Embed Size (px)
Citation preview

Document of The World Bank
Report No: ICROOOOl490
IMPLEMENT A TION COMPLETION AND RESULTS REPORT (TF-54404)
ONA
GRANT FROM THE WORLD BANK IRAQ TRUST FUND
IN THE AMOUNT OF US$25.0 MILLION
TO THE
MINISTRY OF HEALTH OF THE REPUBLIC OF IRAQ
FORAN
EMERGENCY HEALTH REHABILITATION PROJECT
Human Development Sector MNC02
December 31, 2010
Middle East and North Africa Region
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

ARADO BOQ EHRP EMS ER ESSAF FMA FMR HNP IBRD ICB IDA ILO IQD IRFFI ISN ISR ITF KPI MA MIM MOF MOH MOPDC NCB PDO PIM PMT PP SBD SOE SWIFT TA TES TOR
CURRENCY EQUIVALENTS
(Exchange Rate Effective 12/03/2010)
Currency Unit = Iraqi Dinar Iraqi Dinar 1,000 = US$0.85 US$ 1.00 = Iraqi Dinar 1,157
FISCAL YEAR
January 1 - December 31
ABBREVIATIONS AND ACRONYMS
Arab Administrative Development Organization Bill of Quantities Emergency Health Rehabilitation Project Emergency Medical Services Emergency Room Environmental and Social Screening and Assessment Framework Fiduciary Monitoring Agent Financial Monitoring Report Health, Nutrition and Population International Bank for Reconstruction and Development International Competitive Bidding International Development Association International Labor Organization Iraq - Dinar International Reconstruction Fund Facility for Iraq Interim Strategy Note Implementation Status and Results Report (World Bank) Iraq Trust Fund Key Performance Indicator Monitoring Agent Master Implementation Manual Ministry of Finance Ministry of Health Ministry of Planning and Development Cooperation National Competitive Bidding Project Development Objective Project Implementation Manual Project Management Team Procurement Plan Standard Bidding Document Statement of Expenses Society for Worldwide Interbank Financial Telecommunication Technical Assistance Technical Specifications Terms of Reference
ii

UNDG UNICEF VO WEI WHO
United Nations Development Group United Nations Children's Fund Variation Order World Bank Institute World Health Organization
Vice President: Shamshad Akhtar
Country Director: Hedi Larbi
Sector Director: Steen Lau Jorgensen
Sector Manager: Akiko Maeda
Task Team Leader: Afrah Alawi AI-Ahmadi
ICR Team Leader: Afrah Alawi AI-Ahmadi
iii
__________ ~_J


REPUBLIC OF IRAQ EMERGENCY HEALTH REHABILITATION PROJECT
CONTENTS
DATA SHEET A. BASIC INFORMATION B. KEY DATES C. RATINGS SUMMARY D. SECTOR AND THEME CODES E. BANK STAFF F. RESULTS FRAMEWORK ANALYSIS G. RATINGS OF PROJECT PERFORMANCEIN.ISRS H RESTRUCTURING I. DISBURSEMENT GRAPH
]. PROJECT CONTEXT, DEVELOPMENT OBJECTNES AND DESIGN ................................................................ ] 2. KEY FACTORS AFFECTING IMPLEMENTATION AND OUTCOMES ............................................................... 6 3. ASSESSMENT OF OUTCOMES .................................................................................................................. ] 6 4. ASSESSMENT OF RISK TO DEVELOPMENT OUTCOME ............................................................................. 2]
5. ASSESSMENT OF BANK AND BORROWER PERFORMANCE .................................. ; ................................... 2] 6. LESSONS LEARNED ................................................................................................................................ 25 7. COMMENTS ON ISSUES RAISED BY GRANTEElIMPLEMENTING AGENCIES/DoNORS ............................... 27 ANNEX]. PROJECT COSTS AND FINANCING .............................................................................................. 28 ANNEX 2. OUTPUTS BY COMPONENT ........................................................................................................ 29 ANNEX 3. ECONOMIC AND FINANCIAL ANALYSIS ..................................... : ............................................... 36 ANNEX 4. GRANT PREPARATION AND IMPLEMENTATION SUPPORT/SUPERVISION PROCESSES .................. 37 ANNEX 5. BENEFICIARY SURVEY RESULTS ..................................................................... ; ......................... 39 ANNEX 6. STAKEHOLDER WORKSHOP REPORT AND RESULTS .................................................................. 40 ANNEX 7. SUMMARY OF GRANTEE'S ICR AND/OR COMMENTS ON DRAFT ICR ......................................... 4] ANNEX 8. COMMENTS OF CO FINANCIERS AND OTHER PARTNERS/STAKEHOLDERS ................................. 52 ANNEX 9. LIST OF SUPPORTING DocUMENTS ....................................................................................... : .... 53 ANNEX] O. THE MASTER IMPLEMENTATION MANUAL (MIM) AND THE PROJECT IMPLEMENTATION MANUAL (PIM) ....•..•.•.•.•••.•.......•..•..••...........•.•....•..••••.......•••••••••••••.•..••.••••••••••••.••••.•.••..••..•••...••...........•.•.• 54 ANNEX] ]. WORLD BANK ITF - FIDUCIARY MONITORING AGENT - TERMS OF REFERENCE (JANUARY 2010) - PROCUREMENT AND FINANCIAL MANAGEMENT SERVICES .......................................................... 56 MAP IBRD 33422 .................................. : .................................................................................................... 66
iv


'Country:
12/3112010
Lending Instrument: 'ERL
Original Total lCommitment:
USD25.0M
Revised Amount: iUSD 23.8 M
iICR Type:
Grantee:
IDisbursed Amount:
lCore ICR
iMINISTRYOF IHEALTH
iUSD23.8M
Envi~~n~~~~~~at~g()ry-=-.!J... , ____ .'_._. __ . __ .. _.'_ ... ________ . ___ ... _~ ___ , ________ ... , __ ." ...... _ .. ____ , .......... " .. :Implementing Agendes: Ministry of Htlfllth
Co finanders and Other External Partners:
Process
Concept Review:
Appraisal:
Approval: "
0911512004
10/09/2004
1113012004
;q!:~~~_tiIT[~=E~~';,· C.I Perf{)rmance Ratillg~y"~R Outcomes:
Risk!() Development qut~~me: , Bank Performance:
Process
:Effectiveness:
Original Date
..
Revised 1 Actual ,D8:!~(s)
12/03/2004
Mid-term Review: 04/04/2007 04/04/2007 ....... ¥- "
.j~I~~~!l~: """ . . ",}~/~y~~~~ ...... , ... ~~28/2010
"'.~()~tl!/:l!(l!y~~t.isf~~!°r:¥._,_ .. ,.". :Substantial
••• _-' ,.", u __ " " "_" '_.' ... ",' __ ._~" •••••• _ • ..,. __ ••• ~" ~.".h •. _ 0' ~" __ " __ ~._ ~ .~.~~ ~._ ,",,~ .~"=_ .. _. ~ ... _~~~-. ._ .".",.~ ",_ ... _. "_M" •
. "." .... __._.}~~(l!~~!y_~~!~~f~~~,_ ... __ ._.___,, __ .. _._ .... _ ....... . Grantee Performance:, . ... ................ _ .. __ ._ .... , . __ ._~~d.(lI!~~~_~.~~!~f!!:~!~!Y_. __ .. ___ ,._. ___ ."."._. __ ._ ..... .
. . ....•...• ". ..". ." __ . ., ..... "."._ ._'" __ ." ___ .'.'''' ... ". . .•. _~._ ... _._ .•. __ ... H" __ "_' .•. _ .•.. __ ._._~. __ ~. ____ .... _._"h .... _~ .... _.". ___ .• _v •• __ •• ____ ~._ ••• h_.h._." .... ~. __ . ____ " __ .. h ... __ .. __ . ___ ._" .. _. _____ .. <"'._~." •.....
C.2 Detailecl Ra~ngs of Bank and,~r~'\Ve!'_~~~".I!!l.n,~~J~Y~~:l!l, .. """ ... , ... ", . . ...... _, __ ~~!1,~., __ ,_ .. ,. __ ." .. _____ ~~!'JI~ __ .. ," .... _____ . Bo~~!....._. ____ ._.~ti~~,, __ . __ __
Quality at Entry: ModeratelySatisfactory:9ove~"nt: !M<Xierately Satisfactory
Q ). fS .. 'M diS . &. 'Implementing M diS . &. . ua lty 0 upervlslon:. 0 erate y atislactory:A encylA encies: : 0 erate y atlslactory ..g,..S ..
Overall Bank Moderately satisfactory 'pOvrfieraU Borrower !Moderately Satisfactory Performance: ; e ormance:
v
Actual
Sec!or CodeJas 0/0 of t~tal BanJ(. .. f!~~!1~!!1gL_. _."_ ... ,, ... __ . __ . ___ .............. _._ ........ _ ... __ ....... _. __ .......................... _ .. Health 100 100
.!!t_t:!!I~_~~~~_l~_'Y.!.~_!.~~t~.~~.!l!<!n~.~~!l!gL_~ ____ . ___________ ~_._ .. , __ ._. ___ ~_. ___ ._.~_,~_ .
... ~.~~I!E:_sl~!~~P~!i()~~E~~_._ .... ________ ~_. ________ .~ _____ ~ __ !~ ___ ~_~ ______ .~. __ ~~Q ___ ~._~, ____ _
Country Oirector: IHedi Larbi . Joseph P. Saba •• ".. • ••• ' •• ~ _~ " •• _ ......... _ •••••• _ >, .. ", , ...................... _.~ •• _ ._ ••• _ ..... _ '" ..... ~e··· "._ ," __ ... __ .... ____ .• _ ... _"". __ • __ ._ .. __ .H •.•. _ ...• _. " ___ •• _ .• _ •.. ___ "'--..•.. __ "__,"_ ... ___ ._._. " __ '_'_', __ .••• H ______ "_._.,_h ......... _" ••.••. _. __ ... __ .••. _. _ .....•
Se~tor MaJla~er: Akiko ·~~e.~tl. ____ ~~ .. _ .. ____ . ___ .. ______ .. _~.t\~~()_Mf:le~f:l_. _._.. . ...
P~oject Team Letl~~!:._._ !\r~!i~ .. ~!~~!~!:~I!l~~~. ______ . __ ._}_~~~!~91:!~~~~_~~~ . _____ _ ICR Team Leader: Afrah Alawi AI-Ahmadi
ICR Primary Author: 'Paul Geli
F. Results Framework Analysis
Project Development Objectives (from Project Appraisal Document) The objective of the Project is to improve access to quality emergency services in selected health facilities to serve the urgent needs of the Iraqi population.
Revised Project Development Objectives (as approved by original approving authority)
Not Applicable
VI

(a) PD~ Indicator(s)
Indicator 1
Value
Indicator 2
Indicator 3
Value (quantitative or
Indicator 4
of emergency units rehabilitated (Re: component 1 on rehabilitation
o 12 9
works contracts for Yarmouk, Ramadi and Baquba hospitals were ",,"'L"''''''"'Y,I a drug warehouse was added to the scope of works.
emergency equipment packages procured for the facilities 1 on rehabilitation of nrl,nMI"V
12 13
exceeded because an emergency equipment package was given also to the facilities that were not rehabilitated with the ITF Grant.
emergency pharmaceutical packages nrr."II'r",d and distributed (Re: IPnrnnr\n .. ,nt 2 on of essential em,erl1enc~v
o 12 13
fFnrlf'!rl7p.llC!V pharmaceutical packages were distributed to 13 emergency units. I,..."."IE'VP", actual procurement was for 30 generic pharmaceuticals only, instead
the 58 that were
See comments
3 separate training activities, 47 physicians and 60 nurses and paramedics trained on emergency medical services.
vii

management of EMS (Re: component 3 on
See comments
two physicians were trained in EMS management. Only two physicians (renlam on duty; the others have left.
of MOB staff trained in health planning, management and 3 on
Not specified See comments
MOH staffs were trained on health sector reform and sustainable financing, 16 PMTIMOH staffs were trained on procurement and financial
Indicator 7 management team inside the MOB with the capacity to prepare,
monitor and manage project activities (Re: component 4 on project
Not applicable See comments
attendance at training courses, on-the-job training and interaction with and FMA staffs, PMT capacity has been considerably strengthened.
G. Ratings of Project Performance in ISRs
DateISR Actual
No. DO IP Disbursements Archived (USD millions)
1 04/27/2005 Satisfactory Satisfactory 0.03 2 07/2112005 Unsatisfactory Unsatisfactory 0.09 3 10/29/2005 Unsatisfactory Moderately Satisfactory 0.38
4 06/1312006 Moderately
Moderately Satisfactory 0.82 Unsatisfactory
viii

5 11110/2006 Moderately Unsatisfactory
6 ; OS/25/2007 Moderately . Unsatisfactory
7 11130/2007 Moderat~ly Satisfactory 8 OS/24/2008 Moderately Satisfactory 9 12/27/2008 Satisfactory 10 OS/26/2009 Satisfactory 11 12/23/2009 Satisfactory
H. Restructuring (if any) Not Applicable
I. Disbursement Profile
Moderately Unsatisfactory
Moderately Unsatisfactory
Moderately Satisfactory Moderately Satisfactory Moderately Satisfactory Moderately Satisfactory Moderately Satisfactory
- Original ---- Formally Revised -- Aaual
1.55
3.64
8.37 11.96 14.00 16.87 20.09
30-r----------------------------~------~--~--~--~---~~
25
20
i 15 I '" 10 11\ =
5
0 N 3 N 3 a 3 N 3 S 3 a "" 3 .... t:I t:I C'i t:I t:I 11'1. 11'1 lei lei .... .... .. .. 0\ 0\ • • • .... • • • • • • • • • •• .... .... .... .... • • • • • • • • • • • • • • N N N N N N !"'II !"'II N !"'II N N N !"'II
ix


1. Project Context, Development Objectives and Design (this section is descriptive, taken from other documents, e.g., PADI/SR, not evaluative)
1.1 Context at Appraisal (brief summary of country and sector background, rationale for Bank assistance)
1.1.1 Abundant natural and human resources enabled Iraq to attain the status of a middleincome country in the 1970s. Since that time, successive wars and a state-dominated economic system have stifled growth and' development and debilitated basic infrastructure and social services. International trade sanctions imposed in 1991 took a toll on the economy. At the time of appraisal of the project, Iraq's human development indicators were among the lowest in the region despite the country's rich resource endowment. In addition to a complicated political transition, Iraq needed to rebuild social cohesion and implement an economic transition from a centrally planned economy to a diversified market economy. It was particularly important to mitigate the temporary adverse effects of the political and economic transition on the poor and vulnerable.
1.1.2 A Needs Assessment covering fourteen sectors carried out in 2003 by the World Bank and United Nations Development Group (UNDG) estimated that Iraq required about US$36.0 billion for reconstruction over four years. At an International Donors' Conference for Iraq in Madrid on October 23-24, 2003, donors expressed support for the Needs Assessment and pledged about US$32.0 billion for the four-year period covered by the Needs Assessment. Donors also asked the World Bank and UNDG to set up an International Reconstruction Fund Facility for Iraq (IRFFI) to ensure swift, flexible, and coordinated donor financing for priority investments consistent with the Needs Assessment. IRFFI comprised two trust funds-a World Bank Iraq Trust Fund (ITF) and a UNDG Trust Fund.
1.1.3 Once considered one of the best in the region, the Iraqi health system had suffered the consequences of three major wars, inappropriate policies, poor management and the absence of adequate resource allocation. The health system's physical infrastructure was suffering from severe deterioration due to neglect over time and consequences from the' war and looting, whereby most of the health infrastructure was in poor condition and was critically lacking essential equipment. Also, the Ministry of Health (MOH) capacity to formulate and implement policies, and manage the provision of basic services was very weak. Substantial investments were urgently needed to build up a sufficient capacity at the central, Governorate, and district levels.
1.1 4 According to the 2003 UNICEFIWHO Health and Nutrition Watching Brief, Iraq had the region's second-highest infant mortality (83/1,000 live births in 2002) and underfive mortality rates (117/1,000 in 2001), a stark reversal from the improvements in the late 1970s and early 1980s. During the 1990s, maternal mortality grew close to threefold (it was estimated to be 300 per 100,000 live births), with an estimated 30% of women giving birth without a qualified health worker in attendance. '
1

1.1.5 In a meeting in July 2004· between the senior staff of the MOH and the donor community (World Bank, UN agencies, and some bilateral agencies), the following twelve priority areas were identified by the Ministry: (i) pharmaceuticals, vaccines and medical equipment; (ii) emergency medical services; (iii) essential infrastructure rehabilitation; (iv) health information system; (v) communicable disease control and surveillance; (vi) communication equipment (hardware); (vii) capacity building and human resources development; (viii) communication and health promotion strategy for the health sector; (ix) health management; (x) primary health care; (xi) food safety; and (xii) donor coordination. Given the situation in the health sector, the Minister of Health requested assistance from the World Bank in addressing the most urgent rehabilitation needs to strengthen the Iraqi health system and increase its capacity to alleviate the currently soaring infant.and maternal mortality rates. Areas of priority would include: (a) hospital rehabilitation, particularly Emergency Services capabilities and provision of essential emergency equipment and pharmaceuticals; and (b) capacity-building and training ofMOH staff.
1.1.6 In January 2004, the World Bank's Board of Executive Directors discussed an Interim Strategy Note of the World Bank Group for Iraq and authorized the Bank to act as administrator of the World Bank Iraq Trust Fund. The strategy focused on: (i) building Iraqi capacity which was urgently needed for the reconstruction program; (ii) preparing and implementing emergency operations to generate employment and restore essential infrastructure and services; and (iii) laying the foundation for the medium-term program, through studies and policy advice. The strategy relied on the World Bank Iraq Trust Fund (ITF) to finance projects, and on Bank budget for the economic and sector work and policy advice needed. A~cording to the Technical Annex on the Project, in addition to· rehabilitating much-needed health facilities, the Emergency Health Rehabilitation Project (EHRP) would be used to establish a model for planning, procurement and financial management within the health sector. It would also allow for the development of a stan.dardized approach to rehabilitation of health facilities and would constitUte the most effective way for the MOH to acquire the capacity it needs to manage longer-term reconstruction and rehabilitation activities. The amount of the ITF financing fot. the EHRP was modest, compared· to the substantial amounts to be provided by other inte~ational donors to finance some of the other priorities of the health sector identified by the MOH. .
1.2 Original Project Development Objectives (PDO) and Key Indicators (as approved)
1.2.1 The Project Development Objective (PDO) was to improve access to quality emergency services in seleCted health facilities to serve the urgent needs of the Iraqi population. The wording of the PDO· in the Trust Fund Grant Agreement and the Technical Annex was the same.
1.2.2 The Technical . Annex and the Project Grant Agreement listed the same Key Performance Indicators (KPI), as follows:
2

Rehabilitation of priority emergency services in 12 hospitals a. Number of emergency units rehabilitated. b. Basic emergency equipment packages procured for the facilities rehabilita~.
Provision of essential emergency drugs c. Basic emergency pharmaceutical packages procured and distributed.
Capacity-building and training of MOB staff d. Number of training activities conducted on emergency medical services (EMS)
for facility EMS staff. e. Number of staff trained in management of EMS. f. Number ofMOH staff trained in health planning, management and procurement.
Project management g. Project management team inside the MOH with the capacity to prepare, issue,
monitor and manage project activities.
1.3 Revised PDO (as approved by original approving authority) and Key Indicators, and reasons/justification .
1.3.1 The PDO was not -revised.
. 1.4 Main Beneficiaries, (original and revised, briefly describe the ''primary target group" identified in the PAD and as captured in the P DO, as well as any other individuals and organizations expected to benefit from the project)
1.4.1 According to the Technical Annex, the benefits of the project were expected to be substantial, as the Project would address urgent needs in the health sector in an environment of devastated infrastructure, deteriorating quality, and escalating requirements. It was estimated that approximately 14.5 million persons living in the surrounding areas of the rehabilitated facilities would have access to high quality emergency medical services that otherwise would not have been adequately delivered. .
1.5 Original Components (as approved)
1.5.1 The Project comprised four components, to be implemented over a period of up to 24 months. It was fully funded as a Grant under the World Bank Iraq Trust Fund (ITF), operating under OP 8.50, Emergency Recovery Assistance. Annex 2 provides detailed information on these four components, which are briefly described below:
Component 1,' Rehabilitation of Priority Emergency Services (estimated total cost US$19.5 million). This component would support the repair, rehabilitation and equipping activities of hospital emergency facilities to restore fully functional emergency services in 12 carefully selected hospitals in 9 Governorates of Iraq. These activities were identified and prioritized using explicit criteria of need, feasibility and affordability.
3

Component 2: Provision of Essential Emergency Drugs (estimated total cost US$3.2 million). This component would support the procurement and distribution of a 3 to 6 month supply of up to 37 essential emergency drugs to be used at the 12 emergency facilities rehabilitated under Component 1.
Component 3: Capacity Building and Training (estimated total cost US$1.6 million). This component would support capacity-building and training activities in Emergency Medical Services for the 12 selected sites. These activities would include: (i) technical training of emergency 5-person teams from each selected site to improve the quality of emergency services; (ii) training in management of emergency services; and (iii) the development of a comprehensive national plan for strengthening emergency health care services. Additionally, the Project would support training to build the general capacity of MOH in health planning and management at both the central and Governorate levels.
Component 4: Project Management (estimated total cost US$O.7 million). The objective of this component was to ensure effective administration and coordination of the project activities. The Project Management Team (PMT) would comprise 11 staff, five of whom would be local consultants hired under the Project.
1.6 Revised Components
1.6.1 The project components were not revised.
1.7 Other significant changes (in design, scope and scale, implementation arrangements and schedule, and funding allocations)
1.7.1 There were changes in the number of hospital emergency units to be rehabilitated with the ITF Grant and in funding allocations. With respect to civil works, the original 12 construction packages became 13 packages with the addition of the rehabilitation of a drug warehouse in Baghdad that was completed in 2007. On the other hand, three civil works contracts totaling US$4.15 million were canceled. In 2006, the civil works contract for the Yarmouk Teaching Hospital (US$1.93 million) was canceled when the Government decided to use its own funds to construct a new emergency unit with a capacity of 75 beds. Although the designs for both hospitals had been completed, the civil works contracts for the Al Ramadi General Hospital (US$I.03 million) and Baquba General Hospital (US$I.19 million) were postponed indefinitely in 2006-2007, and then canceled in April 2007 because of the deterioration in the security situation "in the governorates of Diyala and Anbar. Also, the Suleimaniyah-Jumhuri General Hospital was dropped by the Project in May 2006 when it was converted into a military hospital, but in September 2006, it was replaced by the Suleimaniyah Maternity Hospital. The US$4.15 million allocated for the three canceled contacts were used to cover cost increases due to inflation for the remaining contracts and the cost of the Suleimaniyah Maternity Hospital (US$3.2 million) which was substantially higher than the appraisal estimate for the Suleimaniyah-Jumhuri General hospital (US$0.95 million). " However, as a result of these changes, the total amount spent on civil works contracts was 2.24% less
4

than the appraisal estimate for that category. It should be noted that all 12 selected hospital emergency units (including the ones that were not rehabilitated with the proceeds of the ITF Grant) plus the Suleimaniyah Maternity Hospital received the basic emergency equipment packages (medical equipment and medical furniture) and pharmaceuticals, and their doctors and nurses were trained under component 3 of the Project.
1.7.2 Expenditures for goods and consultant services were about the same as the appraisal estimates. There were savings in training (due in part to the fact that Saudi Arabia funded entirely the cost of training 47 physicians in hospital-based emergency physicians training at the King Abdul Aziz Medical Center). On the other hand, the allocation for operating costs was substantially increased because the' original allocation was insufficient to cover all the expenses incurred by the PMT, including travel to Amman; also, the project period was a little more than five years instead of two years. Overall, there was a surplus/saving ofUS$I.16 million that was canceled on September 10,2010. As a result of these changes, there were four reallocations of Grant proceeds: on July 11, 2006; June 21, 2007; June 22, 2009 and February 18,2010.
1.7.3 The table below shows that for the main item~ namely civil works and goods, the actual expenditures were very close to the appraisal estimates:
Category Appraisal Actual Actual; as a % estimates (in US$ of appraisal (in US$ thousands) , estimates
thousands) Civil works 12,915 12,621 98% Goods 8,350 8,371 100% Consultant services 1,767 1,614 91% . Training 1,862 840 45% Operating costs 105 391 372% Sub.;total 25,000 23:837 ,95% Surplus (for cancelation) - ' 1,163 Total 25,000 25,000 100%
1.7.3 Overall, the PDO remained relevant, particularly in the deteriorating security context which increased the need for emergency hospital services. Hence, while there were adjustments in funding, the project scope remained the same and it was determined that there was no need to revise the PDO. However, the February 18,2010 reallocation was processed as a level II restructuring in accordance with the guidelines for Investment Lending Reform.
1.7.4 The closing date of the Trust Fund Grant was extended twice (on July 11, 2006 and June 21, 2007). In both cases, the justification for the extensions referred to the need to provide sufficient time to complete the civil works at the hospital sites, procure the necessary equipment and pharmaceuticals for these sites, and carry out the training
5

activities. During the period 2005 to 2007, the deteriorating security conditions. and MOH leadership vacuum led to considerable delays in project implementation. Ultimately, despite all the difficulties arising from the security problems, the PMTIMOH managed to continue with the implementation of the Project. Therefore, the decision was taken to stay the course and extend the closing date of the Project. The timing of these extensions was also influenced by the closing dates of the World Bank ITF. On July 11, 2006, the closing date of the Project was initially extended from December 31, 2006 to September 30, 2007. A longer extension would have been more appropriate, but at that time, the World Bank ITF closing date was December 31,2007. In June 2007, the World Bank ITF closing date was extended once more to December 31, 2010. At that time, the closing date of the Project was extended a second time to February 28,2010.
1.7.5 The Trust Fund Grant Agreement was amended twice during the project life:
a) Because there was a lack of responsive bidders for pharmaceutical procurement, the MOH decided to procure drugs through the World Health Organization (WHO). On September 16, 2006 the Grant Agreement was amended to include a provision for the procurement of drugs from UN Agencies in accordance with the provisions of paragraphs 3.1 and 3.9 of the Procurement Guidelines.
b) On March 16, 2007, the Grant Agreement was amended to change the deadline for audit report submission from four months to six months after the end of the relevant fiscal year. A six-month deadline for submission of an audit report is
. standard.
2. Key Factors Affecting Implementation and Outcomes
2.1 Project Preparation, Design and Quality at Entry (including whether lessons 0/ earlier operations were taken into account, risks and their mitigations identified, and adequacy o/participatory processes,.as applicable)
Soundness of the background analysis
2.1.1 This project was designed to address 5 of the 12 priority areas articulated by the MOH in 2004. Taking into account the priority areas identified by the MOH and the donor community, the Project would meet several of the urgent needs listed by the MOH in response to the post-conflict situation. The Project would address the following five areas: (i) pharmaceuticals and medical equipment; (ii) emergency medical services; (iii) essential infrastructure rehabilitation; (iv) capacity building and human resources development; and (v) health management.
2.1.2 This Project was prepared in accordance with Emergency Recovery Assistance Procedures (Operational Policy 8.50). 1 The focus on outputs was most appropriate, given
1 OP 8.50 was replaced in March 2007 by OP 8.00 on "Rapid Responses to Crises and Emergencies."
6

the emergency nature of the operation and the short time-line. Conditions in the country were difficult; the Project addressed the most urgent needs to improve health services, and the main concern was to obtain concrete results and to obtain them quickly. In some respects, a reference to outcomes (or, at least, intermediate outcomes) would have been preferable. However, given the security and other risks, the Bank was prudent to limit the commitments to output results because so much else was outside of the scope of influence of the Bank and the MOH.
2.1.3 The detailed information included in the Technical Annex shows that considerable work had gone into the preparation of the Project. Project preparation took into account lessons from the Bank's recent experience in post-conflict countries, such as the importance of designing a simple project that can be quickly and visibly implemented and of including capacity building for the implementing institutions and entities in order to improve their ability to implement current and consecutive programs.
Assessment of project design
2.1.4 The Project was commendably simple and relatively unambitious in scope in response to the difficult conditions in the country at the time of appraisal, as appropriate under the prevailing security conditions and client capacity. On the other hand, the implementation period of 24 months was too ambitious and unrealistic. Even in a much less challenging environment, a limited rehabilitation in 12 sites would not reasonably be expected to be completed within 24 months.
2.1.5 The absence of quantitative targets for some KPIs, as well as the fact that arrangements for monitoring and evaluation were not described in the Technical Annex,2 were weak points of the project design. The linkage between the PDO (referring to "access" and "quality") and the KPIs (based exclusively on "outputs") was relatively weak, especially in the absence of quantitative targets for some KPIs. For this type of emergency project in a fragile state, it would have been better if the PD~ had been based on outputs only.
Government commitment
2.1.6 The Project responded to a request from the Government's health sector leadership at the time and was envisioned as entry to broader discussions on health strategy. The sector leadership was committed to the PDO, and at the time, the MOH had a number of competent and motivated staffwho participated in project preparation.
2 The Bank Task Team had to use a template for the Technical Annex which did not include a section for M&E.
7

Assessment of risks
2.1.7 In designing the Project, the Bank was fully aware of the high security and fiduciary risks and took reasonable actions to mitigate these risks. According to the Technical Annex, the political and security environment in Iraq was very unstable and uncertain, and posed obvious risks to the Project. The identified risks included administration changes in MOH - jeopardizing current commitment to project design and inputs - and deterioration of security conditions, making access by contractors to sites and supervision difficult. To mitigate these risks, the Project had a simple design, and procurement and disbursement arrangements were developed to make implementation as straightforward as possible. The security situation posed the most significant risk for the rehabilitation of the emergency services sites in the 12 selected hospitals. Mitigation measures included the use of local contractors and local Bank staff for supervision. There were also significant fiduciary risks to the Project. These risks would be mitigated through the selection of qualified staff in the PMT, as well as through the use of procurement and financial management consultants to support the day-to-day implementation of the Project. In view of the possible difficulties of making payments to contractors and suppliers, all payments above US$1 0,000 would be made through direct payments by the Bank. Should security conditions prevent access by Bank staff, supervision would be undertaken by independent consultants and Fiduciary Monitoring Agents (FMA) on behalf of the Bank. Financial management, procurement and overall project risks were appropriately rated as high in a detailed and candid section of the Technical Annex. Security conditions turned out to,be much worse than expected originally, but generally the mitigation measures proposed would have appeared adequate at the design stage.
2.2 Implementation (including any project changes/restructuring, mid-term review, Project at Risk status, and actions taken, as applicable)
2.2.1 The grant provided from the World Bank Iraq Trust Fund (ITF) was approved in October 2004 and signed in December 2004 at a time of guarded optimism regarding post-war rehabilitation. However, within six months of approval, security conditions in the country deteriorated dramatically and remained extremely fragile for more than two years. The MOH, which was relatively weak at the start of the Project, became virtually non-functioning. During most of the 2005-2007 period, the PMT was largely unable to communicate with the MOH. Even the Bank was unable to obtain responses to multiple communications during this prolonged period, for understandable reasons, since MOH staff lived in great danger. That danger would have been greatly enhanced by contact with Bank staff. The Bank Task Team and the PMT displayed great courage and dedication during this period, with PMT members literally risking their lives (in 2006, the Deputy Minister of Health was kidnapped and has never been seen again). Conditions started to improve towards the end of 2007 with a change in the leadership of the MOH, and the Project began to be implemented in earnest.
8

2.2.2 The following factors affected project implementation:
a) Terrorism and the critical security situation in the country had a major impact on all aspects of life. Ownership/commitment greatly diminished due to the deterioration of security conditions in many parts of the country, which made it difficult for MOH staff and contractors to move about in the country and carry out their assignments.
b) The volatile political situation during the transitional stage in establishing the new Iraqi Government, and the intense political struggle and instability within the MOH. The continued sectarian conflict had a major impact on the MOH. Between 2003 and 2006, Iraq went through four different governments, with frequent changes in Minister and Deputy Ministers as well as administrative changes at the MOH.
c) Limited communication between the central and regional levels of the MOH d) The presence of coalition forces and the politicization of the Bank image,
identified as allied with the U.S. forces. e) The lack of capacity within the MOH to manage the project implementation. The
MOH possessed technical capacity, although relatively weak, at the outset of the project, but this virtually disappeared for two years because of the security situation and the loss of staff.
f) Staffing of the PMT has been unstable. In addition, because of their limited experience in project management and Bank procedures; PMT staff needed a lot of training. Support to the PMT by senior MOH officials and technical staff has been erratic, in particular during the period 2005 - mid-2007.
g) MOH and PMT lack of familiarity with Bank procedures and guidelines. However, the Project benefited from an excellent Master Implementation Manual (MIM) developed by the Bank to be used by Iraqi Ministries for all ITF -financed projects, and a specific Project Implementation Manual (PIM) for this Project.
h) Delays in the recruitment of consultants, particularly for design and supervision services for facility rehabilitation.
i) The weak capacity of the private sector due to years of isolation, wars and the security environment.
j) Major procurement delays, particularly for pharmaceuticals. k) Recruitment of an international procurement advisor. Cooperation between the
advisor and the PMT produced better results in procurement and in monitoring and reporting.
I) Cash flow problems, since no special/designated account could be established. m) Inability of the Bank Task Team to visit the country and of the PMT to visit the
project sites. However, this shortcoming was offset somewhat by the work of the FMA.
2.2.3 During implementation, the Bank fiduciary staff working on the ground in Iraq, the PMT staff, and the FMA faced very dangerous situations such as: death threats,
9

kidnappings. the constant potential for random hann. or to be uncovered as being associated with an international organization; yet. most still worked with incredible dedication.
2.3 Monitoring and Evaluation (M&E) Design, Implementation and Utilization
M&Edesign
2.3.1 At appraisal. the quality of the results framework to achieve the PD~ was rather low. Although the focus on outputs made sense given the short-time line and the nature of the operation. the linkage between the PD~ (referring to "access" and "quality") and the Key Performance Indicators - KPIs (based on "outputs") was weak. For the rehabilitation of priority emergency services. the target was set at 12 hospitals; the targets for capacity-building and training of MOH staff were not quantified. The arrangements for monitoring and evaluation were not described in the Technical Annex. Although the PMT did not include a specific M&E Specialist. the M&E functions were to be carried out by the PMT Technical Coordinator.
M&E implementation
2.3.2 During implementation. the Bank Task Team helped the MOHIPMT Team to monitor the implementation of the project components through the preparation of detailed output monitoring tables for each emergency unit. This is important for a project focused on outputs. The Technical Coordinator left the PMT in early 2006. and subsequently. the Bank recommended that the MOH contract an M&E Specialist for the Project. but this did not occur. Also. on many occasions. the Bank drew the attention of senior MOH officials to the need to track the project achievements more closely in terms of improvements in access and quality of services, in particular during the mid-2007 period.
M&E utilization
2.33 Monitoring tables were prepared and used by the PMT to monitor the implementation of project components.
2.4 Safeguard and Fiduciary Compliance (focusing on issues and their resolution, as applicable)
Fiduciary Monitoring Agent (FMA)
2.4.1 .When the ITF was created in 2003. the ITF donors required that the Bank, as Administrator of the ITF, engage a Fiduciary Monitoring Agent (FMA). The main purpose. of the FMA was to help the Bank monitor physical delivery/progress, and the recipients' compliance with financial management and procurement procedures. As part of this function, the FMA provided on-the-job training to the PMTs. The TORs of the FMA (January 2010) hired under the ITF to assist the Bank in monitoring the ITFfinanced projects under World Bank management are in Annex 11.
10

2.4.2 The FMA is a Baghdad-based management consultant finn that deploys about two dozen Iraqi professionals (mainly engineers and accountants) recruited from the private sector with experience in procurement and financial management and accounting. The FMA visited all EHRP sites throughout Iraq every month and carried out physical verification with digital photographs of ongoing works and goods supplied and the production of a fact sheet for each contract, alerting the Bank to deficiencies in quality and implementation. The Bank Task Team for EHRP kept close communication with the FMA during implementation, and invited the FMA to participate in all supervision missions. The perfonnance of the FMA, including the quality of the personnel, has improved over time.' .
2.4.3 The work of the FMA has been very beneficial to the Project. The cost of the FMA fluctUated over the years, in the USS200,000-USS250,OOO range, per project per year. This is a substantial amount, which had to be spent since there was no alternative worth considering. The FMA perfonnance demonstrates that, in contexts where the Bank cannot carry out nonnal supervision missions, the Bank can mitigate risks for its program by employing a Monitoring Agent to monitor physical implementation of projects and verify that funds are spent for the purpose intended and in accordance with Bank rules; the detailed TORs should also encourage quality professional advice on technical issues and follow-up until these issues are resolved, rather than simpl~ mechanical reporting.
Procurement
2.4.4 As mentioned above, the Bank employed a FMA to assist in monitoring procurement transactions, including conducting physical checks of all civil works and all deliveries of goods. This 100 percent check done on behalf of the Bank is a very interesting feature of the Project; usually, under the best of circumstances, the Bank is able to check only 15 percent or so of the outputs. The Bank prior-reviewed over 90% of all procurement under the Project, and the remaining contracts were reviewed by the FMA. MOH did not recruit an international finn to assist in procurement as originally planned because of its high cost in such a highly insecure environment; instead, during implementation, MOH recruited an international procurement adviser who, over time, helped produce better results in procurement and also helped in resolving procurement issues with suppliers.
2.4.5 An Independent Procurement Review (IPR) carried out in 2009 did not find any cases of misprocurement, but it identified a few shortcomings, for example, in bid evaluation reports, completion and delivery periods, changes in the substance of bids, and record keeping and filing. The review also commented that the minimum qualifying criteria prescribed in the bidding documents for works were not adequate to ensure that the lowest evaluated and substantially responsive bidder who meets the post qualification test has the required capacity to complete the works in a timely and efficient manner. The Bank staff clarified that, in order to encourage the participation of the private sector which had been weakened by years of isolation, instability and insecurity, the Bank had decided to lower the qualification criteria to allow more competition. This was reflected
11

in the SBDs (small works) included in the MIM3 developed by the Bank for the use of Iraqi Ministries for all ITF-financed projects.
2.4.6 There have been significant gaps between the physical completion of civil works and the physical delivery of goods, and payments to contractors/suppliers. This was due in part to the security problems, as well as inadequate contract management by the PMTIMOH. It contributed to the slow disbursement under the Project and was raised by the Bank as an issue requiring urgent attention by the PMT and the MOR. In mid 2009, somewhat late in the project cycle, the PMT added two more staff for contract management.
2.4.7 Due to a lack of responsive bidders for pharmaceutical procurement, the MOH in March 2007 turned to the World Health Organization (WHO) to procure about US$2 million worth of drugs. However, there were problems with WHO procurement, and only 7 (valued at US$189,0 13) of the originally planned 38 items were finally procured and delivered by WHO. In the meantime, the MOH procurement process managed to meet the emergency pharmaceutical needs, and the MOH· confirmed that it would not require further procurement of pharmaceuticals under the Grant. WHO was asked to refund (to the Bank) the amount that was not utilized under the WHO-MOH agreement but that was already paid by the Bank for the items that should have been procured by WHO. There were significant delays in WHO response, but on September 15, 2009 US$660,626 were refunded to the Bank, and the special commitment issued by the Bank in favor of WHO was canceled on November 30, 2009.
Financial management and disbursements'
2.4.8 According to the Technical Annex, disbursements would be made primarily through direct payment by the Bank to the contractors, suppliers and consultants. Once authorized by the MOH, payments above the threshold of US$1 0,000 would be made by the World Bank directly into the account of the contractor, supplier or consultant in a commercial bank capable of receiving funds transferred from the international banking system. There would be no special/designated account. Payments for the project management component and payments below the threshold of US$10,000 would normally be made by the MOHlRecipient from its own resources. These payments made from the MOHlRecipient's own resources would be reimbursed, on a periodic basis, by the Bank to the MOH upon presentation of proof of payment and a signed withdrawal application.
2.4.9 Financial management (FM) risk mitigation measures described in the Technical Annex were put into place. There were no major changes to FM during project implementation. The absence of a special/designated account was a considerable hindrance for the PMTIMOH during the whole project, because the proposed reimbursement arrangements mentioned above did not work. Since all payments above
3 Volume 3 of the MIM - SBDs - Bid Data Sheet - 3.2a & 3.2c refer to the minimum required annual volume of construction work and to the list of essential equipment to be made available for the contract, respectively.
12

US$10,000 were direct payments by the Bank, the amounts to be deposited in the special/designated account would have been sma1l4 (to cover some expenditure for capacity building and project management) and the risks would have been limited.
2.4.10 The disbursement rate lagged significantly during the project life. The main reasons for the disbursement lag include: (i) slow physical implementation; (ii) lack of capacity within the PMTIMOH for contract management; (iii) lack of familiarity of contractors with internationally accepted business practices, especially the monthly submission of invoices and full documentation of invoices; and (iv) payment delays to contractors due to the weak Iraqi banking system (for example, the PMT had problems with getting accurate contractors' bank account addresses).
2.4.11 The PMTIMOH staffing for financial management was adequate. The FM team consisted of a Financial Officer (FO), an internal auditor and two accountants; the team worked on a full time basis on two ITF-financed Projects (Emergency Health Rehabilitation and Emergency Disabilities). The performance of the financial management team improved during project implementation, and the team did a relatively good job overall. The project FO was the first, among other projects' financial officers, to deal with the problem of delay of receipt of payments in Iraqi Dinars (lQD). Due to the prevailing inefficient banking system in Iraq and the lack of SWIFTS, payments denominated in IQD used to be transferred through many banks in Jordan and Iraq until they reached the project or the beneficiary. The FO took the initiative of establishing contacts at each of these banks and, literally, moving the payments from one bank to another until reaching the project bank account. There was no problem with payments made in US Dollars.
2.4.12 The Fiduciary Monitoring Agent (FMA) that was hired by the Bank for fiduciary purposes was effective. FMA staff visited the PMTIMOH two to three times per month on average to: (i) review the PMT's FMRs and reconcile the PMT records to the Bank records; (ii) monitor unclaimed expenditures; (iii) verify disbursement plan updates; and (iv) provide on-the-job training in FM matters. The FMA included the PMT-prepared FMRs in their quarterly reports, as well as the adjusted FMRs (with their review comments and recommendations for the PMT FMRs). FMRs were usually submitted in a timely manner. The FMA also conducted, on a sample basis, pre-screening and postreview of withdrawal applications for direct payments and reimbursements.
2.4.13 During the project period, there have been issues related to weaknesses in the internal control system of the PMT, budgeting, flows of funds, excessive payment to a contractor, failure of the PMT to reconcile regularly the EHRP records with the Bank client connection, and delays in payments reaching the beneficiary accounts due to weaknesses of the banking system. Most of these problems were progressively resolved thanks to the high commitment and pro-activity of the PMT and FO and the implementation support provided by the Bank Task Team and the FMA.
4 Actually, the payments below US$lO,OOO did not represent more than 3 percent of the Grant amount. S Society for Worldwide Interbank Financial Telecommunications.
13

2.4.14 Financial Monitoring Reports (FMRs) were satisfactory and were submitted in a timely mi:UUler. Audit reports have usually been submitted late to the Bank, but have been unqualified except for 2008. The 2008 audit report was qualified due to identified ineligible expenditures; it had a number of shortcomings (missing elements, instances of inconsistency, inaccurate amounts, as well as incomplete disclosures in the notes to the financial statements) so that the report had to be revised and resubmitted. In its management letter, the auditor made recommendations in order to avoid such cases of ineligible expenditures and other problems in the future. As requested by the Bank, in January 2010 the PMT submitted an action plan to remedy the weaknesses identified by the external auditor. The next EHRP audit report will cover the period from January 1, 2009 up to the closing date (February 28, 2010) plus a 4-month grace period and is be . due by August 31, 2010. At the time of this writing, the audit report has not yet been received.
Safeguards
2.4.15 The project was appropriately classified as B. The Technical Annex had a number of interesting sections and documents on safeguards, including: (i) Environmental and Social Screening and Assessment Framework (ESSAF); (ii) Codes of Practice for Prevention and Mitigation of Environmental Impacts; and (iii) Safeguards Procedures for Inclusion in the Technical Specifications of Contracts. The ESSAF was devised and approved by Bank management in March 2004 to provide practical procedures. of environmental assessment and control to be included in the ITF-financed projects carried out in a "post-conflict" country situation, similar to the frameworks prepared for postconflict reconstruction programs in Afghanistan and Kosovo.
2.4.16 According to the Technical Annex, impacts would be those associated mainly with: (i) rehabilitation works (e.g., safety, dust, noise, waste material, traffic); (ii) provision of sanitary services, water supply and waste management; and (iii) maintenance of facilities. Because of the emergency conditions, the requirement to carry out a limited Environmental Analysis as part of project preparation would be waived but, for subprojects with adverse environmental impacts, a limited Environmental Analysis would be done during project implementation but before sub-project approval. The Environmental and Social Screening and Assessment Framework (ESSAF) outlined the standards to be applied during implementation. The Bank would recruit another Monitoring Agent to monitor environmental and social safeguards for ITF-financed projects, but this did not happen6. Initially, the Bank tried to combine the ESSAF monitoring task with the TORs for the FMA, but this combination proved unfeasible. An attempt to recruit an environmental consulting firm also failed because the proposals that were received were not found responsive. At about the same time (April 2005), an independent review of the Bank project portfolio concluded that ''the project counterpart teams and contractors cannot possibly abide by all the provisions outlined in the ESSAF" and "the Bank should
6 Minutes of Meeting of December 13, 200S chaired by the Country Director of MNC02 on "Iraq - Environmental an!i Social Safeguards Framework".
14
adopt more honest and realistic measures that can be implemented in the current environment". One of the main reasons for this conclusion was that, in fact, the "current environment" was one of an "in-conflict" country rather than a "post-conflict" country, making full application of the ESSAF unrealistic. In April 2006, the Bank approved a revision of the ESSAF to ensure minimum due diligence in managing potential environmental and social risks in IDA- and ITF-financed operations in Iraq. Under the revised ESSAF, Environmental Assessments will be carried out for category "A" projects only; for category "B" projects, environmental mitigation measures will be included, as appropriate, in the technical specifications to be attached to the civil works, goods and services contracts.
2.4.17 During project implementation, attention to safeguards by the Bank and MOH was minimal, perhaps because of the limited involvement of safeguards specialists: the MOH safeguards specialist left after six months and was not replaced; and for most of the project period there was no Bank safeguards specialist assigned to the Project. For several years, the rating for Safeguards in the ISRs was "Satisfactory" despite the fact that the safeguards arrangements were not implemented. PMTIMOH claimed that they systematically monitored environmental issues in their routine assessments of the civil works contracts under the project. On several occasions, Bank supervision missions discussed with PMTIMOH the need for regular monitoring of the civil works rehabilitation sites to ensure that the environmental safeguards (especially with respect to the safe collection and disposal of infectious medical waste) were being followed by the site consultants and contractors and by the MOH. Government appointed the Ministry of Environment to check that environmental requirements were being complied with at the sites. Also, towards the end of 2009, the PMT designated two of its staff to act as Environmental Safeguards Focal Points, to follow up at the project sites with the consultants and contractors to ensure that they were adhering to their obligations regarding the environmental safeguards. Checklist forms for the hospital sub-projects were finally completed and submitted to the Bank in early 2010.
2.5 Post-completion OperationlNext Phase (including transition arrangement to post-completion operation of investments financed by present operation, Operation & Maintenance arrangements, sustaining reforms and institutional capacity, and next phaseIJollow-up operation, if applicable)
2.5.1 The delivery of health services by the MOH is a continuous operation independent of the duration of any project, so that there is not really a need for explicit transition arrangements.
2.5.2 The recurrent costs of the hospital emergency facilities will be met from the MOH operational budget, and do not constitute a sustainability problem. Most of the trained medical staff are back on site and available. Availability of drugs is also not likely to be an issue; during project implementation, the MOH indicated that it had sufficient resources to finance drug procurement and no longer required the Project's support for the procurement of emergency pharmaceuticals. Recent visits to a number of hospitals confirmed that drugs procured by the MOH are available.
15

2.5.3 The Capacity-Building and Training Component was aimed at building capacity, inter alia, for subsequent health projects. During the difficult 2005-2007 period, no meaningful dialogue on health has taken place but, with the progress made by the EHRP and the EDP, there should now be better prospects for a fruitful relationship between the MOH and the Bank.
3. Assessment of Outcomes
3.0 The ICR Template and Guidelines which have to be followed are not appropriate for a project in an in-conflict country. The ICR format. does not lend itself to effectively telling any complex story of project implementation, including the specific pressures and constraints of a conflict-affected situation and a discussion of whether or not the project was worth doing given the risks to the Bank and Government Teams. In assessing the project outcome as well as the performance of the Recipient and the Bank, the format does not facilitate giving adequate weight to the limitations imposed by the insecurity and the volatile political situation. There is a need for a modified version of the ICR format that would be more suitable for emergency projects (OP8.00 Operations) in countries that are in-conflict.
3.1 Relevance of Objectives, Design and Implementation (to current country and global priorities, and Bank assistance strategy)
3.1.1 The objectives, design and implementation of the Project were and remain highly relevant to Iraq's priorities to rebuild its essential infrastructure and services. The difficult situation in many areas of Iraq pointed to the need for more effective emergency services, and this need continues to exist at present. The objectives are also consistent with the Interim Strategy Notes (lSN) for Iraq. The third ISN, which is dated February 19, 2009, covers the period FY lO-FY 11 , and envisages three thematic areas of engagement, the first theme being continuing support to ongoing reconstruction and socio-economic recovery efforts. That theme responds to the goals of the International Compact with Iraq (ICI) which are related to Iraq's reconstruction and recovery efforts. Activities under this theme will support Government policies and public investments that will help restore and modernize Iraq's physical and human capital. The Bank program will be decided through Annual Business Planning (ABP) exercises to support reforms and/or sectors for which "champions" have been identified, and when there is a commitment to engage with the Bank Group to achieve concrete results on the ground.
3.2 Achievement of Project Development Objectives (including brief discussion of causal linkages between outputs and outcomes, with details on outputs in Annex 2)
3.2.1 In this emergency project to be implemented quickly in a difficult country context of post-conflict, or even in-conflict, the focus on outputs was the right approach. In the PD~ wording, the terms ''to improve access to quality emergency services in selected
16

health facilities" meant ensuring the availability of rehabilitated health facilities with equipment in place and operational, pharmaceuticals delivered, and the trained emergency room staffing provided. The KPIs based on outputs are thus proxy indicators for "access to quality emergency services". This is in line with Iraq's priorities to rebuild its essential infrastructure and services, and with the ISN approach.
3.2.2 Annex 2 provides detailed information on all outputs. The Project's achievements have been substantial for the most important part of the Project, namely the rehabilitation and equipment of priority emergency services.
a) The target of 12 has been met, and even exce.eded for Component 1 on the rehabilitation and equipment of hospital priority emergency services. This is the most important project component, which accounts for over 80 percent of project costs. The ITF Grant financed the civil works rehabilitation of only nine units. However, basic emergency equipment packages were procured, delivered and installed for 13 emergency facilities: the 12 units that had been selected originally (including the ones that were not rehabilitated using the ITF Grant) and the Suleimaniyah Maternity Hospital that was added in 2006.
b) Thirty generic pharmaceuticals were procured and distributed, compared to the 37 that were planned and listed in the Technical Annex. Drugs were made available to 13 emergency facilities. There were adequate supplies of drugs available in the hospitals visited after project completion.
c) Doctors and nurses of the 13 emergency facilities benefitted from the training provided under Component 3 of the Project. The training activities are swnmarized below. As there were no quantitative targets set for training, it is not possible to determine whether satisfactory achievements were met in quantitative terms. However, a significant number of staff were trained in relevant areas, and many have been retained in their positions.
• In three separate training activities, 47 physicians and 59 nurses and paramedics were trained on emergency medical services (EMS). Of the 47 physicians trained, 43 have been retained by the facilities, and of the 59 nurses trained, 52 have been retained by the facilities (most of the non retained physicians and nurses are still in their jobs as emergency health care providers but in other, non targeted facilities).
• Twenty two physicians were trained in EMS management. Six physicians are still in the job; the others have either left, or do not have the responsibility of managing Emergency Services.
• Four MOH staff were trained on health sector reform and sustainable financing, and 16 PMTIMOH staff were trained on procurement and financial management; hence capacity in project management has been built in the Ministry.
3.2.3 The rehabilitation of all the selected hospital emergency units has been completed, the medical equipment and furniture have been delivered and installed, and the pharmaceuticals have been delivered and consumed. All the completed emergency room facilities have been handed over to the MOH. After the completion of the Project, the PMT and the FMA, with some participation by the Baghdad-based Bank team, visited
17

seven rehabilitated hospitals7 to assess how the emergency units (EUs) of these hospitals are functioning. The PMT and the FMA were able to obtain some information for five EUs only: Al Kindi TH, Kirkuk GH, Al Hussien GH, Al Kharkh, and Sulimanyah Maternity. The visits confirmed that those EUs are functioning, with an adequate supply of drugs and trained staff, and equipment in good condition. The major complaint from the hospital staff is that in some cases, the design could have been improved to allow for a better use of the space for efficient flow of patients8. However, in general, the hospital managers and EU staff acknowledged that the Project improved the response to emergencies, particularly in areas of the Baghdad and Kerbala governorates where most of the violence and emergency cases occurred. The table below shows the increases in the' numbers of patients for the five EUs.
Hospital EU Number of EU patients Number ofEU patients before the rehabilitation after the rehabilitation
(per year} (per year} Al Hussain TH 8,000 110,000 (1) Al Kindi TH 38,981 44,220 Al Kharkh 19,572 n.a. (2) KirkukGH 83,973 85,110 Sulimanyah Maternity 28,657 13,201 (3)
(1) This number includes visitors from outside Karbala during the religious events. (2) Started in 2010 (3) For 5 months only (from May 1 to September 30,2010) corresponding to about 31,700 on an annual basis.
3.2.4 In the implementation of the training component, MOHIPMT emphasized the need for the staff that has been trained to continue to work in the hospitals that have been rehabilitated and equipped in order to transmit their knowledge to others working in the same facilities or fields. In one of the hospitals (Yarmouk in Baghdad), the newly trained emergency physicians are training their colleagues in new approaches and techniques. Building on the newly acquired knowledge and skills of those physicians who have received training abroad, MOH intends to move ahead with the Training of Trainers (TOT) approach within Iraq, beginning with the project-related hospitals.
3.2.5 In addition to supporting the expansion of the EU capacity in the selected sites and improving the quality of emergency services more generally, the Project built the technical and management capacity of the MOH. The PMT staff training played an active role in building their capacities and expertise and contributed to tangible improvements in project implementation. Through attendance at training courses, on-the-
7 Some hospitals ceuld not be visited because of security and accessibility issues. The hospitals visited were: AI· Kindi Teaching Hospital, AI Karkh General Hospital (both in Baghdad), Rizgari Teaching Hospital (ErbiJ governorate-KRG), Kirkuk General Hospital, AI Hussien General Hospital (Karbela governorate) and Sulimanyah Maternity Hospital (Sulimanyah governorate) and Samara General Hospital (Salahuddin governorate). 8 Some hospital managers and EUs mentioned that it would have been better if the EU and hospital engineers had been consulted during the design stage about the specific needs and requirements of the facilities.
18

job training and interaction with Bank and FMA staff, PMT capacity has been considerably strengthened.
3.3 Efficiency (Net Present Value/Economic Rate of Return, cost effectiveness, e.g., unit rate norms, least cost, and comparisons; and Financial Rate of Return)
3.3.1 During preparation and appraisal, limited attention was given to financial and economic aspects, given the emergency nature of the operation and taking into account the country context. The Project was prepared as part of the interim strategy of the World Bank in addressing the pressing needs of the sector and according to the emergency recovery assistance procedures (OP 8.50). The lack of reliable statistics, the limited economic information, and the speed with which the Project was prepared have prevented more detailed analysis, a familiar constraint in such operations. However, the benefits of the Project's investment were expected to be substantial compared to its costs, as it addressed urgent needs in an environment of devastated infrastructure, deteriorating quality, and escalating needs.
3.3.2 No economic evaluation of the Project has been carried out upon its completion, and none is planned. This is an area where Iraqi expertise is not strong, so that if such an evaluation were to be carried out, it would have to be done by an external specialist; this is not possible for the time being because of the continuing security situation.
3.3.3 As noted in the Recipient's ICR (Annex 7), the majority of the goods were procured under International Competitive Bidding (lCB). There were an acceptable number of bidders for each contract, and the ICB method enabled the PMT to attract better firms, qualities and prices. Unfortunately, the ICR mission could not obtain information on the efficiency9 of the health facility rehabilitations financed by the ITF Grant. In the circumstances, although there is no reason to believe that Iraq did not also get good value for money for the facility rehabilitation, the rating for efficiency is: "Not rated".
3.4 Justification of Overall Outcome Rating (combining relevance, achievement ofPDOs, and efficiency) Rating: Moderately Satisfactory
3.4.1 After the collapse of the regime in 2003, Iraq was at the early stage of emerging from a prolonged period of wars, United Nations sanctions, military occupation, transitional government, and instability and uncertainty. The country faced an extremely difficult security environment which had major impacts on all aspects of life, including the implementation of reconstruction and development projects. The Bank fiduciary staff working on the ground in Iraq, the PMT staff, and the FMA faced unbelievable situations, much worse than what was expected at the time of project design. In addition, years of isolation and instability led to weak implementing capacity by the Government (including weak capacity to make decisions) and the private sector. Thus, the Iraq context
9 For example, comparisons with the costs of similar rehabilitations carried out under other projects.
19

is a unique situation that needs to be acknowledged and considered in any evaluation of the Project. The performance of both the Bank Task Team and PMT staff has been truly remarkable; they have worked under conditions of great danger and stress.
3.4.2 The Project's objectives, design and implementation were and remained highly relevant to current country priorities and the ISN. The outputs for the most important part of the Project (the rehabilitation and equipment of hospital priority emergency services) have been substantial. The investment improved the quality of the emergencies services in the selected facilities, which are already treating an increasing number of patients. The capacity built in such a low capacity context was also a great achievement. ThC? information on outcomes is good, but unfortunately it is limited. Although many physicians, nurses and paramedics have been trained, it is difficult to assess the achievement for training because there were no defined quantitative targets. In view of this slight shortcoming, the overall project outcome is rated "Moderately Satisfactory."
3.5 Overarching Themes, Other Outcomes and Impacts (if any, where not previously covered or to amplify discussion above)
(a) Poverty Impacts, Gender Aspects, and Social Development
3.5.1 The context in which this emergency project wllS designed did not lend itself to an elaborate consideration of social issues. Project interventions targeted the whole population around the selected hospitals and ensured access to quality emergency services for this population.
3.5.2 Throughout the Project, the Bank monitored closely the security situation and intensity of violence. Two hospitals were removed from the Project because of the security situation. One further hospital was removed when it was converted into a military hospital, but it was replaced by a maternity hospital. The project intervention in that maternity hospital enhanced the quality of Emergency Obstetric Health, benefiting women.
(b) Institutional Change/Strengthening (particularly with reference to impacts on longer-term capacity and institutional development)
3.5.3 .The reconstruction effort may not have led to the establishment of a sustainable model for planning, procurement and financial management, as was envisaged at appraisal. However, it did allow for the development of a standardized approach to the rehabilitation of health facilities and proved to be an effective way for the MOH to acquire the capacity it needs to manage longer-term reconstruction/rehabilitation activities. The Bank was the only development partner that worked through Iraqi institutions, which did help to build institutional capacity and was appreciated by Iraqi officials.
20

(c) Other Unintended Outcomes and Impacts (positive or negative)
3.5.4 Although this may not have been entirely "unintended", the Project's successful completion has paved the way for the Bank's future dialogue with the Iraqi authorities on health. Albeit as a short term response to an emergency, the Project has an added value beyond the project "outputs". It has a demonstration effect, proving the reliability of partnership with client; it provides the foundation for a subsequent engagement on a longer term basis.
3.6 Summary of Findings of Beneficiary Survey and/or Stakeholder Workshops (optional/or Core ICR, required/or ILl, details in annexes)
Not applicable
4. Assessment of Risk to Development Outeome Rating: Substantial
4.1 The survey of project sites showed that the emergency rooms are operational and treating patients; they are adequately staffed with trained personnel, the equipment is working, and operating budgets and pharmaceuticals are available. Based only on these considerations, the risk to development outcome could be assessed as "low". However, the situation in Iraq remains fragile, and' there is a risk of collapse for lack of security. The ICR rates the overall risk to development outcome - i.e., the risk that development outcomes will not be maintained - as "Significant".
s. Assessment of Bank and Borrower Performance (relating to design, implementation and outcome issues)
S.l Bank Performance
(a) Bank Performance in Ensuring Quality at Entry (i.e., performance through lending phase) Rating: Moderately Satisfactory
5.1.1 The Bank strategy in Iraq was to ensure Iraqi ownership and strengthen institutional capacity by financing operations that are implemented by Iraqi Ministries and other recipient entities. As noted earlier, for this project, the Bank did a good job on focusing on outputs and assessing risks (although the security situation turned out to be much worse than expected at the design stage). The Project addressed the most urgent needs to improve health services, and the main concern was to obtain concrete results and to obtain them quickly.
5.1.2 The design of the Project was simple and its scope was manageable. A Quality Assessment of L~nding Portfolio (QALP-l) carried out in late 2008, with the final report issued on January 7, 2009, rated the quality of design as "Moderately Satisfactory". The Project was well prepared for an emergency project. The Technical Annex was
21

comprehensive: it included the list of emergency facilities to be rehabilitated and detailed lists of medical equipment, furniture and drugs to be purchased and delivered, as well as information on procurement and financial management arrangements, the prevention and mitigation of environmental impacts, a project implementation schedule and a resultsbased supervision plan. The Project benefited from an excellent Master Implementation Manual (MIM) developed by the Bank to be used by Iraqi Ministries for all ITF-financed projects, and a specific Project Implementation Manual (PIM) for the Project. However, the implementation period (24 months) was too ambitious and unrealistic, the arrangements for monitoring and evaluation were not detailed and the linkage between the PD~ (referring to "access" and "quality") and the Key Performance Indicators - KPIs (based on "outputs") was weak.
5.1.3 The ICR rates the Bank performance in ensuring quality at entry as "Moderately Satisfactory" .
(b) Quality of Supervision (including of fiduciary and safeguards policies) Rating: Moderately Satisfactory
5.1.4 The Bank Task Team for this project has worked under difficult conditions with great stress. Its ability to respond to implementation problems was constrained by the security conditions on the ground which prohibited on-site supervision, and the team had to operate from Amman, with the PMT and MOH staff traveling to Amman. Also, Bank efforts were not productive when the MOH was nearly paralyzed for more than two years.
5.1.5 The main strengths of Bank supervision were the following:
a) To substitute for the lack of on-site supervision, the task team made good use of the FMA, which was working on all ITF-financed projects, by maintaining close communication with the FMA personnel during implementation and inviting them to participate in all supervision missions. In addition to its primary function of helping the Bank conduct its fiduciary oversight, the FMA provided technical assistance to the Project.
b) Overall, the Bank task team paid good attention to financial management and procurement aspects of the project, with extensive coverage in the aide memoires and ISRs. (i) The level of Bank attention to financial management was noteworthy. Constant attention to training off site of project financial management staff ensured progress was made, even if there were times when results were slow in reporting and audit submission. The Bank's follow up through the FMA on control procedures, fixed asset verification, and SOE payment verification under the US$10,000 level has been essential in risk mitigation. (ii) Adequate attention was also given to procurement. The Bank provided regular off-site training to PMT staff in procurement procedures and contract management. After the failed attempts to recruit an international procurement firm for PMT, the task team succeeded in getting agreement of
22

MOHIPMT to recruit an international procurement advisor with considerable expertise. The Bank's procurement staff was able to support and monitor procurement. One case of fraud and corruption was well handled by the task team (sent to INT and followed up with the PMT); the Bank task team also followed up on a few cases of complaints. Following delays in the procurement of pharmaceuticals through WHO, the task team took appropriate actions to solve the issue by realigning the procurement arrangements through the use of shopping and direct contracting of the items in question.
c) Through the preparation of detailed outputs monitoring tables for each emergency unit, during implementation the Bank Task Team helped the MOHIPMT Team to . monitor the implementation of the project components. This is important for a project focused on outputs.
5.1.6 The shortcomings of Bank supervision were the following:
a) Less than satisfactory performance on oversight of safeguards - environment issues (See Section on Safeguards).
b) Limited focus on sustainability. A greater focus on sustainability did not happen because of the Government situation ( throughout the escalation of violence period)
c) On many occasions, the Bank drew the attention of senior MOH officials to the need to track the project achievements in terms of improvement of access and quality of services. However, efforts to find out how the hospital emergency units were functioning were limited during the life of the Project, and a survey had to be undertaken after the project's closing date.
5.1.7 The Barik constantly monitored the security situation and intensity of violence. Within the limitations imposed by existing constraints, the task team was alert to the weaknesses in governance. Management gave high priority to this project, and invested a great deal of time in assisting the task team. The budget was appropriately large for this difficult project (US$253,000 for lending and US$888,000 for the five years of supervision) and was put to good use. There has been excellent continuity in staffing with the appropriate skills mix, with the original task team leader remaining involved in the Project. In aide memoires and ISRs, the candor, degree of detail, and meticulous reporting of project progress or lack thereof were of high quality. However, the ratings for DO and IP were somewhat generous for 2006 and 2007 (they should have been "Unsatisfactory") and, in the absence of evidence, the rating for Safeguards (environment) should have been "Unsatisfactory" or, at best ''Not Rated". The Quality Assessment of Lending Portfolio (QALP-l) carried out in late 2008 rated the quality of Bank supervision as "Moderately Satisfactory", and the panel commended the Bank Staff Team for its overall performance under extremely difficult circumstances.
5.1.8 Based on the above strengths and shortcomings, the Quality of Bank Supervision is rated "Moderately Satisfactory".
(c) Justification of Rating for Overall Bank Performance Rating: Moderately Satisfactory .
23

5.1. 9 The overall Bank performance in supporting the MOH's priorities is rated as "Moderately Satisfactory", given the same rating for both quality at entry and supervision.
5.2 Borrower I Recipient Performance
(a) Government Performance Rating: Moderately Satisfactory
5.2.1 To assess the Government performance, one needs to distinguish between three different periods in the project life; (i) the preparation/appraisal stage and the project launch; (ii) the 2005 to end of 2007 period; and (iii) the period from end of 2007 to project closing.
5.2.2 During preparation and appraisal and the project launch, with respect to the ownership and commitment of the Government, the Project was a high priority for the MOH leadership. Although relatively weak, MOH did possess a reasonable level of technical capflcity at the outset of the project and was able to make a meaningful contribution to project preparation. It was a time when one could be optimistic about the Iraq post-war rehabilitation.
5.2.3 Soon after approval, MOH was engulfed and engaged in the sectarian conflict and barely functioned for a prolonged period (2005 to end of 2007). The initial capacity in MOH virtually disappeared, and the Ministry was nearly paralyzed for a period of more than two years. The MOH leadership was seriously affected by the political context, and this resulted in periodic gaps in leadership at the Minister and Deputy Minister level. Even when present, they were often unable or unwilling to provide the leadership required for project implementation. Little was accomplished during those years. The priority given earlier to the Project by MOH leadership declined substantially in the politically fluid context and extreme security conditions. During that period, the PMT, as well as the Bank, were unable to communicate with the MOH.
5.2.4 Starting in late 2007, with the appointment of new leadership in the MOH, the Project began to implement more smoothly, due to the increased attention of the Ministry leadership (both the Minister and the Deputy Minister for Donor Affairs) and the stability and growing effectiveness of the PMT which had gained experience in project management. However, MOH's effectiveness at resolving issues in a timely manner remained weak throughout the project period.
5.2.5 The positive role of the PMT (which was a requirement for ITF-financed projects) is an important feature of the Project. The PMT staff were employed and paid by MOH at regular salary levels, thereby avoiding the disadvantages of project units which would erode civil service institutional capacity over the medium and long term. When security conditions in the country deteriorated dramatically, the PMT staff displayed great
24

courage and dedication, literally. risking their lives to carry out their duties (in 2006, the Deputy Minister of Health was kidnapped and has never been seen again). .
5.2.6 With Bank support, the MOHIPMT Team was able to monitor the implementation of the project components on the basis of detailed outputs monitoring tables for each emergency unit. On the other hand, going beyond the focus on outputs, the MOHlPMT efforts were limited dUring the project life to track the project achievements with respect to access and quality of services.
5.2.7 Because of the instability within the MOH during the 2005-2007 periods and the lack of security in the country, it took more than five years (and not two, as planned) to complete the project. But, in the end, the project was satisfactorily completed despite all the problems and difficulties. The Quality of Implementation by the BorrowerlRecipient is rated "Moderately Satisfactory."
(b) Implementing Agency or Agencies Performance Rating: Moderately Satisfactory
5.2.8 The implementing agency was the MOH. Since the MOH is part of the Government, the assessment ofits performance is included in 5.2 (a) above.
(c) Justification of Rating for Overall Borrower I Recipient Performance Rating: Moderately Satisfactory
5.2.9 Because of the very fragile political and security context, the Government performed poorly in the early years of the Project. With the stability in the MOH leadership and the increased capacity of the PMT in project management, the situation improved significantly in the last two years. On balance, the Overall BorrowerlRecipient Performance is rated "Moderately Satisfactory."
6. Lessons Learned (both project-specific and of wide general application)
(1) A review should be carried out by the Bank as to whether, in evaluating emergency projects (OP8.00 Operations) implemented in countries that are in-conflict, a different or modified version of the ICR format should be developed that would be more suitable.
(2) It is important for the Bank to "stay the course" with ongoing projects in the face of difficult circumstances, as these instruments are a critical means for building country knowledge and leveraging future policy dialogue.
(3) The Bank should always assume low institutional capacity and high. turnover in a conflict, post-conflict, fragile situation.
(4) In fragile states, the design of e.mergency projects in conflict-affected situations should be very simple, manageable in scope and suitable to context, with a primary focus
25

on outputs. In line with the focus on outputs, the PDO should also be based on outputs only. Safeguard requirements should be simplified and the necessary resources should be applied to satisfy them.
(5) The Bank should support the counterparts in establishing M&E systems and methodology in the context of project design, to ensure effective oversight of their programs. In situations where the project management team is relatively inexperienced, Bank support for monitoring outputs may be very valuable to project management.
(6) In contexts where normal supervision missions are not possible, the Bank can mitigate risks for its program by recruiting a monitoring agent to help in monitoring physical implementation of projects and verifying that funds are spent for the purpose intended and in accordance with Bank rules; the detailed TORs should also encourage quality professional advice on technical issues and follow-up until these issues are resolved, rather than simple mechanical reporting.
(7) The Bank Task Team should keep close communication with the monitoring agent during implementation, and invite the monitoring agent to participate in all supervision missions. This has been good practice for building the capacity of the PMT.
(8) A Master Implementation Manual (MIM) and a Project Implementation Manual (PIM) that provide a clear definition of implementation procedures are important elements for successful projects.
(9) In fragile states where the capacity to implement projects is weak, it is important to assess accurately the capacity of the staff responsible for project implementation in various disciplines in order to plan for a whole gamut of capacity-building activities:
• Build in advisory support early in the project. • Design and conduct workshops in the initial stages of implementation to deal with
procurement, not only procedures and guidelines but also contract packaging and contract management.
• Have frequent intensive implementation support missions with lots of hands on training built in, and also provide implementation support through frequent workshops, video and audio conferences, and e-mail communications.
• Provide periodic training opportunities for project management staff in management and IT skills and in Bank policies and procedures (procurement, FM and environmental safeguards).
(10) The delays encountered in attempting to utilize a UN agency for pharmaceutical procurement are not unique to this operation. The use of such UN procurement systems, which are often promoted as the best approach for emergencies, should be contingent upon a satisfactory assessment of the capacity of the UN agency to deliver on time. Such assessment should be carried out early in the project life.
26

(11) Lessons related to financial management include the following: (i) disbursement mechanisms used by the Bank must be appropriate and efficient (a special/designated account is essential to facilitate the implementation of an investment project); (ii) having disbursements made directly in US Dollars was successful; and (iii) using the payment monitoring sheet helped the PMT in monitoring payment transactions for direct payments, submitted by contractors, suppliers, consultants, until the amounts are credited into beneficiaries' bank account as well as identifying any potential bottlenecks.
(12) In order to implement projects with due diligence and efficiency, the project management team must have the right mix of expertise and the authority to make decisions to ensure satisfactory outcomes.
7. Comments on Issues Raised by GranteelImplementing Agencies/Donors
(a) GranteelImplementing agencies
Regarding quality at entry, the statement in the Recipient's ICR (Annex 7) that "the design of the project at the time of preparation and appraisal was not complete does not seem to take into account the fact that this was an "emergency" project.
(b) Co financiers/Donors
None
(c) Other partners and stakeholders (e.g. NODs/private sectorlcivil society)
None
27

Annex 1. Project Costs and Financing
(a) Project Cost by Component ( in USD Million equivalent)
Appraisal Estimate Actual/Latest Percentage of Components Estimate (USD (USD millions)· millions)
Appraisal
1. Rehabilitation of Priority 21.434 20.556 96%
~mergency Services 2. Provision of Essential
2.911 1.657 57% ~mergency Drugs 3. Capacity Building and
1.669 0.602 36% Irraining 4. Project Management 0.911 0.995 109%
Total Baseline Cost 26.925 23.810 88%
Physical Contingencies 0.000 0.000
Price Contingencies 0.000 0.000
Total Project Costs 26.925 23.810 88%
Project Preparation Costs 0.000 0.000
Total Financing Required 26.925 23.810 88%
(b) Financin2 Appraisal Actual/Latest
Source of Funds Type of Estimate Estimate Percentage of
Cofinancing (USD (USD Appraisal millions) millions)
Trust Fund 25.000 23.810 95%
Government 1.925 Not
applicable n.a.
Comments on "Government financing":
(1) According to the Technical Annex, the percentage of financing by the ITF was 100 . percent for all categories in the allocation of the Grant proceeds. The estimated Government contribution of US$I.925 million included. US$I.8 million for temporary emergency units to be used while existing units were being rehabilitated (component I), and US$0.125 million for project management (component 4). Actually, the Government made available temporary emergency units, as required. It was essentially an in-kind contribution, with very small cash payments.
(2) According to the PMTIMOH, during project implementation the Government spent about US$700,000 for the salaries ofPMT staff.
28

Annex 2. Outputs by Component
Component 1: Rehabilitation of Priority Emergency Services (actual cost: US$20.56 million, or 96% of the appraisal estimate of US$21.434 million)
1.1 According to the Technical Annex, the Project would support the repair, rehabilitation and equipping activities of hospital emergency facilities to restore fully functional emergency services in 12 carefully selected hospitals in 9 Governorates of Iraq. These activities were identified and prioritized using explicit criteria of need, feasibility and affordability listed in the Technical Annex. Repairs and rehabilitation would focus on the priority structural, electrical, mechanical and heating/air conditioning systems for: (a) emergency room reception and administrative counter; (b) triage areas; (c) diagnostic services rooms; (d) patient examination areas; (e) patient wards; (f}minor surgery operating theater; (g) doctors' and nurses' offices and rest areas; (h) nurses' station; (i) emergency drug dispensary; and (j) other support areas (sterilization room, kitchen, restrooms, storage, janitorial space). The Project would also provide the selected facilities with their most urgent needs in diagnostic and therapeutic equipment for emergency services, including specific emergency room equipment. Examples of such equipment that were selected and listed in the Technical Annex (about 20 items ranging from US$360 to US$45,000 had been identified) are: diagnostic equipment, emergency resuscitation equipment, and emergency life support equipment.
1.2 The Project provided financing for the rehabilitation activities, the technical assistance for design and supervision of the sites, and emergency medical equipment and furniture.
1.3 Responsibility for the implementation of this component rested with the MOHIPMT in coordination with the health authorities at the Directorate and hospital levels. Within MOH, the Emergency Medicine Department of the Directorate of Specialized Medical Services was responsible for the rehabilitation activities and the delivery of the medical equipment. The PMT coordinated with this department to ensure that the activities were carried out according to the project implementation plan. To accelerate the start-up process, PMT/MOH hired different consulting firms to prepare the architectural designs for the hospital emergency units. These firms were managed by the MOH Governorate level engineer, in coordination with the hospital management. MOH arranged for the use of temporary substitute sites for the emergency facilities that were being rehabilitated so that the emergency services were not compromised by the project activities during the rehabilitation phase.
Design and Supervision Services (actual cost: US$ 1.303 million. or 98% of the appraisal estimate of US$I.328 million).
1.4 Design and supervision services were procured from local consultants for 9 of the 13 construction packages (including the drug warehouse). No consultancy was needed for Yarmouk Teaching Hospital as the MOH decided to undertake larger scale rehabilitation at Yarmouk with its own funds. However, the Emergency Unit of Yarmouk received medical equipment and training for its staff under the project. Only design services were
29

completed for the two cancelled project sites (Ramadi and Baquba), and the supervision component of these contracts was cancelled. Design services for Al Karkh G.H were completed by a second firm, because the original contract was terminated for lack of performance. The final cost of design and supervision services was US$I.303 million.
Construction (actual cost: US$12.624 million. or 98% of the awraisal estimate of US$12.915 million)
1.5 The original 12 construction packages became 13 with the addition of the Drug Warehouse. Three contracts were subsequently cancelled. Al Ramadi G.H. (US$1.03 million) and Baquba G.H. (US$1.19 million) were canceled because of the deterioration in the security situation in the governorates of Diyala and Anbar, and the Yarmouk T. H. (US$1.93 million) was canceled when Government decided to use its own funds. The US$4.15 million allocated for these three packages were made available to cover cost overrun for the remaining 10 contracts (including the Drug Warehouse). One hospital (Suleimaniyah-Jumhuri GH) was dropped when it was converted into a military hospital, but it was replaced by the Suleimaniyah Maternity Hospital.
1.6 The following 10 contracts have been completed (figures in parentheses are adjusted final contract values including variation orders):
• Al Imam Ali G. H - BaghdadlRisafa (US$1.390 million)
• Al Sadder O. H. - Amara/Missan (US$0.657 million)
• Samarra G. H. - Salaheddin (US$1.326 million)
• Al Hussein O. H. - Karbala (US$1.136 million)
• Kirkuk G. H. - Kirkuk (US$I.053 million)
• Al Kindy T. H. - Baghdad (US$I.385 million)
• Risgari G. H. - Erbil (US$0.960 million)
• Al Karkh G. H. - BaghdadlKarkh (US$I.436 million)
• Suleimaniyah Maternity Hospital (US$3.201 million)
• The Drug Warehouse - Baghdad (US$0.079 million)
30

Medical and Laboratory Eguipment for 13 Hospitals (actual cost: US$5.758 million, or 143% of the appraisal estimate ofUS$4.024 million)
1.7 Forty two generic items of medical and laboratory equipment (891 units) were purchased; 17 generic items were for 12 sites and 25 generic items were for one site (Suleimaniyah Maternity Hospital). Items purchased included cardio respiratory emergency resuscitation kits, lab auto analyzers, ventilators, nebulizers, mobile X-Rays radiographic units, ultra sound scanners, and anesthetic neonatal care equipment. All items were purchased, delivered, installed and tested, and end-users were trained. The total cost of the medical and laboratory equipment was US$5.758 million, distributed as follows (by method of procurement): US$3.538 million under ICB, US$0.034 million under shopping and US$2.186 million under direct contracting.
Medical and Non-Medical Furniture (actual cost: US$0.875 million or 71% of the appraisal estimate ofUS$1.238 million)
1.8 Eleven generic items of medical furniture (821 units) were purchased for 9 sites and 9 generic items (97 units) were purchased for one sit~ (Suleimaniyah Maternity Hospital). In addition, 8 generic items of medical appliances (28 units) were purchased for one site (Sufeimaniyah Maternity Hospital). Items purchased included hospital beds, bedside lockers, patient trolleys, pharmaceuticals cupboards and oxygen regulators. The total cost of the medical and non-medical furniture and appliances was US$0.875 million, distributed as follows (by method of procurement): US$0.613 million under ICB, US$0.134 million under shopping and US$0.128 under direct contracting.
Recapitulation for Component 1: Rehabilitation of Priority Emergency Services
1.9 Civil works activities are completed, the medical equipment and furniture have been delivered and installed, and end-users have been trained. All the completed emergency room (ER) facilities have been handed over to the MOH.
Categories/actual costs USS million Design and Supervision Services 1.303 Construction 12.624 Medical and Laboratory Equipment 5.758 Medical and Non-Medical Furniture 0.875 Total 20.560
Component 2: Provision of Essential Emergency Drugs (actual cost: US$1.656 million, or 57% of the appraisal estimate ofUS$2.911 million)
2.1 According to the Technical Annex, the Project included the procurement and distribution of a 3 to 6 month supply of up to 37 essential emergency drugs to be used at the 12 emergency facilities rehabilitated under Component 1. Categories of essential emergency drugs included the following: (i) general anesthetics; (ii) preoperative
31

medication and sedatives; (iii) anti-infective drugs; (iv) cardiovascular drugs; and (v) oral and parenteral solutions. Procurement and distribution directly to the selected hospitals would be the responsibility of the MOH. The drug lists and quantities had already been prepared and included in the Technical Annex. The pharmaceuticals would be procured through one tender for 1,411,840 units of 36 essential emergency drugs, using ICB procedures, except for one direct contract for the procurement of 427 units of alteplase injection as there is only one manufacturer in the world. Technical assistance would also be provided to assist the MOH to develop an improved drug supply chain for the country.
2.2 The implementation of this component was quite a challenge. PMT tried twice to procure the 36 essential emergency drugs under a single ICB tender with several lots but there were no responsive bidders for all the lots, so that the MOH had to make other arrangements for pharmaceutical procurement, including repackaging the ICB procurement, and procurement through the World Health Organization (WHO) and through shopping and direct contracting. In March 2007, MOH entered into an agreement with WHO to procure about U8$2.1 million worth of drugs, and consequently a special commitment was issued by the Bank in favor of WHO and part of the funds were transferred to WHO. Of the 38 items that WHO had agreed to supply by December 2007, for reasons that are not clear, WHO was able to procure and deliver only 7 itemslO
costing U8$189,014. WHO reimbursed the unused funds after a long delay and the 8pecial Commitment was canceled. Additional contracts had to be arranged due to the urgent need for life-saving drugs in emergency units.
2.3 In the end, the actual procurement was for 30 generic pharmaceuticals only, as follows:
a) 18 generic items (IV fluids and injectables) procured under International Competitive Bidding -- ICB (U8$1.248 million);
b) 2 generic items (injectables) were procured under shopping (8H) method (U8$0.168 million);
c) 3 generic items (injectables) were procured under direct contract (DC) method (U8$0.051 million); and
d) 7 generic items were procured by WHO (U8$0.189 million).
2.4 All pharmaceuticals procured under the project have been delivered to the drug warehouse built in Baghdad using the project funds (see under Component 1) and forwarded to the 13 hospital emergency units; the pharmaceuticals have been fully dispensed. In 2009, MOH officials informed the Bank that the Government was now able to supply the hospitals with the necessary drugs through the MOH procurement process and, therefore, they will not require further procurement of pharmaceuticals under the ITF Grant.
10 Actually, WHO procured 9 items, but two had to be returned because they did not comply with the required validity period.
32

Component 3: Capacity Building and Training (actual cost: US$0.602 million or 36% of the appraisal estimate ofUS$1.669 million)
3.1 According to the Technical Annex, the Project would support capacity-building and training activities in Emergency Medical Services for the 12 selected sites. These activities would include: (i) technical training of emergency 5-person teams from each selected site to improve the quality of emergency services; (ii) training in management of emergency services for the hospital directors, emergency chief doctors, head nurses and central-level emergency services planners; and (iii) the development of a comprehensive national plan for strengthening emergency health care services. Additionally, the Project would support training to build the general capacity of MOH in health planning and management at both the central and Governorate levels. A number of short-term training programs would allow for the constitution of a core group of public health and health management specialists. These trainings would involve MOH staff in these areas from both central and Directorate levels. The project would also provide assistance to the MOH in developing a sustainable plan for procurement and distribution of essential emergency drugs.
3.2 Responsibility for the implementation of this component rested with PMTIMOH in coordination with the Department of Emergency Medicine of the Directorate of Specialized Medical Services. The PMT was responsible for ensuring the provision and coordination of necessary inputs with the relevant departments.
3.3 Activities included emergency preparedness management and technical training of MOH staff. The planned training included 3 programs:
(1) Medical operation department managers training course for 22 physicians, in one batch in August 2006 (US$124,745 for tuition onlyll). The training was provided in Cairo by the University of Maryland. Six physicians are still in their jobs; the others have either left, or do not have the responsibility of managing Emergencies Services.
(2) Hospital-based ER physicians training for 47 physicians from the 12 targeted hospitals, in one batch in February 2008 at the King Abdul Aziz Medical Center (KAMC) in Saudi Arabia. The provider KAMC had been selected following the Bank guidelines, and the estimated cost was more than US$200,000. However, the training was funded entirely by Saudi Arabia. Of the 47 physicians that were trained, 43 have been retained by the facilities.
(3) Hospital ER team training for 59 nurses and paramedics from the 12 targeted hospitals, in two batches in March and May 2008 (US$ 233,160 for tuition only). The training took place in Beirut, and the provider was the American University in Beirut Medical Center (AUB-MC). Of the 59 participants, 52 have been retained by the facilities.
II For the whole project period, travel and subsistence expenses for all the training amounted to US$442,628.
33

3.4. In addition, four participants (2 physicians - one of them was a PMT member - and 2 pharmacists) attended a Flagship Course on health sector reform and sustainable financing at the World Bank Institute (WBI) in Washington in October 2009 (US$12,000 for tuition only).
3.5 In the implementation of the component, MOHIPMT emphasized the need for the staffs that have been trained to continue to work in the hospitals that have been rehabilitated and/or equipped in order to transmit their knowledge to others working in the same facilities and fields. Actually, in one of the hospitals (Yarmouk in Baghdad) the newly trained emergency physicians are training their colleagues in new approaches and techniques. MOR intends to do more by implementing a "Training of Trainers" (TOT) program, building on the newly acquired knowledge and skills of those physicians who have received training abroad. A TOT training program for 12 people was to take place in Saudi Arabia, but it was canceled because of problems with visas, and PMTIMOH could not make alternative arrangements before the closing of the project. MOH still intends to move ahead with the TOT approach within Iraq.
3.6 In summary, most of the originally planned training activities have been completed. Despite the difficulties due to the country situation, the implementation of that· component is satisfactory. However,PMTIMOH could have done more to monitor the impact of the training courses and the whereabouts of the individuals trained.
Component 4: Project Management (actual cost: US$0.995 million, or 109% of the appraisal estimate ofUS$0.911 million)
4.1 Accor4ing to the Technical Annex, the objective of this component was to ensure effective administration and coordination of the project activities. The Project Management Team (PMT) would comprise 11 staff, five of whom would be local consultants hired under the Project. PMT would include: (i) a Project Director to manage and coordinate the implementation of the Project, including liaising with the World Bank and the MOH Departments implementing project components; (ii) a Deputy Project Director to be responsible for day-to-day management of the Project; (iii) a Technical Coordinator to ensure that the technical aspects of the project are being implemented; (iv) a Procurement Officer, assisted by three specialists (civil works, equipment/drugs, and consultant services) to supervise tendering, purchasing and delivery of works, goods and services; (v) a Financial Officer, assisted by an accountant, to maintain project financial records; and (vi) an Administrative Secretary and a Junior Secretary. The PMT would act as both the coordinating unit for technical implementation of the components, and the "business office" for the project. Some selected MOH staff had received training in the areas of procurement, financial management, monitoring and evaluation, and in project management; this training would be continued periodically under the project. There was a Master Implementation Manual (MIM) for the Iraq Trust Fund (ITF), and a Project Implementation Manual (PIM) was being prepared in conjunction with the relevant technical staff in the MOH central and Governorate offices.
34

4.2 In terms of staffing of the PMT, the component was implemented as planned. The MIM and· the PIM which were well prepared and turned out ;to be very useful. On the other hand, the absences of a Monitoring and Evaluation (M&E) person and of clear lines of responsibility for environmental aspects were problems during implementation. It should be noted that, late in 2005, the PMT became responsible for coordinating the implementation of two projects financed by the ITF: the Emergency Health Rehabilitation Project (EHRP) and the Emergency Disabilities Projec~ (EDP).
4.3 The PMT suffered from instability during the early years of the Project, but fortunately the situation improved. Actually, the PMT has been stable for the past two years, and its staff has gained considerable experience in project management. Some of the problems areas are highlighted below.
4.4 Procurement. In the early years of the project, the PMTI MOH encountered some difficulties in dealing with procurement due to lack of familiarity with the international business community and the Bank's procurement guidelines. During the project period, 16 PMTIMOH staff attended a three-week training course in procurement (for civil works, equipment and drugs) and financial management at the ILO center in Turin (US$26,813 for tuition only). This training, together with.the full use of the skills and guidance of the International Procurement Advisor (Consultant), contributed to a noticeable improvement in PMT's performance.
4.5 Monitoring and Evaluation (M&E). The Bank had to remind the PMTIMOH of the importance of monitoring the key performance indicators of the project. Somewhat late in the project cycle, it was agreed that a national consultant would be hired to collect data on the project activities per site, and that these data would be reflected in the monitoring tables. Site visits to the facilities would focus on the implemented activities per project component, including the percentage of utilization of equipment packages, the usefulness of the training, the number of patients before and after rehabilitation, etc. Unfortunately, the recruitment of the consultant could not take place.
4.6 Contract management. The PMTIMOH could have done a better job of managing contracts, many of which involved issues that needed to be assessed and resolved. The Bank urged the PMT to follow each of the contracts closely, with frequent visits to the relevant sites, and more rigorous contract management, with quick resolution of issues that might arise.
4.7 The component financed: (i) minor refurbishment of the PMT offices agreed between the MOH and the Bank; (ii) adequate office equipment and supplies; (iii) technical assistance and training for PMT staff in project management, procurement and financial management; (iv) annual external audit of the project; and (v) operating costs for the PMT, including vehicle and equipment operation and maintenance, communications costs, banking fees, transportation costs, meeting expenses, advertisement fees,and representation.
35

Annex 3. Economic and Financial Analysis (including assumptions in the analysis)
3.1 The Project was prepared as part of the interim strategy of the World Bank in addressing the pressing needs of the sector and according to the emergency recovery assistance procedures (OP 8.50). The lack of reliable statistics, the limited economic information, and the speed with which the project was prepared have prevented more detailed analysis, a familiar constraint in such operations. However, the benefits of the project's investment were expected to be substantial compared to its costs, as it addressed urgent needs in an environment of devastated infrastructure, deteriorating quality, and escalating needs.
3.2 The persons living in the surrounding perimeters of the selected facilities now have access to high quality emergency medical services that otherwise would not have been adequately delivered. However, no economic evaluation of the Project has been carried out upon its completion, and none is planned. This is an area where Iraqi expertise is not strong, so that if such an evaluation were to be done, it would have to be carried out by Bank staff; this is not possible for the time being because of the security situation.
3.3 As noted in the Recipient's ICR (Annex 7), the majority of the goods were procured under International Competitive Bidding (ICB). There were an acceptable number of bidders for each contract, and the ICB method enabled the PMT to attract better firms, qualities and prices. Unfortunately, the ICR mission could not obtain information on the efficiency12 of the health facility rehabilitations financed by the ITF Grant. In the circumstances, although there is no reason to believe that Iraq did not also get good value for money for the facility rehabilitation, the rating for efficiency is: "Not Rated".
12 For example, comparisons with the costs of similar rehabilitations carried out under other projects.
36

Annex 4. Grant Preparation and Implementation Support/Supervision Processes
. (a) Task Team members
Names Title Unit Responsibility/
Specialty lLending/Grant Preparation Jean-Jacques Frere Sr. Health Specialist MNSHD lTask Team Leader Virginia H. Jackson Sr. Operations Officer/Consultant MNSHD Operations
Vasilios C. Demetriou Sr. Implementation
MNSHD Implementation Specialist/Consultant
Mira Hong Operations Officer MNSSP \Operations Emma Paulette Etori Language Program Assistant MNSHD lAcs Nazaneen Ismail Ali Procurement Specialist/Consultant MNAPR Procurement
David Webber Lead Financial Management
LOAG} lFinance Specialist
Hiroko Imamura Sr. Counsel LEGES lLegal
Ayman Abu-Haija Sr. Financial Management
MNACS lFinance Specialist
Ali Awais Legal Counsel LEGES lLegal Stefanie Brackmann Environmental Specialist MNSRE IEnvironment Oroub EI Abed Social Scientist MNSES Social Aspects Monica Larrieu Health Specialist/Consultant MNSHD lHealth Walid AI-Tawil Health Specialist/Consultant MNSHD ilfealth Dick Lindberg Health Facility Planner/Consultant MNSHD Planning Robert Bou Jaoude Sr Financial Management Specialist MNAFM Finance Majed EI-Bayya Sr. Procurement Specialist MNACS Procurement Nancy-Jean Seigel Team Assistant MNSHD ACS
SupervisionlICR Jean-Jacques Frere Sr. Health Specialist MNSHD Task Team Leader Francisca Avodeji Akala Sr. Health Specialist MNSHD rrask Team Leader Afrah Alawi AI-Ahmadi Sr. Human Development Specialist MNSHD riask Team Leader Nazaneen Ismail Ali Senior Procurement Specialist MNAPR Procurement VasiIios C. Demetriou Consultant MNSHD Implementation Majed EI-Bayya ILead Procurement Specialist ECSC2 Procurement Mona EI-Chami Sr Financial Management Specialist MNAFM inance Emma Paulette Etori lLanguage Program Assistant MNSHD lAcs Mira Hong Operations Officer MNSSP Operations Virginia H. Jackson Consultant LCSHH pperations
Nedim Jaganjac Sr Health Specialist ECSHI lHealth Layla Gumer Kuleib ~onsultant MNSHD Operations Antonio C. Lim /Operations Officer ECSS2 Operations Jad Raji Mazahreh inancial Management Specialist MNAFM lFinance Mario Antonio Zelaya Consultant MNSSD Implementation Paul Geli Consultant MNSHD ICR
37

b) Staff Time and Cost Staff Time and Cost (Bank Budlet Only)
Stage of Project Cycle No.ofstaffweeks
USD Thousands (including travel and consultant costs)
Lending FYOS 35 253.38
Total: 35 253.38 SupervisionllCR
FYOS 8 46.57 FY06 69 213.76 FY07 40 198.79 FY08 23 163.21 FY09 21 135.91 FYIO 23 130.21
Total:1 184 888.45
38

Annex 5. Beneficiary Survey Results (ifany)
N/A
39

Annex 6. Stakeholder Workshop Report and Results (ifany)
N/A
40

Annex 7. Summary of Grantee's ICR and/or Comments on Draft ICR
Implementation Completion Report (lCR) EMERGENCY HEALTH REHABILITATION PROJECT (EHRP)
January 2010
Prepared by the Project Management Team (PMT) Ministry of Health (MOH)
Republic of Iraq
ACRONYMS
ARADO Arab Administrative Development Organization BOQ Bill of Quantities
ER Emergency Room
ICB International Competitive Bid ILO International Labor Organization
ITF Iraqi Trust Fund IV Intra Venous MOH Ministry of Health
NCB National Competitive Bid PDO Project Development Objectives PMT Project Management Team
TES Technical Specification
VO Variation Order WBI World Bank Institute
WHO World Health Organization
Executive Summary
This report is prepared by Project Management Team PMT/ MOH, to reflect an overview of project implementation experience focusing on the points of strength and weakness confronted by the PMTIMOH throughout implementing the project and the impact of factors Ilffected the progress.
After the recent war Iraq has been confronted. with institutional insufficiencies and infra structure failure, especially in the health sector leading to a deteriorated level in health care and emergency facilities performance and capacities, therefore MOH identified the factors contributing in health status deterioration: poor investment in the health sector, poorly maintained health infrastructure, inappropriate management of the health sector, and unhealthy lifestyles and behaviors.
41
In July 2004 a meeting had been held between MOH senior staff and the donor community (World Bank, UN agencies, and some bilateral), and this meeting yielded fmdings and priorities, the Emergency medical services, pharmaceuticals, and essential infrastructure rehabilitation, medical equipment, and capacity building and human resources development.
Given the situation in the health sector, the Minister of Health has approached the World Bank to request assistance in addressing the most urgent rehabilitation needs of the aforementioned priorities.
Based on the meetings mentioned above, Grant Agreement with amount of $25 million was allocated to MOHlIraq under the Iraqi Trust Fund for an Emergency Health Rehabilitation Project on Nov.30th, 2004.
This report is to demonstrate the activities which actually had been executed under each component of the project.
Introduction
As the Emergency Health Rehabilitation Project comes closer to its completion and closing date, this report is prepared to demonstrate the points experienced throughout implementing the project.
Th~ design of this project was intended to provide key elements needed to administer emergency cases and capacity building necessary for this action by targeted personnel capacity development and compensate the insufficiency in essential equipments, appliances, bed capacity and life saving pharmaceuticals, in accordance to global criteria that suit and take into consideration the hard situation and challenges Iraq encounters.
Furthermore, this project has taken an active role in strengthening practical aspects and familiarity with international work and World Bank guidelines, in addition to direct connection with global institutes and firms by its assorted contextures and expertise which actively enriched PMT's experience in order to transmit this knowledge to MOH.
In addition to providing opportunities to the private sector to take its role in reviving and reconstructing the infrastructure of health sector to achieve merger with the governmental.
Purpose .wad objectives
The main purpose for ~e emergency health rehabilitation project was to address the most urgent rehabilitation needs in order to strengthen the Iraqi health system and increase its capacity to provide more effective and successful health service and to alleviate the public suffer caused by the lag in health sector efficiency, thus enhancing the infrastructure and well-performing health care.
42

The project was proposed to address the most urgent needs of the health sector stemming from years of neglect, the subsequent conflicts and dramatic increases in violence in areas especially after 2003.
In addition, the project aimed to establish a concrete model for planning, procurement and financial management within the health sector, as well as development of a standardized approach to rehabilitation of health facilities and to constitute most effective pattern for MOH of Iraq to acquire the capacity its essential needs to manage longer-term reconstruction and rehabilitation activities.
As of the area of priorities would include:
1. Hospital rehabilitation, particularly emergency· services capabilities and provision of essential emergency equipment and pharmaceuticals.
2. Capacity building and training ofMOH staff.
Project components
The Project comprised four components, being fully funded as a Grant under the World Bank Iraq Trust Fund; the four components are described below:
Component 1: Rehabilitation of Priority Emergency Services
The Project supported the repair, rehabilitation and equipping activities of hospital emergency facilities to restore fully functional emergency services in 9 carefully selected in Iraq. These activities have been identified and prioritized using explicit criteria of need, feasibility and affordability. Repairs and rehabilitation will focus on the priority structural, electrical, mechanical and heating/air conditioning systems for: (a) emergency room reception and administrative counter; (b) triage areas; (c) diagnostic services rooms; (d) patient examination areas; (e) patient wards; (f) minor surgery operating theatre; (g) doctors' and nurses' offices and rest areas; (h) nurses' station; (i) emergency drug dispensary; and (j) other support areas (sterilization room, kitchen, reS1rooms, storage, janitorial space).
The Project also provided the selected facilities with their most urgent needs in diagnostic and therapeutic equipment for emergency services, including specific emergency room equipment. Examples of such equipment selected are: diagnostic equipment, emergency resuscitation equipment, and emergency life support equipment.
The first phase of the reconstruction effort has concentrated on establishment of a . sustainable model for planning, procurement and financial management. Also allowed for the development of a standardized approach to the rehabilitation of health facilities and constitute the most effective way for the MOH to acquire the capacity it needs to manage longer-term reconstruction/rehabilitation activities. In addition, the Project provided financing for the rehabilitation activities, emergency medical equipment and technical assistance for design and supervision of the sites.
43

The number of center allover the country has encountered some factors lead to the reduction and delay in the overall project progress; represented in:
a. Deterioration insecurity situation in some governorates (Diyala and Anbar) caused cancelling these two sites.
b. Utilization and occupation of Sulaimaniya Jumhury Hospital by the military caused replacing the planned work site with SUlaimaniya maternity hospital.
c. Yarmuk hospital was also cancelled due to being included in MOH's plan to be provided with medical equipments and conducting training to its staff.
d. 26% increase in quantities of goods procured for MOH under the project due to the urgent need in ERs.
Component 2: Provision of Essential Emergency Drugs
The Project supported the procurement and distribution of a 3 to 6 month supply of up to 58 essential emergency drugs to be used at the 12 emergency facilities. Categories of essential emergency drugs included the following: (i) general anesthetics; (ii) preoperative medication and sedatives; (iii) anti-infective drugs; (iv) cardiovascular drugs; and (v) oral and parental solutions. This component was supported through the provision of pharmaceuticals.
A number of the items under this component were procured, but there was some hindrance in WHO performance to provide all items agreed to through its agreement with MOH, but WHO failed to fulfill its obligations toward this agreement leading both parties to agree upon partial procurement of the previously agreed items and cancelling the others consequently.
Additional contracts were arranged due to the urgent need for life-saving drugs in emergency units, some of them were implemented under shopping and others were under direct contract, in order to cover this need as much as could.
Component 3: Capacity Building and Training
The Project supported capacity-building and training activities in Emergency Medical Services for the 12 selected sites. These activities included: (i) technical training of emergency 5-person teams from each selected site to improve the quality of emergency services; (ii) training in management of emergency services for the hospital directors, emergency chief doctors, head nurses and central-level emergency services planners; and (iii) the development of a comprehensive national plan for strengthening emergency health care services. Additionally, support training to build the general capacity of MOH in health planning and· management at both the central and Governorate levels. A number of short-term training programs has allowed for the constitution of a core group of public health and health management specialists. The project also provided assistance to the MOH in developing a sustainable plan for procurement and distribution of essential emergency drugs. This component meant to be supported through the provision of technical assistance and training activities.
44

Component 4: Project Management
The objective of this component is to ensure effective administration and coordination of the project activities. The Project Management Team (PMT) comprises staff of local consultants hired under the Project and MOH staff. PMT staff includes: a Project Director to manage and coordinate the implementation of the Project; a Deputy Project Director to be responsible for day-to-day management of the project; a Technical Coordinator to ensure that the technical aspects of the project are being implemented; a Procurement Officer, assi~ted by three staff, to supervise tendering, purchasing and delivery of works, goods and services; a Financial Officer, assisted by an accountant, to maintain project financial records; an Administrative Secretary, and a Junior Secretary to support the needs of the office. Drivers for the project vehicles and a messenger also been hired to support the project.
The component financed: (i) minor refurbishment of the PMT offices agreed between the MOH and the Bank; (ii) adequate office equipment and supplies, and project vehicles; (iii) technical assistance and training for PMT staff in project management, procurement and financial management; (iv) annual external audit of the project; and (v) operating costs for the PMT, including vehicle and equipment operation and maintenance, communications costs, banking fees, transportation costs, meeting expenses, advertisement fees, representation, and office security arrangements.
Financing of the project
The World Bank as a donor and by the grant of $25 million which was expected to be disbursed under the scheduled time line provided its strategy in Iraq to ensure Iraqi ownership and strengthen institutional capacity by financing operations that are implemented by Iraqi Ministries and other recipient entities. And its implementation to be performed and facilitated by trained project management team (PMT) in addition to ensure compliance with fiduciary and other safeguards. PMT would be employed and paid by the implementing agency at regular salary levels, thereby avoiding the disadvantages of stand-alone Project Implementation agency Units, which would erode civil service institutional capacity over the medium and long term.
The project was intended to finance specialized technical support in procurement, financial management, and other areas as needed. In addition, to ensure that the project funds are used for the purpose intended and help carry out project supervision, the Bank to employ two independent firms as fiduciary and safeguard monitoring agents.
As a further compensating control, disbursements will be made primarily through direct payment by the Bank to the contractors, consultants, and vendors. Once authorized by the MOH, direct payments will be made by the World Bank directly into the account of the contractor, consultant, or vendor in a commercial bank capable of receiving funds transferred from the international banking system.
45

the Bank and by the fund allocated to Iraqi Ministry of Health provided the opportunity for the Health Sector to improve the health care in the field of emergency units to support the activity of alleviating the public suffer that affected the health care over decades.
Quality at entry
1. The design of the project at the time of preparation and appraisal was not complete, as regarded to the lack of familiarity with the Bank guidelines as well as weak knowledge in regard to WB methodology, and;
2. There was no sufficient readiness on the part of the Ministry to implement the project due to the hard circumstances at that time in Iraq, but upon the relative security stability during 2007, the MOH (represented by Minister of Health, Deputy Minister for reconstruction and donors affairs, director general of projects directorate & engineering services, and director general of medical operations directorate) provided its complete support and backup to the PMT, in order to expedite the implementation to meet the project objectives.
Project implementation experience described by components
Component 1:
Design and supervision
Throughout implementation several points have been marked, as follows:
1. It's been noticed that some requirements and notes nominated by beneficiaries reveal exaggeration and luxury being incompatible with PDOs if project considered as urgent case (emergency project), imposing several components and finishing points causing some distraction to implementation.
2. Overall security situation, caused in delay and affection to implementation. 3. Lack of consultant and contractors' familiarity with Bank's guidelines. 4. The sites under rehabilitation have been chosen carefully to provide services as
good as possible. S. There was some lag in consultants' performance during preparing VOs and final
measurements, which demands more familiarity with Bank's guidelines on the side of the consultant.
6. It was obvious that in the stage of bidding the offer of the contractor takes higher priority, discarding the most important aspects such as; similar assignments and staff, then to take the bid price as second level priority in awarding criteria for NCB bidders.
46

Goods
Medical equipments: Majority of the goods were procured under (international competitive bidding) ICB method which enabled PMT to attract better firms, qualities and prices, with acceptable number of Bidders for each contract. And the selected specifications were in need for further study,' taking· into consideration some points such as; systems to be closed or open, in addition to consumables prices, being confronted with delays throughout implementation caused by:
a. Lack ofPMTI equipments specialist's familiarity with Bank's guidelines.
b. Lack of familiarity on the side of some suppliers:
c. MOH guidelines of goods delivery, hand-over, inspection reports and acceptance minutes and committee related aspects.
Component 2:
Essential emergency drugs for 12 hospitals
This component has encountered several critical stages, lack of familiarity with Bank's guidelines for some contractors caused failure or delays, in addition to inaccurate implementation for some items' supply even subsequent delays caused cancelling some items accordingly, as elaborated below:
1. 58 life-saving pharmaceuticals had been initially agreed to be procured under this component, the actual procurement was only for 30 generic pharmaceuticals.
2. The procured items were categorized into 10 packages under the following:
a. 18 items procured under International competitive bidding (ICB);
- 9 generic items (IV fluids).
- 5 generic items (injectables).
- 3 generic items (injectables).
- 1 generic item (injectable).
b. 2 generic items (injectables) were procured under shopping method.
c. 3 generic items (injectables) were procured under direct contract method.
d. WHO agreement: 38 items were intended to be procured under this agreement by WHO, in April 2007. Out of these items; only 7 generic items had been procured and distributed, and 2 generic items had been procured but recalled (due to its incompliance with the required shelf-life).
WHO had only procured 7 and apologized for the rest 31 items.
47
e. Meanwhile, MOR resumed supplement of non-procured life-saving pharmaceuticals.
Component 3:
Training
Hospital based physicians and paramedics
It was needed to emphasize on trained staff to work on the profession trained on and to work in the hospitals under rehabilitation, in order to transmit their knowledge to others whom work in the same facility and field. .
The planned training included 3 programs (medical operation department managers training course for 22 physicians in one batch, hospital based ER physicians training for 47 physicians in one batch, and hospital ER based paramedics training for 60 paramedics in two batches). The trainees of the last two programs were from the 12 targeted hospitals.
In addition; 4 participants, 2 physicians (one of them was a PMT member), 2 pharmacists attended Flagship course (health sector reform and sustainable financing) at World Bank Institute (WBI).
PMT capacity building
It was obvious that PMT training played an active role in building their capacities and expertise reflecting tangible acceleration in project implementation pattern.
Component 4:
At early stage of the project the PMTI MOR encountered some difficulties in dealing with Bank's' guidelines due to lack of familiarity with the international business community and procurement guidelines, a number of PMT members had attended training courses at different international institutes including ILO, WBI, and ARADO. Leading to a noticeable enhancement in PMT's performance and the capability to utilize the knowledge obtained through the training which reflected in expediting project implementation per components, and overcome the obstacles hindering the overall progress, in addition to transmit the experience to MOR staff through a PMT core, yielding a more acquainted staffs with the standards of consistent project planning and implementation. .
Financier (World Bank) performance
The World Bank, as the Iraq Trust Fund (ITF) administrator, has supervised ITF-funded operations in accordance with the Bank's applicable policies and procedures. While staff
48

traveling to Iraq was restricted or hard; in regard to the current country circUmstances, supervision of recipient-executed operations been carried out through consultants and the monitoring agents. And in every ITF-funded operation it was required to include a resultbased supervision plan that reflects reality on the ground.
The Bank required a financial statement audit of the ITF to be performed by the Bank's external auditors on an annual basis. The costs of such an audit, including the internal costs of the Bank with respect to the audit, were charged to the ITF. The Bank provided each donor with a copy of the auditor's report. Furthermore, the Bank maintained close consultation and coordination with the donors. And it provided each donor to the ITF with semi-annual reports on its quarterly ex-post evaluation of the activities undertaken by the monitoring agent. Within six months of completion of the activities or of full disbursement of the contributions, whichever comes later, the Bank provided its close support to the PMT by maintaining continuous follow up for each step and level in implementing the project, provided a practical context for the PMT based on international experience of managing projects and works, effectively elevating the level of PMT in administering project components and aspects and ensuring wide-spectrum knowledge to backup its performance.
Factors affecting implementation and outcomes
1. There were several factors affected the implementation were out of the control of the Iraqi government represented by: a. Iraq experienced severe unstable security in years 2005 - 2007 accompanied with
unstable MOH / PMT staff for many reasons mostly related to the security issues, which was the main reason behind the cancellation of civil works in two sites (Baquba, Ramadi) ,and awarding civil works of other sites to the local contractors in spite of their limited experience and non familiarity with the international business community guidelines, unstable security delayed the delivery, installation of equipment and dispensing of pharmaceuticals, PMT faced a lot of difficulties and challenges in implementing the training courses e.g. ( visa, air transportation ) noting that all the training activities implemented outside Iraq, and inability of many trainees to join the training or retained in their sites after training for the same reason. Overall; unstable security situation has prevented WB task team presence in Baghdadi Iraq.
b. Transitional stage in establishing the new Iraqi government, and;
Some factors within the control of the government; Lack of familiarity with Bank's guidelines yielded some disagreements with some ministries and directorates, due to the conflict with Iraqi government's guidelines, such as; refusal to allocate pieces of areas and delays in some governmental procedures.
2. Some factors within the control ofMOH; a. Instability in the framework of MOH. b. Instability in the framework of PMT, and;
49

Factors within the control of PMT; a. Noticeable payment delay related to the lagging of contractors to submit their
payments linvoice periodically based on contract accomplishments, a part from contractor's non familiarity with international banking guidelines and procedures. To minimize this factor, PMT provided continuous site training to the contractors and consultants concerning correct methods for payments claiming, and avoiding further delay.
b. Insufficiency in some hired local consultants' expertise which needed reiterative training to elevate their level of experience to meet the required qualification.
c. Impact due to role of consultants and construction industry in the project implementation.
Despite the aforementioned, no financial or administrative corruption has been noticed throughout the project implementation, and no complaints raised in this regard by the contractors, fiduciary or the Bank.
Lessons learned
By implementing two projects supervised and supported by the World Bank and the international procurement advisor, it would be easier to diagnose more specific points that should lead to a successful implementation for a project:
1. Necessity of complete client involvement during the preparation/design of the project for Bank appraisal, represented by constant members.
2. Applicability of the World Bank's procurement procedures and guidelines have led the PMT to manage the project activities smoothly and motivated MOH to adopt similar methods in the procurement of goods and civil works which reflects the usefulness of familiarity with those guidelines in the international business community.
3. Selection of staff under special criteria of administrational, technical, and professional characteristics, consolidated with authoritative level in order to expedite implementation and facilitating decisions making to insure satisfying outcomes.
4. Outside I Inside PMT and Focal points capacity building in the fields of ( civil works, pharmaceutical procurement, financial and administrative, project and health sector management) were very useful and was one of the Factors that enhanced the project implementation smoothly without influential technical obstacles.
5. Providing essential requirements (such as; location of work, services, means of transportation and communication, and capacity building) to the staff.
6. The periodic supervision missions with the WB task team were very useful for the project reviewing, progress evaluation, solving major obstacles and presented sustainable assistance to the PMT, a part from daily E-mails, correspondences and continuous advisory role of Bank's task team.
7. The necessity of time-scheduled implementation for each item in project components based on consistent time schedule.
50

8. In case of Force Majeure (see factors affecting implementation and outcomes), amendments and addendums for the project time and framework should be preceded by precise calculation for periods needed and the impact expected.
51

Annex 8. Comments of Co financiers and Other Partners/Stakeholders
N/A
52

Annex 9. List of Supporting Documents
a) EHRP - Criteria for Selecting Priority Hospital Facilities for RehabilitationSeptember 3, 2004
b) Iraq - EHRP - E 1 026 - Environmental and Social Screening and Assessment Framework (ESSAF) - 2004
c) EHRP - Environmental Management Plan for Rehabilitation of Emergency Unit Buildings - October 5, 2004
d) Iraq - EHRP - Minutes ofthe Ad Hoc Review Meeting - November 12,2004 e) Project Information Document (PID) - Appraisal Stage - November 19, 2004 -
World Bank Report No. AB1235 f) Agreed Minutes of Negotiations - November 24,2004 g) Emergency Health Rehabilitation Project - Technical Annex - November 30,
2004 - World Bank Report No. T7644-IQ h) Iraq - EHRP - ITF Grant Agreement - Grant Number TF054404 - December 4,
2004 i) Master Implementation Manual (MIM) - ITF - July 2005 j) Minutes of Meeting of December 13,2005 chaired by the Country Director of
MNC02 on Iraq - Environmental and Social Safeguards Framework k) Office Memorandum dated April 21, 2006 from MNSRE (through MNA VP) to
the Managing Director on Iraq - Revision of the Environmental and Social Screening and Assessment Framework (ESSAF)
1) Project Implementation Manual (PIM) - Ministry of Health m) Operational Manual- OP 8.00 - Rapid Response to Crises and Emergencies-
World Bank - March 2007 n) Implementation Status and Results Report (ISR) - Numbers 1 to 11. 0) Aide Memoires of Bank missions for implementation support. p) Fact Sheets - ITF - Projects - EHRP - prepared by Etiman Management
Consulting Services (EMCS) - Procurement Management. q) Iraq EHRP - Quality Assessment of the Lending Portfolio (QALP) - Final Report
- January 2009 r) Interim Strategy Note for the Republic oflraq for the Period Mid FY09-FYll -
World Bank Group Report No. 47303-IQ - February 19,2009 s) Environmental Report for the maternity hospital in Suleimaniyah - by Manager of
Suleimaniyah Environment Directorate - Dec 12, 2009 t) Fiduciary Monitoring Agent (FMA) - Contract No. 8002518 - Modification "L"
- Appendix A - Terms of Reference (January 2010) and Appendix B - reporting Requirements.
u) Implementation Completion Report (lCR) - Emergency Health Rehabilitation Project (EHRP) - January 2010 - Prepared by Project Management Team (PMT) - Ministry of Health (MOH)
53

Annex 10. The Master Implementation Manual (MIM) and the Project Implementation Manual (PIM)
The implementation of the EHRP was facilitated by the existence of two manuals: a Master Implementation Manual (MIM) and a Project Implementation Manual (PIM).
MIM
Designed as a Master Implementation Manual, the MIM was the basis for project specific implementation manuals, such as the PIM, which will regulate and guide project activities funded by the ITF and, subsequently, IDA, in accordance with World Bank guidelines for financial management and procurement.
The MIM aims to:
• introduce good practice; • provide uniform policies and procedures for projects; • encourage transparency, probity and accountability; • facilitate optimum efficiency, effectiveness and value for money; and • ensure compliance with the World Bank guidelines and with the law.
It is organized into three volumes to be of use to different audiences within an implementing agency: line management, project manager, the project management team, and staff (principally financial management and procurement staff) within the agency providing services to the project management team.
The MIM deals with: (i) project set-up and organization; and (ii) procurement and financial management in some detail, including step by step guidance and standard bidding documents, model forms and general conditions of contracts.
PIM
The Project Implementation Manual (hereafter referred to as the PIM) is designed to help the Project Management Team (PMT) to carry out the objectives of the Emergency Health Rehabilitation Project (EHRP). The PIM is designed as a guide to the implementation of the project activities, in particular in the areas of implementation planning, procurement, disbursement and financial reporting. In addition, the Iraq Master Implementation Manual (MIM) is designed to provide guidance on procedures and documentation. However, the most relevant parts of the MIM with respect to this project have been inserted in the PIM for convenience.
The PIM comprises the following parts:
• 1. Introduction.
• 2. The Project.
54

-. 3. Project Management.
• 4. Implementation Details by Component.
• 5. Procurement.
• 6. General Guidance Annexes.
• 7. Overview of Procurement Procedures in the Master Implementation Manual.
• 8. Master Files and Other Relevant Documents & Tools.
The PIM is meant to be a "living" document. During the implementation of the EHRP, it will be useful to update the information in the PIM to adapt to the project as it moves forward, clarifying and improving the procedures described in the document. Changes should be made after consultation with and review by the World Bank, as the administrator of the Iraq Trust Fund, which is providing the grant financing for the project.
This project is the first in the health sector to be financed from the World Bank Iraq Trust Fund (WBITF) within the International Reconstruction Fund Facility for Iraq (IRFFI). The Ministry of Planning and Development Cooperation (MOPDC) is the Government's designated donor coordination agency for Iraq's reconstruction program.
55
Annex 11. World Bank ITF - Fiduciary Monitoring Agent - Terms of Reference (January 2010) - Procurement and Financial Management Services
I. INTRODUCTION
1. In 2003, the International Reconstruction Fund Facility for Iraq (IRFFI) was established to help donors channel their resources and coordinate their support for reconstruction and capacity building development activities in Iraq within its priority program. IRFFI comprises two trust funds: (i) the World Bank Iraq Trust Fund (ITF) administered by the World Bank; and (ii) the UN Development Group Iraq Trust Fund administered by the United Nations Development Programme (UNDP). The World Bank and the UN administer these trust funds in accordance with the policies of their own organization. Close coordination between the two trust funds is to be achieved through a common governance structure, including through a joint IRFFI Donor Committee and Executive Committee. The Donor Committee oversees the activities of IRFFI as a whole and endorses its overall strategic priorities. The Executive Committee is chaired by the Chairperson .of the Iraqi Strategic Review Board (ISRB) and is comprised of the IRFFI Donor Committee Chairperson, and representatives of the United Nations and the World Bank. T?e Executive Committee is responsible for day-to-day management of IRFFI.
II. BACKGROUND
2. The ITF is a multi-donor trust fund; as such, all funds are commingled in one account. The ITF is financed by contributions from the following donors: Australia, Canada, European Community, Finland, Iceland, India, Japan, Republic of Korea, Kuwait, Netherlands, Norway, Qatar, Spain, Sweden, Turkey, United Kingdom, and United States, as well as investment income earned. The ITF finances grants for rehabilitation/reconstruction and capacity building technical assistance projects. While the terms of the ITF allow both public and private bodies to be grant recipients, all of the current recipients are Iraqi governmental agencies, including ministries and the Mayoralty of Baghdad.
3. The ITF has financed 21 grants valued at US$507 million, exceeding donor contributions by US$13 million and committing 103% of donor deposits to projects. Of the 21 grants, 18 are active projects valued at US$447 million; three projects, valued at US$60 million, are completed.
4. The vast majority ofITF projects are implemented by Iraqi agencies (15 out of the 18 active projects, amounting to US$434 million) to help the Government of Iraq (GOI) develop effective institutions to ensure country ownership. ITF projects aim to help the GOI strengthen its institutional capacity to deliver services, utilize its resources in an efficient and transparent manner, and implement key reforms. ITF grants finance textbooks, schools, pharmaceuticals and health clinics, improved social safety nets, water supply and sanitation, irrigation and drainage, electricity, environmental management, private sector development, and banking and public finance management reform efforts. The ITF also finances technical assistance to help strengthen Iraqi institutions develop
56

baseline poverty data, and improve social safety net targeting mechanisms. More information about the ITF-financed projects under implementation and in the pipeline can be found on the website www.irffi.org. Additio.nal projects may be approved depending on the availability of ITF funds.
5. To ensure country ownership and that the ITF finances Iraq's development priorities, the potential recipient submits a proposed project to the Iraqi Strategic Review Board (ISRB). The ISRB is chaired by the Ministry of Planning and Development Cooperation (MoPDC), and is responsible to review all externally financed projects to ensure they are consistent with Iraq's priority program, filling a gap, and not overlapping with other programs. The World Bank appraises and jointly negotiates the project with the recipient and, subsequently, signs a grant agreement with the recipient, which details the scope and conditions for the use and disbursement of funds. The recipient entity implements the project.
6. The World Bank supervises ITF-funded projects in accordance with the World Bank's policies and procedures. Projects financed by the ITF are subject to the same internal controls to ensure that funds are properly used for the purposes intended and that the objectives of each project are achieved. Since the difficult security situation prevents World Bank and ministry staff from freely traveling throughout Iraq to visit project sites, the World Bank employs special measures to mitigate risks for its program in Iraq. One of these measures is the engagement of a Fiduciary Monitoring Agent (FMA) to help the World Bank supervise projects implemented by Iraqi agencies.
7. Typically, the recipient agency establishes a Project Management Team (PM1) to be responsible for day-to-day project implementation, which must be carried out in accordance with the operational procedures specified in the Grant Agreement. For each project, the Recipient must: (i) establish and maintain adequate procurement and financial management arrangements, including the systems for planning, organization and procedures, record keeping. accounting for funds. managing disbursements. and contract management that are documented in the Master Implementation. Manual (MIM); and (ii) appoint competent procurement and financial management personnel to operate the systems. The Recipient is expected to develop institutional capacity project implementation. based on World Bank operational policies and procedures. PMTs should understand that the World Bank procurement procedures are, in fact, a set of procedures and tools of internationally accepted public procurement methods, and are not specifically devised for World Bank financed procurement alone--other multilateral development banks, such as the Islamic Development Bank, use them as well, adapted to their specific requirements.
8. In general; two categories of expenditures are eligible for financing under ITF grants, including: (i) investment and capital expenditures, including incremental recurrent costs related to the supported investment and capital expenditures; and (ii) technical assistance and training programs for Iraq's public and private entities to strengthen the capacity of Iraqi entities and to assist in the preparation of projects/programs. In order to help ensure that the funds are used for purposes intended, in December 2005, in accordance with the World Bank's applicable procurement guidelines, the World Bank
57

engaged Etiman Management Consulting Services (EMCS) as the FMA for the ITF. The FMA verifies the physical implementation of projects and monitors compliance with fiduciary policies, including financial management and procurement procedures. The initial contract covered the period of December 2005 through end-December 2007, which was the initial termination date of the ITF.
9. Following negotiations with EMCS in November 2007, the duration of the FMA assignment was extended for the period of January 1,2008 to December 31, 2010, which was the revised termination date of the ITF. The contract was renewabl~ annually subject to: (i) satisfactory performance on the basis of annual evaluation in the eleventh month of the year; (ii) submission of satisfactory updated technical and financial proposals for the FMA services for the next calendar year; (iii) the ITF remaining in place; and (iv) the continuation of ITF project implementation. (The ITF has since been extended for a second time, and the termination date is now December 31, 2013.)
10. The revised IRFFI Terms of Reference, which were endorsed at the IRFFI Donor Committee Meeting on October 29, 2007, and a sample Financing Agreement between the World Bank and the Recipient are provided separately for reference and guidance in the performance of the FMA assignment.
11. Following negotiations with the FMA in November 2009, the duration of the FMA assignment has been extended for the period January 1 through December 31,
.2010, subject to continuation of the ITF funding during this period.
III. OBJECTIVES OF THE ASSIGNMENT
12. Within the World Bank's overall fiduciary responsibilities as Administrator of the ITF, the FMA's specific assignments will be based on the following general objectives:
(i) To monitor the full cycle of procurement transactions and financial management requirements under each project implemented by an Iraqi agency;
(ii) To support institutional capacity building initiatives of the World Bank to strengthen the fiduciary capabilities of implementing agencies;
(iii) To support the World Bank in conducting its reviews, verification and audits; and
(iv) To report on the status of project implementation and compliance with procurement and financial management procedure to the World Bank.
IV. SCOPE OF SERVICES
A. Financial Management
13. The FMA will have the following dual roles in financial management:
58

(i) The first role is towards the World Bank: through verifying and validating the projects' financial management arrangements and internal controls to ensure that they comply with the World Bank's requirements as agreed the implementing entities.
(ii) The second role is towards the Recipients and the projects financed by the ITF through providing technical assistance/advisory services related to the projects' financial management arrangements and the generation of periodic and reliable financial reports.
14. Specifically, the responsibilities will be as follows:
(iii)Follow-up with implementing agencies to ensure that the preparation of project budgets/disbursement plans are linked to the procurement plans and the projects' closing dates.
(iv)Follow-up with the implementing agencies to monitor individual project accounts and generate timely and reliable reports including the Financial Monitoring Reports (FMRs) and Interim Un-audited Financial Reports (IFRs) that reconcile with their records. Any un-reconciled items should be followed up by the FMA to ensure clearance by the PMTs before submitting the FMRsIIFRs to the Bank
(v) Provide fiduciary technical assistance, advisory support, and on-the-job training to the implementing agencies on project financial management to enable them to manage individual project accounts and generate the FMRslIFRs. On-the-job training will be guided by a regular updated training schedule agreed among the FMA, the implementing agencies and the Bank.
(vi)Perform on site random verification of the projects' assets purchased through ITF funds, and report on the findings. A fixed asset register, listings goods purchased under the project, should be maintained by every implementing agency.
(vii) Familiarize the PMTs with the Bank auditing requirements and support them in performing the auditor's selection process. Follow up with the PMTs on the submission of acceptable auditing reports and the implementation of the auditor's recommendations on the identified weaknesses in internal controls as per the management letters.
(viii) Assist the PMTs with the pre-screening withdrawal applications for reimbursement, replenishments and direct payment transactions, using the World Bank Loan Department pre-screening checklist. Pre-screening will conducted on a sample basis using a risk based approach, to ensure compliance, accuracy and completeness of the information. Report on
59

the pre-screening in the periodic reports prepared for the World Bank and PMT.
(ix) Post-review and follow-up on withdrawal applications for direct payments, reimbursements, and replenishments on sample basis using a risk based approach, to ensure that the associated internal controls had been properly applied and that they are in compliance, and that withdrawal applications are accurate and complete.
(x) Advise the World Bank about any modification, addition or deletion relating to the accounting and financial laws applicable to public sector or state owned enterprises during the assignment.
(xi)Review the projects' bank reconciliation statements, including the Designated Account, and follow up with the PMTs on any outstanding items (e.g. uncleared checks, for which a payment would appear in the PMTs records but not yet in the World Bank statement).
(xii) On a sample basis, monitor payment transactions for direct payments, submitted by contractors, suppliers, consultants until the amounts are credited into beneficiaries' bank accounts, using the PMT's monitoring sheets. (PMTs monitor each payment step against their service standards, from initiating the request to carrying out the technical review, financial management review, obtaining the authorization, and preparing and signing withdrawal application.) Report any excessive delays to the World Bank without waiting for the monthly/quarterly reporting cycle.
Reporting
(xiii) In addition to reporting on compliance with procedures, identifying issues and making recommendations, the FMA should report on the specific actions taken by the PMT to follow up on FMA and/or World Bank team recommendations to resolve previously-identified issues.
(xiv) Information included in the reports should be checked with the PMT Financial Officer for accuracy before sending it to the Bank. However, if this delays the FMA report cycle, the FMA should arrange to meet with the PMT to review the final report after they have been sent to the World Bank and PMT.
15. Work implies frequent interaction with the following:
1. Counterparts in government including PMTs, finance departments of various implementing agencies, procurement staff, and a variety of professional organizations.
60

11. World Bank staff teams in charge of Iraq and whose projects are being supervised.
B. Procurement Management
16. The FMA will have the following dual roles in monitoring compliance with procurement procedures:
1. The first role is towards the World Bank, through monitoring the physical implementation of projects, and verifying that the projects' procurement management and internal control arrangements comply with World Bank requirements.
11. The second role is towards the implementing agency by providing advisory services and technical support concerning procurement management and the generation of periodic and reliable procurement reports.
17. The FMA will monitor the procurement of goods, works, and consulting services to verify that they are in accordance with the World Bank's financial, procurement and audit procedures. The FMA will have access to all documents and accounts of the ITF project held by the implementing agencies. The FMA's specific tasks will include:
(i) Review the adequacy and reliability of the procurement organization of implementing agencies to carry out activities financed under the ITF.
(ii) Familiarize the implementing agencies with the World Bank's standard policies, procedures, and documentation, and provide guidance in implementation, as necessary. Assist them in the use and application of the MIM. Provide on-the-job training that will be guided by a regularly updated training schedule agreed between the FMA, the implementing agencies, and the World Bank.
(iii) Review the implementation of procurement plans of projects, and ensure that the PMTs continuously update them when procurement steps are reached. A model procurement plan for goods, works and consulting services in Excel has been provided separately for PMTs to use to prepare specific project procurement plans.
(iv) Assist the implementing agencies to establish and maintain an adequate procurement filing system, a sample of which is provided separately, and ensure that at least one person is assigned to be responsible for the filing system and is trained to maintain it. Follow-up and report on the status and effectiveness of the PMT's filing.
61

(v) Monitor the full cycle of procurement transactions to ensure that the procurement practices undertaken by implementing agencies are conducted in accordance with the requirements of the Grant Agreement covering the project Report on the reasonableness of prices under the prevailing market conditions, under each project/program.
(vi) Monitor physical delivery of all goods, works and consulting services and acceptance by the recipients. Review the timeliness and completeness of consultants' deliverables.
(vii) Verify if the staff stated in the consultancy contracts are mobilized during implementation of the consultancy assignment, if any consultant staff has been replaced, and if this replacement was approved by the implementing agency as required in the contract
(viii) Follow-up with implementing agencies on the actions taken in response FMA reported weaknesses of supervising engineering firms and inform the World Bank if no action is taken.
(ix) Ensure that implementing agencies establish appropriate linkages between the procurement process and the corresponding withdrawal/disbursement processes, in order to ensure timely payments to contractors, suppliers and consultants.
(x) Conduct, in accordance with the new electronic format provided by the World Bank, ex-post procurement reviews/audits of at least 20 percent of procurement cases for goods, works and services subjected to post-review process under the Grant Agreements even for projects in which there is only one contract. The selection of subprojects for post review shall be geographically distributed.
(xi) Undertake specific procurement reviews as directed by the World Bank in response to emerging needs.
(xii) Provide periodic information to the World Bank on the above as directed in Appendix B (A), and highlight the procurement management risk associated with each project.
v. COMMUNICATION ARRANGEMENTS
18. The FMA's primary contact with the World Bank and evaluating supervisor will be the ITF Program Manager, Mrs. Jane Distelhorst Sansbury ([email protected]) or her designate. In addition, the FMA shall: (i) communicate on the status/issues of projects with the Senior Country Officer for Iraq, Ms. Janet Dooley ([email protected]) and the responsible Task Team Leaders; (ii) discuss FMA findings/recommendations and reports with the Senior Procurement Specialist (Ms. Nazaneen Ali: [email protected] ) and the Financial Management Specialists (Mr. Jad Raji Mazahreh: [email protected] and Ms. Mona El-
62

Chami: [email protected]); (iii) maintain regular contact with the World Bank's Country Manager in Baghdad (Mr. Jean-Michel Happi, [email protected]) and the Head of Mission of the World Bank's Interim Office for Iraq in Amman (Mr. Ziad Badr, [email protected] ); and (iv) provide for half-yearly - or as needed - management visits to the World Bank's office in Amman and/or Washington DC and regular participation of its staff in World Bank supervision missions and workshops with Iraqi implementing agencies.
VI. QUALIFICATION AND ORGANIZATION OF AGENT
19. The FMA will possess adequate knowledge of World Bank policies and guidelines and have sufficient resources, including language skills, to provide the needed support to the implementing agencies and to generate the progress reports.
20. For the implementation of the financial management requirements of the Terms of Reference, the FMA will: (i) employ at all times an experienced financial officer, holder of the CP AfCA title, plus an accountant; (ii) at all times be equipped with an adequate accounting software, capable of consolidating the projects information received from the implementing entities in the form of FMRs; and (iii) be able to generate accurate, reliable, and timely project reports to facilitate effective project monitoring.
21. The FMA has been provided with copies of the relevant documents/publications of the World Bank, e.g., Operational Policy 13.50 (Supervision), 10.02 (Financial Management); Financial Monitoring Reports Handbook; Disbursement Handbook; and the audit policy. For Procurement, Operational Policy 11.00 has been provided. The FMA has also been provided access to relevant documents containing policies of the Government of Iraq.
22. For the implementation of the procurement management requirements of the Terms of Reference, the FMA will: (i) include in its team experts familiar with procurement and with knowledge and experience in policies, guidelines and procedures of the World Bank; and (ii) be guided by the procurement arrangements agreed in projects/programs documents and related grant agreements, "Guidelines for Procurement under IBRD Loans and Credits" (May, 2004) and "Guidelines for Selection and Employment of Consultants by World Bank Borrowers" (May, 2004) and the MIM developed by the World Bank for all projects in Iraq.
23. The FMA shall maintain: (i) A back-up plan in case assigned staff is on leave or not available prior to the expiry date of the assignment; and (ii) Quality assurance arrangements in delivering its work.
24. The FMA is expected to coordinate with the implementing agencies to achieve the scope and objective of its assignment.
VII. REVIEW BY THE WORLD BANK
25. The World Bank will supervise the ITF-funded projects in accordance with the World Bank policies and procedures. The World Bank has the responsibility to perform ex-post evaluation of activities undertaken by the FMA.. The FMA will make available
63

for review by the World Bank or its auditors at any time, all records, accounts and systems used in monitoring the use of grant funds and the activities of the implementing entities.
APPENDIX B - (A) REPORTING REQUIREMENTS
The FMA will be required to prepare and submit, as directed, the following written reports, electronically, to the Iraq Task Team Leaders, and Procurement and Financial Management Specialists, copied to the ITF Program Manager.
I. For Procurement:
(a) Monthly Fact Sheets: the FMA will send Fact Sheets after each site visit, and/or visit to PMTs, in a format agreed with the World Bank, to the World Bank's Task Teams.
Fact Sheets are designed to: (i) highlight project implementation progress and/or deficiencies in contracts for civil works, goods or consulting services; (ii) document delivery of goods and works with digital photographs; and (iii) recommend remedies to correct any implementation difficulties and/or deficiencies so identified.
Fact Sheets should report on: (i) whether difficulties/deficiencies previously identIfied have been resolved; (ii) what actions have been taken to address outstanding issues; and (iii) what action is further recommended. To the extent possible, the FMA should document that the issue has been resolved through digital photographs.
(b) Quarterly Procurement Reports for Projects: The quarterly report should contain: (i) consolidated information on physical progress with related digital photographs; (ii) the projects' procurement progress compared to the agreed procurement plan; (iii) project disbursements compared to the disbursement plan; (iv) the list of site visits carried out during the preceding quarter and planned for the next quarter; and (v) the status of the procurement management risk in terms of "low risk", "moderate risk", "high risk", as explained in the Technical AnnexlEmergency Project Paper
(c) Monthly Consolidated Procurement Report should include: (i) consolidated project "Findings and Recommendations" from the monthly Fact Sheets and PMRs; (ii) the consolidated procurement plan and disbursement status, to be submitted to the ITF Administrator not . later than 15 days after the end of the reporting month; and (iii) the list of site visits carried out during the preceding month and planned for the next month.
(d) Quarterly Procurement Post Review (PPR) reports should be prepared separately (as required in paragraph 18h), in accordance with the new format agreed between the FMA and the World Bank.
64

(e) Monthly Summary of Procurement Progress and Commitments should report on the grant amounts for which tenders have been issued, and the amount committed for each ITF financed project and be submitted not later than 5 days after the end of the reporting month.
(f) Other Reporting: Procurement and/or physical verification issues that require urgent follow-up with the PMTs or the World Bank Task Team will be communicated to the Task Team Leader bye-mail or telephone calls, without waiting for the regular reporting cycle.
II. For Financial Management:
(g) Monthly Consolidated Financial Management Report that reflects figures on monthly and cumulative disbursement, commitments, and unclaimed disbursements, arriving at the World Bank on or before the 15th of the following month.
(h) Quarterly Financial Management Reports will include: (a) the quarterly reviews of the PMTs' Financial Monitoring ReportslInterim Un-audited Financial reports (FMRsIIFRs); and (b) the analysis of cross-cutting issues of financial management in the form of a matrix. The Quarterly Financial Management Reports should arrive at the World Bank 45 days after the close of the quarter (May-August-November-February).
III. The Quarterly Implementation Report will include: (i) an analysis of project issues, recommended steps and solutions; (ii) EMCS's opinion about whether the projects are reaching their stated development objectives and implementation targets; and (iii) EMCS' view on the evolution of cross-cutting issues as identified during the CPPR of May 2009.
All Reports should be succinct and tabularized, based on standardized formats agreed with the World Bank.
65
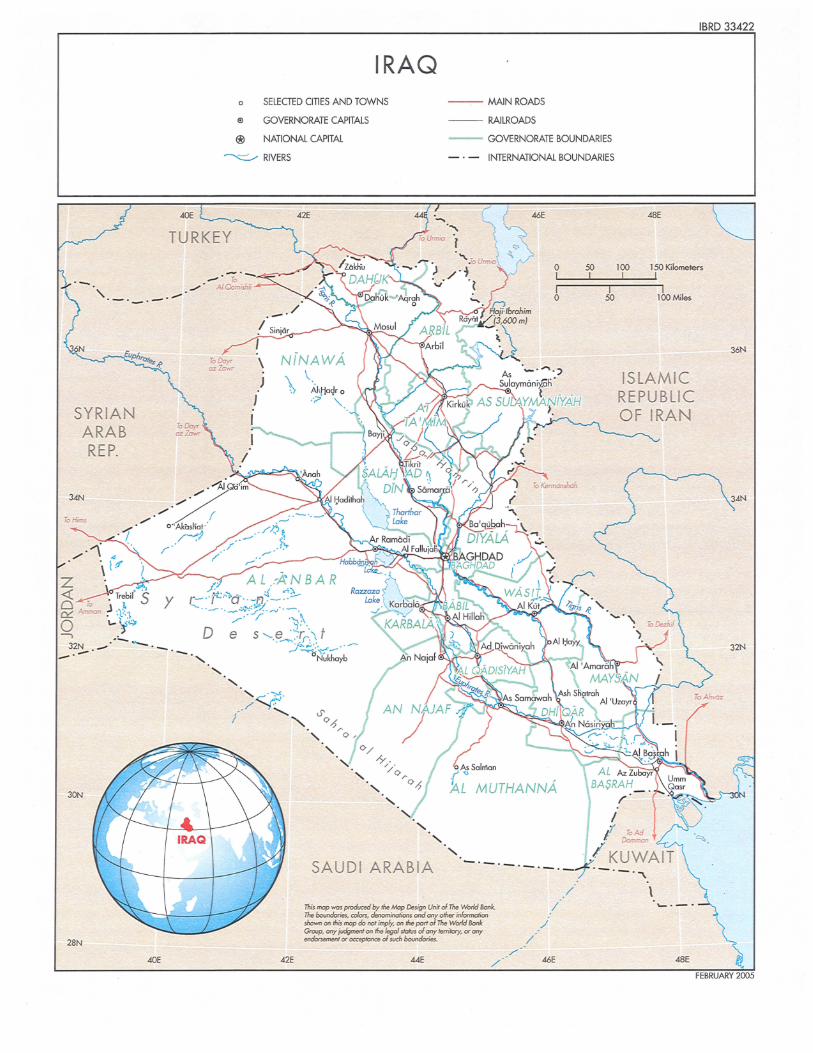
IRAQ a SELEGED CITIES AND TOWNS --- MAIN ROADS
® GOVERNORATE CAPITALS -- RAILROADS
® NATIONAL CAPITAL -- GOVERNORATE BOUNDARIES
~ RIVERS - . - INTERNATIONAL BOUNDARIES
<lOE 46E
TURKEY
_.
SYRIAN ARAB REP.
To Hims
z «~. Trebil' 5 ~ ~n ~ :t\ o \,.. ~">
-.-
y
~ #~ 32N . _ . -. _ . _ -.-
30N
28N
<lOE
./
!~ \ J
J
<l2E
SAUDI ARABIA
1Ioi, map wa, prodvced by the Mop De'ign Unit d The world Bonk. TM boundorie$, ccIon, denominations oncJ any other inFormation shown on thi' map do not imply, on the port of 110. world Bonk Groop, any iudgment on the legal sJctu, d any lerrilory, 01" any endon<ment 01" o<xepIance d such bovndori ...
M E /
/ /'
0 50 I I I I 0 50
/ /
/
46E
IBRD 33422
48E
100 150 Kilometers I I
I 100 Miles
ISLAMIC REPUBLIC OF IRAN
\ \..-. - -
48E
36N
3<1N
32N