Embed Size (px)
Citation preview

1
Work package 5
Improving capacity for high quality comprehensive reporting
(as part of Deliverable n°4 )
Report from the working group on
Linking databases on perinatal health (Topic 2)
Euro-Peristat Action Project
Working group members
Marie Delnord
Katarzyna Szamotulska Ashna Monhangoo
Mika Gissler Carmen Barona Henrique Barros
Sylvie Berrut Jim Chalmers
Nirupa Dattani Luule Sakkeus
Isira Zile Jennifer Zeitlin
May 2014

2
Introduction
One of the difficulties of perinatal surveillance in Europe is the heterogeneity of data sources
used for reporting in European countries. In 2013, the Euro-Peristat project published a perinatal
health report on maternal and infant health indicators with data from 29 countries. To construct the
indicator set, most countries had to use data from multiple sources, including birth certificates, death
certificates, medical birth registers, specific registers or audits, hospital discharge data, professional
databases and surveys. When combining data from these registries, differences in data collection
processes, inclusion criteria and use for the registry (civil registry, hospital discharge database,
perinatal registry) can affect data completeness and comparability.
Record linkage of multiple data sources has the potential to overcome many of these
problems and improve the overall validity of registry data by harmonizing data systems, ensuring
completeness of coverage and increasing the information available about each birth. For example,
because unique patient identifiers are rarely included within patient registries for anonymity
purposes, linkage can resolve discordant or missing information for mother and child dyads and
improve ascertainment of short and long term perinatal outcomes. In fact, studies increasingly
report on the added-value of using linked data to answer complex research questions; in the
literature, such techniques have been successfully applied to both maternal and infant health.
Whereas some countries integrate data linkage into their routine perinatal health
surveillance systems and make these data available for research, this is not systematic practice
across Europe. Optimizing the validity of perinatal data is necessary to realize cross-country
comparisons of health indicators and produce evidence-based recommendations applicable to
mothers and infants. Having common recommendations in the EU about which linkages are most
useful for perinatal health reporting would be one way to improve the quality and breadth of
European perinatal health surveillance.

3
To this aim, the Euro-Peristat project carried out a comprehensive review of publications on
perinatal health based on linkage of routine data sources published in the last decade. The objective
was to describe sources that have been used for the study of perinatal health, the themes that have
been explored using linkage. We also sought to identify countries and systems in which linkage was
routinely undertaken to permit other countries to benefit from this knowledge base.
Methods Review of publications based on linked data from routine sources
Using EndNote 9, we searched PubMed for perinatal health studies using routinely linked
data and published in the last ten years from September 2001 to January 2011. Record linkage was
defined as linkage of two registries, of a cohort database to a routinely updated dataset, or by pairing
of mother and baby records within a single registry. Particular attention was paid to only include
studies crossing datasets together (i.e. using manual, probabilistic or deterministic techniques) as
opposed to simply combining data from multiple sources.
For this search, the following terms were used solely and/or combined: data linkage,
perinat*, matern*, link*, registr*, medical record linkage, infant newborn and birth certificates.
Study titles and abstracts provided the basic information for inclusion in this review. To increase the
comprehensiveness of our study, we contacted members of the Euro-Peristat network for any
additional research citing linkage use and that we might have missed. We excluded studies which did
not match our inclusion criteria as well as data published in conference reports, summaries and other
reviews. 521 studies met our inclusion criteria.
From each abstract, we identified the types of datasets which were linked and the main
outcomes of the study. Data for this review came from the following registries (1) Birth records (2)
Death records (3) congenital anomalies registry (4) hospital records (5) Professional registries
(midwives, obstetricians, pediatricians) (6) Cancer registry 7) Other illness/disability registry (8)
Medical birth registries , Census data (9) Cohort (10) Screening registry (11) Psychiatry registry (12)

4
Assisted Reproductive Technology registry (13) Prescription registry (14) Conscription registry (15)
Education registry (16) Insurance registry (17).
Registries could be cross-categorized based on the type of data collected. For instance, the
Midwives’ Birth notification System of New South Wales, Australia is a health professional registry
which functions like a medical birth registry and was coded as such in our review - based on all
applicable registry categories (ie. Medical birth registry AND professional registry). Because individual
registries were also identified by name, this did not impact on the number of datasets recorded per
study. Similarly, linked datasets such as the Oxford Record Linkage Study were accounted for once
but were coded based on all composite parts namely: the Registrar General, hospital discharge data,
and domiciliary midwives case notes registries. Datasets used in less than 10% of our total study
sample were aggregated in the “Other” category.
Next, we grouped studies into 5 themes: fertility, fetal, neonatal and child health, maternal
health, health services, and methods in record linkage. We also identified studies based on outcomes
occurring either during the perinatal period (pregnancy, delivery and the postpartum) or outside this
period (pre-pregnancy or after the post-partum period). All studies were further coded by
publication year and country of origin. I
Inclusion criteria and coding were validated by a second author prior to data analysis. To
describe trends in perinatal health record linkage research, we calculated percentage rates of
publication by research theme and linkage types within countries and by year. Data were analyzed
using STATA 10.0 software (StataCorp LP, College Station, TX, USA).
Review of current linkage practices in routine perinatal health surveillance systems in Europe
We used data from the Euro-Peristat project to describe current linkage of routine perinatal
health surveillance systems in Europe. The Euro-Peristat project collects population-based aggregate
data on a set of core and recommended perinatal health indicators using a common protocol and
data collection instrument.[25, 26] Scientific committee (SC) members (clinicians, statisticians, or

5
researchers) from each participating country are responsible for data collection. In 2013, the Euro-
Peristat project released The European Perinatal Health Report: The Health and Care of Pregnant
Women and Babies in Europe in 2010. This publication brings together data from 26 European Union
member states, plus Iceland, Norway and Switzerland. For this report, SC members provided
information on the datasources which were used to construct the Euro-Peristat indicators and on
linkage between data sources. Based on our literature review, we identified recurrent linkage types
used for perinatal health research and requested further information on routine linkages for
perinatal health surveillance done at the national level. More specifically, we asked SC members to
confirm the availability of the following linked data: linkage of birth and death certificates, vital
statistics and medical birth registry data, medical birth registry data and hospital discharge data, and
other routine linkages.
Results
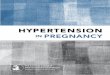
Publications using linked data 525 studies fit our inclusion criteria. Studies were concentrated in
a few countries, as illustrated in Figure 1; nearly half were from the US, Sweden and the UK.
Linkage of vital statistics data, hospital records, medical birth registers and cohort studies were
performed to conduct original life-course analyses, confidential enquiries, provide subgroup
estimates of maternal or infant mortality, and to study trends in perinatal health indicators. This is
illustrated in Figure 2. Most of the studies linked data from birth certificates, death certificates,
medical birth registers, Databases included congenital anomaly registers (50), Insurance (21)
prescription data and specific registers : cancer (61), congenital anomalies (50) professional (43)
psychiatric (18), screening (17), ART (16). Data were also linked to census (62) and educational data
bases (10).
6
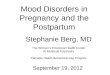
Twenty out of 32 (62.5%) European countries conduct routine perinatal health linkages; these
linkages were used to derive Euro-Peristat perinatal indicators in 2010.

7
Discussion
Routine linkage of data sources is an effective technique to enhance the validity of perinatal
health data by harmonizing data systems, ensuring completeness of coverage and increasing the
information available about each birth. Although routine linkage of data sources is a cost-effective
tool which has been shown to further perinatal health research and public policy planning, our
review shows that this technique is largely under-used in many countries.
One main advantage of linking routine surveillance databases for research is that studies
based on this type of data collection can be considered highly cost-effective cohort studies. By
linking 2 or more registries, a group of people (i.e. All women of reproductive age within a specific
time period) can be identified and monitored without having to incur the costs of a long follow-up
time. In fact, most population data collection systems already hold individual level data on
characteristics such as: age, sex, place of birth, place of residence, or occupation. Perinatal health
researchers can make further use of these data by linking to hospital discharge data which will

8
provide information on care, services and outcomes – this type of linkage has been used to recreate
women’s reproductive histories or to follow-up of babies born at risk of adverse health and social
outcomes (ie very preterm babies). Linkages with other specific registries such as to population
registers and/or medical birth registries also provide opportunities to research the etiology of chronic
conditions such as diabetes or hypertension.
Linkage of surveillance data increases researchers’ capacity to conduct original life-course
analyses. Data linkage has been extensively used applied in cancer research to explore the
association between environmental exposures in the perinatal period and malignancies diagnosed
later in life (i.e. childhood cancers such as neuroblastomas). These techniques have also allowed
researchers to explore other perinatal health issues longitudinally such as cognitive outcomes of
babies born with congenital health defects for instance.
Linkage of routine datasets is a tool which scientists can use to answer complex research
questions by optimizing the use of current available resources. Merging datasets can allow scientists
to cost-effectively increase the power of their statistical analyses by collecting information on a
larger number of individuals and explore geographic and temporal trends that may confirm specific
research hypotheses or provide impetus for new research.
Besides furthering the perinatal health research field, routine linkage of data systems enables
countries to develop their capacity for high quality perinatal health surveillance and reporting.
Results from studies based on linkage can be used to derive evidence-based public health strategies
targeting mothers and babies. Additionally, linkage of data systems can limit the number of missing
data items for key perinatal health variables (ie. Gestational age) and enables the external validation
of routine surveillance systems within networks, regions, or countries. These techniques have been
applied for confidential enquiries and in providing estimates of maternal or infant mortality or to
study trends in severe maternal morbidity.
Where birth and deaths records are linked in routine, data by subgroups such as birthweight
or gestational age are made available to health policy planners for them to set benchmarks or goals

9
for targeted public health initiatives. Another example, hospital discharge data contain valuable
information about medical acts and diagnoses, but their primary use in many countries is for hospital
management and financing and not for epidemiological surveillance; these data do not include basic
socioeconomic and demographic information often collected as part of vital statistics reporting.
Linkage of both hospital discharge data and population datasets can be used in ascertaining health
disparities in maternal deaths. Where medical birth registry and vital statistics, data on births by
other factors such as mother’s age become available and can be used in strategizing on the
prevention of teenage pregnancy which is a policy concern in many countries.
Based on our survey, perinatal health experts across Europe, recommend the following
linkage types for routine perinatal health surveillance: -linkage of birth and death certificates, vital
statistics and medical birth registry data, medical birth registry data and hospital discharge data.
These linkage types enhance the data available for surveillance of perinatal health and have been
used to provide data for the Euro-Peristat indicators
Conclusion and key messages
Linking existing data on perinatal health is a readily available option for improving the quality and
completeness of some indicators, for both policy and research use. This technique has been
successfully used in some countries, whereas in others it is largely under-used. Countries should be
encouraged to develop capacity to generate high quality perinatal health data based on linkage of
routine datasets thereby adding value to existing national and international investments in health
information systems. Broader adoption of linkage techniques which are already in force in many
countries could yield substantial gains for research and surveillance of perinatal health nationally and
internationally

10
Annex 1. Coverage of the linked dtasources in the European Perinatal Health Report: Health and care of pregnant women and babies in Europe in 2010
Country Source Data administrator Coverage Includes nationals who are residents?
Includes nationals who deliver outside the
country?
Includes non-national
residents?
Includes non-nationals who are
not residents?
Denmark The Medical Birth Registry SSI, Statens Serum Institut, under the Danish Ministry of Health
± 100 % Yes No No No
Germany Destatis Statistisches Bundesamt Wiesbaden (Federal Statistical Office)
± 100 % Yes No Yes No
Estonia Estonian Medical Birth Registry National Institute for Public Health
± 100 % Yes No Yes Yes
Estonia Estonian Cause of Death Registry National Institute for Public Health
± 100 % Yes Yes Yes Yes
Estonia Linked Data from EMSR ( Medical Birth) and SPR (Causes of Death
Estonian Institute for Population Studies, Tallinn University
± 100 % Yes Yes Yes Yes
France ENCMM Inserm U953 ± 100 % Yes No Yes Yes
Cyprus Death Registry 2004-2010, Health Monitoring Unit, Cyprus Ministry of Health
Health Monitoring Unit ,Cyprus Statistical Service
± 100 % Yes Yes Yes No
Lithuania Database of the Demographic Statistics
Central Statistical Office ± 100 % Yes Yes Yes No
Lithuania Causes of Death register Institute of Hygiene Healf Information Centre (HI HIC)
± 100 % Yes Yes Yes Yes
Luxembourg Registre des causes de décès du certificat de décès
Ministry of Health - Direction of Health
± 100 % Yes Yes Yes Yes
Luxembourg Registre des causes de décès du certificat de décès périnatal
Ministry of Health - Direction of Health
± 100 % Yes Yes Yes Yes
The Netherlands
PRN The Netherlands Perinatal Registry
96% Yes No Yes Yes
Austria birth + cause of death statistics for infant death
Statistics Austria ± 100 % Yes No No No
Portugal General Directorate for Health - Maternal Deaths
General Directorate for Health
NA Yes No Yes Yes
Portugal RENAC - Portuguese Birth Defect Registry
Department of Epidemiology, National
During the period 2002-2007 the mean coverage was 67%.
Yes No Yes No

11
Health Institute Dr Ricardo Joge.
Portugal Hospital Discharge Data Central Administration of the Health System (ACSS)
All Public Hospitals in the country.
Yes No Yes Yes
Romania NCSIPH DRG NCSIPH Country level public hospitals only
Yes No Yes No
Finland Population Statistics Statistics Finland ± 100 % Yes No Yes No
Sweden Medical Birth Registry The National Board of Health and Welfare
99.4 % Yes No Yes Yes
Scotland Scottish Stillbirth and Infant Death Enquiry
Information Services Division of National Services Scotland
The population is complete for stillbirths and infant deaths but not for terminations.
Scotland Scottish Morbidity Record (SMR02) Information Services Division of the NHS National Services Scotland
98%
Scotland Maternity and Neonatal Linked dataset (SMR02, SMR11, Scottish Birth Record, Stillbirth and NeoNatal Deaths records)
Information Services Division at NHS National Services for Scotland
95%.
Norway Medical Birth Registry of Norway The Medical Birth Registry of Norway, the National Institute of Public Health
±100% for live births, some fetal deaths missing
Yes No Yes Yes
Switzerland BEVNAT, statistics of natural population change (vital statistics)
Federal Office of Justice, Swiss Federal Statistical Office
± 100 %, some underreporting of fetal deaths
Yes Yes Yes No
Switzerland MS, Medical Hospital Statistics The Swiss Federal Statistical 97,5% Yes No Yes No

12