Embed Size (px)
Citation preview
Work-related stress among health professionalsworking in Swiss hospitals, nursing homes and homecare organisationsCitation for published version (APA):
Peter, K. A. (2020). Work-related stress among health professionals working in Swiss hospitals, nursinghomes and home care organisations: an analysis of stressors, stress reactions and long-termconsequences of stress at work among Swiss health professionals. Ridderprint.https://doi.org/10.26481/dis.20200922kp
Document status and date:Published: 01/01/2020
DOI:10.26481/dis.20200922kp
Document Version:Publisher's PDF, also known as Version of record
Please check the document version of this publication:
• A submitted manuscript is the version of the article upon submission and before peer-review. There canbe important differences between the submitted version and the official published version of record.People interested in the research are advised to contact the author for the final version of the publication,or visit the DOI to the publisher's website.• The final author version and the galley proof are versions of the publication after peer review.• The final published version features the final layout of the paper including the volume, issue and pagenumbers.Link to publication
General rightsCopyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyrightowners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with theserights.
• Users may download and print one copy of any publication from the public portal for the purpose of private study or research.• You may not further distribute the material or use it for any profit-making activity or commercial gain• You may freely distribute the URL identifying the publication in the public portal.
If the publication is distributed under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license above,please follow below link for the End User Agreement:
www.umlib.nl/taverne-license
Take down policyIf you believe that this document breaches copyright please contact us at:
providing details and we will investigate your claim.
Download date: 05 Apr. 2022
Work-related stress among health professionals working in Swiss hospitals, nursing homes and
home care organisations
An analysis of stressors, stress reactions and long-term consequences of stress at work among Swiss health professionals
Karin Anne Peter
The research presented in this thesis was conducted at Care and Public Health Research Institute (CAPHRI), Department of Health Services Research (HSR) of Maastricht University in collaboration with Bern University of Applied Sciences, Department of Health Professions, Applied Research and Development in Nursing, Bern, Switzerland. All the studies presented in this thesis were financially supported by the Bern University of Applied Sciences (BFH) and the State Secretariat for Education and Research (SER) of Switzerland. Copyright © Karin A. Peter, Maastricht, 2020 All rights reserved. No part of this thesis may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recoding on any information storage or retrieval system without permission from the author, or when appropriate, from the publisher of the publications. ISBN: 978-94-6416-059-8 Printing: Ridderprint BV Cover image: Fotolia
Work-related stress among health professionals working in Swiss hospitals, nursing homes and
home care organisations
An analysis of stressors, stress reactions and long-term consequences of stress at work among Swiss health
professionals
DISSERTATION
to obtain the degree of Doctor at Maastricht University, on the authority of the Rector Magnificus, Prof. Dr. Rianne M. Letschert
in accordance with the decision of the Board of Deans, to be defended in public
on Tuesday, 22 September 2020, at 10.00 hours
by
Karin Anne Peter
Supervisors Prof. Dr. J.M.G.A. Schols Prof. Dr. S. Hahn (Bern University of Applied Sciences) Co-Supervisor Dr. R.J.G. Halfens Assessment committee Prof. Dr. J.P.H. Hamers (Chair) Prof. Dr. R.A.C. Ruiter Dr. N.P.G. Boumans Prof. Dr. G. Meyer (Martin Luther University of Halle-Wittenberg) Dr. R. Schwendimann (University Hospital Basel)
Contents Chapter 1 General Introduction 8
Chapter 2 Work-related stress among health professionals in Swiss acute care and rehabilitation hospitals – a cross-sectional study
26
Chapter 3 Factors associated with work-private life conflict and leadership qualities among line managers of health professionals in Swiss acute and rehabilitation hospitals – a cross-sectional study
62
Chapter 4 Investigating work-related stress among health professionals at different hierarchical levels – a cross-sectional study
86
Chapter 5 Development and psychometric testing of an observation-based assessment tool focusing work-related stressors among health professionals: the STRAIN - External Observation of work Stressors
106
Chapter 6 Assessing work stressors in the health care sector by combining external observation and health professionals’ self-report in a cross-sectional study design
132
Chapter 7 General Discussion 150
Summary 172
Samenvatting 180
Valorisation 188
Acknowledgements 194
About the author 198
Publications 202
Chapter 1
General Introduction
General Introduction
8
Introduction
Health systems around the globe are struggling with the shortage of qualified health professionals.1, 2 However, health systems depend on the availability and performance of health professionals, and a shortage has the potential to destabilize the availability of and access to health services as well as the quality of the services provided.1 Demographic challenges with an ageing population and the occurrence of chronic diseases along with resulting high demands for treatment and nursing care are relevant aspects of the workforce shortage of health professionals.1, 2 In addition, an under-investment in education and a mismatch between education strategies and population needs as well as many expected retirements plus health professionals leaving their profession prematurely are further exacerbating the problem.1 In Switzerland, one of seven physicians and over 40% of nurses, midwives and medical-technical professionals have left patient care in the healthcare sector prematurely.3, 4 In comparison with other sectors, calculations reveal the greatest future staff requirement among health professionals in Switzerland.5 Moreover, the calculation of various scenarios for estimating personnel requirements up to 2030 has shown that an increase of around 30% of nursing staff alone is needed (reference scenario).6 Considering demographic trends, upcoming retirements and nurses leaving their profession prematurely, an additional number of 65,000 nursing staff will be needed by 2030 to meet the needs of the Swiss healthcare system in a population of 8.5 million inhabitants.6 However, not only nursing staff, but also physicians, medical-therapeutic and medical-technical professionals will be part of a potential future shortage of skilled workers.7
Stress at work, poor working conditions and reward frustration among the health professions all play an important role and are associated with health professionals’ intention to leave their career prematurely.8-10 In addition, a poor staffing level not only decreases health professionals’ job satisfaction and safety at work, it also decreases patient safety and quality of care provided.11, 12 Therefore, it is important to reduce stress at work and improve working conditions among health professionals for effective staff retention.13, 14
This thesis describes various aspects of stress at work through an analysis of (1) the extent of work stressors and their association with health professionals’ stress reactions and their long-term consequences in acute care and rehabilitation hospitals, (2) the extent of stressors, stress reactions and long-term consequences at different hierarchy levels as well as (3) the extent of health professionals’ self-reported and externally observed work stressors in Swiss hospitals, nursing homes and home care organisations. The first chapter introduces the prevalence and consequences of stress at work and gives a definition of stress at work. In addition, it presents an overview of relevant models and theories, approaches to assessing stress at work as well as aims and objectives of this PhD project.
General Introduction
9
1. Stress at work - prevalence and consequences
Stress at work is becoming increasingly relevant, with one in six European employees reporting chronic health problems.15 The European Foundation for the Improvement of Living and Working Conditions evaluates stress at work every five years throughout Europe. Their latest results from 2019 revealed that 17% of European employees were affected by chronic health problems, with especially women reporting on average a lower sense of well-being, more work-related health problems and a poorer quality of sleep than men.15
In Switzerland, 21% of employees experienced stress at work ‘often to always’ in 2017.16 Especially in the health care sector, a significant increase from 18% to 23% in work-related stress was reported during the last few years.16 Health professionals are particularly affected by work-related stress, since their daily work involves many stressors such as high emotional and physical demands at work, working under time pressure and understaffing. Also, long working hours, work-privacy conflicts as well as the exposure to infectious diseases, hazardous substances or work-related violence are frequent stressors of health professionals.8, 17, 18
Stress at work can not only negatively affect health professionals’ job satisfaction and intention to leave, but also their safety at work and health status.19 Study results reveal that health professionals affected by high levels of work-related stress are more likely to suffer from burnout-symptoms, musculoskeletal disorders, coronary artery disease or poor sleep quality.20-22 Furthermore, stress at work accounts for 24% of the total health-related product losses due to absenteeism and presenteeism.23 In Switzerland, those costs correspond to 3.2% of employees’ average monthly earnings.23
2. Definition of stress at work
For this thesis, ‘stress at work’ or ‘work-related stress’ is defined as ‘a pattern of reactions that occurs when employees presented with demands or pressures (stressors) that are not matched to their knowledge, abilities and skills and which challenge their ability to cope’ (p.4/2).21, 24 In the context of this, ‘stressors’ or ‘risks for work-related stress’ refer to aspects of the design and management of the work as well as to the social and organisational contexts that have a potential for adverse psychological, physical or social outcomes for workers.25, 26
General Introduction
10
3. Models and theories of stress at work
There are many models and theories of stress, but two models - the ‘Job Demand-Control Model’ and the ‘Effort-Reward Imbalance Model’ - have especially dominated the literature.21 The model of ‘causes and consequences of work-related stress’ contains those two models and gives a more comprehensive picture of stress at work.21, 27 These three models are presented in more detail below.
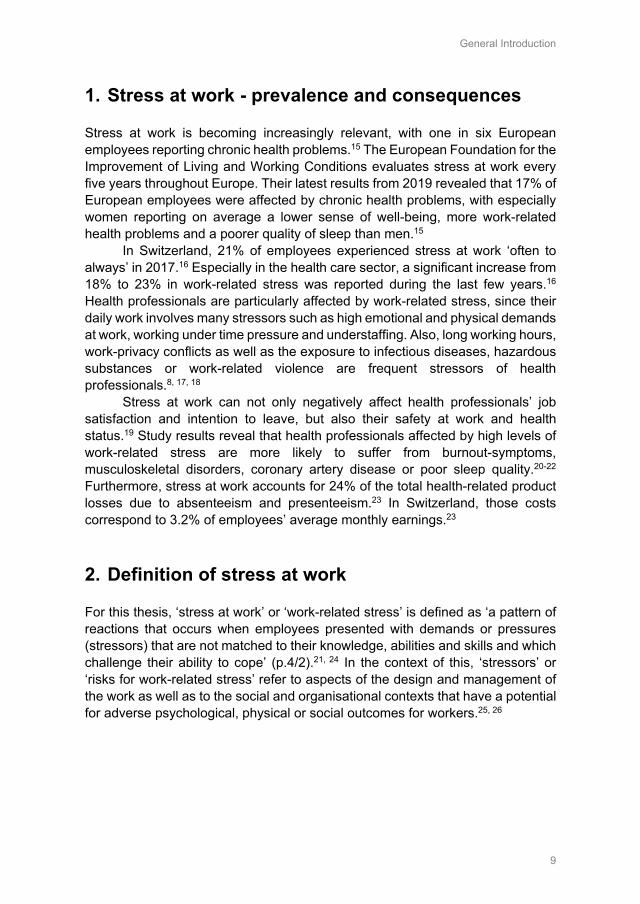
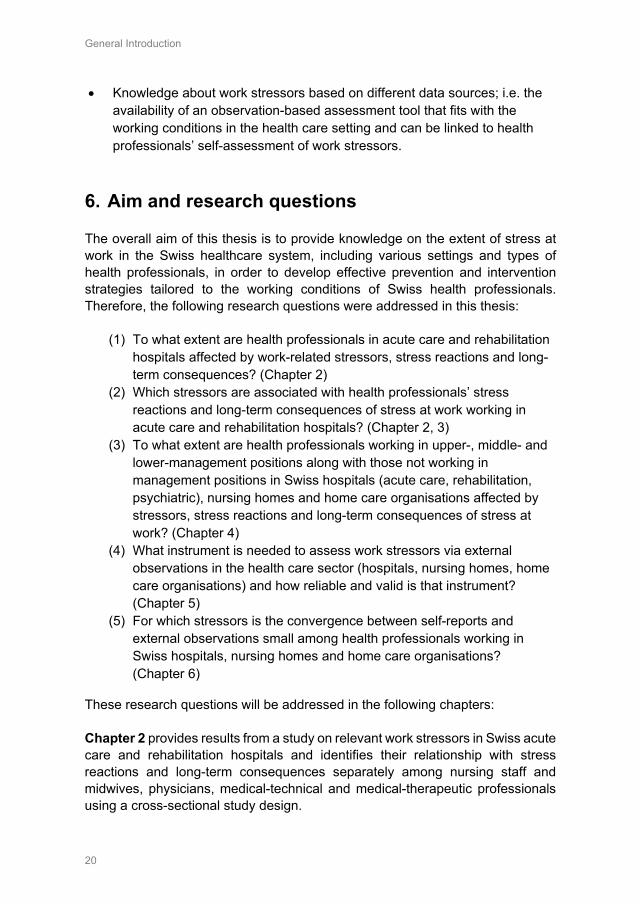
3.1 The Job Demand-Control Model The Job Demand-Control (JDC) model of Karasek28 considers the interaction of job demands (e.g. work pace, conflicting demands) and job decision latitude (e.g. decision authority, control). As shown in Figure 1, both may be present in low and high levels. If job demands and decision latitude are high, Karasek speaks of active jobs.28 While high decision latitude and low-moderate job demands are considered good, especially the combination of high job demands and low decision latitude is predicted to result in worse health and job dissatisfaction among employees.28
Figure 1 The Job Strain Model of Karasek28 The JDC model was extended in 1988 by Johnson and Hall29 to the Job Demand-Control-Support (JDCS) model. The assumption is that high job strain situation occurs if there is a high level of job-demands, low decision latitude and low social support at work. In the JDCS model the additional dimension of occupational social support by employees and superiors becomes an essential resource that buffers the effect of high demands and low decision latitude and therefore, psychological strain.29
General Introduction
11
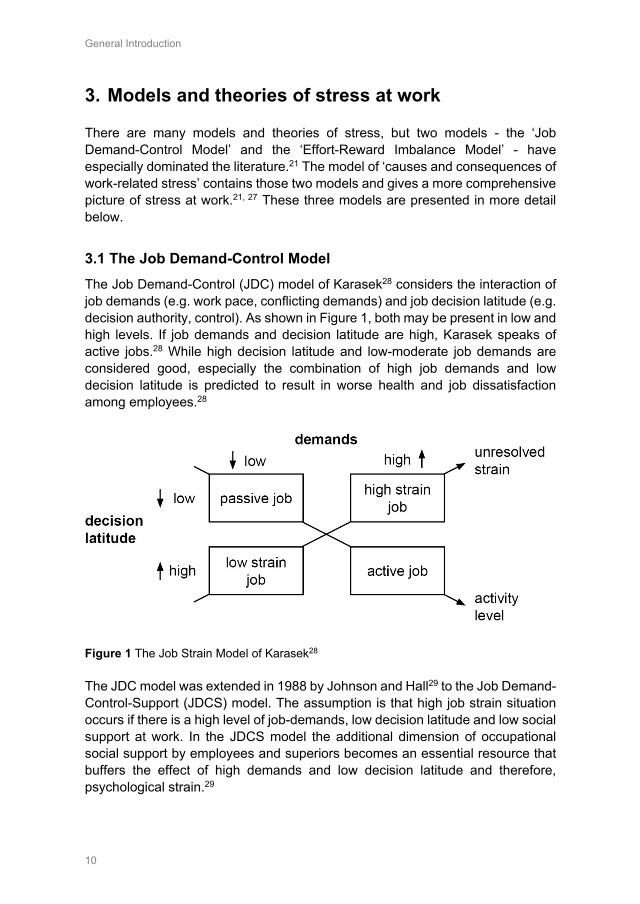
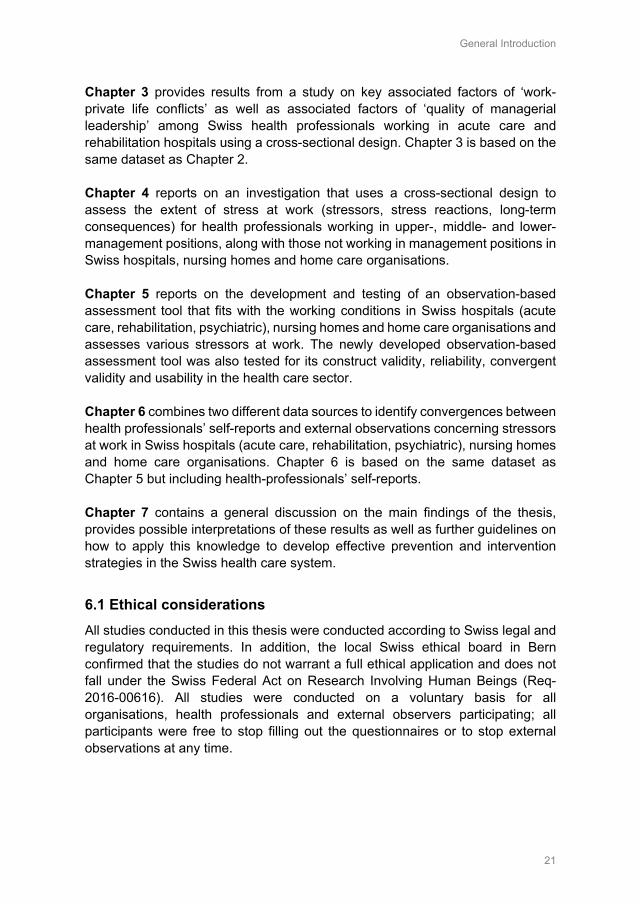
3.2 The Effort-Reward Imbalance Model The Effort-Reward Imbalance (ERI) model by Siegrist30 focuses on the reward rather than the control structure of work and is another model used to identify a stressful psychosocial work environment and its effects on employees’ stress-related health risks.31 As shown in Figure 2, the efforts at work and occupational rewards are two important key characteristics of this model.
Figure 2 The Effort-Reward Imbalance Model30, 31 The ERI model is based on the assumption that an imbalance between efforts and rewards results in strains, whereby high costs (effort) spent and low-gain (reward) received at work causes negative emotions, stress reactions and stress-related long-term effects on health.30-32 Efforts represents job demands and/or obligations at work, such as time pressures, physical demands or responsibility, which are imposed on the employee. Occupational rewards are distributed by the employer and include money (salary, wage), received esteem as well as promotion prospects and job security.31, 33 An existing over-commitment (personal characteristic, intrinsic) of the employees has the potential to intensify this process, whereby a highly overcommitted employee is more likely to respond with more strain reaction to an effort-reward imbalance than is a less overcommitted employee.33
3.3 The model of causes and consequences of work-related stress The model of ‘causes and consequences of work-related stress’ was originally developed from Kompier and Marcelissen27 and further adapted by different authors.21, 24 This model contains the JDC and the ERI Model and reveals stress as the result of a mismatch between individual needs and demands as well as those of the environment.21 Figure 3 presents the adapted model of ‘causes and consequences of work-related stress’ adapted by the Word Health
General Introduction
12
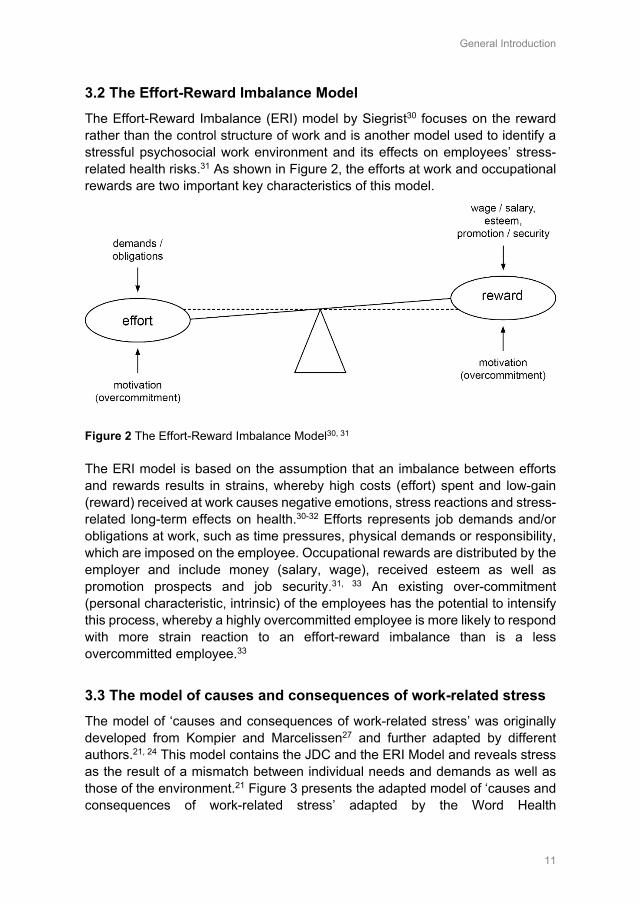
Organisation.21 This model illustrates the causes of stress (risks for work-related stress, stressors), stress reactions (short-term) and consequences of work-related stress (long-term) on the employee, individual characteristics of the employee as well as their inter-reactions.24
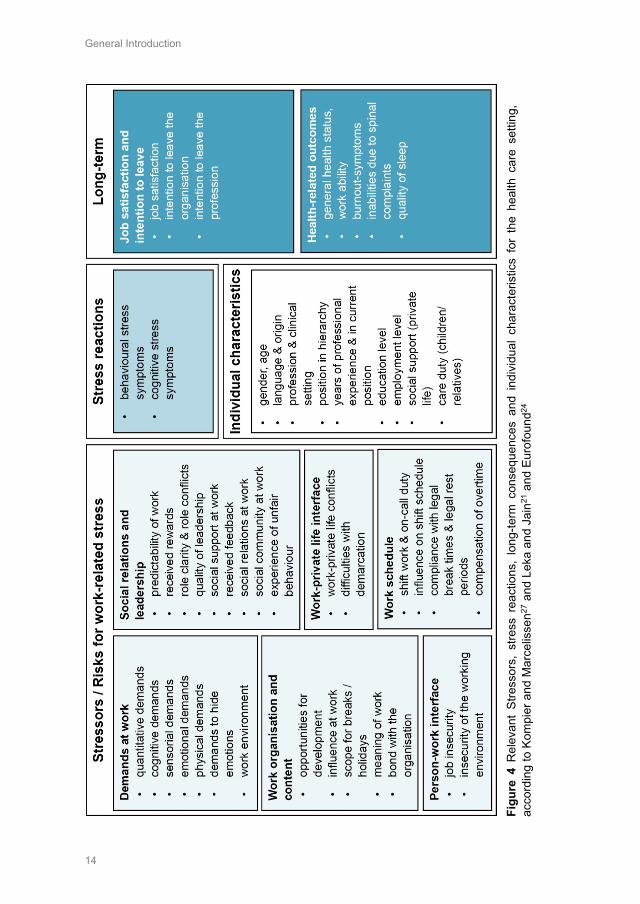
Figure 3 The model of causes and consequences of work-related stress based on Kompier and Marcelissen27, adapted from Leka and Jain21 and Eurofound24 Risks for work-related stress can arise from the job content (e.g. lack of variety, under-use of skills), the workload and work pace (e.g. overload of work, time pressure), the work schedule (e.g. shift work, long working hours), the control (e.g. decision authority) or the environment and equipment (e.g. lack of space, excessive noise) of the employee.21 Further risks for work-related stress can occur regarding the organisational culture (e.g. poor communication), the interpersonal relationships at work (e.g. poor relationships with superior and colleagues, lack of support at work), the role in the organisation (e.g. role clarity / ambiguity / conflict), the career development (e.g. job insecurity, under-promotion, poor salary) or the home-work interface (e.g. work-private life conflicts) or other risks (e.g. physical risks, aggression at work) of the employee.21 If employees are exposed to risk factors at work that are not matched to their knowledge, abilities, skills and ability to cope, stress reactions may result.24
Stress reactions may be physiological, behavioural, emotional or cognitive and have the potential to lead to more permanent health outcomes (long-term consequences) if they persist over a long time.24 Long-term consequences for the employee can result in less reversible psychological and social outcomes (e.g. mental health problems, cognitive

General Introduction
13
impairment) or physiological and physical (e.g. musculoskeletal disorder, cardiovascular disease, fatigue) or other outcomes (e.g. intention to leave the job / profession, absenteeism).24
Individual characteristics refer to characteristics of the employee, such as gender, age, educational level, values, competitiveness, over-commitment, family situation, social support in private life, physical fitness or his/her ability to cope with stressful situations. As Figure 3 shows, employee characteristics can have an impact on how an employee is able to deal with risks for work-related stress, and can also act as precursors or buffers of short-term and long-term consequences of stress at work.24
The model of ‘causes and consequences of work-related stress’ based on Kompier and Marcelissen27, adapted from Leka and Jain21 and Eurofound24 was used as a theoretical framework to guide this thesis because of its comprehensive picture of stress at work. However, this theoretical framework is rather general and is not specific to the health care sector. Therefore, possible stressors, stress reactions, long-term consequences and individual characteristics were identified to guide this thesis from the European longitudinal Nurses’ Early Exit study34, 35 and the RN4CAST study18 presented in Figure 4.
General Introduction
14
Figu
re 4
Rel
evan
t St
ress
ors,
stre
ss r
eact
ions
, lo
ng-te
rm c
onse
quen
ces
and
indi
vidu
al c
hara
cter
istic
s fo
r th
e he
alth
car
e se
tting
, ac
cord
ing
to K
ompi
er a
nd M
arce
lisse
n27 a
nd L
eka
and
Jain
21 a
nd E
urof
ound
24
General Introduction
15
4. Ways to measure stress at work
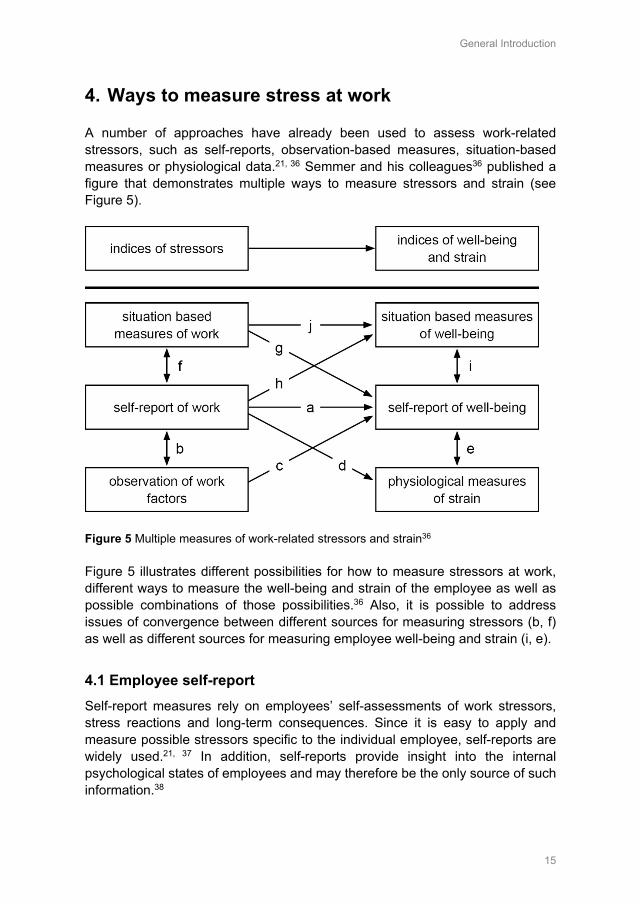
A number of approaches have already been used to assess work-related stressors, such as self-reports, observation-based measures, situation-based measures or physiological data.21, 36 Semmer and his colleagues36 published a figure that demonstrates multiple ways to measure stressors and strain (see Figure 5).
Figure 5 Multiple measures of work-related stressors and strain36 Figure 5 illustrates different possibilities for how to measure stressors at work, different ways to measure the well-being and strain of the employee as well as possible combinations of those possibilities.36 Also, it is possible to address issues of convergence between different sources for measuring stressors (b, f) as well as different sources for measuring employee well-being and strain (i, e).
4.1 Employee self-report Self-report measures rely on employees’ self-assessments of work stressors, stress reactions and long-term consequences. Since it is easy to apply and measure possible stressors specific to the individual employee, self-reports are widely used.21, 37 In addition, self-reports provide insight into the internal psychological states of employees and may therefore be the only source of such information.38
General Introduction
16
The advantages of self-report questionnaires are that they are easy to use, cost saving, yield large amounts of data in a short time and are mostly easy to analyse.39 However, using employee self-reporting is not free from potential biases and errors, e.g., which may influence an employee’s response style (social desirability, acquiescence), negative affectivity or other personality characteristics or individual attribution processes.36, 39 Thus, employee self-report can be a useful data source, if design criteria for a good questionnaire development are fulfilled (e.g. neutral wording, no mixing of assessing stressors and consequences).39
In their review, Leka and Jain21 summarized most relevant self-report questionnaires. The Copenhagen Psychosocial Questionnaire (COPSOQ)40 is one of the most widely used self-report questionnaires that assesses psychosocial stressors and stress reactions, as well as individual health and well-being21 and has the advantage of a strong scientifically grounded theoretical background.39 The ERI questionnaire is also often used and is based on the theoretical background of the Effort-Reward Imbalance model30, including specific questions about an employee’s effort, reward and overcommitment. The Job-Content Questionnaire (JCQ) based on the JDC model of Karasek41 is also a well-known self-report questionnaire and assesses an employee’s demands, control and support at work.21
4.2 Situation-based measures Situation-based measures refer to employees’ self-observation of events, experiences and actions related to stress at work, using event or time-sampling procedures.36, 42 For example, an employee writes a description of a stressful event that occurred in the prior month, consequences of this event for her-/himself and others as well as her/his experienced feelings and reactions and coping strategies.38, 43
The main advantages of situation-based measures are that the employee is free to assess stressors and effects that are relevant from their point of view, rather than presenting them with a predetermined set of answers.38 In addition, situation-based measures have the potential to reveal knowledge about what exactly happens in stressful situations, employee’s experiences, feelings and successful or non-successful coping strategies.44 Moreover, using event- or time-sampling procedures may decrease retrospective biases of employees, since they do not rely on memories over an extended time period.36 However, difficulties with this method of data collection can be the question of which events are considered to be stressful and which are not. Semmer and his colleagues36 illustrate this with an example: if a person is chronically affected by a high workload, she/he may not report ongoing time pressure as a current ‘event’ (p.241).36 Therefore, more stable and permanent stressors at the workplace may be less well represented using event-based measures.36 In addition, some of the

General Introduction
17
reported events may not be representative or typical and are in fact very rare, regarding employee’s overall working conditions and environment (e.g. current restructuring, move to another building).36 This depends also on the duration of the sampling period, while short periods over which events were sampled can limit the results.43 Moreover, situation-based measures are based on an employee’s self-assessment of stressful events and, therefore, have the same potential biases and errors as those described in the self-report.36 Nevertheless, situation-based measures can be a useful data source regarding stressors and employees’ well-being and strain, provided that the limitations, potential biases and errors described above are taken into account.
4.3 Observation-based measures Another possible source for assessing stressors at work is to use observation-based data (e.g. using external observers or superiors). Observation-based measures are expected to provide a more independent view (independent from the employee) of possible stressors at work.38 These measures are typically filled out by external observers, supervisors or are based on employee interviews.21 Most common stress observation measures are job and task analysis (e.g. work function, tasks), company analysis (company stress diagnosis) or observational-based checklists of work stressors.21, 45 Archival data is also often used, such as data on sickness absences or accidents at work.39
The advantages of using observational measures are that the work environment can be assessed directly, free from the possible influences of an employee’s personal characteristics or attributions.36 Nevertheless, it is not that easy to objectively capture stressors at the workplace and using observation-based measures can also be afflicted with problems and measurement errors. Observations can be cost consuming and, therefore, mostly only a limited time can be observed.46 This limited information that observers unavoidably have can lead to over-generalisation and the observer’s compensation for any missing data with the use of predominant information (e.g. halo-effect).36 Also, common stereotypes, which are related to the observer’s interpretation and level of knowledge are possible.36 In addition, many strains are internal states (e.g. emotional pressure, feeling unable to cope) or based on mental processes of the employees and, therefore, are not easy to observe externally.36, 37 Being observed can also influence employees’ behaviour and workflows. The presence of an external observer has the potential to influence the behaviour of the observed employee, e.g. due to personal characteristics of the observer (personal reactivity) or because they feel observed (procedural reactivity).46, 47 Moreover, using external observers can also introduce subjective bias according to the observer’s own experiences, perceptions or memories.36, 46 Also, the association of externally assessed (independent of the employee) stressors and an employee’s health outcomes are usually weaker than the employee’s self-
General Introduction
18
assessed stressors.21 Nevertheless, observation-based measures of stressors can be a useful data source, if attention is paid to personal and procedural reactivity, extensive training of observers, appropriate sampling procedures (e.g. duration and timing of observation) and observation-based data are used as a complement to rather than a substitute for self-reported data.36, 46
4.4 Physiological measures A further data source for assessing stress among employees at work is to use physiological measures. The focus of physiological measures of stress lies mainly on cardiovascular symptoms (such as an employee’s heart rate or blood pressure), biochemical symptoms (e.g. level of blood sugar, steroid hormones, cholesterol, catecholamines such as adrenaline, noradrenaline or level of uric acid) or gastrointestinal symptoms (such as peptic ulcers).36, 38, 48
The advantages of using physiological measures in assessing stress reactions is seen as an alternative to an employee’s self-assessment and the focus on central physiological stress responses.38, 39 In addition, physiological data are considered more robust and not easily adjusted to expectations of the employee and her/his subjective perception of stress and well-being.36 However, when using physiological measures to collect data on stress, it must be taken into account that ‘physiological systems are bodily systems in their own right’ (p. 224)36, following their own laws, and are therefore not simply another source for gathering data on stress.36 As Kompier describes, such bodily systems follow their own laws and are sometimes only partly coupled with each other and with other response systems (e.g. psychological and behavioural reactions to stress).39 This is also reflected in the inconsistency of the relation between self-reported mental stress and cortisol output in a previous review49, where no apparent associations could be found. In addition, collecting physiological data is not only more expensive than using employee’s self-reports, but also more cumbersome to collect and presupposes a certain level of employee compliance.36 Moreover, the validity of physiological assessments can be affected by numerous factors, such as stable factors of the employee (e.g. genetic tendency, race, age, sex), factors according to the time and amount of data collection, the environment (temperature, humidity), the behaviour of the employee (consumption of caffeine, nicotine, alcohol, food or their physical fitness) and the employee’s current health status.36, 38 Furthermore, physiological measures may provide knowledge about an employee’s physical reactions and give limited information about its cause (stressors) linked to those physical reactions.39 Nevertheless, physiological measures can be a useful data source of an employee’s stress reactions, if multiple measures over time are used, influencing factors are controlled as well as possible, a uniform procedure for handling the samples is used and base rate measures (in relaxed situations) are used to compare with measures of stressful situations at work.36, 38

General Introduction
19
4.5 Multi source measures Each of the above described ways of data collection brings its advantages and disadvantages. However, the convergence among different data sources is mostly low, which can make the interpretation of the results difficult and may raise the question of which source of data is more valid. For example, the convergence of subjectively and objectively assessed stress indicators usually ranges between 10 and 30%.21, 36 However, none of these measures is ‘superior’ to another, since each source of data in some way covers different perspectives, such as permanent or stable stressors and strain, certain stressful events, coping responses, external assessment of stressors or physiological response systems. Therefore, objectively assessed stressors should not be seen as ‘the true reality’ but rather as complementary to subjectively assessed stressors that provide further insights into the current work situation.36 Therefore, a combination of different sources of data contributes to a more complete picture of stress at work and is, therefore, recommended by various authors.36, 37, 39
5. Problem statement
Reducing stress at work and improving working conditions is essential for retaining health professionals at work.8, 18 Therefore, the determination of salient stressors at work and their association with health professionals’ stress reactions as well as the long-term consequences of stress at work are key to developing appropriate prevention and intervention strategies.50 Although some recent studies have been undertaken, these studies had a special focus on stress at work specifically among nurses51-53 or their results covered only a specific area of the Swiss healthcare system.8, 20, 54 In general, studies focusing on stress at work among different health professional disciplines, stress at work at different hierarchical levels or assessing stressors using different data sources are scarce. Thus, several gaps in our knowledge have been identified. They are: • Knowledge about the extent of stressors, stress reactions and long-term
consequences among different health disciplines (nursing staff and midwives, physicians, medical-technical and medical-therapeutic professionals), especially in Swiss hospitals.
• Knowledge about relevant work stressors associated with health professionals’ stress reactions and long-term consequences.
• Knowledge about the extent of work-related stress among health professionals working at different hierarchical levels.
General Introduction
20
• Knowledge about work stressors based on different data sources; i.e. the availability of an observation-based assessment tool that fits with the working conditions in the health care setting and can be linked to health professionals’ self-assessment of work stressors.
6. Aim and research questions
The overall aim of this thesis is to provide knowledge on the extent of stress at work in the Swiss healthcare system, including various settings and types of health professionals, in order to develop effective prevention and intervention strategies tailored to the working conditions of Swiss health professionals. Therefore, the following research questions were addressed in this thesis:
(1) To what extent are health professionals in acute care and rehabilitation hospitals affected by work-related stressors, stress reactions and long-term consequences? (Chapter 2)
(2) Which stressors are associated with health professionals’ stress reactions and long-term consequences of stress at work working in acute care and rehabilitation hospitals? (Chapter 2, 3)
(3) To what extent are health professionals working in upper-, middle- and lower-management positions along with those not working in management positions in Swiss hospitals (acute care, rehabilitation, psychiatric), nursing homes and home care organisations affected by stressors, stress reactions and long-term consequences of stress at work? (Chapter 4)
(4) What instrument is needed to assess work stressors via external observations in the health care sector (hospitals, nursing homes, home care organisations) and how reliable and valid is that instrument? (Chapter 5)
(5) For which stressors is the convergence between self-reports and external observations small among health professionals working in Swiss hospitals, nursing homes and home care organisations? (Chapter 6)
These research questions will be addressed in the following chapters: Chapter 2 provides results from a study on relevant work stressors in Swiss acute care and rehabilitation hospitals and identifies their relationship with stress reactions and long-term consequences separately among nursing staff and midwives, physicians, medical-technical and medical-therapeutic professionals using a cross-sectional study design.
General Introduction
21
Chapter 3 provides results from a study on key associated factors of ‘work-private life conflicts’ as well as associated factors of ‘quality of managerial leadership’ among Swiss health professionals working in acute care and rehabilitation hospitals using a cross-sectional design. Chapter 3 is based on the same dataset as Chapter 2. Chapter 4 reports on an investigation that uses a cross-sectional design to assess the extent of stress at work (stressors, stress reactions, long-term consequences) for health professionals working in upper-, middle- and lower-management positions, along with those not working in management positions in Swiss hospitals, nursing homes and home care organisations. Chapter 5 reports on the development and testing of an observation-based assessment tool that fits with the working conditions in Swiss hospitals (acute care, rehabilitation, psychiatric), nursing homes and home care organisations and assesses various stressors at work. The newly developed observation-based assessment tool was also tested for its construct validity, reliability, convergent validity and usability in the health care sector. Chapter 6 combines two different data sources to identify convergences between health professionals’ self-reports and external observations concerning stressors at work in Swiss hospitals (acute care, rehabilitation, psychiatric), nursing homes and home care organisations. Chapter 6 is based on the same dataset as Chapter 5 but including health-professionals’ self-reports. Chapter 7 contains a general discussion on the main findings of the thesis, provides possible interpretations of these results as well as further guidelines on how to apply this knowledge to develop effective prevention and intervention strategies in the Swiss health care system.
6.1 Ethical considerations All studies conducted in this thesis were conducted according to Swiss legal and regulatory requirements. In addition, the local Swiss ethical board in Bern confirmed that the studies do not warrant a full ethical application and does not fall under the Swiss Federal Act on Research Involving Human Beings (Req-2016-00616). All studies were conducted on a voluntary basis for all organisations, health professionals and external observers participating; all participants were free to stop filling out the questionnaires or to stop external observations at any time.
General Introduction
22
References 1. World Health Organisation. Global strategy on human resources for health: workforce 2030.
Geneva: World Health Organization, 2016. 2. Marć M, Bartosiewicz A, Burzyńska J, Chmiel Z, Januszewicz P. A nursing shortage – a prospect
of global and local policies. International Nursing Review. 2019;66(1):9-16. doi:10.1111/inr.12473 3. Streit S, da Costa BR, Christensen S, Tal K, Tandjung R, Juni P. One in seven Swiss physicians
has left patient care - results from a national cohort study from 1980-2009. Swiss Medical Weekly. 2019;149:w20116. doi:10.4414/smw.2019.20116
4. Lobsiger M, Kägi W, Burla L. Berufsaustritte von Gesundheitspersonal (Obsan Bulletin 7/2016). Neuchâtel: Schweizerisches Gesundheitsobservatorium, 2016.
5. Wunsch C, Buchmann M, Wedel S. Arbeits- und Fachkräftebedarf der Schweiz bis 2060. Basel: Abteilung Arbeitsmarktökonomie Wirtschaftswissenschaftliche Fakultät., 2014.
6. Merçay C, Burla L, Widmer M. Gesundheitspersonal in der Schweiz. Bestandesaufnahme und Prognosen bis 2030 (Obsan Bericht 71). Neuchâtel: Schweizerisches Gesundheitsobservatorium, 2016.
7. Kägi W, Lobsiger M, Morlok M, Frey M, Oswald A. Fachkräftemangel in der Schweiz - Ein Indikatorensystem zur Beurteilung der Fachkräftenachfrage in verschiedenen Berufsfeldern. Basel: Staatssekretariat für Wirtschaft (SECO), 2014.
8. Hämmig O. Explaining burnout and the intention to leave the profession among health professionals - a cross-sectional study in a hospital setting in Switzerland. BMC Health Service Research. 2018;18(1):785. doi:10.1186/s12913-018-3556-1
9. Lee YW, Dai YT, Chang MY, Chang YC, Yao KG, Liu MC. Quality of Work Life, Nurses’ Intention to Leave the Profession, and Nurses Leaving the Profession: A One-Year Prospective Survey. Journal of Nursing Scholarship. 2017;49(4):438-444. doi:10.1111/jnu.12301
10. Li J, Galatsch M, Siegrist J, Muller BH, Hasselhorn HM, European NSg. Reward frustration at work and intention to leave the nursing profession--prospective results from the European longitudinal NEXT study. International Journal of Nursing Studies. 2011;48(5):628-635. doi:10.1016/j.ijnurstu.2010.09.011
11. Aiken LH, Sermeus W, Van den Heede K, Sloane DM, Busse R, McKee M, et al. Patient safety, satisfaction, and quality of hospital care: cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ. 2012;344:e1717. doi:10.1136/bmj.e1717
12. Schubert M, Schaffert-Witvliet B, De Geest S, Glass T, Aiken L, Sloane DM, et al. RICH - Nursing Study. Rationing of Nursing Care in Switzerland = CH. Basel: Institut für Pflegewissenschaft im Auftrag des Bundesamts für Gesundheit, 2005.
13. Addor V, Schwendimann R, Gauthier JA, Wernli B, Jäckel D, Paignon A. «nurses at work» – Studie zu den Laufbahnen im Pflegeberuf über die letzten 40 Jahre in der Schweiz Neuchâtel: Schweizerisches Gesundheitsobservatorium, 2016.
14. Hasselhorn HM, Conway PM, Widerszal-Bazyl M, Simon M, Tackenberg P, Schmidt S, et al. Contribution of job strain to nurses' consideration of leaving the profession - results from the longitudinal European nurses' early exit study. Scandinavian Journal of Work Environment & Health. 2008;34(6):75-82.
15. Eurofound. Working conditions and workers' health. Luxembourg: Publications Office of the European Union, 2019.
16. Swiss Federal Statistical Office. Schweizerische Gesundheitsbefragung (SGB) - Arbeitsbedingungen und Gesundheitszustand, 2012–2017. Bern: Bundesamt für Statistik2019.
17. NIOSH. Exposure to Stress: National Institute for Occupational Safety and Health, 2008. 18. Aiken LH, Sloane DM, Bruyneel L, Van den Heede K, Sermeus W, Consortium RC. Nurses'
reports of working conditions and hospital quality of care in 12 countries in Europe. International Journal of Nursing Studies. 2013;50(2):143-153. doi:10.1016/j.ijnurstu.2012.11.009
19. European Commission. Occupational health and safety risks in the healthcare sector - Guide to prevention and good practice. Luxembourg: Publications Office of the European Union, 2011.
20. Hausler N, Bopp M, Hammig O. Effort-Reward Imbalance, Work-Privacy Conflict, and Burnout Among Hospital Employees. J Occup Environ Med. 2018;60(4):e183-e187. doi:10.1097/JOM.0000000000001287
21. Leka S, Jain A. Health impact of psychosocial hazards at work: An overview. Geneva: World Health Organization, 2010.
General Introduction
23
22. Taylor M, Bithoney W. 10 Steps to Developing a Culture of Health for Hospital and Health System Employers. Chicago: Truven Health Analytics, 2012.
23. Brunner B, Igic I, Keller AC, Wieser S. Who gains the most from improving working conditions? Health-related absenteeism and presenteeism due to stress at work. The European Journal of Health Economics. 2019;20(8):1165-1180. doi:10.1007/s10198-019-01084-9
24. Eurofound. Work-related stress. Dublin: Eurofound, 2005. 25. Cox T, Griffiths A. The nature and measurement of work-related stress: theory and practice. In:
Wilson JR, Corlett N, editors. Evaluation of Human Work. 3 ed. London: CRS Press, 2005. 26. Leka S, Griffiths A, Cox T. Work Organization and Stress. Geneva: World Health
Organisation2003. 27. Kompier M, Marcelissen F. Handbook of Work Stress: A Systematic Approach for Organizational
Practice. Amsterdam: NIA, 1990. 28. Karasek RA. Job demands, job decision latitude, and mental strain: Implications for job redesign.
Administrative science quarterly. 1979:285-308. doi:10.2307/2392498 29. Johnson JV, Hall EM. Job strain, work place social support and cardio-vascular disease: a cross-
sectional study of a random sample of the Swedish population. American journal of public health. 1988;78:1336-1342.
30. Siegrist J. Adverse health effects of high effort - low reward conditions at work. Journal of Occupational Psychology. 1996;1:27-43. doi:10.1037/1076-8998.1.1.27
31. Siegrist J. The Effort–Reward Imbalance Model. The Handbook of Stress and Health. Hoboken: John Wiley & Sons Ltd., 2017.
32. Siegrist J, Wege N, Puhlhofer F, Wahrendorf M. A short generic measure of work stress in the era of globalization: effort-reward imbalance. Int Arch Occup Environ Health. 2009;82(8):1005-1013. doi:10.1007/s00420-008-0384-3
33. van Vegchel N, de Jonge J, Bosma H, Schaufeli W. Reviewing the effort-reward imbalance model: drawing up the balance of 45 empirical studies. Social Science & Medicine. 2005;60(5):1117-1131. doi:10.1016/j.socscimed.2004.06.043
34. Estryn-Behar M, Van der Heijden BI, Oginska H, Camerino D, Le Nezet O, Conway PM, et al. The impact of social work environment, teamwork characteristics, burnout, and personal factors upon intent to leave among European nurses. Medical Care. 2007;45(10):939-950. doi:10.1097/MLR.0b013e31806728d8
35. Hasselhorn HM, Müller BH, Tackenberg P, Kümmerling A, Simon M. Berufsausstieg bei Pflegepersonal: Arbeitsbedingungen und beabsichtigter Berufsausstieg bei Pflegepersonal in Deutschland und Europa: Wirtschaftsverlag NW, Verlag für Neue Wissenschaften, 2005.
36. Semmer NK, Grebner S, Elfering A. Beyond self-report: Using observational, physiological, and situation-based measures in research on occupational stress. In: Perrewe PL, Ganster DC, editors. Research in Occupational Stress and Well Being 3ed. Amsterdam: Emerald Group Publishing Limited, 2004. p. 205-263.
37. Frese M, Zapf D. Methodological issues in the study of work stress: Objective vs. subjective measurement of work stress and the question of longitudinal studies 1988.
38. Connell P, Lee VB, Spector PE. Job stress assessment methods. JC Thomas (Vol. Ed.) and M. Hersen (Ed.), Comprehensive handbook of psychological assessment: Industrial and organizational assessment. 2004;4:455-469.
39. Kompier M. Assessing the psychosocial work environment--"subjective" versus "objective" measurement. Scandinavian Journal of Work, Environment & Health. 2005;31(6):405-408.
40. Kristensen TS, Hannerz H, Høgh A, Borg V. The Copenhagen Psychosocial Questionnaire-a tool for the assessment and improvement ofthe psychosocial work environment. Scandinavian Journal of Work, Environment & Health. 2005;31(6):438-449.
41. Karasek R, Brisson C, Kawakami N, Houtman I, Bongers P, Amick B. The Job Content Questionnaire (JCQ): an instrument for internationally comparative assessments of psychosocial job characteristics. J Occup Health Psychol. 1998;3(4):322-355. doi:10.1037/1076-8998.3.4.322
42. Csikszentmihalyi M, Larson R. Validity and reliability of the Experience-Sampling Method. J Nerv Ment Dis. 1987;175(9):526-536. doi:10.1097/00005053-198709000-00004
43. Grebner S, Elfering A, Semmer NK, Kaiser-Probst C, Schlapbach M-L. Stressful Situations at Work and in Private Life among Young Workers: An Event Sampling Approach. Social Indicators Research. 2004;67(1):11-49. doi:10.1023/B:SOCI.0000007333.96382.3a
44. Elfering A, Grebner S, K. Semmer N, Kaiser-Freiburghaus D, Lauper-Del Ponte S, Witschi I. Chronic job stressors and job control: Effects on event-related coping success and well-being. Journal of Occupational and Organizational Psychology. 2005;78(2):237-252. doi:10.1348/096317905x40088
General Introduction
24
45. Corradini I, Marano A, Nardelli E. Work-Related Stress Risk Assessment: A Methodological Analysis Based on Psychometric Principles of an Objective Tool. SAGE Open. 2016;6(3):1-9. doi:10.1177/2158244016666888
46. Foster P. Observational Research. In: Sapsford R, Jupp V, editors. Data Collection and Analysis. London: SAGE, 2006.
47. Monahan T, Fisher JA. Benefits of "Observer Effects": Lessons from the Field. Qualitative Research. 2010;10(3):357-376. doi:10.1177/1468794110362874
48. Sonnentag S, Fritz C. Endocrinological Processes Associated With Job Stress: Catecholamine and Cortisol Responses to Acute and Chronic Stressors. In: Pamela LP, Daniel CG, editors. Employee Health, Coping and Methodologies: Emerald Group Publishing Limited, 2006. p. 1-59.
49. Hjortskov N, Garde AH, Ørbæk P, Hansen ÅM. Evaluation of salivary cortisol as a biomarker of self-reported mental stress in field studies. Stress and Health. 2004;20(2):91-98. doi:10.1002/smi.1000
50. Ruotsalainen JH, Verbeek JH, Marine A, Serra C. Preventing occupational stress in healthcare workers. Cochrane Database od Systematic Reviews. 2014(11):Cd002892. doi:10.1002/14651858.CD002892.pub3
51. Dhaini SR, Zuniga F, Ausserhofer D, Simon M, Kunz R, De Geest S, et al. Care workers health in Swiss nursing homes and its association with psychosocial work environment: A cross-sectional study. International Journal of Nursing Studies. 2016;53:105-115. doi:10.1016/j.ijnurstu.2015.08.011
52. Sermeus W, Aiken LH, Van den Heede K, Rafferty AM, Griffiths P, Moreno-Casbas MT, et al. Nurse forecasting in Europe (RN4CAST): Rationale, design and methodology. BMC Nursing. 2011;10(6):6. doi:10.1186/1472-6955-10-6
53. Dhaini SR, Denhaerynck K, Bachnick S, Schwendimann R, Schubert M, De Geest S, et al. Work schedule flexibility is associated with emotional exhaustion among registered nurses in Swiss hospitals: A cross-sectional study. International Journal of Nursing Studies. 2018;82:99-105. doi:10.1016/j.ijnurstu.2018.03.019
54. Lambert VA, Lambert CE. Literature review of role stress/strain on nurses: An international perspective. Nursing & health sciences. 2001;3(3):161-172. doi:10.1046/j.1442-2018.2001.00086.x
Chapter 2
Work-related stress among health professionals in Swiss acute care and rehabilitation hospitals – a cross-sectional study
Peter KA, Hahn S, Schols JMGA, Halfens RJG. Work-related stress among health professionals in Swiss acute care and rehabilitation hospitals-A cross-sectional study. Journal of clinical nursing. 2020;29(15-16):3064-3081. doi:10.1111/jocn.15340
Chapter 2
26
Abstract
Aims and objectives: This study aimed to identify significant work stressors associated with stress symptoms, job satisfaction, intention to leave and health-related outcomes among health professionals. Background: The workforce shortage of health professionals is a current concern and a reduction of work-related stress is thus essential for retaining health professionals. Studies on the extent of work-related stress in different health professions are limited. Methods: The research was conducted with a cross-sectional study encompassing 26 randomly selected acute care and rehabilitation hospitals. The sample consisted of 3398 health professionals. The study was undertaken in accordance with the STROBE checklist for observational studies. Results: Work-private life conflicts were significantly associated with health professionals’ stress symptoms, job satisfaction, intention to leave the organisation and profession, their general health status, burnout symptoms and quality of sleep. Also, opportunities for development, the behaviour of the direct line manager (e.g. quality of leadership, unfair behaviour, rewards given) along with various profession-specific stressors were the important predictors revealed. Conclusions: This study shows the high relevance of preventing and reducing work-private life conflicts, enhancing leadership qualities as well as opportunities for development among health professionals working in acute care and rehabilitation hospitals. Also, differences between health professions should be taken into consideration in developing strategies for reducing stress at work. Relevance to clinical practice: The results of this study are particularly relevant for health professional leaders and reveal the urgent need in hospital practice for effective strategies to improve health professionals’ work-private life balance, opportunities for development and quality of leadership.

Chapter 2
27
Summary statement
What does this paper contribute to the wider global clinical community? • Existing work-private life conflicts, lacking opportunities for development
and the behaviour of the direct line manager were identified as relevant stressors at work and were associated with health professionals’ stress symptoms, job satisfaction as well as health and motivation to remain at work.
• Health professional leaders play an important role in reducing work-related stress among their employees, and our study results indicate where interventions to improve working conditions in acute and rehabilitation hospitals are needed.
• The paper also reveals the extent of work-related stress in different health professions and how essential it is to develop individual strategies separately shaped to the specific working conditions of each health profession.
Chapter 2
28
1. Introduction
The shortage of health professionals is becoming increasingly acute, and in several countries healthcare systems are struggling with recruiting a qualified health workforce.1, 2 Work-related stress, poor working conditions and reward frustration among the health professions play an important role and are associated with health professionals’ intention to leave their career prematurely.3-
5 Work-related stress is defined as ‘a pattern of reactions that occurs when
workers are presented with demands or pressures (stressors) that are not matched to their knowledge, abilities and skills and which challenge their ability to cope’.6, 7 Stress among health professionals can be caused by high emotional, mental and physical demands at work, along with time pressures, understaffing and experiences of work-related aggression.3, 8, 9 Other study results indicate that high workload, work-private life conflicts, a lack of work schedule flexibility, long working hours and shift work can lead to a higher rate of emotional exhaustion and burnout among health professionals.10-12 However, the study of Gilles, Burnand13 indicates that the relevance of these stressors for health professionals’ burnout-symptoms, intention to leave and job satisfaction can differ between the various health care professions, since there was for example a stronger association between workload and burnout among physicians, nurses and laboratory staff compared to other health professionals.
2. Background
Health professionals’ perceived stress at work can not only increase their intention to leave their job, but also negatively affect their mental and physical health, job satisfaction and safety at work.14-16 Health professionals are especially affected by severe burnout-symptoms, musculoskeletal disorders and carry a higher risk for adverse cardiovascular health than do workers in other areas or labour segments.17-19 Furthermore, high levels of stress and understaffing at work also show negative associations with patient safety and quality of care.9, 15
Reducing salient stressors at work and improving working conditions is thus essential for retaining health professionals3, 9. Therefore, determining the most salient stressors in the work environment is key to developing appropriate prevention strategies.20 Although some recent studies have been undertaken for Swiss nurses10, there is still a lack of clarity on the situation for various health professionals in Switzerland.
Chapter 2
29
Therefore, the aim of this study was to identify relevant work stressors in Swiss hospitals, and to identify their relation to stress reactions and long-term consequences separately among nursing staff and midwives, physicians, medical-technical and medical-therapeutic professionals.
3. Methods
3.1 Design This study utilized a cross-sectional design, and is part of the national STRAIN study, ‘work-related STRess Among health professionals IN Switzerland’. The national STRAIN study is a cluster randomised controlled trial (Clinical Trials registration: NCT03508596) that is based on three data measures (T0, T1, T2) and aims to reduce the level of work-related stress among different health professional disciplines with a 2-day intervention program for leaders between T1 and T2. The data presented in this study is based on the STRAIN base rate measure T0 and was collected from September 2017 until the end of March 2018 in Swiss acute care and rehabilitation hospitals. The study adhered to the STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) checklist (see Appendix 1).
3.2 Recruitment This study was conducted in the Swiss healthcare system, which is highly complex and includes aspects of managed competition as well as influences of direct democracy. The 293 Swiss hospitals can vary in size from 2-3 beds to more than 2000 beds, which may seem rather small size compared to other countries, and include acute care, rehabilitation and psychiatric hospitals.21
For this study, both acute care and rehabilitation hospitals were included, since many of the Swiss acute care hospitals have integrated their rehabilitation wards internally. Hospitals that were too small (average number of beds < 20, and/or fewer than 7 employees) or specialised (e.g. only gynaecology or neonatology) were excluded. Acute care and rehabilitation hospitals were randomly selected from a list of all registered hospitals obtained from the Swiss Federal Statistical Office in 2016. To ensure a sufficiently large sample, a total of 70 acute and rehabilitation hospitals were randomly selected (using randomizer.org) and invited to participate. Therefore, a flyer containing information about the study was sent directly to the CEO or head of Human Resources of these organisations. In the end, 26 hospitals (acute care and rehabilitation) took part in the study.
Chapter 2
30
3.3 Sample and data collection Data collection began with a contact person in each organisation distributing the questionnaires via email or printed-paper version to all nursing staff, midwives, physicians, medical-technical and medical-therapeutic professionals, at all skill levels. A short film and a written study flyer were used to inform employees about the study. The participants had one month to complete the questionnaire and received a standardized reminder after two weeks. The questionnaire for employees was available in all Swiss languages (German, French and Italian) online (via either umfrageonline® or surveymonkey®) and in a printed-paper version.
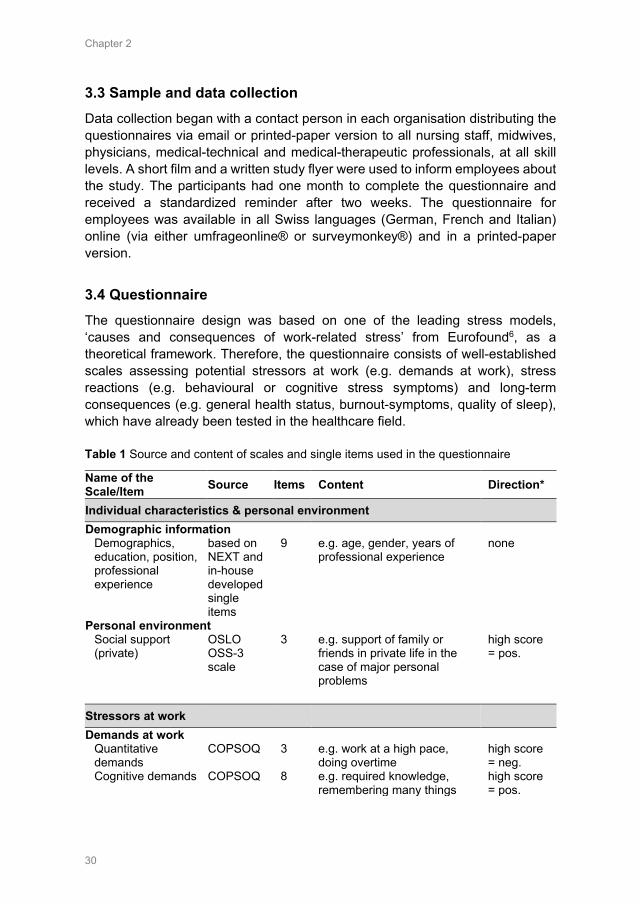
3.4 Questionnaire The questionnaire design was based on one of the leading stress models, ‘causes and consequences of work-related stress’ from Eurofound6, as a theoretical framework. Therefore, the questionnaire consists of well-established scales assessing potential stressors at work (e.g. demands at work), stress reactions (e.g. behavioural or cognitive stress symptoms) and long-term consequences (e.g. general health status, burnout-symptoms, quality of sleep), which have already been tested in the healthcare field. Table 1 Source and content of scales and single items used in the questionnaire
Name of the Scale/Item Source Items Content Direction*
Individual characteristics & personal environment Demographic information
Demographics, education, position, professional experience
based on NEXT and in-house developed single items
9 e.g. age, gender, years of professional experience
none
Personal environment Social support (private)
OSLO OSS-3 scale
3 e.g. support of family or friends in private life in the case of major personal problems
high score = pos.
Stressors at work Demands at work
Quantitative demands
COPSOQ 3 e.g. work at a high pace, doing overtime
high score = neg.
Cognitive demands COPSOQ 8 e.g. required knowledge, remembering many things
high score = pos.
Chapter 2
31
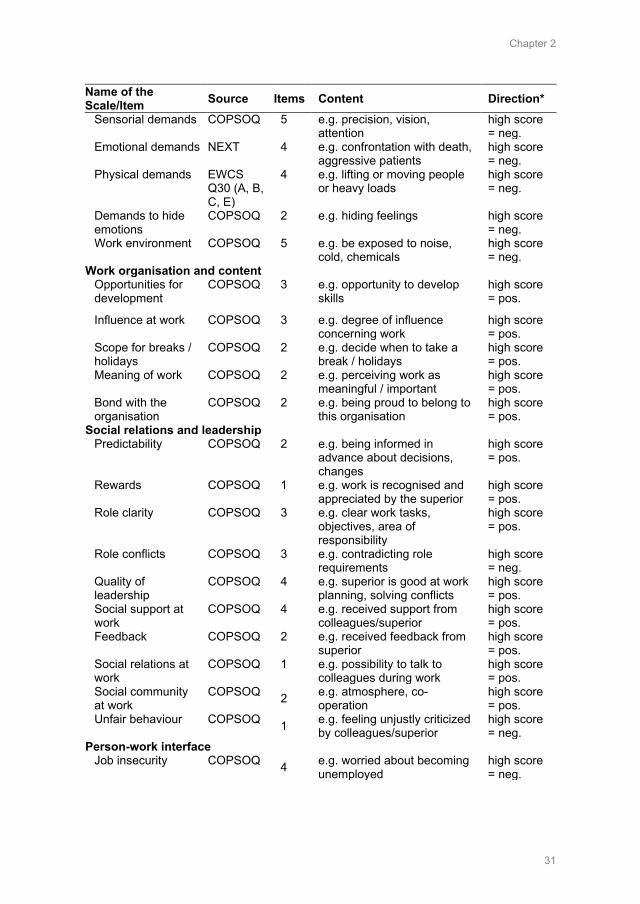
Name of the Scale/Item Source Items Content Direction*
Sensorial demands COPSOQ 5 e.g. precision, vision, attention
high score = neg.
Emotional demands NEXT 4 e.g. confrontation with death, aggressive patients
high score = neg.
Physical demands EWCS Q30 (A, B, C, E)
4 e.g. lifting or moving people or heavy loads
high score = neg.
Demands to hide emotions
COPSOQ 2 e.g. hiding feelings high score = neg.
Work environment COPSOQ 5 e.g. be exposed to noise, cold, chemicals
high score = neg.
Work organisation and content Opportunities for development
COPSOQ 3 e.g. opportunity to develop skills
high score = pos.
Influence at work COPSOQ 3 e.g. degree of influence concerning work
high score = pos.
Scope for breaks / holidays
COPSOQ 2 e.g. decide when to take a break / holidays
high score = pos.
Meaning of work COPSOQ 2 e.g. perceiving work as meaningful / important
high score = pos.
Bond with the organisation
COPSOQ 2 e.g. being proud to belong to this organisation
high score = pos.
Social relations and leadership Predictability COPSOQ 2 e.g. being informed in
advance about decisions, changes
high score = pos.
Rewards COPSOQ 1 e.g. work is recognised and appreciated by the superior
high score = pos.
Role clarity COPSOQ 3 e.g. clear work tasks, objectives, area of responsibility
high score = pos.
Role conflicts COPSOQ 3 e.g. contradicting role requirements
high score = neg.
Quality of leadership
COPSOQ 4 e.g. superior is good at work planning, solving conflicts
high score = pos.
Social support at work
COPSOQ 4 e.g. received support from colleagues/superior
high score = pos.
Feedback COPSOQ 2 e.g. received feedback from superior
high score = pos.
Social relations at work
COPSOQ 1 e.g. possibility to talk to colleagues during work
high score = pos.
Social community at work
COPSOQ 2 e.g. atmosphere, co-operation
high score = pos.
Unfair behaviour COPSOQ 1 e.g. feeling unjustly criticized by colleagues/superior
high score = neg.
Person-work interface Job insecurity COPSOQ 4 e.g. worried about becoming
unemployed high score = neg.
Chapter 2
32
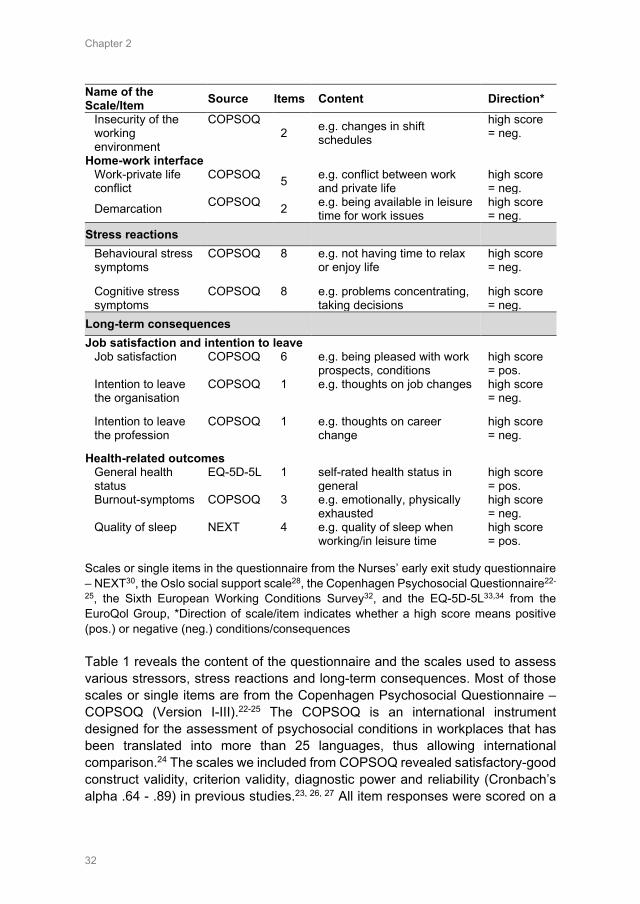
Name of the Scale/Item Source Items Content Direction*
Insecurity of the working environment
COPSOQ 2 e.g. changes in shift
schedules
high score = neg.
Home-work interface Work-private life conflict
COPSOQ 5 e.g. conflict between work and private life
high score = neg.
Demarcation COPSOQ 2 e.g. being available in leisure time for work issues
high score = neg.
Stress reactions Behavioural stress symptoms
COPSOQ 8 e.g. not having time to relax or enjoy life
high score = neg.
Cognitive stress symptoms
COPSOQ 8 e.g. problems concentrating, taking decisions
high score = neg.
Long-term consequences Job satisfaction and intention to leave
Job satisfaction COPSOQ 6 e.g. being pleased with work prospects, conditions
high score = pos.
Intention to leave the organisation
COPSOQ 1 e.g. thoughts on job changes high score = neg.
Intention to leave the profession
COPSOQ 1 e.g. thoughts on career change
high score = neg.
Health-related outcomes General health status
EQ-5D-5L 1 self-rated health status in general
high score = pos.
Burnout-symptoms COPSOQ 3 e.g. emotionally, physically exhausted
high score = neg.
Quality of sleep NEXT 4 e.g. quality of sleep when working/in leisure time
high score = pos.
Scales or single items in the questionnaire from the Nurses’ early exit study questionnaire – NEXT30, the Oslo social support scale28, the Copenhagen Psychosocial Questionnaire22-
25, the Sixth European Working Conditions Survey32, and the EQ-5D-5L33,34 from the EuroQol Group, *Direction of scale/item indicates whether a high score means positive (pos.) or negative (neg.) conditions/consequences Table 1 reveals the content of the questionnaire and the scales used to assess various stressors, stress reactions and long-term consequences. Most of those scales or single items are from the Copenhagen Psychosocial Questionnaire – COPSOQ (Version I-III).22-25 The COPSOQ is an international instrument designed for the assessment of psychosocial conditions in workplaces that has been translated into more than 25 languages, thus allowing international comparison.24 The scales we included from COPSOQ revealed satisfactory-good construct validity, criterion validity, diagnostic power and reliability (Cronbach’s alpha .64 - .89) in previous studies.23, 26, 27 All item responses were scored on a

Chapter 2
33
five-point Likert scale with five options: always, often, sometimes, seldom, never/hardly ever or to a very large extent, to a large extent, somewhat, to a small extent, to a very small extent.
In addition, for assessing social support in private life, the OSLO OSS-3 scale from Sarason, Levine28 was used. Furthermore, the scale on ‘emotional demands’ originally developed from de Jonge, Mulder29, adapted and translated in the Nurses’ Early Exit study (NEXT) of Hasselhorn, Tackenberg30 was used as well as the scale on ‘quality of sleep’, likewise developed and tested in the NEXT study.31 To assess ‘physical demands’, we used the EWCS Q30 items from the Sixth European Working Conditions Survey, developed and tested by Eurofound.32 Furthermore, to assess general health status, the internationally used EQ-5D-5L from the EuroQol Group33, 34 was used. All scales were available in the Swiss languages (German, French, Italian) and showed satisfactory-good validity and reliability (Cronbach’s alpha .64 - .78).
For all scales used in the questionnaire, consent was obtained from the original authors for their use. The questionnaire included a total of 100 questions and took participants on average 35 minutes to complete.
3.5 Ethical considerations The local Swiss ethical board in Bern confirmed that the study does not warrant a full ethical application and does not fall under the Swiss Federal Act on Research Involving Human Beings (Req-2016-00616). The study was on a voluntary basis for all organisations and health professionals participating; all participants were free to stop filling out the questionnaire at any time.
3.6 Data analysis Data were analysed using SPSS 25®. For data analysis, all Items assessing ‘stressors’, ‘stress reactions’ and ‘long-term consequences’ (see Table 1) were transformed and standardised on a value range from 0 to 100 points (0 was the minimum value, 100 the maximum value), considering reverse scored items. Items/scales on ‘individual characteristics & personal environment’ were excluded from this transformation. If less than half of the questions in a scale had been answered, no average score was calculated.22
First, descriptive statistics describing the study sample, as well as for all scales assessing ‘stressors’, ‘stress reactions’ and ‘long-term consequences’ were calculated. To further test for significant differences between the health professional groups ‘nurses & midwives’, ‘physicians’, ‘medical-technical’ and ‘medical-therapeutic professions’, the Kruskal-Wallis H test (significance level of 0.05) and pairwise comparisons (using the Bonferroni correction for multiple tests) was used, since the test of homogeneity of variance was significant and there were no equal-sized samples of data.

Chapter 2
34
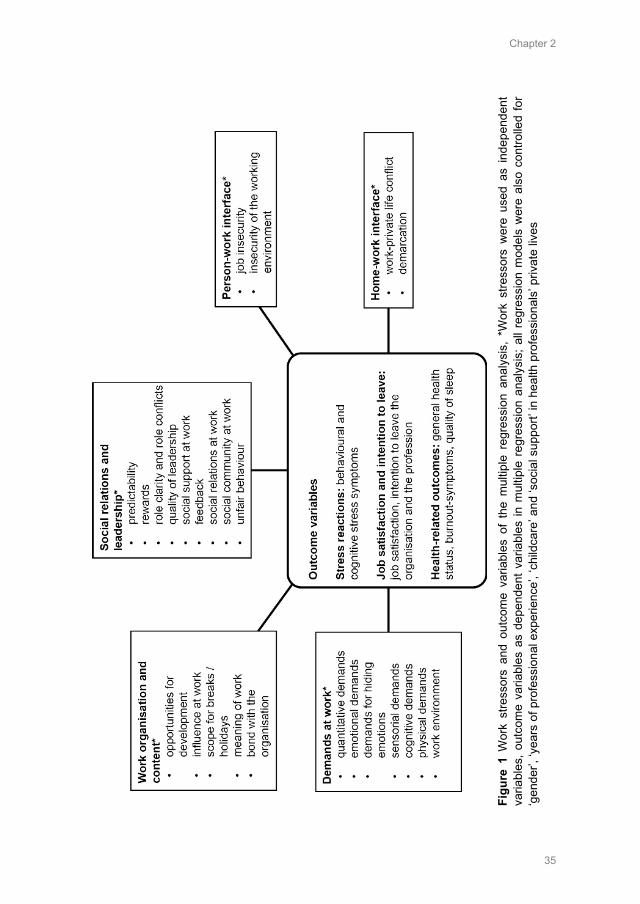
Second, multiple regression models were calculated using the forced entry method, in which all predictors (stressors at work) are entered simultaneously into the model, according to the theoretical framework of Eurofound (2005) and in accordance with thematic fields of COPSOQ.26 According to this theoretical background, scales assessing ‘stressors’ at work were used as independent variables and scales assessing ‘stress reactions’ and ‘long-term consequences’ as used as outcome variables (dependent variables) in the regression analysis (see Figure 1). For each outcome variable (e.g. behavioural stress symptoms) a multiple linear regression model was calculated for nurses and midwives, physicians, medical-technical and medical-therapeutic professionals separately (due to similar working conditions in these groups) and controlled for ‘gender’, ‘years of professional experience’, ‘childcare’ and ‘social support’ in their private lives. No multicollinearity between the estimated regression coefficients was found using the variance inflation factor (VIF) in each regression model. Moreover, beta coefficients to estimate the effect of all predictors and to assess the explained variance (R square) of the outcome variable, as well as t-statistics and p-values (2-tailed), were computed. Since the assumption of homoscedasticity was not met for all regression models, standard errors, p-values and confidence intervals were computed based on bootstrap (r=1000 bootstrap, bias corrected and accelerated, 95% CI).
Chapter 2
35
Figu
re 1
Wor
k st
ress
ors
and
outc
ome
varia
bles
of
the
mul
tiple
reg
ress
ion
anal
ysis
, *W
ork
stre
ssor
s w
ere
used
as
inde
pend
ent
varia
bles
, out
com
e va
riabl
es a
s de
pend
ent v
aria
bles
in m
ultip
le r
egre
ssio
n an
alys
is; a
ll re
gres
sion
mod
els
wer
e al
so c
ontro
lled
for
‘gen
der’,
‘yea
rs o
f pro
fess
iona
l exp
erie
nce’
, ‘ch
ildca
re’ a
nd ‘s
ocia
l sup
port’
in h
ealth
pro
fess
iona
ls’ p
rivat
e liv
es
Chapter 2
36
4. Results
4.1 Study sample In total, 3398 health professionals working in acute care or rehabilitation hospitals took part in the study. Of these, 80% were from the German-speaking and 20% from the French-speaking regions of Switzerland. The response rate of participants was 37%. The study sample consisted of 66% nurses, 2% midwives, 11% physicians, 9% medical-technical professionals and 9% medical-therapeutic professionals. Participants were mostly highly educated (academic level) (79%), female (81%), with a mean age of 40 years. Most participants (67%) were born in Switzerland, another 13% in Germany, 4% in France and 16% in other countries (e.g. Italy, Portugal, Kosovo). Participating health professionals were mostly employed on a permanent basis (81%) and 74% worked 33-42 hours per week. Of those participants who did not work full time (42h/week), 39% stated that they do not want to work more hours due their work-life balance and 35% due to work stress (e.g. physical demands or psychological stress, shift work).
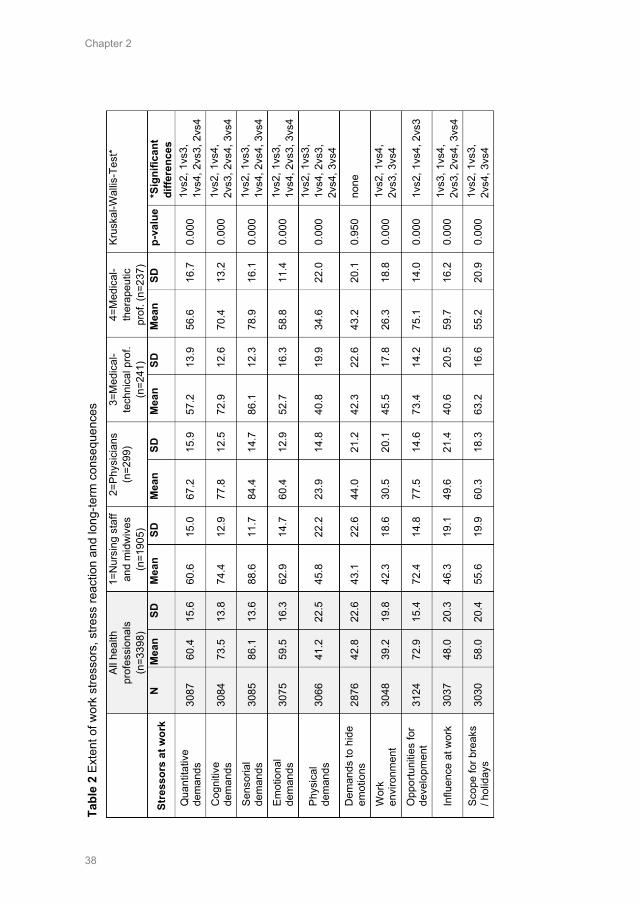
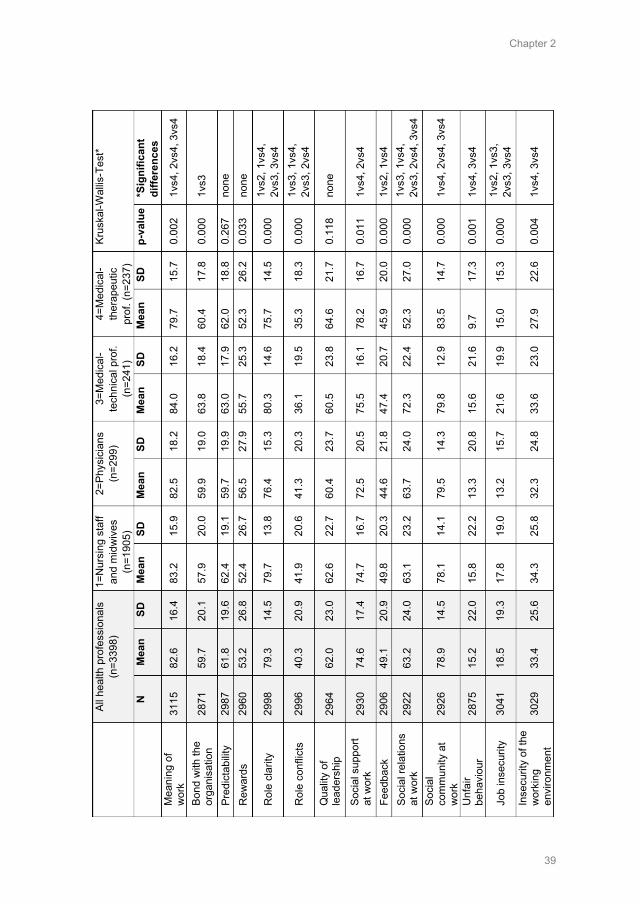
4.2 Results regarding different health professional groups Table 2 presents an overview of stressors at work, stress reaction and long-term consequences for all health professionals (i.e., administration, research personnel included) and separately for nurses and midwives, physicians, medical-technical and medical-therapeutic professionals, using Kruskal-Wallis tests to identify significant differences between these four groups.
Nurses and midwives showed the highest scores on ‘sensorial’ (M=88.6, SD=11.7), ‘emotional’ (M=62.9, SD=14.7) and ‘physical demands’ at work (M=45.8, SD=22.2) compared to the other health professionals. They also showed a more demanding work environment (M=42.3, SD=18.6) than physicians (M=30.5, SD=20.1) and medical-therapeutic professionals (M=26.3, SD=18.8). In addition, nurses and midwives reported fewer ‘opportunities for development’ (M=72.4, SD=14.8), than physicians (M=77.5, SD=14.6) and medical-therapeutic professionals (M=75.1, SD=14.0). Also, they reported a lower ‘scope for breaks and holidays’ (M=55.6, SD=19.9) than physicians (M=60.3, SD=18.3) and medical-technical professionals (M=63.2, SD=16.6). In addition, they had higher scores regarding ‘role conflicts’ (M=41.9, SD=20.6) than medical-technical (M=36.1, SD=19.5) and medical-therapeutic professionals (M=35.3, SD=18.3). Regarding long-term consequences, nurses and midwives revealed to have the lowest scores on ‘job satisfaction’ (M=67.5, SD=14.6) and the highest scores on ‘intention to leave the profession’ (M=18.9, SD=22.4). They also reported poorer ‘quality of sleep’ (M=65.8, SD=18.3) than medical-technical (M=69.0, SD=18.7) and medical-therapeutical professionals (M=70.5, SD=17.8).
Chapter 2
37
Physicians had the highest scores on ‘quantitative demands’ (M=67.2, SD=15.9) compared to other health professionals. In addition, they reported lower ‘role clarity’ (M=76.4, SD=15.3) than nurses and midwives (M=79.7, SD=13.8) and medical-technical professionals (M=80.3, SD=14.6). Also, physicians showed higher scores regarding ‘role conflicts’ (M=41.3, SD=20.3) than did medical-technical (M=36.1, SD=19.5) and medical-therapeutic professionals (M=35.3, SD=18.3). In addition, ‘work-private life conflicts’ (M=50.2, SD=22.2) and difficulties with ‘demarcation’ (M=49.6, SD=25.1) were highest among physicians. Regarding long-term consequences, physicians reported the highest scores regarding ‘behavioural stress symptoms’ (M=30.6, SD=20.7). In addition, they reported poorer ‘quality of sleep’ (M=64.0, SD=19.8) than medical-technical (M=69.0, SD=18.7) and medical-therapeutic professionals (M=70.5, SD=17.8).
Medical-technical professionals experienced a more ‘demanding work environment’ (M=45.5, SD=17.8) than physicians (M=30.5, SD=20.1) and medical-therapeutic professionals (M=26.3, SD=18.8). Also, they reported having fewer opportunities for development (M=73.4, SD=14.2) than physicians (M=77.5, SD=14.6). Overall, they tended to have the lowest ‘influence at work’ (M=40.6, SD=20.5) and highest ‘job insecurity’ (M=21.6, SD=19.9).
Medical-therapeutic professionals reported the lowest scores on ‘cognitive demands’ at work (M=70.4, SD=13.2) and experienced a lower ‘scope for breaks and holidays’ (M=55.2, SD=20.9) than did physicians (M=60.3, SD=18.3) and medical-technical professionals (M=63.2, SD=16.6). In addition, their ‘meaning of work’ (M=79.7, SD=15.7) and ‘social relations’ at work ratings (M=52.3, SD=27.0) were lowest compared to other health professionals. Also, they reported lower ‘role clarity’ (M=75.7 SD=14.5) than nurses and midwives (M=79.7, SD=13.8) and medical-technical professionals (M=80.3, SD=14.6).
Chapter 2
38
Al
l hea
lth
prof
essi
onal
s (n
=339
8)
1=N
ursi
ng s
taff
and
mid
wiv
es
(n=1
905)
2=Ph
ysic
ians
(n
=299
) 3=
Med
ical
-te
chni
cal p
rof.
(n=2
41)
4=M
edic
al-
ther
apeu
tic
prof
. (n=
237)
Krus
kal-W
allis
-Tes
t*
Stre
ssor
s at
wor
k N
M
ean
SD
Mea
n
SD
Mea
n SD
M
ean
SD
Mea
n SD
p-
valu
e *S
igni
fican
t di
ffere
nces
Q
uant
itativ
e de
man
ds
3087
60
.4
15.6
60
.6
15.0
67
.2
15.9
57
.2
13.9
56
.6
16.7
0.
000
1vs2
, 1vs
3,
1vs4
, 2vs
3, 2
vs4
Cog
nitiv
e de
man
ds
3084
73
.5
13.8
74
.4
12.9
77
.8
12.5
72
.9
12.6
70
.4
13.2
0.
000
1vs2
, 1vs
4,
2vs3
, 2vs
4, 3
vs4
Sens
oria
l de
man
ds
3085
86
.1
13.6
88
.6
11.7
84
.4
14.7
86
.1
12.3
78
.9
16.1
0.
000
1vs2
, 1vs
3,
1vs4
, 2vs
4, 3
vs4
Emot
iona
l de
man
ds
3075
59
.5
16.3
62
.9
14.7
60
.4
12.9
52
.7
16.3
58
.8
11.4
0.
000
1vs2
, 1vs
3,
1vs4
, 2vs
3, 3
vs4
Phys
ical
de
man
ds
3066
41
.2
22.5
45
.8
22.2
23
.9
14.8
40
.8
19.9
34
.6
22.0
0.
000
1vs2
, 1vs
3,
1vs4
, 2vs
3,
2vs4
, 3vs
4 D
eman
ds to
hid
e em
otio
ns
2876
42
.8
22.6
43
.1
22.6
44
.0
21.2
42
.3
22.6
43
.2
20.1
0.
950
none
Wor
k en
viro
nmen
t 30
48
39.2
19
.8
42.3
18
.6
30.5
20
.1
45.5
17
.8
26.3
18
.8
0.00
0 1v
s2, 1
vs4,
2v
s3, 3
vs4
Opp
ortu
nitie
s fo
r de
velo
pmen
t 31
24
72.9
15
.4
72.4
14
.8
77.5
14
.6
73.4
14
.2
75.1
14
.0
0.00
0 1v
s2, 1
vs4,
2vs
3
Influ
ence
at w
ork
3037
48
.0
20.3
46
.3
19.1
49
.6
21.4
40
.6
20.5
59
.7
16.2
0.
000
1vs3
, 1vs
4,
2vs3
, 2vs
4, 3
vs4
Scop
e fo
r bre
aks
/ hol
iday
s 30
30
58.0
20
.4
55.6
19
.9
60.3
18
.3
63.2
16
.6
55.2
20
.9
0.00
0 1v
s2, 1
vs3,
2v
s4, 3
vs4
Tabl
e 2
Exte
nt o
f wor
k st
ress
ors,
stre
ss re
actio
n an
d lo
ng-te
rm c
onse
quen
ces
Chapter 2
39
Al
l hea
lth p
rofe
ssio
nals
(n
=339
8)
1=N
ursi
ng s
taff
and
mid
wiv
es
(n=1
905)
2=Ph
ysic
ians
(n
=299
) 3=
Med
ical
-te
chni
cal p
rof.
(n=2
41)
4=M
edic
al-
ther
apeu
tic
prof
. (n=
237)
Krus
kal-W
allis
-Tes
t*
N
M
ean
SD
Mea
n
SD
Mea
n SD
M
ean
SD
Mea
n SD
p-
valu
e *S
igni
fican
t di
ffere
nces
M
eani
ng o
f w
ork
3115
82
.6
16.4
83
.2
15.9
82
.5
18.2
84
.0
16.2
79
.7
15.7
0.
002
1vs4
, 2vs
4, 3
vs4
Bond
with
the
orga
nisa
tion
2871
59
.7
20.1
57
.9
20.0
59
.9
19.0
63
.8
18.4
60
.4
17.8
0.
000
1vs3
Pred
icta
bilit
y
2987
61
.8
19.6
62
.4
19.1
59
.7
19.9
63
.0
17.9
62
.0
18.8
0.
267
none
Rew
ards
29
60
53.2
26
.8
52.4
26
.7
56.5
27
.9
55.7
25
.3
52.3
26
.2
0.03
3 no
ne
Rol
e cl
arity
29
98
79.3
14
.5
79.7
13
.8
76.4
15
.3
80.3
14
.6
75.7
14
.5
0.00
0 1v
s2, 1
vs4,
2v
s3, 3
vs4
Rol
e co
nflic
ts
2996
40
.3
20.9
41
.9
20.6
41
.3
20.3
36
.1
19.5
35
.3
18.3
0.
000
1vs3
, 1vs
4,
2vs3
, 2vs
4
Qua
lity
of
lead
ersh
ip
2964
62
.0
23.0
62
.6
22.7
60
.4
23.7
60
.5
23.8
64
.6
21.7
0.
118
none
Soci
al s
uppo
rt at
wor
k 29
30
74.6
17
.4
74.7
16
.7
72.5
20
.5
75.5
16
.1
78.2
16
.7
0.01
1 1v
s4, 2
vs4
Feed
back
29
06
49.1
20
.9
49.8
20
.3
44.6
21
.8
47.4
20
.7
45.9
20
.0
0.00
0 1v
s2, 1
vs4
Soci
al re
latio
ns
at w
ork
2922
63
.2
24.0
63
.1
23.2
63
.7
24.0
72
.3
22.4
52
.3
27.0
0.
000
1vs3
, 1vs
4,
2vs3
, 2vs
4, 3
vs4
Soci
al
com
mun
ity a
t w
ork
2926
78
.9
14.5
78
.1
14.1
79
.5
14.3
79
.8
12.9
83
.5
14.7
0.
000
1vs4
, 2vs
4, 3
vs4
Unf
air
beha
viou
r 28
75
15.2
22
.0
15.8
22
.2
13.3
20
.8
15.6
21
.6
9.7
17.3
0.
001
1vs4
, 3vs
4
Job
inse
curit
y 30
41
18.5
19
.3
17.8
19
.0
13.2
15
.7
21.6
19
.9
15.0
15
.3
0.00
0 1v
s2, 1
vs3,
2v
s3, 3
vs4
Inse
curit
y of
the
wor
king
en
viro
nmen
t 30
29
33.4
25
.6
34.3
25
.8
32.3
24
.8
33.6
23
.0
27.9
22
.6
0.00
4 1v
s4, 3
vs4
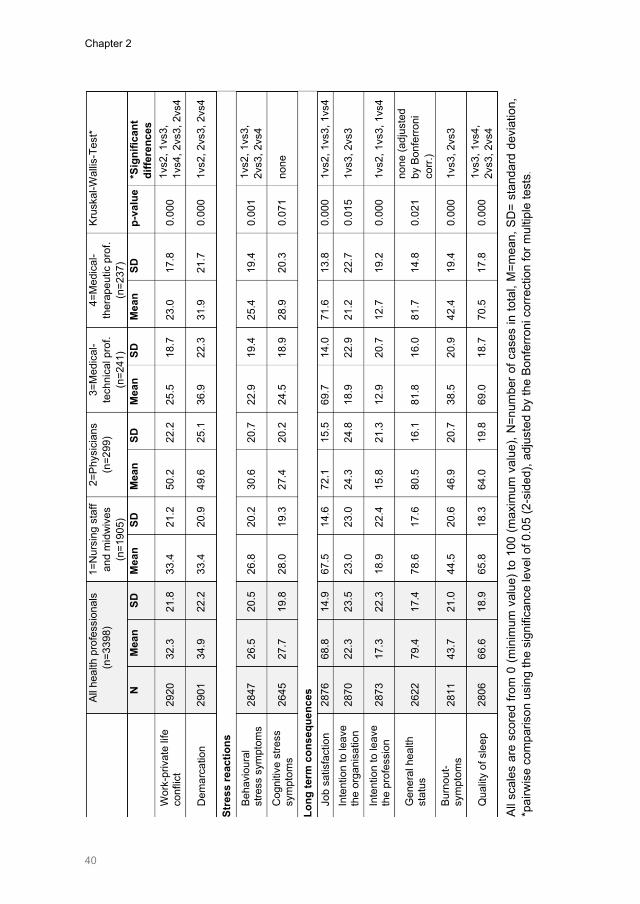
Chapter 2
40
Al
l hea
lth p
rofe
ssio
nals
(n
=339
8)
1=N
ursi
ng s
taff
and
mid
wiv
es
(n=1
905)
2=Ph
ysic
ians
(n
=299
) 3=
Med
ical
-te
chni
cal p
rof.
(n=2
41)
4=M
edic
al-
ther
apeu
tic p
rof.
(n=2
37)
Krus
kal-W
allis
-Tes
t*
N
M
ean
SD
Mea
n
SD
Mea
n SD
M
ean
SD
Mea
n SD
p-
valu
e *S
igni
fican
t di
ffere
nces
W
ork-
priv
ate
life
conf
lict
2920
32
.3
21.8
33
.4
21.2
50
.2
22.2
25
.5
18.7
23
.0
17.8
0.
000
1vs2
, 1vs
3,
1vs4
, 2vs
3, 2
vs4
Dem
arca
tion
2901
34
.9
22.2
33
.4
20.9
49
.6
25.1
36
.9
22.3
31
.9
21.7
0.
000
1vs2
, 2vs
3, 2
vs4
Stre
ss re
actio
ns
Beha
viou
ral
stre
ss s
ympt
oms
2847
26
.5
20.5
26
.8
20.2
30
.6
20.7
22
.9
19.4
25
.4
19.4
0.
001
1vs2
, 1vs
3,
2vs3
, 2vs
4
Cog
nitiv
e st
ress
sy
mpt
oms
26
45
27.7
19
.8
28.0
19
.3
27.4
20
.2
24.5
18
.9
28.9
20
.3
0.07
1 no
ne
Long
term
con
sequ
ence
s Jo
b sa
tisfa
ctio
n 28
76
68.8
14
.9
67.5
14
.6
72.1
15
.5
69.7
14
.0
71.6
13
.8
0.00
0 1v
s2, 1
vs3,
1vs
4 In
tent
ion
to le
ave
the
orga
nisa
tion
28
70
22.3
23
.5
23.0
23
.0
24.3
24
.8
18.9
22
.9
21.2
22
.7
0.01
5 1v
s3, 2
vs3
Inte
ntio
n to
leav
e th
e pr
ofes
sion
28
73
17.3
22
.3
18.9
22
.4
15.8
21
.3
12.9
20
.7
12.7
19
.2
0.00
0 1v
s2, 1
vs3,
1vs
4
Gen
eral
hea
lth
stat
us
2622
79
.4
17.4
78
.6
17.6
80
.5
16.1
81
.8
16.0
81
.7
14.8
0.
021
none
(adj
uste
d by
Bon
ferro
ni
corr.
) Bu
rnou
t-sy
mpt
oms
2811
43
.7
21.0
44
.5
20.6
46
.9
20.7
38
.5
20.9
42
.4
19.4
0.
000
1vs3
, 2vs
3
Qua
lity
of s
leep
28
06
66.6
18
.9
65.8
18
.3
64.0
19
.8
69.0
18
.7
70.5
17
.8
0.00
0 1v
s3, 1
vs4,
2v
s3, 2
vs4
All s
cale
s ar
e sc
ored
from
0 (m
inim
um v
alue
) to
100
(max
imum
val
ue),
N=n
umbe
r of c
ases
in to
tal,
M=m
ean,
SD
= st
anda
rd d
evia
tion,
*p
airw
ise
com
paris
on u
sing
the
sign
ifica
nce
leve
l of 0
.05
(2-s
ided
), ad
just
ed b
y th
e Bo
nfer
roni
cor
rect
ion
for m
ultip
le te
sts.

Chapter 2
41
4.3 Results of multiple regression analysis The results of the multiple regression analysis provide further insights into which stressors are related to which stress reactions and long-term consequences.
4.3.1 Stress reactions Results of the multiple regression models using bootstrap (Table 3) indicate that severe ‘work-private life conflicts’ were associated with higher ‘behavioural stress symptoms’ among all health professionals (nurses & midwives: β=0.36, p<0.001, physicians: β=0.46, p<0.001, medical-technical professionals: β=0.41, p<0.001, medical-therapeutic professionals: β=0.54, p<0.001). Higher ‘demands to hide emotions’ also proved to be related to higher ‘behavioural stress symptoms’ (nurses and midwives: β=0.11, p<0.001, physicians: β=0.18, p<0.01, medical-technical professionals: β=0.13, p<0.05). A more frequent experience of ‘unfair behaviour’ by colleagues or the superior was also associated with higher ‘behavioural stress symptoms’ among nurses and midwives (β=0.06, p<0.01) and medical-technical professionals (β=0.17, p<0.01).
Results on ‘cognitive stress symptoms’ also revealed severe ‘work-private life conflicts’ as a significant predictor equally for all health professionals (nurses & midwives: β=0.28, p<0.001, physicians: β=0.31, p<0.001, medical-technical professionals: β=0.30, p<0.01, medical-therapeutic professionals: β=0.34, p<0.001). Also, a relevant stressor associated with higher ‘cognitive stress symptoms’ was lower ‘role clarity’ (nurses & midwives: β=-0.14, p<0.001, medical-therapeutic professionals β=-0.32, p<0.01). More profession-specific predictors of behavioural and cognitive stress symptoms are shown in Table 3.
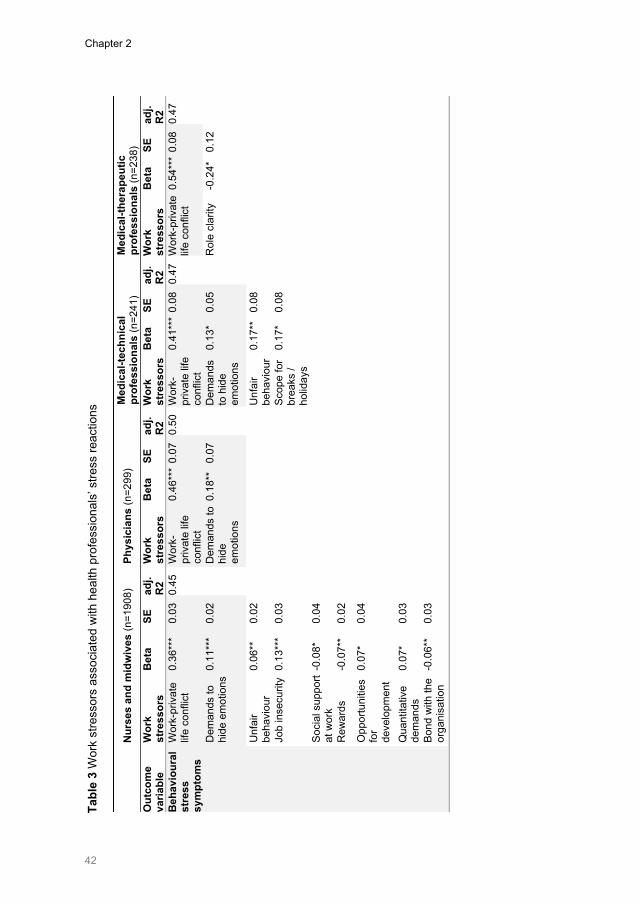
Chapter 2
42
N
urse
s an
d m
idw
ives
(n=1
908)
Ph
ysic
ians
(n=2
99)
Med
ical
-tech
nica
l pr
ofes
sion
als
(n=2
41)
Med
ical
-ther
apeu
tic
prof
essi
onal
s (n
=238
) O
utco
me
varia
ble
Wor
k st
ress
ors
Bet
a SE
ad
j. R
2 W
ork
stre
ssor
s B
eta
SE
adj.
R2
Wor
k st
ress
ors
Bet
a SE
ad
j. R
2 W
ork
stre
ssor
s B
eta
SE
adj.
R2
Beh
avio
ural
st
ress
sy
mpt
oms
Wor
k-pr
ivat
e lif
e co
nflic
t 0.
36**
* 0.
03
0.45
W
ork-
priv
ate
life
conf
lict
0.46
***
0.07
0.
50
Wor
k-pr
ivat
e lif
e co
nflic
t
0.41
***
0.08
0.
47
Wor
k-pr
ivat
e lif
e co
nflic
t 0.
54**
* 0.
08
0.47
Dem
ands
to
hide
em
otio
ns 0.
11**
* 0.
02
D
eman
ds to
hi
de
emot
ions
0.18
**
0.07
Dem
ands
to
hid
e em
otio
ns
0.13
* 0.
05
R
ole
clar
ity
-0.2
4*
0.12
Unf
air
beha
viou
r 0.
06**
0.
02
U
nfai
r be
havi
our
0.17
**
0.08
Job
inse
curit
y 0.
13**
* 0.
03
Sc
ope
for
brea
ks /
holid
ays
0.17
* 0.
08
Soci
al s
uppo
rt at
wor
k -0
.08*
0.
04
Rew
ards
-0
.07*
* 0.
02
Opp
ortu
nitie
s fo
r de
velo
pmen
t
0.07
* 0.
04
Qua
ntita
tive
dem
ands
0.
07*
0.03
Bond
with
the
orga
nisa
tion
-0.0
6**
0.03
Tabl
e 3
Wor
k st
ress
ors
asso
ciat
ed w
ith h
ealth
pro
fess
iona
ls’ s
tress
reac
tions
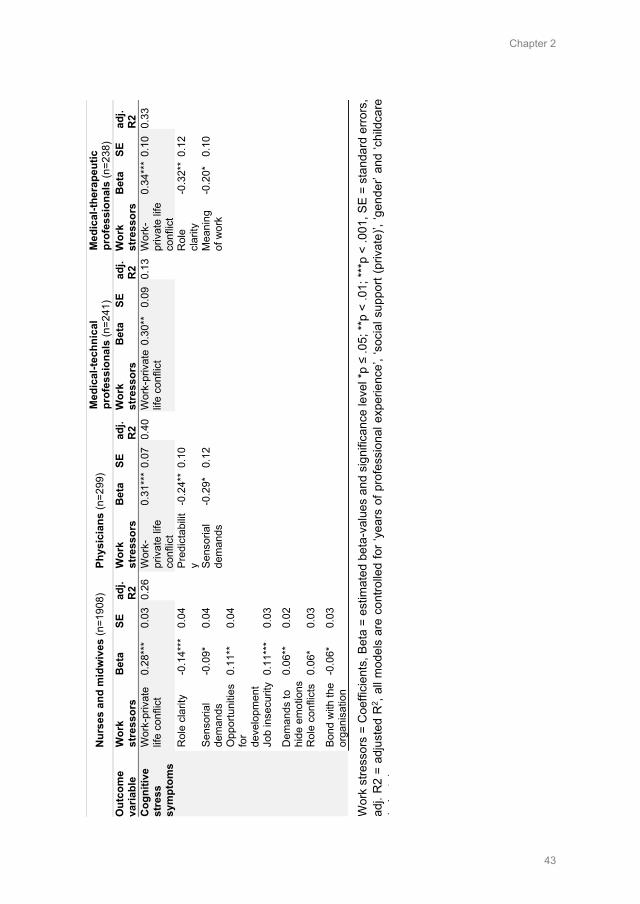
Chapter 2
43
N
urse
s an
d m
idw
ives
(n=1
908)
Ph
ysic
ians
(n=2
99)
Med
ical
-tech
nica
l pr
ofes
sion
als
(n=2
41)
Med
ical
-ther
apeu
tic
prof
essi
onal
s (n
=238
) O
utco
me
varia
ble
Wor
k st
ress
ors
Bet
a SE
ad
j. R
2 W
ork
stre
ssor
s B
eta
SE
adj.
R2
Wor
k st
ress
ors
Bet
a SE
ad
j. R
2 W
ork
stre
ssor
s B
eta
SE
adj.
R2
Cog
nitiv
e st
ress
sy
mpt
oms
Wor
k-pr
ivat
e lif
e co
nflic
t 0.
28**
* 0.
03
0.26
W
ork-
priv
ate
life
conf
lict
0.31
***
0.07
0.
40
Wor
k-pr
ivat
e lif
e co
nflic
t 0.
30**
0.
09
0.13
W
ork-
priv
ate
life
conf
lict
0.34
***
0.10
0.
33
Rol
e cl
arity
-0
.14*
**
0.04
Pred
icta
bilit
y -0
.24*
* 0.
10
R
ole
clar
ity
-0.3
2**
0.12
Sens
oria
l de
man
ds
-0.0
9*
0.04
Sens
oria
l de
man
ds
-0.2
9*
0.12
Mea
ning
of
wor
k -0
.20*
0.
10
Opp
ortu
nitie
s fo
r de
velo
pmen
t
0.11
**
0.04
Job
inse
curit
y 0.
11**
* 0.
03
Dem
ands
to
hide
em
otio
ns 0.
06**
0.
02
Rol
e co
nflic
ts
0.06
* 0.
03
Bond
with
the
orga
nisa
tion
-0.0
6*
0.03
Wor
k st
ress
ors
= C
oeffi
cien
ts, B
eta
= es
timat
ed b
eta-
valu
es a
nd s
igni
fican
ce le
vel *
p ≤
.05;
**p
< .0
1; **
*p <
.001
, SE
= st
anda
rd e
rrors
, ad
j. R
2 =
adju
sted
R2 ,
all m
odel
s ar
e co
ntro
lled
for ‘
year
s of
pro
fess
iona
l exp
erie
nce’
, ‘so
cial
sup
port
(priv
ate)
’, ‘g
ende
r’ an
d ‘c
hild
care
(
it
)

Chapter 2
44
4.3.2 Job satisfaction Results of multiple regression models for ‘job satisfaction’ (Table 4) revealed several similar predictors among all health professionals. A stronger bond with the organisation was associated with higher ‘job satisfaction’ among nurses and midwives (β=0.12, p<0.001), physicians (β=0.13, p<0.01), medical-technical professionals (β=0.17, p<0.001) and medical-therapeutic professionals (β=0.11, p<0.01). Also, a better ‘social community at work’ was associated with a higher ‘job satisfaction’ among all health professionals (nurses & midwives: β=0.16, p<0.001, physicians: β=0.18, p<0.01, medical-technical professionals: β=0.14, p<0.05, medical-therapeutic professionals: β=0.20, p<0.001). In addition, severe ‘work-private life conflicts’ were associated with a decrease in health professionals’ ‘job satisfaction’ (nurses & midwives: β=-0.07, p<0.001, physicians: β=-0.09, p<0.05, medical-technical professionals: β=-0.09, p<0.05, medical-therapeutic professionals: β=-0.09, p<0.05). Furthermore, if health professionals perceived the ‘leadership qualities’ of their direct line manager as better, they tended to have higher ‘job satisfaction’ (nurses & midwives: β=0.17, p<0.001, medical-technical: β=0.20, p<0.001, medical-therapeutic professionals: β=0.08, p<0.05). In addition, more ‘opportunities for development’ at work (nurse & midwives β=0.13, p<0.001, physicians: β=0.24, p<0.001) was also associated with higher ‘job satisfaction’, while a lack of ‘rewards’ from their direct line manager was significantly related to a lower ‘job satisfaction’ among nurses’ and midwives’ (β=0.03, p<0.01) and physicians’ (β=0.09, p<0.01). However, more ‘role conflicts’ due to contradictory role requirements at work among nurses and midwives (β=-0.05, p<0.001) and medical-therapeutic professionals (β=-0.09, p<0.05) was also related to lower ‘job satisfaction’.
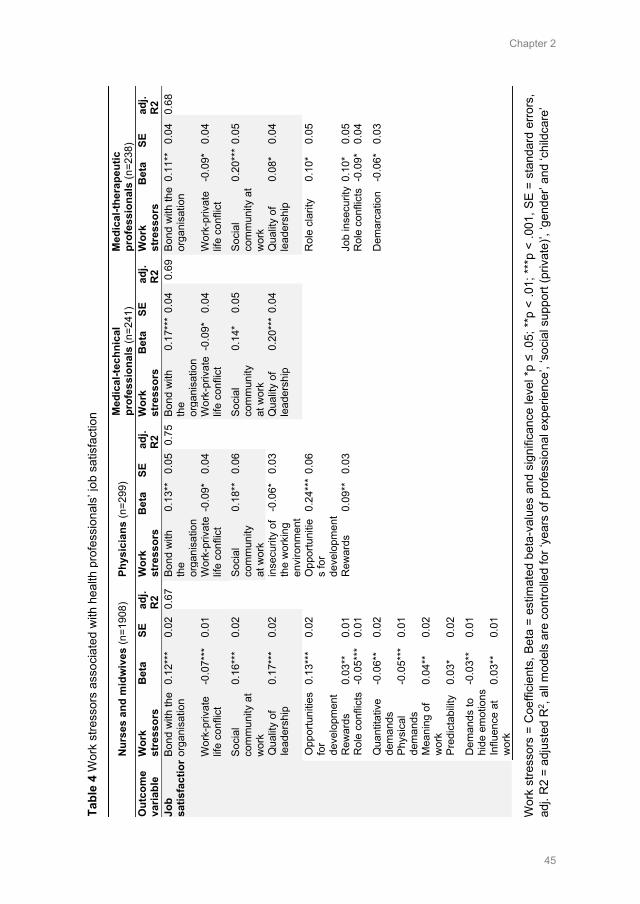
Chapter 2
45
Nur
ses
and
mid
wiv
es (n
=190
8)
Phys
icia
ns (n
=299
) M
edic
al-te
chni
cal
prof
essi
onal
s (n
=241
) M
edic
al-th
erap
eutic
pr
ofes
sion
als
(n=2
38)
Out
com
e va
riabl
e W
ork
stre
ssor
s B
eta
SE
adj.
R2
Wor
k st
ress
ors
Bet
a SE
ad
j. R
2 W
ork
stre
ssor
s B
eta
SE
adj.
R2
Wor
k st
ress
ors
Bet
a SE
ad
j. R
2 Jo
b sa
tisfa
ctio
n Bo
nd w
ith th
e or
gani
satio
n 0.
12**
* 0.
02
0.67
Bo
nd w
ith
the
orga
nisa
tion
0.13
**
0.05
0.
75
Bond
with
th
e or
gani
satio
n
0.17
***
0.04
0.
69
Bond
with
the
orga
nisa
tion
0.11
**
0.04
0.
68
Wor
k-pr
ivat
e lif
e co
nflic
t -0
.07*
**
0.01
Wor
k-pr
ivat
e lif
e co
nflic
t -0
.09*
0.
04
W
ork-
priv
ate
life
conf
lict
-0.0
9*
0.04
Wor
k-pr
ivat
e lif
e co
nflic
t -0
.09*
0.
04
Soci
al
com
mun
ity a
t w
ork
0.16
***
0.02
Soci
al
com
mun
ity
at w
ork
0.18
**
0.06
Soci
al
com
mun
ity
at w
ork
0.14
* 0.
05
So
cial
co
mm
unity
at
wor
k
0.20
***
0.05
Qua
lity
of
lead
ersh
ip
0.17
***
0.02
inse
curit
y of
th
e w
orki
ng
envi
ronm
ent
-0.0
6*
0.03
Qua
lity
of
lead
ersh
ip
0.20
***
0.04
Qua
lity
of
lead
ersh
ip
0.08
* 0.
04
Opp
ortu
nitie
s fo
r de
velo
pmen
t
0.13
***
0.02
Opp
ortu
nitie
s fo
r de
velo
pmen
t
0.24
***
0.06
Rol
e cl
arity
0.
10*
0.05
Rew
ards
0.
03**
0.
01
R
ewar
ds
0.09
**
0.03
Job
inse
curit
y 0.
10*
0.05
Rol
e co
nflic
ts
-0.0
5***
0.
01
R
ole
conf
licts
-0.
09*
0.04
Qua
ntita
tive
dem
ands
-0
.06*
* 0.
02
D
emar
catio
n -0
.06*
0.
03
Phys
ical
de
man
ds
-0.0
5***
0.
01
Mea
ning
of
wor
k 0.
04**
0.
02
Pred
icta
bilit
y 0.
03*
0.02
Dem
ands
to
hide
em
otio
ns -0
.03*
* 0.
01
Influ
ence
at
wor
k 0.
03**
0.
01
Tabl
e 4
Wor
k st
ress
ors
asso
ciat
ed w
ith h
ealth
pro
fess
iona
ls’ j
ob s
atis
fact
ion
Wor
k st
ress
ors
= C
oeffi
cien
ts, B
eta
= es
timat
ed b
eta-
valu
es a
nd s
igni
fican
ce le
vel *
p ≤
.05;
**p
< .0
1; *
**p
< .0
01, S
E =
stan
dard
erro
rs,
adj.
R2
= ad
just
ed R
2 , al
l mod
els
are
cont
rolle
d fo
r ‘ye
ars
of p
rofe
ssio
nal e
xper
ienc
e’, ‘
soci
al s
uppo
rt (p
rivat
e)’,
‘gen
der’
and
‘chi
ldca
re’
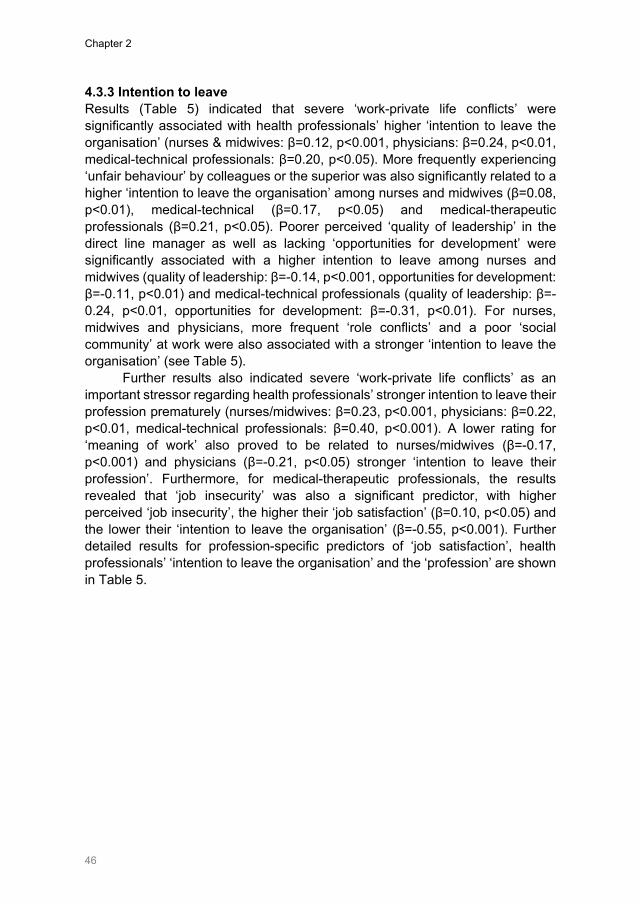
Chapter 2
46
4.3.3 Intention to leave Results (Table 5) indicated that severe ‘work-private life conflicts’ were significantly associated with health professionals’ higher ‘intention to leave the organisation’ (nurses & midwives: β=0.12, p<0.001, physicians: β=0.24, p<0.01, medical-technical professionals: β=0.20, p<0.05). More frequently experiencing ‘unfair behaviour’ by colleagues or the superior was also significantly related to a higher ‘intention to leave the organisation’ among nurses and midwives (β=0.08, p<0.01), medical-technical (β=0.17, p<0.05) and medical-therapeutic professionals (β=0.21, p<0.05). Poorer perceived ‘quality of leadership’ in the direct line manager as well as lacking ‘opportunities for development’ were significantly associated with a higher intention to leave among nurses and midwives (quality of leadership: β=-0.14, p<0.001, opportunities for development: β=-0.11, p<0.01) and medical-technical professionals (quality of leadership: β=-0.24, p<0.01, opportunities for development: β=-0.31, p<0.01). For nurses, midwives and physicians, more frequent ‘role conflicts’ and a poor ‘social community’ at work were also associated with a stronger ‘intention to leave the organisation’ (see Table 5).
Further results also indicated severe ‘work-private life conflicts’ as an important stressor regarding health professionals’ stronger intention to leave their profession prematurely (nurses/midwives: β=0.23, p<0.001, physicians: β=0.22, p<0.01, medical-technical professionals: β=0.40, p<0.001). A lower rating for ‘meaning of work’ also proved to be related to nurses/midwives (β=-0.17, p<0.001) and physicians (β=-0.21, p<0.05) stronger ‘intention to leave their profession’. Furthermore, for medical-therapeutic professionals, the results revealed that ‘job insecurity’ was also a significant predictor, with higher perceived ‘job insecurity’, the higher their ‘job satisfaction’ (β=0.10, p<0.05) and the lower their ‘intention to leave the organisation’ (β=-0.55, p<0.001). Further detailed results for profession-specific predictors of ‘job satisfaction’, health professionals’ ‘intention to leave the organisation’ and the ‘profession’ are shown in Table 5.
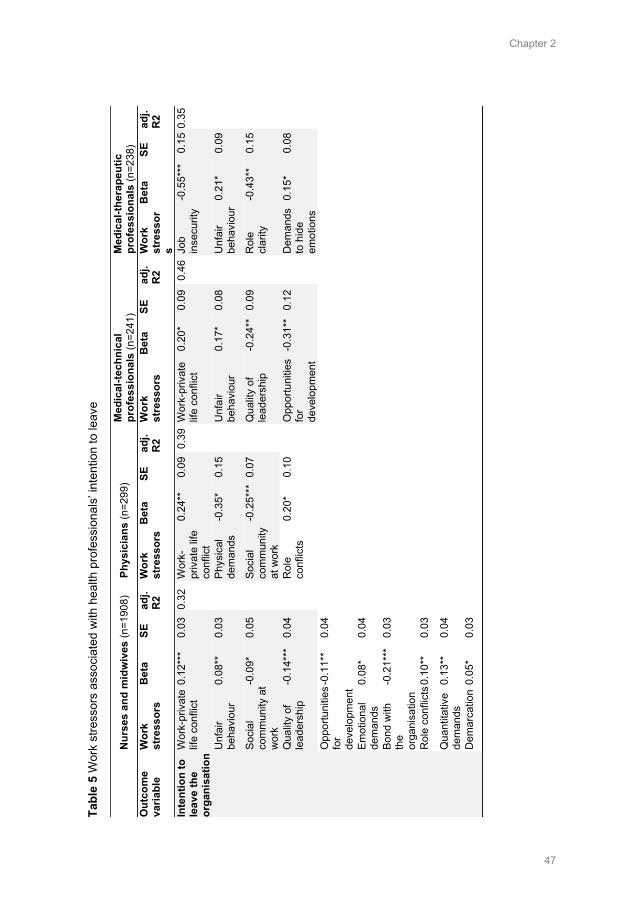
Chapter 2
47
N
urse
s an
d m
idw
ives
(n=1
908)
Ph
ysic
ians
(n=2
99)
Med
ical
-tech
nica
l pr
ofes
sion
als
(n=2
41)
Med
ical
-ther
apeu
tic
prof
essi
onal
s (n
=238
) O
utco
me
varia
ble
Wor
k st
ress
ors
Bet
a SE
ad
j. R
2 W
ork
stre
ssor
s B
eta
SE
adj.
R2
Wor
k st
ress
ors
Bet
a SE
ad
j. R
2 W
ork
stre
ssor
s
Bet
a SE
ad
j. R
2
Inte
ntio
n to
le
ave
the
orga
nisa
tion
Wor
k-pr
ivat
e lif
e co
nflic
t 0.
12**
* 0.
03
0.32
W
ork-
priv
ate
life
conf
lict
0.24
**
0.09
0.
39 W
ork-
priv
ate
life
conf
lict
0.20
* 0.
09
0.46
Job
in
secu
rity
-0.5
5***
0.
15 0
.35
Unf
air
beha
viou
r 0.
08**
0.
03
Ph
ysic
al
dem
ands
-0
.35*
0.
15
U
nfai
r be
havi
our
0.17
* 0.
08
U
nfai
r be
havi
our
0.21
* 0.
09
Soci
al
com
mun
ity a
t w
ork
-0.0
9*
0.05
Soci
al
com
mun
ity
at w
ork
-0.2
5***
0.0
7
Qua
lity
of
lead
ersh
ip
-0.2
4**
0.09
Rol
e cl
arity
-0
.43*
* 0.
15
Qua
lity
of
lead
ersh
ip
-0.1
4***
0.
04
R
ole
conf
licts
0.
20*
0.10
Opp
ortu
nitie
s fo
r de
velo
pmen
t
-0.3
1**
0.12
Dem
ands
to
hid
e em
otio
ns
0.15
* 0.
08
Opp
ortu
nitie
s fo
r de
velo
pmen
t -0.1
1**
0.04
Emot
iona
l de
man
ds
0.08
* 0.
04
Bond
with
th
e or
gani
satio
n
-0.2
1***
0.
03
Rol
e co
nflic
ts 0
.10*
* 0.
03
Qua
ntita
tive
dem
ands
0.
13**
0.
04
Dem
arca
tion
0.05
* 0.
03
Tabl
e 5
Wor
k st
ress
ors
asso
ciat
ed w
ith h
ealth
pro
fess
iona
ls’ i
nten
tion
to le
ave
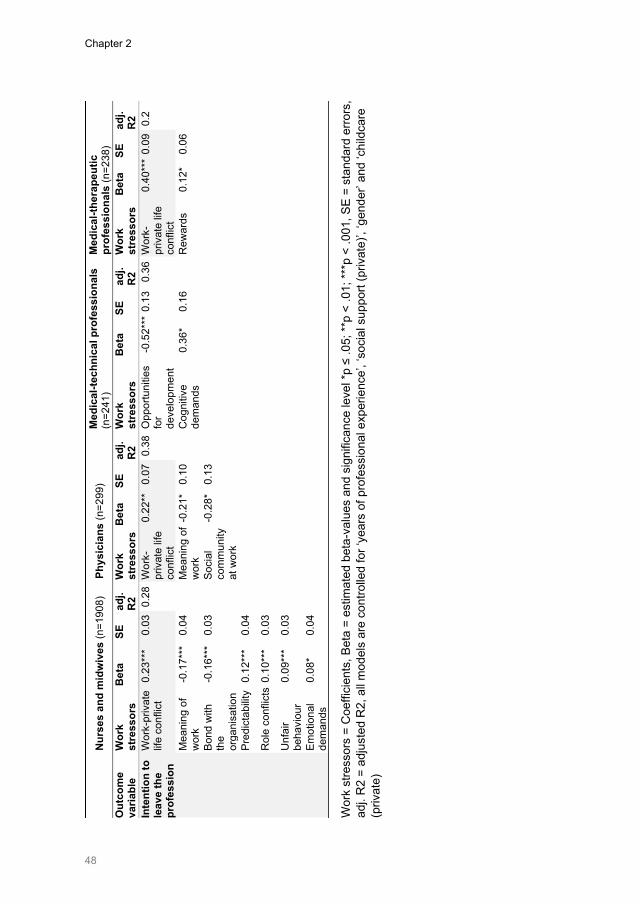
Chapter 2
48
N
urse
s an
d m
idw
ives
(n=1
908)
Ph
ysic
ians
(n=2
99)
Med
ical
-tech
nica
l pro
fess
iona
ls
(n=2
41)
Med
ical
-ther
apeu
tic
prof
essi
onal
s (n
=238
) O
utco
me
varia
ble
Wor
k st
ress
ors
Bet
a SE
ad
j. R
2 W
ork
stre
ssor
s B
eta
SE
adj.
R2
Wor
k st
ress
ors
Bet
a SE
ad
j. R
2 W
ork
stre
ssor
s B
eta
SE
adj.
R2
Inte
ntio
n to
le
ave
the
prof
essi
on
Wor
k-pr
ivat
e lif
e co
nflic
t 0.
23**
* 0.
03
0.28
Wor
k-pr
ivat
e lif
e co
nflic
t
0.22
**
0.07
0.
38 O
ppor
tuni
ties
for
deve
lopm
ent
-0.5
2***
0.1
3 0.
36 W
ork-
priv
ate
life
conf
lict
0.40
***
0.09
0.
2
Mea
ning
of
wor
k -0
.17*
**
0.04
Mea
ning
of
wor
k -0
.21*
0.
10
C
ogni
tive
dem
ands
0.
36*
0.16
Rew
ards
0.
12*
0.06
Bond
with
th
e or
gani
satio
n
-0.1
6***
0.
03
So
cial
co
mm
unity
at
wor
k
-0.2
8*
0.13
Pred
icta
bilit
y 0.
12**
* 0.
04
Rol
e co
nflic
ts 0
.10*
**
0.03
Unf
air
beha
viou
r 0.
09**
* 0.
03
Emot
iona
l de
man
ds
0.08
* 0.
04
Wor
k st
ress
ors
= C
oeffi
cien
ts, B
eta
= es
timat
ed b
eta-
valu
es a
nd s
igni
fican
ce le
vel *
p ≤
.05;
**p
< .0
1; **
*p <
.001
, SE
= st
anda
rd e
rrors
, ad
j. R
2 =
adju
sted
R2,
all
mod
els
are
cont
rolle
d fo
r ‘ye
ars
of p
rofe
ssio
nal e
xper
ienc
e’, ‘
soci
al s
uppo
rt (p
rivat
e)’,
‘gen
der’
and
‘chi
ldca
re
(priv
ate)
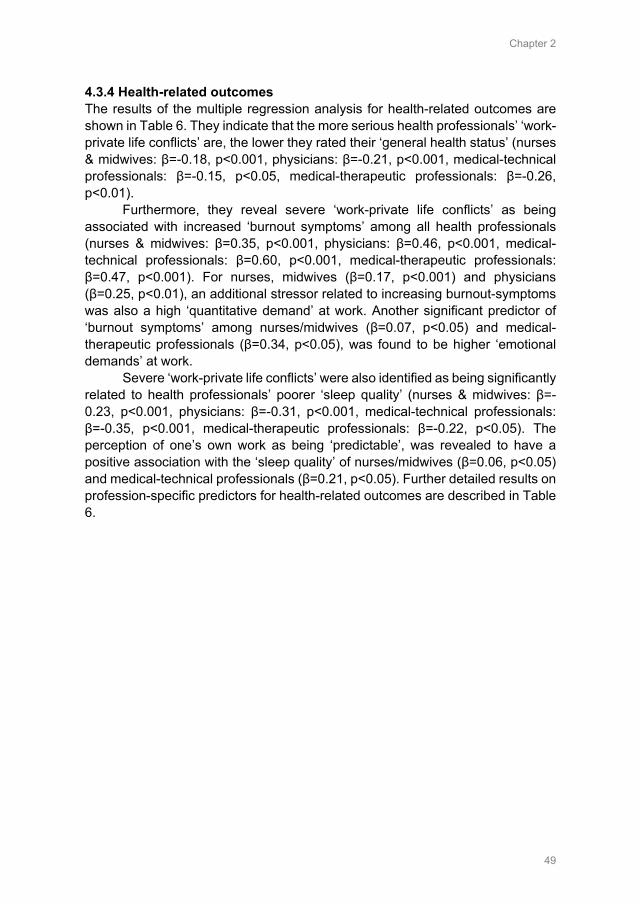
Chapter 2
49
4.3.4 Health-related outcomes The results of the multiple regression analysis for health-related outcomes are shown in Table 6. They indicate that the more serious health professionals’ ‘work-private life conflicts’ are, the lower they rated their ‘general health status’ (nurses & midwives: β=-0.18, p<0.001, physicians: β=-0.21, p<0.001, medical-technical professionals: β=-0.15, p<0.05, medical-therapeutic professionals: β=-0.26, p<0.01).
Furthermore, they reveal severe ‘work-private life conflicts’ as being associated with increased ‘burnout symptoms’ among all health professionals (nurses & midwives: β=0.35, p<0.001, physicians: β=0.46, p<0.001, medical-technical professionals: β=0.60, p<0.001, medical-therapeutic professionals: β=0.47, p<0.001). For nurses, midwives (β=0.17, p<0.001) and physicians (β=0.25, p<0.01), an additional stressor related to increasing burnout-symptoms was also a high ‘quantitative demand’ at work. Another significant predictor of ‘burnout symptoms’ among nurses/midwives (β=0.07, p<0.05) and medical-therapeutic professionals (β=0.34, p<0.05), was found to be higher ‘emotional demands’ at work.
Severe ‘work-private life conflicts’ were also identified as being significantly related to health professionals’ poorer ‘sleep quality’ (nurses & midwives: β=-0.23, p<0.001, physicians: β=-0.31, p<0.001, medical-technical professionals: β=-0.35, p<0.001, medical-therapeutic professionals: β=-0.22, p<0.05). The perception of one’s own work as being ‘predictable’, was revealed to have a positive association with the ‘sleep quality’ of nurses/midwives (β=0.06, p<0.05) and medical-technical professionals (β=0.21, p<0.05). Further detailed results on profession-specific predictors for health-related outcomes are described in Table 6.
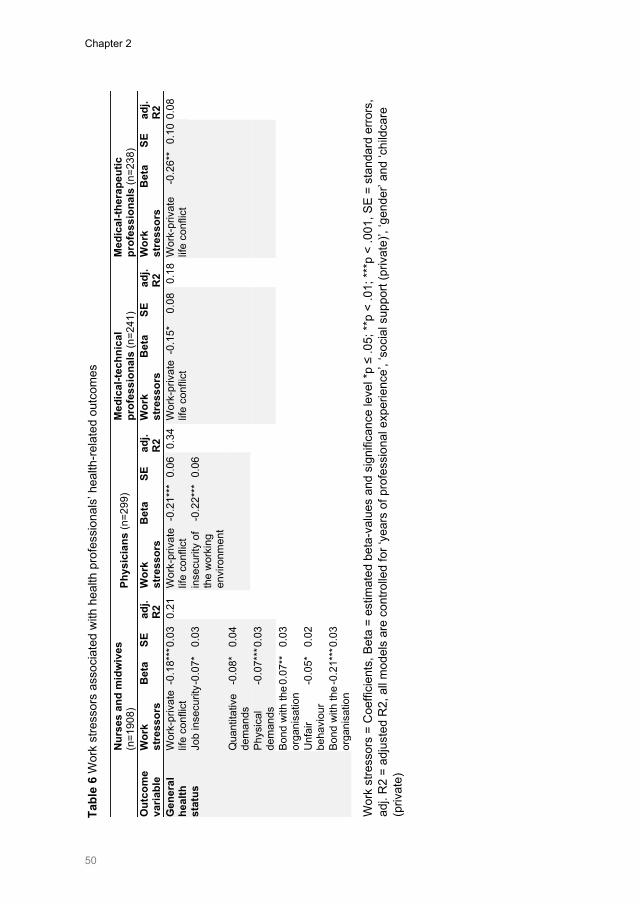
Chapter 2
50
N
urse
s an
d m
idw
ives
(n
=190
8)
Phys
icia
ns (n
=299
) M
edic
al-te
chni
cal
prof
essi
onal
s (n
=241
) M
edic
al-th
erap
eutic
pr
ofes
sion
als
(n=2
38)
Out
com
e va
riabl
e W
ork
stre
ssor
s B
eta
SE
adj.
R2
Wor
k st
ress
ors
Bet
a SE
ad
j. R
2 W
ork
stre
ssor
s B
eta
SE
adj.
R2
Wor
k st
ress
ors
Bet
a SE
ad
j. R
2 G
ener
al
heal
th
stat
us
Wor
k-pr
ivat
e lif
e co
nflic
t -0
.18*
** 0.
03
0.21
W
ork-
priv
ate
life
conf
lict
-0.2
1***
0.0
6 0.
34
Wor
k-pr
ivat
e lif
e co
nflic
t -0
.15*
0.
08
0.18
Wor
k-pr
ivat
e lif
e co
nflic
t -0
.26*
* 0.
10 0
.08
Job
inse
curit
y -0.
07*
0.03
inse
curit
y of
th
e w
orki
ng
envi
ronm
ent
-0.2
2***
0.0
6
Qua
ntita
tive
dem
ands
-0
.08*
0.
04
Phys
ical
de
man
ds
-0.0
7***
0.03
Bond
with
the
orga
nisa
tion
0.07
**
0.03
Unf
air
beha
viou
r -0
.05*
0.
02
Bond
with
the
orga
nisa
tion
-0.2
1***
0.03
Tabl
e 6
Wor
k st
ress
ors
asso
ciat
ed w
ith h
ealth
pro
fess
iona
ls’ h
ealth
-rela
ted
outc
omes
Wor
k st
ress
ors
= C
oeffi
cien
ts, B
eta
= es
timat
ed b
eta-
valu
es a
nd s
igni
fican
ce le
vel *
p ≤
.05;
**p
< .0
1; **
*p <
.001
, SE
= st
anda
rd e
rrors
, ad
j. R
2 =
adju
sted
R2,
all
mod
els
are
cont
rolle
d fo
r ‘ye
ars
of p
rofe
ssio
nal e
xper
ienc
e’, ‘
soci
al s
uppo
rt (p
rivat
e)’,
‘gen
der’
and
‘chi
ldca
re
(priv
ate)
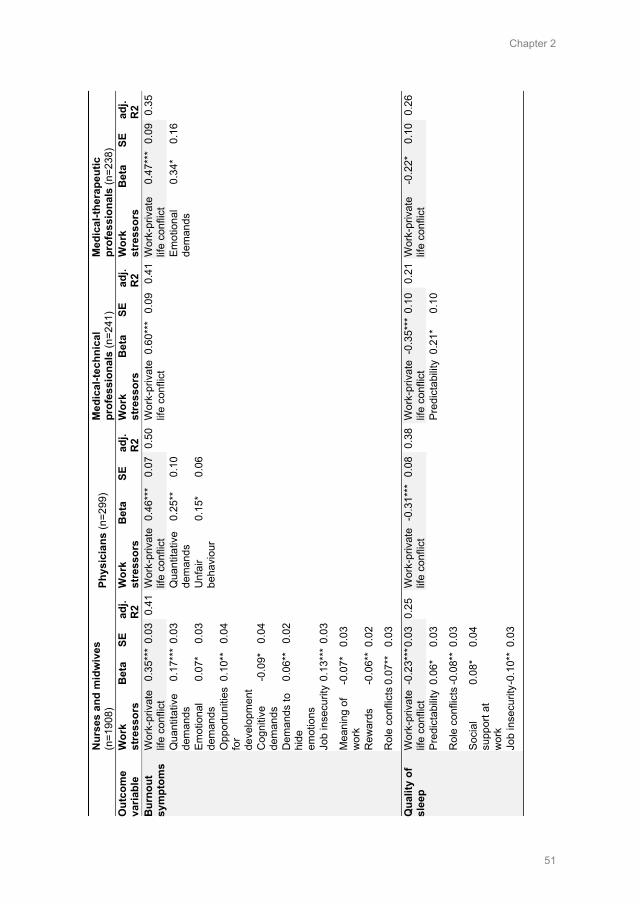
Chapter 2
51
N
urse
s an
d m
idw
ives
(n
=190
8)
Phys
icia
ns (n
=299
) M
edic
al-te
chni
cal
prof
essi
onal
s (n
=241
) M
edic
al-th
erap
eutic
pr
ofes
sion
als
(n=2
38)
Out
com
e va
riabl
e W
ork
stre
ssor
s B
eta
SE
adj.
R2
Wor
k st
ress
ors
Bet
a SE
ad
j. R
2 W
ork
stre
ssor
s B
eta
SE
adj.
R2
Wor
k st
ress
ors
Bet
a SE
ad
j. R
2 B
urno
ut
sym
ptom
s W
ork-
priv
ate
life
conf
lict
0.35
***
0.03
0.
41 W
ork-
priv
ate
life
conf
lict
0.46
***
0.07
0.
50
Wor
k-pr
ivat
e lif
e co
nflic
t 0.
60**
* 0.
09
0.41
Wor
k-pr
ivat
e lif
e co
nflic
t 0.
47**
* 0.
09
0.35
Qua
ntita
tive
dem
ands
0.
17**
* 0.
03
Q
uant
itativ
e de
man
ds
0.25
**
0.10
Emot
iona
l de
man
ds
0.34
* 0.
16
Emot
iona
l de
man
ds
0.07
* 0.
03
U
nfai
r be
havi
our
0.15
* 0.
06
Opp
ortu
nitie
s fo
r de
velo
pmen
t
0.10
**
0.04
Cog
nitiv
e de
man
ds
-0.0
9*
0.04
Dem
ands
to
hide
em
otio
ns
0.06
**
0.02
Job
inse
curit
y 0.
13**
* 0.
03
Mea
ning
of
wor
k -0
.07*
0.
03
Rew
ards
-0
.06*
* 0.
02
Rol
e co
nflic
ts 0
.07*
* 0.
03
Qua
lity
of
slee
p W
ork-
priv
ate
life
conf
lict
-0.2
3***
0.03
0.
25
Wor
k-pr
ivat
e lif
e co
nflic
t -0
.31*
** 0
.08
0.38
W
ork-
priv
ate
life
conf
lict
-0.3
5***
0.1
0 0.
21 W
ork-
priv
ate
life
conf
lict
-0.2
2*
0.10
0.
26
Pred
icta
bilit
y 0.
06*
0.03
Pred
icta
bilit
y 0.
21*
0.10
Rol
e co
nflic
ts -0
.08*
* 0.
03
Soci
al
supp
ort a
t w
ork
0.08
* 0.
04
Job
inse
curit
y -0.
10**
0.0
3
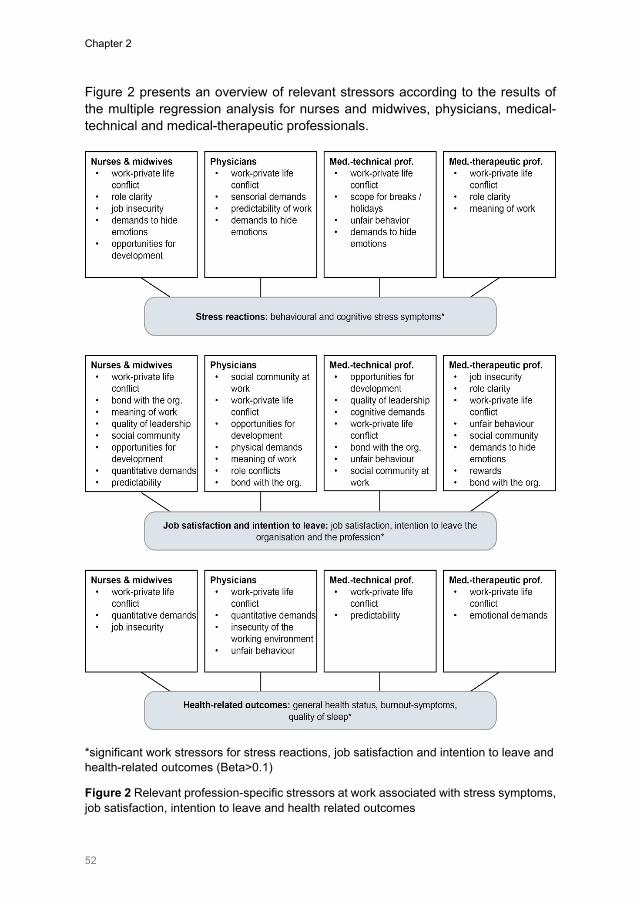
Chapter 2
52
Figure 2 presents an overview of relevant stressors according to the results of the multiple regression analysis for nurses and midwives, physicians, medical-technical and medical-therapeutic professionals.
*significant work stressors for stress reactions, job satisfaction and intention to leave and health-related outcomes (Beta>0.1)
Figure 2 Relevant profession-specific stressors at work associated with stress symptoms, job satisfaction, intention to leave and health related outcomes
Chapter 2
53
5. Discussion
This study provides, for the first time, important information on the extent of work stressors, stress reactions and long-term consequences for nurses and midwives, physicians, medical-technical and medical-therapeutic professionals in Swiss acute care and rehabilitation hospitals.
Regarding work stressors associated with health professionals’ stress reactions and their long-term consequences, ‘work-private life conflicts’ were revealed to be most relevant across all health professionals. These results confirm findings from other studies, in which ‘work-private life conflicts’ among health professionals was also determined to be relevant for increased ‘burnout symptoms’, the ‘intention to leave’ or actually ‘leaving the profession’.3, 12, 18 On the other hand, this study contributes to the existing literature by exploring ‘work-private life conflicts’ also associated with health professionals’ ‘behavioural’ and ‘cognitive stress symptoms’, ‘job satisfaction’, ‘general health status’ and ‘sleep quality’. Shivakumar and Pujar35 explain the increasing work-private life conflict in the healthcare sector as a result of a paradigm shift in the definition of family itself. Additionally, there are conflicts between the health professionals themselves, their social interests and families, as well as with meeting the expectations of their employers.12, 35 In particular, due to the healthcare sector operating 24 hours a day, it is essential for health organisations to develop effective strategies to reduce work-private life conflicts, in order to enhance health professionals’ job satisfaction and commitment to the organization.36 Other studies have shown, however, that work-private life conflicts among health professionals can be significantly reduced, for example, by using an open-rotation system for shift planning or by direct line managers exhibiting family-supportive behaviours.37, 38
Lacking opportunities for development was also found to affect nurses’ and midwives’ ‘stress reactions’, ‘job satisfaction’, ‘intention to leave the organisation’ and ‘burnout symptoms’, as well as physicians’ ‘job satisfaction’ and ‘intention to leave’ among medical-technical professionals. Moreover, the perceived behaviour of the line manager, such as his/her ‘quality of leadership’, existing ‘role clarity’ for employees, ‘unfair behaviour’ and lack of ‘reward’ appeared to be important regarding health professionals’ ‘stress symptoms’, ‘job satisfaction’ and ‘intention to leave’. The importance of good leadership in the healthcare setting has also been discussed in the literature as affecting employees’ job satisfaction, commitment to the organisation, work-performance and productivity.39, 40 Leaders on all levels play an important role in reducing work-related stress in their employees, and our study results support the call for good leaders and specific interventions to improve leadership quality in healthcare.41 However, health care leaders themselves are exposed to high demands (e.g. heavy workloads) in their daily work42, which should be taken into account when developing effective interventions to reduce stress at work.
Chapter 2
54
Moreover, the results of the regression models imply that different health professionals have differing needs for action regarding, for example the ‘demands to hide emotions’. In this example, ‘demands to hide emotions’ was associated with nurses and midwives, and with physicians and medical-technical professionals, it was associated with ‘behavioural stress symptoms’. However, for medical-therapeutic professionals, ‘demands to hide emotions’ was associated with their ‘intention to leave the organisation’. Additionally, ‘quantitative demands’ at work were associated with nurses’, midwives’ and physicians’ ‘burnout-symptoms’, but not with the medical-technical and medical-therapeutic professionals. Overall, the results indicate, that the extent of stressors and their association with possible outcomes varies greatly between different health professions. Previous studies also indicated that health professionals are confronted with different stressors at work, depending on their specific professional role and work environment (e.g. experience of aggression from patients and visitors or stress resulting from malpractice lawsuits).13, 43-
47Therefore, it seems to be essential to analyse the extent of work stressors specifically for each discipline, as well as their association with stress reactions and long-term consequences. This would assist in developing individual strategies to prevent and reduce stress at work, shaped to the specific working conditions of each health profession separately.
5.1 Strengths and limitations This study differs from other studies mainly because of the many outcome variables and including health professionals from various disciplines. Therefore, the findings do not provide information on a single outcome or health profession, but on several important outcome variables as well as from multiple regression analysis for different disciplines separately. This has the advantage of identifying important predictors for several outcomes at the same time and of being able to reveal relevant similarities and differences between the various professional groups. In addition, this study provides the first findings for various health professionals from the German- and French-speaking part of Switzerland (not only from one language area as did most studies) with a sufficiently large sample for both language parts. Moreover, the questionnaire and data analysis are based on a strong theoretical background from Eurofound6 the questionnaire consists of well established, reliable and valid scales, which supports the validity of the current results.
On the other hand, because this study utilized a cross-sectional design, causal conclusions cannot be drawn from the results. Participation in the study was voluntary for randomized health organisations as well as for health professionals; therefore, a selection bias is possible (e.g. that health professionals with a higher level of work-related stress did not participate for reasons of time, or, in organisations with a lower response rate, the level of work-
Chapter 2
55
related stress may have been higher). Moreover, the higher number of cases of nurses in the study sample has resulted in more significant predictors in the regression models. It is possible that a larger number of participants from other professions (e.g. physicians) could also have revealed more significant predictors. Furthermore, the generalisability of the results may be limited, as nurses and midwives are slightly overrepresented in the study sample.
6. Conclusion
This study not only identifies the extent of salient work stressors, but also their association with stress reaction and long-term consequences for various categories of health professionals and, therefore, makes an important contribution towards a better understanding of stress at work in acute care and rehabilitation hospitals. However, further research is still needed to obtain more detailed and longitudinal data on possible work stressors among the different health professions. Furthermore, profession-specific prevention programmes are necessary in order to reduce stressors in a targeted manner.
6.1 Relevance to clinical practice The results of this study are particularly relevant for health professional leaders as well as occupational nurses and physicians in order to prevent and reduce stress at work among health professionals. The results reveal the urgent need in hospital practice for effective strategies to improve health professionals’ work-private life balance, opportunities for development and quality of leadership. This is important in order to improve health professionals’ job satisfaction, health and motivation to remain at work. In addition, the results of this study highlight the importance of examining stressors at work separately for different healthcare professions, as they can vary substantially. This is particularly important to consider when designing and evaluating interventions with various healthcare professions.
Chapter 2
56
Acknowledgements We are very grateful to all organisations and healthcare professionals who participated in this study for sharing their experience and time so generously. Additionally, we thank Dr. Reto Bürgin, who shared his expertise in statistical analysis with us. Conflict of interest “No conflict of interest has been declared by the author(s)”. Funding This study was financially supported by the University of Applied Sciences, Health Division, Bern, Switzerland, and the State Secretariat for Education and Research (SER) of Switzerland. The funders had no influence or control on the planning, conduct, or reporting of the study. Availability of data and materials The raw dataset analysed in the current study is available from the corresponding author (Karin Anne Peter) on reasonable request. Authors' contributions KP and SH designed the questionnaire and recruited the participating health organisations. KP collected and analysed the data. RH und JS made substantial contributions to the interpretation of data and in writing the manuscript. All authors read and approved the final manuscript.
Chapter 2
57
References 1. World Health Organisation. Global strategy on human resources for health: workforce 2030.
Geneva: World Health Organization, 2016. 2. Marć M, Bartosiewicz A, Burzyńska J, Chmiel Z, Januszewicz P. A nursing shortage – a prospect
of global and local policies. International Nursing Review. 2019;66(1):9-16. doi:10.1111/inr.12473 3. Hämmig O. Explaining burnout and the intention to leave the profession among health
professionals - a cross-sectional study in a hospital setting in Switzerland. BMC Health Service Research. 2018;18(1):785. doi:10.1186/s12913-018-3556-1
4. Li J, Galatsch M, Siegrist J, Muller BH, Hasselhorn HM, European NSg. Reward frustration at work and intention to leave the nursing profession--prospective results from the European longitudinal NEXT study. International Journal of Nursing Studies. 2011;48(5):628-635. doi:10.1016/j.ijnurstu.2010.09.011
5. Lee YW, Dai YT, Chang MY, Chang YC, Yao KG, Liu MC. Quality of Work Life, Nurses’ Intention to Leave the Profession, and Nurses Leaving the Profession: A One-Year Prospective Survey. Journal of Nursing Scholarship. 2017;49(4):438-444. doi:10.1111/jnu.12301
6. Eurofound. Work-related stress. Dublin: Eurofound, 2005. 7. Leka S, Jain A. Health impact of psychosocial hazards at work: An overview. Geneva: World
Health Organization, 2010. 8. Pekurinen V, Willman L, Virtanen M, Kivimäki M, Vahtera J, Välimäki M. Patient Aggression and
the Wellbeing of Nurses: A Cross-Sectional Survey Study in Psychiatric and Non-Psychiatric Settings. Int J Environ Res Public Health. 2017;14(10):1245.
9. Aiken LH, Sloane DM, Bruyneel L, Van den Heede K, Sermeus W, Consortium RC. Nurses' reports of working conditions and hospital quality of care in 12 countries in Europe. International Journal of Nursing Studies. 2013;50(2):143-153. doi:10.1016/j.ijnurstu.2012.11.009
10. Dhaini SR, Denhaerynck K, Bachnick S, Schwendimann R, Schubert M, De Geest S, et al. Work schedule flexibility is associated with emotional exhaustion among registered nurses in Swiss hospitals: A cross-sectional study. International Journal of Nursing Studies. 2018;82:99-105. doi:10.1016/j.ijnurstu.2018.03.019
11. Hausler N, Bopp M, Hammig O. Effort-Reward Imbalance, Work-Privacy Conflict, and Burnout Among Hospital Employees. Journal of Occupational and Environmental Medicine. 2018;60(4):e183-e187. doi:10.1097/JOM.0000000000001287
12. Albertsen K, Rafnsdottir GL, Grimsmo A, Tomasson K, Kauppinen K. Workhours and worklife balance. Scandinavian Journal of Work Environment & Health. 2008;5:14-21.
13. Gilles I, Burnand B, Peytremann-Bridevaux I. Factors associated with healthcare professionals' intent to stay in hospital: a comparison across five occupational categories. Int J Qual Health Care. 2014;26(2):158-166. doi:10.1093/intqhc/mzu006
14. Lim J, Bogossian F, Ahern K. Stress and coping in Australian nurses: a systematic review. International Nursing Review. 2010;57(1):22-31. doi:10.1111/j.1466-7657.2009.00765.x
15. Sturm H, Rieger MA, Martus P, Ueding E, Wagner A, Holderried M, et al. Do perceived working conditions and patient safety culture correlate with objective workload and patient outcomes: A cross-sectional explorative study from a German university hospital. PloS one. 2019;14(1):e0209487. doi:10.1371/journal.pone.0209487
16. Khamisa N, Peltzer K, Ilic D, Oldenburg B. Work related stress, burnout, job satisfaction and general health of nurses: A follow-up study. International Journal of Nursing Practice. 2016;22(6):538-545. doi:10.1111/ijn.12455
17. Weigl M, Schmuck F, Heiden B, Angerer P, Müller A. Associations of understaffing and cardiovascular health of hospital care providers: A multi-source study. International Journal of Nursing Studies. 2019;99:103390. doi:doi.org/10.1016/j.ijnurstu.2019.103390
18. Lee R, Seo B, Hladkyj S, Lovell BL, Schwartzmann L. Correlates of physician burnout across regions and specialties: a meta-analysis. Human Resources for Health. 2013;11(1):48. doi:10.1186/1478-4491-11-48
19. Long MH, Johnston V, Bogossian F. Work-related upper quadrant musculoskeletal disorders in midwives, nurses and physicians: A systematic review of risk factors and functional consequences. Applied Ergonomics. 2012;43(3):455-467. doi:10.1016/j.apergo.2011.07.002
20. Ruotsalainen JH, Verbeek JH, Marine A, Serra C. Preventing occupational stress in healthcare workers. Cochrane Database of Systematic Reviews. 2014(11):Cd002892. doi:10.1002/14651858.CD002892.pub3
Chapter 2
58
21. De Pietro C, Camenzind P, Sturny I, Crivelli L, Edwards-Garavoglia S, Spranger A, et al. Switzerland: Health system review. Health Systems in Transition. 2015;17(4):1–288.
22. Kristensen TS. A new tool for assessing psychosocial factors at work: The Copenhagen Psychosocial Questionnaire. Copenhagen: National Institute of Health, 2000.
23. Kristensen TS, Hannerz H, Høgh A, Borg V. The Copenhagen Psychosocial Questionnaire-a tool for the assessment and improvement ofthe psychosocial work environment. Scandinavian Journal of Work, Environment & Health. 2005;31(6):438-449.
24. Llorens C, Pérez-Franco J, Oudyk J, Berthelsen H, Dupret E, Nübling M, et al. Agreed guidelines for the use of COPSOQ III2018.
25. Nübling M, Vomstein M, Nolle I, Lindner A, Haug A, Lincke HJ. Deutsche Standard-Version des COPSOQ 2017. Freiburg: FFAW-Freiburger Forschungsstelle für Arbeitswissenschaften GmbH, 2017.
26. Nübling M, Stössel U, Hasselhorn HM, Michaelis M, Hofmann F. Measuring psychological stress and strain at work: Evaluation of the COPSOQ Questionnaire in Germany. GMS Psycho-Social-Medicine. 2006;3:1-14.
27. Nübling M, Stößel U, Hasselhorn HM, Michaelis M, Hofmann F. Methoden zur Erfassung psychischer Belastungen: Erprobung eines Messinstruments (COPSOQ). Dortmund: Bundesanstalt für Arbeitsschutz und Arbeitsmedizin, 2005.
28. Sarason IG, Levine HM, Basham RB, Sarason BR. Assessing Social Support - the Social Support Questionnaire. Journal of Personality and Social Psychology. 1983;44(1):127-139. doi:Doi 10.1037/0022-3514.44.1.127
29. de Jonge J, Mulder MJ, Nijhuis FJ. The incorporation of different demand concepts in the job demand-control model: effects on health care professionals. Social Science & Medicine. 1999;48(9):1149-1160. doi:10.1016/s0277-9536(98)00429-8
30. Hasselhorn HM, Tackenberg P, Müller H. Working conditions and intent to leave the profession among nursing staff in Europe. Sweden: National Institute for Working Life, 2003.
31. Camerino D, Conway PM, Sartori S, Campanini P, Estryn‐Béhar M, van der Heijden BIJM, et al. Factors Affecting Work Ability in Day and Shift‐Working Nurses. Chronobiology International. 2008;25(2-3):425-442. doi:10.1080/07420520802118236
32. Eurofound. Sixth European Working Conditions Survey - Questionnaire. Luxembourg: Publications Office of the European Union, 2015.
33. Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Quality of Life Research. 2011;20(10):1727-1736. doi:10.1007/s11136-011-9903-x
34. Janssen MF, Pickard AS, Golicki D, Gudex C, Niewada M, Scalone L, et al. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: a multi-country study. Quality of Life Research. 2013;22(7):1717-1727. doi:10.1007/s11136-012-0322-4
35. Hasselhorn HM, Conway PM, Widerszal-Bazyl M, Simon M, Tackenberg P, Schmidt S, et al. Contribution of job strain to nurses' consideration of leaving the profession - results from the longitudinal European nurses' early exit study. Scandinavian Journal of Work Environment & Health. 2008;34(6):75-82.
36. Shivakumar K, Pujar V. Work Life Balance in the Health Care Sector. Amity Journal of Healthcare Management. 2017;1(2):45-54. doi:10.13140/RG.2.2.19413.73440
37. Azeem SM, Akhtar N. The Influence of Work Life Balance and Job Satisfaction on Organizational Commitment of Healthcare Employees. International Journal of Human Resource Studies. 2014;4(2):18-24. doi:10.5296/ijhrs.v4i2.5667
38. Hammer LB, Kossek EE, Anger WK, Bodner T, Zimmerman KL. Clarifying work-family intervention processes: the roles of work-family conflict and family-supportive supervisor behaviors. Journal of Applied Psychology. 2011;96(1):134-150. doi:10.1037/a0020927
39. Pryce J, Albertsen K, Nielsen K. Evaluation of an open‐rota system in a Danish psychiatric hospital: a mechanism for improving job satisfaction and work–life balance. Journal of Nursing Management. 2006;14(4):282-288.
40. Daly J, Jackson D, Mannix J, Davidson P, Hutchinson M. The importance of clinical leadership in the hospital setting. Journal of Healthcare Leadership. 2014;2014(6):75-83. doi:10.2147/jhl.S46161
41. Mosadeghrad AM, Ferdosi M. Leadership, job satisfaction and organizational commitment in healthcare sector: proposing and testing a model. Mater Sociomed. 2013;25(2):121-126. doi:10.5455/msm.2013.25.121-126
42. Kelloway EK, Barling J. Leadership development as an intervention in occupational health psychology. Work and Stress. 2010;24(3):260-279. doi:10.1080/02678373.2010.518441
Chapter 2
59
43. Labrague LJ, McEnroe-Petitte DM, Leocadio MC, Van Bogaert P, Cummings GG. Stress and ways of coping among nurse managers: An integrative review. Journal of clinical nursing. 2018;27(7-8):1346-1359. doi:10.1111/jocn.14165
44. Fileni A, Magnavita N, Mammi F, Mandoliti G, Luca F, Magnavita G, et al. Malpractice stress syndrome in radiologists and radiotherapists: perceived causes and consequences. Radiol Med. 2007;112(7):1069-1084. doi:10.1007/s11547-007-0206-9
45. Magnavita N, Fileni A, Magnavita G, Mammi F, Mirk P, Roccia K, et al. Work stress in radiologists. A pilot study. Radiol Med. 2008;113(3):329-346. doi:10.1007/s11547-008-0259-4
46. Hahn S, Hantikainen V, Needham I, Kok G, Dassen T, Halfens RJ. Patient and visitor violence in the general hospital, occurrence, staff interventions and consequences: a cross-sectional survey. Journal of Advanced Nursing. 2012;68(12):2685-2699. doi:10.1111/j.1365-2648.2012.05967.x
47. Magnavita N. The Exploding Spark: Workplace Violence in an Infectious Disease Hospital—A Longitudinal Study. BioMed Research International. 2013;2013:1-9. doi:10.1155/2013/316358
48. Magnavita N, Sestili C, Mannocci A, Ercoli E, Boccia A, Bonaga G, et al. Mental and physical well-being in oncology-hematology-unit personnel. Arch Environ Occup Health. 2018;73(6):375-380. doi:10.1080/19338244.2017.1361901
Chapter 3
Factors associated with work-private life conflict and leadership qualities among line managers of health professionals in Swiss acute and rehabilitation hospitals – a cross-sectional study
Peter KA, Halfens RJG, Hahn S, Schols JMGA. Factors associated with work-private life conflict and leadership qualities among line managers of health professionals in Swiss acute and rehabilitation hospitals – a cross-sectional study. (submitted)
EMBARGOED
This chapter is embargoed at request
Chapter 4
Investigating work-related stress among health professionals at different hierarchical levels – a cross-sectional study
Peter KA, Schols JMGA, Halfens RJG, Hahn S. Investigating work-related stress among health professionals at different hierarchical levels: A cross-sectional study. Nursing Open. 2020;7(4):969-979. doi:10.1002/nop2.469

Chapter 4
86
Abstract
Background: Since stress at work is an important issue affecting health professionals’ job satisfaction and health, further knowledge is needed about its extent at various management levels. Aim: To determine the extent of stress at work among health professionals working in upper, middle and lower-management positions and those not working in management positions. Design: Cross-sectional design and randomly selected hospitals, nursing homes and home care organisations. Methods: The study sample included nursing staff and midwives, physicians, medical-technical and medical-therapeutic professionals at all hierarchical levels (N=8,112). Data was collected using self-report questionnaires and analysed using multiple regression models. Results: Health professionals in upper and middle-management positions reported higher quantitative demands, severe work-private life conflicts (p<0.05) as well as less role clarity in middle-management positions (B=-1.58, p<0.05). In lower-management positions, health professionals reported higher physical (B=3.80, p<0.001) and emotional demands (B=1.79, p<0.01), stress symptoms (B=1.81, p<0.05) and job dissatisfaction (B=-1.17, p<0.05). Health professionals without management responsibilities reported the poorest working conditions in relation to various stressors, job satisfaction (B=-5.20, p<0.001) and health-related outcomes (e.g. burnout-symptoms: B=1.89, p<0.01). Conclusion: The results imply that to effectively prevent and reduce stress; it is important to develop separate interventions at each hierarchical level.

Chapter 4
87
1. Introduction
The workforce shortage among health professionals is an acute issue worldwide, and has the potential to destabilise the availability and quality of care provided in individual countries.1, 2 As research indicates, a high level of work-related stress is a key reason for health professionals’ increasing absenteeism (e.g. due to burnout), job dissatisfaction or their intention to leave the profession prematurely.3, 4 Work-related stress can be defined as ‘a pattern of reactions that occur when workers are confronted with demands or pressures that are not matched to their knowledge, abilities and skills, and which challenge their ability to cope’.5, 6 Health professionals are particularly affected as their daily work involves many stressors, such as high emotional and physical demands, working under time pressure, long working hours, work-private life conflicts, aggressive patients and visitors, as well as exposure to infectious diseases or hazardous substances.3, 7, 8
Leaders of healthcare organisations play a key role, as their behaviour has the potential to influence the perceived level of work-related stress among their employees.4, 9, 10 Leadership is defined as ‘constituting a process of social influence that is enacted by designated individuals who hold formal leadership roles in organisations’.10 A previous literature review9 revealed that not only the behaviour of leaders (e.g. supportive, empowering) or their leadership style, but also their own perceived level of work-related stress can affect the well-being of their employees. More specifically, an association between leaders’ and employees’ burnout, as well as their experience of emotions (e.g., negative emotions were even more strongly experienced by employees than by their leaders) was identified.9, 11 Additionally, a systematic review and meta-analysis on the association of leadership and well-being at work demonstrated that leadership has the potential to affect employee job satisfaction, well-being and sick leave.12
2. Background
In order to effectively reduce work-related stress, it is important not only to know the relevant associations between leaders and their employees, but also the extent of work-related stress at various management levels.13 Previous study results revealed higher levels of demands at work, as well as higher degrees of control in decision-making, freedom at work and possibilities for development among leaders.14, 15 In addition, studies have shown that leaders experienced fewer burnout-symptoms as well as an improvement in perceived health status, in comparison to the colleagues they manage.13, 16 However, little has been
Chapter 4
88
published regarding the extent of work-related stress among health professionals working at different hierarchical levels.17, 18
Therefore, this study aimed to investigate the extent of stress at work (stressors, stress reactions, long-term consequences) for health professionals working in upper-, middle- and lower-management positions, along with those not working in management positions in Swiss hospitals, nursing homes and home care organisations.
3. Methods
3.1 Design This was a prospective, cross-sectional study conducted in Swiss acute care hospitals, rehabilitation and psychiatric hospitals, nursing homes and home care organisations. The study is part of the national STRAIN project, ‘work-related stress among health professionals in Switzerland’. The results presented in this study are based on the STRAIN baseline-measurement, which took place between September 2017 and March 2018. The STRAIN project consists of a cluster randomised clinical trial (Clinical Trials registration: NCT03508596), and is based on three measurements (baseline, first and second). It also includes an intervention consisting of a two-day education program for health professional leaders between the first and second measurement.
3.2 Recruitment of healthcare organisations Healthcare organisations were randomly selected from all hospitals, nursing homes, and home care organisations registered from the Swiss Federal Statistical Office in 2016. Organisations which were too small (average number of beds < 20, fewer than 7 employees), or which were specialised (e.g. in gynaecology or neonatology), were excluded. Computer-based randomisation (randomizer.org) was conducted, and a total of 100 hospitals (acute, rehabilitation and psychiatric), 100 nursing homes and 100 home care organisations were invited to participate. Consideration was also given to ensuring a geographically representative sample for Switzerland (69% Swiss or Standard German-speaking, 23% French-speaking, 8% Italian-speaking).
The recruitment process initially consisted of providing the randomly selected organisations with information about the study by email or telephone. Afterwards, a flyer and a short film containing information about the study were sent directly to the CEO or the head of Human Resources. A total of 36 acute care, rehabilitation or psychiatric hospitals (23 German-speaking, 12 French-speaking, 1 Italian-speaking) took part in this study. Additionally, 86 nursing homes (56 German-speaking, 24 French-speaking, 6 Italian-speaking) and 41
Chapter 4
89
home care organisations (36 German-speaking, 3 French-speaking, 2 Italian-speaking) participated.
3.3 Study sample and management-levels The study included health professionals from several disciplines working in acute care hospitals, rehabilitation or psychiatric hospitals, nursing homes or home care organisations in Switzerland. The study sample consisted of nursing staff and midwives, physicians, medical-technical and medical-therapeutic professionals at all hierarchical levels. The term ‘hierarchical levels’ in regard to management denotes that power or authority is delegated downwards, since leaders at a higher level have a greater scope of responsibility.19 Accordingly, the management levels for this study are divided as follows:
- upper-management level (e.g. directors, hospital directors, clinic directors) - middle-management level (e.g. divisional managers, senior or leading
physicians) - lower-management level (e.g. team leaders, ward managers) - health professionals without management responsibilities (e.g. registered
nurses, physicians, physiotherapists).
3.4 Data collection Data was collected using both an online version of the questionnaire (employees with or without a personal email-address) and a written version available in German, French and Italian. A contact person for each organisation was involved in the distribution of the questionnaire within their organisation and ensured that it was available to all health professionals. Participation by the organisations as well as health professionals was on a voluntary basis. They also received a reminder email or postcard two weeks later. Healthcare employees could complete the questionnaire between September 2017 and March 2018. The questionnaire required 20-45 minutes to complete.
3.5 Ethics The local Swiss ethical board in Bern confirmed that the study does not warrant a full ethical application and does not fall under the Swiss Federal Act on Research Involving Human Beings (Req-2016-00616). The study was on a voluntary basis for all organisations and health professionals participating; all participants were free to stop filling out the questionnaire at any time.

Chapter 4
90
3.6 Questionnaire In the questionnaire, one section focused on identifying the hierarchical level of the participants and their manager-to-staff ratio. The STRAIN questionnaire was utilised to assess the extent of stressors at work (e.g. demands, role clarity, influence) and stress reactions (e.g. behavioural stress reactions), including their long-term consequences (e.g. burnout-symptoms, intention to leave). The STRAIN questionnaire is based on the theoretical background of ‘causes and consequences of work-related stress’ from Eurofound5. Therefore, the questionnaire is divided into scales assessing stressors at work (demands at work, work organisation and job content, work-individual interface, social relations and leadership, and home-work interface), employees’ stress reactions and long-term consequences (job satisfaction, intention to leave and health-related outcomes). It consists of well-established, valid and reliable scales from the Copenhagen Psychosocial Questionnaire (COPSOQ)20, 21, the questionnaire used in the ‘Nurses Early Exit Study’ (NEXT)22, the Sixth European Working Conditions Survey - EWCS23, the self-rated general health status using EQ-5D-5L24, the Work-Ability Index (WAI)25 and the Inability due to Spine Complaints26. More information on the STRAIN questionnaire was published in Golz, Peter and Hahn.27
3.7 Data analysis Data was analysed using SPSS 25®. All Items from the COPSOQ, EWCS and NEXT were transformed to having a value range from 0 (minimum value) to 100 points (maximum value) according to.20, 23 If fewer than half of the questions in a scale had been answered, no average score was calculated.20 Further, the index for WAI and the score on the Inability due to spine complaints were calculated according the original authors’ method.25, 26 Data analysis for the different management levels was performed using multiple linear regression analysis. A separate regression model was calculated using each scale (e.g. quantitative demands) as a dependent variable. Multicollinearity between the estimated regression coefficients was tested using the variance inflation factor (VIF) in each regression model. The four hierarchical levels, along with gender (male, female) and setting (acute care, rehabilitation and psychiatric hospitals, nursing homes, home care organisations), were used as dummy-coded independent variables. Hierarchical levels were the independent variable of interest, whilst gender and setting served as control variables, since previous study results determined branch/organisational and gender differences on different levels in working life.14,
28 The dummy coding was organised so that the sum of the estimated coefficients was equal to zero (sum to zero contrasts) for each independent variable. The intercept (constant) of the model can be interpreted as an unweighted mean value of the independent variable, given the regression adjustment.

Chapter 4
91
4. Results
4.1 Study sample description A total of 8,112 health professionals participated in the study, with 84% from the German-speaking, 14% from the French-speaking and 2% from the Italian-speaking region of Switzerland. The overall response rate of participants was 43% (acute care, rehabilitation or psychiatric hospitals: 37%, nursing homes: 52%, home care organisations: 40%). A total of 42% of participating health professionals worked in acute or rehabilitation hospitals, 26% in psychiatric hospitals, 21% in nursing homes and 11% in home care organisations (see Table 1). Most participants were female (82%), the mean age of the same was 42 years (SD=12) and the mean years of professional experience was 17 (SD=11). Health professionals included nurses and midwives (75%), medical-therapeutic professionals (9%), or physicians (7%), and many of them were highly educated (68% had a higher vocational training and above). Regarding the different hierarchical levels, 83% of the participating healthcare employees had no management responsibilities, while 11% of them worked at the lower-management level, 4% at the middle-management level and 2% at the upper-management level. Among all leaders, the manager-to-staff ratio for direct subordinate employees was 12 (median) and for overall subordinate employees 19 (median).
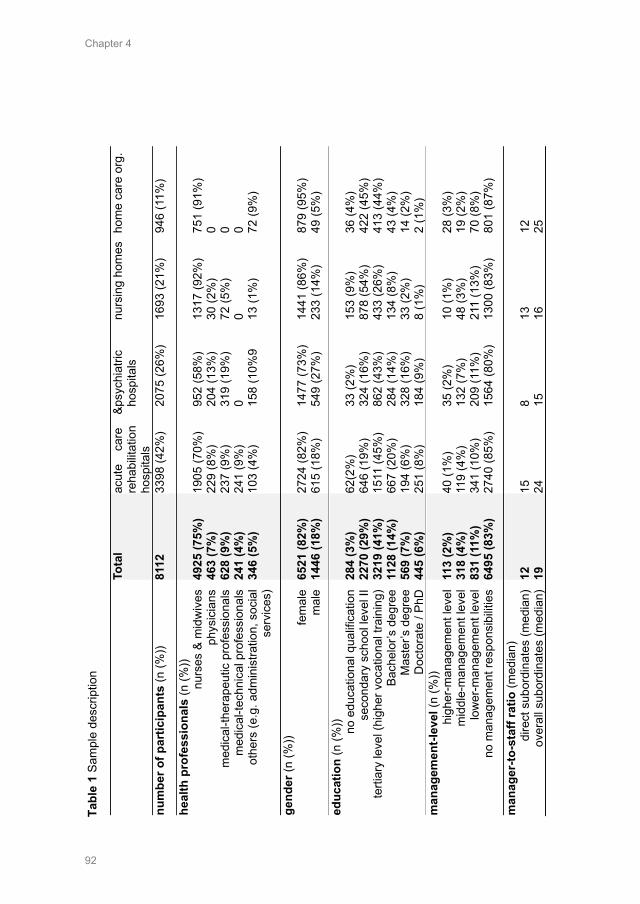
Chapter 4
92
To
tal
acut
e ca
re
& re
habi
litat
ion
hosp
itals
psyc
hiat
ric
hosp
itals
nu
rsin
g ho
mes
ho
me
care
org
.
num
ber o
f par
ticip
ants
(n (%
)) 81
12
3398
(42%
) 20
75 (2
6%)
1693
(21%
) 94
6 (1
1%)
heal
th p
rofe
ssio
nals
(n (%
)) nu
rses
& m
idw
ives
ph
ysic
ians
m
edic
al-th
erap
eutic
pro
fess
iona
ls
med
ical
-tech
nica
l pro
fess
iona
ls
othe
rs (e
.g. a
dmin
istra
tion,
soc
ial
serv
ices
)
4925
(75%
) 46
3 (7
%)
628
(9%
) 24
1 (4
%)
346
(5%
)
1905
(70%
) 22
9 (8
%)
237
(9%
) 24
1 (9
%)
103
(4%
)
952
(58%
) 20
4 (1
3%)
319
(19%
) 0 15
8 (1
0%9
1317
(92%
) 30
(2%
) 72
(5%
) 0 13
(1%
)
751
(91%
) 0 0 0 72
(9%
)
gend
er (n
(%))
fem
ale
mal
e
6521
(82%
) 14
46 (1
8%)
2724
(82%
) 61
5 (1
8%)
1477
(73%
) 54
9 (2
7%)
1441
(86%
) 23
3 (1
4%)
879
(95%
) 49
(5%
)
educ
atio
n (n
(%)) no e
duca
tiona
l qua
lific
atio
n se
cond
ary
scho
ol le
vel I
I te
rtiar
y le
vel (
high
er v
ocat
iona
l tra
inin
g)
Bach
elor
’s d
egre
e M
aste
r’s d
egre
e D
octo
rate
/ Ph
D
284
(3%
) 22
70 (2
9%)
3219
(41%
) 11
28 (1
4%)
569
(7%
) 44
5 (6
%)
62(2
%)
646
(19%
) 15
11 (4
5%)
667
(20%
) 19
4 (6
%)
251
(8%
)
33 (2
%)
324
(16%
) 86
2 (4
3%)
284
(14%
) 32
8 (1
6%)
184
(9%
)
153
(9%
) 87
8 (5
4%)
433
(26%
) 13
4 (8
%)
33 (2
%)
8 (1
%)
36 (4
%)
422
(45%
) 41
3 (4
4%)
43 (4
%)
14 (2
%)
2 (1
%)
man
agem
ent-l
evel
(n (%
)) hi
gher
-man
agem
ent l
evel
m
iddl
e-m
anag
emen
t lev
el
low
er-m
anag
emen
t lev
el
no m
anag
emen
t res
pons
ibilit
ies
113
(2%
) 31
8 (4
%)
831
(11%
) 64
95 (8
3%)
40 (1
%)
119
(4%
) 34
1 (1
0%)
2740
(85%
)
35 (2
%)
132
(7%
) 20
9 (1
1%)
1564
(80%
)
10 (1
%)
48 (3
%)
211
(13%
) 13
00 (8
3%)
28 (3
%)
19 (2
%)
70 (8
%)
801
(87%
)
man
ager
-to-s
taff
ratio
(med
ian)
di
rect
sub
ordi
nate
s (m
edia
n)
over
all s
ubor
dina
tes
(med
ian)
12
19
15
24
8 15
13
16
12
25
Tabl
e 1
Sam
ple
desc
riptio
n
Chapter 4
93
4.2 Results on stress at work at different management levels Results of the multiple linear regression analysis are presented in Tables 2 and 3. Table 2 presents the results from the four hierarchical levels for demands at work, work organisation and job content, work-individual interface and social relations, and leadership. In Table 3, further results regarding home-work interface, stress reaction and long-term consequences are shown.
4.2.1 Demands at work Results revealed significantly higher reported quantitative demands (e.g. working at a high pace, overtime) among leaders in the upper- (M=66.02, B=5.60, p<0.001) and middle-management positions (M=63.87, B=3.44, p<0.001), than among health professionals without management responsibility (M=51.73, B=-8.70, p<0.001). Also, significantly higher cognitive demands at work (e.g. knowledge required, remembering multiple things, making quick decisions) were identified for health professional leaders’ working in upper- (M=81.25, B=4.54, p<0.001) and middle-management (M=78.83.25, B=2.12, p<0.01) than for employees without management responsibilities (M=70.45, B=-6.26, p<0.001). In contrast, health professionals without management responsibilities (M=82.49, B=3.78, p<0.001) or in lower-management positions (M=81.56, B=2.85, p<0.001) reported higher sensory demands (e.g. precision, vision, attention) than leaders in upper-management positions (M=72.73, B=-5.98, p<0.001). Also, physical demands (e.g. tiring or painful body positions, lifting or moving people/heavy loads) were significantly higher among health professionals without management responsibilities (M=37.53, B=8.08, p<0.001) or in lower-management (M=33.24, B=3.80, p<0.001) than among leaders in middle- (M=25.10, B=-4.35, p<0.001) and upper- (M=21.91, B=-7.53, p<0.001) management. In addition, higher demands regarding work environment (e.g. noise, chemicals, extreme temperatures, risk of infection) were also reported by employees without management responsibilities (M=33.97, B=7.14, p<0.001) or in lower-management (M=32.88, B=6.06, p<0.001) than by employees in middle- (M=22.74, B=-4.08, p<0.001) and upper-management (M=17.71, B=-9.12, p<0.001). Employees without management responsibilities also reported having higher emotional demands (e.g. confrontation with death, suffering, aggressive patients) (M=60.85, B=3.12, p<0.001) and having to hide their emotions more (M=40.01, B=2.81, p<0.001) than employees working in the upper-management level.
4.2.2 Work organisation and job content Results on work organisation and content, revealed that leaders at an upper-management level had significantly higher opportunities for development (M=85.17, B=7.42, p<0.001) and influence at work (e.g. degree of influence concerning work, amount of work, duties) (M=73.36, B=11.11, p<0.001) than
Chapter 4
94
health professionals without management responsibilities. Further, results showed a greater influence on breaks and holidays among leaders in upper- (M=75.95, B=5.31, p<0.001) and middle-management positions (M=74.83, B=4.19, p<0.001) than employees without a management position (M=61.30, B=-9.33, p<0.001). Leaders in upper-management perceived their work as being more meaningful (M=88.24, B=2.46, p<0.05) and as having more of a bond with the organisation (M=72.34, B=5.26, p<0.01) than employees without management responsibilities.
4.2.3 Work-individual interface Heath professionals without a management position reported having a higher level of job insecurity (e.g. worried about becoming unemployed) (M=19.75, B=5.02, p<0.001) as well as insecurity regarding their work environment (e.g. unforeseen changes in shift schedules, working times) (M=31.60, B=8.93, p<0.001) than did health professionals working in an upper-management position.
4.2.4 Social relations and leadership Results on social relations and leadership indicated higher levels of predictability at work (e.g. being informed in advance about important decisions, changes or plans) for leaders in upper-management positions (M=74.02, B=6.89, p<0.001) than for employees working in lower management (M=64.43, B=-2.71, p<0.001) or without a management position (M=64.11, B=-3.02, p<0.001). Furthermore, leaders in upper- (M=69.59, B=4.89, p<0.05) and middle-management positions (M=67.60, B=2.90, p<0.05) reported receiving more rewards at work than employees without a leading position (M=57.72, B=-6.98, p<0.001). Role clarity (e.g. clear work tasks, objectives, expectations and areas of responsibility) was lowest among leaders in middle-management positions (M=76.42, B=-1.58, p<0.05); however, it was highest among leaders in upper-management positions (M=81.19, B=3.19, p<0.01). The perceived quality of leadership regarding one’s leader (M=64.67, B=-2.17, p<0.01) and the feedback one received (M=50.08, B=-2.65, p<0.001) was lowest among employees without management responsibilities. Moreover, social relations (e.g. possibility to talk to colleagues during work) were revealed as being the lowest among leaders in middle-management positions (M=56.52, B=-3.58, p<0.01), and highest among those in upper-management positions (M=64.62, B=4.52, p<0.05). However, health professionals without management responsibilities reported experiencing unfair behaviour more often (M=13.97, B=2.51, p<0.001) than health professionals working at the upper-management level (M=7.74, B=-3.72, p<0.05).
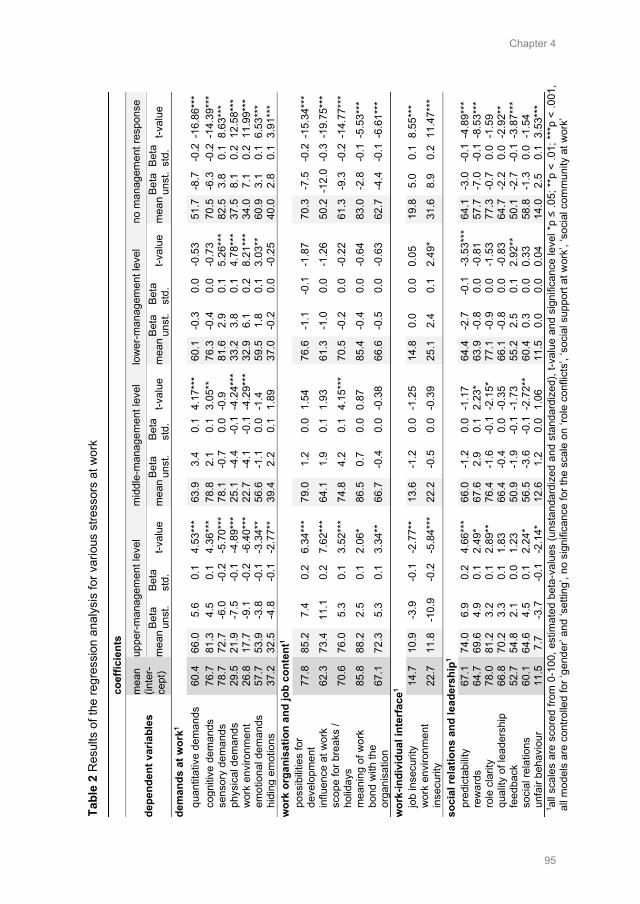
Chapter 4
95
Ta
ble
2 R
esul
ts o
f the
regr
essi
on a
naly
sis
for v
ario
us s
tress
ors
at w
ork
co
effic
ient
s
depe
nden
t var
iabl
es
mea
n (in
ter-
cept
)
uppe
r-man
agem
ent l
evel
m
iddl
e-m
anag
emen
t lev
el
low
er-m
anag
emen
t lev
el
no m
anag
emen
t res
pons
e
mea
n Be
ta
unst
. Be
ta
std.
t-v
alue
m
ean
Beta
un
st.
Beta
st
d.
t-val
ue
mea
n Be
ta
unst
. Be
ta
std.
t-v
alue
m
ean
Beta
un
st.
Beta
st
d.
t-val
ue
dem
ands
at w
ork1
quan
titat
ive
dem
ands
60
.4
66.0
5.
6 0.
1 4.
53**
* 63
.9
3.4
0.1
4.17
***
60.1
-0
.3
0.0
-0.5
3 51
.7
-8.7
-0
.2 -
16.8
6***
co
gniti
ve d
eman
ds
76.7
81
.3
4.5
0.1
4.36
***
78.8
2.
1 0.
1 3.
05**
76
.3
-0.4
0.
0 -0
.73
70.5
-6
.3
-0.2
-14
.39*
**
sens
ory
dem
ands
78
.7
72.7
-6
.0
-0.2
-5
.70*
**
78.1
-0
.7
0.0
-0.9
81
.6
2.9
0.1
5.26
***
82.5
3.
8 0.
1 8.
63**
* ph
ysic
al d
eman
ds
29.5
21
.9
-7.5
-0
.1
-4.8
9***
25
.1
-4.4
-0
.1 -
4.24
***
33.2
3.
8 0.
1 4.
78**
* 37
.5
8.1
0.2
12.5
8***
w
ork
envi
ronm
ent
26.8
17
.7
-9.1
-0
.2
-6.4
0***
22
.7
-4.1
-0
.1 -
4.29
***
32.9
6.
1 0.
2 8.
21**
* 34
.0
7.1
0.2
11.9
9***
em
otio
nal d
eman
ds
57.7
53
.9
-3.8
-0
.1
-3.3
4**
56.6
-1
.1
0.0
-1.4
59
.5
1.8
0.1
3.03
**
60.9
3.
1 0.
1 6.
53**
* hi
ding
em
otio
ns
37.2
32
.5
-4.8
-0
.1
-2.7
7**
39.4
2.
2 0.
1 1.
89
37.0
-0
.2
0.0
-0.2
5 40
.0
2.8
0.1
3.91
***
wor
k or
gani
satio
n an
d jo
b co
nten
t1 po
ssib
ilitie
s fo
r de
velo
pmen
t 77
.8
85.2
7.
4 0.
2 6.
34**
* 79
.0
1.2
0.0
1.54
76
.6
-1.1
-0
.1
-1.8
7 70
.3
-7.5
-0
.2 -
15.3
4***
influ
ence
at w
ork
62.3
73
.4
11.1
0.
2 7.
62**
* 64
.1
1.9
0.1
1.93
61
.3
-1.0
0.
0 -1
.26
50.2
-12
.0 -
0.3
-19.
75**
* sc
ope
for b
reak
s /
holid
ays
70.6
76
.0
5.3
0.1
3.52
***
74.8
4.
2 0.
1 4.
15**
* 70
.5
-0.2
0.
0 -0
.22
61.3
-9
.3
-0.2
-14
.77*
**
mea
ning
of w
ork
85.8
88
.2
2.5
0.1
2.06
* 86
.5
0.7
0.0
0.87
85
.4
-0.4
0.
0 -0
.64
83.0
-2
.8
-0.1
-5.
53**
* bo
nd w
ith th
e or
gani
satio
n 67
.1
72.3
5.
3 0.
1 3.
34**
66
.7
-0.4
0.
0 -0
.38
66.6
-0
.5
0.0
-0.6
3 62
.7
-4.4
-0
.1 -
6.61
***
wor
k-in
divi
dual
inte
rfac
e1 jo
b in
secu
rity
14.7
10
.9
-3.9
-0
.1
-2.7
7**
13.6
-1
.2
0.0
-1.2
5 14
.8
0.0
0.0
0.05
19
.8
5.0
0.1
8.55
***
wor
k en
viro
nmen
t in
secu
rity
22.7
11
.8
-10.
9 -0
.2
-5.8
4***
22
.2
-0.5
0.
0 -0
.39
25.1
2.
4 0.
1 2.
49*
31.6
8.
9 0.
2 11
.47*
**
soci
al re
latio
ns a
nd le
ader
ship
1 pr
edic
tabi
lity
67.1
74
.0
6.9
0.2
4.66
***
66.0
-1
.2
0.0
-1.1
7 64
.4
-2.7
-0
.1
-3.5
3***
64
.1
-3.0
-0
.1 -
4.89
***
rew
ards
64
.7
69.6
4.
9 0.
1 2.
49*
67.6
2.
9 0.
1 2.
23*
63.9
-0
.8
0.0
-0.8
1 57
.7
-7.0
-0
.1 -
8.53
***
role
cla
rity
78.0
81
.2
3.2
0.1
2.89
**
76.4
-1
.6
-0.1
-2.
15*
77.1
-0
.9
0.0
-1.5
3 77
.3
-0.7
0.
0 -1
.59
qual
ity o
f lea
ders
hip
66.8
70
.2
3.3
0.1
1.83
66
.4
-0.4
0.
0 -0
.35
66.1
-0
.8
0.0
-0.8
3 64
.7
-2.2
0.
0 -2
.92*
* fe
edba
ck
52.7
54
.8
2.1
0.0
1.23
50
.9
-1.9
-0
.1 -
1.73
55
.2
2.5
0.1
2.92
**
50.1
-2
.7
-0.1
-3.
87**
* so
cial
rela
tions
60
.1
64.6
4.
5 0.
1 2.
24*
56.5
-3
.6
-0.1
-2.
72**
60
.4
0.3
0.0
0.33
58
.8
-1.3
0.
0 -1
.54
unfa
ir be
havi
our
11.5
7.
7 -3
.7
-0.1
-2
.14*
12
.6
1.2
0.0
1.06
11
.5
0.0
0.0
0.04
14
.0
2.5
0.1
3.53
***
1 all
scal
es a
re s
core
d fro
m 0
-100
, est
imat
ed b
eta-
valu
es (u
nsta
ndar
dize
d an
d st
anda
rdiz
ed),
t-val
ue a
nd s
igni
fican
ce le
vel *
p ≤
.05;
**p
< .0
1; *
**p
< .0
01,
all m
odel
s ar
e co
ntro
lled
for ‘
gend
er’ a
nd ‘s
ettin
g’, n
o si
gnifi
canc
e fo
r the
sca
le o
n ‘ro
le c
onfli
cts’
, ‘so
cial
sup
port
at w
ork’
, ‘so
cial
com
mun
ity a
t wor
k’
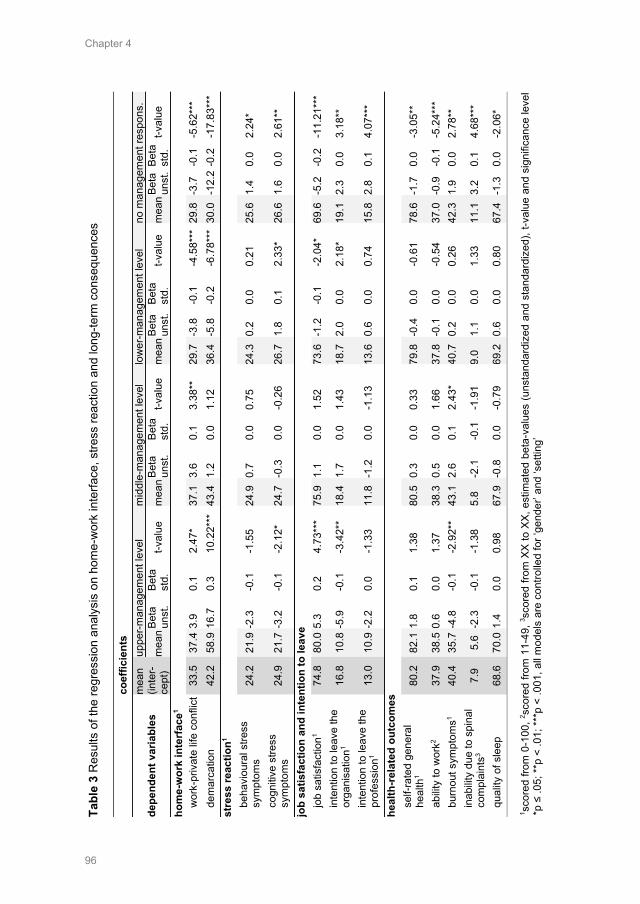
Chapter 4
96
Ta
ble
3 R
esul
ts o
f the
regr
essi
on a
naly
sis
on h
ome-
wor
k in
terfa
ce, s
tress
reac
tion
and
long
-term
con
sequ
ence
s
coef
ficie
nts
depe
nden
t var
iabl
es
mea
n (in
ter-
cept
)
uppe
r-man
agem
ent l
evel
m
iddl
e-m
anag
emen
t lev
el
low
er-m
anag
emen
t lev
el
no m
anag
emen
t res
pons
.
mea
n Be
ta
unst
. Be
ta
std.
t-v
alue
m
ean
Beta
un
st.
Beta
st
d.
t-val
ue
mea
n Be
ta
unst
. Be
ta
std.
t-v
alue
m
ean
Beta
un
st.
Beta
st
d.
t-val
ue
hom
e-w
ork
inte
rfac
e1 w
ork-
priv
ate
life
conf
lict
33.5
37
.4 3
.9
0.1
2.47
* 37
.1
3.6
0.1
3.38
**
29.7
-3
.8
-0.1
-4
.58*
** 2
9.8
-3.7
-0
.1
-5.6
2***
de
mar
catio
n 42
.2
58.9
16.
7 0.
3 10
.22*
**
43.4
1.
2 0.
0 1.
12
36.4
-5
.8
-0.2
-6
.78*
** 3
0.0
-12.
2 -0
.2
-17.
83**
* st
ress
reac
tion1
beha
viou
ral s
tress
sy
mpt
oms
24.2
21
.9 -
2.3
-0.1
-1
.55
24.9
0.
7 0.
0 0.
75
24.3
0.
2 0.
0 0.
21
25.6
1.
4 0.
0 2.
24*
cogn
itive
stre
ss
sym
ptom
s 24
.9
21.7
-3.
2 -0
.1
-2.1
2*
24.7
-0
.3
0.0
-0.2
6 26
.7
1.8
0.1
2.33
* 26
.6
1.6
0.0
2.61
**
job
satis
fact
ion
and
inte
ntio
n to
leav
e jo
b sa
tisfa
ctio
n1 74
.8
80.0
5.3
0.
2 4.
73**
* 75
.9
1.1
0.0
1.52
73
.6
-1.2
-0
.1
-2.0
4*
69.6
-5
.2
-0.2
-1
1.21
***
inte
ntio
n to
leav
e th
e or
gani
satio
n1 16
.8
10.8
-5.
9 -0
.1
-3.4
2**
18.4
1.
7 0.
0 1.
43
18.7
2.
0 0.
0 2.
18*
19.1
2.
3 0.
0 3.
18**
inte
ntio
n to
leav
e th
e pr
ofes
sion
1 13
.0
10.9
-2.
2 0.
0 -1
.33
11.8
-1
.2
0.0
-1.1
3 13
.6
0.6
0.0
0.74
15
.8
2.8
0.1
4.07
***
heal
th-r
elat
ed o
utco
mes
se
lf-ra
ted
gene
ral
heal
th1
80.2
82
.1 1
.8
0.1
1.38
80
.5
0.3
0.0
0.33
79
.8
-0.4
0.
0 -0
.61
78.6
-1
.7
0.0
-3.0
5**
abilit
y to
wor
k2 37
.9
38.5
0.6
0.
0 1.
37
38.3
0.
5 0.
0 1.
66
37.8
-0
.1
0.0
-0.5
4 37
.0
-0.9
-0
.1
-5.2
4***
bu
rnou
t sym
ptom
s1 40
.4
35.7
-4.
8 -0
.1
-2.9
2**
43.1
2.
6 0.
1 2.
43*
40.7
0.
2 0.
0 0.
26
42.3
1.
9 0.
0 2.
78**
in
abilit
y du
e to
spi
nal
com
plai
nts3
7.9
5.6
-2.3
-0
.1
-1.3
8 5.
8 -2
.1
-0.1
-1
.91
9.0
1.1
0.0
1.33
11
.1
3.2
0.1
4.68
***
qual
ity o
f sle
ep
68.6
70
.0 1
.4
0.0
0.98
67
.9
-0.8
0.
0 -0
.79
69.2
0.
6 0.
0 0.
80
67.4
-1
.3
0.0
-2.0
6*
1 sco
red
from
0-1
00, 2 s
core
d fro
m 1
1-49
, 3 sco
red
from
XX
to X
X, e
stim
ated
bet
a-va
lues
(uns
tand
ardi
zed
and
stan
dard
ized
), t-v
alue
and
sig
nific
ance
leve
l *p
≤ .0
5; **
p <
.01;
***p
< .0
01, a
ll m
odel
s ar
e co
ntro
lled
for ‘
gend
er’ a
nd ‘s
ettin
g’
Chapter 4
97
4.2.5 Home-work interface Work-private life conflicts were reported more often by health professionals working at upper- (M=37.41, B=3.92, p<0.05) and middle-management levels (M=37.05, B=3.57, p<0.01) than from health professionals working at lower-management levels (M=29.72, B=-3.76, p<0.001) or without management responsibilities (M=29.77, B=-3.72, p<0.001). Difficulties with demarcation (e.g. being available for work issues during leisure time) were also significantly higher among leaders in upper-management positions (M=58.88, B=16.71, p<0.001) than among employees in lower-management positions (M=36.43, B=-5.75, p<0.001) or those without management responsibilities (M=29.99, B=-12.18, p<0.001).
4.2.6 Stress reaction Results on behavioural stress symptoms (e.g. lack of time for relaxation or leisure) revealed that health professionals not working in a management position were more strongly affected (M=25.57, B=1.40, p<0.05). Also, more cognitive stress symptoms were identified for health professionals working in a lower-management position (M=26.74, B=1.81, p<0.05) or non-management position (M=26.57, B=1.64, p<0.01).
4.2.7 Job satisfaction and intention to leave Results on health professionals’ job satisfaction showed the highest levels among leaders working in upper-management positions (M=80.00, B=5.25, p<0.001). Lower levels of satisfaction were reported for employees working in lower-management positions (M=73.58, B=-1.17, p<0.05) or for those in a non-management position (M=69.55, B=-5.20, p<0.001). Moreover, health professionals’ intention to leave was lower when working in upper management (M=10.82, B=-5.94, p<0.01) and higher when working in lower management (M=18.73, B=1.97, p<0.05) or with no management responsibilities (M=19.08, B=2.32, p<0.01). Health professionals’ intention to leave their profession was also higher among employees without management responsibilities (M=15.77, B=2.75, p<0.001).
4.2.8 Health-related outcomes Health professionals working in a non-management position had the lowest ratings on both their general health status (M=78.55, B=-1.69, p<0.01) and work ability (M=37.01, B=-0.89, p<0.001). However, severe burnout symptoms were reported by health professionals working in middle-management positions (M=43.07, B=2.64, p<0.05) and no management responsibilities (M=42.32, B=1.89, p<0.01). Symptoms of burnout were less prevalent among leaders at upper-management levels (M=35.68, B=-4.75, p<0.01). Moreover, more
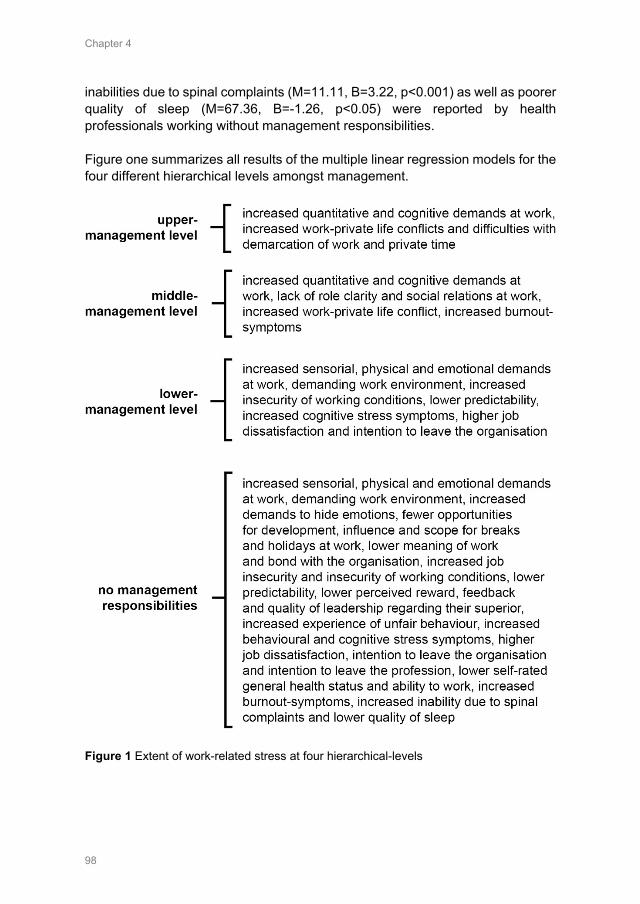
Chapter 4
98
inabilities due to spinal complaints (M=11.11, B=3.22, p<0.001) as well as poorer quality of sleep (M=67.36, B=-1.26, p<0.05) were reported by health professionals working without management responsibilities. Figure one summarizes all results of the multiple linear regression models for the four different hierarchical levels amongst management.
Figure 1 Extent of work-related stress at four hierarchical-levels
Chapter 4
99
5. Discussion
This study presents important results on the extent of work-related stress among Swiss health professionals working at four different management levels. The main finding indicates that work stressors, along with their long-term consequences, are experienced to a larger extent among health professionals at lower-management levels, and especially among those without management responsibilities. This overall tendency corroborates previous study results15, and might be explained by the fact that leaders reported having a higher degree of control and, in general, had a more positive perception of their working conditions than did their employees.
In particular, some individual stressors and long-term consequences were pronounced at certain management levels. The main findings on health professionals working in upper-management positions revealed severe quantitative demands at work, work-private life conflicts and difficulties with work/life demarcation. Among health professionals in middle-management positions, severe work-private life conflicts and quantitative demands, lack of role clarity, poor social relations at work and severe burnout-symptoms were pronounced. Health professionals working in lower-management positions experienced significantly greater physical and emotional demands, less predictability at work, more severe stress symptoms, and higher job dissatisfaction and intention to leave the organisation. Additionally, health professionals working without management responsibilities appeared to have the poorest working conditions, job satisfaction and health-related outcomes. They reported being affected by higher demands at work (physical, emotional, having to hide emotions), fewer possibilities for development, a lack of influence and predictability, fewer rewards, a lack of feedback and a lack of quality leadership. In addition, decreased job satisfaction, the intention to leave, burnout-symptoms, inability to work due to back pain, reduced quality of sleep as well as a lower self-rated general health and work ability were reported.
Previous study results also identified severe work-private life conflicts for leaders working in higher-management positions, although they had a higher degree of authority relating to decision-making and more control and flexibility in comparison to their employees.13, 14, 29 Moreover, previous results indicated higher levels of demands and conflicts at work among leaders.15, 17 With regard to the extent of demands at work among leaders in upper- and middle-management positions, the results of this study corroborate those of previous studies concerning the severe workload.15 However, they do not match with previous findings regarding high emotional, sensorial and physical demands on upper and middle management. In contrast, the results of this study showed higher stress scores among health professionals working in lower- or non-management positions. In addition, contradictory results were found regarding

Chapter 4
100
leaders’ perceived managerial support, and support from peers, which were reported as both higher and lower.13, 15, 17
Comparability with other study results is, however, limited, as many studies presented results for managers in total, and did not distinguish between different management levels or different demands at work. Moreover, most potentially comparable studies were conducted among leaders in various industries and are not specific to health professionals. Health professionals are more affected by certain stressors, such as emotional demands in their daily work, which could account for many differences. Moreover, it is clear that surveying different healthcare management levels revealed a poorer working environment among health professionals at the lowest levels. It is also possible that personality factors (e.g. self-confidence) or individual resilience differ among employees at the different management levels, and that leaders may have more personal resources to deal with the various stressors present at work.13, 15
Several studies also indicated that leaders’ behaviour and their leadership style could affect the extent to which their employees perceive stress at work.10,
30, 31 Health professionals in leadership positions not only have a key role in preventing and reducing stress at work but are also role models for their employees. They set an example as to how to deal with stressors at work, or how to develop safe work practices.10 However, the question remains as to how leaders should be aware of and reduce certain stressors at work among their subordinates when they themselves are greatly affected by it (e.g. by severe work-private life conflicts or quantitative demands at work). Therefore, it seems essential that leaders first reduce the most salient stressors in their own field of work and set a good example when it comes to balancing their work and private life or managing the high quantitative demands at work. At the same time, it is essential to enhance the working conditions for health professionals working without management responsibilities. Our study indicates how severely health professionals not working in a management position are affected by stressors at work. It reveals serious consequences for their health and job satisfaction and shows how important it is to implement effective top-down strategies to enhance their conditions at work.
5.1 Strengths and limitations One strength of this study is that it presents its results on four separate management levels, which has not been done in many previous studies (where often only employee vs. manager levels are investigated). This provides a more differentiated picture of the stressors and the consequences of stress at work, revealing the necessity for interventions targeting the management-level as well. In addition, the study focuses exclusively on the healthcare sector with a sufficiently large study sample and does not include participants from different labour segments, as most other studies do. This is advantageous, as it provides

Chapter 4
101
both broad and in-depth results on the topic of stress at work among health professionals in Switzerland. Moreover, the use of sophisticated statistical analysis software allowed relevant results for each hierarchical level to be analysed separately.
The study also has limitations. First, the cross-sectional design does not allow causal conclusions to be drawn. In addition, the results (e.g., working hours) are influenced by Swiss labour law; therefore, results from other countries might differ. Moreover, the study sample is not exactly representative for Switzerland, since the German-speaking part was somewhat overrepresented. Also, participation was fully voluntary for organisations as well as for health professionals, which probably led to a certain selection bias. It is, for example, possible that more health professionals with low job satisfaction participated, which could have led to an overestimation of stress at work. Conversely, some health professionals with a high level of stress may not have filled out the questionnaire due to lack of time, which could have led to an underestimation. These possibilities should be considered when interpreting the results.
6. Conclusions
Our results imply that effective prevention and reduction of stress at work is important at all management levels. However, since individual stressors at work seem to differ markedly between the hierarchical-levels, it is essential to look at each management level separately, in order to develop and implement appropriate interventions. For example, at the upper-management level, interventions to reduce work-private life conflicts would be beneficial. In regard to the middle-management level, an increase in role clarity would be advantageous. At the lower-management level, a reduction in physical and emotional demands on workers would be valuable. Furthermore, our results indicate that in order to effectively enhance the compatibility of health professionals’ work and private lives, there is a need to intervene at the management level. This would facilitate health professionals in leadership positions in being good role models for their employees. Moreover, and perhaps most importantly, since health professionals without management responsibilities seem to be most affected by stress at work, leaders must ensure the reduction of stress among these employees to enhance their ability to function optimally in the healthcare work environment.
Chapter 4
102
Acknowledgements We are very grateful to all organisations and healthcare professionals who participated in this study for sharing their experience and time so generously. Additionally, we thank Dr. Reto Bürgin, who shared his expertise in statistical analysis with us. Conflict of interest “No conflict of interest has been declared by the author(s)”. Funding This study was financially supported by the University of Applied Sciences, Health Division, Bern, Switzerland, and the State Secretariat for Education and Research (SER) of Switzerland. The funders had no influence or control on the planning, conduct, or reporting of the study. Ethics approval and consent to participate The local Swiss ethical board in Bern confirmed that the study does not warrant a full ethical application and does not fall under the Swiss Federal Act on Research Involving Human Beings (Req-2016-00616). The study was on a voluntary basis for all organisations and health professionals participating; all participants were free to stop filling out the questionnaire at any time. Availability of data and materials The raw dataset analysed in the current study is available from the corresponding author (Karin Anne Peter) on reasonable request. Authors' contributions KP and SH: designed the questionnaire and recruited the participating health organizations. KP: collected and analysed the data. RH and JS: made substantial contributions to the interpretation of data and in writing the manuscript. All authors read and approved the final manuscript.
Chapter 4
103
References 1. World Health Organisation. Global strategy on human resources for health: workforce 2030.
Geneva: World Health Organization, 2016. 2. Aiken LH, Sermeus W, Van den Heede K, Sloane DM, Busse R, McKee M, et al. Patient safety,
satisfaction, and quality of hospital care: cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ. 2012;344:e1717. doi:10.1136/bmj.e1717
3. Aiken LH, Sloane DM, Bruyneel L, Van den Heede K, Sermeus W, Consortium RC. Nurses' reports of working conditions and hospital quality of care in 12 countries in Europe. International Journal of Nursing Studies. 2013;50(2):143-153. doi:10.1016/j.ijnurstu.2012.11.009
4. Suadicani P, Olesen K, Bonde JP, Gyntelberg F. Psychosocial work conditions associated with sickness absence among hospital employees. Occupational Medicine. 2014;64(7):503-508. doi:10.1093/occmed/kqu064
5. Eurofound. Work-related stress. Dublin: Eurofound, 2005. 6. Leka S, Jain A. Health impact of psychosocial hazards at work: An overview. Geneva: World
Health Organization, 2010. 7. NIOSH. Exposure to Stress: National Institute for Occupational Safety and Health, 2008. 8. Hämmig O. Explaining burnout and the intention to leave the profession among health
professionals - a cross-sectional study in a hospital setting in Switzerland. BMC Health Service Research. 2018;18(1):785. doi:10.1186/s12913-018-3556-1
9. Skakon J, Nielsen K, Borg V, Guzman J. Are leaders' well-being, behaviours and style associated with the affective well-being of their employees? A systematic review of three decades of research. Work & Stress. 2010;24(2):107-139. doi:10.1080/02678373.2010.495262
10. Kelloway EK, Barling J. Leadership development as an intervention in occupational health psychology. Work and Stress. 2010;24(3):260-279. doi:10.1080/02678373.2010.518441
11. Glasø L, Einarsen S. Experienced affects in leader–subordinate relationships. Scandinavian Journal of Management. 2006;22(1):49-73. doi:10.1016/j.scaman.2005.09.003
12. Kuoppala J, Lamminpaa A, Liira J, Vainio H. Leadership, job well-being, and health effects--a systematic review and a meta-analysis. Journal of Occupational Environment & Medicine. 2008;50(8):904-915. doi:10.1097/JOM.0b013e31817e918d
13. Lundqvist D, Reineholm C, Gustavsson M, Ekberg K. Investigating work conditions and burnout at three hierarchical levels. Journal of Occupational & Environmental Medicine. 2013;55(10):1157-1163. doi:10.1097/JOM.0b013e31829b27df
14. Bernin P, Theorell T. Demand–control–support among female and male managers in eight Swedish companies. Stress and Health. 2001;17:231–243. doi:10.1002/smi.905
15. Skakon J, Kristensen TS, Christensen KB, Lund T, Labriola M. Do managers experience more stress than employees? Results from the Intervention Project on Absence and Well-being (IPAW) study among Danish managers and their employees. Work. 2011;38(2):103-109. doi:10.3233/wor-2011-1112
16. Marmot MG, Stansfeld S, Patel C, North F, Head J, White I, et al. Health inequalities among British civil servants: the Whitehall II study. The Lancet. 1991;337(8754):1387-1393. doi:10.1016/0140-6736(91)93068-K
17. Johansson G, Sandahl C, Hasson D. Role stress among first-line nurse managers and registered nurses - a comparative study. Journal of Nursing Management. 2013;21(3):449-458. doi:10.1111/j.1365-2834.2011.01311.x
18. Haggman-Laitila A, Romppanen J. Outcomes of interventions for nurse leaders' well-being at work: A quantitative systematic review. Journal of advanced nursing. 2018;74(1):34-44. doi:10.1111/jan.13406
19. Thompson J, Buchbinder S, Shanks N. An overview of Healthcare Management. Massachusetts: Jones and Bartlett Publishers, 2012.
20. Kristensen TS, Hannerz H, Høgh A, Borg V. The Copenhagen Psychosocial Questionnaire-a tool for the assessment and improvement ofthe psychosocial work environment. Scandinavian Journal of Work, Environment & Health. 2005;31(6):438-449.
21. Nübling M, Vomstein M, Nolle I, Lindner A, Haug A, Lincke HJ. Deutsche Standard-Version des COPSOQ 2017. Freiburg: FFAW-Freiburger Forschungsstelle für Arbeitswissenschaften GmbH, 2017.
22. Hasselhorn HM, Tackenberg P, Müller H. Working conditions and intent to leave the profession among nursing staff in Europe. Sweden: National Institute for Working Life, 2003.
Chapter 4
104
23. Eurofound. Sixth European Working Conditions Survey - Questionnaire. Luxembourg: Publications Office of the European Union, 2015.
24. Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Quality of Life Research. 2011;20(10):1727-1736. doi:10.1007/s11136-011-9903-x
25. Tuomi K, Ilmarinen J, Jahkola A, Katajarinne L, Tulkki A. Work Ability. 2 ed. Helsinki: Finnish Institute of Occupational Health, 1998.
26. Von Korff M, Ormel J, Keefe FJ, Dworkin SF. Grading the severity of chronic pain. Pain. 1992;50(2):133-149. doi:10.1016/0304-3959(92)90154-4
27. Golz C, Peter KA, Hahn S. Cognitive Pretesting and pretest of the STRAIN questionnaire to elaborate work-related stress of health care staff in Switzerland. International Journal of Health Professions. 2018;5(1):109-120. doi:10.2478/ijhp-2018-0011
28. Eurofound. Working conditions and workers' health. Luxembourg: Publications Office of the European Union, 2019.
29. Kossek E, Lautsch B. Work-Life Flexibility for Whom? Occupational Status and Work-Life Inequality in Upper, Middle, and Lower Level Jobs. Academy of Management Annals. 2017;12:1-76. doi:10.5465/annals.2016.0059
30. Kelloway EK, Turner N, Barling J, Loughlin C. Transformational leadership and employee psychological well-being: The mediating role of employee trust in leadership. Work and Stress. 2012;26(1):39-55. doi:10.1080/02678373.2012.660774
31. Shirey MR. Leadership practices for healthy work environments. Nursing Management. 2017;48(5):42-50. doi:10.1097/01.NUMA.0000515796.79720.e6
Chapter 5
Development and psychometric testing of an observation-based assessment tool focusing work-related stressors among health professionals: the STRAIN -External Observation of work Stressors
Peter KA, Stadelmann E, Schols JMGA, Halfens RJG, Hahn S. Development and psychometric testing of an observation-based assessment tool focusing work-related stressors among health professionals: the STRAIN-External Observation of work Stressors. (accepted in the Journal of Occupational Medicine and Toxicology)

Chapter 5
106
Abstract
Background: Health professionals are especially affected by various stressors in their daily work, such as a high workload, physical and emotional challenges. The aim of this study was to develop and test the validity, reliability and usability of an observation-based instrument designed to assess work stressors in the healthcare sector. Methods: Using a cross sectional design, 110 health professionals were observed during one entire shift by an external observer. Factor analysis was used to test construct validity, Cronbach’s alpha to test internal consistency and correlations using Kendall’s Tau were computed to test for convergent validity. Results: For 9 out of 10 tested scales the results showed a one-factor solution for all observation scales (explained variance ranged from 55.5% to 80.2%), satisfactory reliability (Cronbach’s alpha between .67 and .92), sufficient usability and satisfactory convergent validity. Conclusions: The newly developed STRAIN-EOS, an observation-based assessment tool designed to assess stressors specifically in the healthcare sector, was shown to be potentially useful. However, further refinement and testing is necessary before it can be widely used.
Chapter 5
107
1. Background
Stress at work is becoming increasingly problematic, with one in six European employees reporting chronic stress-related health problems.1 Health professionals are particularly affected by long working hours and high workloads, shift work and consequences for their work-private life, understaffing, emotional demands through confrontation with suffering, death or aggression at work and varying physical challenges.2-4 Stressors at work usually originate in aspects of the design and management of the work, and in the social and organisational contexts. They have a potential for adverse psychological, physical or social outcomes for employees.5 Besides physical and mental health problems, stress can also negatively influence job satisfaction, intention to leave the job and safety at work.6-9
Over the last few decades, various approaches and methods have been developed and used to assess stressors at work. Most notable among these are self-report questionnaires and observation- or situation-based measures10, each of which has its strengths and weaknesses.11 While self-report questionnaires are most commonly used due to their simple, cost-saving application and the possibility of obtaining large data samples, observation-based instruments seem to provide a more independent view of possible stressors at work.12 The most common observational instruments focus on job and task analysis (e.g. work function, tasks), company analysis (company stress diagnosis, e.g. CANEVAS) or are observation-based checklists of work stressors.5, 13
Previous studies have shown that it is not easy to objectively capture stressors in the workplace. Many aspects of strain are difficult to observe, being internal states (e.g. emotional pressure, inability to cope, perceived lack of support) and mental processes.12, 14 Also, associations between objective stressors and the health outcomes of employees are usually weaker than employees’ subjectively assessed stressors.5 In addition, external observers are individuals with their own experiences, perceptions and memories, all of which can contribute to subjective bias.10, 15 It should also be noted that the convergence between different measures of stressors, for example subjectively and objectively assessed stress indicators, is generally rather low, ranging mostly between 10 and 30%.5, 10 Objectively assessed stressors should, therefore, not be seen as ‘the true reality’ but rather as a complement to other measures (e.g. subjectively assessed stressors) providing further insights into the current work situation with an ‘objective’ external view.10 Moreover, external observations can be costly, so that external observers are usually restricted in observation time, which in turn means that only a limited range of working hours/participants can be observed.15 This can result in the observer compensating for any missing data by using predominant information (e.g. the halo-effect) or common stereotypes related to the observer’s interpretation and level of knowledge.10 In addition, the presence of external
Chapter 5
108
observers may influence the behaviour of the employees, e.g. due to personal characteristics of the observer (personal reactivity) or simply because they are being observed (procedural reactivity).15, 16
Observational instruments can also be difficult to apply in the health sector, due to its 24-hour operation or unforeseen events. Health sector studies employing observational methods therefore mostly focus on a specific topic (e.g. workload, teamwork, hierarchies)17-20 using activity and/or work analysis procedures,21, 22 or else apply instruments that have not been developed and tested specifically in the healthcare sector.13 Observation-based assessment tools that focus on various possible stressors in the healthcare sector are however clearly necessary, and can be used as an alternative or complement to commonly used self-assessment tools.
Therefore, the aim of this study was to develop and test a new observation-based assessment tool that more closely fits working conditions in the healthcare setting and is capable of assessing a number of work-related stressors. The newly developed observation-based assessment tool was then tested for its construct validity, reliability, convergent validity and usability in the healthcare sector.
2. Method
2.1 Design This study is part of the national STRAIN project, “work-related stress among health professionals in Switzerland”. The STRAIN project combines data on stress at work from different data sources. First, health professionals’ self-reports regarding work stressors, stress reactions and long-term consequences from more than 160 participating Swiss health organisations using the STRAIN Questionnaire23, 24 have been collected three times (2017/2018, 2019, 2020). Second, parallel to the health professionals’ self-assessments, relevant key figures on work-related stress are collected in the participating organisations (e.g. absenteeism, turnover-rates). Third, external observers were used to provide an additional perspective on work-related stress. Thus, this study aimed to develop and test an observation-based assessment tool using a cross-sectional study design, the psychometric properties of which were tested in the healthcare setting. The observations were conducted by external observers and the assessment instrument was called STRAIN-EOS (STRAIN - External Observation of Work Stressors).

Chapter 5
109
2.2 Development of the STRAIN-EOS assessment tool The STRAIN-EOS was developed (see Figure 1) on the basis of the STRAIN-Questionnaire (employees’ self-reports), using standardised, validated and reliable self-assessment scales which, according to previous studies, are also externally observable.5, 10, 25 Scales were selected from the German version of the Copenhagen Psychosocial Questionnaire26-29 (COPSOQ) and the 6th European Working Conditions Survey30 (EWCS). According to the COPSOQ, scales were selected based on the thematic fields: a) demands at work, b) work organisation and content, and c) social relation and leadership. The demands at work scales included questions on quantitative, sensorial and physical demands with a response option on a five- or seven-point Likert scale. A high score in these scales indicates a high risk for work-related stress. The scales on work organisation and content are based on questions about opportunities for development, influence at work and degree of freedom at work. Response options are on a five-point Likert scale (always to never). A low score in these scales indicates a high risk for work-related stress. The scales in the social relations and leadership group include questions on predictability, social support, social community, rewards, unfair behaviour and on social relations at work. A low score indicates a high risk for work-related stress. The psychometric properties of these self-report scales had shown good reliability (Cronbach’s alpha >0.7) and satisfactory construct and criterion validity in previous testing.29,
31
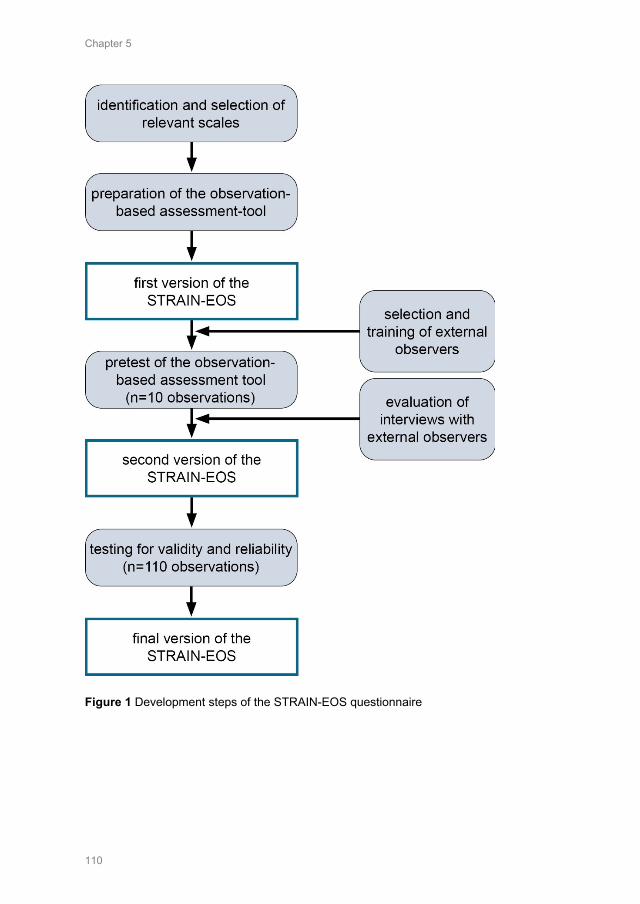
Chapter 5
110
Figure 1 Development steps of the STRAIN-EOS questionnaire

Chapter 5
111
In a second step, the items of each scale were reformulated so that they could be used as an observational assessment instrument and still be comparable with the underlying self-report scales. Therefore, the same number of items were used as in the self-report scales, and care was taken to ensure that the wording in the STRAIN-EOS items were similar to that used in the self-report (e.g. “Does the observed person have to work very fast?”, for external for observers and “Do you have to work very fast?” for self-reports). Furthermore, a few items for the external observers were added, for example the date of observation, the shift observed, area of work, profession and role of the observed person. One additional question concerning the overall perceived workload in the observed shift was added (according to LEP-AG32) to test the reactivity of the observation scales: if an external observer perceived the overall workload as high, this should also result in a higher ranking on observed demand scales. To obtain information about the usability of the STRAIN-EOS, external observers had the opportunity to comment on items (e.g. those which were not observable, difficult to understand). Furthermore, the number of missing values was used as an indication of the STRAIN-EOS’s usability.
In a third step, we pre-tested a first version of the STRAIN-EOS by studying 10 observations in a general hospital setting. The aim was to determine whether all items could be captured by external observers during an entire shift of 9-12 hours. Pre-testing indicated that the two scales on ‘rewards’ and ‘unfair behaviour’ were too difficult to assess (not observable in 3 to 9 of the 10 cases). The item ‘the observed person has to do overtime’ (always – never) of the scale on ‘quantitative demands’ was also not observable during one shift. Since all other items were assessable during one shift, these items were excluded from the STRAIN-EOS. Table 1 presents the resulting STRAIN-EOS.
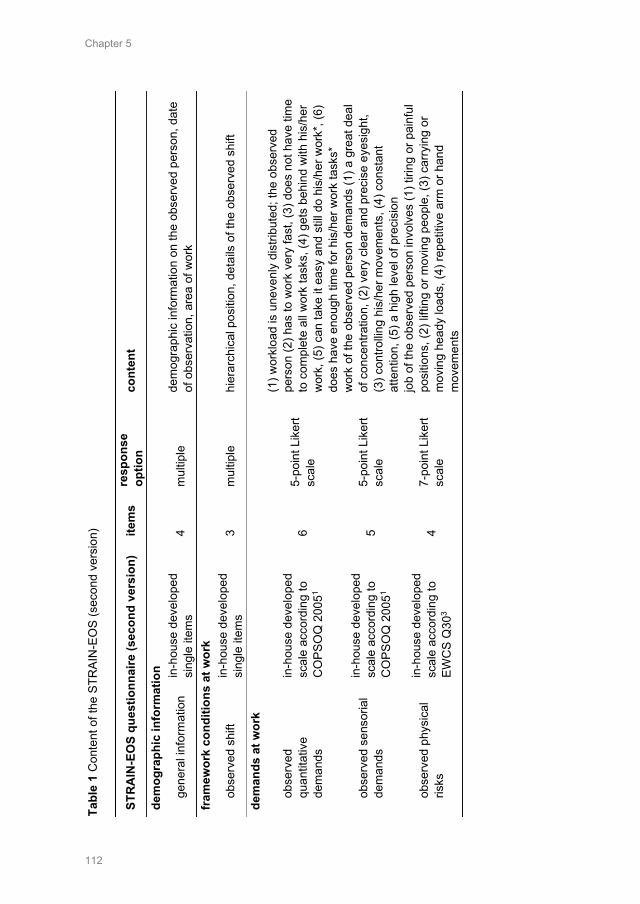
Chapter 5
112
Ta
ble
1 C
onte
nt o
f the
STR
AIN
-EO
S (s
econ
d ve
rsio
n)
STR
AIN
-EO
S qu
estio
nnai
re (s
econ
d ve
rsio
n)
item
s re
spon
se
optio
n co
nten
t
dem
ogra
phic
info
rmat
ion
gene
ral i
nfor
mat
ion
in-h
ouse
dev
elop
ed
sing
le it
ems
4 m
ultip
le
dem
ogra
phic
info
rmat
ion
on th
e ob
serv
ed p
erso
n, d
ate
of o
bser
vatio
n, a
rea
of w
ork
fram
ewor
k co
nditi
ons
at w
ork
obse
rved
shi
ft in
-hou
se d
evel
oped
si
ngle
item
s 3
mul
tiple
hi
erar
chic
al p
ositi
on, d
etai
ls o
f the
obs
erve
d sh
ift
dem
ands
at w
ork
obse
rved
qu
antit
ativ
e de
man
ds
in-h
ouse
dev
elop
ed
scal
e ac
cord
ing
to
CO
PSO
Q 2
0051
6 5-
poin
t Lik
ert
scal
e
(1) w
orkl
oad
is u
neve
nly
dist
ribut
ed; t
he o
bser
ved
pers
on (2
) has
to w
ork
very
fast
, (3)
doe
s no
t hav
e tim
e to
com
plet
e al
l wor
k ta
sks,
(4) g
ets
behi
nd w
ith h
is/h
er
wor
k, (5
) can
take
it e
asy
and
still
do h
is/h
er w
ork*
, (6)
do
es h
ave
enou
gh ti
me
for h
is/h
er w
ork
task
s*
obse
rved
sen
soria
l de
man
ds
in-h
ouse
dev
elop
ed
scal
e ac
cord
ing
to
CO
PSO
Q 2
0051
5 5-
poin
t Lik
ert
scal
e
wor
k of
the
obse
rved
per
son
dem
ands
(1) a
gre
at d
eal
of c
once
ntra
tion,
(2) v
ery
clea
r and
pre
cise
eye
sigh
t, (3
) con
trollin
g hi
s/he
r mov
emen
ts, (
4) c
onst
ant
atte
ntio
n, (5
) a h
igh
leve
l of p
reci
sion
obse
rved
phy
sica
l ris
ks
in-h
ouse
dev
elop
ed
scal
e ac
cord
ing
to
EWC
S Q
303
4 7-
poin
t Lik
ert
scal
e
job
of th
e ob
serv
ed p
erso
n in
volv
es (1
) tiri
ng o
r pai
nful
po
sitio
ns, (
2) li
fting
or m
ovin
g pe
ople
, (3)
car
ryin
g or
m
ovin
g he
ady
load
s, (4
) rep
etiti
ve a
rm o
r han
d m
ovem
ents
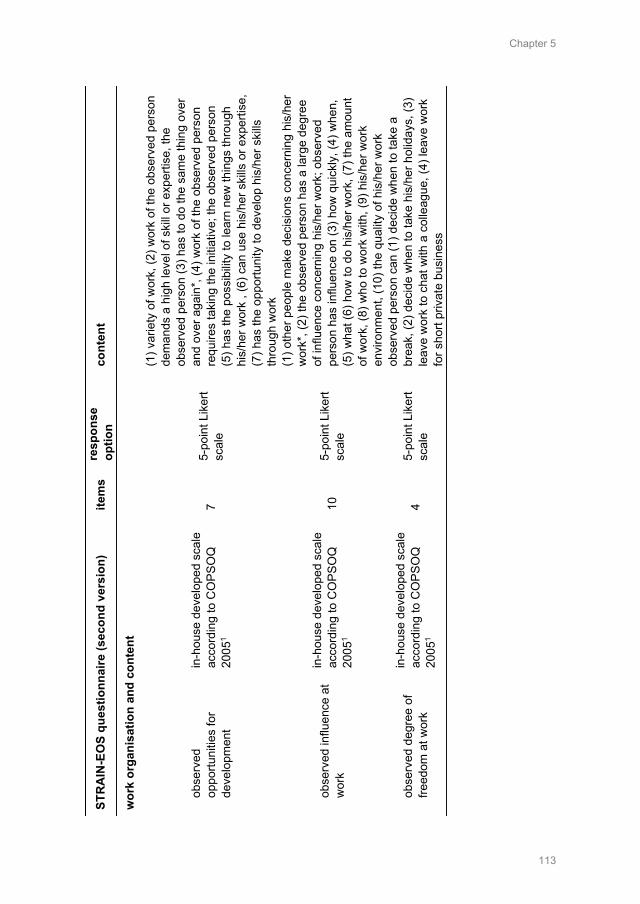
Chapter 5
113
ST
RA
IN-E
OS
ques
tionn
aire
(sec
ond
vers
ion)
ite
ms
resp
onse
op
tion
cont
ent
wor
k or
gani
satio
n an
d co
nten
t
obse
rved
op
portu
nitie
s fo
r de
velo
pmen
t
in-h
ouse
dev
elop
ed s
cale
ac
cord
ing
to C
OPS
OQ
20
051
7 5-
poin
t Lik
ert
scal
e
(1) v
arie
ty o
f wor
k, (2
) wor
k of
the
obse
rved
per
son
dem
ands
a h
igh
leve
l of s
kill
or e
xper
tise,
the
obse
rved
per
son
(3) h
as to
do
the
sam
e th
ing
over
an
d ov
er a
gain
*, (4
) wor
k of
the
obse
rved
per
son
requ
ires
taki
ng th
e in
itiat
ive;
the
obse
rved
per
son
(5) h
as th
e po
ssib
ility
to le
arn
new
thin
gs th
roug
h hi
s/he
r wor
k , (
6) c
an u
se h
is/h
er s
kills
or e
xper
tise,
(7
) has
the
oppo
rtuni
ty to
dev
elop
his
/her
ski
lls
thro
ugh
wor
k
obse
rved
influ
ence
at
wor
k
in-h
ouse
dev
elop
ed s
cale
ac
cord
ing
to C
OPS
OQ
20
051
10
5-po
int L
iker
t sc
ale
(1) o
ther
peo
ple
mak
e de
cisi
ons
conc
erni
ng h
is/h
er
wor
k*, (
2) th
e ob
serv
ed p
erso
n ha
s a
larg
e de
gree
of
influ
ence
con
cern
ing
his/
her w
ork;
obs
erve
d pe
rson
has
influ
ence
on
(3) h
ow q
uick
ly, (
4) w
hen,
(5
) wha
t (6)
how
to d
o hi
s/he
r wor
k, (7
) the
am
ount
of
wor
k, (8
) who
to w
ork
with
, (9)
his
/her
wor
k en
viro
nmen
t, (1
0) th
e qu
ality
of h
is/h
er w
ork
obse
rved
deg
ree
of
freed
om a
t wor
k
in-h
ouse
dev
elop
ed s
cale
ac
cord
ing
to C
OPS
OQ
20
051
4 5-
poin
t Lik
ert
scal
e
obse
rved
per
son
can
(1) d
ecid
e w
hen
to ta
ke a
br
eak,
(2) d
ecid
e w
hen
to ta
ke h
is/h
er h
olid
ays,
(3)
leav
e w
ork
to c
hat w
ith a
col
leag
ue, (
4) le
ave
wor
k fo
r sho
rt pr
ivat
e bu
sine
ss
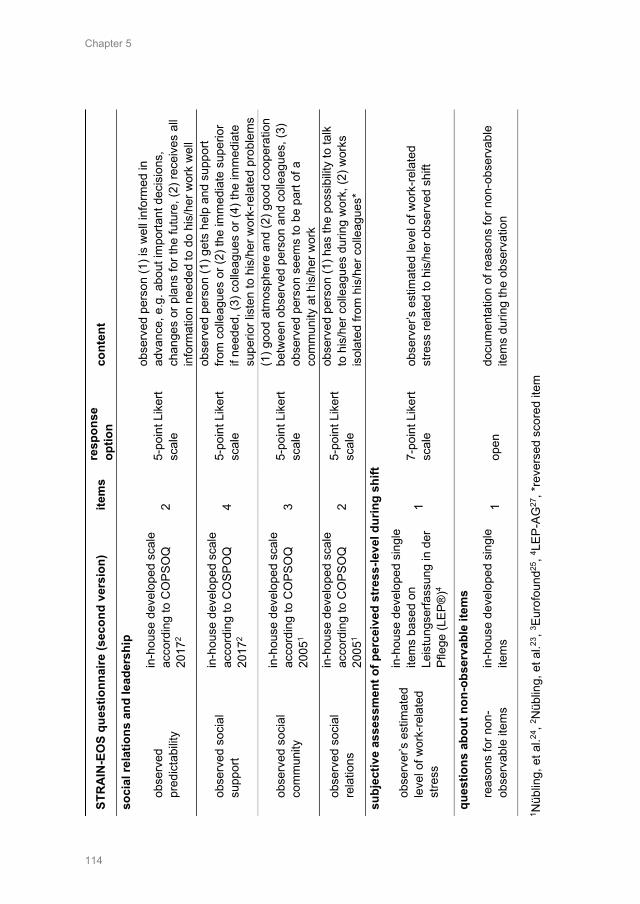
Chapter 5
114
ST
RA
IN-E
OS
ques
tionn
aire
(sec
ond
vers
ion)
ite
ms
resp
onse
op
tion
cont
ent
soci
al re
latio
ns a
nd le
ader
ship
obse
rved
pr
edic
tabi
lity
in-h
ouse
dev
elop
ed s
cale
ac
cord
ing
to C
OPS
OQ
20
172
2 5-
poin
t Lik
ert
scal
e
obse
rved
per
son
(1) i
s w
ell i
nfor
med
in
adva
nce,
e.g
. abo
ut im
porta
nt d
ecis
ions
, ch
ange
s or
pla
ns fo
r the
futu
re, (
2) re
ceiv
es a
ll in
form
atio
n ne
eded
to d
o hi
s/he
r wor
k w
ell
obse
rved
soc
ial
supp
ort
in-h
ouse
dev
elop
ed s
cale
ac
cord
ing
to C
OSP
OQ
20
172
4 5-
poin
t Lik
ert
scal
e
obse
rved
per
son
(1) g
ets
help
and
sup
port
from
col
leag
ues
or (2
) the
imm
edia
te s
uper
ior
if ne
eded
, (3)
col
leag
ues
or (4
) the
imm
edia
te
supe
rior l
iste
n to
his
/her
wor
k-re
late
d pr
oble
ms
obse
rved
soc
ial
com
mun
ity
in-h
ouse
dev
elop
ed s
cale
ac
cord
ing
to C
OPS
OQ
20
051
3 5-
poin
t Lik
ert
scal
e
(1) g
ood
atm
osph
ere
and
(2) g
ood
coop
erat
ion
betw
een
obse
rved
per
son
and
colle
ague
s, (3
) ob
serv
ed p
erso
n se
ems
to b
e pa
rt of
a
com
mun
ity a
t his
/her
wor
k
obse
rved
soc
ial
rela
tions
in-h
ouse
dev
elop
ed s
cale
ac
cord
ing
to C
OPS
OQ
20
051
2 5-
poin
t Lik
ert
scal
e
obse
rved
per
son
(1) h
as th
e po
ssib
ility
to ta
lk
to h
is/h
er c
olle
ague
s du
ring
wor
k, (2
) wor
ks
isol
ated
from
his
/her
col
leag
ues*
su
bjec
tive
asse
ssm
ent o
f per
ceiv
ed s
tres
s-le
vel d
urin
g sh
ift
obse
rver
’s e
stim
ated
le
vel o
f wor
k-re
late
d st
ress
in-h
ouse
dev
elop
ed s
ingl
e ite
ms
base
d on
Le
istu
ngse
rfass
ung
in d
er
Pfle
ge (L
EP®
)4
1 7-
poin
t Lik
ert
scal
e ob
serv
er’s
est
imat
ed le
vel o
f wor
k-re
late
d st
ress
rela
ted
to h
is/h
er o
bser
ved
shift
ques
tions
abo
ut n
on-o
bser
vabl
e ite
ms
reas
ons
for n
on-
obse
rvab
le it
ems
in-h
ouse
dev
elop
ed s
ingl
e ite
ms
1 op
en
docu
men
tatio
n of
reas
ons
for n
on-o
bser
vabl
e ite
ms
durin
g th
e ob
serv
atio
n
1 Nüb
ling,
et a
l.24, 2 N
üblin
g, e
t al.23
, 3 Eur
ofou
nd25
, 4 LEP
-AG
27, *
reve
rsed
sco
red
item
Chapter 5
115
2.3 Calculation of the sample size A sample size calculation using a Monte Carlo method was performed and Cronbach’s alpha was computed for various sample sizes, using an 8-item scale with a response option on a five-point Likert scale originating from COPSOQ as a proxy. Therefore, datasets on this 8-item scale of varying sizes (10, 50, 100, 150, 200, 300, 500) were generated based on averages and ICCs retrieved from previous results29 on COSOQ. The accuracy of the Cronbach’s alpha for a given sample size was estimated based on 5'000 such simulated datasets. The analyses indicated that an accuracy of 0.1 points is achieved with approximately 100 observations (95% confidence interval); therefore, a sample size of 100 to 110 participating health professionals was targeted.
2.4 Recruitment of health professionals Since the participation of organisations as well as individual health professionals was on a voluntary basis, this study is based on a convenience sample using the authors’ professional network. In total, two acute care hospitals, two nursing homes, one home care organisation and two psychiatric hospitals, all located in the German-speaking part of Switzerland, declared themselves willing to participate. Health professionals from various disciplines in these organisations (e.g. nurses, medical-technical-therapeutic-professionals, physicians) who had direct patient contact, were working part- or full-time and working on all shifts were invited to participate. They received a written study flyer with detailed information on the study. Health professionals willing to participate in the study had the option to send an e-mail directly to the research team with more information regarding the shift and date for a possible observation.
2.5 Recruitment and training of external observers Eight external observers with a professional background in the healthcare sector were recruited through advertisement. These external observers were aged between 22 and 40 years, were female, had professional training in nursing, physiotherapy or psychology, and had professional experience ranging from 2 to 19 years. All external observers were given a standardised training session of 10 hours. During this training, external observers received information on how to behave during the observations and discussed the comprehensibility and interpretation of each item included in the STRAIN-EOS assessment tool.
2.6 Interobserver reliability Since it was not possible for more than one external observer to accompany the observed health professional during the shift (requested by participants / organisations / patients), interobserver reliability was tested using 10 video
Chapter 5
116
sequences of various health professionals at work in order to represent reality in practice as well as possible. All external observers watched the same video sequences (30-50 minutes) and assessed the observed stressors separately, using the observation-based questionnaire. The mean intraclass correlation coefficient (ICC, ‘1 - each target is rated by a different set of k judges, randomly selected from a larger population of judges’)33 for all items included in an observation scale varied between 0.05 (scale on predictability) and 0.54 (scale on quantitative demands).
2.7 Data collection Data was collected between December 2017 and May 2018. Participating health professionals were observed by one external observer for an entire shift or working day (9 to 12 hours). External observers were permitted to talk to the health professionals they observed, but not to support or help them with their work. The external observers took notes during the observation period and completed the questionnaire (10 - 15 minutes) at the end of the shift/working day. Data was collected in acute care hospitals (inpatient medical, surgical and rehabilitation wards, emergency department, physiotherapy, operating room), psychiatric hospitals (general psychiatric wards and forensic), nursing homes and a home care organisation.
2.8 Analyses Data was analysed using SPSS 25®. For data analysis, all Items were transformed and standardised on a value range from 0 to 100 points (0 being the minimum value, 100 the maximum). The analysis procedure (construction and calculation of scales) was carried out according to the underlying self-report scales.26, 30 If fewer than half of the questions in a scale had been answered, no average score was calculated.26.
The final STRAIN-EOS is supposed to deliver an average score per scale as well as per thematic field according to the COPSOQ self-report scales.27 Therefore, an exploratory factor analysis (FA) with orthogonal rotation (varimax) and a listwise deletion of missing cases for each scale and each thematic field (a) demands at work, b) work organisation and content, c) social relations and leadership) was performed to check the one-dimensionality of each scale as well as the possible cross-loading of items (>0.5). Sampling adequacy for FA was measured by the Kaiser-Meyer-Olkin measure. Second, items were reduced in a stepwise manner using the Cronbach’s alpha value and poor factor loadings in the factor analyses of items as an indicator. We computed the final Cronbach’s alpha values as a test for the reliability of the scales. Third, convergent validity was tested, for which (1) Kendall’s tau-b correlations (most scales were skewed) were computed by combining the additional question about observers’ overall
Chapter 5
117
perceived workload in the observed shift compared to their ratings in the STRAIN-EOS, and (2) the mean values of the STRAIN-EOS were graphically compared with the STRAIN questionnaire from the first STRAIN measurement 2017/2018 (8112 self-reports of health professionals24).
Finally, the usability of the instrument was tested by descriptively analysing missing values, along with a qualitative content analysis of observers’ comments on questions which were not observable, or which were difficult to understand.
3. Results
3.1 Description of the external observation sample In total, 110 external observations of health professionals were included. External observations were conducted in a psychiatric hospital (n=36), a nursing home (n=30), home care situations (n=24) or an acute care hospital (20). A total of 55% were registered nurses (n=60), 37% nurse’s aides (n=41), 6% medical-technical-therapeutic professionals (n=7) and 2% physicians (n=2). Observations were conducted during a day shift (63%, n=69), an evening shift (24%, n=26), a night shift (4%, n=4) or another shift form, e.g. a divided shift (9%, n=11). Most observations were conducted during weekdays (Monday=20 observations, Tuesday=20, Wednesday=20, Thursday=15, Friday=18, Saturday=9, Sunday=8). Overall, external observations encompass 996 hours (including individual break times of usually 36 minutes for a shift of 9 hours), this includes 543 hours of observation for registered nurses, 369 hours for nurse’s aides, 63 hours for medical-technical-therapeutic professionals and 21 hours for physicians.
3.2 Construct validity Results of the factor analysis indicated a one-factor solution for all observation scales (explained variance ranged from 55.5% to 80.2%). No factor analysis could be calculated for the observation scale on ‘degree of freedom’ at work. The Kaiser-Meyer-Olkin criterion of a bare minimum of .5 was not met, and no one-factor solution could be identified for this scale. Figure 2 shows all scales included in the STRAIN-EOS, each with its factor loadings and percentage of total variance explained.
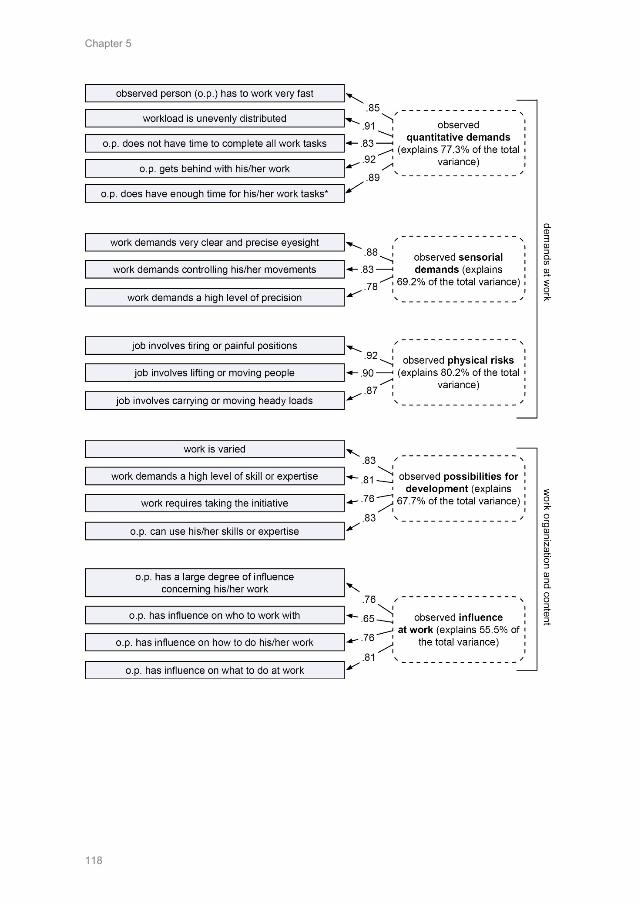
Chapter 5
118
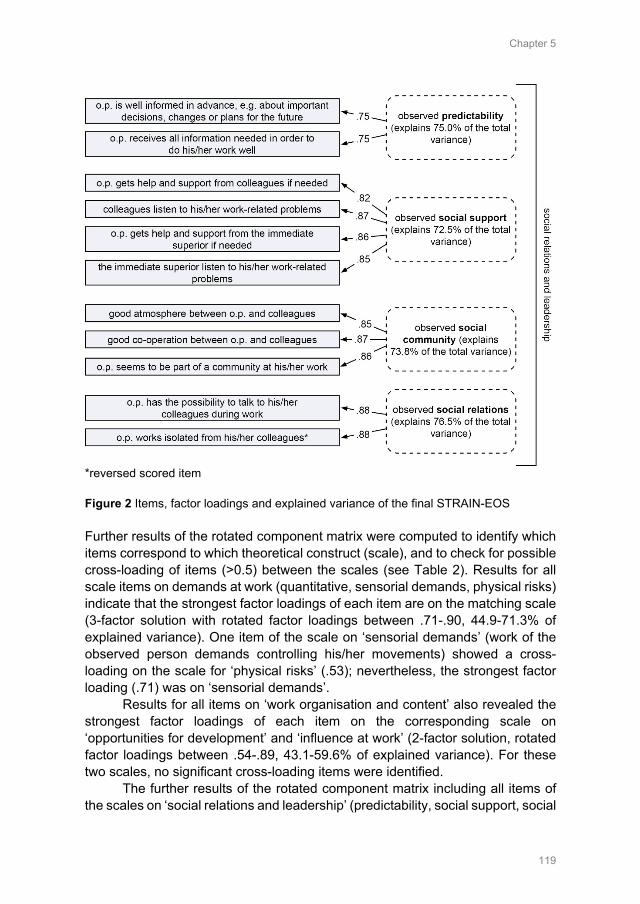
Chapter 5
119
*reversed scored item Figure 2 Items, factor loadings and explained variance of the final STRAIN-EOS Further results of the rotated component matrix were computed to identify which items correspond to which theoretical construct (scale), and to check for possible cross-loading of items (>0.5) between the scales (see Table 2). Results for all scale items on demands at work (quantitative, sensorial demands, physical risks) indicate that the strongest factor loadings of each item are on the matching scale (3-factor solution with rotated factor loadings between .71-.90, 44.9-71.3% of explained variance). One item of the scale on ‘sensorial demands’ (work of the observed person demands controlling his/her movements) showed a cross-loading on the scale for ‘physical risks’ (.53); nevertheless, the strongest factor loading (.71) was on ‘sensorial demands’.
Results for all items on ‘work organisation and content’ also revealed the strongest factor loadings of each item on the corresponding scale on ‘opportunities for development’ and ‘influence at work’ (2-factor solution, rotated factor loadings between .54-.89, 43.1-59.6% of explained variance). For these two scales, no significant cross-loading items were identified.
The further results of the rotated component matrix including all items of the scales on ‘social relations and leadership’ (predictability, social support, social
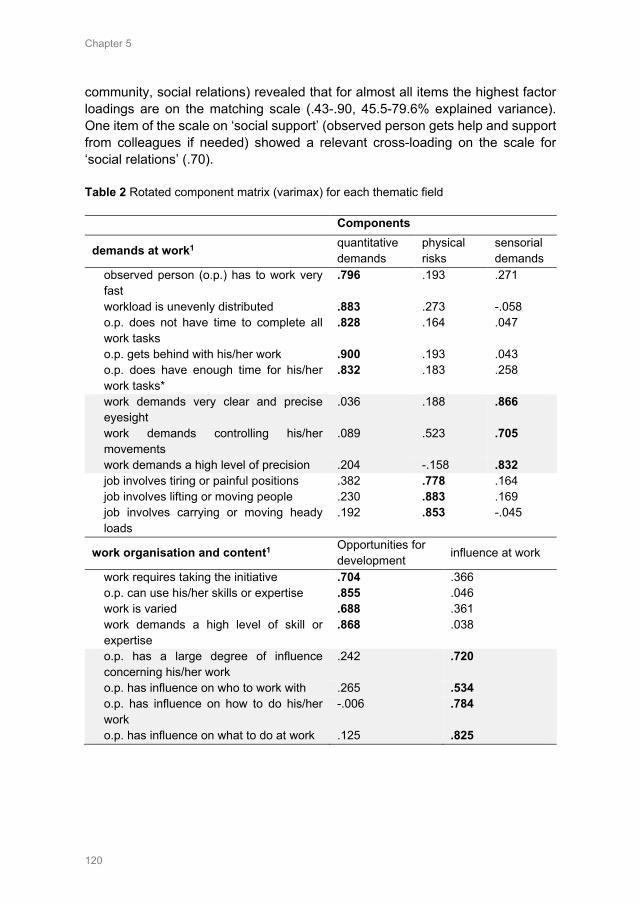
Chapter 5
120
community, social relations) revealed that for almost all items the highest factor loadings are on the matching scale (.43-.90, 45.5-79.6% explained variance). One item of the scale on ‘social support’ (observed person gets help and support from colleagues if needed) showed a relevant cross-loading on the scale for ‘social relations’ (.70). Table 2 Rotated component matrix (varimax) for each thematic field
Components
demands at work1 quantitative demands
physical risks
sensorial demands
observed person (o.p.) has to work very fast
.796 .193 .271
workload is unevenly distributed .883 .273 -.058 o.p. does not have time to complete all work tasks
.828 .164 .047
o.p. gets behind with his/her work .900 .193 .043 o.p. does have enough time for his/her work tasks*
.832 .183 .258
work demands very clear and precise eyesight
.036 .188 .866
work demands controlling his/her movements
.089 .523 .705
work demands a high level of precision .204 -.158 .832 job involves tiring or painful positions .382 .778 .164 job involves lifting or moving people .230 .883 .169 job involves carrying or moving heady loads
.192 .853 -.045
work organisation and content1 Opportunities for development influence at work
work requires taking the initiative .704 .366 o.p. can use his/her skills or expertise .855 .046 work is varied .688 .361 work demands a high level of skill or expertise
.868 .038
o.p. has a large degree of influence concerning his/her work
.242 .720
o.p. has influence on who to work with .265 .534 o.p. has influence on how to do his/her work
-.006 .784
o.p. has influence on what to do at work .125 .825
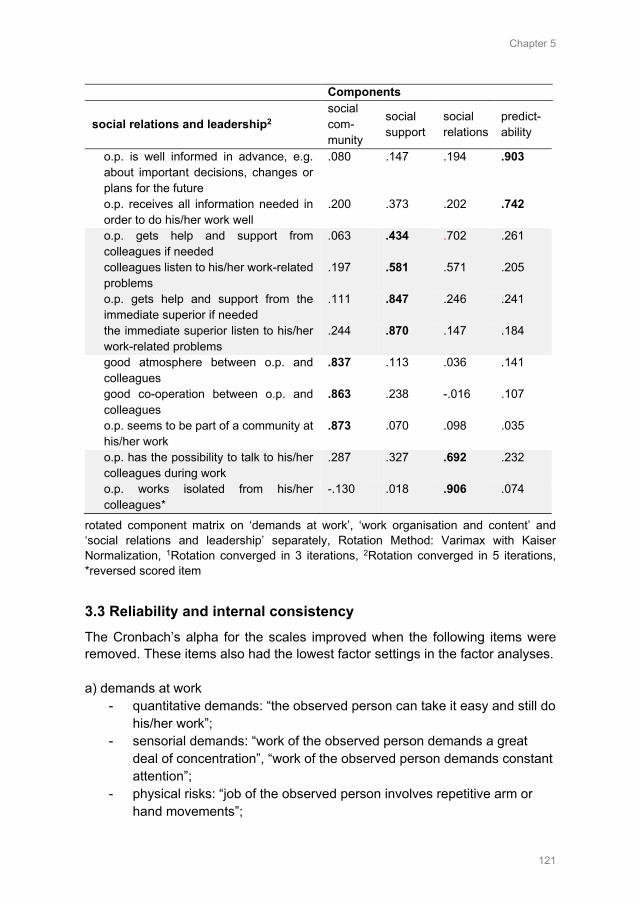
Chapter 5
121
Components
social relations and leadership2 social com-munity
social support
social relations
predict-ability
o.p. is well informed in advance, e.g. about important decisions, changes or plans for the future
.080 .147 .194 .903
o.p. receives all information needed in order to do his/her work well
.200 .373 .202 .742
o.p. gets help and support from colleagues if needed
.063 .434 .702 .261
colleagues listen to his/her work-related problems
.197 .581 .571 .205
o.p. gets help and support from the immediate superior if needed
.111 .847 .246 .241
the immediate superior listen to his/her work-related problems
.244 .870 .147 .184
good atmosphere between o.p. and colleagues
.837 .113 .036 .141
good co-operation between o.p. and colleagues
.863 .238 -.016 .107
o.p. seems to be part of a community at his/her work
.873 .070 .098 .035
o.p. has the possibility to talk to his/her colleagues during work
.287 .327 .692 .232
o.p. works isolated from his/her colleagues*
-.130 .018 .906 .074
rotated component matrix on ‘demands at work’, ‘work organisation and content’ and ‘social relations and leadership’ separately, Rotation Method: Varimax with Kaiser Normalization, 1Rotation converged in 3 iterations, 2Rotation converged in 5 iterations, *reversed scored item
3.3 Reliability and internal consistency The Cronbach’s alpha for the scales improved when the following items were removed. These items also had the lowest factor settings in the factor analyses. a) demands at work
- quantitative demands: “the observed person can take it easy and still do his/her work”;
- sensorial demands: “work of the observed person demands a great deal of concentration”, “work of the observed person demands constant attention”;
- physical risks: “job of the observed person involves repetitive arm or hand movements”;
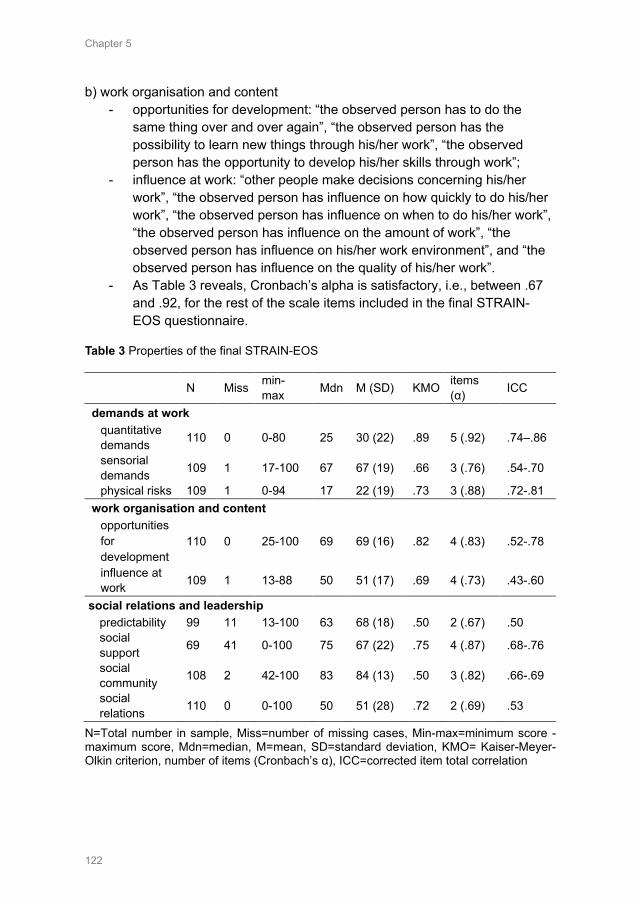
Chapter 5
122
b) work organisation and content - opportunities for development: “the observed person has to do the
same thing over and over again”, “the observed person has the possibility to learn new things through his/her work”, “the observed person has the opportunity to develop his/her skills through work”;
- influence at work: “other people make decisions concerning his/her work”, “the observed person has influence on how quickly to do his/her work”, “the observed person has influence on when to do his/her work”, “the observed person has influence on the amount of work”, “the observed person has influence on his/her work environment”, and “the observed person has influence on the quality of his/her work”.
- As Table 3 reveals, Cronbach’s alpha is satisfactory, i.e., between .67 and .92, for the rest of the scale items included in the final STRAIN-EOS questionnaire.
Table 3 Properties of the final STRAIN-EOS
N Miss min-max Mdn M (SD) KMO items
(α) ICC
demands at work quantitative demands 110 0 0-80 25 30 (22) .89 5 (.92) .74–.86
sensorial demands 109 1 17-100 67 67 (19) .66 3 (.76) .54-.70
physical risks 109 1 0-94 17 22 (19) .73 3 (.88) .72-.81 work organisation and content
opportunities for development
110 0 25-100 69 69 (16) .82 4 (.83) .52-.78
influence at work 109 1 13-88 50 51 (17) .69 4 (.73) .43-.60
social relations and leadership predictability 99 11 13-100 63 68 (18) .50 2 (.67) .50 social support 69 41 0-100 75 67 (22) .75 4 (.87) .68-.76
social community 108 2 42-100 83 84 (13) .50 3 (.82) .66-.69
social relations 110 0 0-100 50 51 (28) .72 2 (.69) .53
N=Total number in sample, Miss=number of missing cases, Min-max=minimum score - maximum score, Mdn=median, M=mean, SD=standard deviation, KMO= Kaiser-Meyer-Olkin criterion, number of items (Cronbach’s α), ICC=corrected item total correlation
Chapter 5
123
3.4 Convergent validity Table 4 shows the additional question integrated into the external observers’ questionnaire, “How do you perceive the overall workload in the observed shift?”. Since this question addresses especially the observer’s perceived quantitative demands at work, the results revealed, as expected, the highest significant positive correlation with the scale on ‘quantitative demands’ (rτ=.60, p<.001). Also, significant positive correlations were demonstrated for the scale on ‘physical risks’ (rτ=.24, p<.01). Furthermore, a high workload as perceived by external observers, was negatively correlated (adverse scorings) with observation scales on work organisation and content (p>.05), as well as on social relations and leadership (p<.05). Results revealed negative correlations with observers’ overall perceived workload in the observed shift and their ratings on health professionals ‘predictability’ at work (rτ=-.19, p<.05), ‘social support’ (rτ=-.32, p<.01), ‘social community’ (rτ=-.17, p<.05) and ‘social relations’ at work (rτ=-.28, p<.001). Table 4 Correlations of perceived stress-level of observers compared to their rating on the STRAIN-EOS Kendall’s tau-b observation scale correlations
coefficient p-value
demands at work quantitative demands .598 .000*** sensorial demands .087 .252 physical risks .243 .001**
work organisation and content opportunities for development -.016 .835 influence at work -.103 .167
social relations and leadership predictability -.191 .020* social support -.319 .001** social community -.171 .031* social relations -.275 .000***
*correlation is significant at: *p < .05; **p < .01; *** p < .001 (2-tailed)
In Figure 3, mean values from the STRAIN-EOS using external observations (n=110) were combined with mean values of 8112 health professionals’ self-reports on work stressors using the STRAIN questionnaire (first STRAIN measurement in 2017/2018).24 The self-report STRAIN questionnaire is comparable to the STRAIN-EOS, since they are based on the same underlying
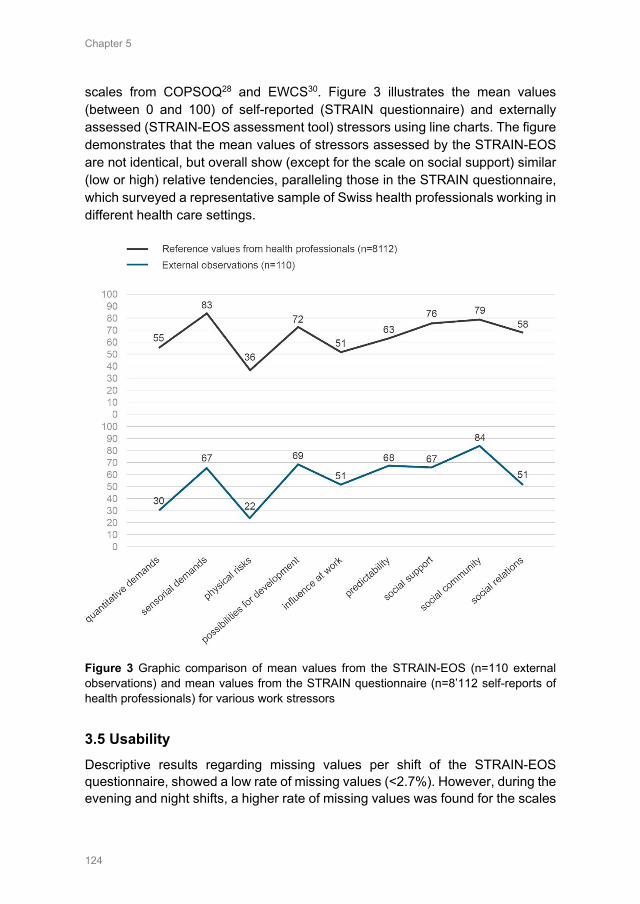
Chapter 5
124
scales from COPSOQ28 and EWCS30. Figure 3 illustrates the mean values (between 0 and 100) of self-reported (STRAIN questionnaire) and externally assessed (STRAIN-EOS assessment tool) stressors using line charts. The figure demonstrates that the mean values of stressors assessed by the STRAIN-EOS are not identical, but overall show (except for the scale on social support) similar (low or high) relative tendencies, paralleling those in the STRAIN questionnaire, which surveyed a representative sample of Swiss health professionals working in different health care settings.
Figure 3 Graphic comparison of mean values from the STRAIN-EOS (n=110 external observations) and mean values from the STRAIN questionnaire (n=8’112 self-reports of health professionals) for various work stressors
3.5 Usability Descriptive results regarding missing values per shift of the STRAIN-EOS questionnaire, showed a low rate of missing values (<2.7%). However, during the evening and night shifts, a higher rate of missing values was found for the scales
Chapter 5
125
on predictability (>40%) and social support (>50%), since some items were no longer observable (e.g. no colleagues or supervisor present during the night shift). According to the qualitative content analysis of the comments from the external observers, all questions were understandable. A total of 43 written comments from external observers were analysed. Most reasons declared by external observers for non-observable items were that the observed persons had "no contact with supervisors" during the observed shift (29 comments) or that a certain situation did not occur (e.g., the question on predictability ‘At your place of work, are you informed well in advance concerning for example important decisions, changes, or plans for the future?’) and, therefore, was not observable during the shift (12 comments).
4. Discussion
The results of this study revealed that 9 of the 10 tested observation scales were internally consistent, had good content and construct validity, and to some extent, convergent validity as well as sufficient usability. However, the results also demonstrated that the STRAIN-EOS questionnaire needs further testing, for example regarding the convergent validity with other observation-based assessment tools or interobserver reliability.
In regard to the observation scales on the ‘degree of freedom at work’, no factor analysis could be calculated. Since one item from the self-assessment scale, “Can the observed person take holidays when he/she wishes?”, was not observable during one shift only, the observation scale on degree of freedom consisted of 3 instead of 4 items. It is conceivable that the observation scale will show construct validity if this item is replaced.
Further results on the cross-loading of items gives confirmation of the construct validity and reveals that all items, except one, in the STRAIN-EOS had their strongest loading on the matching scale. The item of the scale on ‘social support’ showed a cross-loading on the scale ‘social relations. This can be explained by the fact that the item ‘the observed person gets help and support from colleagues if needed’ cannot be easily separated from the scale of ‘social relations’ at work in terms of content. However, if the STRAIN-EOS is used again, this should be checked again with a new sample.
Furthermore, comparisons between overall perceived workload as rated by observers and their ratings in the STRAIN-EOS reveal several significant correlations in the expected positive or negative direction, but also some weak correlations. The convergence between health professionals’ self-reported and externally assessed stressors regarding the same shift was investigated in a separate study34 and showed convergent scores for 3 of the 9 tested scales. This low convergence when comparing different methods for assessing work stressors is also described in previous literature.10 Therefore, a further analysis of
Chapter 5
126
correlations between the STRAIN-EOS and another validated external observation questionnaire assessing stressors at work could further strengthen the convergent and construct validities of the newly developed instrument.
4.1 Limitations Despite the extensive training of external observers, a possible observer bias cannot be excluded, since all observers differ in age, memories, behaviour and professional experience. Moreover, the STRAIN-EOS was tested in several healthcare settings that included different health professionals. Since a convenience sampling strategy was used, the distribution of observations in the settings, shifts and health professions was not controlled. Therefore, the extent to which this observation-based assessment can be generalized to other settings or specific professions is limited and further research is clearly needed to make a specific statement about the use of this instrument for one specific professional group (e.g. physiotherapists only) or setting (e.g. nursing homes) only. Moreover, the STRAIN-EOS was developed in German and needs to be translated and tested before use in other languages.
4.2 Methodological challenges and limitations A difficulty when using external observations in the healthcare setting was to measure interobserver reliability. On the one hand, patients did not accept having more than one external observer accompany the health professional; on the other hand, this was not possible for organisational reasons (e.g. hygiene guidelines, isolated patients, confined space conditions, disruption of workflows). Consequently, we decided to test interobserver reliability using video sequences. As the results show however, this was not entirely feasible either. Regarding the results of the partly unsatisfactory ICC results assessed by video sequences, it is difficult to draw conclusions. On the one hand, it is quite possible that the video sequences were not suitable, for example, to observe ‘predictability’. On the other hand, it is also possible that the observers` ratings in the STRAIN-EOS strongly diverged from one another. Therefore, we recommend taking into account possible observer effects when analysing the STRIAN-EOS scales (e.g. by using multiple regression analysis in which different observers are included as dummy variables). Moreover, further research is also needed regarding interobserver reliability using the STRAIN-EOS.
Another difficulty for external observers could be not knowing how to behave in certain cases, e.g. patient aggression against the observed health professional, observed violations of safety measures, unexpected deaths of patients or emergency situations such as reanimation. For this reason, we decided on having external observers with a professional background in the healthcare sector, because they are already familiar with such situations and can

Chapter 5
127
deal with them. In addition, we defined a code of conduct for all external observers as to how they should behave in such emergencies (e.g. assistance with reanimation).
A further difficulty was the 24-hour operation of health institutions, observations of evening and night shifts and observed health professionals doing overtime. In order for the external observers to observe evening and night shifts, a special employment contract was drawn up that allowed them to work in those shifts and settled the payment for it. In addition, it was agreed with the external observers that the observation would be continued even if the observed health professional worked overtime, provided it did not exceed 1-2 hours. This could be observed, except for one observation in which the observed health professional worked longer than 2 hours overtime.
Data protection and privacy of patients was also a special topic when doing external observation in the healthcare sector. The external observers were encouraged to maintain silence on patient-specific data. In addition, patients and professionals had the right at any time to send the observed person out of the room in very personal situations (e.g. when inserting a bladder catheter). Also, no patient-specific data were recorded in the STRAIN-EOS either.
5. Conclusion
As the results of the study reveal, the use of external observers in a healthcare system does not occur without effort. However, as the results of the study show, it is important to have a suitable observation tool specifically tailored to the requirements and framework conditions in healthcare. The STRAIN-EOS developed in this study is a first step but needs further testing. Also, research is needed to investigate the interrelationship between health professionals’ self-reports and objective results derived from observation-based assessment tools. With the development of the STRAIN-EOS based on validated and reliable self-assessment scales, such a comparison is conceivable in the future. This will assist in gaining deeper knowledge of the issues concerning work-related stressors in health professions. List of abbreviations COPSOQ: Copenhagen Psychosocial Questionnaire; EWCS: European Working Conditions Survey; LEP: Leistungserfassung in der Pflege; o.p.: observed person; STRAIN: work-related stress among health professionals in Switzerland; STRAIN-EOS: STRAIN - External Observation of work Stressors
Chapter 5
128
Ethical considerations The local Swiss ethics board confirmed that the study did not warrant a full ethics application and did not fall under the Swiss Federal Act on research involving human beings (Req-2016-00616). The study was on a voluntary basis for all organisations, health professionals participating and external observers; all participants were free to stop external observations at any time. Availability of data and STRAIN-EOS Raw data was generated at the Bern University of Applied Sciences, Department of Nursing Research. Derived data supporting the findings of this study is available from the corresponding author ([email protected]) upon request. The STRAIN-EOS questionnaire is also available upon request from the corresponding author. Competing interests The authors declare that they have no competing interests. Funding This study was financially supported by the University of Applied Sciences, Health Division, Bern, Switzerland (50% of the costs) and the State Secretariat for Education and Research (SER) of Switzerland (50% of the costs). The funding bodies had no influence or control over the planning, conduct, or reporting of the study. Authors' contributions KP and ES designed the questionnaire and recruited the participating health organisations. ES and KP collected and analysed the data (quantitative analysis as well as analysis of observers’ comments). SH, RH und JS made substantial contributions to the interpretation of data and writing the manuscript. All authors read and approved the final manuscript. Acknowledgements We are very grateful to all of the organisations involved and especially to the participating healthcare staff for sharing their experience and time so generously. Additionally, we thank Prof. Dr. Eva Soom, who shared her expertise on observation-based studies with us, as well as Dr. Christoph von Dach, who helped us with the recruitment of participants. We also thank Dr. Reto Bürgin, who shared his expertise in statistical analysis with us.
Chapter 5
129
References 1. Eurofound: Working conditions and workers' health. Luxembourg: Publications Office of the
European Union; 2019. 2. Lim J, Bogossian F, Ahern K. Stress and coping in Australian nurses: a systematic review.
International Nursing Review. 2010;57(1):22-31. doi:10.1111/j.1466-7657.2009.00765.x 3. Fuss I, Nubling M, Hasselhorn HM, Schwappach D, Rieger MA. Working conditions and Work-
Family Conflict in German hospital physicians: psychosocial and organisational predictors and consequences. BMC Public Health. 2008;8(1):353-370. doi:10.1186/1471-2458-8-353
4. Hämmig O. Explaining burnout and the intention to leave the profession among health professionals - a cross-sectional study in a hospital setting in Switzerland. BMC Health Service Research. 2018;18(1):785. doi:10.1186/s12913-018-3556-1
5. Leka S, Jain A. Health impact of psychosocial hazards at work: An overview. Geneva: World Health Organization, 2010.
6. Long MH, Johnston V, Bogossian F. Work-related upper quadrant musculoskeletal disorders in midwives, nurses and physicians: A systematic review of risk factors and functional consequences. Applied Ergonomics. 2012;43(3):455-467. doi:10.1016/j.apergo.2011.07.002
7. Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. Journal of the American Medical Association. 2002;288(16):1987-1993. doi:10.1001/jama.288.16.1987
8. Lancet. T. Physician burnout: a global crisis. The Lancet. 2019;394(10193):93. doi:10.1016/S0140-6736(19)31573-9
9. Lee R, Seo B, Hladkyj S, Lovell BL, Schwartzmann L. Correlates of physician burnout across regions and specialties: a meta-analysis. Human Resources for Health. 2013;11(1):48. doi:10.1186/1478-4491-11-48
10. Semmer NK, Grebner S, Elfering A. Beyond self-report: Using observational, physiological, and situation-based measures in research on occupational stress. In: Perrewe PL, Ganster DC, eds. Research in Occupational Stress and Well Being 3ed. Amsterdam: Emerald Group Publishing Limited, 2004: 205-263.
11. Kompier M. Assessing the psychosocial work environment--"subjective" versus "objective" measurement. Scandinavian Journal of Work, Environment & Health. 2005;31(6):405-408.
12. Connell P, Lee VB, Spector PE. Job stress assessment methods. JC Thomas (Vol. Ed.) and M. Hersen (Ed.), Comprehensive handbook of psychological assessment: Industrial and organizational assessment. 2004;4:455-469.
13. Corradini I, Marano A, Nardelli E. Work-Related Stress Risk Assessment: A Methodological Analysis Based on Psychometric Principles of an Objective Tool. SAGE Open. 2016;6(3):1-9. doi:10.1177/2158244016666888
14. Frese M, Zapf D. Methodological issues in the study of work stress: Objective vs. subjective measurement of work stress and the question of longitudinal studies. In: Cooper CL, Payne R, eds. Causes, coping and consequences of stress at work. Chichester: John Wiley & Sons, 1988: 375–411.
15. Foster P. Observational Research. In: Sapsford R, Jupp V, eds. Data Collection and Analysis. London: SAGE, 2006: 57-92.
16. Monahan T, Fisher JA. Benefits of "Observer Effects": Lessons from the Field. Qualitative Research. 2010;10(3):357-376. doi:10.1177/1468794110362874
17. Hull L, Arora S, Kassab E, Kneebone R, Sevdalis N. Assessment of stress and teamwork in the operating room: an exploratory study. The American Journal of Surgery. 2011;201(1):24-30. doi:10.1016/j.amjsurg.2010.07.039
18. Syed I, Daly T, Armstrong P, Lowndes R, Chadoin M, Naidoo V. How do work hierarchies and strict divisions of labour impact care workers' experiences of health and safety? Case studies of long term care in toronto. The journal of nursing home research. 2016;2(1):41-49.
19. Stab N, Hacker W, Weigl M. Work organization in hospital wards and nurses' emotional exhaustion: A multi-method study of observation-based assessment and nurses' self-reports. International Journal of Nursing Studies. 2016;61:52-62. doi:10.1016/j.ijnurstu.2016.05.012
20. Wheelock A, Suliman A, Wharton R, Babu ED, Hull L, Vincent C, et al. The Impact of Operating Room Distractions on Stress, Workload, and Teamwork. Annals of surgery. 2015;261(6):1079-1084. doi:10.1097/SLA.0000000000001051
Chapter 5
130
21. Büssing A, Glaser J. Das Tätigkeits-und Arbeitsanalyseverfahren für das Krankenhaus-Selbstbeobachtungsversion (TAA-KH-S): Hogrefe; 2002.
22. Weigl M, Muller A, Zupanc A, Angerer P. Participant observation of time allocation, direct patient contact and simultaneous activities in hospital physicians. BMC Health Services Research. 2009;9(1):110. doi:10.1186/1472-6963-9-110
23. Golz C, Peter KA, Hahn S. Cognitive Pretesting and pretest of the STRAIN questionnaire to elaborate work-related stress of health care staff in Switzerland. International Journal of Health Professions. 2018;5(1):109-120. doi:10.2478/ijhp-2018-0011
24. Peter KA, Schols JMGA, Halfens RJG, Hahn S. Investigating work-related stress among health professionals at different hierarchical levels: A cross-sectional study. Nursing Open. 2020(00):1-11. doi:10.1002/nop2.469
25. Spector PE, Dwyer DJ, Jex SM. Relation of job stressors to affective, health, and performance outcomes: a comparison of multiple data sources. Journal of Applied Psychology. 1988;73(1):11-19.
26. Kristensen TS. A new tool for assessing psychosocial factors at work: The Copenhagen Psychosocial Questionnaire. Copenhagen: National Institute of Health; 2000.
27. Nübling M, Stössel U, Hasselhorn HM, Michaelis M, Hofmann F. Measuring psychological stress and strain at work: Evaluation of the COPSOQ Questionnaire in Germany. GMS Psycho-Social-Medicine. 2006;3:1-14.
28. Nübling M, Vomstein M, Nolle I, Lindner A, Haug A, Lincke HJ. Deutsche Standard-Version des COPSOQ 2017. Freiburg: FFAW-Freiburger Forschungsstelle für Arbeitswissenschaften GmbH; 2017.
29. Nübling M, Stößel U, Hasselhorn HM, Michaelis M, Hofmann F. Methoden zur Erfassung psychischer Belastungen: Erprobung eines Messinstruments (COPSOQ). Dortmund: Bundesanstalt für Arbeitsschutz und Arbeitsmedizin; 2005.
30. Eurofound. Sixth European Working Conditions Survey - Questionnaire. Luxembourg: Publications Office of the European Union; 2015.
31. Parent-Thirion A, Fernández Macías E, Hurley J, Vermeylen G. Fourth European Working Conditions Survey. Luxembourg: European Foundation for the Improvement of Living and Working Conditions; 2007.
32. LEP-AG. Methode zur Dokumentation und Auswertung von Leistungen im Gesundheitswesen. St. Gallen: LEP AG; 2017.
33. Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychological Bulletin. 1979;86(2):420-428.
34. Peter KA, Hahn S, Stadelmann E, Halfens R, Schols J. Assessing Work Stressors in the Health Care Sector by Combining External Observation and Health Professionals’ Self-report in a Cross-sectional Study Design. Occupational Medicine & Health Affairs. 2020;8(1):303-309.
Chapter 6
Assessing work stressors in the health care sector by combining external observation and health professionals’ self-report in a cross-sectional study design
Peter KA, Hahn S, Stadelmann E, Halfens RJG, Schols JMGA. Assessing Work Stressors in the Health Care Sector by Combining External Observation and Health Professionals’ Self-report in a Cross-sectional Study Design. Occupational Medicine & Health Affairs. 2020;8(1):303-309.

Chapter 6
132
Abstract
Objective: Health professionals are particularly affected by work stressors and various methods have already been used to assess them. Linking health professionals’ self-report and external observations can provide a more detailed assessment of stressors, since conclusions for interventions can be derived from their agreement. Since there is a lack of studies in the health sector linking both data sources, the aim of this study is to identify the convergence between health professionals’ self-reports and external observations. Methods: Data were collected in general hospitals, nursing homes, psychiatric institutions and home-care organisations in a cross-sectional study design. 110 health professionals were observed during one entire shift, by one of eight trained external observers. Health professionals and observer separately filled out a questionnaire on work stressors after the observation. For data analysis multiple regression models using bootstrap were calculated considering possible observer effects. Results: Convergent scores for 3 of 9 tested scales on ‘predictability’ of work, ‘social community’ and ‘social relations’ (p>0.05) at work, were identified. However, health professionals rated their ‘quantitative’ (p=0.001), ‘sensorial’ (p=0.001) and ‘physical demands’ (p=0.001) significantly higher than the external observers did. On the contrary, external observers perceived the ‘possibilities for development’ (p=0.007), ‘influence at work’ (p=0.032) and ‘social support at work’ (p=0.002) as lower than did the health professionals. Results also indicate a significant influence of different work settings (p<0.05) on the convergence of self-assessed and observed work stressors. Conclusion: This study results reveal that results on work stressors can be influenced by the chosen method for data collection, which should be considered when using one method only. Moreover, differences between the settings indicate that results on work stressors from one health-care setting cannot be easily transferred to another.
Chapter 6
133
1. Introduction
Work-related stress is one of the main reasons why health professionals change or leave their jobs.1, 2 In particular, work stressors such as long working hours, shift work, work-family conflicts, emotionally stressful situations, physical demands, understaffing or time pressure can lead to a high level of stress at work.3, 4
Work stressors have been measured in several ways. Self-reports and observational assessments (e.g. analysis of work processes, external observations) are among the most widely used assessment techniques.5, 6 However, each of these sources brings its strong and weak methodological points.7 While self-reports provide insight into the internal psychological states of employees and may therefore be the only reliable source of such information, observational measures can provide more objective information in the sense of being independent of the employee.8 Moreover, external observations of work stressors are able to identify certain circumstances that are already taken for granted by employees and can provide a level of objectivity that is not possible when using self-reports alone.8, 9 Therefore, linking both data sources is important to know whether the objective (externally observed) assessment corresponds to the subjective (self-assessment of employee), since conclusions for interventions can be derived from the extent of that agreement.6
Linking both data sources has been done in various studies.10-12 However, the agreement between self-assessed and observation-based measures is often modest, with a convergence ranging mostly between 10 and 30%.13 Moreover, results indicate that the observed exposures of work stressors are underestimated, while employee self-assessments can be overestimated.12, 13 Nachreiner, et al.14 conclude that an agreement between these two data sources cannot be expected.
Also in the health care sector, studies including both health professionals’ self-reports and observational approaches have been carried out on work-organisation and teamwork, among others.15-19 However, there is a lack of studies linking employee self-report and observation-based assessment among health professionals. Studies linking both data sources are important to gain deeper knowledge of the issues concerning work stressors in the health care sector.
Therefore, the aim of this study is to identify the convergence between health professionals’ self-reports and external observations concerning stressors at work.
Chapter 6
134
2. Method
This study has a cross-sectional design and the data is based on external observations and health professionals’ self-reports on work stressors. This study is also of the national STRAIN study – ‘work-related stress among health professionals in Switzerland’ (clinical trials registration: NCT03508596).
2.1 Study population A convenience sample of health professionals from two acute care hospitals, one home care organisation, a nursing home and two psychiatric institutions in the German-speaking part of Switzerland was used. The study sample consisted of health professionals from various disciplines (e.g. nurses, medical-technical-therapeutic-professionals, physicians) with direct patient contact. Health professionals in the participating health organisations received online study information and were asked whether they would like to participate on a voluntary basis. Health professionals willing to participate could contact the STRAIN research team directly (by email or phone) and an observation date was set for an entire shift. Since the external observation was conducted during one entire shift (9-12 hours), health professionals who worked less than 9 hours a shift (e.g. half days) were excluded.
2.2 Instruments For this study, a self-report questionnaire for health professionals and an observational questionnaire for external observers was developed (see Figure 1). The self-assessment scales are based on the STRAIN questionnaire20 and the questionnaire for external observers on the STRAIN-EOS (STRAIN - External Observation of work Stressors). Both questionnaires contain the same scales but differ in the wording (e.g. “Do you have to work very fast?” for self-reports and, “Does the observed person have to work very fast?”, for external observers). Both questionnaires (self-report and observation) assess information about demands at work, work organisation and content, and social relations and leadership and consist of items from the Copenhagen Psychosocial Questionnaire21, 22 -COPSOQ and the Sixth European Working Condition Survey23 - EWCS.
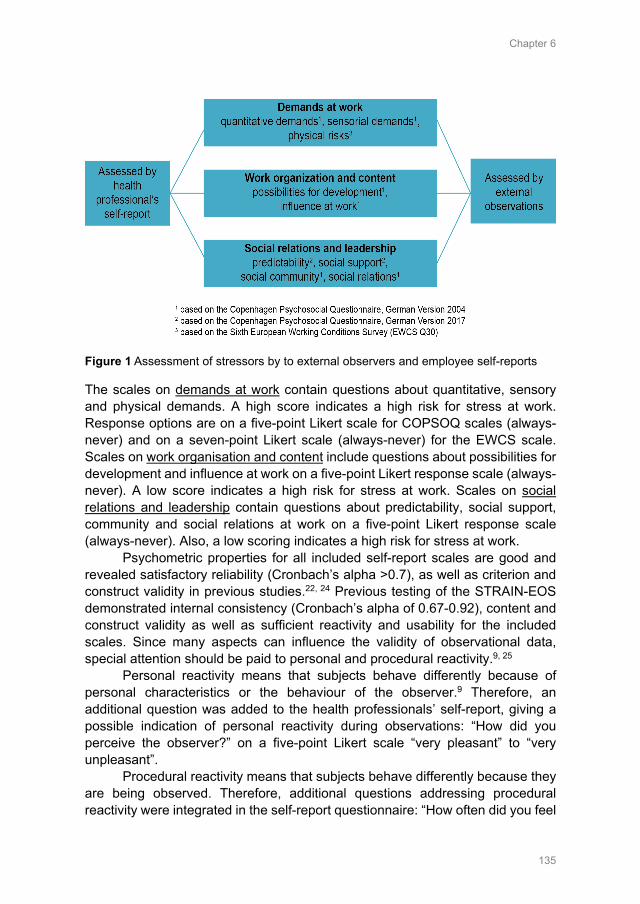
Chapter 6
135
Figure 1 Assessment of stressors by to external observers and employee self-reports
The scales on demands at work contain questions about quantitative, sensory and physical demands. A high score indicates a high risk for stress at work. Response options are on a five-point Likert scale for COPSOQ scales (always-never) and on a seven-point Likert scale (always-never) for the EWCS scale. Scales on work organisation and content include questions about possibilities for development and influence at work on a five-point Likert response scale (always-never). A low score indicates a high risk for stress at work. Scales on social relations and leadership contain questions about predictability, social support, community and social relations at work on a five-point Likert response scale (always-never). Also, a low scoring indicates a high risk for stress at work.
Psychometric properties for all included self-report scales are good and revealed satisfactory reliability (Cronbach’s alpha >0.7), as well as criterion and construct validity in previous studies.22, 24 Previous testing of the STRAIN-EOS demonstrated internal consistency (Cronbach’s alpha of 0.67-0.92), content and construct validity as well as sufficient reactivity and usability for the included scales. Since many aspects can influence the validity of observational data, special attention should be paid to personal and procedural reactivity.9, 25
Personal reactivity means that subjects behave differently because of personal characteristics or the behaviour of the observer.9 Therefore, an additional question was added to the health professionals’ self-report, giving a possible indication of personal reactivity during observations: “How did you perceive the observer?” on a five-point Likert scale “very pleasant” to “very unpleasant”.
Procedural reactivity means that subjects behave differently because they are being observed. Therefore, additional questions addressing procedural reactivity were integrated in the self-report questionnaire: “How often did you feel
Chapter 6
136
observed?”, “Did the observation have an influence on your work organisation or workflow?”, “Do you think that in certain situations you would have behaved differently without being observed?” on a five-point Likert scale “always” to “never”.
2.3 Selection and training of external observers External observers were recruited by advertisements. Care was taken to ensure that the observers were familiar with the health care setting (education in a health profession), and that they were heterogenous regarding age, experience and occupation. A total of eight external observers aged 22-40 years, all female, with a professional training in nursing, physiotherapy or psychology and professional experience of 2 – 19 years were recruited. The external observers carried out between 3 and 27 external observations.
To minimize a possible observer bias, all external observers were trained before starting data collection. Therefore, the training was conducted in two groups and lasted from 8 to 10 hours per training. In the first part, external observers received information about how the thinking process works and how it is influenced. In the second part of the training, all observers watched a total of 10 video sequences including footage of doctors and nurses at work (30 min on average) and assessed stressors using the STRAIN-EOS. After each video sequence, assessed rankings using the STRAIN-EOS were discussed for each item. Also, every item in the questionnaire was then checked for comprehensibility and interpretation. During the observation, external observers were advised that they could speak with the observed person (if necessary), but not to support them at work.
2.4 Data collection Data collection took part between December 2017 and May 2018. All participating health professionals were observed during one entire shift/working day of 9 to 12 hours. At the end of the observation, health professionals and the external observers separately filled out the questionnaire (10-15 min) assessing stressors at work.
2.5 Data Analysis Data analyses were done using IBM SPSS Statistics® 24. All questions about personal and procedural reactivity were analysed descriptively. All items in the self-assessment and observational scales were transformed on a value range from 0 (minimum value) to 100 (maximum value). To analyse the differences between health professional self-reported and externally observed data, multiple regression models for each scale were calculated taking into account possible
Chapter 6
137
observer effects. For the regression models the difference between self-assessment (SE) scores and externally observed (OB) scores (SE-OB) was used as the dependent variable and dummy variables for observers and different healthcare settings as independent variables. The dummy variables were coded in such a way that the sum of observer effects is equal to zero (sum to zero contrasts), whit observer 8 as reference. Using this dummy variable specification, the intercept (constant) of the model can be interpreted as the mean difference between self-reported and externally observed data when adjusting for observer effects. Since the assumption of heteroskedasticity (modelling errors are uncorrelated / uniform) was not met, standard errors, p-values and confidence intervals were computed based on bootstrap (r=1000 bootstrap, bias corrected and accelerated, 95% CI). To check for differences between the health care settings (general hospital, nursing home, home care organisation, psychiatric institution), a linear regression model including dummy variables for observers and dummy variables for the health care settings was used. To test whether there is any difference between health care settings, 2-tailed F-tests were used. In case of a significant F-test (p-value < 0.05), post hoc analyses based on Wald tests were performed to find out which settings differ from each other.
3. Results
3.1 Description of the study sample In total, 110 health professionals were observed (n=110 health professional self-reports, n=110 external observations). The observations were conducted in the acute care hospital (18%), in nursing home (27%), home care setting (22%) and psychiatric institutions (33%). Most observed shifts were day (63%) and evening-shifts (24%). Registered nurses (n=60) and nurse assistants (n=41) were most frequently represented in the study sample. The mean age of the observed health professionals was 40 years (SD = 13) with a mean professional experience of 15 years (SD = 11) in general and 5.5 years (SD = 6) in their current position. Observed health professionals were registered nurses (55%), nurse assistants (37%), medical-technical-therapeutic professionals or physicians (8%).
3.2 Self-reported and observational data Figure 2 reveals a first comparison of the self-assessment and observational data regarding the mean and standard deviation for each scale. In order to show the size of difference between the self- and observation-based assessment (SE-OB), the median of the difference between the self-reports and observations (Mdn of diff.) is also illustrated.
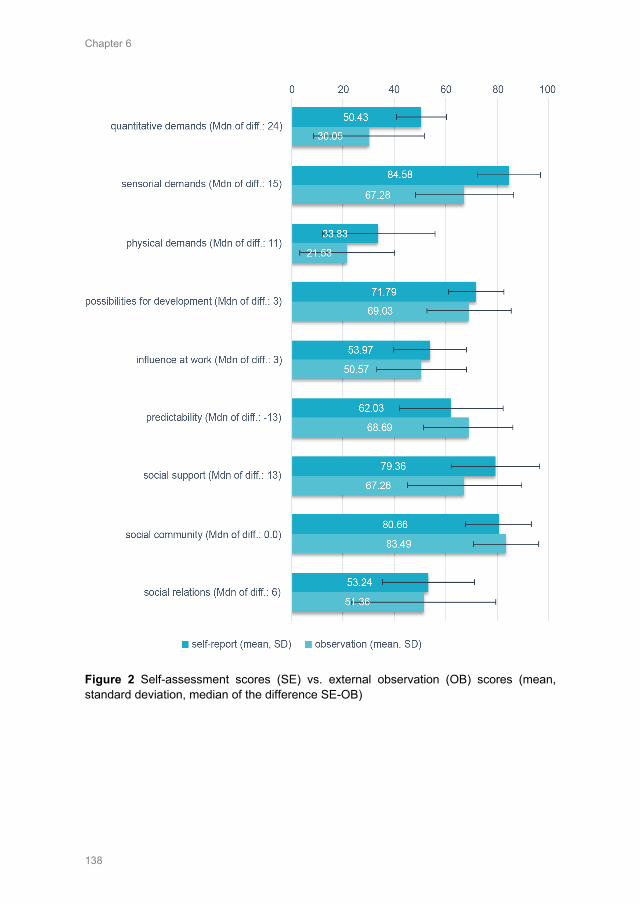
Chapter 6
138
Figure 2 Self-assessment scores (SE) vs. external observation (OB) scores (mean, standard deviation, median of the difference SE-OB)
Chapter 6
139
A first tendency indicated that observed health professionals perceived the demands at work scales (quantitative, sensorial and physical demands) as higher than the external observers. The means of the scale for possibilities for development, influence at work, social support and social relations also showed a tendency for observational data scores to be lower than the self-reported data. On the other hand, a tendency was found for the observation-based assessments of the scale predictability and social community to be ranked higher than for health professionals’ self-assessments.
3.3 Influence of external observers Results of questions on personal reactivity indicate that most observed health professionals (90%) perceived the external observer as ‘very pleasant-pleasant’, 8% as ‘neutral’ and a few (2%) as ‘unpleasant-very unpleasant’ during the external observation sequence.
Further results on procedural reactivity reveal that most of the observed health professionals ‘seldom-never’ felt observed (64%). In addition, most observed health professionals did not think that the external observation had an influence on their work organisation or workflow (84%) and would not have behaved differently if there were not being observed (87%).
Additional results on the observers’ influence indicate significant observer-effects for quantitative and sensorial demands, all scales on work organisation and content and social relation and leadership. Results on observer’s influence are presented in Table one and reveal significant influence (using F-statistics) of the external observers as well as information, which of the observers have differed significantly. Considering all scale, no observers’ influence pattern can be recognized; any observers effects are random.
3.4 Differences between SE and OB Results of robust multiple regression using bootstrap are presented in Table one. The Table includes descriptive statistics for the difference between the self-assessment (SE) and external observations (OB), influence of observer’s as well as the estimated difference (SE-OB) at the level of 0.05 and 0.005 (2-tailed).
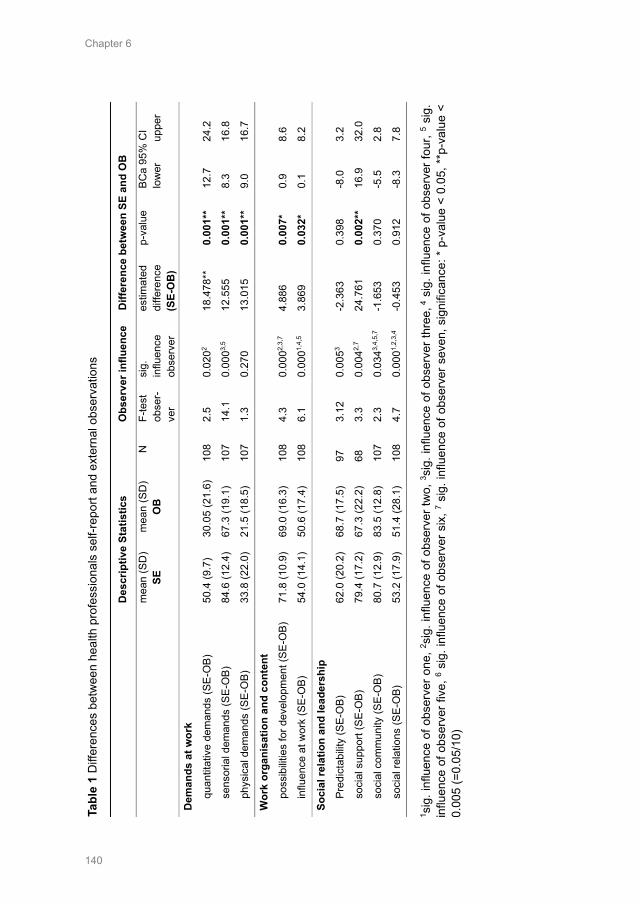
Chapter 6
140
Ta
ble
1 D
iffer
ence
s be
twee
n he
alth
pro
fess
iona
ls s
elf-r
epor
t and
ext
erna
l obs
erva
tions
D
escr
iptiv
e St
atis
tics
O
bser
ver i
nflu
ence
D
iffer
ence
bet
wee
n SE
and
OB
m
ean
(SD
) SE
m
ean
(SD
) O
B
N
F-te
st
obse
r-ve
r
sig.
in
fluen
ce
obse
rver
estim
ated
di
ffere
nce
(SE-
OB
)
p-va
lue
BCa
95%
CI
lo
wer
up
per
Dem
ands
at w
ork
quan
titat
ive
dem
ands
(SE-
OB)
50
.4 (9
.7)
30.0
5 (2
1.6)
10
8 2.
5 0.
0202
18.4
78**
0.
001*
* 12
.7
24.2
sens
oria
l dem
ands
(SE-
OB)
84
.6 (1
2.4)
67
.3 (1
9.1)
10
7 14
.1
0.00
03,5
12.5
55
0.00
1**
8.3
16.8
phys
ical
dem
ands
(SE-
OB)
33
.8 (2
2.0)
21
.5 (1
8.5)
10
7 1.
3 0.
270
13.0
15
0.00
1**
9.0
16.7
Wor
k or
gani
satio
n an
d co
nten
t po
ssib
ilitie
s fo
r dev
elop
men
t (SE
-OB)
71
.8 (1
0.9)
69
.0 (1
6.3)
10
8 4.
3 0.
0002,
3,7
4.88
6 0.
007*
0.
9 8.
6
influ
ence
at w
ork
(SE-
OB)
54
.0 (1
4.1)
50
.6 (1
7.4)
10
8 6.
1 0.
0001,
4,5
3.86
9 0.
032*
0.
1 8.
2
Soci
al re
latio
n an
d le
ader
ship
Pr
edic
tabi
lity
(SE-
OB)
62
.0 (2
0.2)
68
.7 (1
7.5)
97
3.
12
0.00
53 -2
.363
0.
398
-8.0
3.
2
soci
al s
uppo
rt (S
E-O
B)
79.4
(17.
2)
67.3
(22.
2)
68
3.3
0.00
42,7
24.7
61
0.00
2**
16.9
32
.0
soci
al c
omm
unity
(SE-
OB)
80
.7 (1
2.9)
83
.5 (1
2.8)
10
7 2.
3 0.
0343,
4,5,
7 -1
.653
0.
370
-5.5
2.
8
soci
al re
latio
ns (S
E-O
B)
53.2
(17.
9)
51.4
(28.
1)
108
4.7
0.00
01,2,
3,4
-0.4
53
0.91
2 -8
.3
7.8
1 sig
. inf
luen
ce o
f obs
erve
r one
, 2 sig
. inf
luen
ce o
f obs
erve
r tw
o, 3 s
ig. i
nflu
ence
of o
bser
ver t
hree
, 4 s
ig. i
nflu
ence
of o
bser
ver f
our,
5 si
g.
influ
ence
of o
bser
ver f
ive,
6 sig
. inf
luen
ce o
f obs
erve
r six
, 7 sig
. inf
luen
ce o
f obs
erve
r sev
en, s
igni
fican
ce: *
p-v
alue
< 0
.05,
**p
-val
ue <
0.
005
(=0.
05/1
0)
Chapter 6
141
3.4.1 Demands at work Results of multiple regression on the demands at work scales indicate that the observed health professionals rated several demands at work as higher than the external observers did (Table 1). Health professionals’ ratings for ‘quantitative demands’ are significantly higher than those from external observers (estimated difference = 18.5, p=0.001). Also, for the scales on ‘sensorial demands’ (estimated difference = 12.6, p=0.001) and ‘physical demands’ (estimated difference = 13.0, p=0.001) the results of the regression analysis revealed a significant difference between the self-assessment and observation-based scales.
3.4.2 Work organisation and content Here, significant results indicated that the external observers perceived the ‘possibilities for development’ and ‘influence at work’ as being lower than did the health professionals. Results for the scale on ‘possibilities for development’ revealed an estimated difference (SE-OB) of 4.9 (p=0.007). Also, the scale on ‘influence at work’ indicated significant results (estimated difference = 3.9, p=0.032) at the significance level of 0.05, but not at 0.005 (including Bonferroni correction).
3.4.3 Social relations and leadership On the scales for ‘social relations’ and ‘leadership’, health professional self-reports and external observations appeared to be more similar. No significant differences on ‘predictability’ at work (estimated difference = -2.4, p=0.398), ‘social community’ (estimated difference = -1.7, p=0.370) and ‘social relations’ (estimated difference = -0.5, p=0.912) between health professional self-reports and external observations was found. However, the scale for ‘social support’ from colleagues and supervisors indicated significant differences between the two assessments: external observers perceived the ‘support’ received from colleagues and supervisors as significantly lower than did the observed health professionals themselves (estimated difference = 24.8, p=0.002).
3.5 Influence of different health care settings Table two contains further information on whether there are differences between different work settings (general hospitals, nursing homes, home care organisations, psychiatric institutions). No significant differences (p>0.05, 2-tailed) of health professionals’ self-reports and external observations between the general hospital, nursing homes, home care organisations and psychiatric institutions were found for the scales on ‘quantitative’ and ‘physical demands’ as well as ‘social community’ at work.
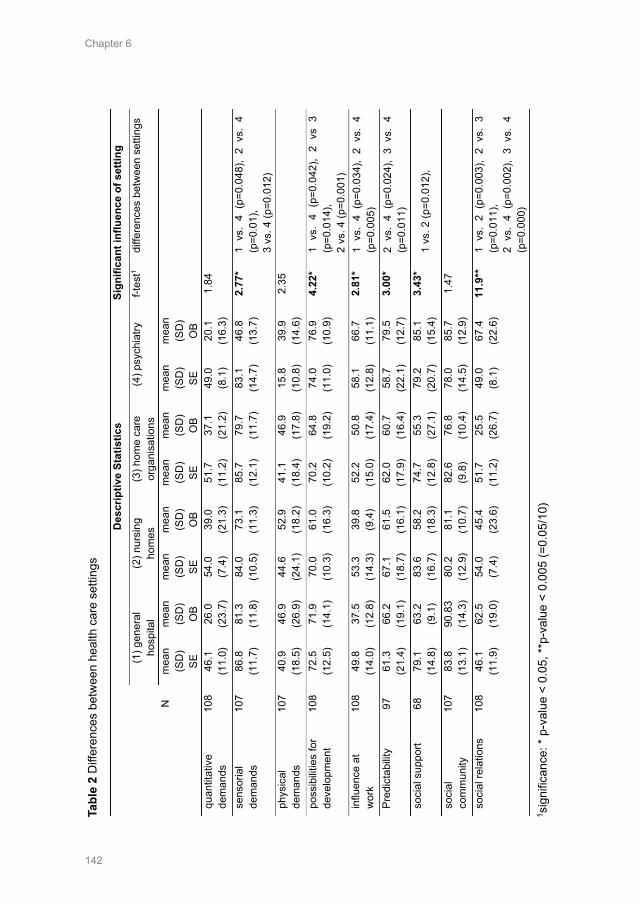
Chapter 6
142
Ta
ble
2 D
iffer
ence
s be
twee
n he
alth
car
e se
tting
s
D
escr
iptiv
e St
atis
tics
Sign
ifica
nt in
fluen
ce o
f set
ting
(1
) gen
eral
ho
spita
l (2
) nur
sing
ho
mes
(3
) hom
e ca
re
orga
nisa
tions
(4
) psy
chia
try
f-tes
t1 di
ffere
nces
bet
wee
n se
tting
s
N
mea
n (S
D)
SE
mea
n (S
D)
OB
mea
n (S
D)
SE
mea
n (S
D)
OB
mea
n (S
D)
SE
mea
n (S
D)
OB
mea
n (S
D)
SE
mea
n (S
D)
OB
quan
titat
ive
dem
ands
10
8 46
.1
(11.
0)
26.0
(2
3.7)
54
.0
(7.4
) 39
.0
(21.
3)
51.7
(1
1.2)
37
.1
(21.
2)
49.0
(8
.1)
20.1
(1
6.3)
1.
84
sens
oria
l de
man
ds
107
86.8
(1
1.7)
81
.3
(11.
8)
84.0
(1
0.5)
73
.1
(11.
3)
85.7
(1
2.1)
79
.7
(11.
7)
83.1
(1
4.7)
46
.8
(13.
7)
2.77
* 1
vs.
4 (p
=0.0
48),
2 vs
. 4
(p=0
.01)
, 3
vs. 4
(p=0
.012
) ph
ysic
al
dem
ands
10
7 40
.9
(18.
5)
46.9
(2
6.9)
44
.6
(24.
1)
52.9
(1
8.2)
41
.1
(18.
4)
46.9
(1
7.8)
15
.8
(10.
8)
39.9
(1
4.6)
2.
35
poss
ibilit
ies
for
deve
lopm
ent
108
72.5
(1
2.5)
71
.9
(14.
1)
70.0
(1
0.3)
61
.0
(16.
3)
70.2
(1
0.2)
64
.8
(19.
2)
74.0
(1
1.0)
76
.9
(10.
9)
4.22
* 1
vs.
4 (p
=0.0
42),
2 vs
3
(p=0
.014
),
2 vs
. 4 (p
=0.0
01)
influ
ence
at
wor
k 10
8 49
.8
(14.
0)
37.5
(1
2.8)
53
.3
(14.
3)
39.8
(9
.4)
52.2
(1
5.0)
50
.8
(17.
4)
58.1
(1
2.8)
66
.7
(11.
1)
2.81
* 1
vs.
4 (p
=0.0
34),
2 vs
. 4
(p=0
.005
) Pr
edic
tabi
lity
97
61.3
(2
1.4)
66
.2
(19.
1)
67.1
(1
8.7)
61
.5
(16.
1)
62.0
(1
7.9)
60
.7
(16.
4)
58.7
(2
2.1)
79
.5
(12.
7)
3.00
* 2
vs.
4 (p
=0.0
24),
3 vs
. 4
(p=0
.011
) so
cial
sup
port
68
79.1
(1
4.8)
63
.2
(9.1
) 83
.6
(16.
7)
58.2
(1
8.3)
74
.7
(12.
8)
55.3
(2
7.1)
79
.2
(20.
7)
85.1
(1
5.4)
3.
43*
1 vs
. 2 (p
=0.0
12),
soci
al
com
mun
ity
107
83.8
(1
3.1)
90
.83
(14.
3)
80.2
(1
2.9)
81
.1
(10.
7)
82.6
(9
.8)
76.8
(1
0.4)
78
.0
(14.
5)
85.7
(1
2.9)
1.
47
soci
al re
latio
ns
10
8 46
.1
(11.
9)
62.5
(1
9.0)
54
.0
(7.4
) 45
.4
(23.
6)
51.7
(1
1.2)
25
.5
(26.
7)
49.0
(8
.1)
67.4
(2
2.6)
11
.9**
1
vs.
2 (p
=0.0
03),
2 vs
. 3
(p=0
.011
),
2 vs
. 4
(p=0
.002
), 3
vs.
4 (p
=0.0
00)
1 sig
nific
ance
: * p
-val
ue <
0.0
5, **
p-va
lue
< 0.
005
(=0.
05/1
0)
Chapter 6
143
However, differences between the health professionals’ and observers’ ratings can be identified for the scales on:
- ‘sensorial demands’ (p<0.05) between the psychiatric institution and all other settings
- ‘possibilities for development’ (p<0.05) between general hospital and psychiatric institution, nursing home and home care organisation and nursing home and psychiatric institution
- ‘influence at work’ (p<0.05) between psychiatric institution and general hospital/nursing home
- ‘predictability’ (p<0.05) between psychiatric institution and nursing home/home care organisation
- ‘social support’ (p<0.05) between general hospital and nursing home - ‘social relations’ (p<0.005) between nursing home and all the other
settings as well as between home care and psychiatric institution.
4. Discussion
This study reveals convergent as well as dissenting assessments of work stressors by health professionals and external observers. Convergent scores (p>0.05) between health professionals self-reported and externally observed ‘predictability’ of work, ‘social community’ and ‘social relations’ at work were identified.
However, further results indicate that health professionals rated their ‘quantitative’, ‘sensorial’ and ‘physical demands’ significantly higher than the external observers did. Similar results on physical risk factors at work using self-report, video observation and direct measurement methods were also found.12 Moreover, some authors suggest results on demands at work as overestimated by employees’ self-assessments and as underestimated by observations.13, 26 A possible reason for this difference could be a higher ‘initial level’ of perceived stress factors by the health professionals over time. Therefore, it is possible, that the health professionals’ and external observers rating are not based on the exactly same situations.10 Certain demands at work may have already been experienced by the employees over a longer period of time and have led to an overall more intensive judgment, while external observers only observed a limited period of time and therefore rate the situation as less demanding.13
Furthermore, significant differences were found for ‘possibilities for development’ and ‘influence at work’. The external observers scored the ‘possibilities for development’ as well as the ‘influence at work’ as lower than observed health professionals. Moreover, significant differences for health professionals self-assessed and externally observed ‘social support’ from colleagues and supervisors at work also indicate that external observers
Chapter 6
144
perceived the ‘social support’ during the observation sequences as being lower than did the observed health professionals. Regarding study results about self-reported and observed ‘social support’ of young couples, Lorenz, et al.10 suspected that hostile and supportive behaviours are more likely to be remembered and therefore may be more superficial in employee self-report. On the other hand, supportive behaviour is more difficult to identify for external observers than hostility.10
Further results reveal that although the external observers have been trained beforehand, there is still a significant influence of the different external observers on the results. However, further findings from personal and procedural reactivity indicate, that most observed health professionals perceived the external observer as ‘pleasant’ and ‘seldom to never’ felt observed. As Guest, Namey, and Mitchell27 stated, a good external observer fits into the observation-based situation ‘well enough to be ignored’. Therefore, it is important that external observers adapt to their observation-based setting (e.g. wearing the same clothes), are familiar with the health care setting and well-trained in advance. Furthermore, it is important to consider a possible observer-influence in the data analysis to avoid a distortion of the results.
Further results indicate a significant influence of different work settings on the convergent of self-assessed and observed work stressors. Most frequently, the difference between self- and externally assessed work stressors in psychiatric institutions (in 11 cases) and nursing homes (in 8 cases) were significantly different from other settings. However, as previous study results28 indicate, there is a significant relationship between the psychological climate (operationalized as employees’ perception) and employees work attitudes, performance and motivation, which could provide a possible explanation for these differences. It seems possible that the psychological climate differs strongly between these health care settings, which could result in a stronger difference between self-reports and external observations.
Overall, this study results reveal that for 6 of 9 tested scales (60%) no convergence between health professionals self-assessed and externally observed work stressors was met, which is in line with previous literature.13 However, one could conclude that one of the data sources (self-reports or external observation) is maybe more valid than the other (captures the true value). Therefore, it is important to note that both methods include ‘true variance’ as well as ‘biasing effects’.13 Moreover, it is to be assumed that both data sources capture the same approach in a different way (e.g. self-reports as ‘intrinsic’ and externally observed as ‘extrinsic’ perception of stressors).14 However, considering that it is the perception of each employee that ultimately determines his or her reaction to the work environment.29
Nevertheless, the complementary perspective of external observers can provide further insights into the current work situation with an ‘objective’ external view. As these study results reveal, this should be considered especially when

Chapter 6
145
assessing ‘demands at work’, ‘possibilities for development’, ‘influence at work’ as well as ‘support’ from colleagues and supervisors, where a double check (self-assessments and external observers) can be useful, before intervention is derived. Moreover, the results on possibilities for development and influence at work (observers rated these as lower than the employees) indicate, that especially here the involvement of external observers can be useful to design more suitable interventions.
4.1 Limitations Since a convenience sampling strategy was used, the distribution of health professions, shifts and cases per setting were not controlled and therefore some settings (e.g. psychiatric institutions) or professionals (e.g. nurses) were more dominant than others. In addition, the comparisons of the different health care settings must be interpreted with caution, as there was only a limited number of cases for each setting.
Furthermore, external observations are time and cost consuming and only a restricted range of time and participants can be observed.9 Therefore, observed data can be influenced by the duration and time (e.g. observed shift) of the external observation a longer observation period (e.g. more shifts) could possibly have produced different results.
Moreover, external observations are not seen as “objective” since external observers are individuals with their own experience, memories, perception or appraisal and therefore also can contribute a subjective bias to the data. Also, the self-report of health professionals can be influenced by their experiences (e.g. from the last two weeks). Therefore, it is not free of bias to compare employee’s self-reports and external observations. However, possible observer effects were considered when analysing the observation-based scales.
Another limitation of this study is the fact that no conclusions can be made about the influence of the self-assessed and externally observed work stressors on possible health outcomes for health professionals.
However, this study consists of valid and reliable self-assessment and observation-based scales, which scores are comparable to each other and tested in the health care sector.
5. Conclusion
These study results contribute important information for future research on work stressors in the health care sector. As the findings of this study reveal, results can strongly differ depending on which method is used to assess work stressors. This should also be considered when interpreting results about work stressors if one method is chosen only (e.g. self-reports). Especially for scales on ‘demands
Chapter 6
146
at work’, ‘possibilities for development’, ‘influence at work’ and ‘social support’, which strongly differ between self-report and external observation, a combination of both methods can provide a more detailed assessment, than using one data source only. Especially when interventions to improve health professionals ‘possibilities for development’ and ‘influence at work’ will be designed, an inclusion of both data sources such as external observers and health professionals’ self-reports could provide additional evidence. However, as this study results reveal, setting specific differences should also be kept in mind when developing interventions for different health organisations to reduce work stressors. Acknowledgements We are very grateful to all of the organisations and especially the health care staff who participated in this study, for sharing their experience and time so generously. Disclosure statement No conflict of interest has been declared by the author(s). Funding This study was financially supported by the University of Applied Sciences, Health Division, Bern, Switzerland, as well as by the State Secretariat for Education and Research of Switzerland.
Chapter 6
147
References 1. Addor V, Schwendimann R, Gauthier JA, Wernli B, Jäckel D, Paignon A. «nurses at work» –
Studie zu den Laufbahnen im Pflegeberuf über die letzten 40 Jahre in der Schweiz Neuchâtel: Schweizerisches Gesundheitsobservatorium, 2016.
2. Kraft E, Loretan L, van der Heiden N. Jeder zehnte Arzt steigt aus. Schweizerische Ärztezeitung. 2016;97(34):1132-1135.
3. Aiken LH, Sloane DM, Bruyneel L, Van den Heede K, Sermeus W, Consortium RC. Nurses' reports of working conditions and hospital quality of care in 12 countries in Europe. International Journal of Nursing Studies. 2013;50(2):143-153. doi:10.1016/j.ijnurstu.2012.11.009
4. NIOSH. Exposure to Stress: National Institute for Occupational Safety and Health, 2008. 5. Leka S, Jain A. Health impact of psychosocial hazards at work: An overview. Geneva: World
Health Organization, 2010. 6. Rau R. Befragung oder Beobachtung oder beides gemeinsam? — Welchen Instrumenten ist der
Vorzug bei Untersuchungen zur psychischen Belastung und Beanspruchung zu geben? Zentralblatt für Arbeitsmedizin, Arbeitsschutz und Ergonomie. 2014;60(9):294-301. doi:10.1007/bf03344299
7. Kompier M. Assessing the psychosocial work environment--"subjective" versus "objective" measurement. Scandinavian Journal of Work, Environment & Health. 2005;31(6):405-408.
8. Connell P, Lee VB, Spector PE. Job stress assessment methods. JC Thomas (Vol. Ed.) and M. Hersen (Ed.), Comprehensive handbook of psychological assessment: Industrial and organizational assessment. 2004;4:455-469.
9. Foster P. Observational Research. In: Sapsford R, Jupp V, eds. Data Collection and Analysis. London: SAGE, 2006: 57-92.
10. Lorenz FO, Melby JN, Conger RD, Surjadi FF. Linking questionnaire reports and observer ratings of young couples' hostility and support. Journal of Family Psychology. 2012;26(3):316-327. doi:10.1037/a0028319
11. Demerouti E. Burnout. Eine Folge konkreter Arbeitsbedingungen bei Dienstleistungs- und Produktionstätigkeiten. Frankfurt am Main: Peter Lang, 1999.
12. Spielholz P, Silverstein B, Morgan M, Checkoway H, Kaufman J. Comparison of self-report, video observation and direct measurement methods for upper extremity musculoskeletal disorder physical risk factors. Ergonomics. 2001;44(6):588-613. doi:10.1080/00140130118050
13. Semmer NK, Grebner S, Elfering A. Beyond self-report: Using observational, physiological, and situation-based measures in research on occupational stress. In: Perrewe PL, Ganster DC, eds. Research in Occupational Stress and Well Being 3ed. Amsterdam: Emerald Group Publishing Limited, 2004: 205-263.
14. Nachreiner F, Tielsch R, Gauggel B, Weiss D. Erfassung psychischer Belastung und Rückwirkung auf die Arbeitsgestaltung: Grenzen der Aussagekraft subjektiver Belastungsanalysen mithilfe von Befragungsinstrumenten aus arbeitswissenschaftlicher Sicht. Kurzfragebogen zur Erfassung psychischer Belastungen (KPB): ein Instrument zur Anwendung in der betrieblichen Praxis: Heider, 2008.
15. Büssing A, Glaser J. Das Tätigkeits-und Arbeitsanalyseverfahren für das Krankenhaus-Selbstbeobachtungsversion (TAA-KH-S): Hogrefe, 2002.
16. Hull L, Arora S, Kassab E, Kneebone R, Sevdalis N. Assessment of stress and teamwork in the operating room: an exploratory study. The American Journal of Surgery. 2011;201(1):24-30. doi:10.1016/j.amjsurg.2010.07.039
17. Stab N, Hacker W, Weigl M. Work organization in hospital wards and nurses' emotional exhaustion: A multi-method study of observation-based assessment and nurses' self-reports. International Journal of Nursing Studies. 2016;61:52-62. doi:10.1016/j.ijnurstu.2016.05.012
18. van den Hombergh P, Kunzi B, Elwyn G, van Doremalen J, Akkermans R, Grol R, et al. High workload and job stress are associated with lower practice performance in general practice: an observational study in 239 general practices in the Netherlands. BMC Health Service Research. 2009;9(1):118-126. doi:10.1186/1472-6963-9-118
19. Wheelock A, Suliman A, Wharton R, Babu ED, Hull L, Vincent C, et al. The Impact of Operating Room Distractions on Stress, Workload, and Teamwork. Annals of surgery. 2015;261(6):1079-1084. doi:10.1097/SLA.0000000000001051
Chapter 6
148
20. Golz C, Peter KA, Hahn S. Cognitive Pretesting and pretest of the STRAIN questionnaire to elaborate work-related stress of health care staff in Switzerland. International Journal of Health Professions. 2018;5(1):109-120. doi:10.2478/ijhp-2018-0011
21. Nübling M, Stössel U, Hasselhorn HM, Michaelis M, Hofmann F. Measuring psychological stress and strain at work: Evaluation of the COPSOQ Questionnaire in Germany. GMS Psycho-Social-Medicine. 2006;3:1-14.
22. Nübling M, Stößel U, Hasselhorn HM, Michaelis M, Hofmann F. Methoden zur Erfassung psychischer Belastungen: Erprobung eines Messinstruments (COPSOQ). Dortmund: Bundesanstalt für Arbeitsschutz und Arbeitsmedizin, 2005.
23. Eurofound. Sixth European Working Conditions Survey - Questionnaire. Luxembourg: Publications Office of the European Union, 2015.
24. Parent-Thirion A, Fernández Macías E, Hurley J, Vermeylen G. Fourth European Working Conditions Survey. Luxembourg: European Foundation for the Improvement of Living and Working Conditions, 2007.
25. Monahan T, Fisher JA. Benefits of "Observer Effects": Lessons from the Field. Qualitative Research. 2010;10(3):357-376. doi:10.1177/1468794110362874
26. Frese M, Zapf D. Methodological issues in the study of work stress: Objective vs. subjective measurement of work stress and the question of longitudinal studies. In: Cooper CL, Payne R, eds. Causes, coping and consequences of stress at work. Chichester: John Wiley & Sons, 1988: 375–411.
27. Guest G, Namey EE, Mitchell ML. Collecting Qualitative Data: A Field Manual for Applied Research. London: SAGE Publications, 2013.
28. Parker CP, Baltes BB, Young SA, Huff JW, Altmann RA, Lacost HA, et al. Relationships between psychological climate perceptions and work outcomes: a meta-analytic review. Journal of Organizational Behavior. 2003;24(4):389-416. doi:10.1002/job.198
29. Glick WH, Jenkins JGD, Gupta N. Method Versus Substance: How Strong Are Underlying Relationships between Job Characteristics and Attitudinal Outcomes? Academy of Management Journal. 1986;29(3):441-464. doi:10.2307/256218
Chapter 7
General Discussion
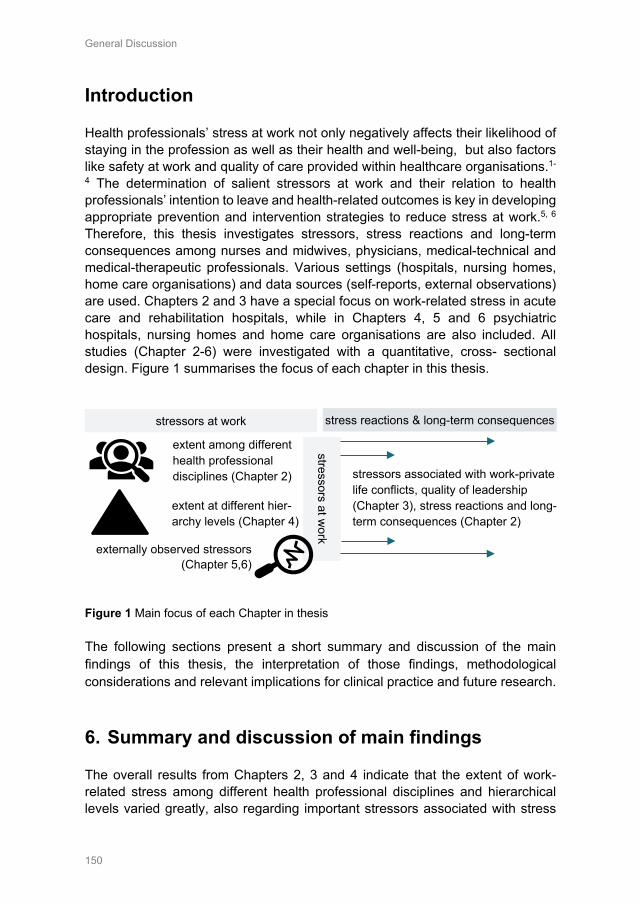
General Discussion
150
Introduction
Health professionals’ stress at work not only negatively affects their likelihood of staying in the profession as well as their health and well-being, but also factors like safety at work and quality of care provided within healthcare organisations.1-
4 The determination of salient stressors at work and their relation to health professionals’ intention to leave and health-related outcomes is key in developing appropriate prevention and intervention strategies to reduce stress at work.5, 6 Therefore, this thesis investigates stressors, stress reactions and long-term consequences among nurses and midwives, physicians, medical-technical and medical-therapeutic professionals. Various settings (hospitals, nursing homes, home care organisations) and data sources (self-reports, external observations) are used. Chapters 2 and 3 have a special focus on work-related stress in acute care and rehabilitation hospitals, while in Chapters 4, 5 and 6 psychiatric hospitals, nursing homes and home care organisations are also included. All studies (Chapter 2-6) were investigated with a quantitative, cross- sectional design. Figure 1 summarises the focus of each chapter in this thesis.
Figure 1 Main focus of each Chapter in thesis The following sections present a short summary and discussion of the main findings of this thesis, the interpretation of those findings, methodological considerations and relevant implications for clinical practice and future research.
6. Summary and discussion of main findings
The overall results from Chapters 2, 3 and 4 indicate that the extent of work-related stress among different health professional disciplines and hierarchical levels varied greatly, also regarding important stressors associated with stress
stressors at work
extent among different health professional disciplines (Chapter 2)
extent at different hier-archy levels (Chapter 4)
externally observed stressors (Chapter 5,6)
stressors at work stress reactions & long-term consequences
stressors associated with work-private life conflicts, quality of leadership (Chapter 3), stress reactions and long-term consequences (Chapter 2)

General Discussion
151
reactions and long-term consequences among nurses and midwives, physicians, medical-technical and medical-therapeutic professionals.
6.1 Extent of stressors among different disciplines Main findings on the extent of stressors among health professionals working in Swiss acute care and rehabilitation hospitals (Chapter 2) indicate that nurses and midwives’ are mostly affected by emotional and physical demands, role conflicts, fewer opportunities for development and lower scope for breaks and holidays at work. Physicians reported being more affected by quantitative demands, role conflicts, work-private life conflicts and lower role clarity at work. Medical-technical professionals seemed to be mostly affected by a demanding work environment, fewer opportunities for development and lack of influence at work, while medical-therapeutic professionals complained of lower scope for breaks and holidays, lack of cognitive demands, social relations and role clarity at work. Previous studies also identified varying extents of work stressors among different health professionals, and presented similar results regarding how nurses’ and physicians’ are affected by stressors at work 8, 9. Overall, the results indicate how important it is to develop profession-specific strategies to prevent and reduce stress at work, shaped to the working conditions of each health profession separately.
6.2 Extent of stressors among different hierarchies The main findings on the extent of stressors at work at different management levels (Chapter 4) indicate that stressors at work are experienced to a larger extent among health professionals at lower-management levels, and especially among those without management responsibilities (see Figure 2). These results refer to hospitals, nursing homes and home care organisations.
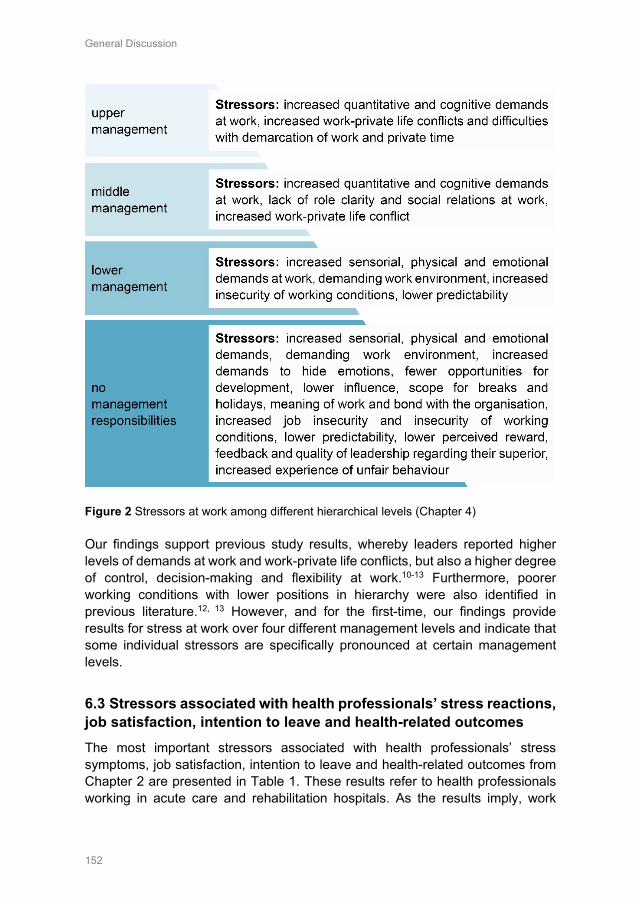
General Discussion
152
Figure 2 Stressors at work among different hierarchical levels (Chapter 4) Our findings support previous study results, whereby leaders reported higher levels of demands at work and work-private life conflicts, but also a higher degree of control, decision-making and flexibility at work.10-13 Furthermore, poorer working conditions with lower positions in hierarchy were also identified in previous literature.12, 13 However, and for the first-time, our findings provide results for stress at work over four different management levels and indicate that some individual stressors are specifically pronounced at certain management levels.
6.3 Stressors associated with health professionals’ stress reactions, job satisfaction, intention to leave and health-related outcomes The most important stressors associated with health professionals’ stress symptoms, job satisfaction, intention to leave and health-related outcomes from Chapter 2 are presented in Table 1. These results refer to health professionals working in acute care and rehabilitation hospitals. As the results imply, work

General Discussion
153
stressors are of different relevance regarding their association with stress reactions and long-term consequences among nurses and midwives, physicians, medical-therapeutic and medical-technical professionals, which is in line with previous study results.8 Health professionals are confronted with different stressors at work regarding their professional role and work environment8, 14-17, which indicates different needs for action when developing strategies to prevent and reduce stress at work.
However, our results also identified stressors that proved to be of common relevance for all health professionals, such as existing work-private life conflicts, the lack of opportunities for development and the behaviour of the direct line manager (Chapter 2). Previous studies also identified existing work-private life conflicts, insufficient opportunities for development and poor leadership qualities as being associated with health professionals’ intention to leave.4, 18-21 Furthermore, our study results add to relevant knowledge regarding stressors associated with stress symptoms, job satisfaction, general health status and quality of sleep among nurses and midwives, physicians, medical-therapeutic and medical-technical professionals. The results indicate that, although many stressors are specific to a health professional’s role and work environment, effective strategies for reducing work-private life conflicts, enhancing opportunities for development and the quality of leadership, could overall contribute to a better and healthier working environment in Swiss acute care and rehabilitation hospitals.
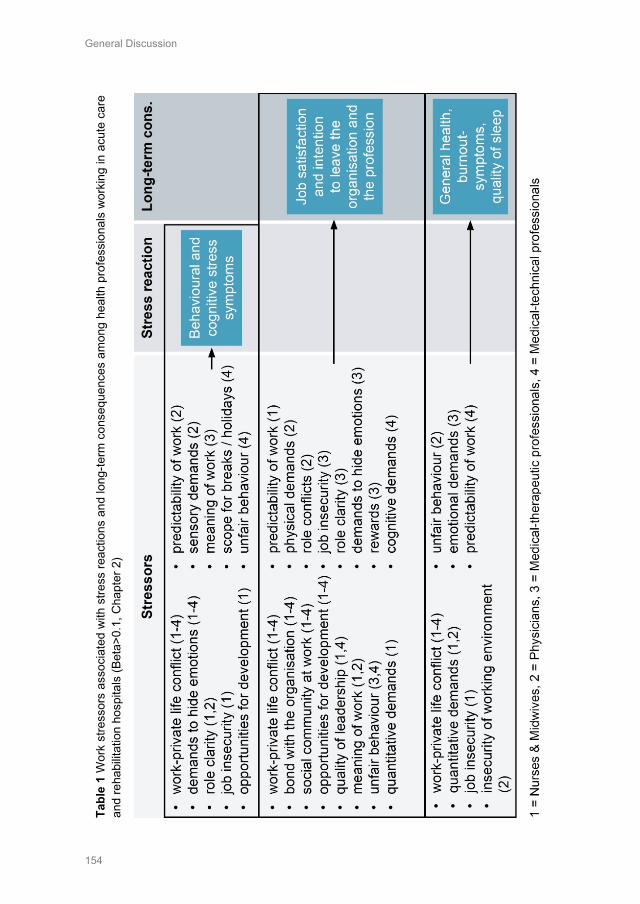
General Discussion
154
Ta
ble
1 W
ork
stre
ssor
s as
soci
ated
with
stre
ss re
actio
ns a
nd lo
ng-te
rm c
onse
quen
ces
amon
g he
alth
pro
fess
iona
ls w
orki
ng in
acu
te c
are
and
reha
bilit
atio
n ho
spita
ls (B
eta>
0.1,
Cha
pter
2)
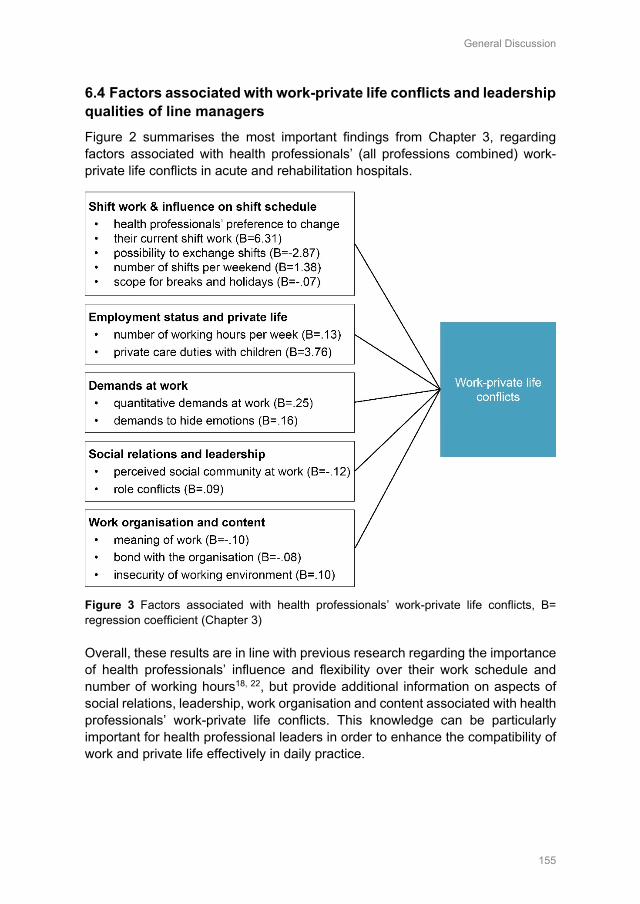
General Discussion
155
6.4 Factors associated with work-private life conflicts and leadership qualities of line managers Figure 2 summarises the most important findings from Chapter 3, regarding factors associated with health professionals’ (all professions combined) work-private life conflicts in acute and rehabilitation hospitals.
Figure 3 Factors associated with health professionals’ work-private life conflicts, B= regression coefficient (Chapter 3) Overall, these results are in line with previous research regarding the importance of health professionals’ influence and flexibility over their work schedule and number of working hours18, 22, but provide additional information on aspects of social relations, leadership, work organisation and content associated with health professionals’ work-private life conflicts. This knowledge can be particularly important for health professional leaders in order to enhance the compatibility of work and private life effectively in daily practice.
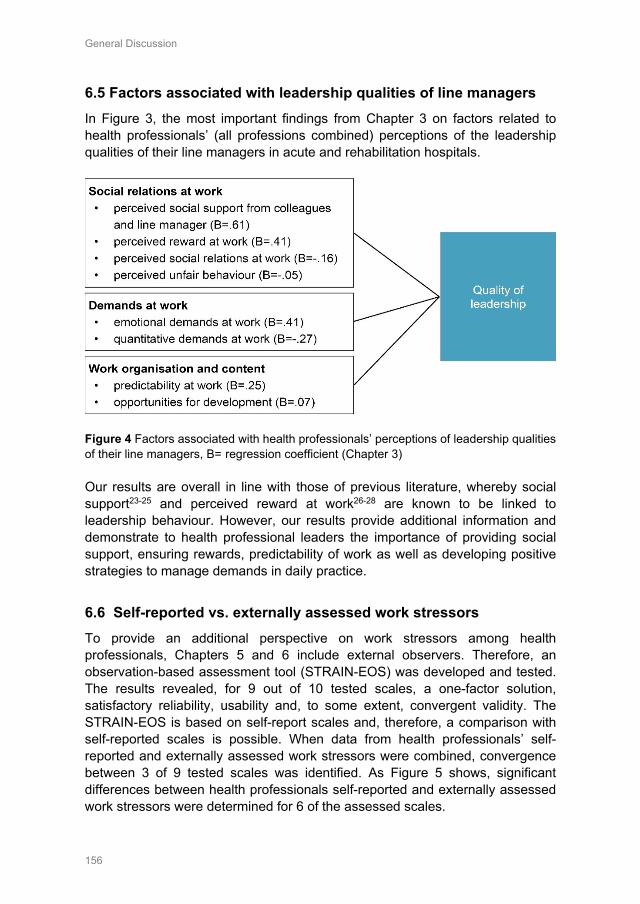
General Discussion
156
6.5 Factors associated with leadership qualities of line managers In Figure 3, the most important findings from Chapter 3 on factors related to health professionals’ (all professions combined) perceptions of the leadership qualities of their line managers in acute and rehabilitation hospitals.
Figure 4 Factors associated with health professionals’ perceptions of leadership qualities of their line managers, B= regression coefficient (Chapter 3) Our results are overall in line with those of previous literature, whereby social support23-25 and perceived reward at work26-28 are known to be linked to leadership behaviour. However, our results provide additional information and demonstrate to health professional leaders the importance of providing social support, ensuring rewards, predictability of work as well as developing positive strategies to manage demands in daily practice.
6.6 Self-reported vs. externally assessed work stressors To provide an additional perspective on work stressors among health professionals, Chapters 5 and 6 include external observers. Therefore, an observation-based assessment tool (STRAIN-EOS) was developed and tested. The results revealed, for 9 out of 10 tested scales, a one-factor solution, satisfactory reliability, usability and, to some extent, convergent validity. The STRAIN-EOS is based on self-report scales and, therefore, a comparison with self-reported scales is possible. When data from health professionals’ self-reported and externally assessed work stressors were combined, convergence between 3 of 9 tested scales was identified. As Figure 5 shows, significant differences between health professionals self-reported and externally assessed work stressors were determined for 6 of the assessed scales.
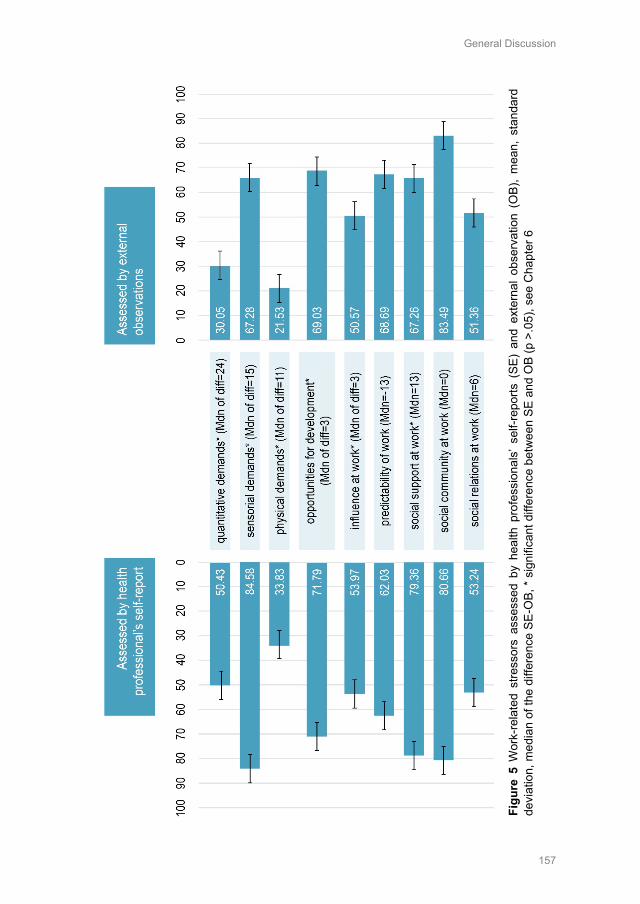
General Discussion
157
Figu
re 5
Wor
k-re
late
d st
ress
ors
asse
ssed
by
heal
th p
rofe
ssio
nals
’ sel
f-rep
orts
(SE
) an
d ex
tern
al o
bser
vatio
n (O
B),
mea
n, s
tand
ard
devi
atio
n, m
edia
n of
the
diffe
renc
e SE
-OB,
* si
gnifi
cant
diff
eren
ce b
etw
een
SE a
nd O
B (p
>.0
5), s
ee C
hapt
er 6

General Discussion
158
Our results appear to be in line with previous literature; Semmer and colleagues29 stated that convergence between observation-based and self-reported assessment is often modest (between 10-30%). Also, some authors suggest that self-reported demands at work are overestimated and observed demands at work are underestimated.29-31 It is possible that the ‘initial level’ of perceived stressors is not the same if, for example, an employee is already exposed to work stressors over a longer period. External observers, on the other hand, have only a limited picture regarding time and duration of their observations and, therefore, may assess the work environment as being less demanding.29 In contrast, external observers rated opportunities for development, their influence and social support as being lower than the observed health professionals did. However, perceived supportive behaviour appears more likely to be remembered (regarding self-reports) and also, it may be more difficult to observe externally.32 Therefore, assessments by health professionals and external observers may not be based on exactly the same situations or experiences.32 In general, regarding the differences between health professionals’ and external observers’ ratings of work stressors, one could conclude that one data source is more valid than another or captures the true value. Semmer and his colleagues29 state that both methods include ‘true variance’ as well as possible biasing effects and, therefore, it is more likely that each source of data captures the same approach in a different way or perception.33 In addition, our study results revealed overall that results on work stressors can be influenced by the method of data source chosen, which one’ should keep in mind when using one source of data only.
7. Interpretation
The interpretation of results generated in this thesis focuses first on acute and rehabilitation hospitals, as this represents the common intersection of all articles. In a further step, however, important implications for practice with regard to all included areas of health care are shown.
7.1 Comparison to other countries and professions To interpret the results of the extent of stress at work among Swiss health professionals in acute care and rehabilitation hospitals, a comparison with other countries is important. We found a study from Germany (n=995)9 and Portugal (n=1016)34, which also used the COPSOQ, was conducted in the hospital setting and included various types of health professionals, which is therefore comparable with our results (n=3398, Chapter 2). However, when comparing results on work-related stress among countries, the available resources (e.g. available hospital beds and health professionals) in the different health care systems should also be considered. Current published indicators from the Organisation for Economic
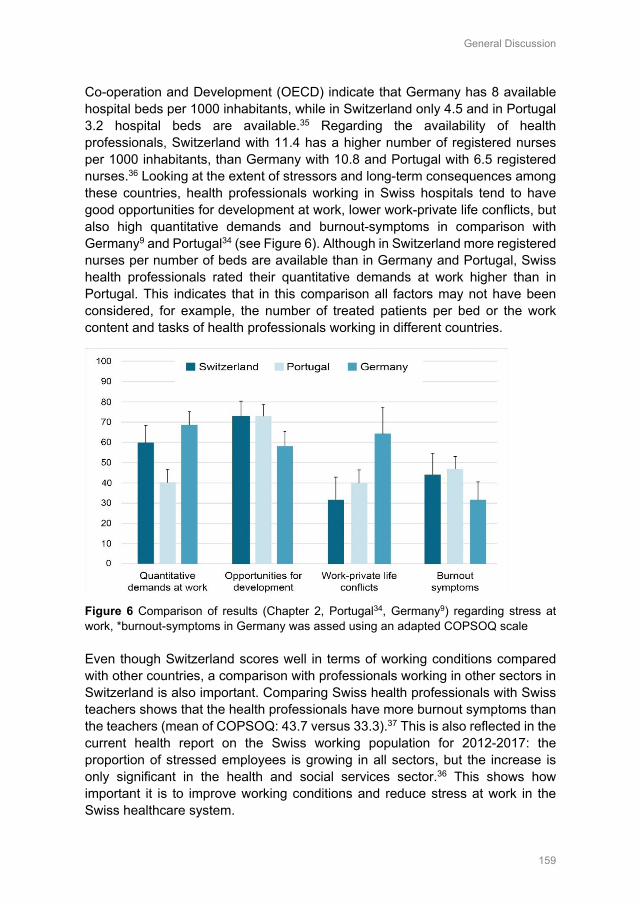
General Discussion
159
Co-operation and Development (OECD) indicate that Germany has 8 available hospital beds per 1000 inhabitants, while in Switzerland only 4.5 and in Portugal 3.2 hospital beds are available.35 Regarding the availability of health professionals, Switzerland with 11.4 has a higher number of registered nurses per 1000 inhabitants, than Germany with 10.8 and Portugal with 6.5 registered nurses.36 Looking at the extent of stressors and long-term consequences among these countries, health professionals working in Swiss hospitals tend to have good opportunities for development at work, lower work-private life conflicts, but also high quantitative demands and burnout-symptoms in comparison with Germany9 and Portugal34 (see Figure 6). Although in Switzerland more registered nurses per number of beds are available than in Germany and Portugal, Swiss health professionals rated their quantitative demands at work higher than in Portugal. This indicates that in this comparison all factors may not have been considered, for example, the number of treated patients per bed or the work content and tasks of health professionals working in different countries.
Figure 6 Comparison of results (Chapter 2, Portugal34, Germany9) regarding stress at work, *burnout-symptoms in Germany was assed using an adapted COPSOQ scale Even though Switzerland scores well in terms of working conditions compared with other countries, a comparison with professionals working in other sectors in Switzerland is also important. Comparing Swiss health professionals with Swiss teachers shows that the health professionals have more burnout symptoms than the teachers (mean of COPSOQ: 43.7 versus 33.3).37 This is also reflected in the current health report on the Swiss working population for 2012-2017: the proportion of stressed employees is growing in all sectors, but the increase is only significant in the health and social services sector.36 This shows how important it is to improve working conditions and reduce stress at work in the Swiss healthcare system.
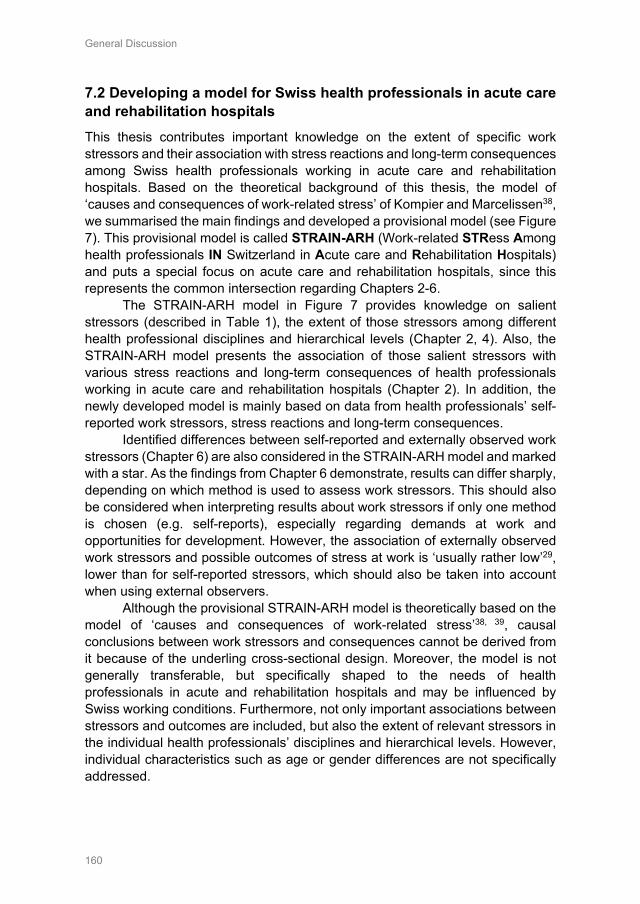
General Discussion
160
7.2 Developing a model for Swiss health professionals in acute care and rehabilitation hospitals This thesis contributes important knowledge on the extent of specific work stressors and their association with stress reactions and long-term consequences among Swiss health professionals working in acute care and rehabilitation hospitals. Based on the theoretical background of this thesis, the model of ‘causes and consequences of work-related stress’ of Kompier and Marcelissen38, we summarised the main findings and developed a provisional model (see Figure 7). This provisional model is called STRAIN-ARH (Work-related STRess Among health professionals IN Switzerland in Acute care and Rehabilitation Hospitals) and puts a special focus on acute care and rehabilitation hospitals, since this represents the common intersection regarding Chapters 2-6.
The STRAIN-ARH model in Figure 7 provides knowledge on salient stressors (described in Table 1), the extent of those stressors among different health professional disciplines and hierarchical levels (Chapter 2, 4). Also, the STRAIN-ARH model presents the association of those salient stressors with various stress reactions and long-term consequences of health professionals working in acute care and rehabilitation hospitals (Chapter 2). In addition, the newly developed model is mainly based on data from health professionals’ self-reported work stressors, stress reactions and long-term consequences.
Identified differences between self-reported and externally observed work stressors (Chapter 6) are also considered in the STRAIN-ARH model and marked with a star. As the findings from Chapter 6 demonstrate, results can differ sharply, depending on which method is used to assess work stressors. This should also be considered when interpreting results about work stressors if only one method is chosen (e.g. self-reports), especially regarding demands at work and opportunities for development. However, the association of externally observed work stressors and possible outcomes of stress at work is ‘usually rather low’29, lower than for self-reported stressors, which should also be taken into account when using external observers.
Although the provisional STRAIN-ARH model is theoretically based on the model of ‘causes and consequences of work-related stress’38, 39, causal conclusions between work stressors and consequences cannot be derived from it because of the underling cross-sectional design. Moreover, the model is not generally transferable, but specifically shaped to the needs of health professionals in acute and rehabilitation hospitals and may be influenced by Swiss working conditions. Furthermore, not only important associations between stressors and outcomes are included, but also the extent of relevant stressors in the individual health professionals’ disciplines and hierarchical levels. However, individual characteristics such as age or gender differences are not specifically addressed.
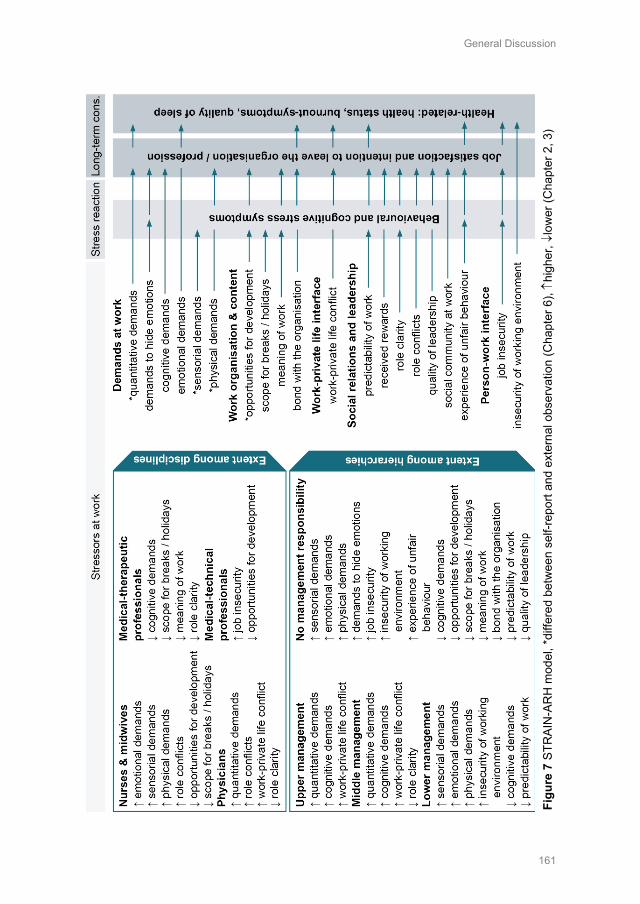
General Discussion
161
Figu
re 7
STR
AIN
-AR
H m
odel
, *di
ffere
d be
twee
n se
lf-re
port
and
exte
rnal
obs
erva
tion
(Cha
pter
6), ↑
high
er, ↓
low
er (C
hapt
er 2
, 3)
General Discussion
162
8. Methodological considerations, strengths, and limitations
8.1 Methodological considerations Overall, this thesis is based on quantitative, cross-sectional data and regression models were often used for data analysis (Chapters 2, 3, 4, 6). In order to avoid mixing stressors and strain reactions40, a well-established and comprehensive theoretical background, the ‘model of causes and consequences of work-related stress’38, 41 was used to guide this thesis from the beginning. This is also supported by the use of widely used and well-designed scales/ questionnaires in (e.g. the COPSOQ42, Work-ability Index43).
In order to provide a comprehensive first overview, this thesis starts with the extent of stress at work as well as stressors associated with stress reactions and long-term consequences among different health professional disciplines (Chapter 2). Chapter 3 further investigates two important stressors identified in Chapter 2. Therefore, the two stressors (work-private life conflicts, quality of leadership) were used as outcomes, while other stressors were used as predictors, taking into account interactions between these stressors. Chapter 4 further focuses on leaders but provides knowledge on the extent of stress at different hierarchical levels and, therefore, also discloses working conditions and strain among leaders themselves.
The results of these three chapters started with findings based on employees’ self-reports, since they are widely used (comparability) and provide insight into internal psychological states of employees.39, 44 In order to provide a further perspective on work stressors, external observers were included (Chapter 5, 6). Although, using external observations in the healthcare sector was challenging, for example, assessing interobserver reliability, dealing with privacy of patients, emergency situations or observed violations of safety measures, this additional perspective was important from a methodological point of view.29 Especially the results on the combination of external observation and health professionals’ self-reports (Chapter 6) determined further knowledge on how much these two perspectives can differ, and that the selected source of data collection can influence the results. However, no data source was considered to be more valid or the true reality29 in this thesis, but, rather, both were included and discussed as different perspectives.
8.2 Strengths This thesis provides, for the first time, detailed data on work-related stress, addressing different health professionals’ disciplines and four different hierarchical levels separately. Also, this thesis included health professionals’ self-
General Discussion
163
reports, but also provides an additional perspective on work stressors by using external observations. Furthermore, this thesis presents a newly developed and tested observation-based measure, especially shaped to assess work stressors in the healthcare sector (STRAIN-EOS) and one that is comparable with employees’ self-reports.
In addition, the results from Chapters 2, 3 and 4 are based on a sufficiently large randomised sample for different health professionals’ disciplines and Swiss language regions (German- and French-speaking part). Furthermore, this thesis is based on a strong theoretical background and includes valid and reliable self-report45-49 scales, which are well established and comparable with national and international studies. Finally, this thesis provides a provisionally developed model, the STRAIN-ARH, and uses state-of-the-art statistical data analysis methods.
8.3 Limitations An obvious limitation of this thesis is that the results are based on a cross-sectional design, which means that no causal conclusions can be drawn (also regarding the provisional STRAIN-ARH in Figure 7). In addition, the thesis focuses on work-related stress in acute care and rehabilitation hospitals in Chapters 2 and 3. Therefore, only limited conclusions can be drawn from the results of those two chapters about work-related stress in other healthcare settings. Also, different health professionals’ disciplines (nurses & midwives, physicians, medical-technical, medical-therapeutic professions) were considered and analysed separately only in Chapter 2. In Chapters 3, 4, 5 and 6 all health professional disciplines were combined into one group for data analysis, which limits the transferability of the results in those chapters to individual professions or disciplines.
Regarding the selected source of data, the results from Chapters 2-4 are based on self-assessments by employees and are therefore not free from the potential biases and errors characteristic of self-reports (e.g. social desirability, negative affectivity).29, 40 This also applies to chapters 5-6, where external observations were used, which may also contain potential biases and errors (e.g. halo-effect, influence of common stereotypes).29 In addition, the results of this thesis are limited to those two data sources; the inclusion of a further data source (e.g. situation-based measures, physiological measures) might have provided additional information and, therefore, would possibly have influenced the interpretation of the results.
Although these healthcare organisations were randomly selected, a selection bias cannot be excluded. Furthermore, all results of this thesis are based on data from the Swiss healthcare sector and thus influenced by Swiss labour law (e.g. regarding working hours). Therefore, results from other country might differ.
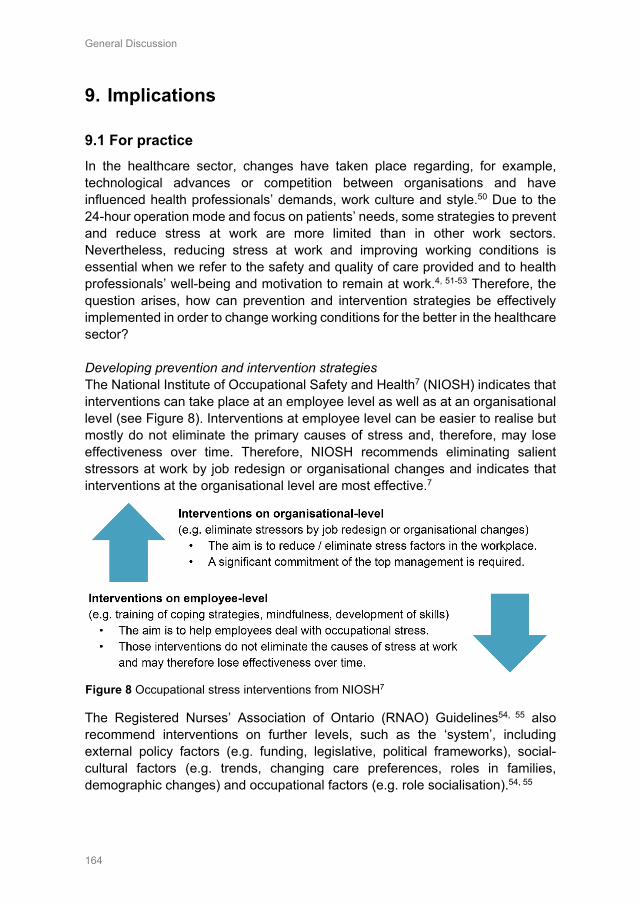
General Discussion
164
9. Implications
9.1 For practice In the healthcare sector, changes have taken place regarding, for example, technological advances or competition between organisations and have influenced health professionals’ demands, work culture and style.50 Due to the 24-hour operation mode and focus on patients’ needs, some strategies to prevent and reduce stress at work are more limited than in other work sectors. Nevertheless, reducing stress at work and improving working conditions is essential when we refer to the safety and quality of care provided and to health professionals’ well-being and motivation to remain at work.4, 51-53 Therefore, the question arises, how can prevention and intervention strategies be effectively implemented in order to change working conditions for the better in the healthcare sector? Developing prevention and intervention strategies The National Institute of Occupational Safety and Health7 (NIOSH) indicates that interventions can take place at an employee level as well as at an organisational level (see Figure 8). Interventions at employee level can be easier to realise but mostly do not eliminate the primary causes of stress and, therefore, may lose effectiveness over time. Therefore, NIOSH recommends eliminating salient stressors at work by job redesign or organisational changes and indicates that interventions at the organisational level are most effective.7
The Registered Nurses’ Association of Ontario (RNAO) Guidelines54, 55 also recommend interventions on further levels, such as the ‘system’, including external policy factors (e.g. funding, legislative, political frameworks), social-cultural factors (e.g. trends, changing care preferences, roles in families, demographic changes) and occupational factors (e.g. role socialisation).54, 55
Figure 8 Occupational stress interventions from NIOSH7
General Discussion
165
Implications for health organisations and leaders To achieve a good and healthy work environment in the organisation, health professional leaders play an essential role. Especially regarding their significant commitment to effective prevention and intervention strategies7, their influence and shaping of culture within the organisation7, 56, leadership skills and abilities as well as their action as a role model of how to deal with stress at work (Chapters 2, 3 & 4). Therefore, healthcare organisations should recruit leaders with positive leadership traits and a focus on improving health professionals’ job satisfaction and well-being.56 Organisational policies and communication strategies, including a proactive and visible commitment to employees’ health and safety at work as part of the organisational culture, are also essential56 and should address the following topics:
- Ensure that employees work reasonable hours, have regular breaks and sufficient rest periods with a special focus on leaders’ compliance with legal break and rest periods as well as avoiding/reducing overtime7, 56 (Chapter 3).
- Ensure an optimal compatibility of work and private life among health professionals, e.g. employee-friendly shift schedule and considering individual preferences, enable part-time work with attractive working hours for health professionals at different stages of life and hierarchy and develop a family-supportive leadership behaviour18, 57, 58 (Chapter 2,3,4).
- Ensure an appropriate management of health professionals’ workload; therefore, health professionals’ quantitative demands should be in line with their capabilities and resources at work56, 59 (Chapters 2, 3).
- Ensure an organisational climate that encourages health professionals to express their opinions and ideas for a better working environment, involve them in decisions affecting their work at all levels of hierarchy and develop a constructive feedback and error culture that is open and guided by respect with a focus on continuously improving systems and processes within the organisation7, 60 (Chapter 2,3,4).
- Ensure support options regarding health professionals’ physical (e.g. back friendly working techniques) and emotional demands (e.g. offering supervision or debriefing sessions) at work54, 56 (Chapter 2,3,4).
- Ensure clearly defined roles and responsibilities within each health profession (e.g. nurses/physicians at different skill levels) as well as for cooperation within an interdisciplinary team, and provide opportunities for social interactions7, 61 (Chapter 2,3,4).
- Ensure good possibilities for development among all health professionals’ disciplines (e.g. by additional education opportunities, enhancement of professional competencies)7, 54, provide clear career development and
General Discussion
166
employment relationships as well as future employment prospects free from uncertainty, with a focus on improving health professionals’ commitment and binding to the organisation7 (Chapter 2,3,4).
Furthermore, prevention and intervention strategies reducing stress at work should also consider the role and work environment of health professionals working in different hierarchies and professional disciplines (Chapters 2,4). In addition, care should be taken to regularly assess the level of work-related stress, using valid and reliable measures to assess the extent of stressors at work, stress reactions and long-term consequences within the organisation.54, 62 Implementation of prevention and intervention strategies When implementing effective prevention and intervention strategies in health care organisations, several key elements are recommended: • Management commitment and prioritisation – The management plays a
key role in whether the intervention will succeed.7 A significant commitment especially by the top management, but also by all leaders within the organisation to support and implement organisational interventions is therefore important.7, 54, 56, 62 In addition, the health and well-being of employees should be a core priority for the top management.56
• Environmental readiness - An organisational culture that supports interventions to reduce stress seems to be essential for success7, 62 and also, the intervention should be tailored to the local context, barriers and facilitators should be assessed and adequate resources for the implementation should be available.54, 56
• Participatory process – Several guidelines state that the involvement of employees in all phases of the intervention (development, action planning, implementation, evaluation) is important for whether the intervention can be successfully implemented in the organisation.7, 51, 54-56, 62
• Promotion and Communication – The raising of awareness and appropriate promotion of the guideline/intervention through routine communication channels, meetings or internal staff briefings is recommended54, 56, 62 as well as creating a clear communication of realistic expectations.56
• Evaluation – A primary baseline assessment and subsequent regular evaluation of the implementation process and impact of the interventions for stress reduction is also recommended7, 51, 54, 56, 62 as well as the direct involvement and support of the line manager in this activity.56
General Discussion
167
9.2 For research The results of this thesis were generated in Swiss hospitals (Chapters 2,3), nursing homes and home care organisations (Chapters 4,5,6) and are to some extent influenced by the labour laws and cultural factors of Switzerland. Therefore, further studies, for example, regarding associated factors of health professionals’ work-private life conflicts or perceived leadership qualities of their line manager in different countries, are needed to confirm and compare our findings. Also, international comparisons of work-related stress among health professionals are important, considering, for example, available resources in the healthcare system or roles and job content of health professionals.
In addition, Chapters 2 and 3 focus on work-related stress in acute care and rehabilitation hospitals only. Therefore, further research is needed regarding the extent of work-related stress as well as stressors associated with health professionals’ stress reactions and long-term consequences in other healthcare settings (e.g. psychiatric hospitals, nursing homes, home care organisations).
Furthermore, our results regarding stressors associated with health professionals’ satisfaction, intention to leave and health-related outcomes from Chapter 2, are divided into the four disciplines of nurses and midwives, physicians, medical-technical and medical-therapeutic professionals. Therefore, further research is necessary among other health professionals (e.g. physiotherapists, nutrition therapists) separately with a sufficiently large sample for each profession.
In addition, further research using longitudinal data is needed, especially to confirm our findings regarding stressors and their influence on possible outcomes in the provisional STRAIN-ARH model and results from Chapter 2 and 3. Also, the use of additional data sources (e.g. situation-based measures) could provide further insights on work-related stress among Swiss health professionals.
In order to improve health professionals’ work environment, intervention studies could provide further knowledge on more effective prevention and intervention strategies in daily practice. Our results implied the relevance of health professionals’ compatibility of work and private life as well as the important role of health professionals’ leaders (Chapter 2,3,4). Therefore, further research is needed to develop and test interventions focused on the improvement of health professionals’ compatibility of work and private life, e.g. by testing more flexible work-time designs. Also, further studies are needed regarding the culture within the organisation, how work-private life conflicts of health professionals’ is addressed (e.g. doing overtime is considered good performance). In addition, qualitative studies could provide further knowledge, focusing on leaders’ attitudes, beliefs, skills and self-efficacy regarding stress at work. Moreover, further research is needed regarding barriers in daily practice that keep leaders from effectively implementing prevention and intervention strategies for reducing stress at work among themselves and their subordinate employees at all hierarchic levels.
General Discussion
168
References 1. Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient
mortality, nurse burnout, and job dissatisfaction. Journal of the American Medical Association. 2002;288(16):1987-1993. doi:10.1001/jama.288.16.1987
2. Aiken LH, Sermeus W, Van den Heede K, Sloane DM, Busse R, McKee M, et al. Patient safety, satisfaction, and quality of hospital care: cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ. 2012;344:e1717. doi:10.1136/bmj.e1717
3. Aiken LH, Sloane DM, Bruyneel L, Van den Heede K, Sermeus W, Consortium RC. Nurses' reports of working conditions and hospital quality of care in 12 countries in Europe. International Journal of Nursing Studies. 2013;50(2):143-153. doi:10.1016/j.ijnurstu.2012.11.009
4. Hämmig O. Explaining burnout and the intention to leave the profession among health professionals - a cross-sectional study in a hospital setting in Switzerland. BMC Health Service Research. 2018;18(1):785. doi:10.1186/s12913-018-3556-1
5. Ruotsalainen J, Serra C, Marine A, Verbeek J. Systematic review of interventions for reducing occupational stress in health care workers. Scandinavian Journal of Work, Environment & Health. 2008;34(3):169-178. doi:10.5271/sjweh.1240
6. Ruotsalainen JH, Verbeek JH, Marine A, Serra C. Preventing occupational stress in healthcare workers. Cochrane Database of Systematic Reviews. 2014(11):Cd002892. doi:10.1002/14651858.CD002892.pub3
7. NIOSH. Exposure to Stress: National Institute for Occupational Safety and Health, 2008. 8. Gilles I, Burnand B, Peytremann-Bridevaux I. Factors associated with healthcare professionals'
intent to stay in hospital: a comparison across five occupational categories. International Journal for Quality in Health Care. 2014;26(2):158-166. doi:10.1093/intqhc/mzu006
9. Wagner A, Rieger MA, Manser T, Sturm H, Hardt J, Martus P, et al. Healthcare professionals’ perspectives on working conditions, leadership, and safety climate: a cross-sectional study. BMC Health Services Research. 2019;19(1):53. doi:10.1186/s12913-018-3862-7
10. Bernin P, Theorell T. Demand–control–support among female and male managers in eight Swedish companies. Stress and Health. 2001;17:231–243. doi:10.1002/smi.905
11. Kossek E, Lautsch B. Work-Life Flexibility for Whom? Occupational Status and Work-Life Inequality in Upper, Middle, and Lower Level Jobs. Academy of Management Annals. 2017;12:1-76. doi:10.5465/annals.2016.0059
12. Lundqvist D, Reineholm C, Gustavsson M, Ekberg K. Investigating work conditions and burnout at three hierarchical levels. J Occup Environ Med. 2013;55(10):1157-1163. doi:10.1097/JOM.0b013e31829b27df
13. Skakon J, Kristensen TS, Christensen KB, Lund T, Labriola M. Do managers experience more stress than employees? Results from the Intervention Project on Absence and Well-being (IPAW) study among Danish managers and their employees. Work. 2011;38(2):103-109. doi:10.3233/wor-2011-1112
14. Fileni A, Magnavita N, Mammi F, Mandoliti G, Luca F, Magnavita G, et al. Malpractice stress syndrome in radiologists and radiotherapists: perceived causes and consequences. Radiol Med. 2007;112(7):1069-1084. doi:10.1007/s11547-007-0206-9
15. Magnavita N, Fileni A, Magnavita G, Mammi F, Mirk P, Roccia K, et al. Work stress in radiologists. A pilot study. La radiologia medica. 2008;113(3):329-346. doi:10.1007/s11547-008-0259-4
16. Hahn S, Hantikainen V, Needham I, Kok G, Dassen T, Halfens RJ. Patient and visitor violence in the general hospital, occurrence, staff interventions and consequences: a cross-sectional survey. Journal of advanced nursing. 2012;68(12):2685-2699. doi:10.1111/j.1365-2648.2012.05967.x
17. Magnavita N. The Exploding Spark: Workplace Violence in an Infectious Disease Hospital—A Longitudinal Study. BioMed Research International. 2013;2013:1-9. doi:10.1155/2013/316358
18. Albertsen K, Rafnsdottir GL, Grimsmo A, Tomasson K, Kauppinen K. Workhours and worklife balance. Scandinavian Journal of Work Environment & Health. 2008;5:14-21.
19. Lee R, Seo B, Hladkyj S, Lovell BL, Schwartzmann L. Correlates of physician burnout across regions and specialties: a meta-analysis. Human Resources for Health. 2013;11(1):48. doi:10.1186/1478-4491-11-48
20. Flinkman M, Laine M, Leino-Kilpi H, Hasselhorn HM, Salanterä S. Explaining young registered Finnish nurses’ intention to leave the profession: A questionnaire survey. International Journal of Nursing Studies. 2008;45(5):727-739. doi:10.1016/j.ijnurstu.2006.12.006
General Discussion
169
21. Lavoie-Tremblay M, Fernet C, Lavigne GL, Austin S. Transformational and abusive leadership practices: impacts on novice nurses, quality of care and intention to leave. Journal of advanced nursing. 2016;72(3):582-592. doi:10.1111/jan.12860
22. Dhaini SR, Denhaerynck K, Bachnick S, Schwendimann R, Schubert M, De Geest S, et al. Work schedule flexibility is associated with emotional exhaustion among registered nurses in Swiss hospitals: A cross-sectional study. International Journal of Nursing Studies. 2018;82:99-105. doi:10.1016/j.ijnurstu.2018.03.019
23. Backman A, Sjogren K, Lovheim H, Edvardsson D. Job strain in nursing homes-Exploring the impact of leadership. Journal of clinical nursing. 2018;27(7-8):1552-1560. doi:10.1111/jocn.14180
24. Gilbreath B, Benson PG. The contribution of supervisor behaviour to employee psychological well-being. Work and Stress. 2004;18(3):255-266. doi:10.1080/02678370412331317499
25. Van der Heijden BI, Mulder RH, Konig C, Anselmann V. Toward a mediation model for nurses' well-being and psychological distress effects of quality of leadership and social support at work. Medicine (Baltimore). 2017;96(15):1-6. doi:10.1097/MD.0000000000006505
26. Siegrist J. The Effort–Reward Imbalance Model. The Handbook of Stress and Health. Hoboken: John Wiley & Sons Ltd., 2017.
27. van Vegchel N, de Jonge J, Bosma H, Schaufeli W. Reviewing the effort-reward imbalance model: drawing up the balance of 45 empirical studies. Social Science & Medicine. 2005;60(5):1117-1131. doi:10.1016/j.socscimed.2004.06.043
28. Siegrist J. Adverse health effects of high effort - low reward conditions at work. Journal of Occupational Psychology. 1996;1:27-43. doi:10.1037/1076-8998.1.1.27
29. Semmer NK, Grebner S, Elfering A. Beyond self-report: Using observational, physiological, and situation-based measures in research on occupational stress. In: Perrewe PL, Ganster DC, eds. Research in Occupational Stress and Well Being 3ed. Amsterdam: Emerald Group Publishing Limited, 2004: 205-263.
30. Frese M, Zapf D. Methodological issues in the study of work stress: Objective vs. subjective measurement of work stress and the question of longitudinal studies. In: Cooper CL, Payne R, eds. Causes, coping and consequences of stress at work. Chichester: John Wiley & Sons, 1988: 375–411.
31. Spielholz P, Silverstein B, Morgan M, Checkoway H, Kaufman J. Comparison of self-report, video observation and direct measurement methods for upper extremity musculoskeletal disorder physical risk factors. Ergonomics. 2001;44(6):588-613. doi:10.1080/00140130118050
32. Lorenz FO, Melby JN, Conger RD, Surjadi FF. Linking questionnaire reports and observer ratings of young couples' hostility and support. Journal of Family Psychology. 2012;26(3):316-327. doi:10.1037/a0028319
33. Nachreiner F, Tielsch R, Gauggel B, Weiss D. Erfassung psychischer Belastung und Rückwirkung auf die Arbeitsgestaltung: Grenzen der Aussagekraft subjektiver Belastungsanalysen mithilfe von Befragungsinstrumenten aus arbeitswissenschaftlicher Sicht. Kurzfragebogen zur Erfassung psychischer Belastungen (KPB): ein Instrument zur Anwendung in der betrieblichen Praxis: Heider, 2008.
34. Cotrim T, Silva C, Amaral V, Bem-haja P, Pereira A. Work ability and psychosocial factors in healthcare settings: Results from a national study. In: Ahram T, Karwowski W, Marek T, editors. Proceedings of the 5th International Conference on Applied Human Factors and Ergonomics AHFE; Poland 2014.
35. OECD. Health at a Glance 2019: OECD Indicators. Paris: OECD Publishing, 2019. 36. Swiss Federal Statistical Office. Schweizerische Gesundheitsbefragung (SGB) -
Arbeitsbedingungen und Gesundheitszustand, 2012–2017. Bern: Bundesamt für Statistik 2019. 37. Kunz Heim D, Sandmeier A, Krause A. Negative Beanspruchungsfolgen bei Schweizer
Lehrpersonen. Beiträge zur Lehrerbildung. 2014;32(2):280-295. 38. Kompier M, Marcelissen F. Handbook of Work Stress: A Systematic Approach for Organizational
Practice. Amsterdam: NIA, 1990. 39. Leka S, Jain A. Health impact of psychosocial hazards at work: An overview. Geneva: World
Health Organization, 2010. 40. Kompier M. Assessing the psychosocial work environment--"subjective" versus "objective"
measurement. Scandinavian Journal of Work, Environment & Health. 2005;31(6):405-408. 41. Eurofound. Work-related stress. Dublin: Eurofound, 2005. 42. Kristensen TS, Hannerz H, Høgh A, Borg V. The Copenhagen Psychosocial Questionnaire-a tool
for the assessment and improvement ofthe psychosocial work environment. Scandinavian Journal of Work, Environment & Health. 2005;31(6):438-449.
General Discussion
170
43. Tuomi K, Ilmarinen J, Jahkola A, Katajarinne L, Tulkki A. Work Ability. 2 ed. Helsinki: Finnish Institute of Occupational Health, 1998.
44. Connell P, Lee VB, Spector PE. Job stress assessment methods. JC Thomas (Vol. Ed.) and M. Hersen (Ed.), Comprehensive handbook of psychological assessment: Industrial and organizational assessment. 2004;4:455-469.
45. Kristensen TS. A new tool for assessing psychosocial factors at work: The Copenhagen Psychosocial Questionnaire. Copenhagen: National Institute of Health, 2000.
46. Burr H, Berthelsen H, Moncada S, Nubling M, Dupret E, Demiral Y, et al. The Third Version of the Copenhagen Psychosocial Questionnaire. Saf Health Work. 2019;10(4):482-503. doi:10.1016/j.shaw.2019.10.002
47. Nübling M, Vomstein M, Nolle I, Lindner A, Haug A, Lincke HJ. Deutsche Standard-Version des COPSOQ 2017. Freiburg: FFAW-Freiburger Forschungsstelle für Arbeitswissenschaften GmbH, 2017.
48. Eurofound. Sixth European Working Conditions Survey - Questionnaire. Luxembourg: Publications Office of the European Union, 2015.
49. Hasselhorn HM, Müller BH, Tackenberg P, Kümmerling A, Simon M. Berufsausstieg bei Pflegepersonal: Arbeitsbedingungen und beabsichtigter Berufsausstieg bei Pflegepersonal in Deutschland und Europa: Wirtschaftsverlag NW, Verlag für Neue Wissenschaften, 2005.
50. Azeem SM, Akhtar N. The Influence of Work Life Balance and Job Satisfaction on Organizational Commitment of Healthcare Employees. International Journal of Human Resource Studies. 2014;4(2):18-24. doi:10.5296/ijhrs.v4i2.5667
51. European Commission. Occupational health and safety risks in the healthcare sector - Guide to prevention and good practice. Luxembourg: Publications Office of the European Union, 2011.
52. Schubert M. Rationing of Nursing Care: Associations with Patient Safety and Quality of Hospital Care. Basel: Medizinischen Fakultät und der Philosophisch-Naturwissenschaftlichen Fakultät der Universität Basel, 2008.
53. Hausler N, Bopp M, Hammig O. Effort-Reward Imbalance, Work-Privacy Conflict, and Burnout Among Hospital Employees. J Occup Environ Med. 2018;60(4):e183-e187. doi:10.1097/JOM.0000000000001287
54. RNAO. Developing and Sustaining Safe, Effective Staffing and Workload Practices (2nd ed.). Toronto: Registered Nurses’ Association of Ontario, 2017.
55. RNAO. Developing and Sustaining Effective Staffing and Workload Practice. Toronto: Registered Nurses’ Association of Ontario, 2007.
56. NICE. Workplace health: management practices - NICE guideline. London: National Institute for Health and Care Excellence, 2015.
57. Hammer L, Kossek E. Family Supportive Supervisor Behaviors (FSSB)- Training Manual 2013. 58. Hammer LB, Kossek EE, Anger WK, Bodner T, Zimmerman KL. Clarifying work-family
intervention processes: the roles of work-family conflict and family-supportive supervisor behaviors. Journal of Applied Psychology. 2011;96(1):134-150. doi:10.1037/a0020927
59. Donaldson‐Feilder E, Yarker J, Lewis R. Line management competence: the key to preventing and reducing stress at work. Strategic HR Review. 2008;7(2):11-16. doi:10.1108/14754390810853110
60. Santa R, Borrero S, Ferrer M, Gherissi D. Fostering a healthcare sector quality and safety culture. International Journal of Health Care Quality Assurance. 2018;31:00-00. doi:10.1108/IJHCQA-06-2017-0108
61. Buchan J, Ball J, O’May F. Determining skill mix in the health workforce: guidelines for managers and health professionals. Issues in health services delivery. Discussion Paper 3. Dept. of Organization of Health Services Delivery. Geneva: World Health Organization, 2000.
62. Leka S, Griffiths A, Cox T. Work Organization and Stress. Geneva: World Health Organisation 2003.
Summary
Summary
172
Summary
Stress at work negatively affects health professionals’ job satisfaction, health and well-being.1-5 In addition, absenteeism and presenteeism due to stress at work accounts for one quarter of total health-related production losses.6 Work-related stress is also associated with health professionals’ increased intentions to leave their profession prematurely and, therefore, further exacerbates workforce shortage in the health care sector.1, 7
Stress at work is defined as ‘a pattern of reactions that occur when employees presented with demands or pressures (stressors) that are not matched to their knowledge, abilities and skills and which challenge their ability to cope’.8, 9 Health professionals are particularly affected, since their daily work involves various stressors, such as a high workload and time-pressure, work-private life conflicts, lack of management support as well as high emotional demands (e.g. aggression from patients/visitors, suffering/dying patients). 1, 10, 11 As the model of ‘causes and consequences of work-related stress’ of Kompier and Marcelissen12 explains, those stressors are associated with stress reactions (short-term) and various long-term consequences for employees themselves and for the organisation.8 Reducing salient stressors at work is therefore essential in order to improve health professionals’ job satisfaction, health status and intention to stay in the organisation and their profession.1, 13
In Switzerland, the health care sector has been struggling with a significant increase in work-related stress among health professionals over the last few years.14 Regrettably, recently undertaken studies have tended either to have a special focus on stress at work specifically among nurses15-17 or to cover a specific area of the healthcare system in Switzerland.1, 5, 18 Thus, studies that include a range of health professional disciplines, using multiple data sources and involving different settings in the Swiss health care system are lacking. Such studies are, however, important in order to identify and effectively reduce salient stressors19 and shape prevention and intervention strategies individually to health professionals’ roles and working environment.
Therefore, the overall aim of this thesis was to investigate stressors, stress reactions and long-term consequences among different health professional disciplines and hierarchical positions. Participants in the study were nurses and midwives, physicians, medical-technical and medical-therapeutic professionals working in Swiss hospitals (acute care, rehabilitation, psychiatric), nursing homes and home care organisations. Also, different data sources were used, including health professionals’ self-reports and external observations. The first two Chapters (1 & 2) of this thesis have a special focus on work-related stress in acute care and rehabilitation hospitals, while Chapters 4, 5 and 6 also include psychiatric hospitals, nursing homes and home care organisations. In addition, all studies presented in Chapters 2-6 were investigated using a quantitative, cross-sectional design and were part of the national STRAIN study ‘work-related

Summary
173
stress among health professionals in Switzerland’ (clinical trials registration: NCT03508596). The local Swiss ethical board in Bern confirmed that the studies included in this thesis do not fall under the Swiss Federal Act on Research Involving Human Beings (Req-2016-00616). Chapter 1 presents a general introduction to the thesis and introduces the topic of stress at work. It starts with an overview of workforce shortage and provides knowledge on the prevalence and consequences of stress at work. Furthermore, the chapter includes a definition of work-related stress and introduces guiding theoretical models, such as the Job-Demand Control Model20, the Effort-Reward Imbalance Model21 and the Model of Causes and Consequences12 of work-related stress. The chapter also presents a summary of different approaches to assessing stress at work, such as self-reports, observation- or situation-based measures, and physiological data. The introduction concludes with the project’s aim, research questions and an outline of the thesis. Chapter 2 investigates the extent of stress at work as well as stressors associated with health professionals’ stress reactions and long-term consequences in acute care and rehabilitation hospitals. The results imply that the extent of stressors, stress reactions and long-term consequences vary greatly between nurses and midwives, physicians and medical-technical and medical-therapeutic professionals. Nurses and midwives reported, for example, higher emotional and physical demands and lower opportunities for development, while physicians reported higher quantitative demands, work-private life conflicts and lack of social support at work. Medical-technical and medical-therapeutic professionals reported lack of influence, role clarity and scope for breaks and holidays. Stressors which are associated with stress reactions and long-term consequences seemed to differ also between nurses and midwives, physicians, medical-technical and medical-therapeutic professionals. Health professionals are confronted with different stressors at work, regarding their professional role and work environment, which indicates different needs for action when developing strategies to prevent and reduce stress at work. However, some stressors proved to be of common relevance for all health professionals, such as work-private life conflicts, lacking opportunities for development and poor leadership of the direct line manager. Therefore, the results also imply that although many stressors are specific to health professionals’ role and work environment, some common strategies to reduce work-private life conflicts, enhance opportunities for development and quality of leadership could overall contribute to better working conditions. Chapter 3 provides in-depth knowledge on two important stressors from Chapter 2 and investigates factors associated with work-private life conflicts and the
Summary
174
quality of managerial leadership among health professionals (all professions combined) working in acute care and rehabilitation hospitals. The results on work-private life conflicts imply, for example, the importance of health professionals’ influence over their shift schedule (e.g. preferences, possibility to exchange shifts), working days and hours or their demands at work (e.g. quantitative demands, demands to hide emotions). Further results regarding leadership qualities of direct line managers revealed the importance of managerial support, employees’ perceived rewards and leaders’ strategies to manage demands (emotional, quantitative demands) and predictability of work in daily practice. Chapter 4 focuses on health professional leaders and provides knowledge on the extent of stressors, stress reactions and long-term consequences for different hierarchical positions. Participants were health professionals (all professions combined) working in upper-, middle- or lower-management positions or without management responsibilities in hospitals, nursing homes and home care organisations. The main findings imply that leaders working in upper- and middle management positions experienced more work-private life conflicts and higher quantitative demands at work, but also reported better opportunities for development, influence and flexibility at work. In general, health professionals working in lower or non-management positions were affected to a greater extent by various stressors, stress reactions and long-term consequences of stress at work. Our results imply that effective prevention and reduction of stress at work is important at all management levels, since individual stressors at work seem to differ markedly between the hierarchical levels, but especially among those without management responsibilities. This requires leaders who ensure good working conditions in order to enhance employees’ health and ability to function in their work environment. In general, Chapters 2-4 are based on health professionals’ self-reports. Self-reports are widely used, are based on employees’ assessment of stressors, stress reactions and long-term consequences and provide insight into internal psychological states of employees.9, 22, 23 Another possible data source to assess stressors at work are external observers. External observers are expected to provide an additional and independent perspective on employees work stressors. 23 Therefore, external observers are used as an additional data source regarding work stressors in Chapters 5 and 6. Chapter 5 starts with the development and psychometric testing of a new observation-based assessment tool (STRAIN-EOS). The tool was designed to assess stressors at work and to fit the working conditions in hospitals, nursing homes and home care organisations. Results of psychometric testing determined a one-factor solution for 9 out of 10 tested scales, satisfactory reliability, usability
Summary
175
and, to some extent, convergent validity. However, further refinement is necessary before it can be widely used.
The STRAIN-EOS is based on widely used self-report scales and is therefore designed for a comparison with self-report scales. Chapter 6 combines external observations (using STRAIN-EOS) and health professionals’ self-reports regarding stressors at work to identify the convergence and differences between those two data sources. The results determined a convergence between health professionals’ self-reported and externally assessed scales on predictability of work, social community and social relations at work. Significant differences between externally observed and health professionals’ self-reported stressors were found for 6 out of the 9 scales. Health professionals perceived demands at work (quantitative, sensorial, physical) as being higher than external observers did. In contrast, external observers rated the opportunities for development, influence at work and social support provided as being lower than health professionals did. However, both methods include possible biasing effects as well as ‘true variance’23 and therefore provide different perspectives on work stressors among health professionals. Chapter 7 summarises all findings from Chapters 2-6 and provides an interpretation by comparing our results on work-related stress to those from other countries (Germany, Portugal) and professions (teachers). In addition, a new model was developed and discussed for Swiss health professionals in acute care and rehabilitation hospitals. Chapter 7 also includes methodological considerations, strengths and limitations of this thesis.
The chapter further includes implications for practice and discusses the essential role of leadership when it comes to preventing and managing stress at work. Leaders act as role models for their employees in daily practice, showing how to deal with stress at work, as well as influence and shape the culture within the organisation. Also, their leadership behaviour and skills as well as their commitment to effective prevention and intervention strategies reducing stress at work are determining factors. Moreover, organisational policies, including a proactive and visible commitment to health professionals’ well-being and safety at work, are essential. Reducing stress at work, improving working conditions and providing a healthy work environment are key to enhancing health professionals’ well-being and motivation to remain at work. 1-5
Chapter 7 concludes with implications for further research and the need for further studies regarding the extent of stress at work in further health care settings as well as more detailed results regarding different health professionals separately (e.g. physiotherapists, nutrition therapists, midwives). Finally, longitudinal data are needed to further confirm the findings of this thesis regarding stressors and their influence on possible outcomes.
Summary
176
References 1. Hämmig O. Explaining burnout and the intention to leave the profession among health
professionals - a cross-sectional study in a hospital setting in Switzerland. BMC Health Service Research. 2018;18(1):785. doi:10.1186/s12913-018-3556-1
2. Khamisa N, Peltzer K, Ilic D, Oldenburg B. Work related stress, burnout, job satisfaction and general health of nurses: A follow-up study. International Journal of Nursing Practice. 2016;22(6):538-545. doi:10.1111/ijn.12455
3. Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. Journal of the American Medical Association. 2002;288(16):1987-1993. doi:10.1001/jama.288.16.1987
4. Gray-Stanley JA, Muramatsu N. Work stress, burnout, and social and personal resources among direct care workers. Res Dev Disabil. 2011;32(3):1065-1074. doi:10.1016/j.ridd.2011.01.025
5. Hausler N, Bopp M, Hammig O. Effort-Reward Imbalance, Work-Privacy Conflict, and Burnout Among Hospital Employees. J Occup Environ Med. 2018;60(4):e183-e187. doi:10.1097/JOM.0000000000001287
6. Brunner B, Igic I, Keller AC, Wieser S. Who gains the most from improving working conditions? Health-related absenteeism and presenteeism due to stress at work. The European Journal of Health Economics. 2019;20(8):1165-1180. doi:10.1007/s10198-019-01084-9
7. World Health Organisation. Global strategy on human resources for health: workforce 2030. Geneva: World Health Organization, 2016.
8. Eurofound. Work-related stress. Dublin: Eurofound, 2005. 9. Leka S, Jain A. Health impact of psychosocial hazards at work: An overview. Geneva: World
Health Organization, 2010. 10. Lim J, Bogossian F, Ahern K. Stress and coping in Australian nurses: a systematic review.
International Nursing Review. 2010;57(1):22-31. doi:10.1111/j.1466-7657.2009.00765.x 11. Hahn S, Hantikainen V, Needham I, Kok G, Dassen T, Halfens RJ. Patient and visitor violence in
the general hospital, occurrence, staff interventions and consequences: a cross-sectional survey. Journal of advanced nursing. 2012;68(12):2685-2699. doi:10.1111/j.1365-2648.2012.05967.x
12. Kompier M, Marcelissen F. Handbook of Work Stress: A Systematic Approach for Organizational Practice. Amsterdam: NIA, 1990.
13. Aiken LH, Sloane DM, Bruyneel L, Van den Heede K, Sermeus W, Consortium RC. Nurses' reports of working conditions and hospital quality of care in 12 countries in Europe. International Journal of Nursing Studies. 2013;50(2):143-153. doi:10.1016/j.ijnurstu.2012.11.009
14. Swiss Federal Statistical Office. Schweizerische Gesundheitsbefragung (SGB) - Arbeitsbedingungen und Gesundheitszustand, 2012–2017. Bern: Bundesamt für Statistik2019.
15. Dhaini SR, Zuniga F, Ausserhofer D, Simon M, Kunz R, De Geest S, et al. Care workers health in Swiss nursing homes and its association with psychosocial work environment: A cross-sectional study. International Journal of Nursing Studies. 2016;53:105-115. doi:10.1016/j.ijnurstu.2015.08.011
16. Sermeus W, Aiken LH, Van den Heede K, Rafferty AM, Griffiths P, Moreno-Casbas MT, et al. Nurse forecasting in Europe (RN4CAST): Rationale, design and methodology. BMC Nursing. 2011;10(6):6. doi:10.1186/1472-6955-10-6
17. Dhaini SR, Denhaerynck K, Bachnick S, Schwendimann R, Schubert M, De Geest S, et al. Work schedule flexibility is associated with emotional exhaustion among registered nurses in Swiss hospitals: A cross-sectional study. International Journal of Nursing Studies. 2018;82:99-105. doi:10.1016/j.ijnurstu.2018.03.019
18. Lambert VA, Lambert CE. Literature review of role stress/strain on nurses: An international perspective. Nursing & health sciences. 2001;3(3):161-172. doi:10.1046/j.1442-2018.2001.00086.x
19. Ruotsalainen JH, Verbeek JH, Marine A, Serra C. Preventing occupational stress in healthcare workers. Cochrane Database of Systematic Reviews. 2014(11):Cd002892. doi:10.1002/14651858.CD002892.pub3
20. Karasek RA. Job demands, job decision latitude, and mental strain: Implications for job redesign. Administrative science quarterly. 1979:285-308. doi:10.2307/2392498
21. Siegrist J, Klein D, Voigt KH. Linking sociological with physiological data: the model of effort-reward imbalance at work. Acta physiologica scandinavica. Supplementum. 1997;640:112-116.

Summary
177
22. Connell P, Lee VB, Spector PE. Job stress assessment methods. JC Thomas (Vol. Ed.) and M. Hersen (Ed.), Comprehensive handbook of psychological assessment: Industrial and organizational assessment. 2004;4:455-469.
23. Semmer NK, Grebner S, Elfering A. Beyond self-report: Using observational, physiological, and situation-based measures in research on occupational stress. In: Perrewe PL, Ganster DC, eds. Research in Occupational Stress and Well Being 3ed. Amsterdam: Emerald Group Publishing Limited, 2004: 205-263.
Samenvatting
Samenvatting
180
Samenvatting
Stress op het werk heeft negatieve gevolgen voor de arbeidsvreugde, de gezondheid en het welzijn van een zorgmedewerker.1-5 Daarbij vormen ziekteverzuim en absenteïsme omwille van stress op het werk een kwart van de totale gezondheid gerelateerde productieverliezen.6 Werk gerelateerde stress wordt ook gekoppeld aan de toenemende intentie van zorgmedewerkers om hun beroep voortijdig te verlaten waardoor het tekort aan arbeidskrachten in de gezondheidssector verder toeneemt.1, 7
Stress op het werk wordt gedefinieerd als “een patroon van reacties dat zich voordoet wanneer werknemers worden geconfronteerd met vragen of spanningen (stressfactoren) die niet afgestemd zijn op hun kennis, capaciteiten en vaardigheden en een uitdaging vormen voor hun vermogen om hiermee om te gaan”.8, 9 Zorgmedewerkers worden in het bijzonder getroffen aangezien hun dagelijks werk talrijke stressfactoren met zich meebrengt, zoals een hoge werklast en tijdsdruk, een strijdige werk-privébalans, gebrek aan managementondersteuning en hoge emotionele eisen (bv. agressie van patiënten/bezoekers, lijdende/stervende patiënten).1, 10, 11 Zoals het model van Kompier en Marcelissen12 “Causes and consequences of work-related stress” aantoont, zijn deze stressfactoren de oorzaak van stressreacties (op korte termijn) en kunnen ze verschillende gevolgen op lange termijn voor de werknemers en voor de organisatie hebben.8 Door belangrijke stressfactoren op het werk te verminderen, krijgt de zorgmedewerker meer arbeidsvreugde, een betere gezondheid en heeft hij/zij de motivatie om zijn/haar beroep verder uit te oefenen in de organisatie.1, 13
In de afgelopen jaren heeft de gezondheidssector in Zwitserland te kampen met een grote toename van werk gerelateerde stress bij zorgmedewerkers.14 Spijtig genoeg hebben recente studies zich met name gericht op stress op het werk bij verpleegkundigen15-17 of onderzochten ze slechts een specifiek domein van het gezondheidssysteem in Zwitserland.1, 5, 18 Hierdoor ontbreken studies die een brede waaier aan vakgebieden in de professionele gezondheidszorg bestuderen, diverse gegevensbronnen gebruiken en verschillende instellingen in het Zwitserse gezondheidssysteem betrekken. Dergelijke studies zijn echter wel belangrijk om de belangrijkste stressfactoren19 te identificeren en deze doeltreffend te verminderen alsook om individuele preventie- en interventiestrategieën voor de taken en werkomgeving van zorgmedewerkers uit te werken.
Om die reden is het algemene doel van dit proefschrift het onderzoeken van stressfactoren, stressreacties en de gevolgen hiervan op lange termijn voor diverse vakgebieden van zorgmedewerkers en hiërarchische posities. De deelnemers aan deze studie waren verpleegkundigen en vroedvrouwen, artsen, medisch-technische en medisch-therapeutische deskundigen die in Zwitserse ziekenhuizen (d.i. de acute zorg, revalidatie en psychiatrie), woonzorgcentra en
Samenvatting
181
thuiszorgorganisaties werken. Er zijn verschillende gegevensbronnen gebruikt, met inbegrip van zelfrapportages van zorgmedewerkers en externe observaties. De eerste twee hoofdstukken (1 & 2) van dit proefschrift richten zich voornamelijk op werk gerelateerde stress in de acute zorg en revalidatieziekenhuizen, terwijl de hoofdstukken 4, 5 en 6 ook psychiatrische ziekenhuizen, woonzorgcentra en thuiszorgorganisaties omvatten. Daarnaast zijn alle studies uit de hoofdstukken 2-6 onderzocht met een kwantitatief, transversaal design en maakten ze deel uit van de nationale STRAIN-studie over “Work-related stress among health professionals in Switzerland” (registratie klinische onderzoeken: NCT03508596). De lokale Zwitserse ethische commissie in Bern bevestigde dat de Zwitserse federale wetgeving inzake mens gebonden onderzoek (Req-2016-00616) niet van toepassing is op de studies die voor dit proefschrift gebruikt werden. In hoofdstuk 1 wordt een algemene inleiding op het thema van het proefschrift gegeven, t.w. ‘stress op het werk. Eerst wordt het probleem van het tekort aan arbeidskrachten toegelicht en wordt er informatie gegeven over de aanwezigheid en de gevolgen van stress op het werk. Verder bevat het hoofdstuk een definitie van werk gerelateerde stress en worden begeleidende theoretische modellen besproken, zoals het Job-Demand Control model20, het Effort-Reward Imbalance-model21 en het Model of Causes and Consequences of work related stress12. Het hoofdstuk bevat ook een samenvatting van de verschillende benaderingen om stress op het werk te evalueren, zoals zelfrapportages, observatie- of situatie gerelateerde maatregelen en fysiologische gegevens. De inleiding sluit af met het doel en opzet van het project, de onderzoeksvragen en de hoofdlijnen van het proefschrift. Hoofdstuk 2 onderzoekt de omvang van stress op het werk als ook de stressfactoren die gekoppeld zijn aan de stressreacties van gezondheidswerkers en de gevolgen op lange termijn in de acute zorg en revalidatieziekenhuizen. De resultaten tonen aan dat de omvang van stressfactoren, stressreacties en gevolgen op lange termijn sterk variëren tussen verpleegkundigen, vroedvrouwen, artsen en medisch-technische respectievelijk medisch-therapeutische deskundigen. Verpleegkundigen en vroedvrouwen rapporteerden bijvoorbeeld hogere emotionele en fysieke eisen en minder ontwikkelingsmogelijkheden, terwijl artsen spraken over hogere kwantitatieve eisen, een moeilijke werk-privébalans en een gebrek aan sociale steun op het werk. Medisch technische en medisch-therapeutische deskundigen meldden een gebrek aan invloed, aan een duidelijke verdeling van taken en aan mogelijkheden om pauzes en vakantie te nemen. Stressfactoren die gekoppeld worden aan stressreacties en gevolgen op lange termijn bleken ook te verschillen tussen verpleegkundigen en vroedvrouwen, artsen, medisch-technische en medisch-therapeutische deskundigen. Zorgmedewerkers worden geconfronteerd met verschillende stressfactoren op
Samenvatting
182
het werk ten aanzien van hun professionele rol en werkomgeving. Deze wijzen ook op verschillende behoeften ten aanzien van het ontwikkelen van acties en strategieën die stress op het werk beogen te voorkomen en verminderen. Sommige stressfactoren werden echter door alle zorgmedewerkers aangegeven, zoals een moeilijke werk-privébalans, het gebrek aan ontwikkelingsmogelijkheden en zwak leiderschap van de rechtstreeks leidinggevende. Hiermee tonen de resultaten ook aan dat, hoewel veel stressfactoren specifiek van toepassing zijn op de specifieke rol en werkomgeving van zorgmedewerkers, algemene strategieën die als doel hebben de werk-privéconflicten te verminderen en de ontwikkelingsmogelijkheden van medewerkers te verhogen en die ook leiden tot een als beter ervaren leiderschap van de leidinggevende, kunnen bijdragen tot betere werkomstandigheden. Hoofdstuk 3 bespreekt in detail twee belangrijke stressfactoren uit hoofdstuk 2 en onderzoekt de factoren die samenhangen met werk-privéconflicten en leiderschapskwaliteiten van het management bij zorgmedewerkers (alle beroepen gecombineerd) die in de acute zorg en revalidatieziekenhuizen werken. De resultaten m.b.t. de werk-privéconflicten wijzen onder meer op het belang van de invloed die zorgmedewerkers hebben op hun werkrooster (bv. voorkeuren, mogelijkheid om van shift te veranderen), werkdagen en werkuren en ook op de eisen die het werk aan hen stelt (bv. kwantitatieve eisen, de noodzaak om emoties te verstoppen etc.). De resultaten omtrent de leiderschapskwaliteiten van rechtstreeks leidinggevenden tonen het belang aan van managementondersteuning, beloningen voor werknemers, de strategieën die leiders toepassen om met (emotionele en kwantitatieve) vragen om te gaan en de voorspelbaarheid van het werk in de dagelijkse praktijk. Hoofdstuk 4 spitst zich toe op de leidinggevenden van zorgmedewerkers en biedt gegevens over de omvang van stressfactoren, stressreacties en gevolgen op lange termijn voor verschillende hiërarchische functies. De deelnemers betroffen zorgmedewerkers (alle beroepen gecombineerd) die de hoogste, middelste of lagere managementfuncties bekleedden in ziekenhuizen, woonzorgcentra en thuiszorgorganisaties. De voornaamste bevindingen tonen aan dat leidinggevenden in de hoogste en middelste managementfuncties meer werk-privéconflicten en grotere kwantitatieve eisen op het werk ervoeren. Zij rapporteerden echter ook betere ontwikkelingsmogelijkheden én meer invloed en flexibiliteit t.a.v. het werk. Zorgmedewerkers die een lagere managementfunctie bekleedden, hadden meer last van uiteenlopende stressfactoren, stressreacties en gevolgen op lange termijn door stress op het werk. Onze resultaten tonen aan dat een doeltreffende preventie en vermindering van stress op het werk belangrijk zijn op alle managementniveaus, aangezien individuele stressfactoren op het werk duidelijk verschillen tussen de hiërarchische niveaus. Om deze reden is het belangrijk om leidinggevenden aan te stellen die goede werkomstandigheden
Samenvatting
183
waarborgen, teneinde de gezondheid van hun werknemers en hun vermogen om in de werkomgeving te functioneren, te verbeteren. Hoofdstukken 2-4 zijn gebaseerd op zelfrapportages van gezondheidswerkers. Deze zelfrapportages zijn gebaseerd op de evaluatie van stressfactoren, stressreacties en gevolgen op lange termijn voor werknemers en geven ook inzicht in de interne psychologische toestand van de werknemers.9, 22, 23 Een andere mogelijke gegevensbron om stressfactoren op het werk te evalueren, betreft externe observaties. Externe observaties geven een aanvullend en onafhankelijk perspectief op de stressfactoren van werknemers op het werk.23 Om die reden werden externe observaties gebruikt als een aanvullende databron voor werk gerelateerde stressfactoren in de hoofdstukken 5 en 6. Hoofdstuk 5 begint met het ontwikkelings- en psychometrische testwerk van een nieuw observationeel beoordelingsinstrument (de STRAIN-EOS). Het instrument werd ontwikkeld om werk gerelateerde stressfactoren te evalueren in het kader van de werkomstandigheden in ziekenhuizen, woonzorgcentra en thuiszorgorganisaties. De resultaten van het psychometrische testwerk bepaalden een één-factor-oplossing voor 9 op de 10 geteste schalen en toonden een bevredigende betrouwbaarheid, bruikbaarheid en, in zekere mate, convergent validity. Het instrument moet echter verder verfijnd worden voordat het op grotere schaal kan worden ingezet. In hoofdstuk 6 worden de externe observaties (met behulp van de STRAIN-EOS) en de zelfrapportages van zorgmedewerkers met betrekking tot stressfactoren op het werk gecombineerd om de overeenkomsten en verschillen tussen deze twee gegevensbronnen te identificeren. De resultaten tonen overeenkomsten aan tussen de door zorgmedewerkers zelf gerapporteerde schalen en de extern geëvalueerde schalen op het vlak van voorspelbaarheid van werk, de sociale gemeenschap en sociale relaties op het werk. Voor 6 van de 9 schalen bestonden er significante verschillen tussen de extern geobserveerde en de door de zorgmedewerkers zelf gerapporteerde stressfactoren. Zorgmedewerkers ervoeren de (kwantitatieve, zintuiglijke en fysieke) eisen op het werk als hoger dan zoals aangegeven door de externe observatoren. Externe observatoren beoordeelden aan de andere kant de ontwikkelingsmogelijkheden, de invloed op het werk en de sociale steun als lager dan de zorgmedewerkers zelf. Beide methoden bevatten echter mogelijk vertekende effecten en “true variance”23, en bieden derhalve verschillende perspectieven op werk gerelateerde stressfactoren onder zorgmedewerkers. Hoofdstuk 7 vat alle bevindingen van de hoofdstukken 2-6 samen en geeft een verdere interpretatie door onze studieresultaten m.b.t. werk gerelateerde stress te vergelijken met die van andere landen (Duitsland, Portugal) en andere
Samenvatting
184
beroepen (leerkrachten). Bovendien wordt een nieuw model ontwikkeld en besproken voor Zwitserse zorgmedewerkers in de acute zorg en revalidatieziekenhuizen. Hoofdstuk 7 bespreekt verder ook de methodologische overwegingen, de kracht en beperkingen van dit proefschrift.
Daarnaast bespreekt het hoofdstuk ook de gevolgen voor de praktijk en de cruciale rol van het leiderschap op het werk, wanneer men spreekt over het voorkomen en aanpakken van stress op het werk. Leidinggevenden vervullen een rolmodel voor hun werknemers, ze tonen hoe men met stress op het werk kan omgaan en hebben invloed op de cultuur van de organisatie. Hun leiderschapsgedrag en -vaardigheden, alsook hun streven naar doeltreffende preventie-en interventiestrategieën om stress op het werk te verminderen, zijn eveneens doorslaggevende factoren. Daarbij zijn organisatorische beleidsmaatregelen, met inbegrip van een proactieve en zichtbare inzet voor het welzijn van zorgmedewerkers en hun veiligheid op het werk, van wezenlijk belang. Minder stress op het werk, betere werkomstandigheden en een gezonde werkomgeving vormen de sleutel tot het versterken van het welzijn van zorgmedewerkers en hun motivatie om te blijven werken in de organisatie.1-5
Hoofdstuk 7 wordt afgesloten met ideeën voor toekomstig onderzoek en de behoefte aan verder onderzoek met betrekking tot de omvang van stress op het werk in ongeacht welk type zorginstelling, alsook aan verder onderzoek ten aanzien van verschillende typen zorgmedewerkers (bv. fysiotherapeuten, voedingstherapeuten, vroedvrouwen etc.). Tenslotte is er behoefte aan longitudinale studies die de bevindingen van dit proefschrift met betrekking tot stressfactoren en hun mogelijke uitkomst, bevestigen.
Samenvatting
185
Referenties 1. Hämmig O. Explaining burnout and the intention to leave the profession among health
professionals - a cross-sectional study in a hospital setting in Switzerland. BMC Health Service Research. 2018;18(1):785. doi:10.1186/s12913-018-3556-1
2. Khamisa N, Peltzer K, Ilic D, Oldenburg B. Work related stress, burnout, job satisfaction and general health of nurses: A follow-up study. International Journal of Nursing Practice. 2016;22(6):538-545. doi:10.1111/ijn.12455
3. Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. Journal of the American Medical Association. 2002;288(16):1987-1993. doi:10.1001/jama.288.16.1987
4. Gray-Stanley JA, Muramatsu N. Work stress, burnout, and social and personal resources among direct care workers. Res Dev Disabil. 2011;32(3):1065-1074. doi:10.1016/j.ridd.2011.01.025
5. Hausler N, Bopp M, Hammig O. Effort-Reward Imbalance, Work-Privacy Conflict, and Burnout Among Hospital Employees. J Occup Environ Med. 2018;60(4):e183-e187. doi:10.1097/JOM.0000000000001287
6. Brunner B, Igic I, Keller AC, Wieser S. Who gains the most from improving working conditions? Health-related absenteeism and presenteeism due to stress at work. The European Journal of Health Economics. 2019;20(8):1165-1180. doi:10.1007/s10198-019-01084-9
7. World Health Organisation. Global strategy on human resources for health: workforce 2030. Geneva: World Health Organization, 2016.
8. Eurofound. Work-related stress. Dublin: Eurofound, 2005. 9. Leka S, Jain A. Health impact of psychosocial hazards at work: An overview. Geneva: World
Health Organization, 2010. 10. Lim J, Bogossian F, Ahern K. Stress and coping in Australian nurses: a systematic review.
International Nursing Review. 2010;57(1):22-31. doi:10.1111/j.1466-7657.2009.00765.x 11. Hahn S, Hantikainen V, Needham I, Kok G, Dassen T, Halfens RJ. Patient and visitor violence in
the general hospital, occurrence, staff interventions and consequences: a cross-sectional survey. Journal of advanced nursing. 2012;68(12):2685-2699. doi:10.1111/j.1365-2648.2012.05967.x
12. Kompier M, Marcelissen F. Handbook of Work Stress: A Systematic Approach for Organizational Practice. Amsterdam: NIA, 1990.
13. Aiken LH, Sloane DM, Bruyneel L, Van den Heede K, Sermeus W, Consortium RC. Nurses' reports of working conditions and hospital quality of care in 12 countries in Europe. International Journal of Nursing Studies. 2013;50(2):143-153. doi:10.1016/j.ijnurstu.2012.11.009
14. Swiss Federal Statistical Office. Schweizerische Gesundheitsbefragung (SGB) - Arbeitsbedingungen und Gesundheitszustand, 2012–2017. Bern: Bundesamt für Statistik2019.
15. Dhaini SR, Zuniga F, Ausserhofer D, Simon M, Kunz R, De Geest S, et al. Care workers health in Swiss nursing homes and its association with psychosocial work environment: A cross-sectional study. International Journal of Nursing Studies. 2016;53:105-115. doi:10.1016/j.ijnurstu.2015.08.011
16. Sermeus W, Aiken LH, Van den Heede K, Rafferty AM, Griffiths P, Moreno-Casbas MT, et al. Nurse forecasting in Europe (RN4CAST): Rationale, design and methodology. BMC Nursing. 2011;10(6):6. doi:10.1186/1472-6955-10-6
17. Dhaini SR, Denhaerynck K, Bachnick S, Schwendimann R, Schubert M, De Geest S, et al. Work schedule flexibility is associated with emotional exhaustion among registered nurses in Swiss hospitals: A cross-sectional study. International Journal of Nursing Studies. 2018;82:99-105. doi:10.1016/j.ijnurstu.2018.03.019
18. Lambert VA, Lambert CE. Literature review of role stress/strain on nurses: An international perspective. Nursing & health sciences. 2001;3(3):161-172. doi:10.1046/j.1442-2018.2001.00086.x
19. Ruotsalainen JH, Verbeek JH, Marine A, Serra C. Preventing occupational stress in healthcare workers. Cochrane Database of Systematic Reviews. 2014(11):Cd002892. doi:10.1002/14651858.CD002892.pub3
20. Karasek RA. Job demands, job decision latitude, and mental strain: Implications for job redesign. Administrative science quarterly. 1979:285-308. doi:10.2307/2392498
21. Siegrist J, Klein D, Voigt KH. Linking sociological with physiological data: the model of effort-reward imbalance at work. Acta physiologica scandinavica. Supplementum. 1997;640:112-116.

Samenvatting
186
22. Connell P, Lee VB, Spector PE. Job stress assessment methods. JC Thomas (Vol. Ed.) and M. Hersen (Ed.), Comprehensive handbook of psychological assessment: Industrial and organizational assessment. 2004;4:455-469.
23. Semmer NK, Grebner S, Elfering A. Beyond self-report: Using observational, physiological, and situation-based measures in research on occupational stress. In: Perrewe PL, Ganster DC, eds. Research in Occupational Stress and Well Being 3ed. Amsterdam: Emerald Group Publishing Limited, 2004: 205-263.
Valorisation

Valorisation
188
Valorisation
This chapter on valorisation provides information on the potential value of this thesis’ results for important stakeholders, the Swiss population in general, further research and education. Furthermore, the chapter concludes with information on activities and products resulting from our findings. Relevance of this thesis Stress at work has many adverse effects on health professionals’ job satisfaction, health and well-being.1-3 Furthermore, stress at work is associated with health professionals’ increasing intention to leave the profession prematurely and generally reduces the attractiveness of practising a health profession.1, 4 Switzerland is, among other countries, currently struggling with a shortage of health professionals.5 However, the availability of well-educated health professionals is essential for a society’s well-being and a shortage of these key workers can destabilise a country's entire health care system.6 The current coronavirus (COVID-19) pandemic has clearly demonstrated the association of limited resources, healthcare burden and mortality in several countries, and how essential the role of health professionals is in such a time of crisis.7 Value for stakeholders, population, research and education Reducing stress at work is therefore not only important to ensure that the healthcare system is adequately prepared for such events, but above all, that enough health professionals are always available in the healthcare sector. The results of this thesis identify important fields of action that should be taken in order to improve working conditions in the Swiss health care system, with a special focus on acute care and rehabilitation hospitals. This may contribute to combating the shortage of skilled health professionals and to ensure optimal health care for the Swiss population. The results of this thesis can therefore also be important for politicians and policy makers in their efforts to promote better working conditions (e.g. regarding compliance with legal breaks and rest periods in the Swiss health care sector).
In addition, this thesis provides important recommendations for organisational policies, and detailed suggestions on topics relevant to improving working conditions in the whole organisation as well as specific topics for different health professional disciplines and various levels of hierarchy. Furthermore, most relevant prerequisites for the effective implementation of prevention strategies in everyday clinical practice are discussed and are intended to support leaders with their implementation in their area of responsibility. Our results, moreover, not only establish the need for further research regarding effective prevention and intervention strategies in order to reduce stress at work

Valorisation
189
among health professionals, but also reveal the need for a stronger focus on stress at work in health professionals’ education. Health professional leaders in particular have an important role to play within their organisation to improve working conditions and reduce stress at work among their employees.8 Therefore, a special focus in their training and education on the assessment and reduction of stress at work as well as on their attitude and leadership behaviours is essential. In addition, the inclusion of legal aspects of working conditions and effective strategies on how to deal with stress at work in the basic education program of Swiss health professionals could support and strengthen their influence in improving their working conditions and coping strategies regarding stress at work Target groups The primary target group of this research were Swiss healthcare organisations (especially acute care and rehabilitation hospitals), their leaders, human resource teams and employees with a remit for occupational health. Health professional leaders received special focus because they are responsible for the protection and improvement of employees’ health, wellbeing, job satisfaction and intention to remain in the organisation and in their profession. Also, they have a key role regarding establishing a positive and supportive organisational culture as well as the development and implementation of organisational policies towards better working conditions and prevention of stress at work.8, 9 In addition, health professionals working without management responsibility can also benefit, since our results shed light on the poorest working conditions, satisfaction and health-related outcomes and thus offer them evidence-based arguments for better working conditions in their daily work. Activities and Products The results of this thesis were part of the first data collection of the national STRAIN study (work-related stress among health professionals in Switzerland). The STRAIN study is a cluster randomised controlled trial (Clinical Trials registration: NCT03508596), conducted in the settings acute care, rehabilitation and psychiatric hospitals, nursing homes and outpatient care in all language regions of Switzerland. The strain study consists of three data collections (T0= 2017/2018, T1= 2019, T2=2020) using a self-report questionnaire10 for employees and a questionnaire to assess institutional key figures. The data from the baseline measurement T0 was analysed in Chapter 2-4 with a focus on acute care and rehabilitation hospitals (Chapter 2,3) and different hierarchies (Chapter 4). Furthermore, the results of the overall STRAIN study also focused on the extent of stress at work and stressors associated with relevant outcomes in other settings (psychiatric hospitals, nursing homes, outpatient care). In addition to these quantitative data, a total of 24 focus group interviews with various health

Valorisation
190
professionals working in different settings of the Swiss health care sector were conducted to collect their ideas and recommendations on how to improve their working environment and reduce stress at work. Additionally, an extensive literature research was conducted in order to identify published international literature on effective prevention and intervention strategies to reduce stress at work. Therefore, 1400 studies (reviews, meta-analysis, intervention studies) and available guidelines were summarised and analysed as to their recommendations. Those three data sources (quantitative, qualitative, literature) served in developing the study intervention that focuses on the health professional leaders working in the lower, middle and upper management levels. The STRAIN intervention program was developed according to the intervention mapping approach from Bartholomew, et al.11. The intervention mapping approach consists of 6 steps and leads towards evidence-based program development, implementation and evaluation.11 The results of this thesis, among others, therefore directly supported the development of the STRAIN intervention program for leaders.
Valorisation
191
References 1. Hämmig O. Explaining burnout and the intention to leave the profession among health
professionals - a cross-sectional study in a hospital setting in Switzerland. BMC Health Service Research. 2018;18(1):785. doi:10.1186/s12913-018-3556-1
2. Hausler N, Bopp M, Hammig O. Effort-Reward Imbalance, Work-Privacy Conflict, and Burnout Among Hospital Employees. J Occup Environ Med. 2018;60(4):e183-e187. doi:10.1097/JOM.0000000000001287
3. Khamisa N, Peltzer K, Ilic D, Oldenburg B. Work related stress, burnout, job satisfaction and general health of nurses: A follow-up study. International Journal of Nursing Practice. 2016;22(6):538-545. doi:10.1111/ijn.12455
4. Streit S, da Costa BR, Christensen S, Tal K, Tandjung R, Juni P. One in seven Swiss physicians has left patient care - results from a national cohort study from 1980-2009. Swiss Medical Weekly. 2019;149:w20116. doi:10.4414/smw.2019.20116
5. Merçay C, Burla L, Widmer M. Gesundheitspersonal in der Schweiz. Bestandesaufnahme und Prognosen bis 2030 (Obsan Bericht 71). Neuchâtel: Schweizerisches Gesundheitsobservatorium, 2016.
6. World Health Organisation. Global strategy on human resources for health: workforce 2030. Geneva: World Health Organization, 2016.
7. Ji Y, Ma Z, Peppelenbosch MP, Pan Q. Potential association between COVID-19 mortality and health-care resource availability. The Lancet Global Health. 2020;8(4):e480. doi:10.1016/S2214-109X(20)30068-1
8. Donaldson‐Feilder E, Yarker J, Lewis R. Line management competence: the key to preventing and reducing stress at work. Strategic HR Review. 2008;7(2):11-16. doi:10.1108/14754390810853110
9. NICE. Workplace health: management practices - NICE guideline. London: National Institute for Health and Care Excellence, 2015.
10. Golz C, Peter KA, Hahn S. Cognitive Pretesting and pretest of the STRAIN questionnaire to elaborate work-related stress of health care staff in Switzerland. International Journal of Health Professions. 2018;5(1):109-120. doi:10.2478/ijhp-2018-0011
11. Bartholomew Eldredge LK, Markham CM, Ruiter RAC, Fernández ME, Kok G, Parcel GS. Planning health promotion programs - an intervention mapping aproach. 4 ed. San Francisco: Wiley, 2016.
Acknowledgements
Acknowledgements
194
Acknowledgements
I want to express my gratitude to everyone who contributed in any form to my PhD trajectory over the last 5 years. My supervisors A special thanks goes to my supervisors, Prof. Dr. Jos M.G.A Schols, Dr. Ruud J.G. Halfens and Prof. Dr. Sabine Hahn for their ongoing support, patience and motivation during my PhD trajectory. Your feedback and support helped me to develop new ideas and solutions, to get me out of a dead end and, most importantly, to develop and improve myself continuously.
Jos, thank you very much for assuming the role of the first supervisor in the middle of my PhD trajectory. Your supportive and positive attitude has motivated me a lot, especially during the more challenging phases of my PhD. Also, the speed at which you provide feedback is unbeatable and your ideas and comments often put me on the right track. Thanks a lot for this!
Ruud, you have played a very central role on my path to the PhD and your guidance through all the ups and downs of my PhD career means a lot to me. Through your honest and objective feedback, I was able to improve not only professionally, but also personally. Thanks a lot for this!
Sabine, with your ideas, experience and practical way of thinking you often helped me to find new solutions when I was at a loss. You have played an important role, not only as my PhD supervisor, but also in my professional career in recent years and have positively influenced, motivated, encouraged and supported me. Thanks a lot for this! The members of the assessment committee I would like to thank Prof. Dr. J.P.H. Hamers, Prof. Dr. R.A.C. Ruiter, Dr. N.P.G. Boumans, Prof. Dr. G. Meyer and Dr. R. Schwendimann (University Hospital Basel) for being part of the assessment committee and, especially, for the time and effort needed to read and evaluate this thesis. Academic advisors I would like to thank Prof. Dr. Eva Soom for sharing her experience and knowledge on observational studies. Also, I thank Prof. Dr. Gerjo Kok for his input on intervention mapping and behaviour change. In addition, I thank Dr. Reto Bürgin for sharing his knowledge in statistics and his help regarding various statistical analyses for this thesis. I also thank Dr. Christoph von Dach, who helped with the recruitment of health professionals participating on external observation sequences. In addition, I would like to thank Prof. Dr. Hans Bosma for sharing his experience and knowledge on work-related stress during the first phase of my PhD trajectory. Furthermore, I would like to thank Prof. Dr. Christa
Acknowledgements
195
Lohrmann and Prof. Dr. Sandra Zwakhalen for your feedback and input during the PhD seminars. All organisations and health professionals who participated I am very grateful to all the healthcare organisations and nurses, midwives, physicians, medical-technical and medical-therapeutic professionals who participated in the research project and shared their experience and time so generously. Without their voluntary participation, this research would not have been possible. Colleagues from the STRAIN project Furthermore, I am very grateful to all the project-partners and colleagues from the STRAIN project. Thank you Prof. Dr. Christian Voirol, Prof. Dr. Annie Oulevey and Typhaine Juvet for your experience, effort, time and support with the recruitment, questionnaire development, data collection and much more in the French-speaking part of Switzerland. Also, I thank Dr. Stefan Kunz for not only sharing his experience and knowledge in economics, but also for his effort and time regarding recruitment, data collection and much more in the Italian-speaking part of Switzerland. Also, I thank all the other colleagues of the STRAIN project; Thomas Schwarze, Fabienne Renggli, Xenia Schmid, Tanja Lazarevic, Christoph Golz, Angela Blasimann, Caroline Gurtner, Dr. med. Albert Zeyer, Prof. Dr. Andrea Gurtner and Prof. Dr. Margit Geiger for sharing your time and experience. The co-authors and contributors to the articles I would like to thank my co-authors for their contribution to the papers. Thank you, Esther Stadelmann for helping with the recruitment, data collection and analysis in Chapter 5. Also, I thank Tannys Helfer and Dr. Heather Murray for their time and effort when reading and correcting all my manuscripts. My fellow PhD students A big thank you goes to all of my fellow PhD students. Thank you very much for all your support and motivation over the last few years. Without all of you and the good times during the PhD seminars, those years would have been much more challenging. I also thank all of you very much for your honest and inspiring feedback on my PhD articles during the seminars. I wish you all lots of success with your ongoing PhD trajectory and hope we will meet again. My Family Another big thank you goes to my family and friends for their motivation and support during my PhD. I thank my husband Matthias, for his support during the ups and downs of my PhD, for the countless English corrections, language trainings and above all for his positive and motivating attitude. You always managed to make me laugh, even after major setbacks. Thank you for this!

Acknowledgements
196
A big thank you also goes to my family, Ines, Daniela and Roger for your ongoing support and encouragement during my PhD trajectory. It is wonderful to know that you are always at my side in all phases of life. Thank you a lot! My friends Furthermore, I am very grateful to all my friends who contributed, supported, encouraged and motivated me in any form during the last 5 years of my PhD trajectory. My special thanks go to Michèle Spörri, Esther Haller, Sonja Höhn, Marina Stähli, Tara Kappes, Lea Alder, Daria Kronig, Andrea Hofer, Stefania Simone, Jasmin Graf, Pascal Kappeler, Stephanie Lüpold, Peter Schöpp, Philippe Luginbühl, and many other friends who supported and encouraged me in any form during my ups and downs in the PhD. My colleagues from BFH I also thank all of my colleagues and friends from the Nursing Science and the Master of Science in Nursing Programme of Bern University of Applied Sciences. Your support, inspiration and many enriching discussions have accompanied and motivated me on my way to a PhD. My special thanks go to Christoph Golz, Niklaus Bernet, Madeleine Bernet, Silvia Thomann, Caroline Gurtner, Fabienne Renggli, Thomas Schwarze, Xenia Schmid, Prof. Dr. Maya Zumstein-Shaha, Prof. Dr. Eva Soom Ammann, Iris Lipp, Dr. Friederike Thilo, Dr. Dirk Richter, Dr. Reto Bürgin, Tannys Helfer, Prof. Dr. Christian Eissler & Andrea Eissler, Dr. Birgit Heckemann and many more. You are a wonderful team and I am very happy to be a part of it.
About the author

About the author
198
About the author
Karin Anne Peter was born in December 1987, in Wetzikon, Switzerland. She started her professional career as a junior nurse (2004 - 2007) on a paediatric oncology ward in an orthopaedic university hospital. During her training, she was already interested in the research department of the hospital and was able to gain early insight into research with spine-injured patients. After finishing her education as a junior nurse, she started her Bachelor of Science in Nursing at the Zürich University of Applied Sciences (2007 – 2010). During her Bachelor studies she worked part-time in a nursing home that specialised in patients with dementia, and thus gained experience in the care of patients in various stages of dementia. Therefore, she wrote her Bachelor thesis on 'Malnutrition in Morbus Alzheimer'.
After her receiving her degree in Nursing Science, she took up a position as a nurse with special responsibilities (Fachexpertin Pflege) in a general surgical department in a district hospital (2010 - 2013). She was responsible for the care and treatment of general surgical patients as well as professional support of nurses in complex patient situations, and further participated in the development of evidence-based nursing guidelines, nursing care paths, nursing concepts, and care-related education programmes.
Alongside her job, she started her Master’s degree in Nursing Science at the Bern University of Applied Sciences (BFH) in 2011, with a special focus on prevention, health promotion, efficacy and efficiency in the healthcare sector. She wrote her Master's thesis on 'Aggression against young nurses', including quantitative as well as qualitative approaches, supervised by Prof. Dr. Sabine Hahn. During her work at the District Hospital she was also frequently confronted with the issue of stress at work. After a demanding night shift in which she alone was responsible for 33 patients, several emergency admissions and patients coming directly from the operating theatre, she finally handed in her resignation due to poor working conditions. Following this experience, Karin A. Peter has set herself the goal of making a contribution towards better working conditions in the healthcare sector.
In 2013 she started a new part-time position as a clinical nurse specialist in the department of plastic /reconstructive surgery at the University Hospital of Zürich and was responsible for three wards. In her role as a clinical nurse specialist, she was responsible for the development and implementation of nursing quality standards as well as the guidance and tutoring of nurses and was authorised to instruct specialised nurses of her team. Also, she was the leader of various practice development and research projects in her department and was the responsible nurse of the CIRS (Critical Incident Reporting System) Committee of Plastic Surgery for nurses and physicians.
At the same time, Karin Peter started working part-time as a research associate in various research projects at the Bern University of Applied Sciences.
About the author
199
In her role as a research associate, she has been involved in various projects and has been the leader of an inter-professional project in the field of 'psychosocial health'. In addition, she carried out teaching activities in a Public Health course, in the Bachelor of Science in Nursing and as a module leader in the Master of Science in Nursing (in the module ‘Intervention & Outcome’). Since 2017 Karin A. Peter has worked as a research associate on a full-time basis.
In 2015, she started her PhD in the European Doctoral Program in Nursing Science, organised by the University of Maastricht, the University of Graz and the Bern University of Applied Sciences. Under the supervision of Prof. Dr. Jos M.G.A. Schols (Maastricht University), Prof. Dr. Sabine Hahn (Bern University of Applied Sciences) and Dr. Ruud J.G. Halfens (Maastricht University), working towards her PhD in the field of work-related stress among health professionals. Her thesis forms part of the STRAIN project, ‘work-related stress among health professionals in Switzerland’, in which she is also project leader. The STRAIN project is one of the largest current research projects in the Swiss health care system, including over 160 participating organisations with the aim of improving long term working conditions through a standardised intervention with health professional leaders.
Since the beginning of 2020, Karin A. Peter holds a management position as Head of the Innovation Field – Healthcare Personnel Skills and Development in the Nursing Research Department at the Bern University of Applied Sciences. She is also part of the Steering Committee and project leader of the BFH-projects in the Competence Network Health Workforce (CNHW), which aims to develop a national strategy against staff shortages in the health care sector.
Publications
Publications
202
Publications in peer-reviewed Journals
- Peter KA, Hahn S, Schols JMGA, Halfens RJG. Work-related stress among health professionals in Swiss acute care and rehabilitation hospitals-A cross-sectional study. Journal of clinical nursing. 2020;29(15-16):3064-3081. doi:10.1111/jocn.15340
- Peter KA, Schols JMGA, Halfens RJG, Hahn S. Investigating work-related stress among health professionals at different hierarchical levels: A cross-sectional study. Nursing Open. 2020;7(4):969-979. doi:10.1002/nop2.469
- Peter KA, Hahn S, Stadelmann E, Halfens R, Schols J. Assessing Work Stressors in the Health Care Sector by Combining External Observation and Health Professionals’ Self-report in a Cross-sectional Study Design. Occupational Medicine & Health Affairs. 2020;8(1):303-309.
- Golz C, Peter KA, Hahn S. Cognitive Pretesting and pretest of the STRAIN questionnaire to elaborate work-related stress of health care staff in Switzerland. International Journal of Health Professions. 2018;5(1):109-120. doi:10.2478/ijhp-2018-0011
- Heckemann B, Peter KA, Halfens RJG, Schols JM, Kok G, Hahn S. Nurse managers: Determinants and behaviours in relation to patient and visitor aggression in general hospitals. A qualitative study. Journal of advanced nursing. 2017:11. doi:10.1111/jan.13366
- Peter KA, Golz C, Richter D, Eichenberger zur Bonsen D, Hahn S. Psychosoziale Gesundheit und Gesundheitsförderung bei Hochschulmitarbeitenden - Ein Praxisprojekt an der Berner Fachhochschule. Pädagogik der Gesundheitsberufe. 2015(2):75-79.
- Peter KA, Hahn S. Aggressionserlebnisse junger Pflegefachpersonen im Akutspital: Eine qualitative Situationsanalyse. Journal für Qualitative Forschung in Pflege- und Gesundheitswissenschaft. 2014;1(1):32-39.
Publications in non-peer-reviewed Journals
- Peter KA, Hahn S. Stress am Arbeitsplatz - Ein Projekt der Berner Fachhochschule will Belastungsfaktoren am Arbeitsplatz reduzieren. NOVAcura. 2017;48(4):13-15.
- Golz C, Beck M, Peter KA. Projekte gegen den Fachkräftemangel in den Spitex-Organisationen. Spitex Magazin. 2017(5):44-45.
Publications
203
- Thomet C., Peter KA. Förderung eines guten Betriebsklimas ist zentral. Krankenpflege. 2015(4):22-23.
- Peter KA, Hahn S. Auswirkungen von Aggression im Akutspital. Krankenpflege. 2014(12):14-15.
Conference contributions
- Peter KA, Hahn S, Schols JM, Halfens, RJG. Work-related stress among health professionals in Swiss acute and rehabilitation hospitals – results of a cross-sectional study. Oral presentation. The 18th European Doctoral Conference in Nursing Science, Graz, Austria, 2019.
- Peter KA, Golz C, Hahn S. The STRAIN Study - assessing and reducing of work-related stress among health professionals in Switzerland – a study protocol. Poster presentation. The 1st International Conference: Countering Staff Shortage Among Health Professions - Together for a Healthy Health Care System, Bern, Switzerland, 2018.
- Hahn S, Richter D, Peter KA, Heckemann B. Aggression and healthcare professionals – different perspectives, different needs. Symposium. STTI 4th European conference, Cambridge, United Kingdom, 2018.
- Peter KA, Golz C, Hahn S, Richter D. Aggression in German Acute Care Hospitals - Results of a Mixed Method Study. Oral presentation and conference paper published in: Needham I, McKenna K, Frank O, Oud N. Fifth International Conference on Violence in the Health Sector Broadening our view - responding together. Dublin, Ireland, 2016.
- Peter KA, Hahn S. Young nurses and experiences of aggression: a qualitative content alanysis. Oral Presentation and conference paper published in: Callaghan P, Oud N, Bjorngaard JH, Nijman H, Palmstierna T, Duxbury J. Violence in clinical psychiatry. Copenhagen, Denmark, 2015.
Blog Publications
- Peter KA, Hahn S. Wie belastbar ist das Schweizer Gesundheitssystem in Krisensituationen? Bern: Competence Network Health Workforce; 2020.
- Peter KA. Arbeitsbelastung in den Gesundheitsberufen: Was können Führungskräfte tun? Knoten & Maschen - BFH Blog zur Sozialen Sicherheit. Bern: Bern University of Applied Sciences; 2019.





























