grantham-McGregor S. et al. Developmental potential in the first 5 years for children in developing countries. Lancet. 2007; 369:9555:60-70.

70 | P a g e
• Dialogic book-sharing (dialogic reading): stimulation package designed according to the
following three principles: (a) use of techniques by the parent to encourage the child to talk
about pictured materials; (b) informative feedback by incorporating expansions, corrective
modelling, and other forms that highlight differences between what the child has said and
what he/she might have said; and (c) an adaptive parent sensitive to the child’s developing
abilities.1
• Depression: an affective disorder characterized by a sense of inadequacy, feelings of
despondency or hopelessness, a decrease in activity and/or reactivity, pessimism, sadness,
irritability, changes in appetite and sleep patterns, and poor concentration.
• Early childhood development (ECD): refers to the physical, socioemotional, cognitive, and
motor development between 0-8 years of age.
• Emotional availability: refers to the ability of the caregiver and child to share a healthy
emotional connection and the quality of emotional exchanges between caregivers and
children. Encompasses both emotional signaling and emotional understanding, as well as the
emotional accessibility of one to the other. The emotionally available dyad is one in which
both mother and infant recognize the other partner’s signals and affirm them.2
• Home visiting programmes: involve visits by nurses to parents and children in their homes
to prevent child maltreatment and promote positive infant, child and parental development by
providing support, education and information.3
• Integration: same as bundling; combining two or more services in a single intervention,
with the goal of maintaining or enhancing the benefits of existing services and gaining some
benefit from the new programme.
• Interventions: attempts to influence or change the course of events by providing care or
information or otherwise manipulating a situation.
• Macronutrients: include carbohydrates, proteins, and fats. Consumed in relatively large
quantities and are important to child linear growth and mental development.4
• Malnutrition: results from deficiencies, excesses or imbalances in the consumption of
macro- and/or micronutrients. Malnutrition may be an outcome of food insecurity, or it may
relate to non-food factors, such as inadequate care practices for children, insufficient health
services, and/or an unhealthy environment.5
o Pediatric malnutrition (undernutrition): an imbalance between nutrient
requirements and intake that results in cumulative deficits of energy, protein or
1 Mol SE, et al. Added value of dialogic parent-child book readings: a meta-Analysis. Early Education and Development. 2008;19:1, 7-26. 2 Saunders H, Kraus A, Barone L, Biringen Z. Emotional availability: theory, research, and intervention. Front Psychol. 2015;6:1069; Bornstein
MH et al. Emotional relationships between mothers and infants: knowns, unknowns, and unknown unknowns. Development and Psychopathology. 2012;24:1, 113-23. 3 World Health Organization. 4 Aboud F & Yousafzai AK. In Black RE, Laxminarayan R, Temmerman M et al., editors.Washington (DC): International Bank for Reconstruction and Development/The World Bank; 2016 Apr 5. 5 Food and Agriculture Organization of the United Nations.
71 | P a g e
micronutrients that may negatively affect growth, development and other relevant
outcomes.1
• (Child) Maltreatment: the abuse and neglect of children under 18 years of age. It includes
all types of physical and/or emotional ill-treatment, sexual abuse, neglect, negligence and
commercial or other exploitation, which results in actual or potential harm to the child’s
health, survival, development or dignity in the context of a relationship of responsibility, trust
or power.2
• Maternal-infant bonding: While widely defined in the literature, a general definition
describes maternal–infant bonding as a process that includes the emotional tie of a mother to
her infant, occurring in the first week or year of an infant's life and that is influenced by
signals and cues from the child as well as the maternal-driven processes.3
• Micronutrients: minerals and vitamins that enable the body to produce enzymes, hormones
and other substances essential for proper growth and development. Consumed in minuscule
amounts, but the consequences of their absence are severe. Iodine, vitamin A and iron are
most important in global public health terms; their lack represents a major threat to the health
and development of populations the world over, particularly children and pregnant women in
low-income countries.4
• Nurturing care: characterized by a caregiving environment that is sensitive to children’s
health and nutritional needs, responsive, emotionally supportive, and developmentally
stimulating and appropriate, with opportunities for play and exploration and protection from
adversities.5
• Nutritional supplementation:
o Multiple vitamin and mineral supplements: multiple micronutrients constitute the
common nutritional supplement provided to young children. Children are often
deficient in many minerals, such as iron and zinc, as well as vitamins. All are critical
for health and growth, and their effects on mental development are becoming clear.9
• Play: a central component of early childhood stimulation and quality parent-child
interactions that is essential to the social, emotional, cognitive, and physical wellbeing of
children beginning in early childhood.6
o Child-led (-driven, -centred) play: play that is directed by the child (though
caregivers may observe or join in), in which children are able to practice decision-
making skills, move at their own pace, and discover their own areas of interest.7
1 Becker et al. Consensus statement of the Academy of Nutrition and Dietetics/American Society for Parenteral and Enteral Nutrition: indicators
recommended for the identification and documentation of pediatric malnutrition (undernutrition). 2015. 2 World Health Organization. 3 Bicking Kinsey C, Hupcey JE . State of the science of maternal-infant bonding: a principle-based concept analysis. Midwifery. 2013;29(12),
10.1016/j.midw.2012.12.019. http://doi.org/10.1016/j.midw.2012.12.019. 4 World Health Organization. 5 Black MM et al. Early childhood development coming of age: science through the life course. Lancet. 2017;389(10064):77-90. 6 Milteer RM. The importance of play in promoting healthy child development and maintaining strong parent-child bond: focus on children in poverty. Pediatrics. 2012;129(1). 7 Ginsburg et al. The importance of play in promoting healthy child development and maintaining strong parent-child bonds. Pediatrics. 2007;19(1).
72 | P a g e
• Positive parenting: consists of five core principles for parents to promote social competence
and emotional self-regulation in children: (1) ensuring a safe, engaging environment, (2)
promoting a positive learning environment, (3) using assertive discipline, (4) maintaining
reasonable expectations, and (5) taking care of oneself as a parent. The emphasis is on
parents learning how to apply these skills to different behavioural, emotional and
developmental issues in children, ranging from common child-rearing challenges (e.g.
toileting, mealtime behaviour, bedtime, behaviour in public) to more intense challenges (e.g.
child aggressive behaviour, fears and anxiety, ADHD difficulties).1
• Psychosocial Stimulation: refers to an external object or event that elicits a physiological
and psychological response in the child.
• Responsiveness: the capacity of the caregiver to respond contingently and appropriately to
the infant’s signals.
• Scaffolding: a concept derived from Vygotsky’s theory of mediated learning, scaffolding is
the process by which someone organizes an event that is unfamiliar or beyond a learner’s
ability in order to assist the learner in carrying out that event.
• Sensitivity: the capacity of the caregiver to be aware of the infant and aware of the infant’s
acts and vocalizations as signals communicating needs and wants.
• Sensitive Discipline: parents’ ability to take into account the child’s perspective and signals
when discipline is required.2
• Stunting: a commonly used indicator of chronic undernutrition, defined as more than two
standard deviations below the age- and gender-specific norm.
• Temperament: an individual’s characteristic mode of responding emotionally and
behaviourally to environmental events. Temperament includes the dimensions of irritability,
activity level, fearfulness and sociability.
• Violent Discipline: actions taken by a parent or caregiver that are intended to cause a child
physical pain or emotional distress as a way to correct behaviour and act as a deterrent.
Violent discipline can take two forms: psychological aggression and physical, or corporal,
punishment. The former includes shouting, yelling and screaming at the child, and addressing
her or him with offensive names. Physical or corporal punishment comprises actions
intended to cause the child physical pain or discomfort but not injuries. Minor physical
punishment includes shaking the child and slapping or hitting him or her on the hand, arm,
leg or bottom. Severe physical punishment includes hitting the child on the face, head or ears,
or hitting the child hard or repeatedly.3
1 Prinz RJ, Sanders MR, Shapiro CJ, Whitaker DJ, Lutzker JR Population-based prevention of child maltreatment: The U.S. Triple P System Population Trial. Prevention Science. 2009;10:1–12. 2 Van Zeijl J et al. Attachment-based intervention for enhancing sensitive discipline in mothers of 1- to 3-year-old children at risk for
externalizing behavior problems: a randomized controlled trial. Journal of Consulting and Clinical Psychology. 2006;74(6): 994-1005. 3 UNICEF.

73 | P a g e
Behaviour Change Techniques
• Information: provision of new information about the link between behaviour and child
development, causes and consequences, and instruction on how to perform the behaviour.1
• Materials: materials that beneficiary families would not normally possess or buy on their
own are provided in order to facilitate behaviour change.
• Media: use of any form of media to bring about behaviour change, including TV
advertisements, flashcards, and organization of role plays and dramas.
• Performance: includes modelling or providing demonstrations, actual rehearsal or practice
of a targeted behaviour in the intervention setting, providing feedback on performance,
contingent rewards, and/or identification of cues to action.
• Problem Solving: includes identifying facilitators and barriers of a targeted behaviour, as
well as solutions to overcoming barriers.
• Social Support: leveraging support from various members of the society/community to
bring about behaviour change; includes motivating peers, family members or authority
figures to encourage parents to engage in behaviour change.
1 Briscoe & Aboud. Behaviour change communication targeting four health behaviours in developing countries: a review of change techniques. Social Science and Medicine. 2012;75(4); 612-21; Aboud FE, Yousafzai AK. Global health and development in early childhood. Annual Review
of Psychology. 2015; 66(1): 433-57.
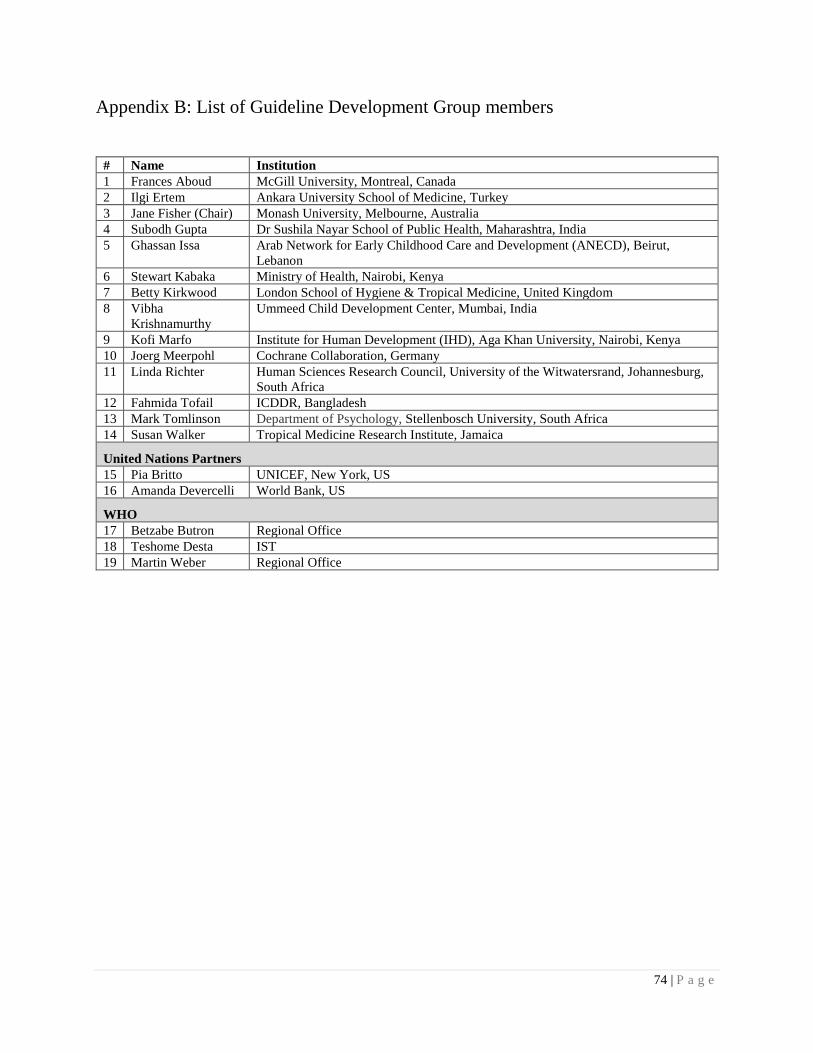
74 | P a g e
Appendix B: List of Guideline Development Group members
# Name Institution
1 Frances Aboud McGill University, Montreal, Canada
2 Ilgi Ertem Ankara University School of Medicine, Turkey
3 Jane Fisher (Chair) Monash University, Melbourne, Australia
4 Subodh Gupta Dr Sushila Nayar School of Public Health, Maharashtra, India
5 Ghassan Issa Arab Network for Early Childhood Care and Development (ANECD), Beirut,
Lebanon
6 Stewart Kabaka Ministry of Health, Nairobi, Kenya
7 Betty Kirkwood London School of Hygiene & Tropical Medicine, United Kingdom
8 Vibha
Krishnamurthy
Ummeed Child Development Center, Mumbai, India
9 Kofi Marfo Institute for Human Development (IHD), Aga Khan University, Nairobi, Kenya
10 Joerg Meerpohl Cochrane Collaboration, Germany
11 Linda Richter Human Sciences Research Council, University of the Witwatersrand, Johannesburg,
South Africa
12 Fahmida Tofail ICDDR, Bangladesh
13 Mark Tomlinson Department of Psychology, Stellenbosch University, South Africa
14 Susan Walker Tropical Medicine Research Institute, Jamaica
United Nations Partners
15 Pia Britto UNICEF, New York, US
16 Amanda Devercelli World Bank, US
WHO
17 Betzabe Butron Regional Office
18 Teshome Desta IST
19 Martin Weber Regional Office
75 | P a g e
Appendix C: Summary of interventions for all included studies in the systematic
reviews
See PDF supplement - Appendix C Jeong, Franchett, Yousafzai.
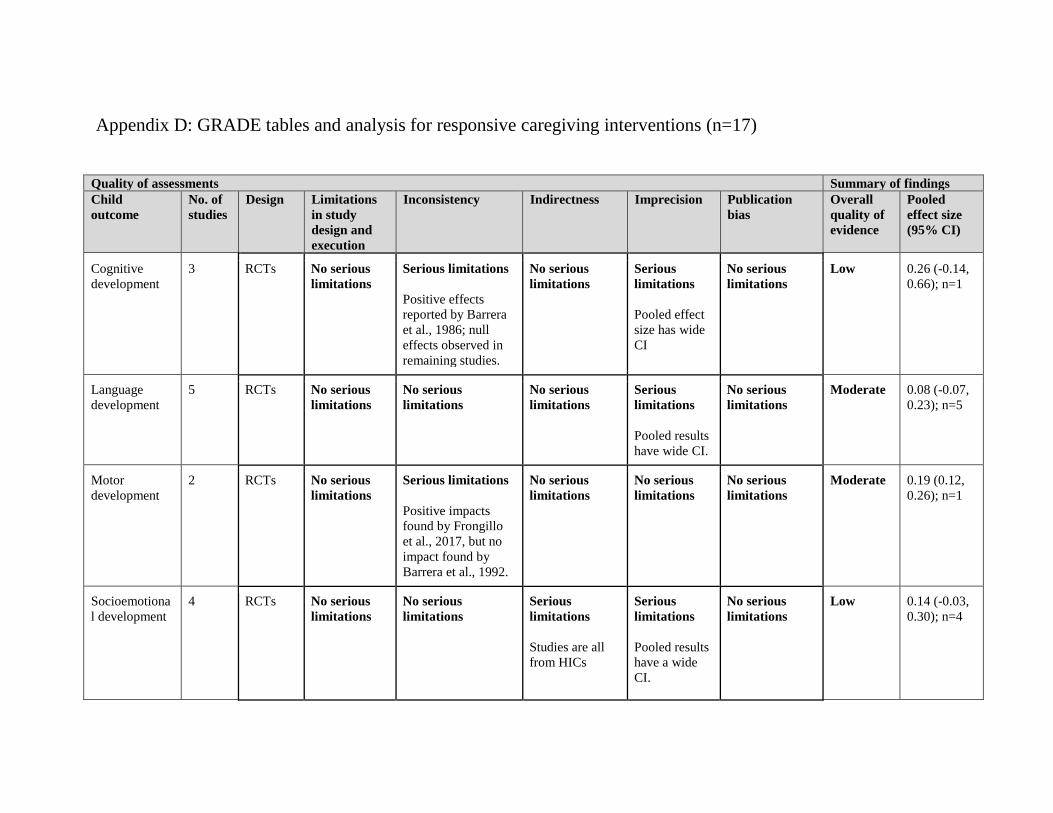
Appendix D: GRADE tables and analysis for responsive caregiving interventions (n=17)
Quality of assessments Summary of findings
Child
outcome
No. of
studies
Design Limitations
in study
design and
execution
Inconsistency Indirectness Imprecision Publication
bias
Overall
quality of
evidence
Pooled
effect size
(95% CI)
Cognitive
development
3 RCTs No serious
limitations
Serious limitations
Positive effects
reported by Barrera
et al., 1986; null
effects observed in
remaining studies.
No serious
limitations
Serious
limitations
Pooled effect
size has wide
CI
No serious
limitations
Low 0.26 (-0.14,
0.66); n=1
Language
development
5 RCTs No serious
limitations
No serious
limitations
No serious
limitations
Serious
limitations
Pooled results
have wide CI.
No serious
limitations
Moderate 0.08 (-0.07,
0.23); n=5
Motor
development
2 RCTs No serious
limitations
Serious limitations
Positive impacts
found by Frongillo
et al., 2017, but no
impact found by
Barrera et al., 1992.
No serious
limitations
No serious
limitations
No serious
limitations
Moderate 0.19 (0.12,
0.26); n=1
Socioemotiona
l development
4 RCTs No serious
limitations
No serious
limitations
Serious
limitations
Studies are all
from HICs
Serious
limitations
Pooled results
have a wide
CI.
No serious
limitations
Low 0.14 (-0.03,
0.30); n=4

77 | P a g e
Behaviour
problems
7 RCTs No serious
limitations
No serious
limitations
Serious
limitations
Studies are all
from HICs.
Serious
limitations
Pooled results
have a wide
CI.
No serious
limitations
Low -0.14 (-0.29,
0.002); n=7
Attachment
outcomes
7 RCTs No serious
limitations
Serious limitations
Six studies found
null effects; one
found positive
effects (Cooper et
al., 2009).
No serious
limitations
Serious
limitations
Pooled results
have a wide
CI.
No serious
limitations
Low 0.13 (-0.11,
0.37); n=3
HAZ
1 RCTs No serious
limitations
No serious
limitations
Serious
limitations
This intervention
was a unique
aspect of
responsive
caregiving as it
focused on
responsive
feeding.
No serious
limitations
No serious
limitations
Moderate 0.10 (0.03,
0.16); n=1
WAZ 1 RCTs No serious
limitations
No serious
limitations
Serious
limitations
This intervention
was a unique
aspect of
responsive
caregiving as it
focused on
responsive
feeding.
No serious
limitations
No serious
limitations
Moderate 0.03 (-0.04,
0.10); n=1
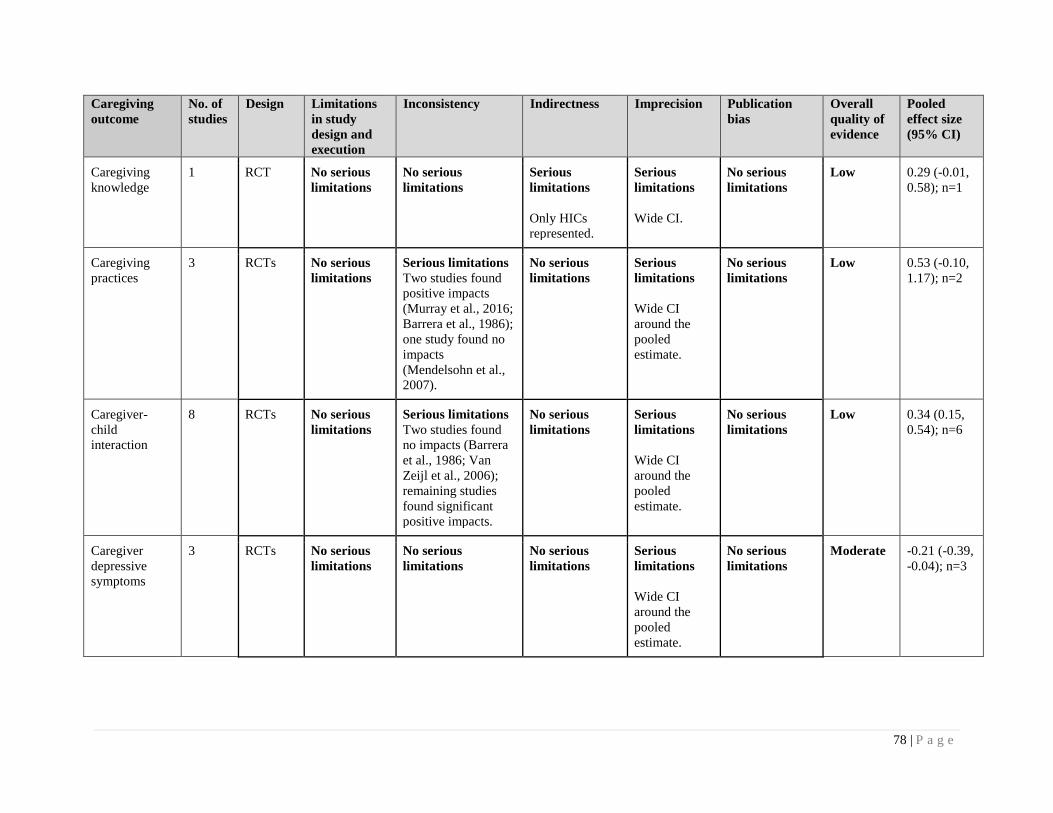
78 | P a g e
Caregiving
outcome
No. of
studies
Design Limitations
in study
design and
execution
Inconsistency Indirectness Imprecision Publication
bias
Overall
quality of
evidence
Pooled
effect size
(95% CI)
Caregiving
knowledge
1 RCT No serious
limitations
No serious
limitations
Serious
limitations
Only HICs
represented.
Serious
limitations
Wide CI.
No serious
limitations
Low 0.29 (-0.01,
0.58); n=1
Caregiving
practices
3 RCTs No serious
limitations
Serious limitations
Two studies found
positive impacts
(Murray et al., 2016;
Barrera et al., 1986);
one study found no
impacts
(Mendelsohn et al.,
2007).
No serious
limitations
Serious
limitations
Wide CI
around the
pooled
estimate.
No serious
limitations
Low 0.53 (-0.10,
1.17); n=2
Caregiver-
child
interaction
8 RCTs No serious
limitations
Serious limitations
Two studies found
no impacts (Barrera
et al., 1986; Van
Zeijl et al., 2006);
remaining studies
found significant
positive impacts.
No serious
limitations
Serious
limitations
Wide CI
around the
pooled
estimate.
No serious
limitations
Low 0.34 (0.15,
0.54); n=6
Caregiver
depressive
symptoms
3 RCTs No serious
limitations
No serious
limitations
No serious
limitations
Serious
limitations
Wide CI
around the
pooled
estimate.
No serious
limitations
Moderate -0.21 (-0.39,
-0.04); n=3
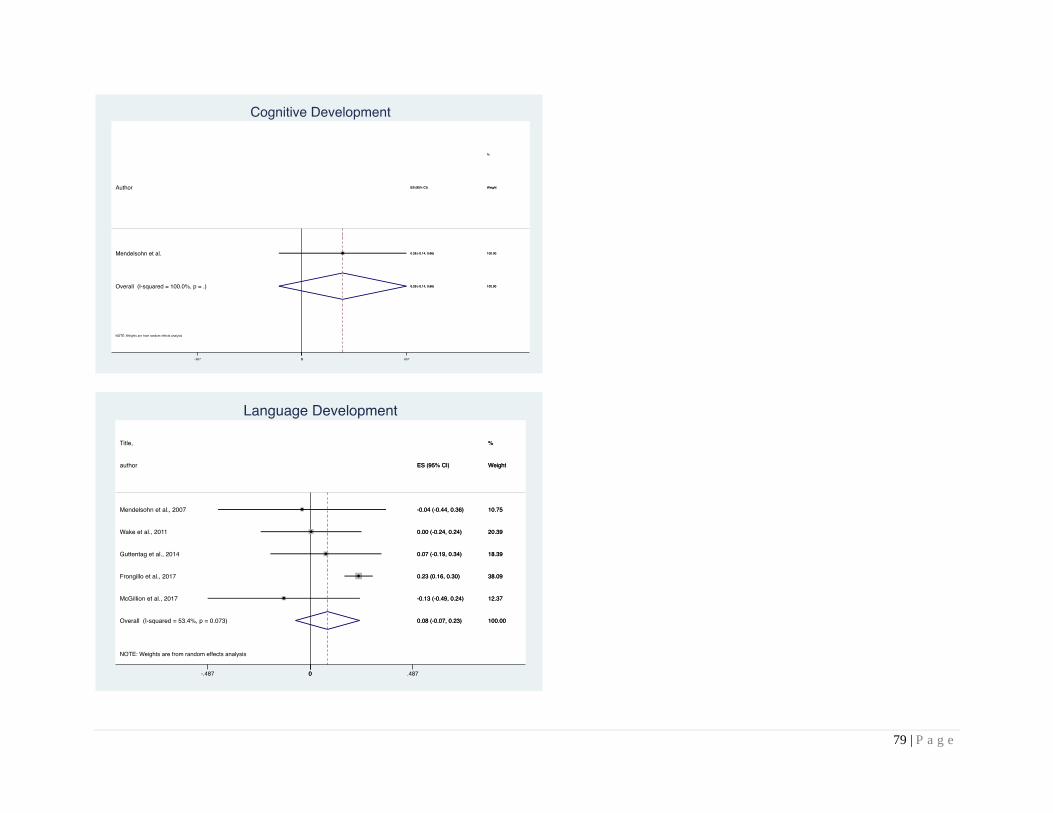
79 | P a g e
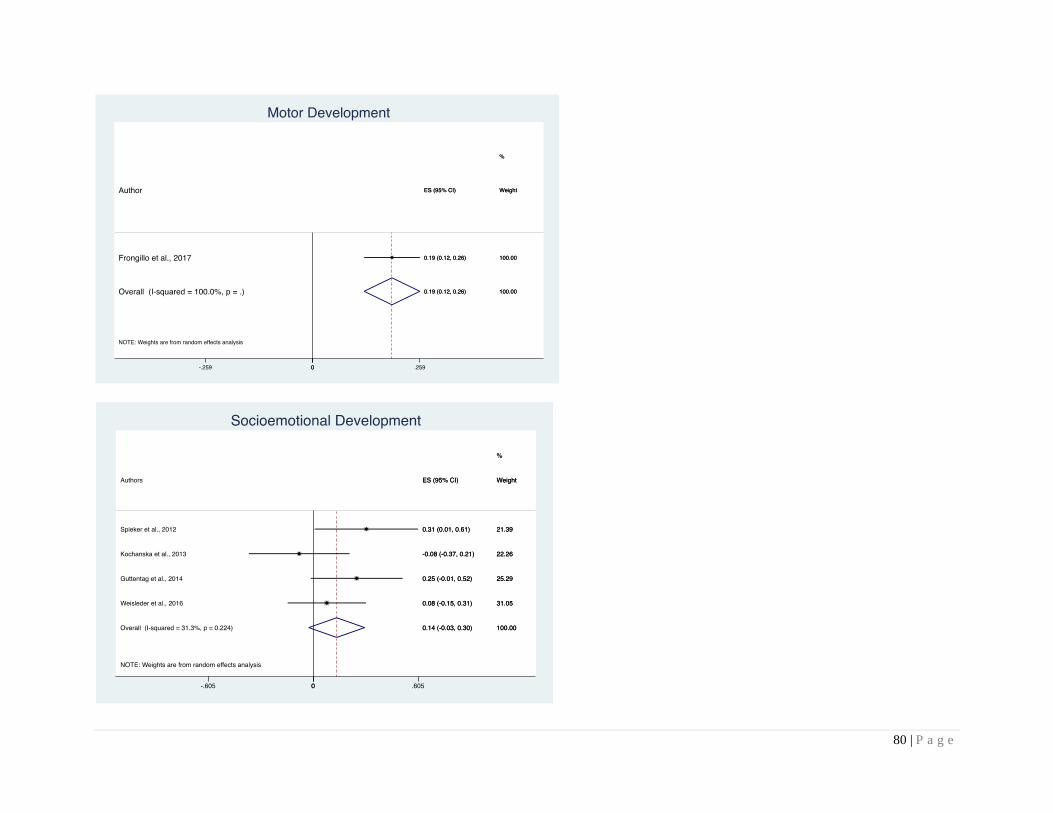
80 | P a g e
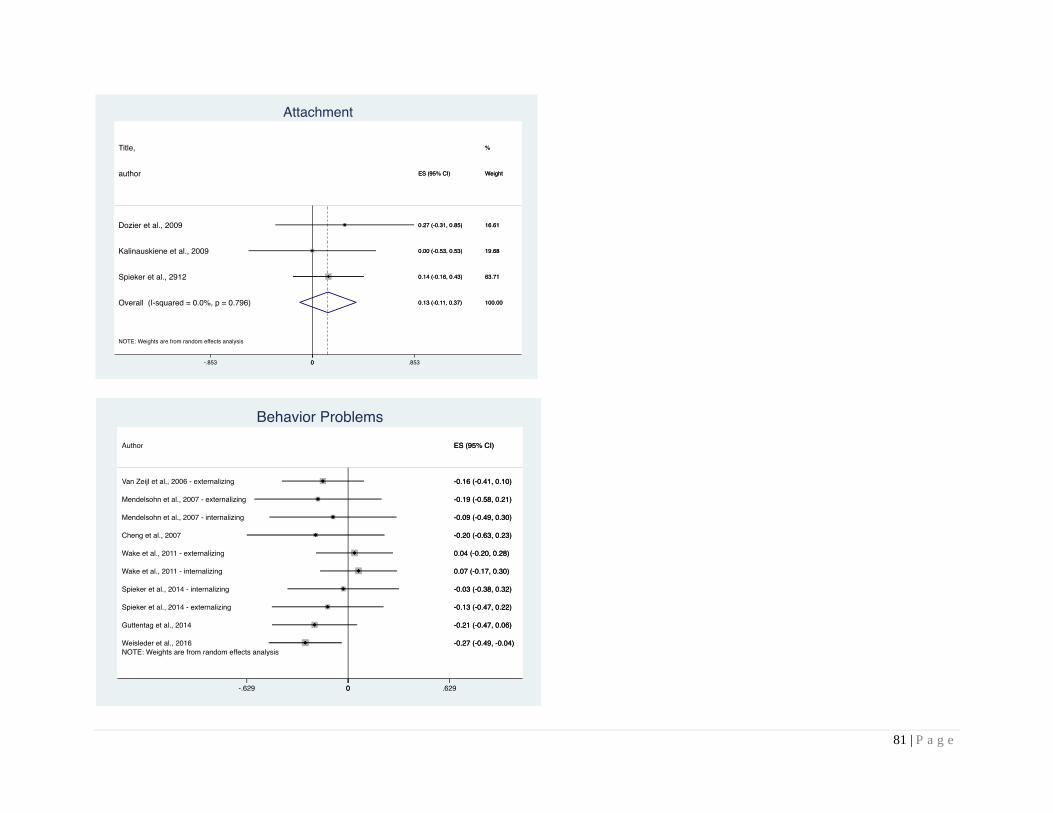
81 | P a g e

82 | P a g e

83 | P a g e
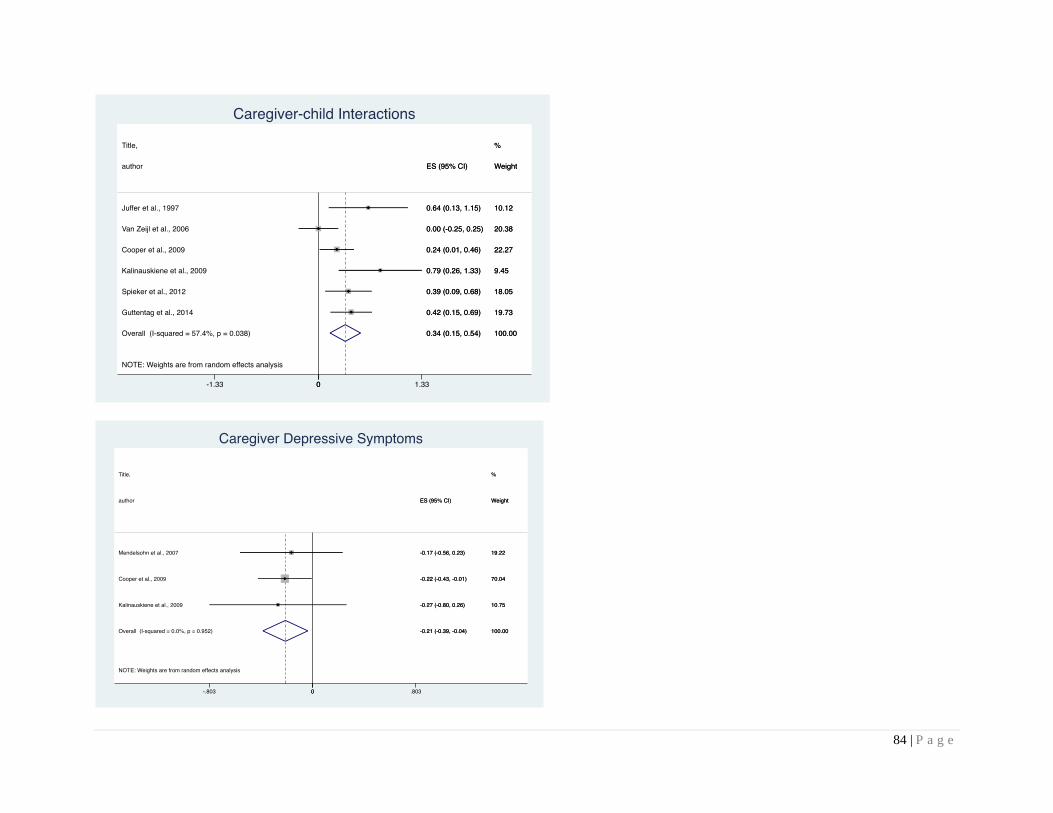
84 | P a g e
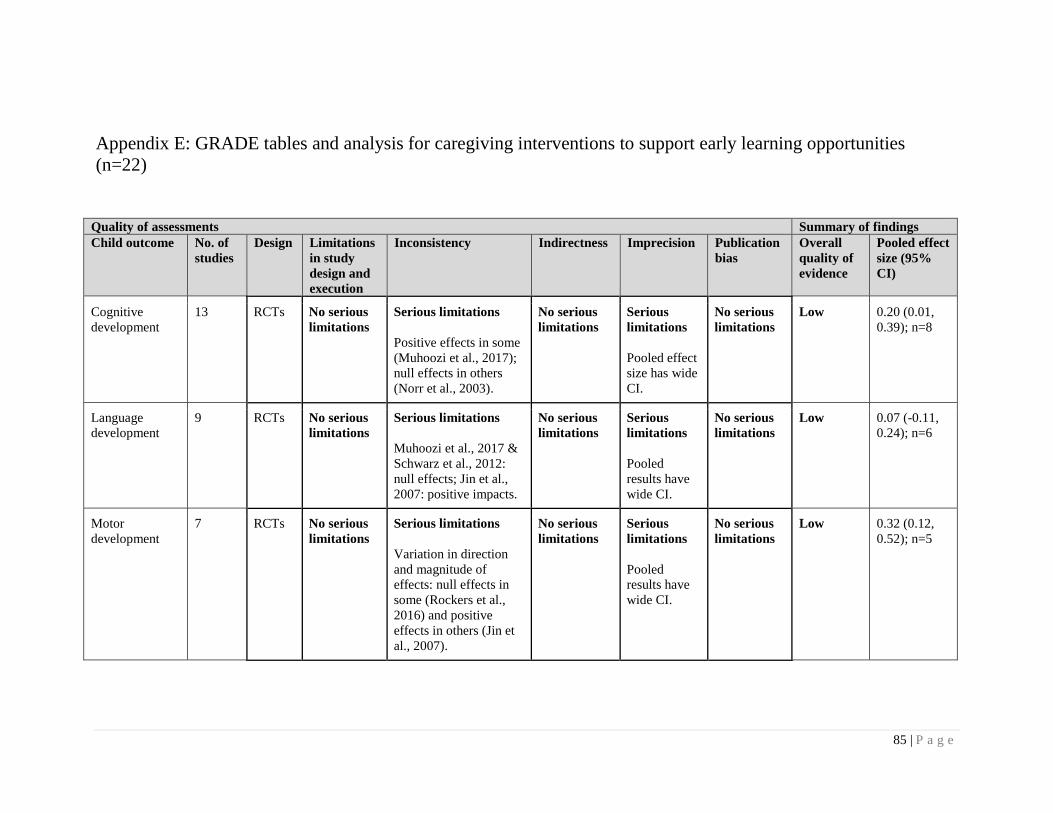
85 | P a g e
Appendix E: GRADE tables and analysis for caregiving interventions to support early learning opportunities
(n=22)
Quality of assessments Summary of findings
Child outcome No. of
studies
Design Limitations
in study
design and
execution
Inconsistency Indirectness Imprecision Publication
bias
Overall
quality of
evidence
Pooled effect
size (95%
CI)
Cognitive
development
13 RCTs No serious
limitations
Serious limitations
Positive effects in some
(Muhoozi et al., 2017);
null effects in others
(Norr et al., 2003).
No serious
limitations
Serious
limitations
Pooled effect
size has wide
CI.
No serious
limitations
Low 0.20 (0.01,
0.39); n=8
Language
development
9 RCTs No serious
limitations
Serious limitations
Muhoozi et al., 2017 &
Schwarz et al., 2012:
null effects; Jin et al.,
2007: positive impacts.
No serious
limitations
Serious
limitations
Pooled
results have
wide CI.
No serious
limitations
Low 0.07 (-0.11,
0.24); n=6
Motor
development
7 RCTs No serious
limitations
Serious limitations
Variation in direction
and magnitude of
effects: null effects in
some (Rockers et al.,
2016) and positive
effects in others (Jin et
al., 2007).
No serious
limitations
Serious
limitations
Pooled
results have
wide CI.
No serious
limitations
Low 0.32 (0.12,
0.52); n=5
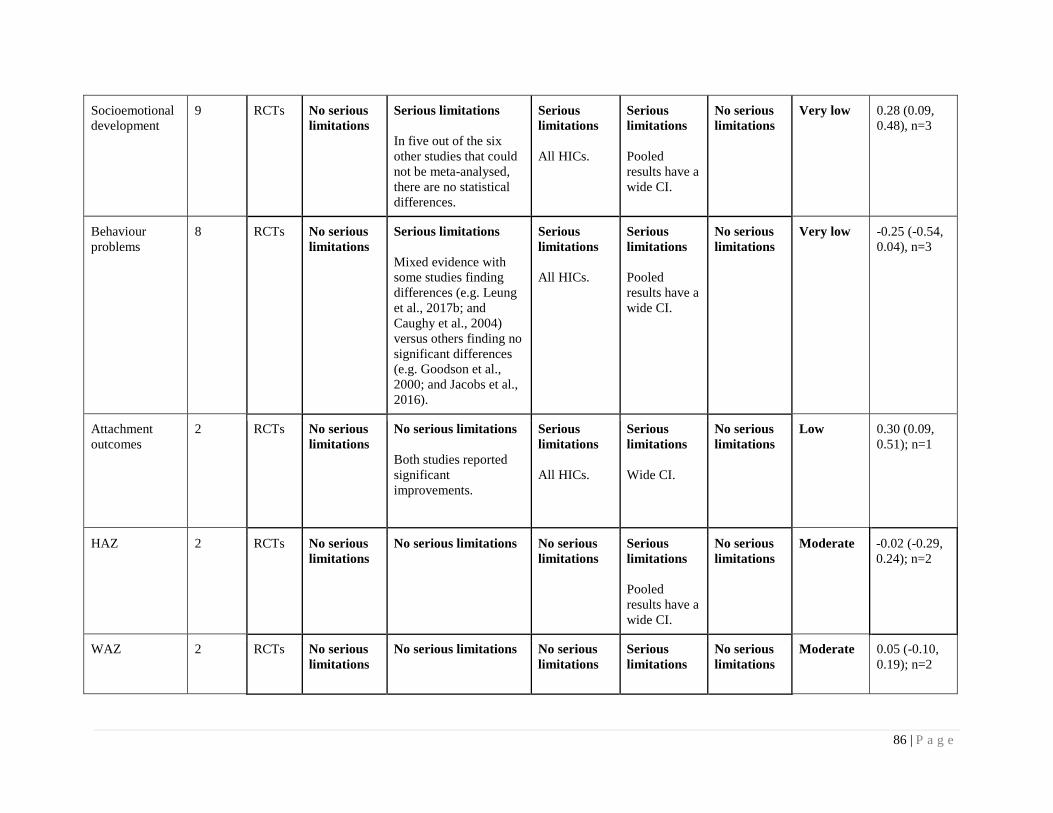
86 | P a g e
Socioemotional
development
9 RCTs No serious
limitations
Serious limitations
In five out of the six
other studies that could
not be meta-analysed,
there are no statistical
differences.
Serious
limitations
All HICs.
Serious
limitations
Pooled
results have a
wide CI.
No serious
limitations
Very low 0.28 (0.09,
0.48), n=3
Behaviour
problems
8 RCTs No serious
limitations
Serious limitations
Mixed evidence with
some studies finding
differences (e.g. Leung
et al., 2017b; and
Caughy et al., 2004)
versus others finding no
significant differences
(e.g. Goodson et al.,
2000; and Jacobs et al.,
2016).
Serious
limitations
All HICs.
Serious
limitations
Pooled
results have a
wide CI.
No serious
limitations
Very low -0.25 (-0.54,
0.04), n=3
Attachment
outcomes
2 RCTs No serious
limitations
No serious limitations
Both studies reported
significant
improvements.
Serious
limitations
All HICs.
Serious
limitations
Wide CI.
No serious
limitations
Low 0.30 (0.09,
0.51); n=1
HAZ
2 RCTs No serious
limitations
No serious limitations
No serious
limitations
Serious
limitations
Pooled
results have a
wide CI.
No serious
limitations
Moderate -0.02 (-0.29,
0.24); n=2
WAZ 2 RCTs No serious
limitations
No serious limitations
No serious
limitations
Serious
limitations
No serious
limitations
Moderate 0.05 (-0.10,
0.19); n=2
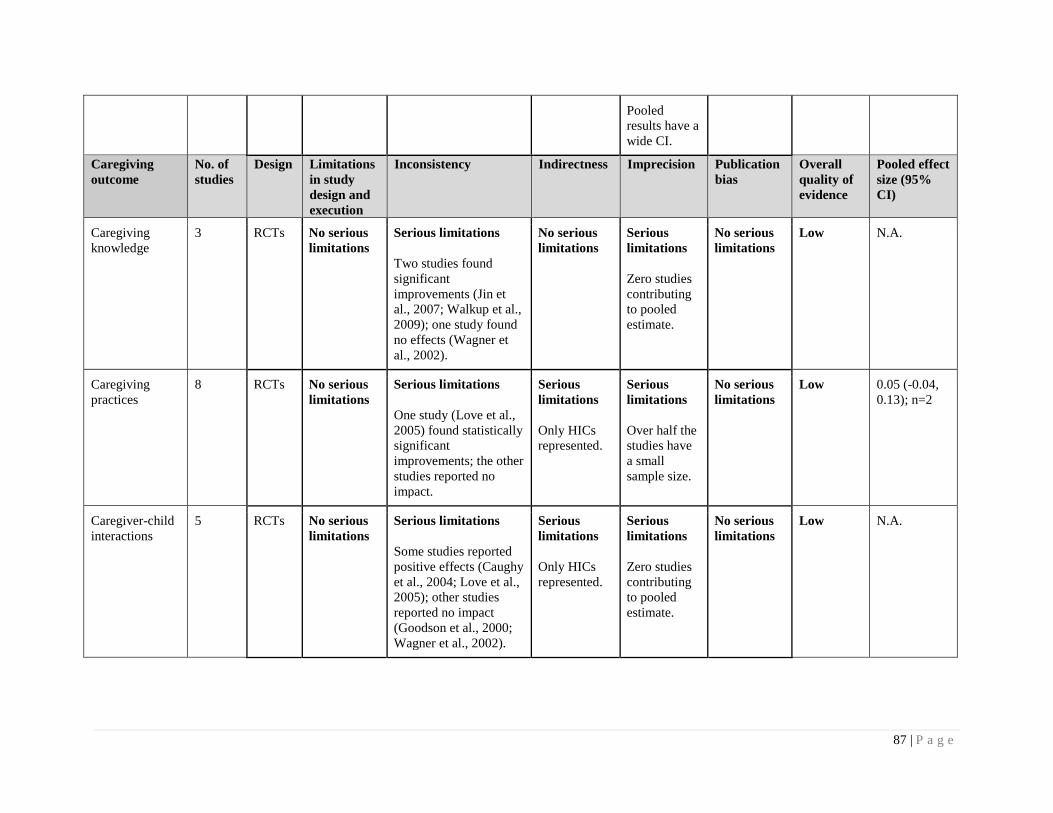
87 | P a g e
Pooled
results have a
wide CI.
Caregiving
outcome
No. of
studies
Design Limitations
in study
design and
execution
Inconsistency Indirectness Imprecision Publication
bias
Overall
quality of
evidence
Pooled effect
size (95%
CI)
Caregiving
knowledge
3 RCTs No serious
limitations
Serious limitations
Two studies found
significant
improvements (Jin et
al., 2007; Walkup et al.,
2009); one study found
no effects (Wagner et
al., 2002).
No serious
limitations
Serious
limitations
Zero studies
contributing
to pooled
estimate.
No serious
limitations
Low N.A.
Caregiving
practices
8 RCTs No serious
limitations
Serious limitations
One study (Love et al.,
2005) found statistically
significant
improvements; the other
studies reported no
impact.
Serious
limitations
Only HICs
represented.
Serious
limitations
Over half the
studies have
a small
sample size.
No serious
limitations
Low 0.05 (-0.04,
0.13); n=2
Caregiver-child
interactions
5 RCTs No serious
limitations
Serious limitations
Some studies reported
positive effects (Caughy
et al., 2004; Love et al.,
2005); other studies
reported no impact
(Goodson et al., 2000;
Wagner et al., 2002).
Serious
limitations
Only HICs
represented.
Serious
limitations
Zero studies
contributing
to pooled
estimate.
No serious
limitations
Low N.A.
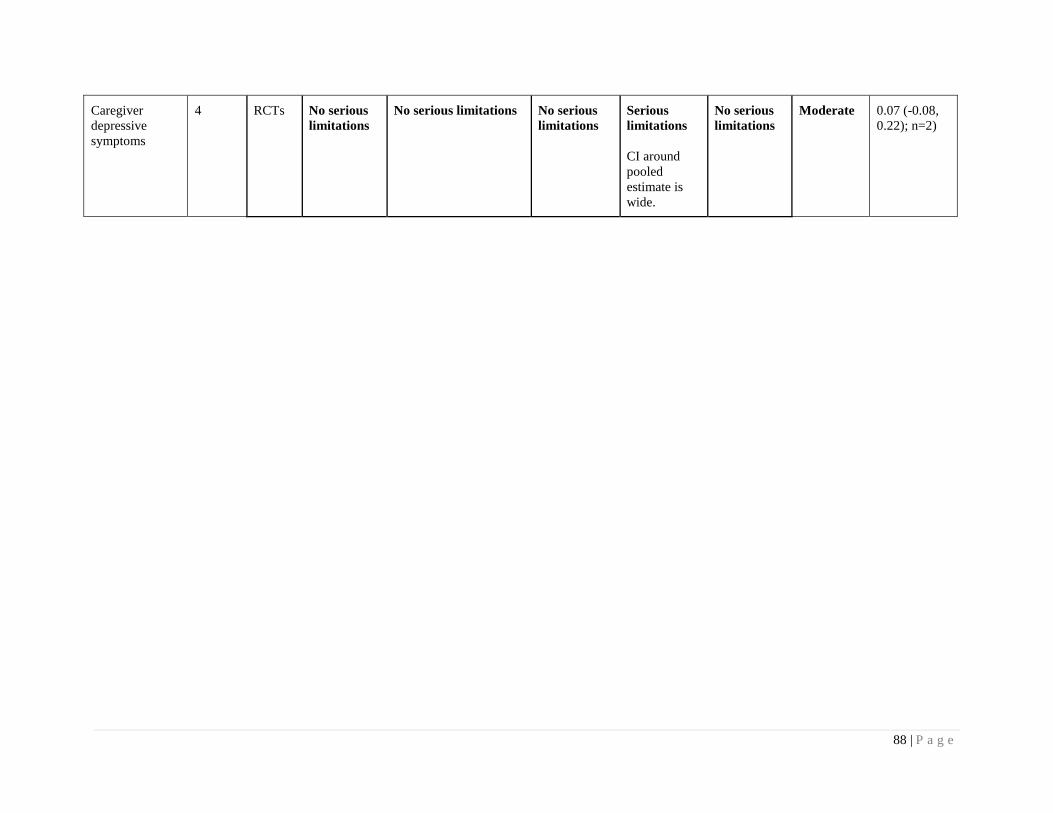
88 | P a g e
Caregiver
depressive
symptoms
4 RCTs No serious
limitations
No serious limitations No serious
limitations
Serious
limitations
CI around
pooled
estimate is
wide.
No serious
limitations
Moderate 0.07 (-0.08,
0.22); n=2)
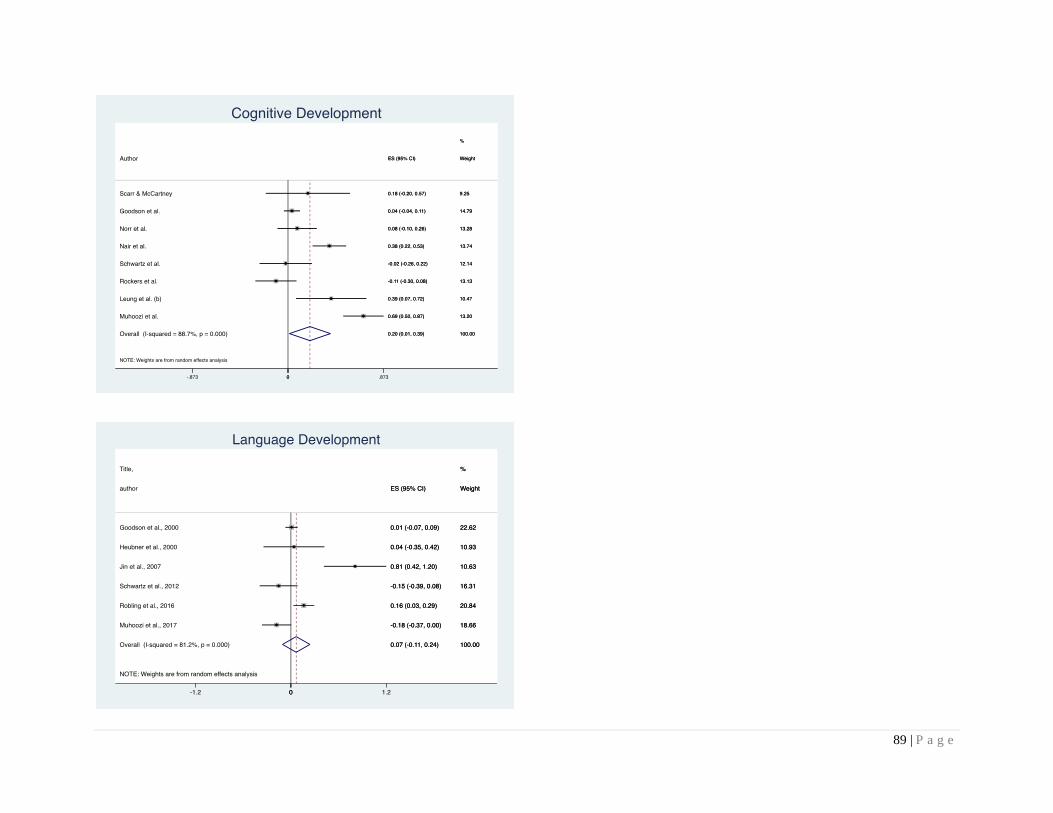
89 | P a g e

90 | P a g e

91 | P a g e

92 | P a g e
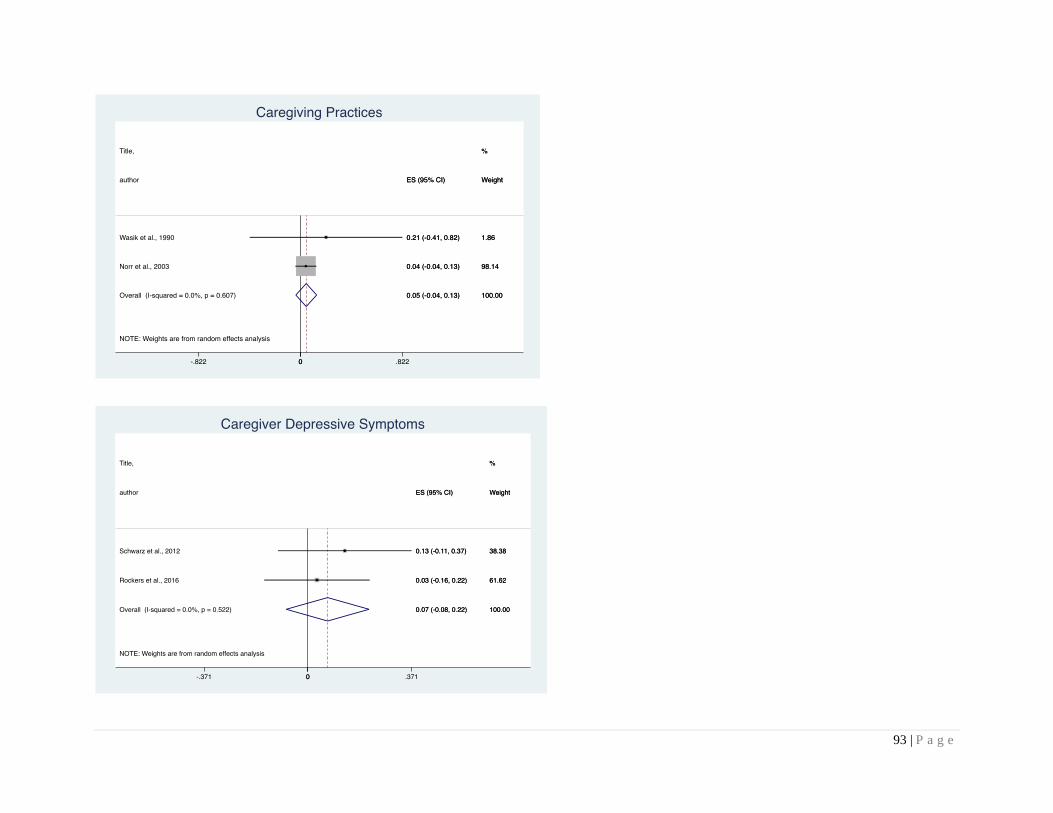
93 | P a g e

94 | P a g e
Appendix F: GRADE tables and analysis for combined responsive caregiving and the promotion of early learning
interventions (n=42)
Quality of assessments Summary of findings
Child outcome No. of
studies
Design Limitations
in study
design and
execution
Inconsistency Indirectness Imprecision Publication
bias
Overall
quality of
evidence
Pooled effect
size (95%
CI)
Cognitive
development
36 RCTs No serious
limitations
Serious limitations
Variation in direction
and magnitude of
effects: some studies
have positive impacts
(Aboud et al., 2013);
others had null effects
(Leung et al., 2017a;
Drotar et al., 2008).
No serious
limitations
Serious
limitations
Pooled effect
size has wide
CI.
No serious
limitations
Low 0.45 (0.25,
0.65); n=20
Language
development
17 RCTs No serious
limitations
Serious limitations
Variation in direction
and magnitude of
effects: some studies
have positive impacts
(Powell et al., 2004;
Vally et al., 2015);
others had null effects
(Goldfeld et al., 2011).
No serious
limitations
Serious
limitations
Pooled
results have
wide CI.
No serious
limitations
Low 0.38 (0.16,
0.60); n=14
Motor
development
18 RCTs No serious
limitations
Serious limitations
Some studies found
positive impacts
(Yousafzai et al., 2014);
others reported no
impacts (Heinicke et al.,
1999).
No serious
limitations
Serious
limitations
Pooled
results have
wide CI.
No serious
limitations
Low 0.25 (0.09,
0.40); n=13

95 | P a g e
Socioemotional
development
4 RCTs No serious
limitations
No serious limitations
No serious
limitations
Serious
limitations
Pooled
results have a
wide CI.
No serious
limitations
Moderate 0.06 (-0.18,
0.28); n=2
Behaviour
problems
7 RCTs No serious
limitations
No serious limitations Serious
limitations
All HICs.
Serious
limitations
Pooled
results have a
wide CI.
No serious
limitations
Low -0.18 (-0.40,
0.04); n=2
Attachment
outcomes
2 RCTs No serious
limitations
No serious limitations
All studies found
positive impacts on
attachment outcomes.
No serious
limitations
Serious
limitations
Zero studies
contributing
to pooled
estimate.
No serious
limitations
Moderate N.A.
HAZ
8 RCTs No serious
limitations
No serious limitations
No serious
limitations
Serious
limitations
Pooled
results have a
wide CI.
No serious
limitations
Moderate -0.04 (-0.15,
0.07); n=8
WAZ 6 RCTs No serious
limitations
No serious limitations
No serious
limitations
No serious
limitations
No serious
limitations
High 0.02 (-0.07,
0.11); n=6
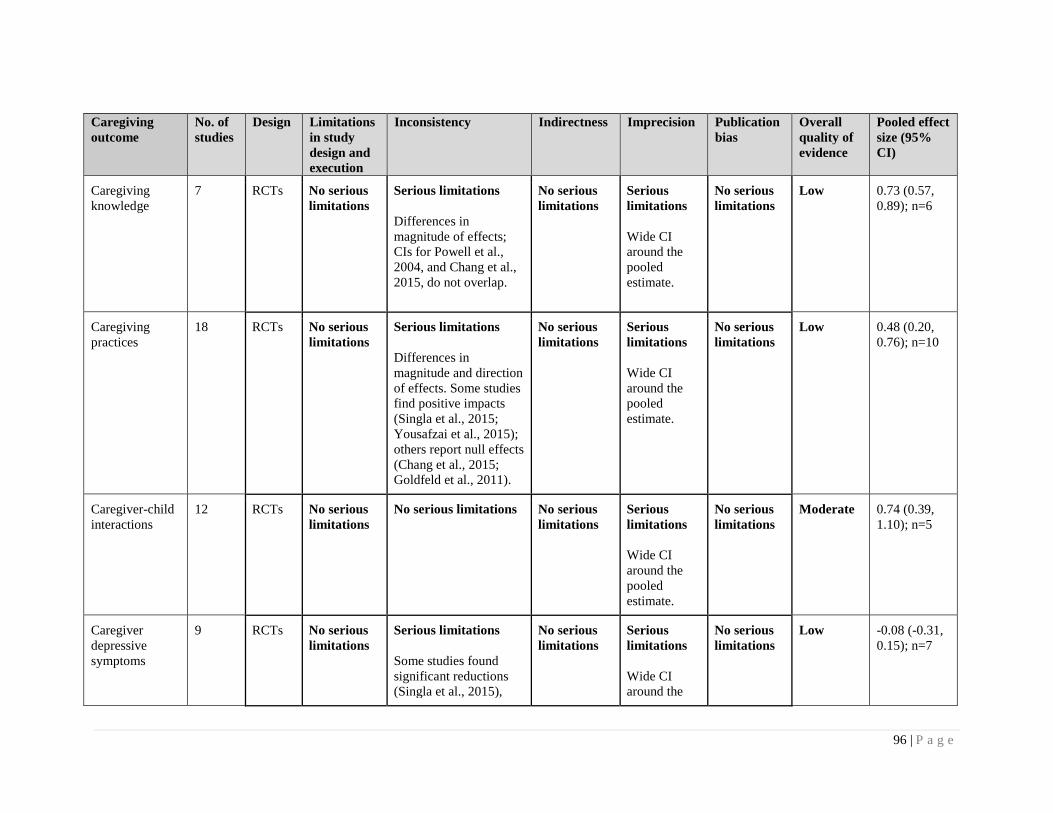
96 | P a g e
Caregiving
outcome
No. of
studies
Design Limitations
in study
design and
execution
Inconsistency Indirectness Imprecision Publication
bias
Overall
quality of
evidence
Pooled effect
size (95%
CI)
Caregiving
knowledge
7 RCTs No serious
limitations
Serious limitations
Differences in
magnitude of effects;
CIs for Powell et al.,
2004, and Chang et al.,
2015, do not overlap.
No serious
limitations
Serious
limitations
Wide CI
around the
pooled
estimate.
No serious
limitations
Low 0.73 (0.57,
0.89); n=6
Caregiving
practices
18 RCTs No serious
limitations
Serious limitations
Differences in
magnitude and direction
of effects. Some studies
find positive impacts
(Singla et al., 2015;
Yousafzai et al., 2015);
others report null effects
(Chang et al., 2015;
Goldfeld et al., 2011).
No serious
limitations
Serious
limitations
Wide CI
around the
pooled
estimate.
No serious
limitations
Low 0.48 (0.20,
0.76); n=10
Caregiver-child
interactions
12 RCTs No serious
limitations
No serious limitations No serious
limitations
Serious
limitations
Wide CI
around the
pooled
estimate.
No serious
limitations
Moderate 0.74 (0.39,
1.10); n=5
Caregiver
depressive
symptoms
9 RCTs No serious
limitations
Serious limitations
Some studies found
significant reductions
(Singla et al., 2015),
No serious
limitations
Serious
limitations
Wide CI
around the
No serious
limitations
Low -0.08 (-0.31,
0.15); n=7
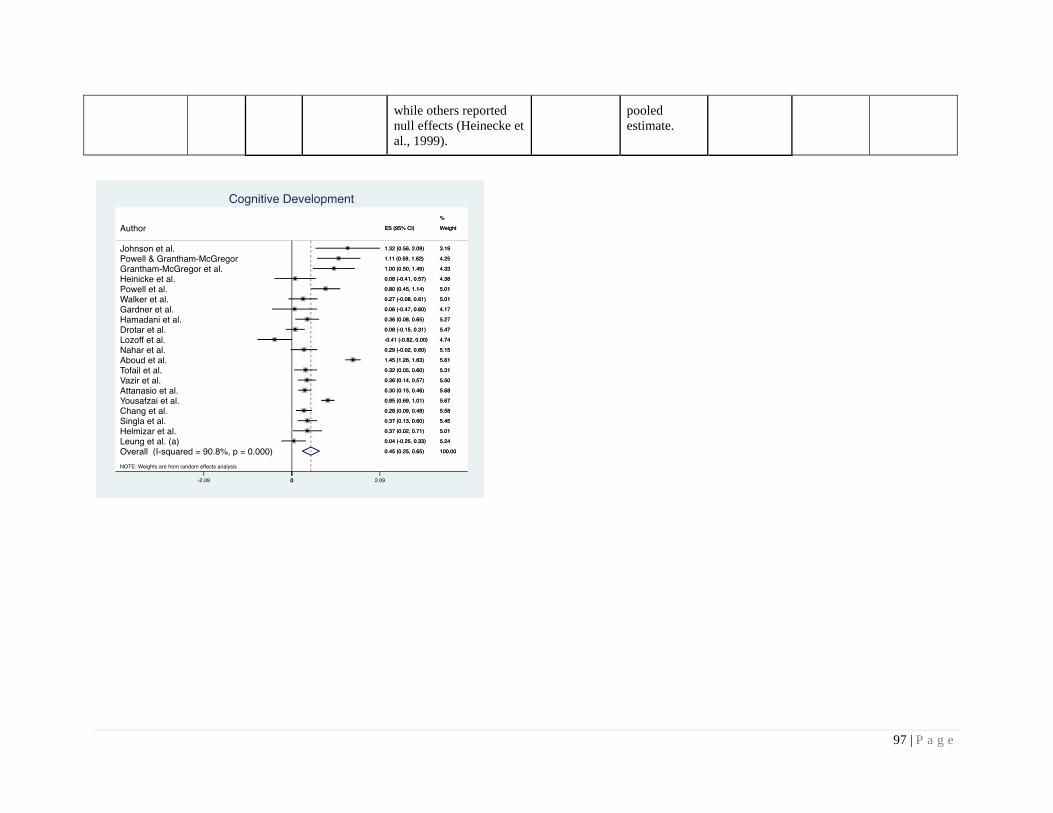
97 | P a g e
while others reported
null effects (Heinecke et
al., 1999).
pooled
estimate.
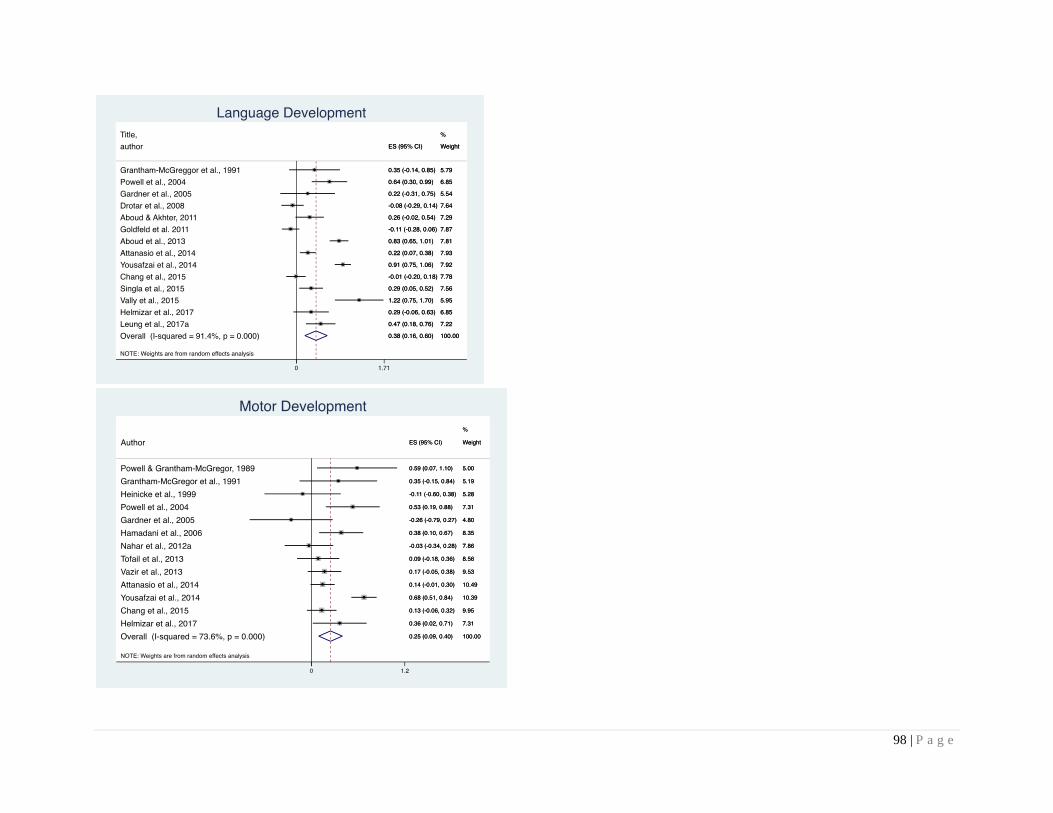
98 | P a g e
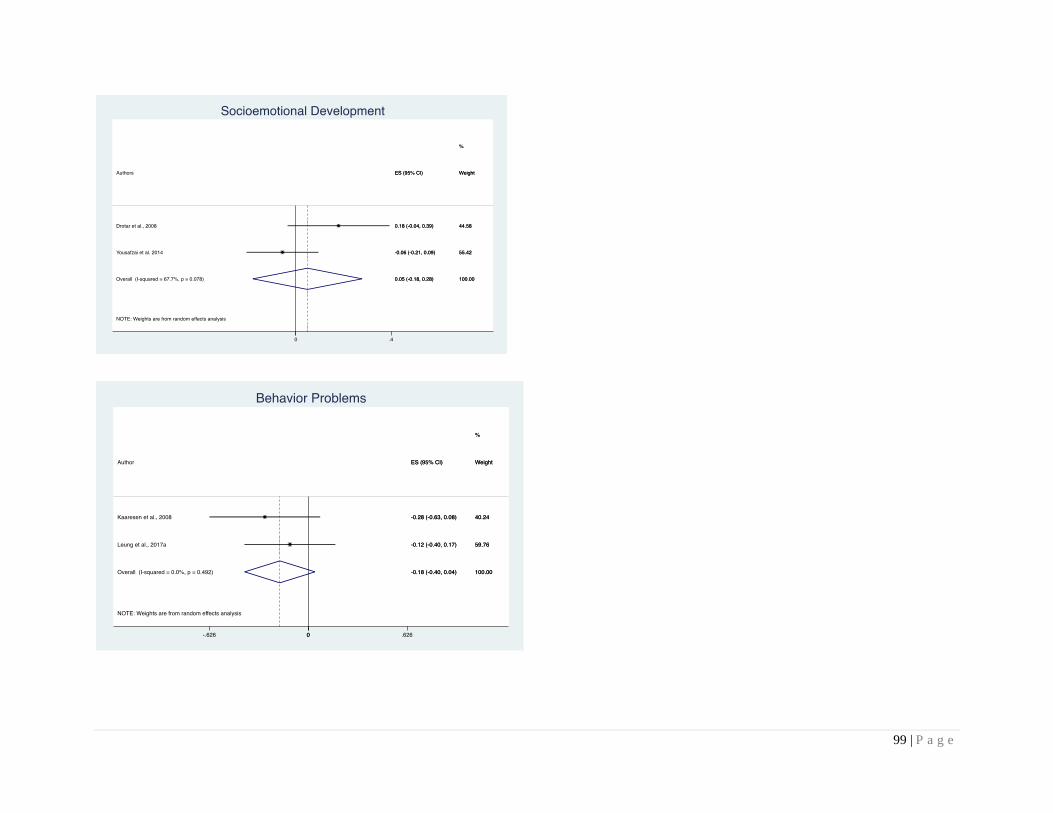
99 | P a g e

100 | P a g e
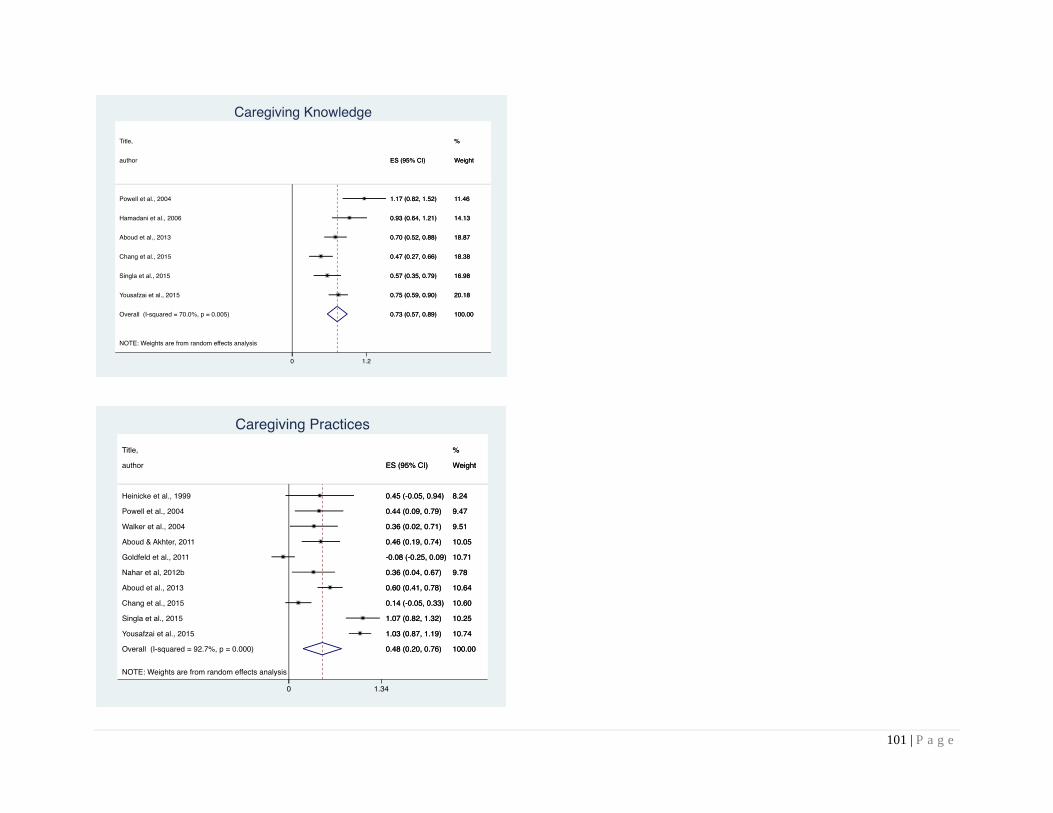
101 | P a g e
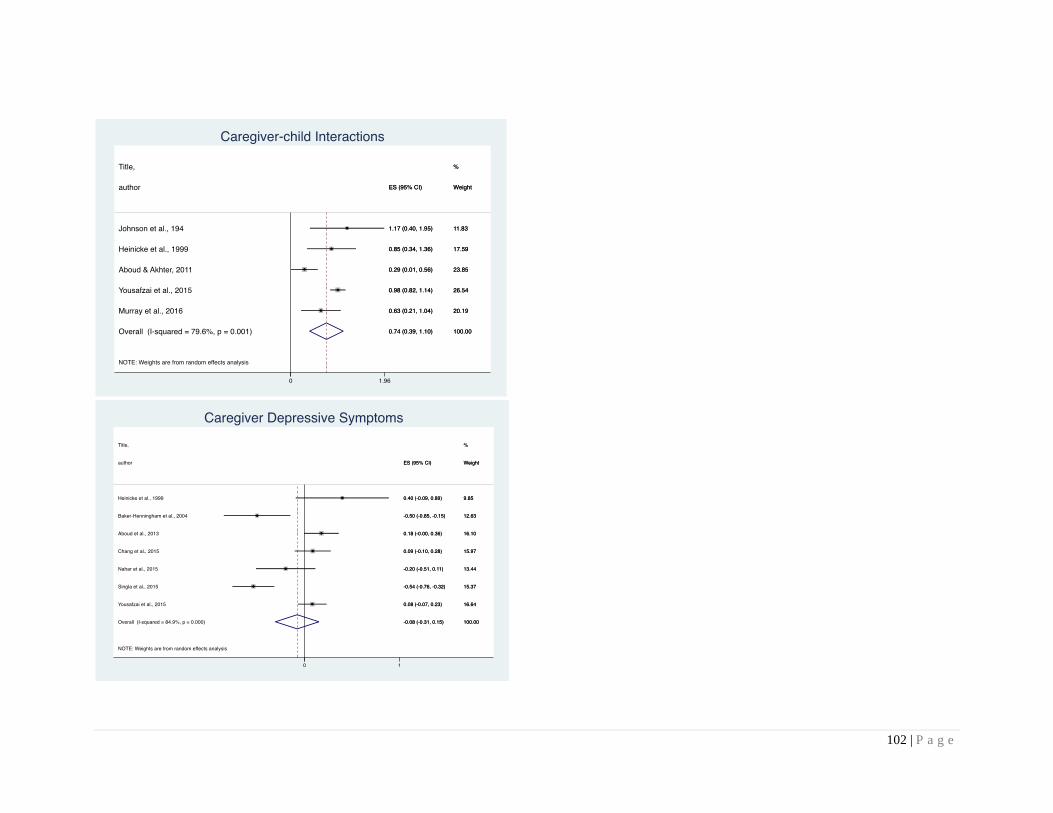
102 | P a g e
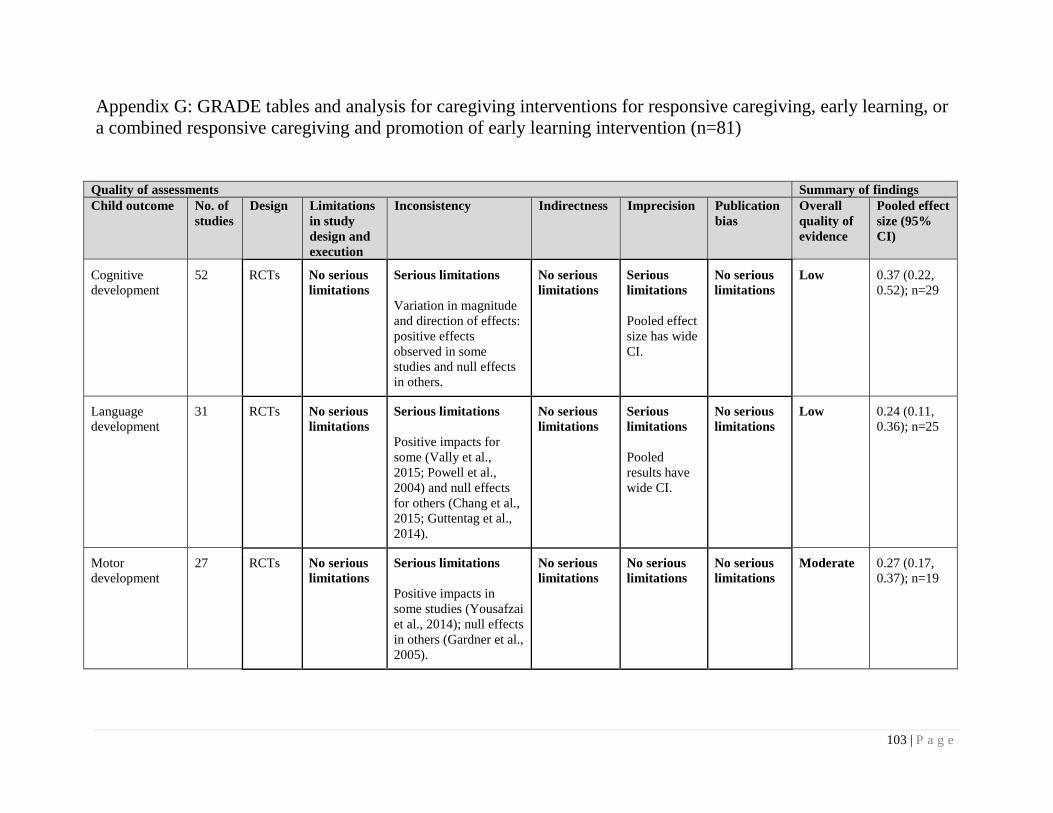
103 | P a g e
Appendix G: GRADE tables and analysis for caregiving interventions for responsive caregiving, early learning, or
a combined responsive caregiving and promotion of early learning intervention (n=81)
Quality of assessments Summary of findings
Child outcome No. of
studies
Design Limitations
in study
design and
execution
Inconsistency Indirectness Imprecision Publication
bias
Overall
quality of
evidence
Pooled effect
size (95%
CI)
Cognitive
development
52 RCTs No serious
limitations
Serious limitations
Variation in magnitude
and direction of effects:
positive effects
observed in some
studies and null effects
in others.
No serious
limitations
Serious
limitations
Pooled effect
size has wide
CI.
No serious
limitations
Low 0.37 (0.22,
0.52); n=29
Language
development
31 RCTs No serious
limitations
Serious limitations
Positive impacts for
some (Vally et al.,
2015; Powell et al.,
2004) and null effects
for others (Chang et al.,
2015; Guttentag et al.,
2014).
No serious
limitations
Serious
limitations
Pooled
results have
wide CI.
No serious
limitations
Low 0.24 (0.11,
0.36); n=25
Motor
development
27 RCTs No serious
limitations
Serious limitations
Positive impacts in
some studies (Yousafzai
et al., 2014); null effects
in others (Gardner et al.,
2005).
No serious
limitations
No serious
limitations
No serious
limitations
Moderate 0.27 (0.17,
0.37); n=19
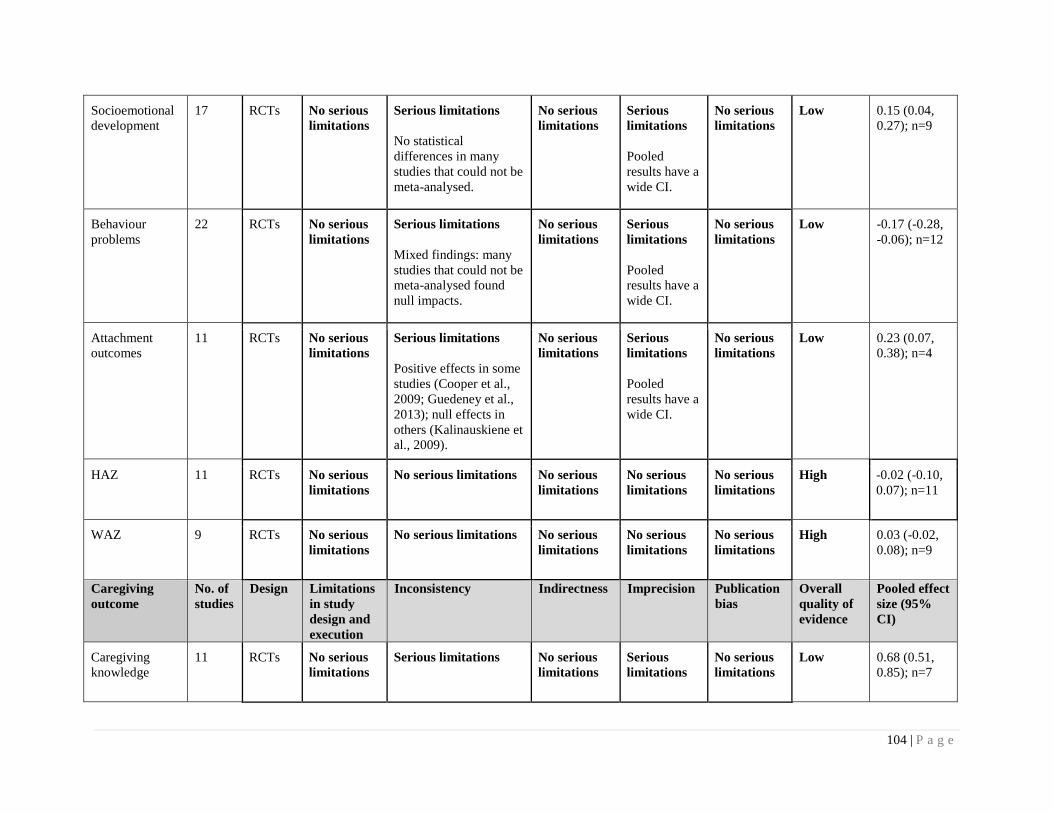
104 | P a g e
Socioemotional
development
17 RCTs No serious
limitations
Serious limitations
No statistical
differences in many
studies that could not be
meta-analysed.
No serious
limitations
Serious
limitations
Pooled
results have a
wide CI.
No serious
limitations
Low 0.15 (0.04,
0.27); n=9
Behaviour
problems
22 RCTs No serious
limitations
Serious limitations
Mixed findings: many
studies that could not be
meta-analysed found
null impacts.
No serious
limitations
Serious
limitations
Pooled
results have a
wide CI.
No serious
limitations
Low -0.17 (-0.28,
-0.06); n=12
Attachment
outcomes
11 RCTs No serious
limitations
Serious limitations
Positive effects in some
studies (Cooper et al.,
2009; Guedeney et al.,
2013); null effects in
others (Kalinauskiene et
al., 2009).
No serious
limitations
Serious
limitations
Pooled
results have a
wide CI.
No serious
limitations
Low 0.23 (0.07,
0.38); n=4
HAZ
11 RCTs No serious
limitations
No serious limitations No serious
limitations
No serious
limitations
No serious
limitations
High -0.02 (-0.10,
0.07); n=11
WAZ 9 RCTs No serious
limitations
No serious limitations
No serious
limitations
No serious
limitations
No serious
limitations
High 0.03 (-0.02,
0.08); n=9
Caregiving
outcome
No. of
studies
Design Limitations
in study
design and
execution
Inconsistency Indirectness Imprecision Publication
bias
Overall
quality of
evidence
Pooled effect
size (95%
CI)
Caregiving
knowledge
11 RCTs No serious
limitations
Serious limitations
No serious
limitations
Serious
limitations
No serious
limitations
Low 0.68 (0.51,
0.85); n=7
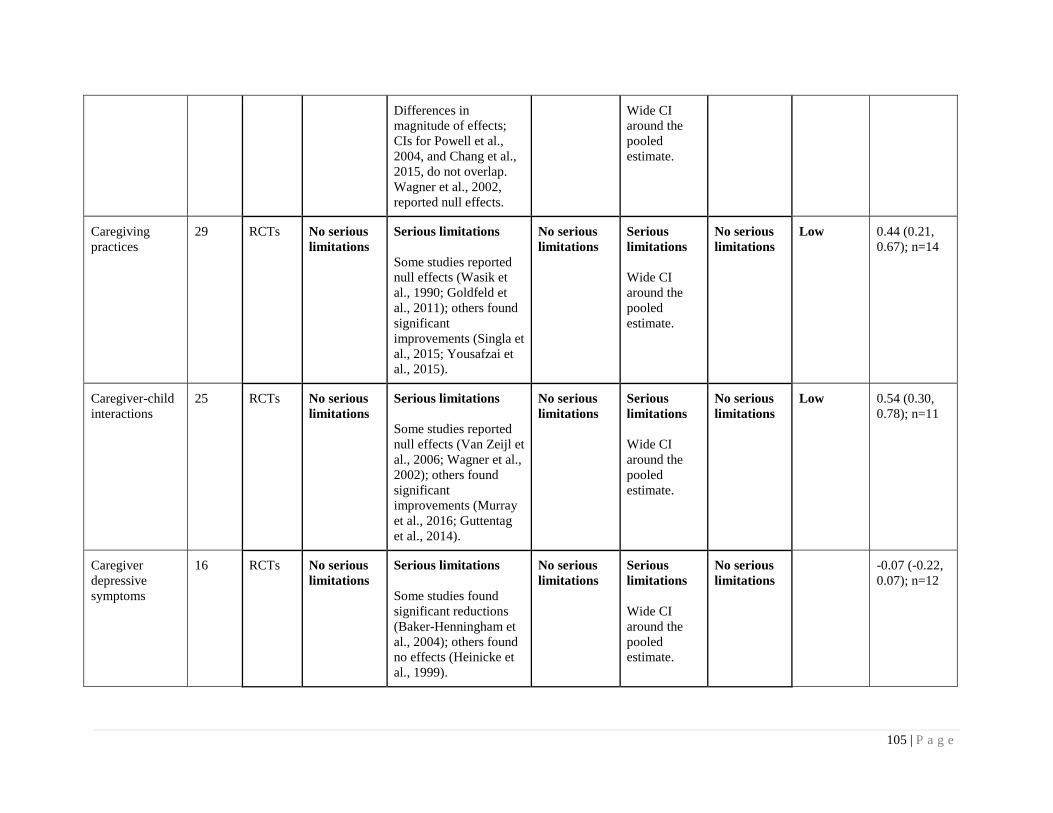
105 | P a g e
Differences in
magnitude of effects;
CIs for Powell et al.,
2004, and Chang et al.,
2015, do not overlap.
Wagner et al., 2002,
reported null effects.
Wide CI
around the
pooled
estimate.
Caregiving
practices
29 RCTs No serious
limitations
Serious limitations
Some studies reported
null effects (Wasik et
al., 1990; Goldfeld et
al., 2011); others found
significant
improvements (Singla et
al., 2015; Yousafzai et
al., 2015).
No serious
limitations
Serious
limitations
Wide CI
around the
pooled
estimate.
No serious
limitations
Low 0.44 (0.21,
0.67); n=14
Caregiver-child
interactions
25 RCTs No serious
limitations
Serious limitations
Some studies reported
null effects (Van Zeijl et
al., 2006; Wagner et al.,
2002); others found
significant
improvements (Murray
et al., 2016; Guttentag
et al., 2014).
No serious
limitations
Serious
limitations
Wide CI
around the
pooled
estimate.
No serious
limitations
Low 0.54 (0.30,
0.78); n=11
Caregiver
depressive
symptoms
16 RCTs No serious
limitations
Serious limitations
Some studies found
significant reductions
(Baker-Henningham et
al., 2004); others found
no effects (Heinicke et
al., 1999).
No serious
limitations
Serious
limitations
Wide CI
around the
pooled
estimate.
No serious
limitations
-0.07 (-0.22,
0.07); n=12
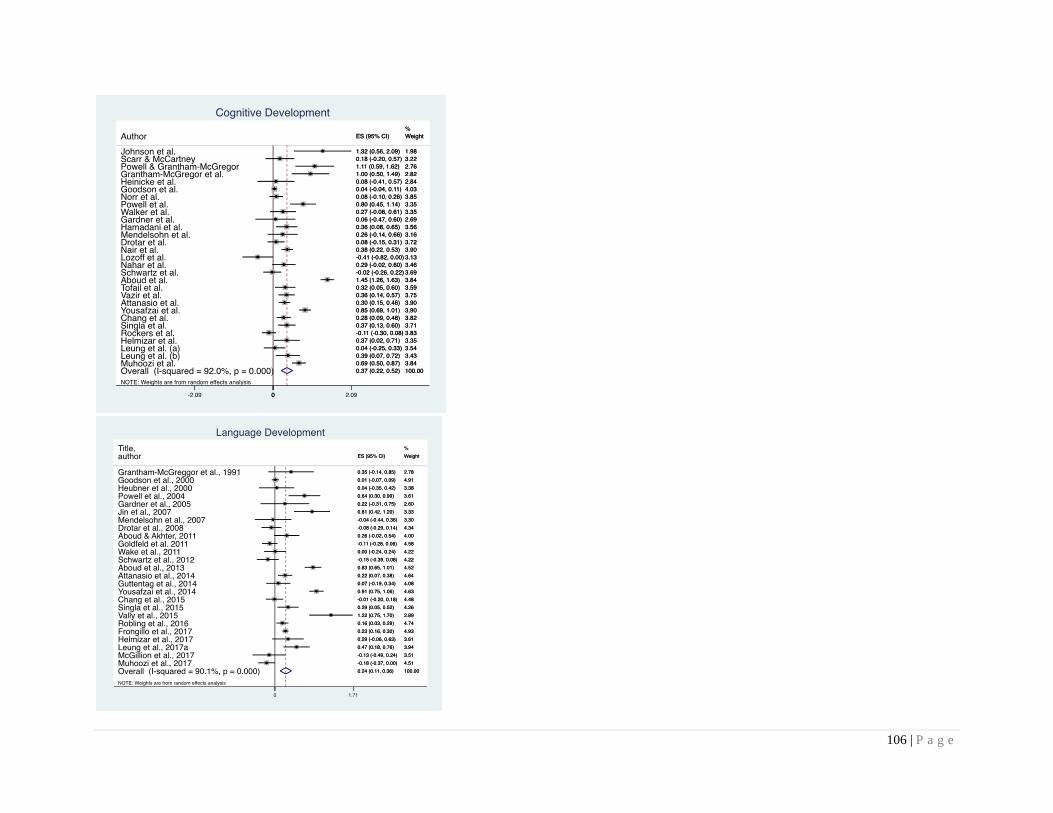
106 | P a g e
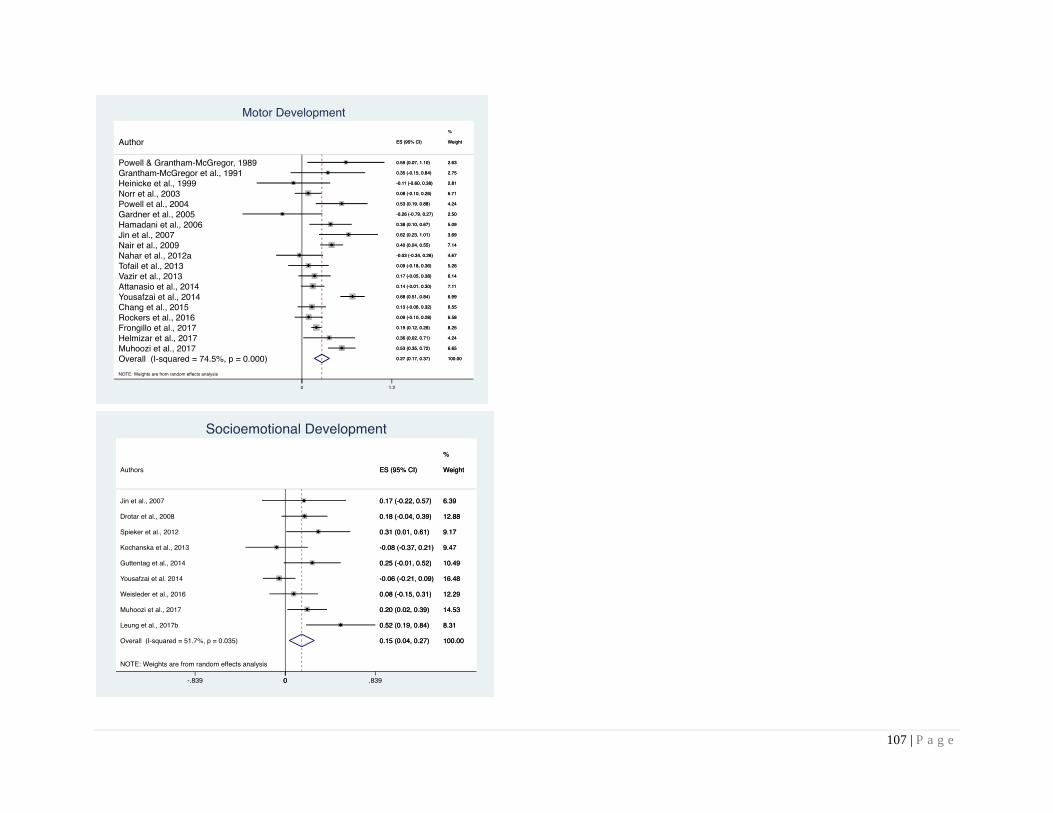
107 | P a g e
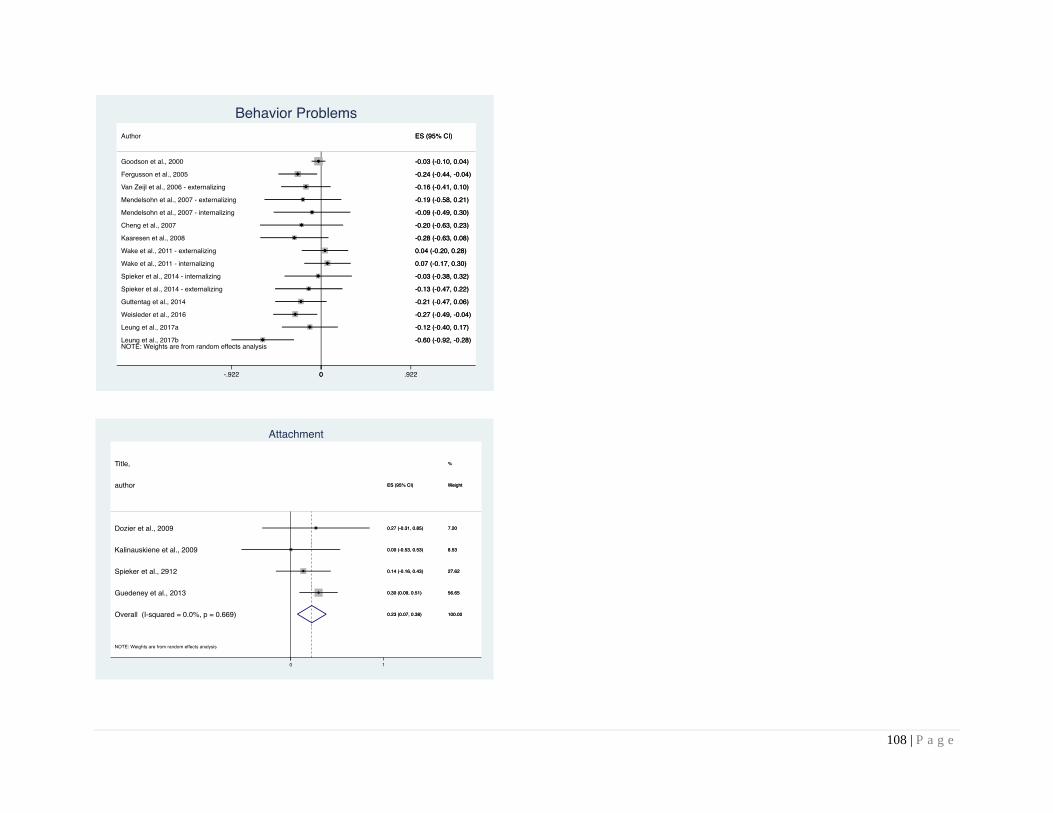
108 | P a g e
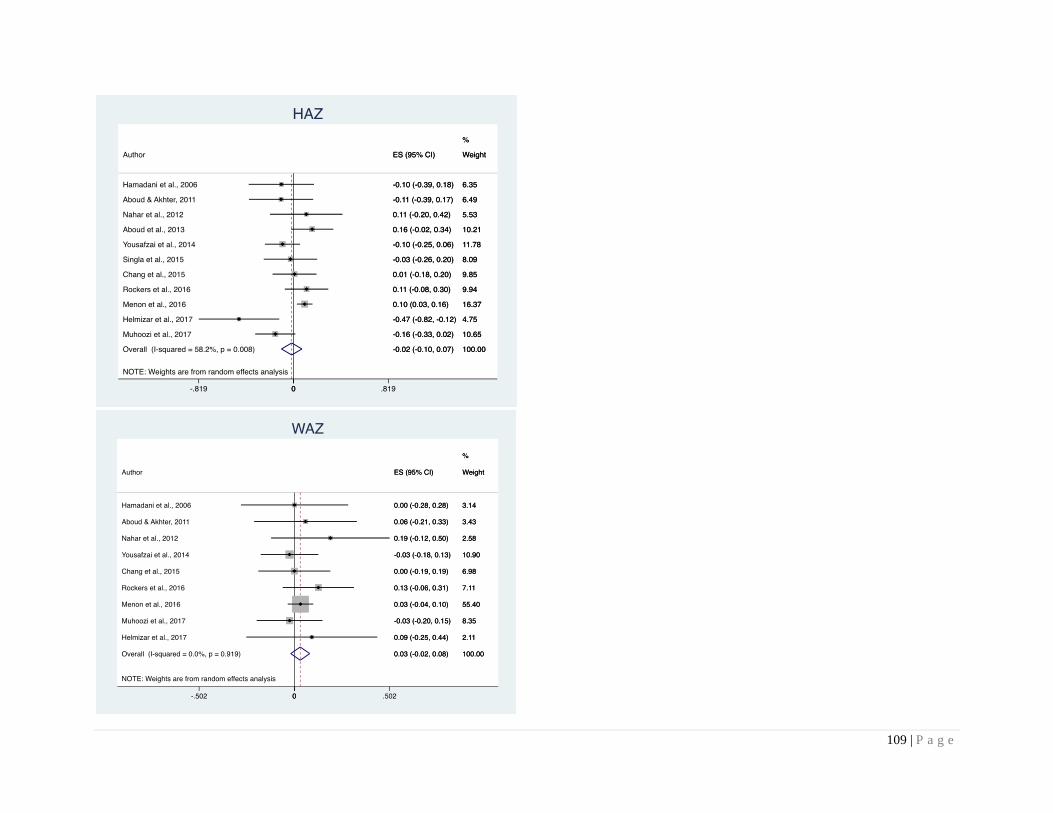
109 | P a g e
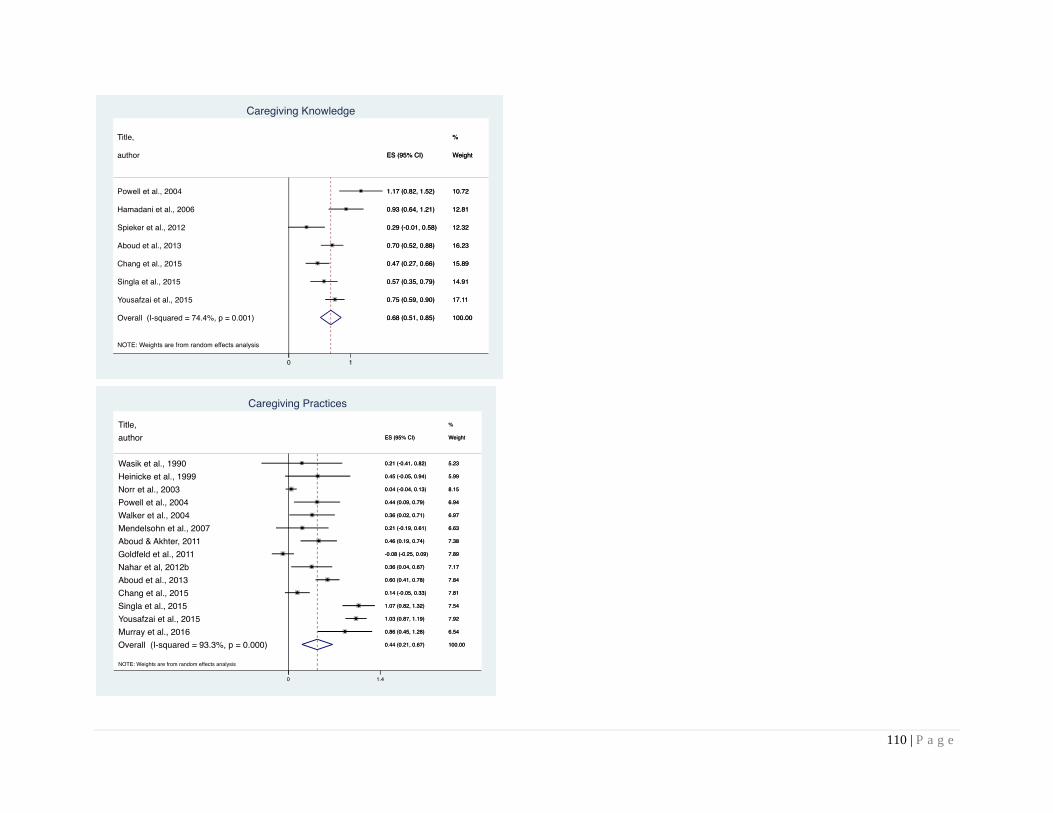
110 | P a g e
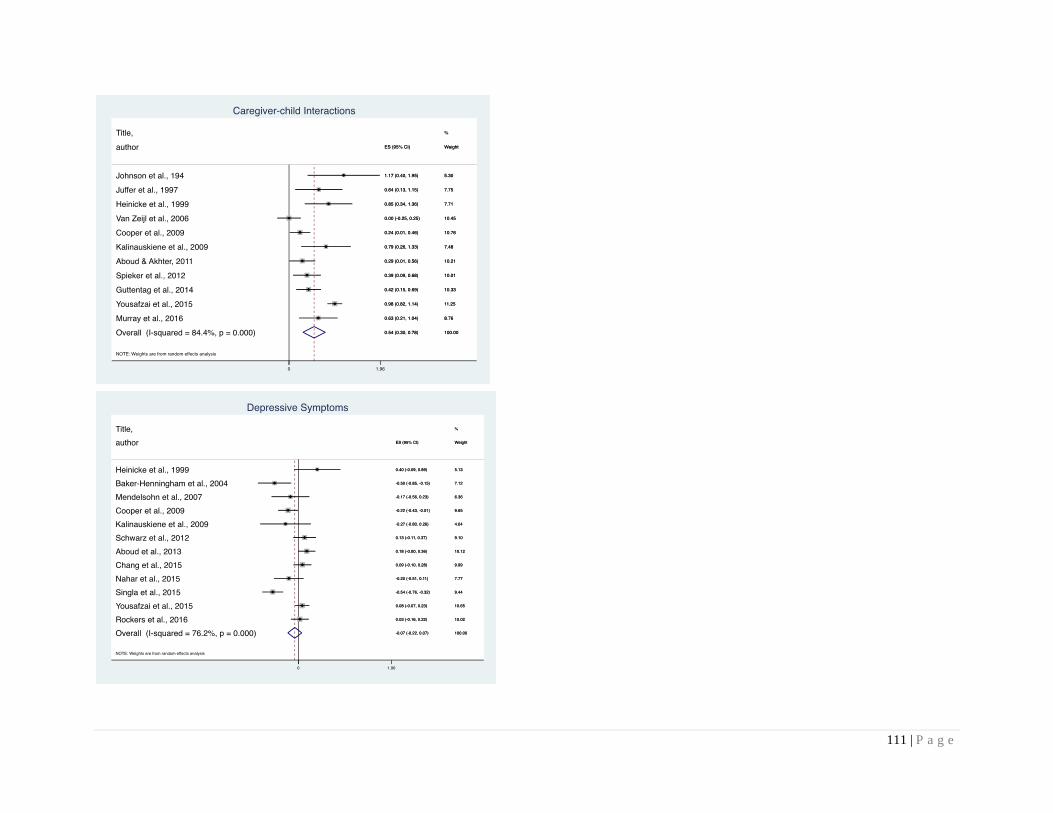
111 | P a g e
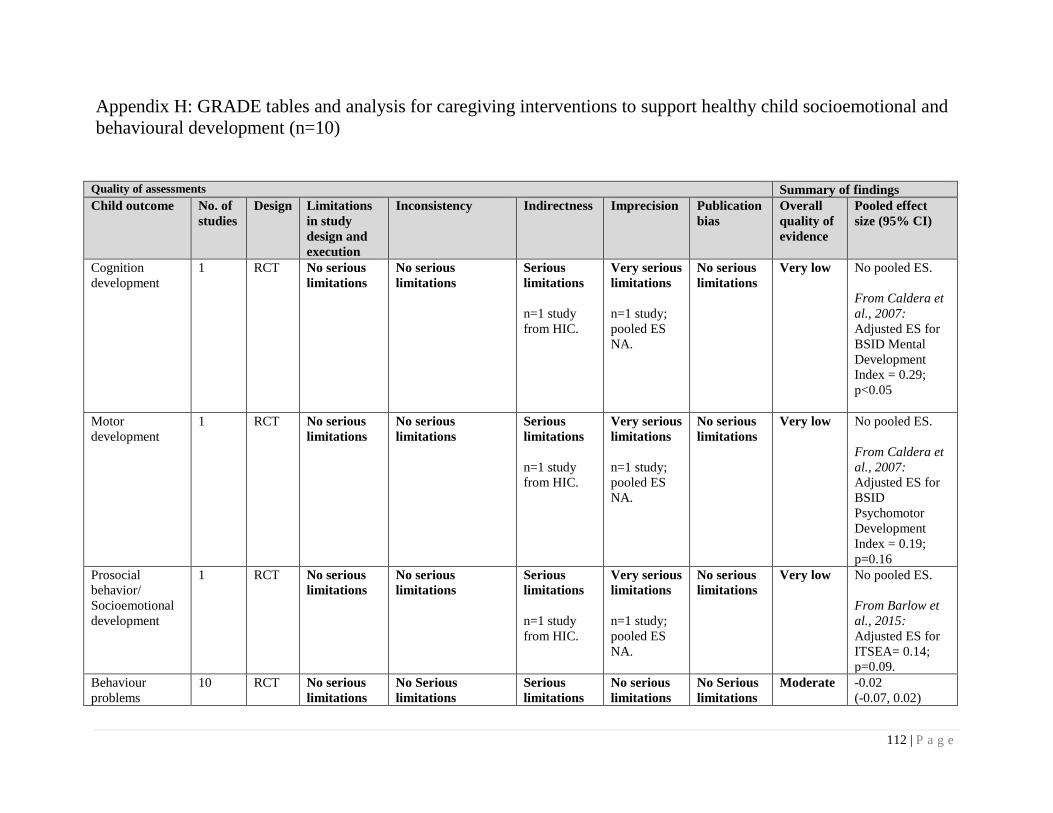
112 | P a g e
Appendix H: GRADE tables and analysis for caregiving interventions to support healthy child socioemotional and
behavioural development (n=10)
Quality of assessments Summary of findings
Child outcome No. of
studies
Design Limitations
in study
design and
execution
Inconsistency Indirectness Imprecision Publication
bias
Overall
quality of
evidence
Pooled effect
size (95% CI)
Cognition
development
1 RCT No serious
limitations
No serious
limitations
Serious
limitations
n=1 study
from HIC.
Very serious
limitations
n=1 study;
pooled ES
NA.
No serious
limitations
Very low No pooled ES.
From Caldera et
al., 2007:
Adjusted ES for
BSID Mental
Development
Index = 0.29;
p<0.05
Motor
development
1 RCT No serious
limitations
No serious
limitations
Serious
limitations
n=1 study
from HIC.
Very serious
limitations
n=1 study;
pooled ES
NA.
No serious
limitations
Very low No pooled ES.
From Caldera et
al., 2007:
Adjusted ES for
BSID
Psychomotor
Development
Index = 0.19;
p=0.16
Prosocial
behavior/
Socioemotional
development
1 RCT No serious
limitations
No serious
limitations
Serious
limitations
n=1 study
from HIC.
Very serious
limitations
n=1 study;
pooled ES
NA.
No serious
limitations
Very low No pooled ES.
From Barlow et
al., 2015:
Adjusted ES for
ITSEA= 0.14;
p=0.09.
Behaviour
problems
10 RCT No serious
limitations
No Serious
limitations
Serious
limitations
No serious
limitations
No Serious
limitations
Moderate -0.02
(-0.07, 0.02)
113 | P a g e
Quality of assessments Summary of findings
Child outcome No. of
studies
Design Limitations
in study
design and
execution
Inconsistency Indirectness Imprecision Publication
bias
Overall
quality of
evidence
Pooled effect
size (95% CI)
I2 = 9.9%
95% CIs are
overlapping.
Additional n=5
studies:
n=1: no effects; n=1:
significant
reductions in mean
scores for child
behaviour problems;
n=3: significant
reductions on some
domains but not all.
n=10 studies
from HICs.
n=5
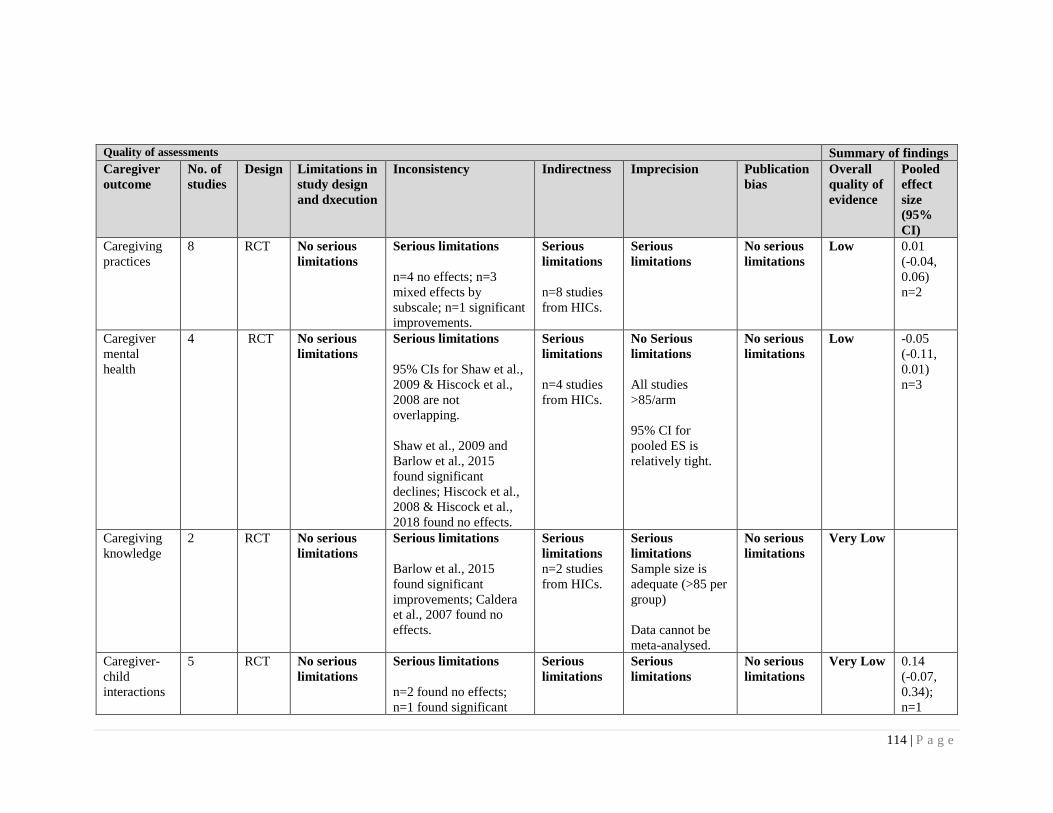
114 | P a g e
Quality of assessments Summary of findings
Caregiver
outcome
No. of
studies
Design Limitations in
study design
and dxecution
Inconsistency Indirectness Imprecision Publication
bias
Overall
quality of
evidence
Pooled
effect
size
(95%
CI)
Caregiving
practices
8 RCT No serious
limitations
Serious limitations
n=4 no effects; n=3
mixed effects by
subscale; n=1 significant
improvements.
Serious
limitations
n=8 studies
from HICs.
Serious
limitations
No serious
limitations
Low 0.01
(-0.04,
0.06)
n=2
Caregiver
mental
health
4 RCT No serious
limitations
Serious limitations
95% CIs for Shaw et al.,
2009 & Hiscock et al.,
2008 are not
overlapping.
Shaw et al., 2009 and
Barlow et al., 2015
found significant
declines; Hiscock et al.,
2008 & Hiscock et al.,
2018 found no effects.
Serious
limitations
n=4 studies
from HICs.
No Serious
limitations
All studies
>85/arm
95% CI for
pooled ES is
relatively tight.
No serious
limitations
Low -0.05
(-0.11,
0.01)
n=3
Caregiving
knowledge
2 RCT No serious
limitations
Serious limitations
Barlow et al., 2015
found significant
improvements; Caldera
et al., 2007 found no
effects.
Serious
limitations
n=2 studies
from HICs.
Serious
limitations
Sample size is
adequate (>85 per
group)
Data cannot be
meta-analysed.
No serious
limitations
Very Low
Caregiver-
child
interactions
5 RCT No serious
limitations
Serious limitations
n=2 found no effects;
n=1 found significant
Serious
limitations
Serious
limitations
No serious
limitations
Very Low 0.14
(-0.07,
0.34);
n=1
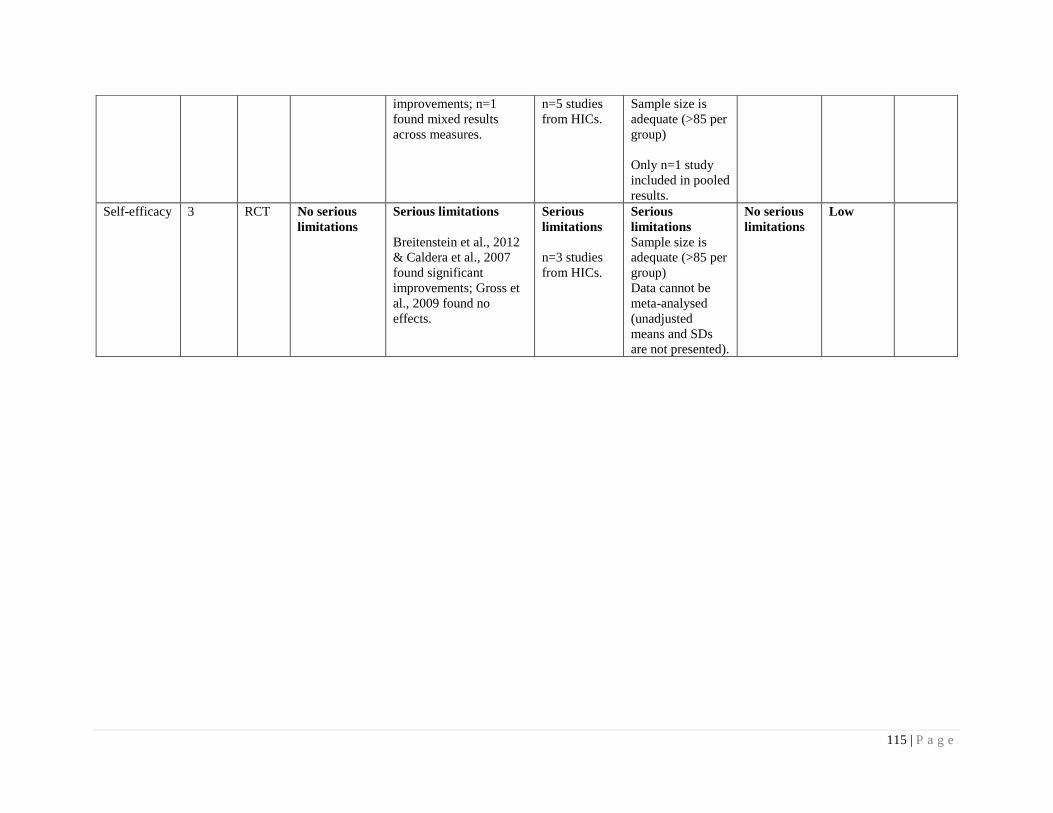
115 | P a g e
improvements; n=1
found mixed results
across measures.
n=5 studies
from HICs.
Sample size is
adequate (>85 per
group)
Only n=1 study
included in pooled
results.
Self-efficacy 3 RCT No serious
limitations
Serious limitations
Breitenstein et al., 2012
& Caldera et al., 2007
found significant
improvements; Gross et
al., 2009 found no
effects.
Serious
limitations
n=3 studies
from HICs.
Serious
limitations
Sample size is
adequate (>85 per
group)
Data cannot be
meta-analysed
(unadjusted
means and SDs
are not presented).
No serious
limitations
Low
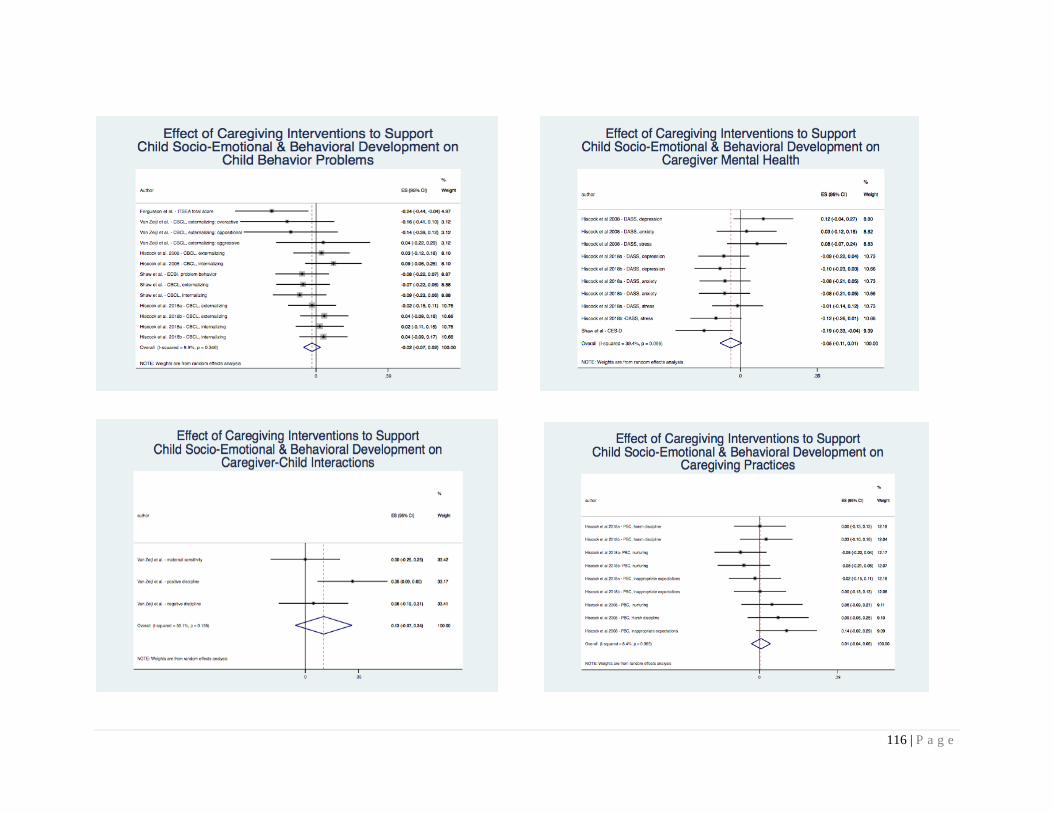
116 | P a g e

117 | P a g e
Appendix I: GRADE tables and analysis for integrated caregiving and nutrition interventions (n=18)
Combined nutrition and caregiving interventions versus standard of care
Quality of assessments Summary of findings
Child outcome No. of
studies
Design Limitations
in study
design and
execution
Inconsistency Indirectness Imprecision Publication
bias
Overall
quality of
evidence
Pooled effect
size (95%
CI)
Cognitive
development
14 RCTs No serious
limitations
Serious limitations
Variation in magnitude
and direction of effects;
some studies have null
effects (Rockers et al.,
2016; Nahar et al.,
2012), while others
have positive effects
(Aboud et al., 2013;
Grantham-McGregor et
al., 1991).
No serious
limitations
Serious
limitations
Pooled effect
size has wide
CI.
No serious
limitations
Low 0.57 (0.32,
0.82); n=13
Language
development
10 RCTs No serious
limitations
Serious limitations
Variation in magnitude
and direction of effects:
Muhoozi et al., 2017,
found negative impacts;
Aboud et al., 2013 &
Yousafzai et al., 2014
found positive impacts.
No serious
limitations
Serious
limitations
Pooled
results have
wide CI.
No serious
limitations
Low 0.40 (0.17,
0.63); n=10
Motor
development
10 RCTs No serious
limitations
Serious limitations
No serious
limitations
Serious
limitations
No serious
limitations
Low 0.4 (0.26,
0.53); n=10

118 | P a g e
Variation in magnitude
and direction of effects.
Nahar et al., 2012, and
Vazir et al., 2013 found
null effects, whereas
others found positive
impacts (Yousafzai et
al., 2014; Muhoozi et
al., 2017).
5 of the 10
studies have
small sample
sizes.
Pooled effect
size has wide
CI.
Socioemotional
development
2 RCTs No serious
limitations
Serious limitations
Yousafzai et al., 2015 –
no impacts; Muhoozi et
al., 2017 – positive
impacts.
No serious
limitations
Serious
limitations
Pooled effect
size has wide
CI.
No serious
limitations
Low 0.09 (-0.11,
0.30); n=2
HAZ
9 RCTs No serious
limitations
Serious limitations
Nahar et al., 2012, and
Helmizar et al., 2017,
found negative impacts;
others found null
effects.
No serious
limitations
Serious
limitations
Pooled
results have
wide CI.
No serious
limitations
Low -0.13 (-0.31,
0.05); n=9
WAZ 7 RCTs No serious
limitations
No serious limitations
No serious
limitations
No serious
limitations
No serious
limitations
High 0.06 (-0.02,
0.13); n=7
WHZ 6 RCTs No serious
limitations
No serious limitations
No serious
limitations
Serious
limitations
Pooled
results have
wide CI.
No serious
limitations
Moderate 0.20 (0.05,
0.34); n=6
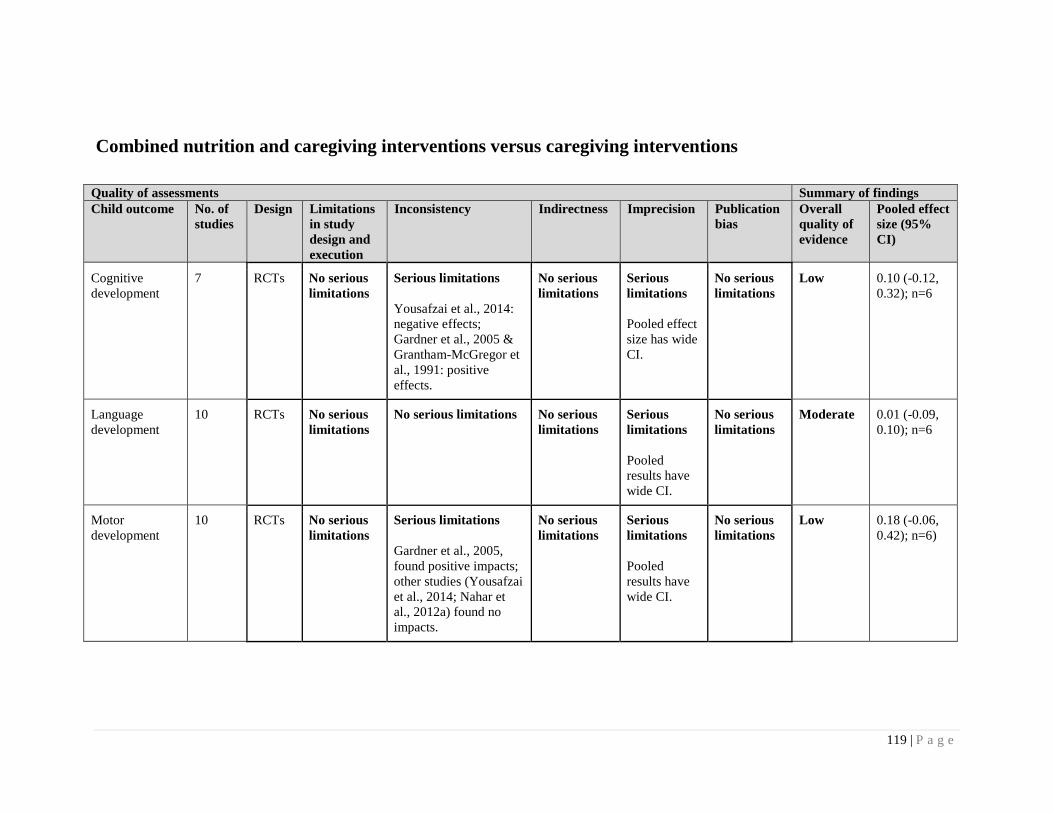
119 | P a g e
Combined nutrition and caregiving interventions versus caregiving interventions
Quality of assessments Summary of findings
Child outcome No. of
studies
Design Limitations
in study
design and
execution
Inconsistency Indirectness Imprecision Publication
bias
Overall
quality of
evidence
Pooled effect
size (95%
CI)
Cognitive
development
7 RCTs No serious
limitations
Serious limitations
Yousafzai et al., 2014:
negative effects;
Gardner et al., 2005 &
Grantham-McGregor et
al., 1991: positive
effects.
No serious
limitations
Serious
limitations
Pooled effect
size has wide
CI.
No serious
limitations
Low 0.10 (-0.12,
0.32); n=6
Language
development
10 RCTs No serious
limitations
No serious limitations
No serious
limitations
Serious
limitations
Pooled
results have
wide CI.
No serious
limitations
Moderate 0.01 (-0.09,
0.10); n=6
Motor
development
10 RCTs No serious
limitations
Serious limitations
Gardner et al., 2005,
found positive impacts;
other studies (Yousafzai
et al., 2014; Nahar et
al., 2012a) found no
impacts.
No serious
limitations
Serious
limitations
Pooled
results have
wide CI.
No serious
limitations
Low 0.18 (-0.06,
0.42); n=6)
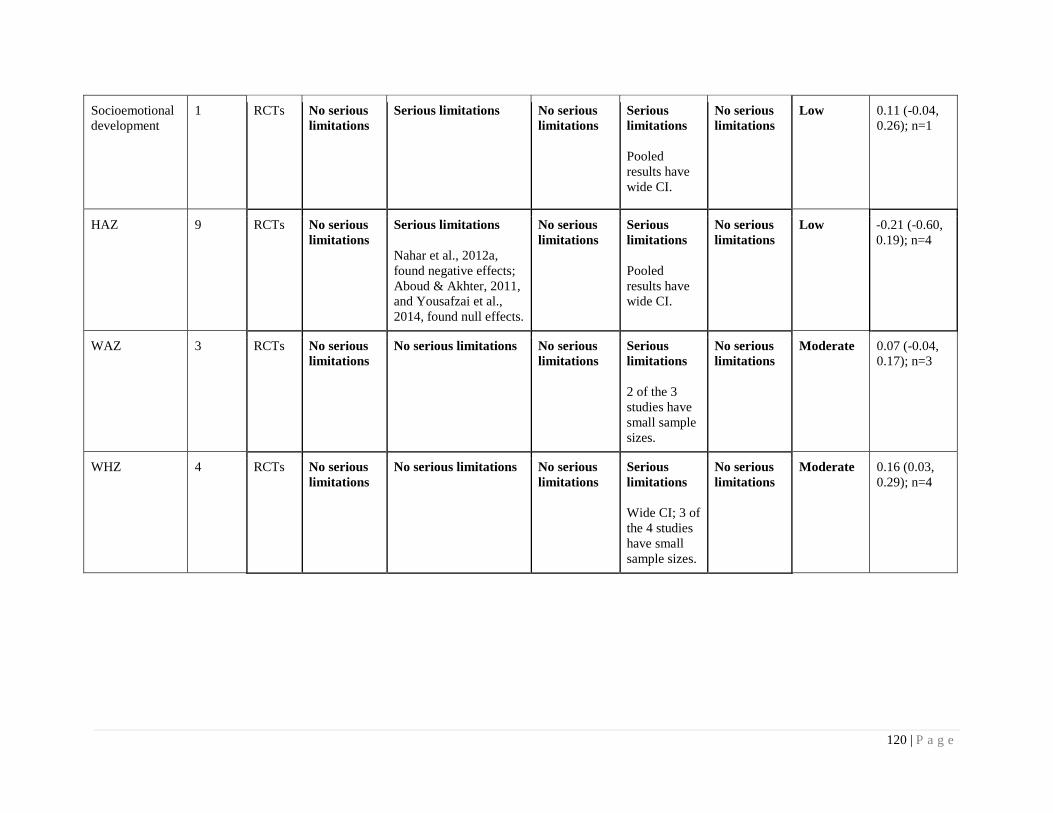
120 | P a g e
Socioemotional
development
1 RCTs No serious
limitations
Serious limitations
No serious
limitations
Serious
limitations
Pooled
results have
wide CI.
No serious
limitations
Low 0.11 (-0.04,
0.26); n=1
HAZ
9 RCTs No serious
limitations
Serious limitations
Nahar et al., 2012a,
found negative effects;
Aboud & Akhter, 2011,
and Yousafzai et al.,
2014, found null effects.
No serious
limitations
Serious
limitations
Pooled
results have
wide CI.
No serious
limitations
Low -0.21 (-0.60,
0.19); n=4
WAZ 3 RCTs No serious
limitations
No serious limitations
No serious
limitations
Serious
limitations
2 of the 3
studies have
small sample
sizes.
No serious
limitations
Moderate 0.07 (-0.04,
0.17); n=3
WHZ 4 RCTs No serious
limitations
No serious limitations
No serious
limitations
Serious
limitations
Wide CI; 3 of
the 4 studies
have small
sample sizes.
No serious
limitations
Moderate 0.16 (0.03,
0.29); n=4
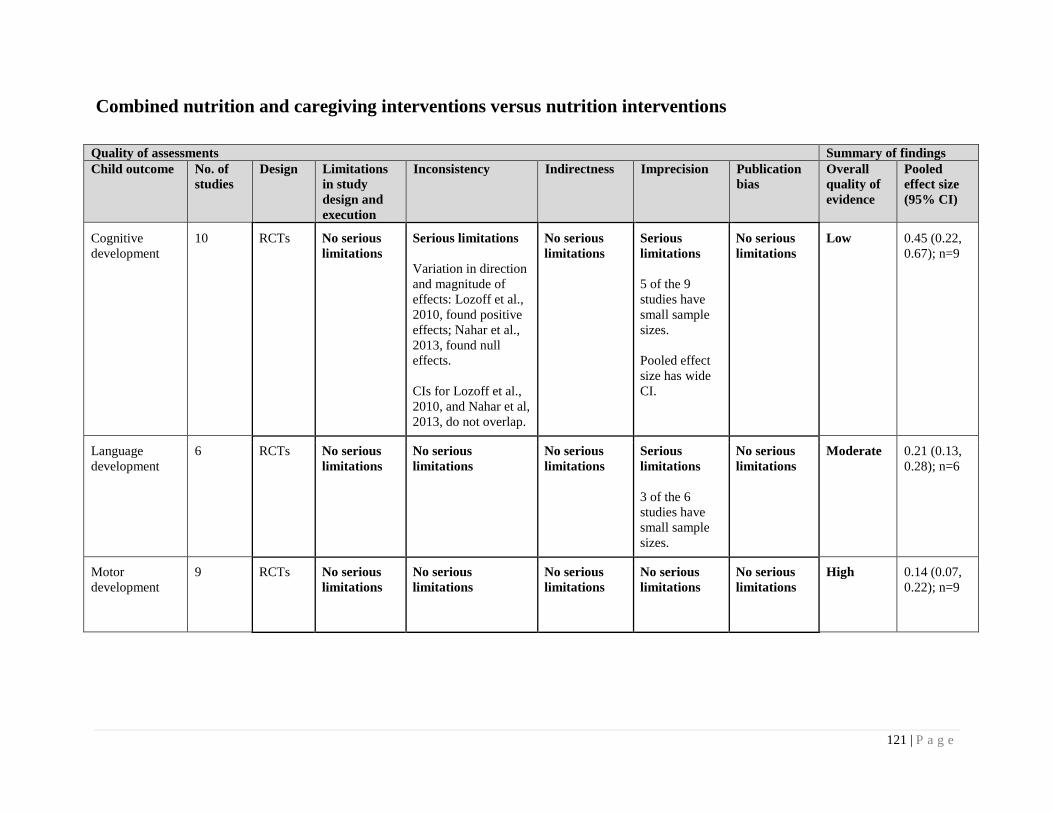
121 | P a g e
Combined nutrition and caregiving interventions versus nutrition interventions
Quality of assessments Summary of findings
Child outcome No. of
studies
Design Limitations
in study
design and
execution
Inconsistency Indirectness Imprecision Publication
bias
Overall
quality of
evidence
Pooled
effect size
(95% CI)
Cognitive
development
10 RCTs No serious
limitations
Serious limitations
Variation in direction
and magnitude of
effects: Lozoff et al.,
2010, found positive
effects; Nahar et al.,
2013, found null
effects.
CIs for Lozoff et al.,
2010, and Nahar et al,
2013, do not overlap.
No serious
limitations
Serious
limitations
5 of the 9
studies have
small sample
sizes.
Pooled effect
size has wide
CI.
No serious
limitations
Low 0.45 (0.22,
0.67); n=9
Language
development
6 RCTs No serious
limitations
No serious
limitations
No serious
limitations
Serious
limitations
3 of the 6
studies have
small sample
sizes.
No serious
limitations
Moderate 0.21 (0.13,
0.28); n=6
Motor
development
9 RCTs No serious
limitations
No serious
limitations
No serious
limitations
No serious
limitations
No serious
limitations
High 0.14 (0.07,
0.22); n=9
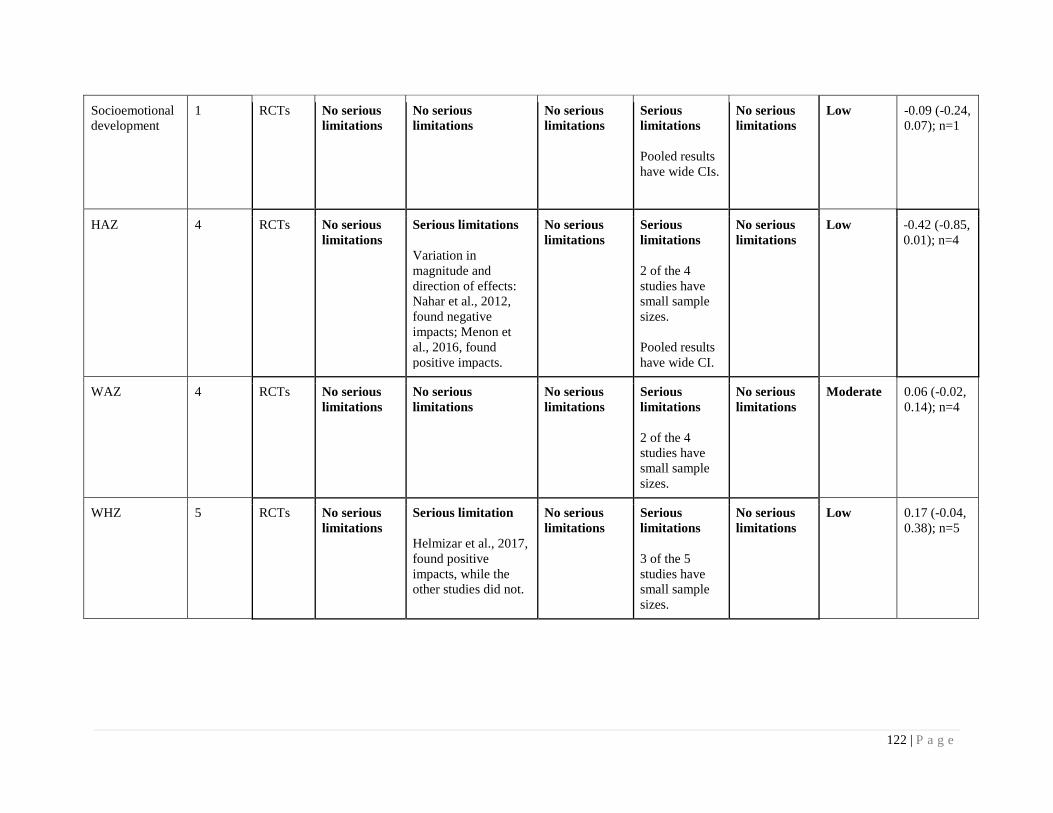
122 | P a g e
Socioemotional
development
1 RCTs No serious
limitations
No serious
limitations
No serious
limitations
Serious
limitations
Pooled results
have wide CIs.
No serious
limitations
Low -0.09 (-0.24,
0.07); n=1
HAZ
4 RCTs No serious
limitations
Serious limitations
Variation in
magnitude and
direction of effects:
Nahar et al., 2012,
found negative
impacts; Menon et
al., 2016, found
positive impacts.
No serious
limitations
Serious
limitations
2 of the 4
studies have
small sample
sizes.
Pooled results
have wide CI.
No serious
limitations
Low -0.42 (-0.85,
0.01); n=4
WAZ 4 RCTs No serious
limitations
No serious
limitations
No serious
limitations
Serious
limitations
2 of the 4
studies have
small sample
sizes.
No serious
limitations
Moderate 0.06 (-0.02,
0.14); n=4
WHZ 5 RCTs No serious
limitations
Serious limitation
Helmizar et al., 2017,
found positive
impacts, while the
other studies did not.
No serious
limitations
Serious
limitations
3 of the 5
studies have
small sample
sizes.
No serious
limitations
Low 0.17 (-0.04,
0.38); n=5
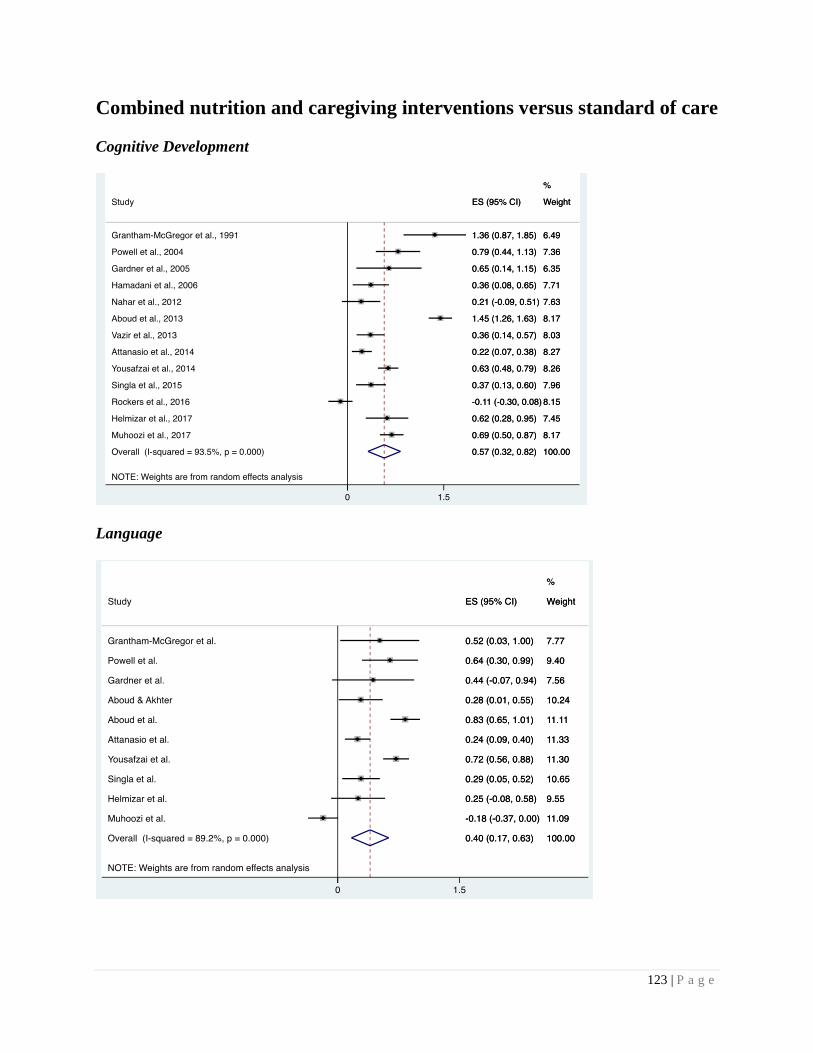
123 | P a g e
Combined nutrition and caregiving interventions versus standard of care
Cognitive Development
Language
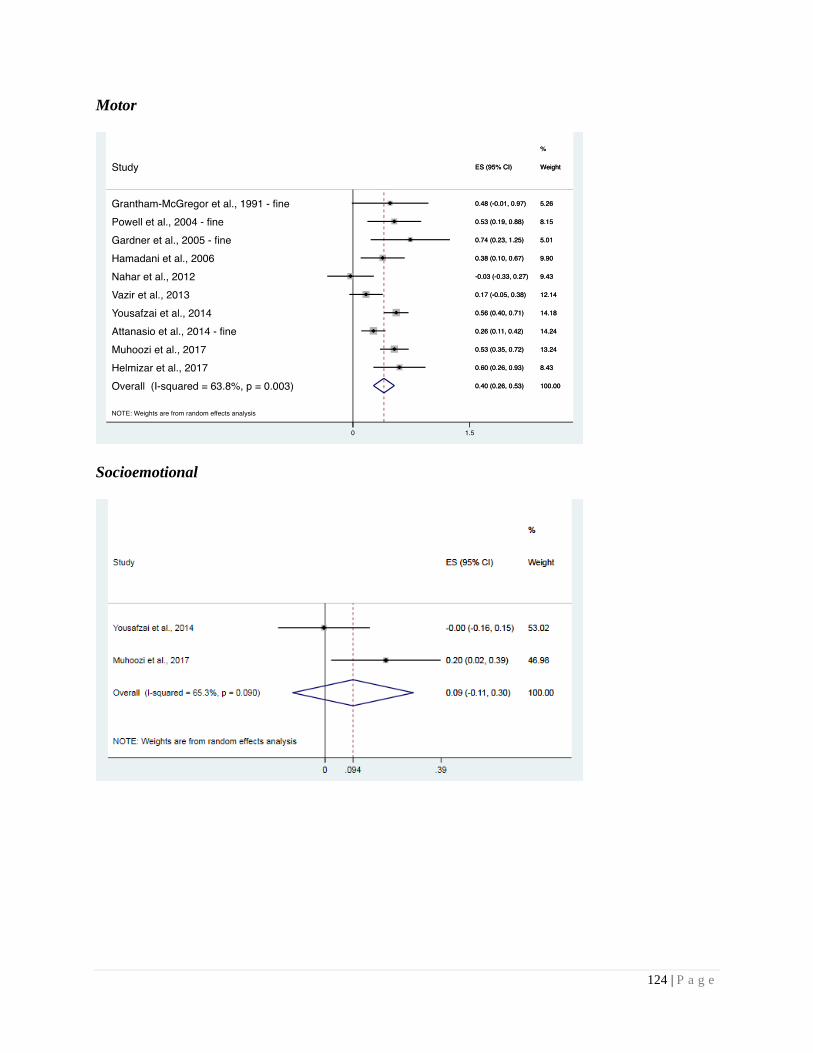
124 | P a g e
Motor
Socioemotional
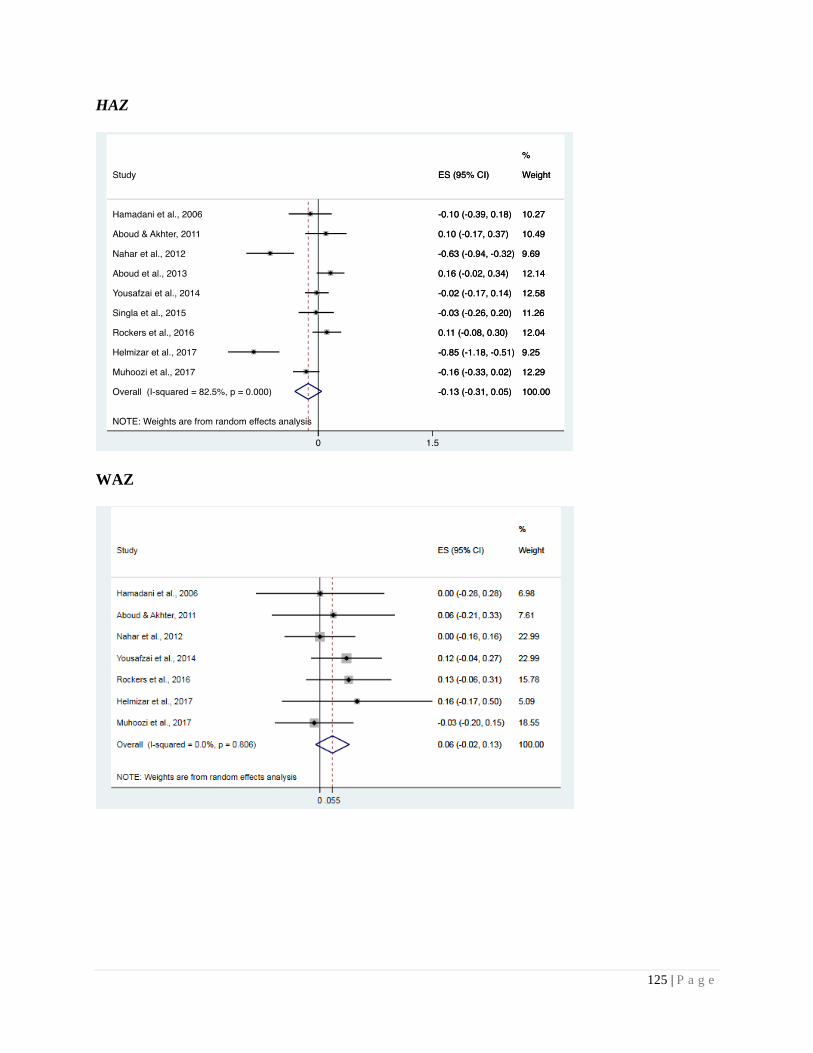
125 | P a g e
HAZ
WAZ

126 | P a g e
WHZ
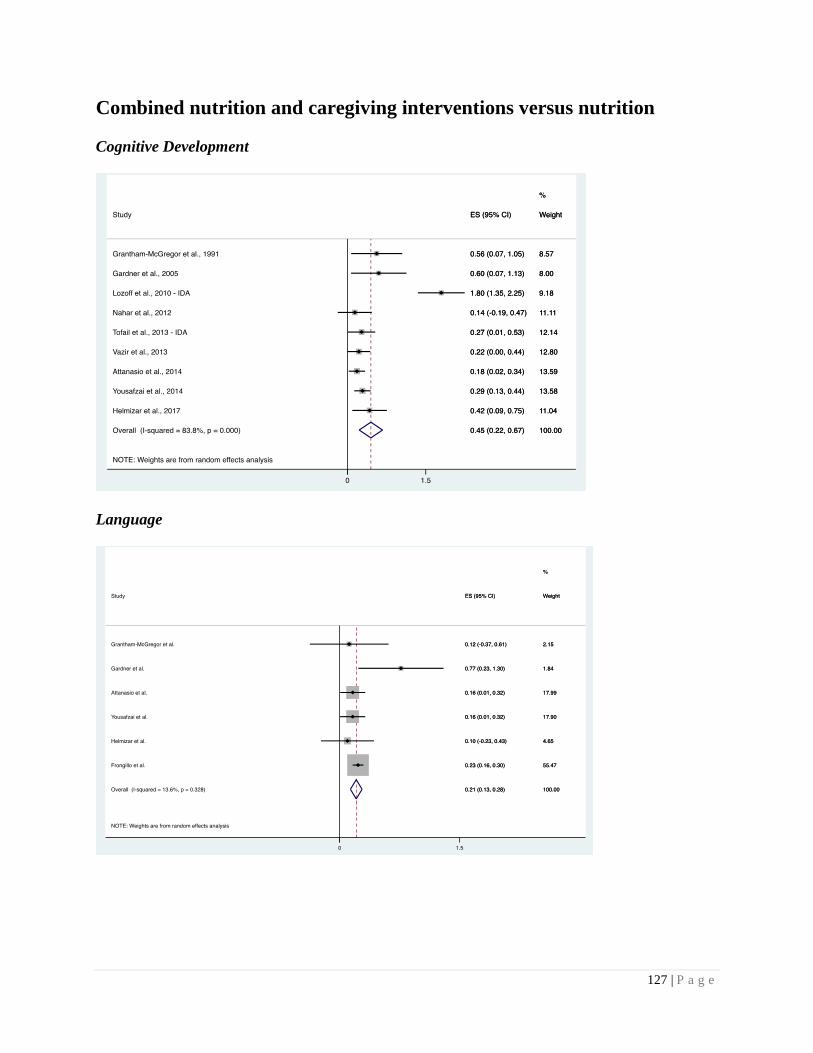
127 | P a g e
Combined nutrition and caregiving interventions versus nutrition
Cognitive Development
Language
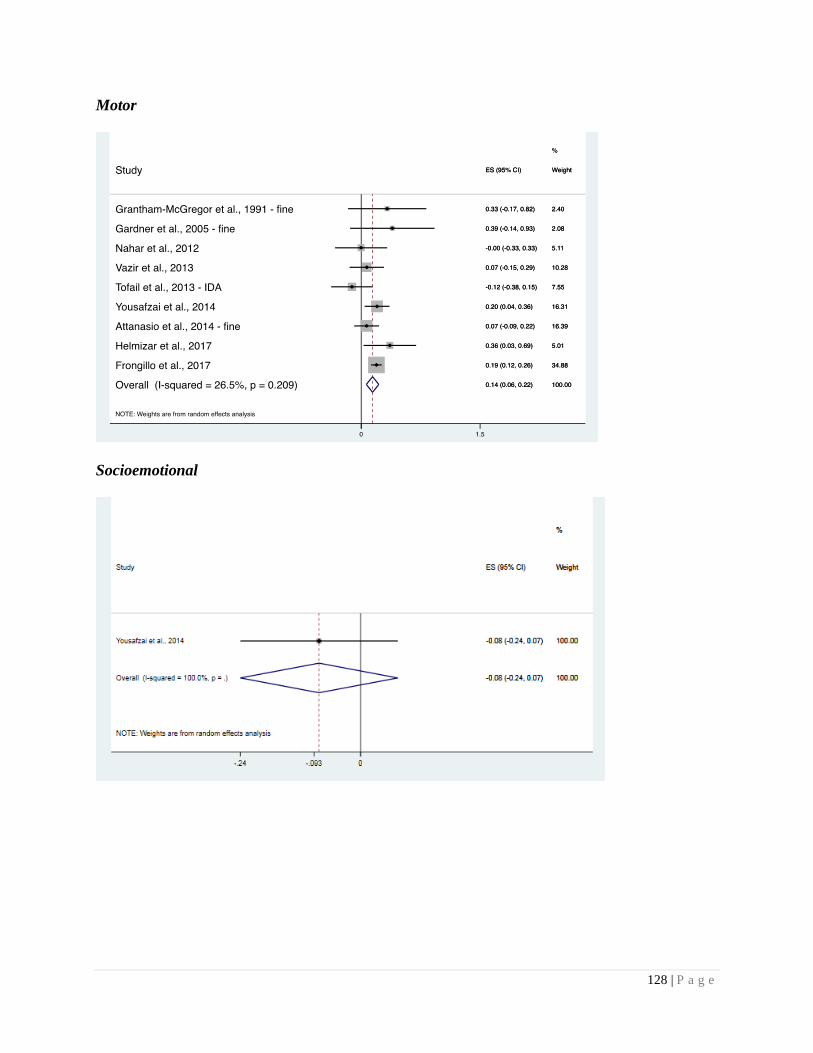
128 | P a g e
Motor
Socioemotional
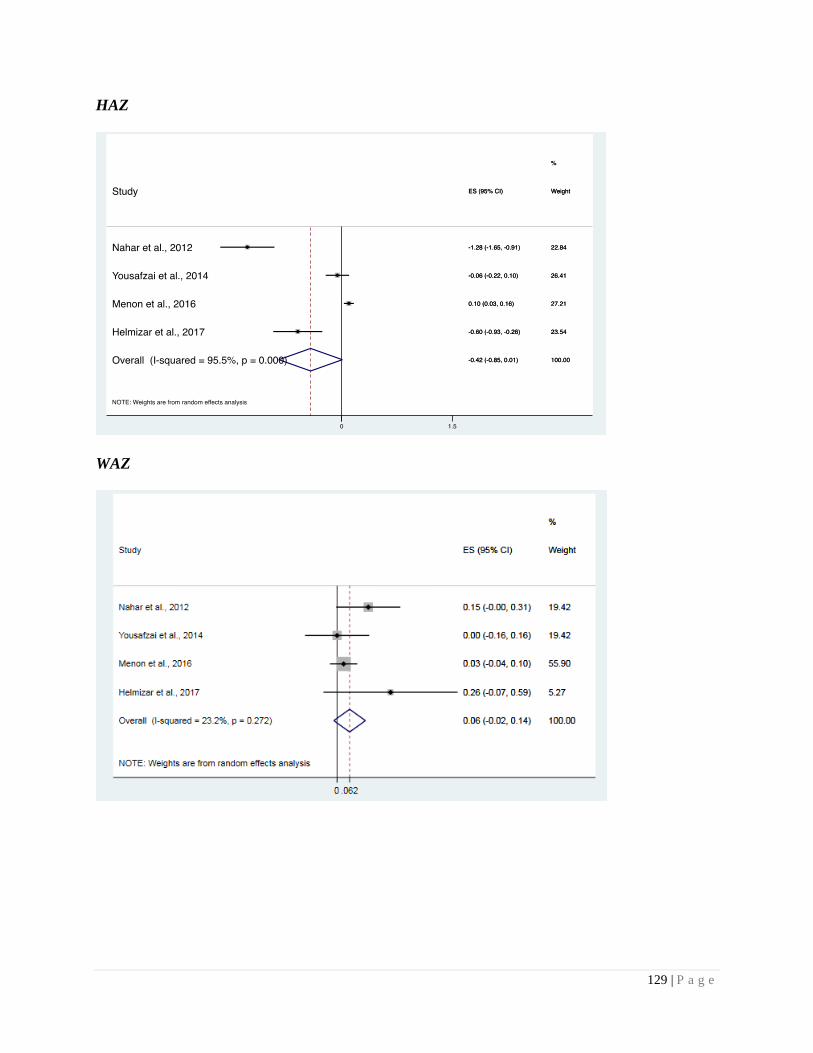
129 | P a g e
HAZ
WAZ
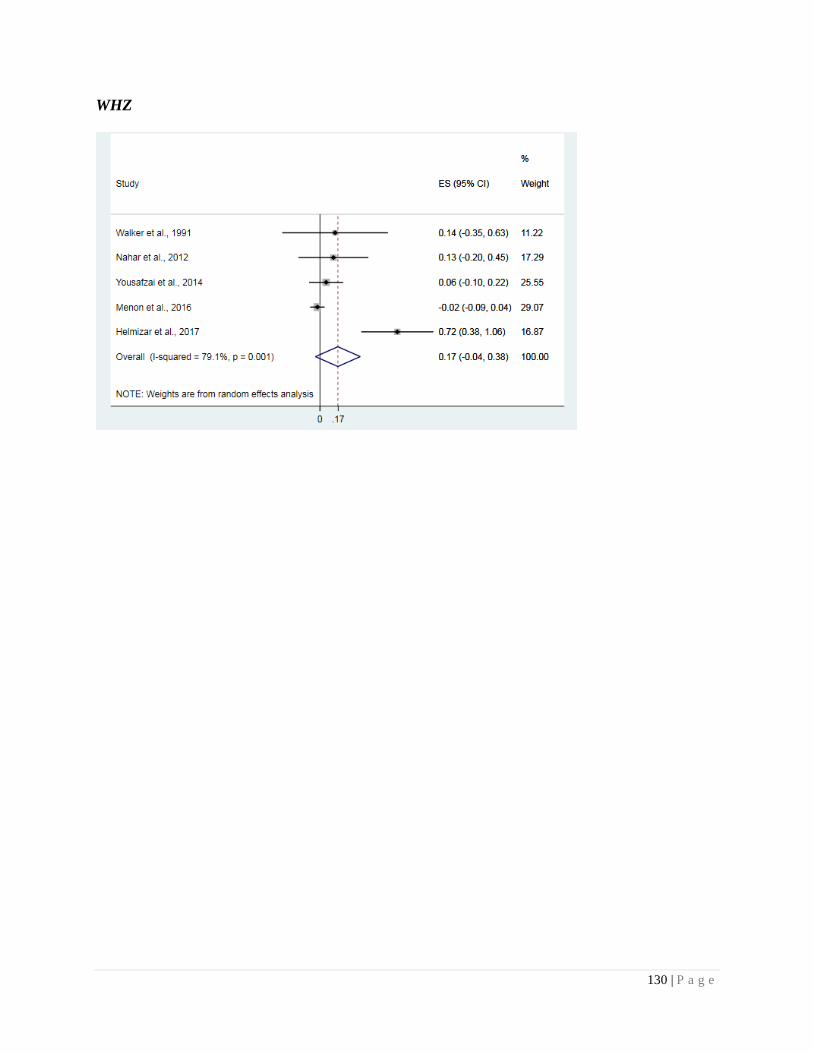
130 | P a g e
WHZ
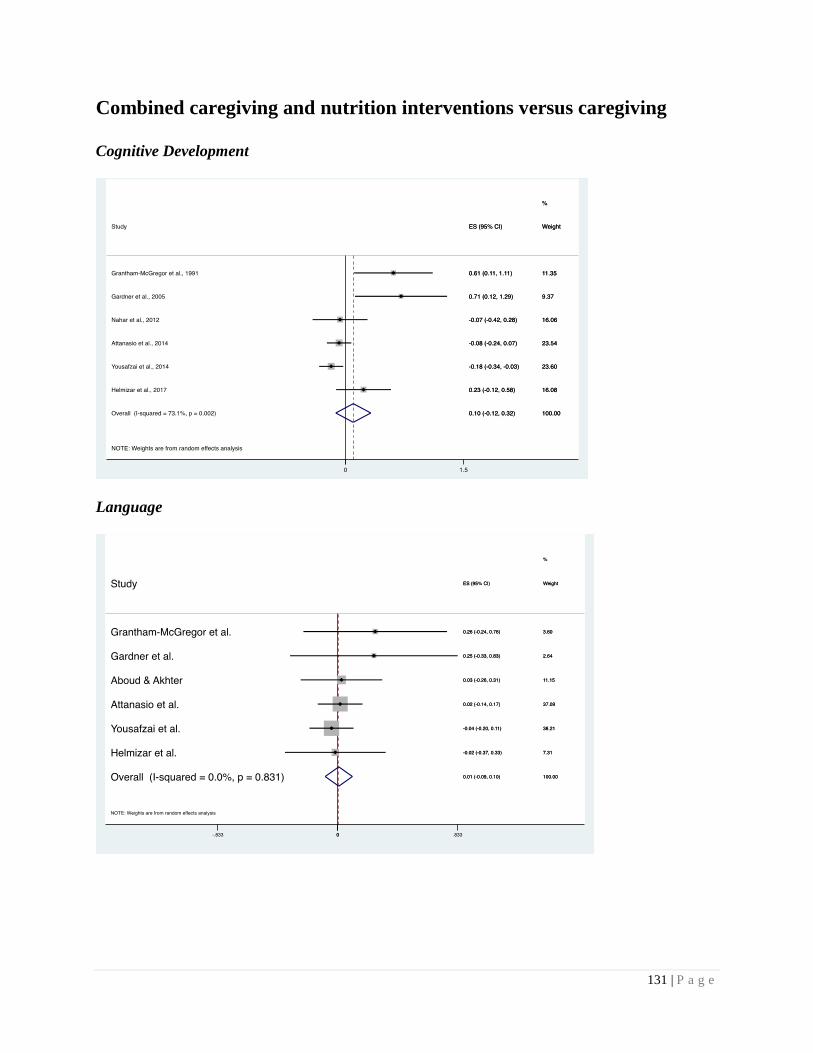
131 | P a g e
Combined caregiving and nutrition interventions versus caregiving
Cognitive Development
Language
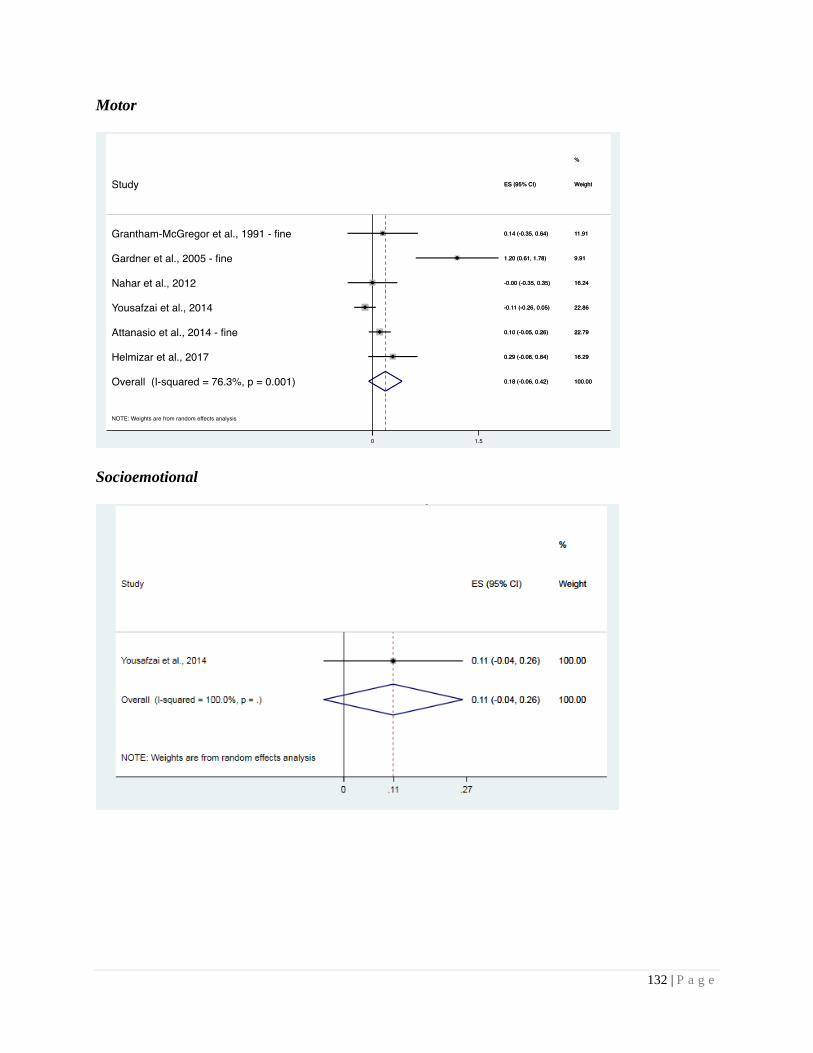
132 | P a g e
Motor
Socioemotional
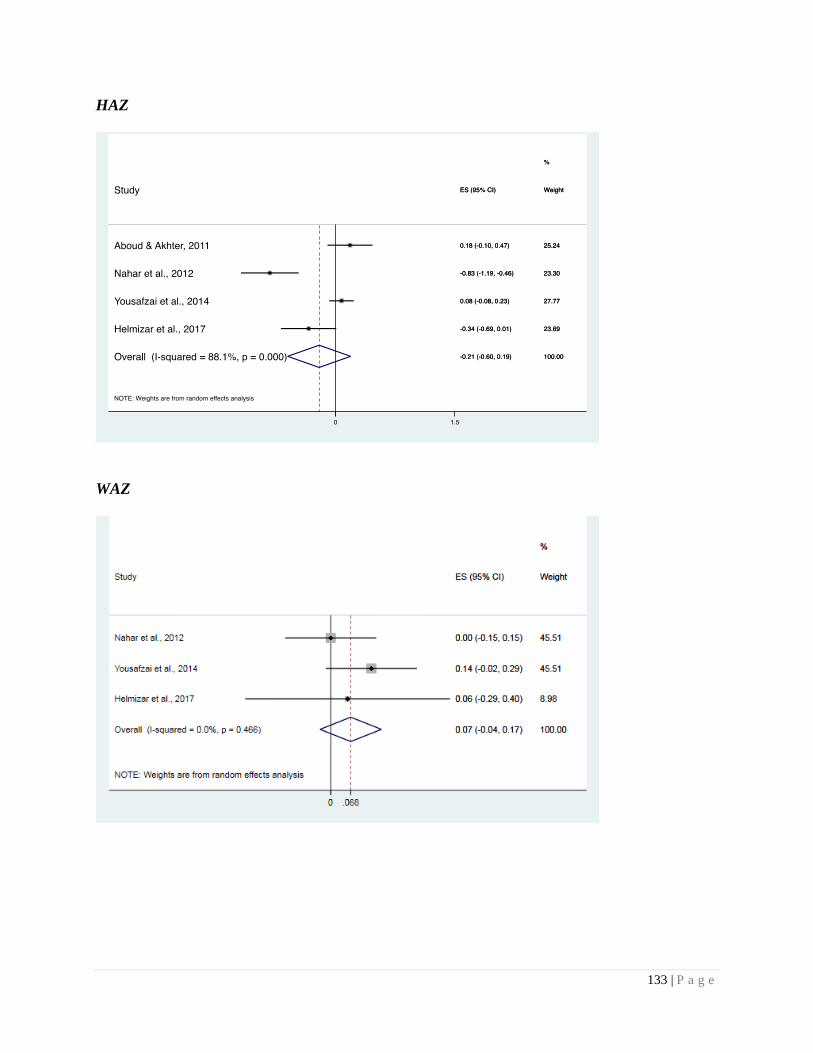
133 | P a g e
HAZ
WAZ

134 | P a g e
WHZ