Embed Size (px)
Citation preview

WORKSHOP: ANALYSIS OF SITTING, WEARING
NEURODYNAMIC GLASSES

Main wish of all wheelchair- dependent people:
to walk.• As long as we have a choice, there is no need for
arguments for or against something. We just do what we want to do.
• Retrospectively, we start wishing the opposite, or „if...“ sentences (after the „why...“ sentences).
• The loss makes us aware of the advantages of the lost.
• Having lost the ability to walk leads to sadness - until I am faster than the others / find another advantage.
• The question is: why should I train to sit in the wheelchair / to move the wheelchair, if I prefer to learn walking again?

Wheelchair is an orthosis - substitution for walking.
• Walking means moving from A to B.
• Do the same sitting in the wheelchair.
• At A you might sit on a chair, at B you might sit on a chair.
• Do the same after having moved with the wheelchair.
• At A you might stand upright, at B you might stand upright.
• Wheelchair is an orthosis - substitution for standing.
• Use different seats!

Substitution for walking and
standing.• For people with a
paraplegic or tetraplegic lesion.
• They cannot move easily from one chair to another.
• Therefore they need a special training for arm strengthening.
• They have to push themselves up several times a day.

Sitting in general:
• How many hours a day do we sit?
• Big changes within the last century.
• Why do we sit?
• Excuses, as „too long time for standing“, „there was a free seat“, „you cannot do computer work in standing“, ..., or break between activities, or at the end of a day....
• Which problems did increase within the last century?
• Back problems.
• Which recommendations do exist?
• Move. Frequently.

At which age are children able to sit for 4 hours or more?
• After the basic school years
• With (full) concentration to the content of the lectures
• Still moving all the time: leaning forwards / backwards / sideways, writing, picking up things from the floor, speaking with neighbours, going to the toilet, raising the arm....
• The longer they have to sit, the more they would need sports - the first item to be cut down
How long can you sit without moving?

The nervous system has two different kinds of tissue:
• Tissue for the impulse transport, e.g. axons, myelin, dendrits
• Supporting tissue, e.g. dura mater, pia mater, arachnoids, meninges, neuroglia, perineurinum, epineurinum.Functions: protection, speed, specificity, storage.

The nervous system should be considered as one organ.
If there is a change in one part of the
system, it will have repercussions to the
whole system. The continuity of the
tissues make this inevitable. (D.Butler)

Biomechanical properties of the nervous system• Variable neural gliding
extraneural and intraneural
• Variable neural elongation (at different parts different elongation)
• intraneurale pressure changes (with diabetes increased intrafascicular pressure)
• Viskoelasticity (delayed tendency to go back into former position)
are dependent upon
Physiological properties of the nervous system
variable intraneural blood supply
variable impulse transport
variable activation of the autonomic nervous system

Neuraxis
from the
medulla
oblongata
to the
filum
terminale.

„Slump-test“• strong test for the whole nervous system
• thoracal flexion down to T8 and neck flexion = thoracal and cervical neuraxis, then SLR +/- sensitising movements
• to reproduce signs and symptoms, if necessary
• to differentiate between muscle and neural tissue
Never use it if you find pain earlier or if you find
local pain in trunc / neck.

Total release position
Opisthotone:
„Convulsively extension of the head, the trunc and the limbs, as a reaction to a severe lesion to the CNS, like intracerebral bleedings, herniation of the brainstem, decerebration, meningitis, tetanus.“ (Pschyrembel)

Would you still follow the description of „hypotone muscles“?
He needs to be „hyperactive“ with the neck muscles in order to keep the balance, being pulled backwards that much.

The patient with ataxia needs more neural pre-loading for stability, the patient with stiffnesses needs more neural release to calm down.
Trunc rotation, either abstract, or with a task.
Bad sitting posture - treatment with overcorrection.
The position of the therapist is important.

Is she course participant or
patient?• Find many of these
positions, that no person could easily find an answer to this question.
• If she would sit in her wheelchair, the question would have been weird.
• The last day she came walking in - what a joy!
• She needed integration of both hands for a symmetric walking.

Transfer with pillows. Do you think he / she likes them?
Feeling save with support from both sides.
Even walking patients need a lot of external support / or points of
reference / feedback.
To be active / to demonstrate engagement, we lean forward.

Neurodynamic tests / lower limb:
SLR
straight leg raise (Lasègue)
sacral plexus L4-S3
PKB
prone knee bend
lumbar plexus L2-L4
If necessary:• neuraxis (”slump-
test”)• sensitising
movements / pre-loading
• differentiation tests for the target tissue
• component concept = sequencing

Sacral plexus
• L4-S3• Sciatic nerve• Tibial nerve• Sural nerve• Plantar nerve• Peroneal nerves


SLR - sensitising / preloading movements
Hip adduction• Hip medial rotation• Foot dorsiflexion• Foot plantarflexion• Heel inversion• Heel eversion• Toes extension• Pelvis depression• Pelvis rotation back• Neck flexion

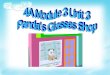
Total release positionThe typical flexion pattern in the leg,
often to be seen with patients lying
unpositioned supine.
The pelvis is retracted and elevated, in
sitting pulled backwards.
Hip joint in flexion, abduction and
lateral rotation, knee flexed, foot
inverted and plantarflexed.
Shacklock Clnical Neuodynamics

Good positions for the feet

Be happy about those patients who cannot tolerate a position for a long time, constantly moving around: at
least they feel the discomfort / ADHD-children.
But still: Take a lot of time to find a good position for them to rest / relax in between, no matter how many pillows / packs / walls they need.

Prerequisite for a good swallowing is a good sitting posture.
Prerequisite for regaining arm- and handfunction is no pulling / compressing damage onto the brachial plexus.

Each correction of the position in lying, sitting or standing has an
influence on neural structures as well.
(BATSA: Basler Anterior Trunc Support Approach, Rehab Basel / CH)
The aim should not be: how long can he sit withoutdamaging himself.
What can he do while sitting: he needs interesting offers.
BUT

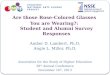
Learning
Lecture 5%
Reading 10%
Audio-visuell 20%
Demonstration 30%
Group discussion 50%
Practice by doing 75%
Teach others 90%