-
8/12/2019 Word of Guidance Med Interns
1/30
2
A WORD OF GUIDANCE TO
MEDICAL INTERNS
Dr. S. Terrence G. R. De Silva,
(MBBS, DPS, DFM, DLSHTM, M.Sc. (Lond), MD)
Deputy Director General (Medical Services) I
(Former Director of the National Hospital of
Sri Lanka, Colombo)
2009
-
8/12/2019 Word of Guidance Med Interns
2/30
3
Copyright 2009 Ministry of Healthcare & Nutrition,Sri
Lanka
Published by Medical Services Division
ISBN 000-000-0000-00-0
Contributors:
Dr. S. Terrence G. R. De SilvaDr. Lakshman Senanayaka
Dr. Deepthi Samarage
.. (Blood Bank)
4
Content Page
You and Your Patients 08
Principals governing provision of medical care .. 21
Eight points concept to enhance positive attitudes towards
patients 22
Avoiding Medical Errors 28
A message from Blood Bank .. 40
Communication skills for Doctors .. 50
Guidance in issuing medical certificates . 56
-
8/12/2019 Word of Guidance Med Interns
3/30
5
Message from the Hon. Minister of Healthcare and
Nutrition
At the outset let me congratulate you for selecting a
nobleprofession as your vocation and successfully completing
your
university degree.
You are about to start the mandatory training period which
would give you the necessary experience and skill which is a
prerequisite to heal the sick with responsibility.
Sri Lanka is proud of its achievements in the field of
health
care, which is amply substantiated by our health indicators
which are comparable to those in the developed world.
One of the important factors that contributed to this
success
story is the commitment and dedication of all the health
care
workers functioning at different levels in the Ministry of
Healthand peripheral institutions. I am happy that the majority of
our
staff working towards providing Quality Health Care to all
SriLankan without any discrimination.
Brief but valuable information in this booklet would guide
you
to be a worthy professional to whom the Sri Lankan publiccould
truly be grateful for.
Nimal Siripala De Silva
Minister of Healthcare and Nutrition
6
Message from the Secretary, Ministry of Healthcare
andNutrition
I wish to welcome you to the Ministry of Healthcare and
Nutrition.
I am very happy that the Ministry of Health was able to
provide
you with this opportunity of training as a medical intern to
improve your knowledge and also gain the necessary
understanding and skills to treat the sick.
It is indeed a challenge to be able to fulfill the ever
increasing
expectations of the public who seek care, within a rapidly
enlarging horizon of technological improvements and access
to
information.
You as a House officer would be playing an important role at
the interphase between the care seekers and the care
providers,
which would indicate the responsiveness of the Health Serviceand
ultimately the fulfillment of the expectations of the patients.
The Guidance gained from this booklet will assist you to
achieve this difficult but essential part of your training.
Dr. Athula KahandaliyanageSecretary
Ministry of Healthcare and Nutrition
-
8/12/2019 Word of Guidance Med Interns
4/30
7
Message from the Director General, Ministry of Healthcareand
Nutrition
While greeting you as young members of the medical
profession, I am glad that you would have the advantage
ofmeeting, examining and treating the large number of patients
attending the Ministry of Health Hospitals which eventually
will transform into a vast deposit of clinical experience for
your
future guidance.
At the commencement of your internship I whish to emphasizethat
it is very important to recognize that you are expected to
treat all your patients with dignity, respect and kindness,
to
which they are rightfully entitled to.
This publication summarizes some of the key issues that
wouldguide you to look after these patients in a manner that you
could
be proud of.
Dr. Ajith Mendis
Director GeneralMinistry of Healthcare and Nutrition
8
You and Your Patients
By Dr. S. Terrence G.R. De Silva,
MBBS, DPS, DFM, DLSHTM, MSc, (Lond), MD
Deputy Director General (Medical Services) I(Former Director of
the National Hospital of Sri Lanka,
Colombo)
A time tested system of providing medical care existed for a
long period. The history taking, the physical examination and
afew basic investigations were done to arrive at the diagnosis
of
ailments. However, some of the recent advances in medical
science, the technological innovations and the different
teachingmethods followed in various medical schools specially,
outside
Sri Lanka, have threatened the existing low cost patient
care
system. The young doctors today, tend to bypass the
historytaking & physical examination and try to rely mainly on
thelaboratory & radiological investigations which are very
expensive and at times beyond the capacity of our hospitals.
In addition, there are increasing public expectations and
demands for high quality service. Many of the patients
haveaccess to medical information via the improved information
technology and they show an increased desire to involve with
the decisions related to their healthcare.
As far as the health indicators are concerned the health
serviceof this country is almost in par with those in the
developed
countries. People of this country are generally satisfied with
the
health service and they have placed their trust and confidence
in
this system. Nevertheless, in recent times, the attitudes of
those
in the sphere of health towards their patients have left much
to
be desired. Perhaps this is part and parcel of the situation in
thesociety at large. It is the duty of everyone to protect our
health
-
8/12/2019 Word of Guidance Med Interns
5/30
9
system. For this it is necessary to strengthen the
positiveattitudes and qualities among the health care staff. This
booklet
A Word of Guidance to Medical Interns was prepared withthe aim
of making an attitudinal change among the young
doctors.
What Your Vision & Mission should be?
Having successfully completed your school education, you
made up your mind, sometimes against many odds, to become a
successful medical professional in this country. Sometimes itmay
have been an aspiration you have had over a number of
years. Becoming a successful medical professional was your
deep rooted vision and by this time you have been partly
successful in realizing this vision.
As a medical professional it is your duty to care for and
treat
with kindness, love and empathy, your fellow human beings
who are ill and incapacitated. This is your mission as a
medicalprofessional. In order to make your vision a complete
success
you must ensure that you carry out your mission withdedication
and commitment.
The Ministry of Health respects your vision and values your
desire and decision to carry out your mission. Recognizing
yourvision and the mission stated above, the Ministry of Health
extends you a warm welcome to the Ministry. Our Ministry isthe
prime healthcare provider of this country.
You are today commencing a journey with a small step but a
giant leap forward. Let me emphasize at this stage that there
is
no red carpet for you to tread on, but a long and yet
satisfyingand meritorious path ahead, if you would only
dedicate
yourselves.
10
Those medical professionals who are already serving theMinistry
of Health and the Professorial Units attached to the
Faculties of Medicine are always ready to help you to carry
outyour mission and to realize the goals you aspired to achieve
in
your life.
The Internship Appointment
I am sure from the day your name appeared in the list of
students who have passed the final MBBS examination on the
Medical Faculty notice board you have been eagerly waiting
forthe internship appointment. You would have been extremely
thrilled on this day over your success at the examination
and
realization that henceforth you will be addressed as Doctor.
We have no doubt that you and all your family members would
have enjoyed this happy moment.
Going through your life, the day you assume duties as an
intern
house officer is going to be another memorable day.
However,internship is not plain sailing. Only once you commence
the
internship you would realize the challenges that come with
it.You will have to spend long sleepless hours, attend to
virtually
never ending ward work and face criticism and sometimes theblame
from your superiors including the Consultants & the
Senior Registrars (who actually have gone through the
samehardships before you). You may feel like a slave, a laborer,
a
prisoner, and at times be in a confused emotional state. Do
notget disheartened about this, but think in terms of
perseverance
and endurance. The Internship period is a compulsory
training
and I should say that to most of us, it is really a hard
time.
During the Internship you will feel the taste of what is
available
for you, sometimes sweet, sometimes sour, sometimes bitterand
all blended with ingredients of hard work, personal
sacrifices, mental fatigue frustration, and of course the
-
8/12/2019 Word of Guidance Med Interns
6/30
11
satisfaction realizing that you have helped a human being
toalleviate his suffering.
In the midst of all this you might even question yourself as
to
your choice of the medical profession. You might even blamethose
who encouraged you to become a medical doctor. I have
seen some interns comparing their lives with those of their
schoolmates who are serving in different fields, with much
free
time and the ability to spend to enjoy life.
You must not be discouraged at this stage and must develop
apositive attitude and gain strength to face all these
situations.
Accept your internship as an opportunity to become a
successful medical professional in future. Many years later
when you walk down the memory lane, you will recall the sadand
happy moments, the lessons you learnt from your superiors
and also from the patients, the skills you were able to
develop
and the superiors who were there to guide you and all
otherthings that made you richer in experience. Most of the
Senior
Registrars and Consultants who trained you and sometimesblamed
you would become lifelong friends. Later on you will
realize that most of them are with you at times of distress
andneed, throughout the rest of your life. This is the beauty of
the
strenuous training.
At present you may be at the bottom rung of the
professionalladder, and you have to climb step by step and one day
you will
reach the top rung. I must emphasize that you may have to
continue to struggle during the rest of your career too, but
am
sure will improve as you go along.
12
What is Special about Your Work in the Health Sector?
The Healthcare Service is saddled with the responsibility of
caring for and pursuing human life. First of all, think of
thecrucial role you play in such an esteemed noble service and
come to terms with the importance of the task you are calledupon
to perform.
Naturally, the position you hold in the Health Care Service
provides you with a livelihood. Yet, in this noble service,
youhave to accept your position, as more of a calling than a
job,
giving you an opportunity for a meritorious service.
The Specific Nature of Your Work
The Health Care Service has its own share of public
liaisonactivities. The hospital is a busier place than a
government
office which serves a limited clientele. Work at a hospital is
of a
more arduous and one may face diverse problems. It is often
difficult to provide a service to please everyone and to meet
theexpectation of people from all walks of life and holding
varied
requirements. It is more so, since the people who come to a
hospital for treatment are patients ailing from various
illnesses.
As an intern and thereafter as a medical officer you may
havecertain specific difficulties. These include the restrictions
in
obtaining leave even for an urgent personal matter, obligation
toreport for work even on Sundays and public holidays which is
a
facility enjoyed by the other state employees, to work on
nightshifts and the need to report for work during such crisis
as
disrupted transport services and being called upon to work
onunexpected work shifts in emergencies.
The medical professionals like anybody else have to face
personal or family problems. Despite all these, you are
expected
-
8/12/2019 Word of Guidance Med Interns
7/30
13
to work in a spirit of dedication. Whatever your
personalconstraints are, when you are on duty at the hospital, your
mind
and heart should go out to the patients. This is the nature of
thework of a medical professional.
Communicating with the Patients
One of the important and challenging part of providing care
during the internship and thereafter as a medical officer or
a
specialist is establishing a good rapport with patients and
their
relations, and communicate with them in such a way to makethem
recognize your commitment and ability to provide care
using your skills and knowledge.
The first impression of any person coming into contact with
you
is governed by the way you appear and the way you carry
andpresent yourself.
You have to be neat, clean and tidy and with your hair
wellcombed and also face well shaven or beard trimmed. It is
important that you conduct yourself like a professional. Theway
you talk, the way you smile, the way you walk and the way
you behave in front of your patients, relations, superiors
etc.should generate respect not fear or disgust. The patients
generally have a perception about how a doctor would look
like.Therefore to start with your appearance and behavior should
be
like a doctor.
14
Bestow Compassion on Patients
Compassion is a must you should have. Your smile costs
younothing, but it makes you a pleasant and comfort person to
the
patient. Go about your work with a smile on your face. Whatgood
will be done by blaming the patient instead of using kind
simple words when you want to advice, which will be of more
effective. In patient care, flexibility is of vital
importance.
Always try to accommodate the requests of patients as far as
possible, because then only they will be able to comply.
When you talk about such matters as personal cleanliness, or
in
instances of giving medical advice, do so after calming your
mind and without anger. When you explain the matters related
to an illness to the patient or to his relations, use the
simplest
language possible, the common, conversational
languageunderstandable to layman. Not only is the medical
terminology
may be beyond their grasp, they may be further confused by
such words, which may be misunderstood in a way totallydifferent
from the way you meant them to be.
It is necessary to address the patients with due respect and it
is
always better to address the patient by name, and ensure that
hisdignity and self-respect remains unsullied. The words that
make
the patient pleased can be used. To cite examples, addressing
apatient as Mr. or Madam may go a long way to win the
confidence of patients and their relations. Using polite words
asplease, help to make patients conduct themselves well during
their stay at the hospital. Similarly, in case of an
inadvertency
on your part, do not hesitate to say sorry with an
explanation.
Making an apology is not something to be ashamed of when
you have done a mistake.
-
8/12/2019 Word of Guidance Med Interns
8/30
15
Who is the VIP at the Hospital?
The VIP at the hospital is the patient and no one else. A
hospitalcould be considered as a sacred place. In the days gone
past,
patient care and cure were associated with temples
andchurches.
A patient enters the hospital in a physically weak and
mentally
depressed state. Your patient expects from you the same
affection, kindness, compassion, attachment and love that a
child expects from his mother, If you can ensure that
thisexpectation is fulfilled, the patient will think of you as
having
divine qualities. If he or she feels so, it will give you a
satisfaction of being special among others. The blessings
the
patient invoke will surely fall on you and your loved ones.
See whether the meaning of the adaptation of this poem taken
from a Sinhala didactic work is relevant to you.
we; ; ak e; ; amr f , dj i qo f k k suy ;y f
-
8/12/2019 Word of Guidance Med Interns
9/30
17
Do unto the patients what you like others do unto you, insimilar
situations. Keep in mind the fact that one kind word
from you gives the patient more relief, than a drug
worththousands of rupees.
Soothe the Pain
In the story of Mother Theresa it is stated that one day she
found a dying woman half infested with maggots and bitten by
rats. Mother Theresa sat besides her stroking her head
gently
till her death. Did you take to medicine to act in the same
spirit?Of course Mother Theresa later on in her life became a
willing
companion for the dying; washing their wounds, soothing
their
sores and preparing them for death with dignity.
Patients like to know about their condition. Thanks to the
freeand compulsory educational policies of the government of
Sri
Lanka 98 % of people are literate. Patients know something
about illness and want to know what is wrong with them,why it
happened, what more will happen and most
importantly what we are going to do with them and whetherany
further problems will happen because of what we do. We
should not assume that simply because we are doctors orbecause
we are providing free medicine they would accept our
word without questions.
As doctors we are obliged to spend adequate time to explainthese
matters and put their minds at ease. On the other hand the
best antidote to fear is providing correct information. Once
the
patient realizes the actual condition of his illness (which is
often
less than he would have imagined) and the balanced view of
the
advantages and disadvantages of the treatment offered to them,it
would be his wish that we should respect. This ability to
communicate you would have developed over the last few years
18
of training. Additional guidance would be available in
thisbooklet.
Patient is also a Member of a Family
When a patient is hospitalized, the patient as well as his
family
members faces a variety of difficulties. Think of a situation
at
your own home if the mother is hospitalized! Those at home
may be deprived of the person who did the cooking and other
essential household activities. If the father is hospitalized,
the
family may miss the sole breadwinner. When you deal withpatients
such factors should also be taken into consideration.
Dont forget the patient is a member of a family. Give a kind
and sympathetic hearing not only to the patients, but their
relatives as well.
Although the state provides free medicines and the services,
they also contribute the same in spending for transport and
other expenses out of pocket. Dont forget that every citizen
ofthis country has contributed to the government coffers by
some
way or other.
Take Pride of What You Have Done to Relieve the Sufferingof the
Sick
Do your duty not merely because of the earnings you make
from the job. Yours is a worthy service the value of whichcannot
be measured in financial terms. Undoubtedly, one needs
an income for a living. Yet real happiness of life can never
be
bought.
Go about your work in a way, that you achieve a sense
ofcontentment in caring for patients. Dont let the patient feel
it,
even if you are facing inconveniences. Learn to enjoy the
satisfaction of seeing your patient recover from his
suffering
-
8/12/2019 Word of Guidance Med Interns
10/30
19
due to your efforts. Thus you achieve nobility in life
asexpounded by the following lines from a famous sinhala song
based on religious teachings.
What other happiness in theworld than health,
What other wealth in the world
than happiness
Most professionals take great pride in their professions and
always strive to maintain high standards and a sense of
greatfulfillment in what they are doing. Similarly we who are in
the
health sector providing care should take pride and comfort
ourselves from what we have done to help to alleviate the
pain
and suffering of fellow human beings.
A Better Future for Our Children
Today we have to play our role properly; if not therepercussions
would not only on us but also fall on future
generations.
One day when you finally leave your stethoscope aside, if
youhave acted in a way that will make you contented that you
have
led a fruitful life, you are a person who has done your best
forthe country. It is certain that one day you will really
enjoy
that spiritual solace you desire.
A few words from the song Heal the World by internationally
renowned pop-singer Michael Jackson are relevant here.
Heal the world
Make it a better place
For you and for me
And the entire human race
20
There are people dyingIf you care enough
For the living
Make a better place
For you and for me
I wish to conclude this bit of advice, with a quotation of
Albert
Einstein. Only a life lived for others, is a life
worthwhile.
-
8/12/2019 Word of Guidance Med Interns
11/30
21
Principals governing provision of medical care
o Each patient shall be treated as a whole,
irreplaceable,unique, and worthy person
o The patients safety, health, or welfare shall be protectedand
shall not be subordinated to organizational, staff,educational, or
research interests or to any other end.
o The privacy of the patient and the confidentiality ofevery
case and record shall be maintained.
o Behavior reflecting the dignity, responsibility, andservice
orientation of health care professionals, worthy
of the publics respect and confidence, shall be practiced
by all individuals.
22
EIGHT POINTS CONCEPT TO ENHANCE POSITIVE
ATTITUDES TOWARDS PATIENTS
01. SmileThe smile costs you nothing but would give much, by way
ofa comforting and a pleasant feeling in your patients. Thepatients
would be on the road to recovery even before youtalk to
him\her.
02. GreetGreet them with a word such as "Ayubowan" and follow
upby addressing him with the name. This will generate a warmfeeling
which would break the ice and make obtaining thehistory so much
easier.
03. CourteousnessBeing polite and speaking to patients with due
respectwithout any discrimination is very important in
publicservice. It is necessary to answer their queries with
courtesybecause patients have a need and a right to know abouttheir
condition as well as about the treatment you offer.
04. AffectionThe patients will be pleased with you only if the
treatmentyou offer is tempered with a feeling of goodwill and
kindnessthat emanate from the bottom of the heart.
05. ListeningThe art of being a good listener is to create the
space withinwhich the patients could air their own feelings and
thoughtswithout fear. A good listening response is often all that
isneeded to help patients to divulge their inner concerns
andfeelings.
-
8/12/2019 Word of Guidance Med Interns
12/30
23
06. SensitiveBeing sensitive to patients needs is an affirmation
made tothe patient by the health care staff that indicates "Yes,
youare sick and I understand that you are not able to do thethings
you would like to do, or have done in the past." We
should at all times help when we can and understand thatpatients
are the ones who have been inconvenienced by theillness.
07. Be SmartBeing presentable, smartly dressed and a having
pleasingpersonality is important to positively impress your
patientsand will increase the patients compliance
towardsrecommended treatment.
08. Be Prompt.Patients need an answer for their suffering and
will not wait
till the formalities and investigations are completed.
Beingquick in providing treatment, even to provide temporaryrelief,
is the expectation of all patients.
24
${ $ $
-
8/12/2019 Word of Guidance Med Interns
13/30
25
${$ $$ $
-
8/12/2019 Word of Guidance Med Interns
14/30
27
05. M
M J
M I P KM
. O O
P M CA .
06.
O
E ' .
F .
F
k P ' F N O A. O J
C P
M K .
07. K
K E Q I K
FJ F
K CA O
O FK .
08.
, H K
F, O i M
. CA , , L
G O F ..
28
Avoiding Medical Errors
Dr. Lakshman SenanayakeFRCOG, FSLCOG, MA
Consultant Obstetrician & GynaecologistConsultant Hospital
Efficiency & Quality, SLHSDP
What are Medical Errors?
A medical error is an adverse event that could have been
prevented if adequate care had been taken by the care
provider, considering the current state of medical
knowledge.(1)
These do not include some adverse events due to treatment
such as side effects of cytotoxic drugs which are
undesirable
though not entirely unexpected.
Are they Common?
In November 1999 the report of the Institute of Medicine
(IOM)
of USA by Lucian Leape and David Bates entitled To Err Is
Human: Building a Safer Health System, focused a great deal
of attention on the issue of medical errors and patient
safety.
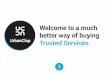
The report indicated that as many as 44,000 to 98,000
people die in hospitals in the United States of America,
each year as the result of medical errors.(2)
-
8/12/2019 Word of Guidance Med Interns
15/30
29
98000
43458
600050
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
100000
Medical
Errors
Traffic
Acci dents
Accid ents
at work
Plane
Crashes
Deaths
Surprisingly in Canada 60 people die due to airplane
accidents
every year where as 24,000 die from medical errors.National
statistics on medical errors are not available in Sri
Lanka, but each of us would know at least of a few instances
either among our relations, friends or patients who had
suffered
on account of a medical error.
I can think of one of my batch mates who had a cautery burnafter
a minor operation which prevented from going for work
for more than two months and a relation who suffered from awrist
drop due to nuropraxia because of the wrong positioning
at surgery.
Recent Media reports of shocking instances of amputation ofthe
wrong leg or accidental cutting off of a finger is still fresh
in
our minds
30
Can they be prevented?
An Australian Study on Adverse Events in hospitals of New
South Wales found that adverse events were preventable in
more than 50% of cases.
A study in U.K. on Adverse Events in Obstetrics andGynaecology
found that more than 50% are preventable.
(3)
Therefore it is important to learn from them and take
measures to prevent them rather than Blame or Shameothers
Why do Medical Errors happen?Medical Errors are mostly due to a
combination of factors rather
than one single factor.
All medical Errors are preventable To err is Human.
To cover up is unforgivable.
To fail to learn is inexcusable.
-
8/12/2019 Word of Guidance Med Interns
16/30
31
Human FactorHuman Error is the aspect which is often highlighted
and you
and I as care providers are directly responsible for
theiroccurrence and we have to individually face the
consequences.
Although every one knows that health care providers do not
cause harm to patients intentionally, the grief reaction of
thevictim and his or her relations usually results in blaming
and
shaming the care providers and sometimes even physically
assaulting them.
Human Errors can be considered underthree headings
Slips and lapses (unintentional)
Mistakes (intentional incorrect action)
Violations (intentional deviation from safe practice)
Slips and LapsesThese are unintentional and may happen because
of:Failure to recognize:
A sign, investigation finding or a change in thecondition of the
patient.
E.g. Not recognizing that the patient is pale indicatinginternal
hemorrhage one may loose the patient brought
to the hospital after a fall from a height. Result is
Patient is lost.
Failure to pay attention to a finding:
Findings such as tachycardia, or tachypnoea may have
been recognized but due attention such as informing
theconsultant, starting a transfusion or correcting the
hydration may not have been done Result is Patient is
lost.
Failure in Memory:An important action may not be done as it has
escaped
your memory. Giving a blood transfusion to a postoperative
patient to compensate the blood loss at surgery
32
in the post op ward. The next call you may get may bethat the
patient has collapsed and bad.
Mistakes
These are intentional and occur when a course of action that
is
incorrect is decided on, and therefore does not have the
desiredresult or even a harmful result.
Rule based:
For example, syntometrine is given for active
management of the third stage in a woman with
hypertension and she subsequently has a fit. A good rulehas been
used in but in the wrong situation.
Knowledge based:
There is a lack of knowledge. Treatment is decided on
without being certain or asking a senior person .It doesnot have
the desired effect. Or worse a harmful effect
Some times a colleague or a nursing officer may point
out the error but the person may not pay attention due tohis ego
or ignorance.
Violations
These are intentional deviation from safe and accepted
practiceor given instructions
Routine:Cutting corners or taking short cuts, e.g. Not
entering
the instructions in the BHT but verbally asking theNursing
Officer to do it.
Reasoned
Interne considers that he can do a forceps for fetal
bradycardia in the delivery room without informing the
senior because the FHS is low or he withholds givingblood to a
patient with a PPH as the blood pressure is
normal although the loss is more than 1000 mls and has
a tachycardia.
-
8/12/2019 Word of Guidance Med Interns
17/30
33
Reckless:Harm is foreseeable but not intended, e.g. Going on
making multiple attempts at a procedure such as LiverBiopsy
without calling for help or imaging assistance or
Going on with uterine massage or Oxytocics for PPH
without calling the Seniors or the Consultant.
What can you do to prevent them Happen?
Communication errors
Communications include not only the verbal discussionsbut the
written communications via the entries in the BHT.
Your notes on the BHT are vital not only for the safety of
the
patient but for your safety as well, in the event of a complaint
or
litigation.
The entries on the BHT mustbe clear, legible and in complete
sentences.The comments on surgical decisions and other
invasive
procedures should indicate:
Justification on what grounds the decision is made
What the decision is
Any instructions others need to follow
Wishes of the patients regarding this decision
Coordinating with other departmentsThe welfare of the patient
depends on the Team Effort .Thougha patient is under one
Consultant, he may desire opinions and
advice from other specialists. Therefore coordinating
thecommunications between different specialists and departments
is vital and is the responsibility of the house officer.This
should be attempted promptly politely and personally by
yourself.
34
Other Important Issues
The prescriptions should be written clearly with the Genericname
of the drug in capitals and the dose and the frequencyof
administering clearly indicated. One patient in USA died
because the cytotoxic drugs were administered four times a
day when the instructions meant that the dose to be givenover a
four day period. Lack of clarity in the entry causedthe death.
Names of the drugs may look and sound similar. E.g.Ergometrine
used in the past for PPH. and Ergotamine for
Migraine, Zantac (ranitidine) for heartburn, Zyrtec
(cetirizine) for allergies, Celebrex (celecoxib) for
arthritisand Celexa (citalopram) for depression.
Do not assume that that other person would do somethingbut
clearly indicate and specifically on the BHT requesting
him to do it. If informing another care provider is urgent, do
it then and
there. You may forget it later.
Keep a check list or a record of things you have to do andtick
them off as you complete.
Labeling Errors
Always check the name of the drug on the vial/bottle
beforeadministering the drug. Do not assume that it is the drug
because it is in the same cupboard or the same container.
Check the details on the label of the blood packs beforestarting
the Transfusions of blood and blood products. Do
not assume that it was checked by some one else. One who
starts the transfusion is responsible.
Check the name and the identification on laboratory report,the
X-ray or other reports before acting on them.
Address the patient by his name as given in the BHT.Whenever you
communicate with him.
-
8/12/2019 Word of Guidance Med Interns
18/30
35
Avoiding Medical Errors in Surgery
Source Ref 4
A mistake made in performing surgery on the wrong side of theleg
could be disastrous not only to the patient but to the surgeon
as well. Though this kind of errors is rare, it continues
tohappen in different parts of the world. A hospital in USA
reported that three patients had surgery done on the wrong
side
of the head within one year.(5)
The points at which errors may happen in surgical procedures
is given in the chart which analyzed errors in USA
Higher Risk of Medical Errors
Patients undergoing multiple surgery Multiple surgeons taking
part
Rushed to finish the surgery
Basic principles in preventing wrong site, wrong
procedure, wrong person surgeryo Avoid relying on memory alone.o
Use a Check List to keep track of essential items that
needs to be done before surgery.
36
o Talk to the patient by name and check with him/her inthe
verification process.
o Discuss with other members of the surgical team.o Adhere to
the protocol of.
the Unit or the instructions of your Consultant.o If there is a
deviation from this, inform the Consultant
immediately.
o Mark the site of the Surgery accordingly.
The following steps are recommended to be taken at every
surgery.
Verification (To be done in the ward)
Purpose: To ensure all required documents and requisites
are complete.o Confirm identity of the patient with the
surgical
procedure
o Pre operative Investigationso Other Requirement s Blood X
match Prosthesis etco Informed Consent mentioning the site and side
of the
surgery
Marking the site of the Surgery (To be done in the ward)
Purpose: To specifically identify the site of surgery in
order
to clearly indicate the site of Surgery
o For procedures involving:o Rt/Lt distinction, the side
Right/Left must be clearly
marked
o Multiple structures such as fingers should be identifiedo
Intended site must be marked so that it would be visible
after covering the patient with towels. E.g. Label on
theforehead
-
8/12/2019 Word of Guidance Med Interns
19/30
37
Final Verification Immediately before starting the operationin
operating theater Time Out
Purpose: To conduct a final verification before starting the
surgery
Check the name of the patient from him/her and confirm
thesurgery/site/side preferably with the participation of
another
member of the team.
Procedure must be started after this had been done. If there
is
any doubt the consultant should be informed immediatelybefore
starting the surgery.
Getting Consent for a surgical or other procedures
Informed Consent includes the following three parts and isthe
responsibility of a medical officer who is, often the
intern house officer. The first part is the explanation to the
patient,
in a language that the patient can understand, of the nature of
a proposed procedure or
treatment,
its potential risks and benefits,
reasonable alternatives which may be available.
The second part is ensuring that
patient understands what has been explained (tothe best of the
patient's intellectual capacity);
the patient accepting the risks;The patient giving his or her
consent to undergo the
procedure or treatment
Finally, the process must be documented clearly in alanguage
that could be understood by the patient
38
References:1 Encyclopedia of Surgery: A Guide for Patients
and
Caregivershttp://www.surgeryencyclopedia.com/La-Pa/Medical-
Errors.html
2 http://www.ahrq.gov/qual/errback.htmMedical Errors Scope of
the Problem
Agency for Health care Research and quality
3 Risk management in obstetrics; Current Obstetrics
&Gynaecology (2005) 15, 237243
4 Sandra Strickland Preventing Medical Error WrongSurgery
Preventive Action Vol 17 No 12004
http://www.firstprofessionals.com/newsletter-pdf/Phys-
winter-04.pdf
5 http://www.msnbc.msn.com/id/21981965/
-
8/12/2019 Word of Guidance Med Interns
20/30
39 40
Blood Bank...,
Director, National Blood Transfusion Service
All Intern House Officers must report to the Blood Bank of
their institution as early as possible for an orientation
programme.
Instructions on basic Blood Bank procedures are given belowfor
easy reference.
ABO & Rh-D Grouping of Patients & Antenatal Mothers
Materials Required
Specimens: Clotted blood sample or EDTA blood sample.
Reagents: Anti A, Anti B, Anti AB, Anti A1Anti D - monoclonal
IgM Anti D
Reagent red cells A1 cells, B cells, O cells
N. Saline/PBS (Phosphate Buffered Saline)
Test tubes, Pipettes,
Metal tube stand
Table top centrifuge
Report forms
Registers for recording results
Procedure
1. Check the sample and request form to ensure that thepatient
identification is correct.
2. Label the sample and request form.3. Centrifuge the sample at
1000- 3000 rpm for 3 min to
separate serum.
-
8/12/2019 Word of Guidance Med Interns
21/30
41
4. Prepare a 5% cell suspension (can be prepared byadding 19
drops of saline to 1 drop of patients red cells
5. Arrange 8 test tubes on a test tube rack and label
withpatient & test identification as following.
E.g.: Pt 1 1 1 1 1 1 1
5% cell Anti Anti Anti A1c Bc Oc
Suspension
A B AB D
Add one drop of anti A, anti B, anti AB & anti D to
first
four tubes. Add one drop of 2- 5% cell suspension of red cells
to be
tested.
Add two drop of patient serum/plasma to test tubes labeledas
A1c, Bc, Oc.
Add one drop of A1reagent red cells to tube labeled as. A1cAdd
one drop of B reagent red cells to tube labeled as Bc.Add one drop
of O reagent red cells to tube labeled as Oc.
Mix the contents of the tubes and centrifuge at 1000rpm
20seconds or keep at room temperature for 5 min.
First take the cell grouping tubes and gently resuspend thecell
buttons and examine for agglutination Grade and record
the results on worksheet
Take the serum grouping tubes and first examine the
serumoverlying the cell button for evidence of haemolysis.
Gently resuspend the cell button and examine
foragglutination.
Grade and record the results on work sheet.
42
Compare and confirm the cell grouping results with theserum
grouping results.
Gently resuspend the cell button of the Rh D typing tubeand look
for agglutination.
If no agglutination seen, repeat the test with 2 drops of
sameAnti D.
Test for detecting weak D is unnecessary for patients whenusing
monoclonal IgM antiserum.
Interpretation
Agglutination of any cell grouping tube and haemolysis
oragglutination on serum tests constitutes a positive result.
The expected agglutination reaction for positive tests is 3+or
4+ in cell tubes.
Agglutination in serum tubes is often weaker. The reactioncan be
enhanced if incubated at room temperature for 15
min.
A smooth suspension of red cells after resuspension of thecell
button is a negative result.
In serum grouping tubes, if the supernatant (beforeresuspension)
is pink/red and if the size of the cell button is
smaller or no cell button is seen it indicates lysis and is
a
positive result.
ABO Grouping
Anti
A
Anti
B
Anti
ABA1c Bc Oc Interpretation
0 0 0 C/L C/L 0 Group O
3/4+ 0 3/4+ 0 C/L 0 Group A
0 3/4+ 3/4+ C/L 0 0 Group B
3/4+ 3/4+ 3/4+ 0 0 0 Group AB
C = clumps L = lysis
-
8/12/2019 Word of Guidance Med Interns
22/30
43
Rh D Type
Anti D (not detecting Dvi variant) Interpretation
+ Positive
0 Negative
After interpretation, the blood group must be compared
withprevious records, if available.
If any discrepancy between present group and previousgroup is
encountered, request for a second sample andconfirm.
If any discrepancy between serum and cell grouping
isencountered, repeat the test using washed cells.
If the discrepancy persists, consider the previous history
ofTransfusions
If there is no discrepancy, record the blood group of
thepatient.
Documentation
Enter the results of the patients grouping in the PreTransfusion
Testing Register.
Complete and counter sign a Blood Report.
Pre Transfusion compatibility testing
Material RequiredEquipment. Refrigerator to store samples and
reagent at +2C to
+6C
. Table top centrifuge
44
. Microscope
. 37C water bathSpecimen. Clotted blood sample of patient. 5%
suspension of red cells prepared forms a selected
donor unit.
Reagents
. 0.9% saline
. 22% Bovine Albumin
. Anti human globulin (AHG)
. LISS Additive. PBS
Glassware. Glass test tubes. Glass slide. Pipettes
Miscellaneous
. Disposal box
. 2 plastic beakersTest tube racks
Procedure
1. Give a serial number to the testing sample and the
requestform before commencing the procedure.
2. Group patients sample for ABO and Rh D as per REF/
SOP/02..and accordingly select a group specific blood unit/s
for cross matching.
3. If the presence of an antibody is confirmed, select
relevantantigen negative blood unit/s and/or if patients
phenotype
is known select blood units according to the phenotype.
-
8/12/2019 Word of Guidance Med Interns
23/30
45
4. Label test tubes as D1, D2 .according to the number ofdonor
blood units requested for the patient. Add one drop of
donor cells to each labeled test tubes.
NISS Method
5. Add three/two drops of patients serum to all test tubes.
6. Add one drop of 5% suspension of cells from donors to
therelevant test tubes
7. Mix the contents and incubate all test tubes at 37 oc for
45minutes.
8. Take out and centrifuge at 250g for 20 seconds.9. Look for
haemolysis and then gently disturb the cell button
to note agglutination of cells.
10.Grade and record the results.11.Add PBS to fill 2/3 of all
test tubes.12.Centrifuge at1000g for 1 min.13.Decant the
supernatant PBS.14.Repeat the same washing steps twice.15.After the
last wash, add two drops of poly specific AHG to
all the dry cell buttons in each test tube.16.Gently disturb the
cell button to note any agglutination of
cells. Record results in the work sheet
Saline Albumin Cross match1. Take two test tubes each for each
Donor pack & label them
as Saline (S) & Albumin (A).2. Add three/two drops of
patients serum to all test tubes.
3. Add one drop of 5% suspension of cells from donors to
therelevant test tubes4. Add 1 drop of 22% bovine albumin into the
tube labelled as
albumin mix the content & incubate at 37oc water bath
for
30 - 45 minutes.
5. After incubation period take the tubes from the water bath
¢rifuge at 250g for 20 seconds.
6. Look for haemolysis & or agglutination microscopically.7.
Grade & record results on the request form.
46
8. If there is no agglutination or haemolysis in both
tubes-proceed to AHG test on Albumin tube.
4.1.Shake the Albumin tube gently to disturb the cells atthe
bottom.
4.2.Fill he tube with normal saline.
4.3.Centrifuge at 1000g for 1 minutes4.4.Decant the supernatant
completely to get a dry cell
button.
4.5.Repeat above steps two more times4.6.After the last wash,
disturb the cell button 7 add poly-
specific AHG reagent4.7.Centrifuge the tube at 250g for
15sec.4.8.Look for macroscopic/microscopic agglutination4.9.If
there is no agglutination the cross match is
compatible.
(Negative IAT results should be validated with Coombs
control
cells, if available.)
LISS Method
1. Take a test tube each for each donor pack.2. Add two drops of
patients serum to all tubes.3. Add one drop of 5% suspension of
cells from donors to the
relevant test tubes.
4. Add 2 drops of LISS Additive into the tube mix the
contentwell & incubate at 37oc water bath for 15 - 20
minutes.
5. After incubation period take the tubes from the water bath
¢rifuge at 250g for 20 seconds.6. Look for haemolysis &
or agglutination microscopically.7. Grade & record results on
the request form.8. If there is no agglutination do the indirect
AHG test
mentioned in saline Albumin method & interpret the
results.9. For all the washing steps use fresh normal saline or
PBS
solution.
10.If there is no agglutination the cross match is
compatible.
-
8/12/2019 Word of Guidance Med Interns
24/30
47
Interpretation
6.1. If cross match is compatible
6.1.1. Write a Compatibility report6.1.2. Attach a reservation
tag to the blood pack & keep
the blood pack in the correct refrigerator
6.1.3. Preserve the tested sample for 7 days in the
refrigerator.
6.2. If the cross match is incompatible
6.2.1. Recheck the patients blood group & donor unit
6.2.2. Do cross match with another unit of blood
6.2.3. If still incompatible contact MO on duty
atImmunohaematology Reference Lab, NBTC.
Documentation
Enter the results in the pre-transfusion compatibility
testing
work sheet and register.
If the cross match is compatible,
. Write a compatibility report and sign.
. Attach a compatibility label to the blood unit.
48
Pre Transfusion Compatibility Testing for Infants
Procedure
01.Wash the babies blood sample 3 times with fresh 0.9%
saline or PBS02. Prepare a 5% suspension of red cells after the
final wash
02.Using the suspension, carry out the ABO and Rh groupingas
above.
03.Carry out the ABO and Rh grouping of the mother as
above.04.Select blood for crossmatch as follows,
. Select blood compatible with the ABO and Rh groupingof the
baby and the mother (refer table annexed).
. Otherwise use group O Rh compatible units
. Select blood within 5 days of collection
. Avoid using blood donated by blood relatives
05.Perform the cross match using mothers Serum and donorcells as
per SOP/REF/09
Infant
Group
A
Group B Group
AB
Group
O
GroupA
Bloodunit A,O
Bloodunit ,O
Bloodunit A,O
Bloodunit, O
Group
B
Blood
unit O
Blood
unitB,O
Blood
unit B,O
Blood
unit O
Group
AB
Blood
unit A,O
Blood
unit B,O
Blood
unitAB,O
Blood
unit O
Mother
Group
O
Bloodunit O
Bloodunit O
Bloodunit O
Bloodunit O
-
8/12/2019 Word of Guidance Med Interns
25/30
49
Documentation
Enter the results in the Pre-transfusion Compatibilitywork
sheet.
Write a compatibility report and a reservation tag.
50
Communication skills for Doctors
Dr. Deepthi Samarage,
Head of Dept. of Medical Education / Faculty of Medical
Sciences,
University of Sri Jayawardanapura
Introduction
Good doctors communicate effectively with patients. They
identify patients' problems more accurately, and patients
are
more
satisfied with the care they receive. Doctors do
not
communicate with their patients as well as they should.
When doctors use communication skills effectively, both theyand
their patients benefit.
Doctors identify their patients'problems more accurately.
Patients are more satisfied with their care and can better
understandtheir problems,
investigations, and treatment options.
Patients are more likely to adhere to treatment and to follow
advice onbehaviour
change.
Patients' distress and their vulnerability to anxiety and
depression arelessened.
Doctors' own
wellbeing is improved. Doctors with good communicationskills
have greater job satisfaction and less work stress
Key tasks in communication with patients
Eliciting the patient's main problems, the patient's perceptions
of
these and the physical, emotional, and social impact of the
patient's
problems on the patient and family
-
8/12/2019 Word of Guidance Med Interns
26/30
51
Tailoring information to what the patient wants to know;
checking his
or her understanding
Eliciting the patient's reactions to the information given and
his or
her main concerns
Determining how much the patient wants to participate in
decision
making
(when treatment options are available)
Discussing treatment options so that the patient understands
the
implications
Unfortunately, doctors often fail in these tasks. Evidence
shows
that only half of the complaints and concerns of patients
are
likely to be elicited. Often doctors obtain little
information
about patients' perceptions of their problems or about the
physical, emotional, and social impact of the problems. When
doctors provide information they do so in an inflexible way
and
tend to ignore what individual patients wish to know. They
pay
little attention to checking how well patients have
understood
what they have been told. Less than half of psychological
morbidity in patients is recognized. Often patients do not
adhere
to the treatment and advice that the doctor offers, and levels
of
patient satisfaction are variable.
Blocking behavior of doctors
offering advice and reassurance before the main problems
have been identified
explaining away distress as normal
52
attending to physical aspects only
switching the topic
"jollying" patients along
Reasons for patients not disclosing problems
belief that nothing can be done
reluctance to burden the doctor
desire not to seem pathetic or ungrateful
concern that it is not legitimate to mention them
doctors' blocking behaviour
worry that their fears of what is wrong with them will be
confirmed
Each of us has our own unique way of relating with others andit
is important to become aware of the impact that our style
has on our relationships. As a doctor you have a
particularresponsibility to develop an interpersonal style that
will
enhance the effectiveness of your relationships and
facilitateeffective communication with your clients/ colleagues.
We
believe that a meaningful relationship and
effectivecommunication is a fundamental component contributing to
the
well-being of the client/ colleague.
Attending: Physical and Psychologicalpresence
Attending is the process by which the doctor pays
closeattention, both verbally and nonverbally, in such a way that
the
client/colleague feels listened to, care about, and
accepted.
Often doctors have developed ways of relating nonverbally
-
8/12/2019 Word of Guidance Med Interns
27/30
53
which discourage clients/ colleagues from becoming engaged
ininteractions with them. Certain facial expressions such as
frowns or curled lips, or other body behaviors such as yawningor
squirming then to inhibit the interaction. By developing
awareness and practicing those behaviors which are perceived
by most people as signs of attention and interest, the
doctordemonstrates physical presence and a willingness to
become
involved in the interaction.
Physical attending includes facing the client/colleague
making
eye contact, leaning forward toward the client/colleague and
having an open and relaxed posture.When the doctor pays close
attention to the client/colleague
he/she demonstrates respect, interest, involvement and
caring,
good attending is also a powerful reinforces as it encourages
the
client/ colleague to become more involved in the
communication process.
Empathy
Empathy is the most critical element in a helping situation
and
is the backbone of the responding skills. Empathy is the
ability
to understand the ideas and feelings of another person.
By using empathy, the doctor can enable the
clients/colleagues
to see themselves and their situation more clearly. Empathythen
enables the client/colleague to feel understood. As a doctor
who is skillful with empathy, you are able to stand in shoes
of
another. You can see and hear how clients/colleagues feel
andthink, and are able to show the client/colleague that you
understand their feelings and situation.
ListeningListening is the key to understanding the meaning of
anothers
experience. Why is it then, that messages are not
heardaccurately and miscommunication abounds?
Factors that interfere with listening.
54
Listed below are some common factors that could interfere
withyour listening ability.
Preoccupation
Often we are distracted from listening by thinking about
other things. We allow our minds to focus on ourconcerns rather
than the person we are listening to.
Speaking vs. listening
At times we are more intent on speaking that listening.
We are so anxious to tell things the way we see themthat we dont
truly hear what the other person is saying.
Judging vs. listening
There are many daily situations which encourage us to
judge what people are saying. To be helpful in asituation
demands an ability to be accepting. Thats
difficult to do if you are used to being critical.
In every conversation there are two components to listen
for:
Content: what the client/colleague is talking about
Feelings: how the client/colleague feels about the
situation.
Respect
Respect, in essence, refers to a belief in the value and
potential
of the other person. Respect is communicated more by
attitude
than by specific response. The respect the doctor shows for
the
client/colleague will enable him to share his concerns more
openly and easily.
Warmth
Warmth is a physical expression of empathy and respect. It
is
generally communicated nonverbally in such ways as: eyecontact,
facial expression, touching, tone of voice, posture and
-
8/12/2019 Word of Guidance Med Interns
28/30
55
gesture. Ordinarily, nonverbal behaviors, such as eye
contact,facial expressions, tone of voice, etc., are not
consciously
exhibited. However, under conditions of attention and
practice,you can increase your awareness of your own nonverbal
expressions and modify your nonverbal behaviors in the
direction of increased warmth.
Clarification
In interactions with a doctor, the client or colleague
presents
many concerns, ideas and feelings. This is often done in an
implied way, perhaps through humour or deliberate
vagueness.Clarification is a method of making the other persons
message
explicit.
Clarification is also a method of confirming the accuracy of
your perceptions about the other persons message. As
doctors,
we often make the assumption that understanding is
occurringwithout validating our perceptions. This can lead us to
making
assessments based on inaccurate information. Clarification
can
serve to correct misperceptions before they
becomemisunderstandings.
Summarizing
In interactions with clients, the doctor may find that many
ideasand feelings are presented. Summarizing involves a process
of
tying together relevant core materials that have been
presentedin a fragmented way. The main purpose of summarizing is
to
systematically highlight the critical aspects of the
clientsstatements and behavior.
We have attempted to provide you with some concepts that we
think are necessary for effective communication. How you use
these tools will depend on your personal beliefs and values
as
you respond in a helping relationship.We cannot make you
communicate more effectively, the desire
has to come from within. Its now up to you!
56
Guidance in issuing medical certificates
For detailed information on issuing medical certificates,
please
refer the following circulars.
General Circular No. 1006 issued by director of health
services
on 20thJune 1979
General Circular No. 1086 issued by director of health
services
on 7th
May 1980
General Circular No. 1481 issued by Director General of
health
services on 21stOctober 1986
General Circular No. 1481 A issued by Director General ofhealth
services on 12
thNovember 1986 (Maternity leaves)
Public administration circular 4 / 2005 ministry of
publicadministration and home affaires 3
rdFebruary 2005
Given below are few salient points regarding issue of
medical
certificates
Those authorised to issue medical certificates in
Teaching,Provincial General, District General and Base Hospital
are;
(I) Wards: Physicians, Surgeons, Paediatricians,Obstetricians,
all the other specialists and House
Officers under the direction of their respective
consultants.
(II) Clinics: Specialist Officers(III) O.P.D: Physician and
Surgeon between the hours
fixed by M.O.I/C, O.P.D. for those who attend the
O.P.D genuinely and primarily for treatment.
Medical Officers O.P.D. only in case of medical
and surgical emergencies, at all hours.
-
8/12/2019 Word of Guidance Med Interns
29/30
57
1) Confirming the Identity of the patient to whomcertificate is
issued;
2) Medical Certificates on Form Medical 170 and 331 areissued
free;
3) The Medical Officer should be satisfied, before issuingthe
Medical Certificate that the incapacitation resulting
from illness or injury is such that the officer/ employee
is unable to perform his/her normal duties;
4) The leave granted should be in keeping with
theincapacitation;
5) Medical officers shall not recommend leave in excess ofa
month at a time and extension of a leave shall not berecommended
for more than a month in the first
instances and more than two weeks in the second and
third instances. Medical leave beyond the period of 3months
would necessitate the individual being sent
before a Medical Board;
6) Medical Certificates issued by private MedicalPractitioners
as well as those issued by Ayurvedic
Medical Practitioners should not be endorsed byGovernment
Medical Officers;
7) The Medical Certificate should not cover more than fivedays
past absence under any circumstances, except in
the case of an in-door patient to cover a period of stay in
hospital;
8) When officers / employees are on transfer orders utmostcare
should be exercise before a decision is made to
recommend sick leave;
58
9) All cases in the Medical Certificate must be completed
in full;
(IV)(V)10)A Medical Certificate whether on Form 170 or Form
331 shall be promptly dispatched direct to theimmediate Superior
of the applicant and, under no
circumstances shall a M.C. be handed over to an
applicant;
11)Medical Officers of Health may issue Medical Certi-ficate
only to the following;
(a)Maternity cases,
(b)Staff working under the M.O.H., and
(c)All cases of communicable disease.
Recommending Maternity leave
Salient points from public administrative circular 4 / 2005
Government has decided to grant female public officers84 days
maternity leaves with full pay, 84 days
maternity leave on half pay and 84 days maternity on nopay in
respect of every child birth;
All female public officers whether permanent,temporally, casual
or trainee are entitle to maternity
leave under this section.
Maternity leave with full payo Female officer is entitle to 84
working days full
pay leaves in respect of every live child birth and
they will not be allow to resume duties beforethe expiry of 4
week after the birth of the child.
-
8/12/2019 Word of Guidance Med Interns
30/30
59
o In calculating maternity leave Public holydaysSaturdays and
Sundays falling with in such
period should not be included.o In the case of a still birth or
the death of a child
before the expiry of 6 weeks from the child birth,
6 weeks leave from the date of child birth shouldbe granted as
special full pay leave.
Maternity leave on half payo After the exhaustion of leave
mentioned in the
previous para the officer is entitled to 84 days
leave on half pay for her to look after the child.
Maternity leave on no payo After the end of leave approved under
the
previous 2 paras, it is possible to grant 84 days
no pay leave only if such leave is required for the
purpose of looking after the child. However, the
approval of the leave would be by the Head of
the relevant Department.
In the case of a miscarriage the officer can avail herselfof the
vacation leave she is entitled to on the production
of the medical certificate.
After the expiration of the maternity leave obtained asdescribed
earlier the officer should be allowed to leave
office one hour before the normal time of departure in
order to breast feed the child provided no maternity
leave on half pay has been availed of.
Further, when the officer researches the fifth month ofpregnancy
she should be allowed to attend office half an
hour later than the normal time of attendance and leaveoffice
half an hour before the normal time of departure.
60


![[PPT]A Manual for Interns and Volunteers - University … · Web viewTypes of Interns & Volunteers Interns Volunteers Interns doing an internship – but not interested in archives](https://img.pdfslide.us/doc/110x75/5ad11a0c7f8b9aff738b54d0/ppta-manual-for-interns-and-volunteers-university-viewtypes-of-interns-volunteers.jpg)