Embed Size (px)
Citation preview

Document of The World Bank
Report No: T-7552-AF
TECHNICAL ANNEX
FOR A PROPOSED GRANT
OF SDR 43.7 MILLION (US$59.6 MILLION EQUIVALENT)
TO
THE TRANSITIONAL ISLAMIC STATE OF AFGHANISTAN
FOR A
HEALTH SECTOR EMERGENCY RECONSTRUCTION
AND DEVELOPMENT PROJECT
May 6,2003
Human Development Unit South Asia Region
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
CURRENCY EQUIVALENT (exchange rate i s Kabul based open market buying rate)
effective as o f April 23,2003
A A C A ADB AGO AHEAD ARI ARTF CHCs BFM BPHS cc C I co CDC CHWs DFID DHMT DPT3 FIC G C M U HFA HHS HIV/AIDS
H M I S HNP ICRC IMR IS/NS IDA LIB MICs MMR MPA
Currency Unit - - Afghani U S $ l - 47.3 AFA -
GOVERNMENT FISCAL YEAR
March 21 - March 20
ABBREVIATIONS AND ACRONYMS
Afghanistan Assistance Coordination Authority Asian Development Bank Auditor General Office Afghan Health and Education Assessment for Development Acute Respiratory-tract Infection Afghanistan Reconstruction Trust Fund Basic Health Centers Budget and Financial Management Basic Package o f Health Services ControlKomparison Contracting In Contracting Out Centers for Disease Control and Prevention Community Health Workers Department for International Development District Health Management Team Diphteria/Pertusis/Tetanus Third Dose Fully Immunized Chi ld Grants and Contracts Management Unit Health facility assessment Household survey Human Immunodeficiency VirudAcquired Immunodeficiency Syndrome Health Management Information System Health, Nutr i t ion and Population International Committee for the Red Cross Infant mortality rate International and/or National Shopping International Development Association Limited International Bidding Multi-Indicator Cluster Survey Maternal mortality ratio Minimum Package o f Activities
.. 11
MOF MOH M O H - S M NBF NGO N I D s ORS PCC PHD PPAs
QCBS sws TB TBA TISA TSS USMR UN UNICEF U S A I D WHO
QBS
Ministry o f Finance Ministry o f Health Ministry o f Health Strengthening Mechanism Non-Bank Financed Non-Govemmental Organization National Immunization Days Oral Rehydration Salts Provincial Coordination Committee Provincial Health Director Per formanc e-b as ed Partner ship Age ements Quality Based Selection Quality and Base Cost Selection Safe Water System Tuberculosis Traditional Birth Attendant Transitional Islamic State o f Afghanistan Transitional Support Strategy Under-five mortality rate United Nations United Nations Children’s Fund United States Agency for International Development World Health Organization
Vice President: Mieko Nishimizu Country Director: Alastair McKechnie Sector Manager: Anabela Abreu Team Leader: Benjamin Loevinsohn
... 111


TRANSITIONAL, ISLAMIC STATE OF AFGHANISTAN
HEALTH SECTOR EMERGENCY RECONSTRUCTION AND DEVELOPMENT PROJECT
TECHNICAL, ANNEX
Table of Contents
I . PROJECT DESIGN SUMMARY ................................................................................. 1
II . PROJECT DESCRIPTION AND BENEFITS .............................................................. 6
A . Components in Detail ......................................................................................................... 6
B . Benefits of the Project ...................................................................................................... 12
111 . IMPLEMENTATION ARRANGEMENTS ................................................................. 14
A . Organizational Structure ................................................................................................. 14
B . Implementation Procedures ............................................................................................ 15
C . Procurement ..................................................................................................................... 17
D . Financial Management and Audit .................................................................................. 17
IV . EXPERIENCE OF CONTRACTING WITH NGOS FOR HEALTH SERVICE DELIVERY ..................................................................................................................... 17
V . ENVIRONMENTAL AND SOCIAL SAFEGUARD ISSUES ..................................... 22
APPENDIX I: PROJECT COST BY COMPONENT ..................................................... 23
APPENDIX 2: FINANCIAL MANAGEMENT. AUDIT. AND DISBURSEMENT ARRANGEMENTS ........................................................................................................ 24
iv


I. PROJECT DESIGN SUMMARY
Sector Related Goal: T o improve human development with specific reference to improving the health status o f impoverished people o f Afghanistan.
Project Development Objectives Development o f a health care system that can efficiently and equitably deliver a package o f basic health services to a large proportion o f the under- served rural population in a sustainable fashion.
Output from each Component
1. M u c h improved delivery o f essential health services, particularly among the under-served rural population. More trained, particularly female, health workers available to deliver effective health services.
0 Infant mortality
0 Malnutrit ion in
Total Fertility Rate Maternal mortality
rate
children
ratio
0 Core output
1) coverage o f adequate prenatal care.
2) contraceptive prevalence rate 3) coverage o f Vi tamin A
4) % o f parents able to identify danger signs o f ARI
5) immunization coverage
(the complete l i s t i s in Table 1 o f the text)
indicators such as:
1.1 % o fPPAs and M O H - S M that are achieving the targets set out in the agreement for the core output indicators. 1.2 % o f sampled health facilities providing the various parts o f the BPHS. 1.3 Increase in the number o f female health workers.
Baseline and follow-on household surveys will provide robust estimates at national level
0 Provincial level household surveys at baseline and 30 months.
0 MOH supervision o f health facilities Performance assessments o f health facilities by 3rd party
analysis o f costs and out o f pocket expenditures
0 Economic
0 Provincial level household surveys at baseline and 30 months later.
0 Routine reporting system
0 Performance assessments o f health facilities by 3rd party
0 MOH supervision o f health facilities
MOH Objectives to Government Objectives
Other key aspects o f human development (e .g. increased access to education) are achieved.
0 Security situation and polit ical process remain stable.
Development Objectives to MOH Objectives
Other factors that influence the health status o f the population (including status o f women, poverty levels, peace and stability, education, water and sanitation, and transportation, etc.) improve significantly.
Outputs to Development Objective
0 Ethnic tensions do not interfere with equitable distribution o f project services.
0 Polit ical considerations do not effect choice o f delivery mechanism.
1
Narrative Summary
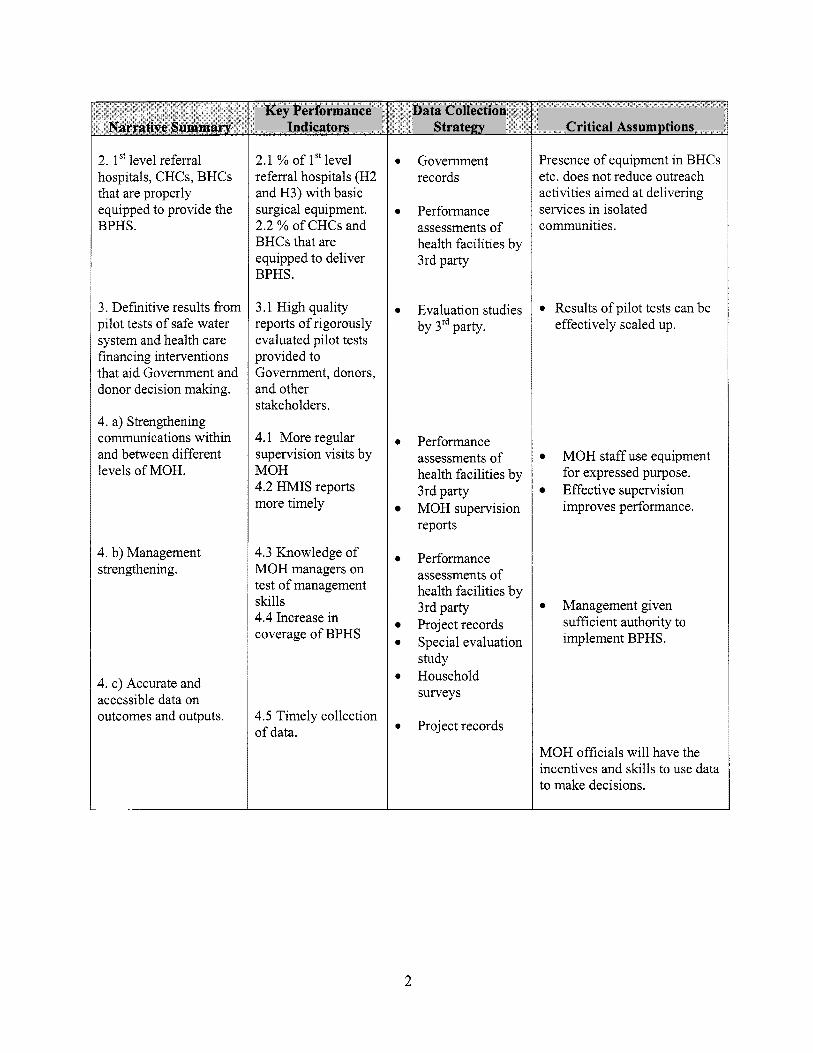
2. 1"level referral hospitals, CHCs, BHCs that are properly equipped to provide the BPHS.
3. Definit ive results f rom pi lot tests o f safe water system and health care financing interventions that aid Government and donor decision making.
4. a) Strengthening communications within and between different levels o f MOH.
4. b) Management strengthening.
4. c) Accurate and accessible data on outcomes and outputs.
Key Performance Indicators
2.1 % o f 1 St level referral hospitals (H2 and H3) with basic surgical equipment. 2.2 % o f CHCs and BHCs that are equipped to deliver BPHS.
3.1 High quality reports o f rigorously evaluated pi lot tests provided to Government, donors, and other stakeholders.
4.1 More regular supervision visits by MOH 4.2 H M I S reports more t imely
4.3 Knowledge o f MOH managers on test o f management skills 4.4 Increase in coverage o f BPHS
4.5 Timely collection o f data.
Data Collection Strategy
0 Government records
0 Performance assessments o f health facilities by 3rd party
0 Evaluation studies by 3rd party.
0 Performance assessments o f health facilities by 3rd party MOH supervision reports
0 Performance assessments o f health facilities by 3rd party Project records
0 Special evaluation study
0 Household surveys
0 Project records
Critical Assumptions
Presence o f equipment in BHCs etc. does not reduce outreach activities aimed at delivering services in isolated communities.
0 Results o f p i lot tests can be effectively scaled up.
0 MOH staff u__ quipment for expressed purpose.
improves performance. Effective supervision
0 Management given sufficient authority to implement BPHS.
MOH officials will have the incentives and s lu l ls to use data to make decisions.
2
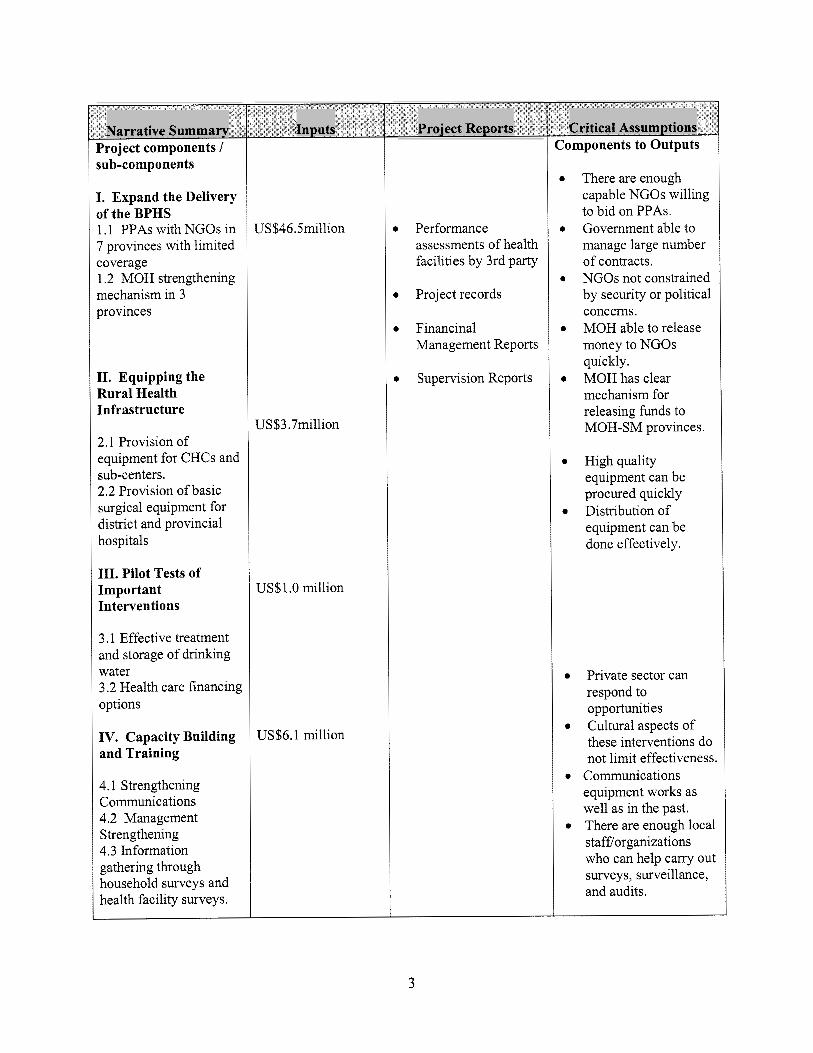
Narrative Summary Project components I sub-components
I. Expand the Delivery o f the BPHS 1.1 PPAs with NGOs in 7 provinces with l imi ted coverage 1.2 MOH strengthening mechanism in 3 provinces
11. Equipping the Rural Health Infrastructure
2.1 Provision o f equipment for CHCs and sub-centers. 2.2 Provision o f basic surgical equipment for district and provincial hospitals
111. Pilot Tests of Import ant Interventions
3.1 Effective treatment and storage o f drinking water 3.2 Health care financing options
IV. Capacity Building and Training
4.1 Strengthening Communications 4.2 Management Strengthening 4.3 Information gathering through household surveys and health facility surveys.
Inputs
U S $ l .O mil l ion
US$6.1 mi l l ion
Project Reports
Performance assessments o f health facilities by 3rd party
Project records
Financinal Management Reports
Supervision Reports
Critical Assumptions Components to Outputs
There are enough capable NGOs willing to bid o n PPAs. Government able to manage large number o f contracts. NGOs not constrained by security or polit ical concems. MOH able to release money to NGOs quickly. MOH has clear mechanism for releasing funds to M O H - S M provinces.
High quality equipment can be procured quickly Distribution o f equipment can be done effectively.
Private sector can respond to opportunities Cultural aspects o f these interventions do not limit effectiveness.
Communications equipment works as wel l as in the past. There are enough local stafflorganizations who can help carry out surveys, surveillance, and audits.
3
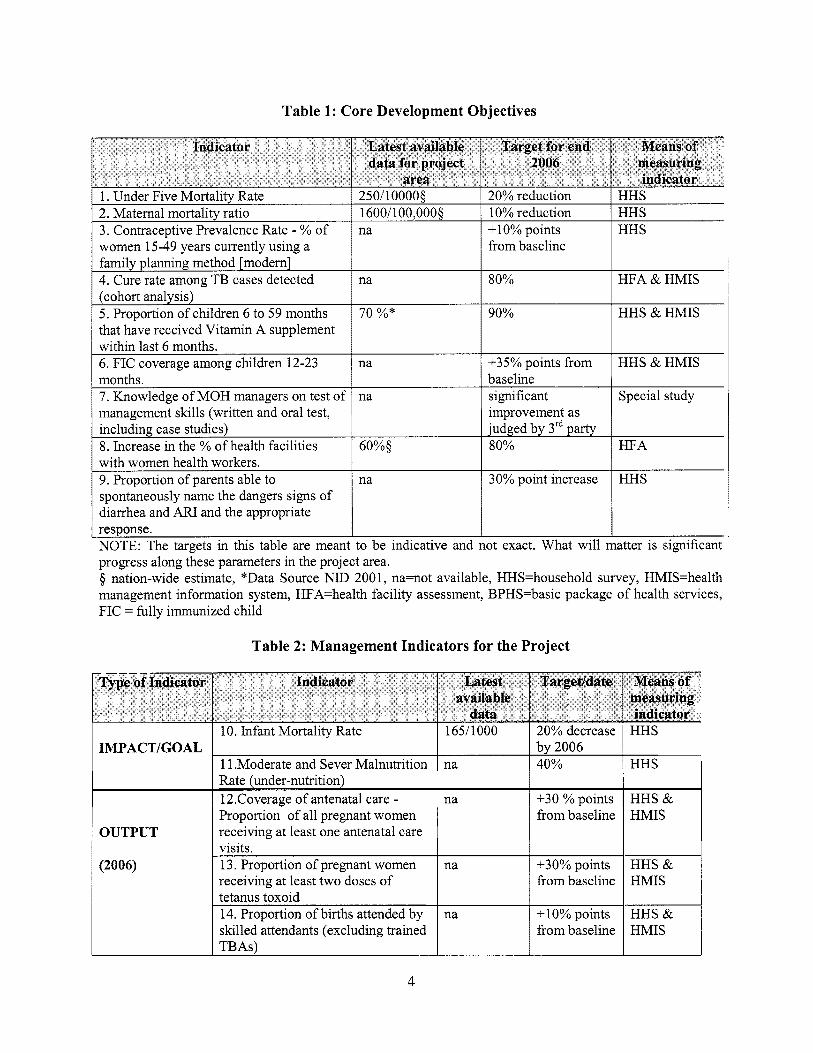
Table 1: Core Development Objectives
Type of Indicator Indicator Latest available
data
diarrhea and ARI and the appropriate
NOTE: The targets in this table are meant to be indicative and not exact. What will matter i s significant progress along these parameters in the project area.
nation-wide estimate, *Data Source NID 200 1, na=not available, HHS=household survey, HMIS=health management information system, HFA=health facility assessment, BPHS=basic package o f health services, F IC = fully immunized child
Targevdate Means of measuring indicator
Table 2: Management Indicators for the Project
IMPACT/GOAL 10. Infant Mortality Rate 165/1000 20% decrease HHS
1 1 .Moderate and Sever Malnutrition na 40% HHS by 2006
Rate (under-nutrition) 12.Coverage o f antenatal care -
__I
na +30 % points HHS &
1 OUTPUT Proportion o f all pregnant women receiving at least one antenatal care
(2006)
1 fi-ombaseline HMIS
4
visits. 13. Proportion o f pregnant women receiving at least two doses o f tetanus toxoid 14. Proportion o f births attended by skilled attendants (excluding trained
na 130% points from baseline
na + 10% points from baseline
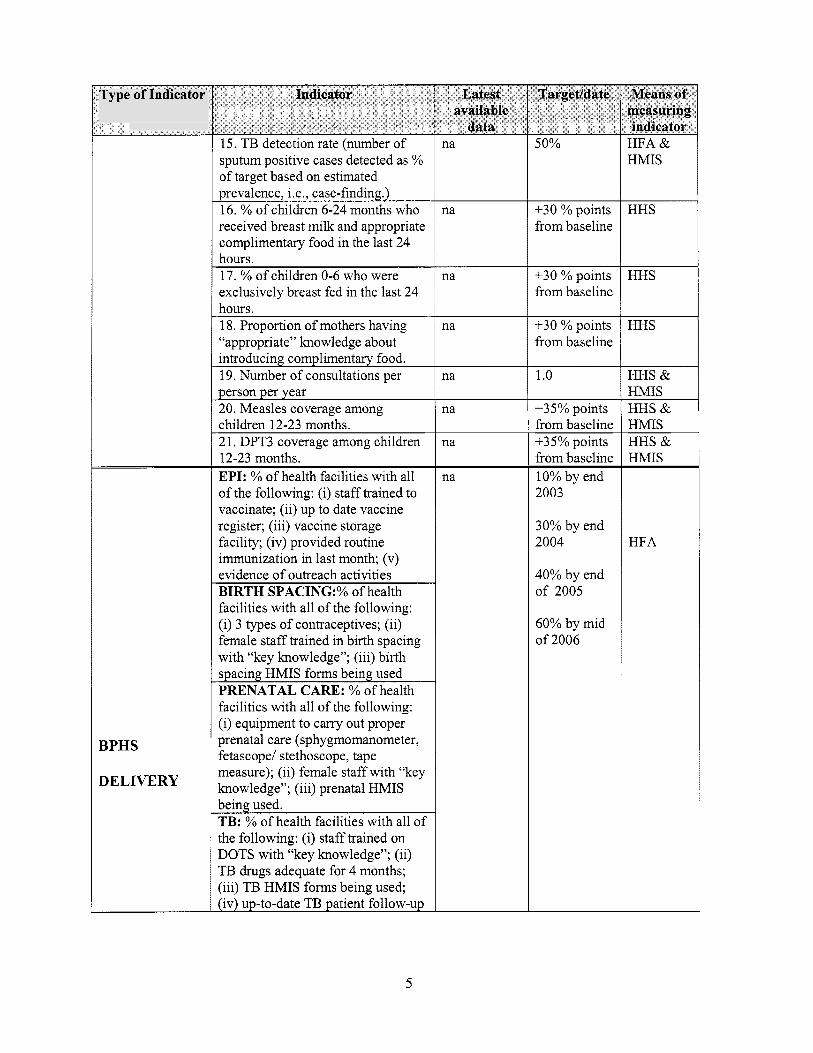
Type of Indicator
BPHS
DELIVERY
Indicator
15. TB detection rate (number o f sputum positive cases detected as % o f target based o n estimated prevalence, i.e., case-finding.) 16. % o f children 6-24 months who received breast milk and appropriate complimentary food in the last 24 hours. 17. % o f children 0-6 who were exclusively breast fed in the last 24 hours. 18. Proportion o f mothers having “appropriate” knowledge about introducing complimentary food. 19. Number o f consultations per person per year 20. Measles coverage among children 12-23 months. 2 1. DPT3 coverage among children 12-23 months. EPI: % o f health facilities with al l o f the following: (i) staff trained to vaccinate; (ii) up to date vaccine register; (iii) vaccine storage facility; (iv) provided routine immunization in last month; (v) evidence o f outreach activities BIRTH SPACING:% o f health facilities with a l l o f the following: (i) 3 types o f contraceptives; (ii) female staff trained in birth spacing with “key knowledge”; (iii) birth
-
spacing HMIS forms being used PRENATAL CARE: % o f health facilities with a l l o f the following: (i) equipment to carry out proper prenatal care (sphygmomanometer, fetascopel stethoscope, tape measure); (ii) female staff with “key knowledge”; (iii) prenatal HMIS being used. TB: % o f health facilities with al l o f the following: (i) staff trained o n DOTS with “key knowledge”; (ii) TB drugs adequate for 4 months; (iii) TB HMIS forms being used; (iv) up-to-date TB patient follow-up
n a
n a
na
na
na
na
na
n a
50%
+30 % points f rom baseline
+30 % points f rom baseline
+30 % points f rom baseline
1 .o
+35% points f rom baseline +35% points f rom baseline 10% by end 2003
30% by end 2004
40% by end o f 2005
60% by m i d o f 2006
HFA & HMIS
HHS
HHS
HHS
HHS & HMIS HHS & HMIS HHS & HMIS
HFA
5
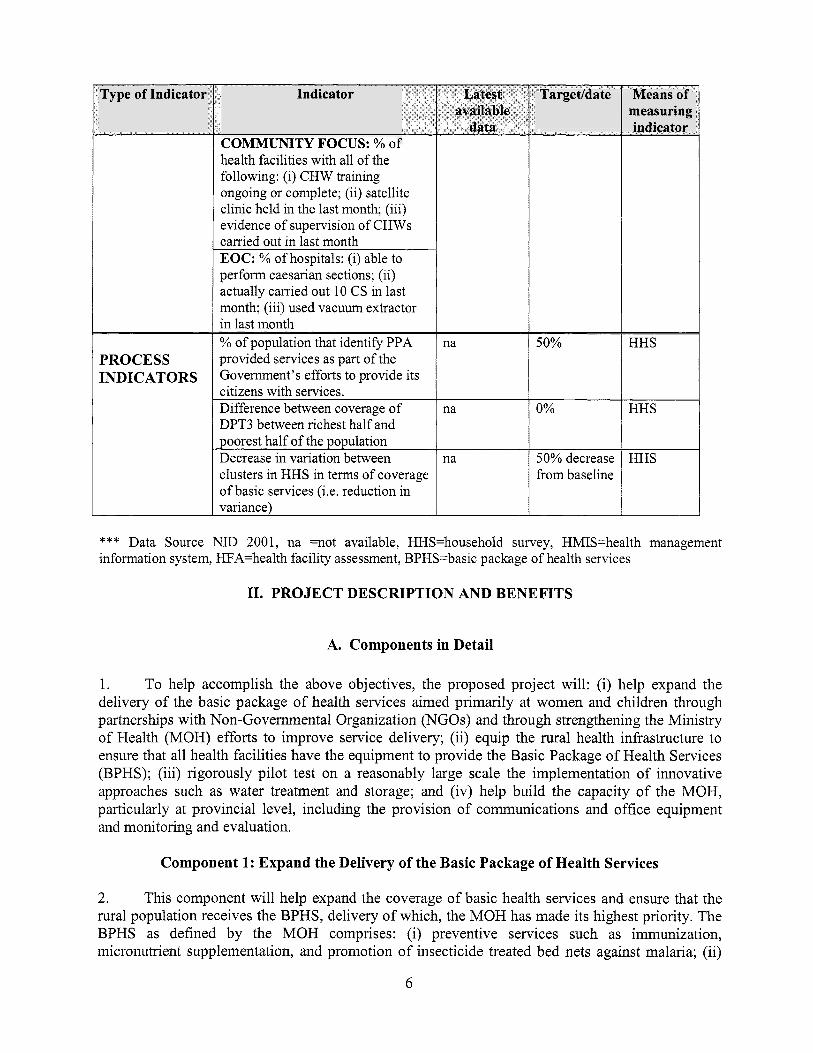
Type of Indicator
PROCESS INDICATORS
Indicator
COIIMMUIYTY FOCZ'S: Yo o f health facilities with al l o f the following: (i) CHW training ongoing or complete; (ii) satellite clinic held in the last month; (iii) evidence o f supervision o f CHWs carried out in last month EOC: % o f hospitals: (i) able to perform caesarian sections; (ii) actually carried out 10 CS in last month; (iii) used vacuum extractor in last month % o f population that identify PPA provided services as part o f the Government's efforts to provide i t s citizens with services. Difference between coverage o f DPT3 between richest ha l f and poorest ha l f o f the population Decrease in variation between clusters in H H S in terms o f coverage o f basic services (Le. reduction in variance)
na
na
na
Targetldate Means of measuring indicator
50%
~
f r om baseline
*** Data Source NID 2001, na =not available, HHS=household survey, HMIS=health management information system, HFA=health facil i ty assessment, BPHS=basic package o f health services
11. PROJECT DESCRIPTION AND BENEFITS
A. Components in Detail
1. To help accomplish the above objectives, the proposed project will: (i) help expand the delivery o f the basic package o f health services aimed primari ly at women and children through partnerships with Non-Govemmental Organization (NGOs) and through strengthening the Ministry o f Health (MOH) efforts to improve service delivery; (ii) equip the rural health infrastructure to ensure that al l health facilities have the equipment to provide the Basic Package o f Health Services (BPHS); (iii) rigorously pi lot test on a reasonably large scale the implementation o f innovative approaches such as water treatment and storage; and (iv) help build the capacity o f the MOH, particularly at provincial level, including the provision o f communications and office equipment and monitoring and evaluation.
Component 1: Expand the Delivery of the Basic Package of Health Services
2. This component wil l help expand the coverage o f basic health services and ensure that the rural population receives the BPHS, delivery o f which, the MOH has made i t s highest priority. The BPHS as defined by the MOH comprises: (i) preventive services such as immunization, micronutrient supplementation, and promotion o f insecticide treated bed nets against malaria; (ii)
6

promotive health services such as increasing prevalence o f breast-feeding and use o f family planning; (iii) basic curative services such as treatment o f acute respiratory tract infections, diarrhea, other childhood illnesses, and tuberculosis; and (iv) reproductive health services such as prenatal care, emergency obstetrical care, and post-partum care. These services wil l be delivered through fixed facilities, outreach activities, and community-based interventions. The MOH has selected seven under-served provinces (see Table 3) spread over different regions o f Afghanistan which will have services enhanced through performance-based partnership agreements (PPAs) with NGOs. Another three provinces wil l have services strengthened in a phased manner through an MOH-Strengthening mechanism (MOH-SM).
WARDAK BADGHIS
Table 3: Seven Under-served Provinces where PPAs will be Implemented
41 3,000 301.200
Province 1 Population IKAPISA I 359,700 I /FARAH I 338.300 I
[TOTAL I 2,764,300 I 3. PPAs will be implemented in the following manner:
(0
(ii)
(iii)
The MOH will use the published BPHS as the defined services and describe the recording and reporting requirements. As part o f the BPHS the PPA will also cover operating the provincial hospital, including emergency obstetrical care and trauma management. In addition, the PPA NGO will be responsible for carrying out training aimed at ensuring that the staffing patterns envisioned in the BPHS are achieved for auxiliary mid-wives, community health workers (CHWs) and traditional birth attendants (TBAs).
The MOH has defined a set o f indicators for judging whether the BPHS is being successfully delivered. For example, in immunization this includes both coverage targets and process indicators, such as proper recording and proper disposal o f used needles, that could be measured during supervisory visits and third party assessments audits.
After discussions with stakeholders, including local and intemational NGOs, MOH, through i t s grants and contracts management unit (GCMU), wil l finalize the bid documents for the PPAs. These wil l include the selection criteria for NGOs (NGOs includes, in this context, other private sector entities), such as: (a) track record in delivering primary health care services; (b) quality o f the key management personnel (the three senior managers to be involved in the project); (c) knowledge o f the PPA area; (d) quality o f the strategic plan for accomplishing the targets explicit in the PPAs; and (e) presence o f audited accounts, demonstrated logistics capacity, etc.
7
MOH will carry out a competitive bidding process where local and international NGOs, as well as any interested private sector entity could freely compete for the PPAs based on the quality and cost o f their technical proposals (quality and cost based selection).
MOH at the central level will evaluate the bids using the criteria in the bid documents. Representatives o f United Nations (UN) agencies, NGOs, and the donor community wil l be included in the evaluation committee(s).
M O H wil l sign a three-year agreement with the winning bidder for the bid amount and there will also be a performance bonus o f up to 10 percent based on exceptional improvements in service delivery. The bonuses wil l be allotted based on the results o f health facility surveys every six months and on the results o f the follow-on household surveys.
The NGO will receive regular payments based o n satisfactory progress as judged by frequent field supervision carried out by M O H staff and a third party.
Monitoring and evaluation o f NGO performance wil l be carried out through baseline and follow-up household surveys, independent health facility assessments carried out by a third party, and community feedback mechanisms. Among the outcomes o f interest is whether the services provided by the NGOs are perceived to be part o f the Government’s efforts. The payment o f performance bonuses will depend on objective accomplishments from the household and health facility surveys.
Results o f the household and health facility surveys wil l be made available to the public through newspapers and other media.
4. MOH-SM: In the three provinces selected for this approach, the aim wil l be to allow MOH staff to expand the health services in a phased manner. Increasing amount o f resources wil l be provided to the selected provinces based on their demonstrated capacity to use resources effectively and maintain proper accounts. Similar to the PPA approach, the M O H will use the provision o f the BPHS as i t s primary goal in these provinces and use already selected indicators to judge success. In addition,
(i) the MOH intends to empower provincial health directors and their staff to develop an annual plan and budget with monthly work plans after receiving training on planning and budgeting. A standard format wil l be provided and the planning and budgeting process will be assisted by a consultant. The final work plan and budget wil l have to be approved by the central MOH;
(ii) the work plan and budget will have to be consistent with Government rules and regulations, including: (a) funds could only be used for expenditures directly related to delivery o f the BPHS; (b) no new MOH staff could be recruited although health workers could be hired o n a contractual basis within MOH recommended salary scales; (c) any incentives paid to MOH staff will have be explicitly permitted under Government decrees (MOF i s working on this issue); (d) procurement o f goods and services wil l have to fol low Government guidelines; and (e) any equipment or drugs procured wil l have to be on the essential drug list and the MOH equipment l ist;
8
(iii) disbursement o f funds wil l be done using a mechanism approved by M O F and acceptable to the Bank and in accordance with the approved work plan and budget. The use o f funds wil l be externally audited;
(iv) the selected provinces wil l receive ongoing technical assistance to help them implement their work plan (see component 4 for more details); and
(v) monitoring and evaluation o f provincial MOH performance wil l be carried out in the same way as the PPAs.
5. Coordinating Mechanisms at Provincial Level. The intention behind the PPAs and MOH- S M i s not to displace any existing efforts but rather to expand and consolidate service delivery. To help ensure careful coordination among service providers, the following strategies wil l be employed: (i) a provincial coordination committee (PCC) will be established chaired by the provincial health director (PHD) and comprising the PPA winning bidder, and other NGOs operating in the province; (ii) in PPA provinces the PHD will be assisted by the PPA NGO in coordinating ongoing activities; (iii) NGOs bidding for the PPAs will have to indicate in their technical proposals how they wil l work with the Provincial Health Department and NGOs already on the ground in the particular province; (iv) NGOs already active in the province where they are bidding wil l receive additional points on their technical score; (v) NGOs coming into the province after the PPA or M O H - S M i s in place wil l only be able to do so with agreement o f the PCC and GCMU; (vi) a simple system o f mediation (comprising one representative each from the central MOH and the NGO community) and arbitration (comprising central level MOH officials and representatives o f the NGO community and donor and UN agencies) wil l be implemented; and (vii) the PPA NGOs or Provincial MOH will be allowed to support the work o f other NGOs in the province if they obtain permission from the central MOH. The NGO with the PPA and the provincial MOH will have an interest in ensuring that progress i s made o n the core output indicators and the other NGOs will presumably be interested in obtaining additional resources to support their work.
Component 2: Equipping the Rural Health Infrastructure
6. Currently most comprehensive health centers (CHCs), basic health centers (BHCs) and maternal and chi ld health centers are missing simple but critically important equipment. Without this equipment i t wil l be very difficult for NGOs or the MOH to deliver the entire BPHS. United States Agency for International Development (USAID) has indicated to the TISA that it has the funds to rehabilitate and/or construct about 500 health facilities over the next three years, although i t could not provide equipment or furniture for these facilities. Hence, project funds will be used to provide basic equipment and furniture for CHCs and BHCs based o n lists developed by the MOH. The equipment provided will be simple with few moving parts so that maintenance and repair can be done locally. The project wil l also finance basic surgical equipment for district and provincial hospitals not being provided equipment by other agencies. The l i s t o f hospital equipment wil l be developed by MOH in consultation with experts, including the International Committee for the Read Cross (ICRC), within a budget envelope o f about US$20,000 per hospital. Most o f this equipment wil l be surgical instruments and the l i ke that requires l imited maintenance.
9
Component 3: Pilot Tests of Important Innovations
7 . While the BPHS wil l address a large proportion o f the current burden o f disease, new interventions wil l need to be developed and rigorously tested to address remaining causes o f ill health. One area where field testing o f new interventions makes sense is the prevention o f diarrhea where recent work provides opportunities to prevent its occurrence in the first place even in areas without good water supplies. In addition to disease interventions, i t wil l be useful to pi lot test health care financing interventions. This wil l help the M O H shift from focusing o n “relief” efforts to addressing “development” issues and wil l offer guidance on sustainable health care financing in the longer term.
8. Diarrhea Prevention. Oral rehydration salts (ORS) may be helpful in preventing deaths from diarrhea but wil l have no effect on preventing diarrhea in the f i rs t place. Improving the quality o f drinking water wil l be important but i t wil l take time and considerable resources to ensure most households in rural areas have access to safe drinking water. Data collected from various sources by the Centers for Disease Control and Prevention (CDC) indicates that less than 5 percent o f rural households have access to improved water supplies. Hence, i t makes sense to test appropriate technologies for safely treating and storing drinking water. CDC experts have developed a “safe water system” (SWS) that uses dilute sodium hypo-chlorite solution to disinfect drinking water that can then be stored in specially designed narrow-necked containers that prevent re-contamination. The storage containers also have a spigot and built-in soap dish that facilitates hand washing. Recent evaluations in other countries have shown that the SWS approach can reduce the incidence o f diarrhea by 44 percent to 85 percent. I t wil l be important to see whether similar results can be obtained under f ield conditions in Afghanistan.
9. To test this approach, experts from CDC will work closely with the MOH, to carry out a f ield trial o f the efficacy o f the SWS in Afghanistan, particularly in comparison to simply improving the water supply. Forty-five villages wil l be randomly allocated to one o f three interventions: (i) the SWS without improvement in water supply; (ii) improvements in water supply without the SWS; and (iii) a combination o f both improved water supply and the SWS. This study wil l provide information on how improving water supplies, which is expensive and may not happen in much o f Afghanistan for many years, compares to the SWS. The study design wil l be reviewed by the M O H and a CDC ethics review committee. In addition, a l l the SWS villages will receive improved water supplies after the study was completed. During the efficacy study the disinfectant and special container will be provided for free, however, PPA NGOs will be encouraged to implement the SWS on a pi lot basis to observe what happens to use when subsidies are reduced. If the efficacy trial is successful project funds and funds from other donors wil l be used to support the social marketing o f the sodium hypo-chlorite solution and the storage containers.
10. Health Care Financing Innovations. To ensure the sustainability o f public health activities, mechanisms will have to be found to generate funds from local sources. Experience in other countries indicates that community-based health insurance i s difficult to manage and has often not been successful. User charges also have a mixed track record although, they have often been efficient and equitable when implemented by NGOs. Another mechanism that has rarely been used but has been quite successful i s a “community health contribution.” Local community leaders agree on and collect a health contribution from households in their own communities soon after the harvest when households have cash. Households that are judged too poor will be exempted from the contribution and wealthy households will be expected to contribute more. In Niger, introduction o f
10

a similar health contribution resulted in a doubling in the use o f services by the poorest 25 percent o f the population. There i s little experience with the latter approach in Afghanistan and so it i s important to pi lot test this approach against alternatives.
11. In order to provide the MOH with credible data o n how various alternatives work, a study wil l be undertaken in which six BHCs in each PPA province will be allocated to one o f three groups: (i) user charges; (ii) community health contribution; or (iii) comparison @e., neither user charges nor community health contributions). The study will examine the effects o f these approaches on beneficiaries, particularly the poor, and the amount o f revenues generated.
Component 4: Capacity Building and Training
12. Helping to ensure that the BPHS i s broadly delivered and that other public health functions are carried out effectively wil l require that the capacity o f the MOH, particularly at central and provincial levels, wil l need to be extensively strengthened. To accomplish this capacity building and training , the project will: (i) strengthen the communications within and between provincial, regional, and central offices o f the MOH; (ii) provide ongoing technical assistance to the provincial M O H s and NGOs with PPAs in order to strengthen their management capacities; and (iii) help collect information for the MOH and other stakeholders o n the performance o f the health care system.
13. Strengthening Communications. Regardless o f their ultimate role, the provincial health offices o f the MOH need to be significantly strengthened. Currently they have limited contact with the MOH, the managers have l imited experience or knowledge o f management and supervision, and they lack the resources to oversee their jurisdictions. In order to address these weaknesses, the project wil l provide the following:
(i) high frequency radios and computers powered by solar panels for voice-data communications wil l be provided to al l the provincial offices. This technology is being successfully used by the World Health Organization (WHO) and has been trouble free. Regardless o f future telecommunications plans such a data radio link would: (a) be o f critical importance during natural or man-made disasters; (b) facilitate communications between the central, regional, and MOH offices which wil l help inform decision making and pol icy dialogue (it wil l also create an MOH that reflects al l o f Afghanistan); (c) assist with delivery o f time sensitive materials such as disease surveillance reports; and (d) facilitate distance education for provincial staff. When regular telecommunication l i n k s are established to the provinces, this system wil l provide a back-up in case o f emergency; and
(ii) transportation to facilitate supervision, monitoring, and emergency response. Provinces that do not have vehicles wil l be provided a heavy duty vehicle suitable for off-road travel (a double cab pick-up type truck). The MOH will develop guidelines for the responsible use and maintenance o f such vehicles.
14. Management Strengthening. Management capacity at the central and provincial levels o f the M O H wil l be strengthened through technical assistance and training. Technical assistance, comprising a long-term international consultant and local experts, wil l be provided to the G C M U to help implement the PPAs and the grantdcontracts o f other donors. Technical assistance to strengthen overall management wil l be provided to selected provincial and central offices, as wel l as
11

to NGOs who win PPAs. A long-term international consultant and two local consultants will be recruited by the MOH. Training courses, either through distance learning or abroad, wil l be provided to selected M O H staff. The individuals selected for training wil l already have facility in English, exhibit leadership potential, and wil l have agreed to continuing to work in the MOH for a time specified in advance by the MOH. Selection o f training candidates wil l be done in a transparent manner by the Executive Board o f the MOH.
15. Information Collection, Monitoring, and Evaluation. In order to provide MOH and other stakeholders with the information they need to assess progress, the project will support a number o f ways o f collecting information:
A household survey wil l be carried out to collect data at provincial level on the indicators described in Tables 1 and 2 (although impact indicators will only be available at national level and by groups o f provinces). The survey wil l be carried out at the beginning o f the project and repeated 30 to 36 months later by third parties. The questionnaire wil l be used to collect information related to education, access to clean water and sanitation, and other factors that directly effect human development. The f i rs t round o f the survey wil l likely be financed by UNICEF and the World Bank education project and the second round wil l be financed by this project;
(ii) Health facility assessments wil l also be carried out by a third party contractor and will examine quality o f care, knowledge o f staff, maintenance and repair o f the facilities, and availability o f drugs and supplies. These performance audits wil l be performed on a sample o f facilities in each province at baseline, 6, 12,24, and 36 months later; and
(iii) Systematic supervision o f health facilities will be carried out by provincial and central level MOH staff using a standardized approach that wil l assess whether the facility is providing the BPHS. The project wil l provide assistance in developing the standardized approach, training for supervisors, and transportation costs for central MOH staff, including high level officials.
16. mi l l ion and i s described in more detail in Appendix 1.
Project Costs. The estimated cost o f the project with contingencies i s about US$59.5
B. Benefits of the Project
17. The project wil l provide benefits to an underserved total population o f about 4.5 mi l l ion people. These benefits wi l l mostly take the form of reductions in under-5 and maternal mortality and morbidity, since the emphasis o f the BPHS will be o n maternal and child health.
18. An attempt was made at estimating the number o f deaths o f women and children that wil l be averted in the with-project situation. Due to a severe lack o f reliable data for Afghanistan, a number o f assumptions based on data obtained from developing countries with similar circumstances were used for baseline health status indicators. Conservative estimates o f the impact o f the Project for decreases in maternal, infant, and chi ld mortality rates were used in the calculations. Baseline health status indicators and targets by the end o f the project period are taken f rom Table 1, Core Output Indicators for the Project, where available. The following assumptions were made for the estimates:
12
19. Population and Mortality Assumptions:
Current population o f the ten participating provinces : About 4.5 million. Annual population growth rate: 3.5 percent Women o f reproductive age (WRA): 22 percent Infants: 3 percent Children under-five: 18 percent Maternal mortality ratio (MMR): 1600 maternal deaths per 100,000 l ive births Infant mortality rate (IMR): 165 per 1000 l ive births Under-five mortality rate (USMR): 250 per 1000 Malaria accounts for 6 percent o f under-five mortality rate Nationwide deaths per year from tuberculosis: 25,000; TB deaths in the project area assumed proportional to national figure. Acute respiratory infection (ARI) accounts for 25 percent o f under-five mortality rate Diarrhea accounts for 25 percent o f under-five mortality rate Vaccine preventable diseases account for 10 percent o f under-five mortality rate
20. targets are met by the end o f the project period, with incremental advances in the first two years:
Effects of Project on Mortality. For each o f the following, it i s assumed that the Project
(i) Maternal health and birth spacing: 20 percent decrease in maternal mortality ratio (MMR) for the targeted 50 percent o f women;
(ii) Tuberculosis: 80 percent cure rate for the 50 percent (tuberculosis) TB diagnosis rate target;
(iii) Malaria: 40 percent target bed net coverage for under-five children results in 30 percent decrease in deaths attributable to malaria;
(iv) Vitamin A: 23 percent decrease in mortality rate for children six months to 59 months old;
(v) Breastfeeding Promotion and Weaning: 10 percent decrease in IMR;
(vi) ARI: 10 percent decrease in U5MR;
(vii) Diarrheal diseases: 10 percent decrease in U5MR; and
(viii) Immunization: 10 percent decrease in the U 5 M R for the targeted 65 percent o f the under-five population.
21. Under the above assumptions, it was estimated that the project will enable averting about 3,700 deaths o f women o f reproductive age and 65,000 deaths o f children under five years o f age in the three-year project implementation period alone. Of these deaths, about 1,500 deaths o f women o f reproductive age and 27,000 deaths o f under-five children wil l be averted in the third year o f project implementation. Beyond project completion, and provided that the activities initiated under the project are sustained (with the same degree o f coverage and effectiveness), i t could be expected that every year a number o f additional deaths will be averted o f a magnitude similar to the number
13
o f deaths averted in the third year o f project implementation. In view o f conceptual difficulties in assigning a monetary value to deaths averted, no estimates o f the project’s economic benefits associated with deaths averted were attempted.
111. IMPLEMENTATION ARRANGEMENTS
A. Organizational Structure
22. Central Level. The project wil l be implemented over a three year period by the MOH. MOH at the central level will have overall responsibility for project oversight and supervision through its Executive Board. The director o f the MOH’s Policy and Planning Department wi l l be the Project Manager and wil l have responsibility for project implementation and will be the focal point for coordination. The day-to-day responsibilities for project implementation will rest with the G C M U manager, and heads o f the relevant administrative units o f the MOH (see Table 3).
23. Provincial Level. The Provincial Coordination Committee (PCC) wil l ensure: (i) coordination o f a l l donor and NGO support in the province; (ii) reduce duplication o f efforts; (iii) prevent gaps in service delivery; and (iv) expand delivery o f the BPHS. The provincial health director wil l chair the PCC. MOH has asked donors to take on the role o f focal donor for a province or set o f provinces. This wil l entail either directly, or through an NGO, supporting the PCC in carrying out i t s functions and building the capacity o f the provincial health department.
24. Some o f the project activities wil l be executed under contracts that will have to be managed by the M O H and this will be handled by the GCMU. The Project wil l support the fimctioning o f the G C M U with long-term technical assistance and needed physical resources. In addition, the MOH will be able to take advantage o f the expertise o f Crown Agents who have a Bank-financed contract with the Government to provide ongoing procurement expertise. The implementation arrangements for each component are as follows and are summarized in Table 4:
14

Table 4: Responsibility for Implementation and Supervision
3rd party evaluation firm/ organization with MOH or
Component/sub- component
MOH- Planning Department
1. PPAs
2. M O H Strengthening mechanism
3. B H C & sub-center equipment
4. Hospital Equipment
5. Safe water system efficacy study
6. Health care financing pilots .7. Training o f CHWs and auxiliary mid-wives-
8. Communication strengthening 9. Management strengthening 10. Household Surveys and evaluations
office
(with assistance from Crown Agents)
" I I
MOH Procurement Unit (with assistance from Crown Agents) MOH through Unicef with CDC technical assistance Environmental
MOH PHC Unit
a) MOH
Health Unit b) special study unit MOH - Planning NGOs with PPA, MOH's
Health Financing Unit Department NGOs with PPA MOH - human
I resource development unit
Contractors MOH - IT unit
I MoH- GCMU Individual consultants
T ISA entity CDC = Centers for Disease Control and Prevention, T ISA = Transitional Is:
Evaluation firm/ organization a) Auditing firm b) 3rd party Evaluation firm/ organization
party evaluation firm/ organization 3'd party evaluation firm/ organization
n i c Government o f Afghanistan, G C M U = Grants and Contracts Management Unit, MOH = Ministry o f Health
B. Implementation Procedures
25. Expansion of Delivery of the BPHS (Component 1) will be done through two modalities:
(i) PPAs through NGOs selected on a competitive basis. The MOH's contracting unit (GCMU) and the provincial directors o f the MOH will evaluate the proposals with technical assistance from UN agencies, and a representative (non-bidder) o f the NGO community. The G C M U and provincial directors will also select the winning NGOs and wil l monitor and supervise their performance. Training o f female staff wil l be
15
(ii)
(iii)
carried out utilizing the competency-based training materials being finalized by MOHs Human Resource Development Unit.
MOH-Strengthening Mechanism will expand service delivery through the provincial health departments, with technical assistance. MOH at the central level wil l monitor and supervise performance. Semi-annual independent evaluations wil l be carried out at the health facilities. Financial mechanisms wil l be established to facilitate the transfer o f funds by the G C M U to the provincial level.
Environmental Management Plan. The activities under this Plan wil l be implemented by the contracted NGOs, under the PPAs, and by the M O H for M O H - S M health facilities. MOH’s Environmental Health Unit wil l monitor and supervise implementation o f the Plan.
26. Equipping the Rural Health Infrastructure (Component 2). Medical and office equipment and vehicles for MOH, at the central and provincial levels, will be procured by the MOH’s Supply and Logistics Unit, with technical assistance from the procurement agent (Crown Agents), and wil l be distributed by the suppliers to the lowest possible administrative level.
27. wil l take place:
Test o f Important Innovations (Component 3). Two pi lot tests o f important innovations
(i) Safe Water System (SWS) field efficacy and effectiveness study (Component 3) will be carried out through the CDC Foundation, in cooperation with, and under the supervision o f the MOH’s Environmental Health Unit and the Special Studies Unit.
(ii) The health care financing pi lot study wil l be carried out through NGOs (under the PPAs) and wil l be evaluated by the third party evaluation firm, in coordination with the Health Financing Unit o f the MOH.
28. coordinated at the MOH’s central level, by the Planning Department.
Capacity Building and Training (Component 4). Activities under this component wil l be
(0
(ii)
(iii)
Procurement o f goods and services wil l be done by the MOH’s Procurement Unit with technical assistance from procurement agents.
The G C M U will monitor the implementation o f the technical assistance and ensure that contractors and suppliers are paid on a timely basis, and also, that transfer o f resources to the Provincial Health Departments takes place efficiently and in a timely manner.
Household surveys and semi-annual health facility evaluations wil l be implemented by firms/organizations hired on contract and supervised by MOH’s Planning, Monitoring and Evaluation, and HMIS Unit.
16

C. Procurement
29. Given limited experience and procurement capacity o f the MOH which is responsible for implementing the proposed Project, the TISA procurement agent (Crown Agents) wil l work on behalf of, and closely with, the MOH to carry out some o f the procurement, where i t has relevant expertise and experience. The following procurement methods will be used:
(0
(ii)
(iii)
Services. There will be seven packages for the PPAs worth about US$40 mi l l ion and this will be done using quality and cost based selection (QCBS). The M O H wil l prepare a shortlist o f NGOs, based on an evaluation o f expressions o f interest to be received by the middle o f M a y 2003. A draft Request For Proposal (RFP) has been prepared and reviewed by the Bank, but complete details in respect o f these packages are s t i l l to be finalized by the MOH. Issuance o f the RFP i s expected by around June 1 , 2003 so that awards could be finalized by mid-August, 2003. Implementation o f the SWS pilot (US$O.8 million) wil l be done by the CDC o n a sole source basis due to their unique expertise in this area. The CDC developed the SWS and has overseen i t s implementation in more than 15 countries worldwide,
Procurement of Goods (US$5.4 million). These items include medical and hospital equipment and vehicles for which international competitive bidding (ICB) procedures will be used to a value o f US$4.5 million. International and/or National Shopping (Isms) procedures wil l apply for procurement of office equipment, radios, computers and furniture (US$O.9 million). Equipment supplies will need to be synchronized with the construction period o f the new facilities to be built under U S A I D funding over the three-year period o f proj ect implementation, for proper utilization.
Individual Consultant Services (US$1.2 million). Two international consultants wil l be recruited using Quality Based Selection (QBS) procedures. This selection process wil l include: (a) inviting expressions o f interest by advertisement in the Development Business and the national press: (b) preparing short lists; and (c) awarding contracts to them.
D. Financial Management and Audit
30. The financial management assessment and action plan i s in Appendix 2.
IV. EXPERIENCE OF CONTRACTING WITH NGOs FOR HEALTH SERVICE DELIVERY
31. This section briefly describes the experience in other post-conflict, l o w income settings, o f contracting with NGOs for delivering primary health care services. The results o f evaluations in Cambodia, Guatemala, and Haiti, are presented. In addition, the results from nutrition projects in Senegal and Madagascar which also used contracting with NGOs are also discussed.
32. Cambodia. Many years o f war and political upheaval l e f t Cambodia with a limited health infrastructure, particularly in rural areas. Health worker morale was poor, management capacity at the district level was very weak, and access to service was inadequate. A 1998 demographic and health survey found that, nation-wide, only 39 percent o f children were fully immunized. To address these serious issues, the MOH devised a “coverage plan” which included: (i) the
17

construction or rehabilitation o f health centers; (ii) merging smaller administrative districts into “operational districts” with a population o f about 150,000; and (iii) developing a minimum package o f activities (MPA) to be carried out at health center and comprising basic preventive and curative services such as immunization, family planning, antenatal care, and provision o f micronutrients.
33. three approaches to improving service delivery:
Approaches Used: Using loan funds from the Asian Development Bank, the M O H tested
(i) Contracting Out (CO) in which the contractors had complete l ine responsibility for service delivery, including hiring, firing and setting wages, procuring and distributing essential drugs and supplies, organizing and staffing health facilities.
(ii) Contracting In (CI) in which the contractors worked within the M O H system and had to strengthen the existing district structure. The contractors could not hire or fire staff, although they could request their transfer. Drugs and supplies were provided to the district through the normal MOH channels. The contractor received a budget supplement o f US$0.25 per capita per year to spend o n incentives for staff, operating expenses, etc.
(iii) ControYComparison (CC) in which the management o f services remained in the hands o f the District Health Management Team (DHMT) and drugs and supplies continued to be provided through normal MOH channels. As with the CI, the DHMT receives a budget supplement o f US$.25 per capita per year to spend o n incentives for staff, operating expenses, etc. Technical assistance and training o n management were provided to the DHMT.
34. Evaluation Methodology. Twelve districts were randomly assigned to the three different approaches and baseline household and health facility surveys were carried out in late 1997. Contracts were signed with the NGOs in December 1998 and follow-on surveys were carried out in August 2001, about 2.5 years after implementation began. The surveys were carried out by a third party and data was collected o n the parameters stipulated in the contract. Households were divided into “poor” or “not poor” based o n observable assets.
35. Results. As can be seen in Figure 1, the districts were very similar at baseline but after 2.5 years o f implementation the CO districts were providing many more services than the C I districts which were providing significantly more services than the Government was in the control districts. This pattern held for a l l the indicators stipulated in the contracts (see Figure 2). The cost o f CO was about US$4.50 per capita per year to the Government, however people in the community were paying significantly less out o f their own pockets (see Figure 3). The difference in cost between the C I and control districts in cost was the price o f the management contracts with the NGOs.
18
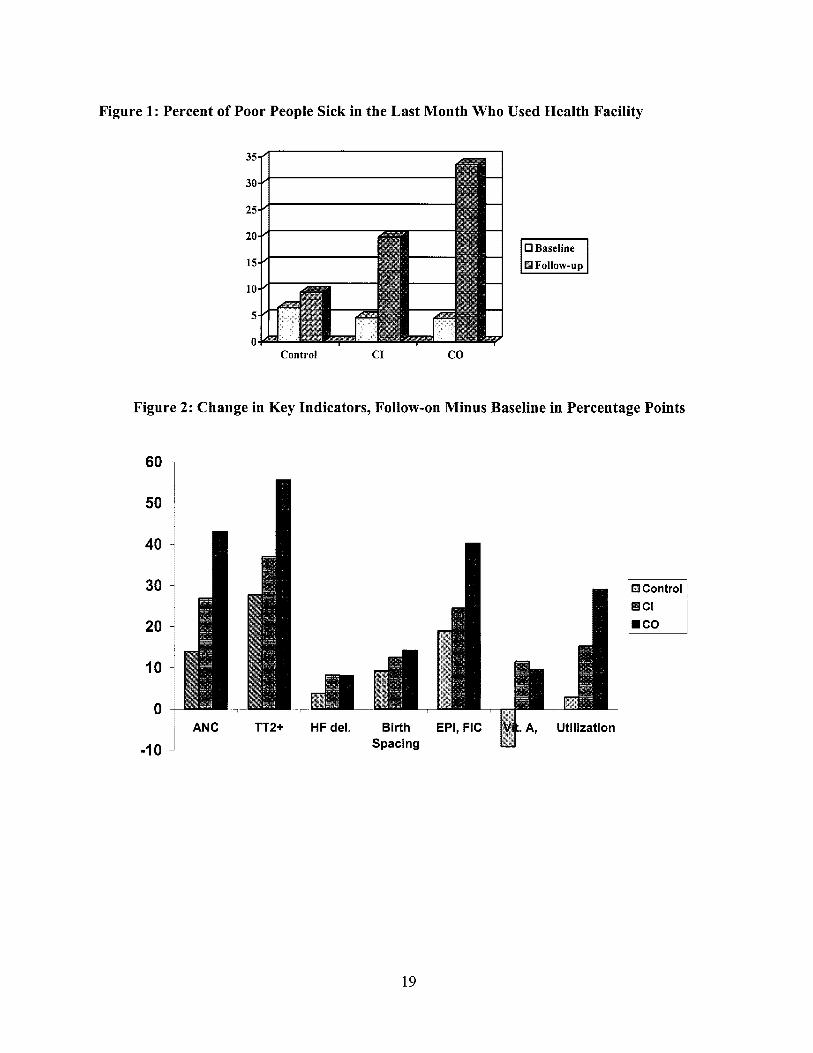
Figure 1: Percent of Poor People Sick in the Last Month Who
_ _
Used Health Facility
0 Baseline
Control C I CO
Figure 2: Change in Key Indicators, Follow-on Minus Baseline in Percentage Points
6o 1 I
50
40 -
30 -
20 -
10 -
0 - TT2+
-1 0 I ANC HF del. Birth EPI, FIC ~ A, Utilization
Spacing %
19

Figure 3: Annual Per Capita Expenditure on Health Care (US$)
% Illiterate
% o f households with MOH facility more than 2 1 km away % o f households in areas with “difficult access”
% o f households with MOH facility less than 10 km. away
30
60 65 62 70 80 44 11 8 24 9 11 23
25
20
15
10
5
0
0 Out-of-pocket Gov’tldonorRVGO
Control C I co
36. Guatemala. As part o f the agreement ending many years o f c iv i l war, the Government o f Guatemala was obliged to improve the delivery o f services to the indigenous people who make up about 50 percent o f the population. The indigenous communities suffered from infant mortality rates that were 50 percent higher than that o f the rest o f the country. To improve the delivery o f primary health care, the Government tried three approaches: (i) in remote areas it contracted out service delivery to NGOs (this was called the “direct method” and resembles “contracting out”); (ii) in less remote areas it gave NGOs contracts to manage existing health facilities (this was called the “mixed” approach and was similar to “contracting in”) based on a per capita fee; and (iii) also in the less remote areas, i t allowed Government officials to manage some o f the facilities (this was called the “traditional” approach and resembled the “control” group in Cambodia).
37. Evaluation Methodology. There was no baseline data available in Guatemala, however three years after the contracting process began, household surveys were carried out in randomly selected areas implementing the three different approaches. Unfortunately, the areas implementing the “direct” approach appear to have been more isolated and had less physical access to services than the other experimental groups (see Table 5).
Table 5: Characteristics of the Areas Implementing the Different Approaches used in Guatemala
Household Characteristics I Traditional 1 Mixed 1 Direct 1 1 % Mavan SDeaking. I 96
38. Results. I t appears that the “mixed” approach performed better than the Government providing services itself in the less remote areas where these two approaches were implemented. I t i s not clear whether the “direct” approach worked wel l or not given the absence o f baseline data and the fact that the areas where i t was implemented were more remote. This study i s usefb l because it was carried out in nearly ha l f the country and so covered a population o f about five mil l ion.
20

Table 6: Results of the Different Approaches to Service Delivery in Guatemala
% Coverage o f prenatal care
% coverage among children o f DPT3 Immunization % coverage among children o f Measles Immunization % o f children with diarrhea receiving ORT
% Tetanus toxoid coverage among pregnant women
Parameter I Traditional I Mixed I Direct I 75 87 78 63 68 57 69 80 63 54 61 51 39 55 36
Parameter NGO #1 NGO #2
Immunization 40 44 79 49 54 69 Coverage Prenatal Care 32 38 36 49 59 44 Coverage
Planning Discontinuation Rate
baseline target followup baseline target followup
Family 32 24 43 43 32 30
39. Haiti. USAlD had been supporting NGOs in Hait i to provide health services in the country- side, because Government service delivery post-conflict had nearly ceased. However, USAID was somewhat disappointed in the performance o f these NGOs who were paid o n the basis o f inputs. In an attempt to improve performance, i t offered NGOs a chance to receive 95 percent o f their contract payment in exchange for the opportunity to receive performance bonuses worth 10 percent o f the contract payment if they achieved specific targets for service delivery. Three NGOs accepted the offer and baseline and follow-on surveys were carried out by a third party, seven months apart.
NGO #3 baseline target followup
35 38 73
18 21 16
26 20 12
40. Results. As can be appreciated from Table 7, al l three NGOs made truly remarkable progress in improving chi ld immunization coverage, given the short period o f observation. The average increase o f 32 percentage points wil l be expected to have a large impact o n chi ld health. However, for other services the picture i s mixed. O n prenatal care no progress was made and for family planning discontinuation rates (the lower the better), and two o f the three NGOs made significant progress while the other actually lost ground.
Table 7: Baseline, Target, and Follow-up Data (in Percent) for Three NGOs in Ha i t i
41. Madagascar and Senegal. Marek et a1 described two Wor ld Bank supported projects in Madagascar and Senegal which contracted with NGOs to provide nutrition services for women and children. The services included: (i) monthly growth monitoring for children; (ii) weekly health and nutrition education activities for the women; (iii) referral o f unvaccinated children, pregnant women, severely malnourished children, and beneficiaries who were sick; and (iv) supplementary feeding for malnourished children. The projects covered 3 1 1,000 and 23 1,000 women and children respectively.
42. Results. There were non-project (control) communities. However, these neighborhoods were “contaminated” by large proportion o f children who participated in the program. Before and
21
after surveys in one project community in Senegal found that severe malnutrition declined from 6 percent to 0 percent and moderate malnutrition declined from 28 percent to 24 percent in 17 months. The study also found that there was a large reduction in malnutrition rates among cohorts o f proj ect participants.
43. Conclusions from the Literature. From the available studies it appears that contracting with NGOs to deliver health or nutrition services i s effective and the improvements can be achieved rapidly. However, there are methodological concerns with al l the studies: (i) the evaluation in Guatemala suffered from a lack o f baseline data and the likelihood that the most difficult communities were contracted out; (ii) the study in Hait i from a l ikely volunteer bias among the NGOs and a lack o f control areas; and (iii) the study in Madagascar and Senegal from the lack o f an uncontaminated control group. Only the study in Cambodia rigorously compared NGO provision o f services to government provision and found that NGOs performed better in terms o f effectiveness, efficiency, and equity. Based on the available information, i t appears l ikely that contracting with NGOs to deliver services wil l provide better results than government provision o f the same services.
V. ENVIRONMENTAL AND SOCIAL SAFEGUARD ISSUES
44. This project i s being prepared under OP8.50 Emergency Recovery Assistance. Nonetheless, the procedures and approaches being proposed under the Environmental and Social Safeguards Framework for other projects in Afghanistan (infrastructure, education, and community driven development) wil l also be applied to this project. The project i s classified as environmental category "B", and safeguards classification "S2".
45. Environmental Issues. Most o f the environmental issues in the proposed project relate to the management o f wastes generated in BHCs and rural hospitals. The most important medical waste arising from these sources wil l be sharps (needles, syringes and lancets) and other pathological materials such as used dressings. The main approach to dealing with health care waste wil l be segregation o f pathological materials and deep burial. Sharps will be collected in safety boxes which will be buried deeply according to WHO guidelines. A draft environmental plan has been developed and disclosed to the public which envisions three phases: (i) pilot testing o f simple and appropriate approaches during the f i rst year o f the project with guidelines and training modules developed based on f ield experience; (ii) widespread dissemination o f and training o n the guidelines will be carried out during the last two years o f the project; and (iii) a longer-term development o f an Action Plan for Management o f Health Care Waste based on analysis o f waste volume and field experience. The procedures to be followed for the collection and disposal o f wastes will be included in the PPAs and monitored as part o f the third party performance audits o f health facilities.
46. Indigenous Peoples. In order to ensure that all ethnic groups obtain equitable benefits from project investments, the MOH will: (i) ensure that the distribution o f BHCs by district is fairly and transparently decided; (ii) ensure that PPAs are differentially focused o n provinces which are currently under-served (many o f which have significant populations o f ethnic minorities); and (iii) use the results o f household surveys to gauge the access o f services to the different ethnic minorities and have the MOH and NGOs make course corrections where needed.
22
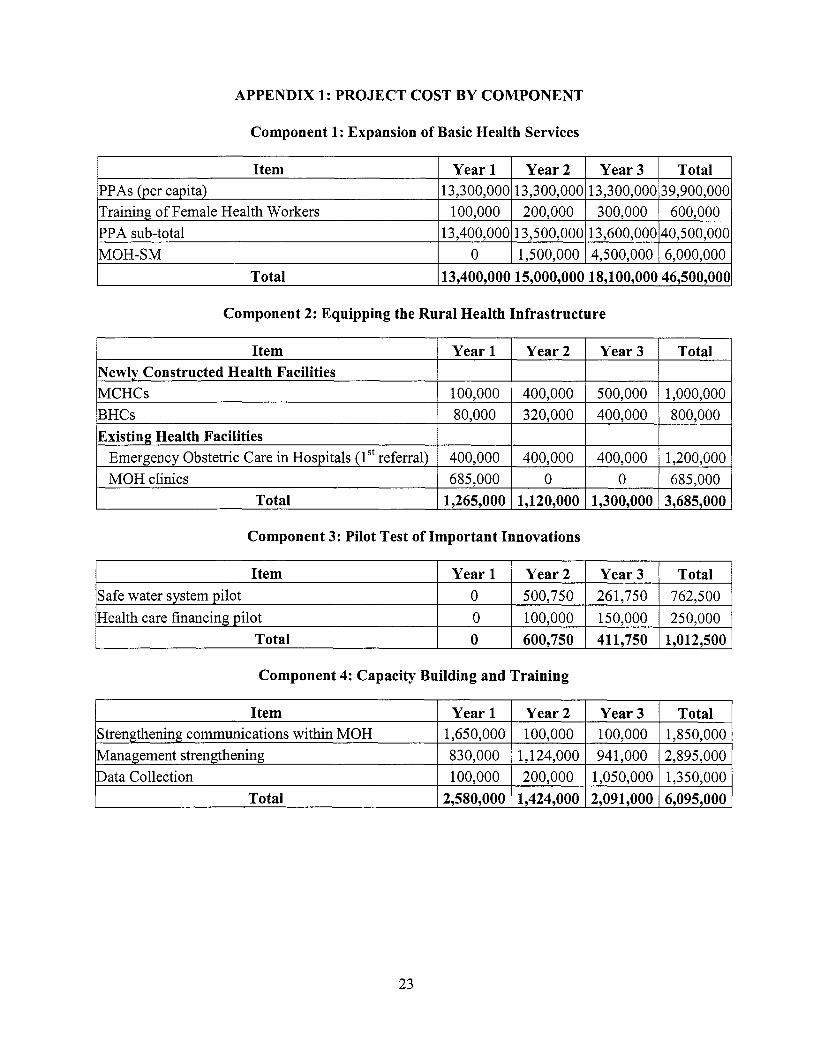
APPENDIX 1: PROJECT COST BY COMPONENT
PPAs (per capita) Training o f Female Health Workers PPA sub-total M O H - S M
Total
Component 1: Expansion of Basic Health Services
1 3,3 00,000 13,3 00,000 13,3 00,000 3 9,900,000 100,000 200,000 300,000 600,000
13,400,000 13,500,000 13,600,000 40,500,000 0 1,500,000 4,500,000 6,000,000
13,400,000 15,000,000 18,100,000 46,500,000
~ Item I Year 1 I Year2 I Year3 I Total 1
Newly Constructed Health Facilities MCHCs BHCs
100,000 400,000 500,000 1,000,000 80.000 320.000 400.000 800.000
Component 2: Equipping the Rural Health Infrastructure
Existing Health Facilities Emergency Obstetric Care in Hospitals ( lSt referral) M O H clinics
Item 1 Year1 I Year2 I Year3 I Total 1
400,000 400,000 400,000 1,200,000 685.000 0 0 685.000
Item Safe water system pi lot Health care financing pi lot
Total
Year 1 Year2 Year3 Total 0 500,750 261,750 762,500 0 100,000 150,000 250,000 0 600,750 411,750 1,012,500
Total I 1,265,000 I 1,120,000 I 1,300,000 13,685,000 I
Item Strengthening communications within MOH Management strengthening Data Collection
Total
Year 1 Year2 Year3 Total 1,650,000 100,000 100,000 1,850,000 830,000 1,124,000 941,000 2,895,000 100,000 200,000 1,050,000 1,350,000
2,580,000 1,424,000 2,091,000 6,095,000
Component 4: Capacity Building and Training
23

APPENDIX 2: FINANCIAL MANAGEMENT, AUDIT, AND DISBURSEMENT ARRANGEMENTS
Country Issues
1. Since there i s no Country Profile o f Financial Accountability (CPFA) or Country Financial Accountability Assessment (CFAA) for Afghanistan, and there is inadequate knowledge o f country issues and related strengths and weaknesses, reliance is to be placed on altemate compensating controls to help ensure that the Project’s financial objectives are accomplished. Financial management capacity in the country i s not yet fully functional. Mit igation measures taken by the Interim Administration include the engagement o f a Financial Management (FM) Agent under the recently approved Intemational Development Agency (IDA) financed Emergency Public Administration Project. Under these contracts, two intemational Agents-Financial Management and Audit-approved by Bank regional management are responsible for working with the Transitional Islamic State o f Afghanistan (TISA) line ministries to carry out these core functions.
Financial Management Arrangements
2. Financial management and audit functions for the proposed project wil l be undertaken with appropriate support from the FM Agent and the Audit Agent. The FM Agent will be responsible for assisting the MOF to maintain the accounts for a l l Government expenditures, including IDA-financed projects and the proposed Project, in addition to building capacity within TISA for these functions. To supplement this function, a Chief Financial Adviser (CFA) with extensive international public sector financial experience will be engaged in the M O H to coordinate financial management and reporting for the Project. The government’s budgeting and accounting systems wil l be used, and systemic accounting and expenditure reports wil l be supplemented with more detailed spreadsheets and analyses as deemed necessary. Quarterly Financial Monitoring Reports will be prepared by the MOH’s accounting unit (the Budget and Financial Management Unit), consolidated by the CFA, reviewed and approved by the MOF, and supported by the FM Agent.
Strengths and Weaknesses
3. In the Interim National Health Policy 2002-2004, the MOH sets as i t s f i rs t goal: “stewardship o f the health sector by the MOH to ensure transparency, accountability, advocacy, and regulation.” The engagement o f the FM Agent and recruitment o f the CFA, along with the TISA’s commitment to transparent and accountable financial management, are strengths o f the project’s financial management system. System protocols and procedures will include preventive controls as far as is practical in the existing environment. Further, the project’s program o f social controls, health surveys and independent field monitoring by journalists and non-governmental organizations (NGOs) will provide additional security that transgressions will be discovered. The MOF has also expressed his preference for the amounts being provided to the provincial health departments to be publicized.
Transitional Islamic Government of Afghanistan, Ministry of Health, Interim Health Strategy, 2002-2004: A Strategy to Lay Foundations (February 2003)
24

4. Accounting Challenges and MOH Strengthening and Suggested Actions.
The weaknesses and suggested corrective action plan are set out below under the sections
Project Staffing
5. The CFA wil l provide a proper interface and systems support to the MOH to assist i t s performance on the Project’s necessary financial management functions. The MOH has selected seven under-served provinces (Kapisa, Farah, Badghis, Nimroz, Hilmand, Wardak, and Sari-Pul) and wil l select another three provinces, to have basic health services enhanced in one o f two ways. In seven provinces NGOs2 wil l be recruited to deliver services under performance-based partnership agreements (PPAs). In the other three provinces, a MOH strengthening mechanism (MOH-SM) wil l be implemented in which the provincial health departments wil l have their capacity strengthened and provided the resources to implement an annual plan that they devise.
6. At the MOH, program monitoring and oversight wil l rest with the BFM under the Management and Administration Department, and reconciliation o f the grant transfers and budgetary allocations wil l be the responsibility o f the Grants and Contracts Management Unit (GCMU) under the Policy and Planning Department. Fol lowing the current reorganization o f the MOH, the staff and capacity within these units will be increased and strengthened in order to perform the required management, work, checks, balances and reconciliations o f project expenditures. Given the existing fiamework and environment, there i s clearly a need to recruit a C F A within the MOH appointed as a consultant in the f i rst year, reporting to the new Director, Management and Administration Department. The incumbent should possess an accounting degree with at least five years o f public sector financial experience and be capable to provide leadership, management and oversight in areas including finance, accounting, auditing, and information systems. In the interim period fol lowing grant effectiveness, the FM Agent will need to provide the MOH with accounting support and capacity (see paragraph 15 below under Accounting Challenges and MOH Strengthening).
7. The need for good financial management systems and people i s shared with most other ministries. Ad hoc donor funding is not a sustainable solution, and IDA is encouraging the government to promulgate a decree allowing market related remuneration o f key personnel in ministries. In addition, the Afghanistan Reconstruction Trust Fund (ARTF) i s financing a Chief Financial Advisers’ project. As Health is one o f the key spending ministries, the funding for the C F A and management and systems support falls under the ambit o f such ARTF funding. If appropriate resources are not available by a mutually agreeable date, project funds could be used to finance this activity. In addition, under the first Afghan Public Administration Project, IDA i s financing a contract with the FM Agent to establish government financial management systems.
Accounting Policies and Procedures
8. The Project wil l fol low standard T ISA financial management policies and procedures, including use o f the TISA Chart o f Accounts to record project expenditures in various l ine ministries, and will be processed by the “Free Balance” automated financial system currently
NGO selection criteria should include audited financial statements with “clean” audit opinions in the past three years, and evidence o f operations on a “going concern” basis..
25
being implemented in the MOF by the FM Agent. The use o f these procedures wil l allow for adequate recording and reporting o f the Health Project expenditures along similar lines to those used for the earlier IDA projects.
9. Project expenditure at the provincial level wil l be maintained by the provincial offices, and monthly reports submitted to the MOH. It i s expected that provincial reporting to the Center wil l be performed o n a timely basis. Accounting records wil l be consolidated centrally by the CFA based at the MOH with the assistance o f the new financial system, and reviewed and approved by the MOF.
Funds Flow
10. The project wil l use the existing government system as much as possible. As i s the practice for government expenditure, al l project payments wil l be routed through the MOF. The FM Agent will assist the MOF in executing and recording project payments.
11. Treasury officials at the MOF will be the authorized persons to operate the U S D Special Account for the IDA projects at the D a Afghanistan Bank (DAB); IDA funds wil l be deposited into the Special Account. When a project payment i s required to be made, implementing agencies (line ministries and other government departments) wil l submit a standard payment request to the MOF-Treasury. Treasury officials, after verifying the documents and checking the availability o f finds in the Special Account and budget will: (a) for payments in Afghanis, issue a check in Afghanis for encashment at the DAB; and (b) for a payment in foreign currency, instruct DAB to execute the payment. Payments to the PPA NGOs will be handled through this funding system controlled at the Center.
12. Project payments to MOH provincial officials implementing the M O H - S M approach, wil l also follow the Government’s financial management and administrative procedures and will be accounted for by the provincial MOH administration and bank accounts at the DAB’S provincial offices, if operational in the selected provinces.
13. For purposes o f funds f low planning, i t is important that the Project’s CFA, NGOs, M O H provincial officials, FM Agents, MOF-Treasury Officials, and DAB staff closely coordinate, monitor and communicate cash f low requirements for project activities.
14. Due to reasons related to security, damaged infrastructure, and a breakdown in communication between the branches and the Kabul office o f DAB, the T ISA will face a challenge in effecting payments throughout the country. Although not a l l o f DAB’S branches are currently fully functional, efforts are being made to rehabilitate the branches so that the TISA’s payment needs throughout the country can be met, including making arrangements for secure transport o f cash notes around the country. In the short term, there could be a shortage o f Afghani currency notes within the government.
15. The PPA NGOs will receive h n d s transfers at the center or in foreign currency outside Afghanistan if they have international bank accounts, and they will be entirely responsible for the transport, custody, safekeeping and distribution o f funds in the provinces and districts. From an MOH perspective, this arrangement presents a far lower level o f fiduciary r i s k than the transfer o f funds to provincial MOH officials in the other three provinces, by use o f the
26
Mustaufiats or through other couriers. Therefore, less than one-third o f proj ect expenditures wil l be vulnerable to a potentially higher level o f risk in the transfer o f funds f rom the center.
Accounting Challenges
16. The MOH i s in the midst o f a major reorganization which is expected to be shortly completed, approved by the Minister o f Health and ratified by the President and cabinet o f the TISA. At that point, the incumbents selected as department directors and unit heads wil l be announced.
(i) As mentioned in paragraph 6 above, the financial, accounting, auditing and information system aspects o f MOH operations wil l need to be led, managed and coordinated by a CFA, a position not currently reflected o n the M O H organogram. As an immediate "stop gap" measure until the new C F A i s recruited as part o f the upcoming ARTF-funded project, i t is imperative that the FM Agent and the M O F assist and support the M O H in providing a sufficient level o f accounting capacity, resource and oversight, to control and protect IDA'S funding and disbursement on this project.
(ii) The new unit head o f the BFM Unit wil l need at least one project accounting staff member with at least three years o f accountinglfinancial experience in the public sector to handle the accounting, reporting, reconciliation and control requirements o f the health project expenditures.
(iii) I t is very l ikely that the accounting and reporting skills o f MOH provincial accounting and financial staff will need to be considerably strengthened and appropriate support, on the job and "classroomyy training wil l need to be provided for at least 12 months through technical and on-site assistance from the MOF FM Agent (and the CFA's team following the appointment), on a continuing, sustainable basis for at least nine to 12 months.
17. The MOH, with support from the Department o f Intemational Development (DFID), has begun to examine its financial management system. In order to adequately handle the processing, accounting, reporting, reconciliation and monitoring o f Project expenditures, the MOH will have to do the following:
(i) MOH project expenditures wil l need to be carefully defined/classified to fit in with the MOF financial system chart o f accounts;
(ii) MOH financial forms/formats will need to be revisedhedeveloped for project transactions;
(iii) MOH central reconciliation and control procedures will need to be developed for oversight, monitoring, checking and reconciling funds transfers to and reporting o f project expenditures by NGOs and provincial health offices; and
27

(iv) Appropriate reconciliation and checking procedures wil l need to be developed between MOH central and provincial accounting records and between M O H and M O F financial records.
18. Payments to the PPA NGOs will be made at the center or in foreign countries if the NGOs have intemational bank accounts. The NGOs assume the entire r isk o f transport, custody, safekeeping, distribution o f and reporting o n the funds received from the government. Payment releases to the MOH provincial health departments under the M O H - S M will be done under a mechanism acceptable to M O F and IDA.
19. Once the above staff recruitments are in process, and procedures and protocols are being implemented, a simple f i rs t draft o f the FM sections o f the MOH Project Implementation Plan wil l need to prepared with the assistance o f the FM Agent, M O F and MOH financial managers and officials on board, in liaison with the IDA FM team. These sections should cover the key recording, accounting, checking, reporting, auditing and monitoring procedures. They should be refined and approved by the MOH CFA o n taking office. MOH senior officials expressed the view that if successful, this approach and manual wil l be “cloned” to other MOH health projects in the interests o f better accountability and transparency.
Suggested Actions
20. For ease of reference, a l i s t of the various suggested actions, other than the immediate need to require the FM Agent and the MOF to assist and support the MOH in providing a sufficient level o f financial consulting and accounting capacity, resource and oversight, i s set out in the following table.
1 .Recruitment o f MOH CFA reporting to Director, Management and Administration Department 2. Recruitment o f Budgeting and Financial Management Unit staff accountant
3. Support and on-the-job training and assistance to MOH provincial accounting and financial staff in M O H - S M Provinces 4. Development and customization o f chart o f accounts
5. Development o f financial management procedures governing M O H - S M acceptable to IDA
MOF officials, MOF assisted by FM Agent. MOH officials, Director, assisted by FM Management and Agent and Administration MOF Department MOH officials, BFM Unit Head/ assisted by FM CFA Agent and M O F M O F officials, MOF assisted by FM Agent M O H officials, Director, assisted by FM Management and Agent and Administration MOF Det.lartment/CFA
Within six months o f grant effectiveness Within thee months o f grant effectiveness
On a continuing basis for nine to 12 months after grant effectiveness Within three months o f grant effectiveness Prior to disbursement funds for the M O H - S M
28
Audit Arrangements
and Special Account
21. The accounts o f the Project will be audited by the Auditor General (with the support o f the Audit Agent), whose appointment has been approved by IDA’S management, and who i s extemal auditor for the earlier IDA Afghan projects on terms o f reference satisfactory to IDA. In l ine with other IDA financed projects in Afghanistan, the accounts will be audited in accordance with International Standards o f Auditing (ISAs) or other auditing standards approved by IDA. The annual Project financial statements to IDA will include a summary o f funds received (showing funds received fi-om al l sources), and a summary o f expenditures shown under the main Project components within the main categories o f expenditures. The format o f the annual Project financial statements wil l be a compilation o f the quarterly Financial Monitoring Reports (FMRs). The audit o f the Project accounts wil l also include an assessment of: (i) the adequacy o f the accounting and internal control systems over Statements o f Expenditure (SOEs) and Special Accounts; and (ii) the eligibility o f incurred expenditures for IDA financing. The annual Project financial statements, audited by the Auditor General, are to be submitted within six months o f the close o f TISA’s fiscal year. The following audit reports wil l be monitored in the Audit Reports Compliance System (ARCS):
General
Reporting and Monitoring
22. Quarterly Financial Monitoring Reports wi l l be produced showing: (i) sources and uses o f funds by disbursement category and project component as applicable; (ii) physical progress if applicable; and (iii) status o f procurement activities. These wil l be submitted to IDA within 45 days o f the end o f the quarter.
Disbursement Arrangements
23. Disbursement Method. Disbursements from the IDA Grant will be transaction-based (replenishment, reimbursement, direct payment, and payments under Special Commitments) with full documentation or against statements o f expenditures as appropriate. All withdrawal applications to the IDA, including replenishment, reimbursement and direct payment applications, wil l be prepared and submitted by the MOF.
29

Allocation of Grant Proceeds
Goods - M O H - S M
Consultant Services & Training-MOH-SM
Incremental Operating Costs-MOH-SM
Consultant Services & Training
Incremental Operating Costs
Sub-Grants Unallocated
Total
1.8 100 4.1 100 3.6 100 1.3 100 0.6 100
40.5 100 2.3 100
59.6 100
24. Financing Percentage. Since collection o f tax revenue has just begun and i s sporadic, disbursement percentages have been set at 100 percent, with the understanding that MOF will submit withdrawal applications on a net-of-tax basis. The TISA’s tax structure wil l be reviewed within six months o f Grant signing, at which time standard disbursement percentages wil l be set and financing percentages amended accordingly.
25. Use of Statements of Expenditures. Disbursements will be made on the basis o f SOEs for: (i) consultants and training for contracts not exceeding US$lOO,OOO for f i r m s and US$50,000 for individuals; (ii) goods for contracts not exceeding US$200,000; and (iii) incremental operating costs.
26. Special Account. A Special Account wil l be opened and maintained in a bank acceptable to IDA, and will be operated by MOF in accordance with the IDA’S operational policies. The Authorized Allocation o f the Special Account wil l be about US$6 million which represents the estimated amount o f expenditures to course through the Special Account in a four-month period. Given the short disbursement period and the immediate need for special account funds, the full amount o f the Authorized Allocation o f the Special Account wil l be available to MOF upon effectiveness. In order to meet immediate cash needs, MOF may convert Special Account funds into Afghani for distribution to provinces outside Kabul. Such advances wil l be limited to estimates o f the cash needs for a 30-day period and must be reconciled within 90 days o f disbursement from the Special Account.
27. Minimum Application Size. Applications for replenishment to the Special Account should be submitted monthly, regardless o f amounts disbursed, and must include reconciled bank statements as wel l as other appropriate supporting documents. The minimum application size for withdrawal applications for reimbursement, direct payment, or for applications for Special Commitments i s 20 percent o f the Authorized Allocation o f the Special Account. In the event that banking facilities are not fully functional at the time o f Grant effectiveness, IDA may, on an exceptional basis, waive minimum application size requirements in order to accommodate urgent needs.
30

28. withdrawal applications to the IDA.
Authority to Withdraw Grant Funds. MOF will retain the right to s i g n and submit
Legal Conditions
29. The following conditions wil l be incorporated into the legal agreements:
(i) Prior to disbursement o f funds under the MOH-SM, the MOH will develop financial management procedures for that component acceptable to the MOF and the Bank.
Supervision Plan
30. The Project will need intensive supervision. The focus during the supervision wil l be on the internal control arrangements for the Project and functioning o f accounting, financial reporting, and auditing.
31