Embed Size (px)
Citation preview

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 1
EXTENDED VERSION
Brief CBT-I for insomnia comorbid with social phobia: A case study
Nicole K. Y. TangDepartment of Psychology, Institute of Psychiatry, King’s College London
Correspondence:Nicole K. Y. Tang
Department of Psychology (PO 77)Institute of Psychiatry, King’s College London
de Crespigny Park, Denmark HillLondon SE5 8AF
Phone: 0207 848 5010Fax: 0207 848 5037
Email: [email protected]

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 2
Abstract
Background: Despite an obvious link between social anxiety and acute state of insomnia, chronic types
of sleep disturbances in people with social phobia have so far received limited research/clinical
attention. This case report aims to illustrate the possibility of rectifying sleep disturbances comorbid
with social phobia, using a brief cognitive behaviour therapy for insomnia (CBT-I).
Method: Treatment involved 5 sessions of CBT-I provided individually on a weekly basis. Major
treatment components included psychoeducation, sleep restriction therapy, stimulus control and
cognitive restructuring.
Results: Treatment effects were assessed using sleep diary and questionnaires over the course of the
treatment and at ~9-month follow-up. The results were encouraging with all targeted sleep parameters
demonstrating improvements that met dual criteria for clinical significance. The gains were well
maintained even at ~9 months after treatment. These improvements in sleep were accompanied by a
reduction in sleep-related anxiety and dysfunctional beliefs and attitudes about sleep. Whilst the
patient also reported a corresponding improvement in daytime functioning and general anxiety, no
gains were observed in depression and social anxiety.
Conclusions: These findings highlight the potential benefits of incorporating brief CBT-I into existing
treatments for social phobia and encourage further research on the intricate relationship between sleep,
mood and social anxiety.
Keywords: Insomnia, Social Phobia, Social Anxiety, Cognitive Behaviour Therapy, Treatment
Outcome, Case Report

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 3
Introduction
Social phobia is characterised by a disabling fear of social situations that may bring upon
embarrassment or humiliation. Exposure to feared social situations is typically either avoided or
endured by the person with great anxiety. In sleep research, social anxiety (through the use of a speech
threat) has been used as a tool to create an acute state of insomnia for investigating the impact of pre-
sleep arousal on subsequent sleep and sleep perception (e.g., Tang & Harvey, 2004b). Interestingly,
despite this established link between social anxiety and acute insomnia, the association between social
phobia and more chronic forms of insomnia has only received minimal research/clinical attention.
There is some initial evidence showing that the diagnosis of social phobia is linked to the
presence of extended insomnia (Degonda & Angst, 1993). Although not everyone with social anxiety
has trouble sleeping, persistent complaints of insomnia are frequently noted amongst social phobics
presenting for treatment in anxiety disorders clinic. Compared to sex-matched and age-comparable
healthy control subjects, patients diagnosed with generalised social phobia report poorer sleep quality,
longer sleep latency, more frequent sleep disturbance and more severe daytime dysfunction than the
healthy controls (Stein, Kroft, & Walker, 1993). There appears to be a positive correlation between the
level of social anxiety and insomnia severity, although such relationship is partially mediated by
depressive symptoms (Buckner, Bernert, Cromer, Joiner, & Schmidt, 2008). It is unclear how exactly
the conditions interact and if they aggravate each other, but previous large-scale epidemiological
studies have shown that insomnia appears mostly at the same time or after the occurrence of an anxiety
disorder (Ohayon & Roth, 2003) and that untreated insomnia increases the risk of developing anxiety
disorders by 2-5 times within an 11-year interval (Necklemann, Mykletun, & Dahl, 2007).
Historically, sleep disturbances co-occurring with another psychological disorder are
conceptualised as “secondary insomnia”, with the psychological condition regarded as the primary
problem and insomnia as a symptom that will resolve when the primary problem is treated. An
unfortunate legacy of this conceptualisation is that the insomnia and its associated problems are mostly
overlooked in treatment. Recently, there has been a growing body of research showing that standard

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 4
cognitive behaviour therapy for primary insomnia (CBT-I) can be fruitfully applied to treat insomnia
co-occurring with depression, posttraumatic stress disorder, cancer, chronic pain, HIV and alcoholism
(Smith, Huang, & Manber, 2005). Yet, the utility of CBT-I in social phobia has remained largely
unexplored. The aim of this clinical report, therefore, is to illustrate the possibility of tackling insomnia
comorbid with a moderately complex case of social phobia using an abbreviated version of CBT-I.
Case Presentation
This case concerned a 32-year old artist, who was referred for assessment and treatment of
social phobia. Lee (a pseudonym) reported feeling extremely nervous every time he encountered social
situations. He constantly worried about making mistakes and used alcohol to help him socialise. Lee’s
social anxiety made it difficult for him to leave his house. He felt that his career was severely
hampered by his social anxiety, as being a selling artist these days involved travelling, networking and
business negotiation.
Lee reported having trouble getting to sleep on most nights. He also reported problems waking
up too early and not being able to get back to sleep. In terms of his mood, Lee had an ongoing problem
of depression. He was previously prescribed antidepressants by his GP and seen by a counsellor for his
low mood, but he found neither of these treatments helpful. Lee felt that his mood would improve if he
was treated for his social anxiety. He also felt that he would not be able to benefit from the social
phobia treatment until his disrupted sleep pattern settled. Lee was therefore offered a sleep assessment,
followed by a brief course of CBT-I, whilst he was waiting for the social phobia treatment.
Assessment of Insomnia
Lee’s sleep disturbances were assessed using the Duke Structured Interview Schedule for the
Diagnoses of DSM-IV-TR and International Classification of Sleep Disorder, Second Edition (ICSD-
2) (Edinger, Kirby, Lineberger, Loiselle, Wohlgemuth, & Means, unpublished). In addition, Lee was
asked to keep a sleep diary for 1 week and to complete a pack of questionnaires that assessed his sleep
quality, insomnia-related thoughts and responses, daytime functioning and general psychological
characteristics. Specifically, the pack included the following:

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 5
Insomnia Severity Index (ISI; Bastien, Vallieres, & Morin, 2001)
The ISI is a 7-item self-report measure used to evaluate insomnia severity in the past month.
Each item is rated on a 5-point scale (0 = “Not at all, 4 = “Extremely”), generating a total score that
ranges from 0 to 28 (with higher scores indicative of more severe insomnia). The ISI has been
validated against both objective (e.g., polysomnography) and subjective (e.g., clinical interview and
sleep diary data) measures of insomnia, demonstrating good levels of internal consistency and
concurrent validity. It has also been shown to be sensitive to improvements in sleep associated with
both drug and non-drug treatments. Following the score interpretation guidelines provided by the
authors, a total score of 0 to 7 indicates “No clinically significant insomnia”, 8 to 14 “Subthreshold
insomnia”, 15 to 21 “Clinical insomnia (moderate severity)” and 22 to 28 “Clinical insomnia (severe)”.
The cut-off of 14 has been found to have optimal sensitivity (94%) and specificity (94%).
Anxiety and Preoccupation about Sleep Questionnaire (APSQ; Tang & Harvey, 2004a)
The APSQ is a 10-item measure used to assess the level of sleep-related anxiety and
preoccupation associated with insomnia in the past week. Each item is rated on a 10-point scale (1 =
“Not true” to 10 = “Very true”), generating a total score that ranges from 10 to 100 (with higher scores
indicative of higher levels of sleep-related anxiety and preoccupation). The APSQ has high internal
consistency and good concurrent validity. Higher scorers on the APSQ are also higher scorers on
established insomnia and anxiety measures, such as the The Pittsburgh Sleep Quality Index (PSQI;
Buysse, Reynolds, Monk, Berman, & Kupfer, 1989) and the Beck Anxiety Inventory (BAI; Beck,
Epstein, Brown, & Steer, 1988).
Dysfunctional Beliefs and Attitudes about Sleep Questionnaire (DBAS-16; Morin, Vallieres, &
Ivers, 2007)
The DBAS-16 is an abbreviated version of the 30-item DBAS. It contains 16 items and is a
self-report questionnaire used to identify and assess various sleep/insomnia-related cognitions. Five
conceptually derived domains of sleep-related beliefs are assessed, namely (i) misconceptions about
the causes of insomnia, (ii) misattribution or amplification of its consequences, (iii) unrealistic sleep

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 6
expectations, (iv) diminished perception of control and predictability of sleep, and (v) faulty beliefs
about sleep-promoting practices. Each item is scored on a 0 (Strongly disagree) to 10 (Strongly agree)
Likert scale. Although there is no absolute right or wrong answer for any single item, their
dysfunctional nature is reflected by the degree to which each item is endorsed. The total score is based
on the average score of all items completed. Comparable to the psychometrics of the long version, the
DBAS-16 has good adequate internal consistency, temporal stability and concurrent validity.
Insomnia Interference Scale (IIS)
In the absence of a suitable alternative, the author developed the IIS to measure insomnia-
related interference based on her experience working with patients with insomnia. The IIS consists of
16 common problems in daytime functioning often encountered by people with insomnia and typically
attributed to their lack of sleep. Example problems listed in the IIS are: “Concentrating on what people
say”, “Focusing on the task at hand”, “Picking up on other people’s feelings”, “Thinking clearly”. The
respondents are asked to rate the extent to which their sleep trouble has caused them difficulties in
each of these areas in the past week, on a 0 (no difficulty) to 10 (major difficulty) scale. The total score
is based on the average score of all items completed, with a higher score indicating greater interference
caused by the insomnia.
Hospital Anxiety and Depression Scale (HAD; Zigmond & Snaith, 1983)
The HAD is a 14-item self-report questionnaire used to measure the overall severity of anxiety
and depression (7 items each) in the past week. Each item is rated on a 4-point scale (0 to 3),
generating a total anxiety/depression score that ranges from 0 to 21. The HAD has good internal
consistency and concurrent validity. Scores of 8 or above identify probable anxiety/depression cases
with around 80% sensitivity and specificity.
Assessment Outcome and Case Formulation
Lee revealed that, although he had always been a ‘light sleeper’, his recent trouble sleeping was
aggravated by his social anxiety and low mood. He regarded his insomnia as equally interfering as
other problems, because he often found himself unable to concentrate or function as well as he hoped.

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 7
His average IIS score was 7 (out of a possible 10) suggesting that his insomnia was severely affecting
his daytime functioning.
Lee reported problems sleeping five nights a week, and he was most bothered by his inability
to go to sleep (taking on average 2 hours to fall asleep) and the lengthy awakenings (of approximately
an hour duration in total). His sleep was generally short (~4 hours), and often of poor quality (not
feeling refreshed upon waking). Lee scored 25 on the ISI, indicating severe clinical insomnia. He met
the DSM-IV-TR criteria for insomnia related to another mental disorder and the ICSD-2 criteria for
‘psychophysiologic insomnia’ and ‘inadequate sleep hygiene’. Lee’s scores on the HAD anxiety and
depression subscales were 18 and 13, respectively, both of which were above the clinical cut-offs (>8).
Whilst his trouble sleeping was exacerbated by his social anxiety and depression, the insomnia was not
exclusively associated with his mood change and his sleep problems were judged to be sufficiently
severe to warrant independent clinical attention.
Lee’s scores on the APSQ (53) and the DBAS (4.81) were high, comparable to those obtained
by primary insomnia patients in previous research. It was conceivable that Lee’s insomnia was partly
maintained by his sleep-related worries. He strongly endorsed questionnaire items such as “I worry
that I won't cope tomorrow if I don't sleep well", “I get overwhelmed by my thoughts at night and
often feel I have no control over this racing mind". These thoughts were likely to create additional
arousal and made it even harder for him to fall asleep. Such cognitive reactions (excessive worries),
together with his behavioural (extending time in bed, painting in the bedroom when unable to sleep)
and emotional (frustration, anxiety, irritation) responses to his not sleeping, were considered to be the
factors perpetuating his insomnia.
Insomnia Treatment
A total of five one-hour sessions were offered to Lee, individually on a weekly basis, plus a
booster session one week after the treatment ended. The treatment comprised several behavioural and
cognitive interventions recommended by the American Academy of Sleep Medicine and featured in
existing treatment protocols known to be effective (Morin & Espie, 2003; Edinger & Carney, 2008).

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 8
These included sleep psychoeducation, sleep restriction, stimulus control and cognitive restructuring,
which are briefly described below.
Psychoeducation
This involves educating the patient about the basics of normal human sleep and individual
differences in sleep needs. This serves to improve their understanding of the environmental and
behavioural factors modifying sleep, enabling them to develop an appreciation of the scientific
rationale of CBT-I.
Sleep Restriction
This strategy works via sleep homeostasis. It aims to consolidate sleep by regulating the sleep-
wake schedule and cutting excessive time in bed. The therapy usually begins with restricting the
number of hours in bed (i.e., sleep window) to the patient’s current sleep requirement, such that a mild
form of sleep deprivation is introduced to increase the sleep pressure, hasten sleep onset, reduce mid-
night awakenings and improve sleep efficiency (SE), which is calculated by the formula: (total sleep
time/time in bed) x 100%. SE of <85% is typically the clinical cut-off for interrupted sleep. The
patient’s sleep window will then be adjusted every week. The length will be extended by an interval of
15 minutes if the patient achieves a sleep efficiency of 85% or higher. The bonus 15 minutes will be
added to the beginning of the sleep window (i.e., allowing for an earlier bedtime), whilst keeping the
getting up time unchanged. This procedure is to be repeated until the ideal length of sleep is achieved
without compromising the sleep efficiency.
Stimulus Control
The rationale behind this intervention is based on the notion that both the timing and sleep
setting are associated with repeated unsuccessful sleep attempts and, over time, the bed and the
bedroom become conditioned cues for arousal that perpetuates insomnia. As such, the goal of this
treatment is to re-establish an association of the bed and bedroom with successful sleep attempts. Five
principles key to successful stimulus control are: (i) refrain from daytime napping, (ii) establish a

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 9
standard wake-up time, (iii) go to bed only when sleepy, (iv) get out of bed whenever awake for long
periods, and (v) use the bed for sleep and sex only.
Cognitive Restructuring
Cognitive restructuring is a method used to alter unhelpful beliefs and attitudes about sleep and
to reduce the patient’s distress associated with sleep, through the flexible use of a range of discussion
techniques (e.g., reappraisal of threat, attention shifting, hypothesis testing). The cognitive component
of the current treatment took the Harvey approach, which emphasises (1) giving equal emphasis to
night-time and daytime symptoms and processes and (2) the use of behavioural experiments rather
than verbal education to challenge and alter potentially unhelpful sleep beliefs, to establish new
beliefs, and to devise ways to reverse processes maintaining the insomnia (Harvey, Sharpley, Ree,
Stinson, & Clark, 2007). The treatment focused not only on helping Lee establish a stable sleep-wake
schedule but also on addressing his concerns about the impact of insomnia on his mood and daytime
performance. Table 1 outlines the treatment content and procedure.
Given the short and intensive nature of the treatment, homework was assigned weekly to
ensure that learning during the session was consolidated. Throughout the treatment, Lee was asked to
keep a daily sleep diary. The information gathered was used to guide the pace of the sleep restriction
therapy. To evaluate treatment outcomes, Lee was also asked to complete (i) a week of sleep diary
before and after treatment and at ~9-month follow-up, (ii) the ISI, APSQ and IIS in each weekly
session, (iii) a long questionnaire (including the ISI, APSQ, ISS, DBAS-16 and HAD) a week before
and after treatment and at follow-up.
For clinical and logistical reasons, Lee's social phobia treatment commenced soon after the
termination of his insomnia treatment, which had denied a clear-cut follow-up opportunity. The
follow-up questionnaire was sent to Lee after his completion of his social phobia treatment. Cautions
should be applied when interpreting these outcomes as they represented the combined effect of both
treatments. For the reader’s information, the social phobia treatment Lee received was cognitive-
oriented (Clark, 2001). It focussed on reversing the maintaining processes specified in the Clark &

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 10
Wells (1995) social phobia model (e.g., self-focussed attention, negative self-processing, safety-
seeking behaviours) and none of which was specifically linked to sleep.
Results
Sleep Parameters
A consistent trend of improvement was observed in Lee’s sleep diary data and self-report
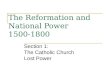
questionnaire. Figure 1 depicts the day-by-day changes in Lee’s sleep pattern, as measured by his
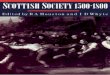
sleep-diary data, over the course of treatment. Figure 2 depicts the week-by-week changes in Lee’s
sleep quality (ISI), sleep-related anxiety (APSQ) and insomnia-related interference (IIS) over the
course of treatment.
Sleep efficiency (SE). The SE increased from a mere 49.7% at baseline to 91.6% at post-
treatment, constituting an 84% improvement in efficiency. This improvement was maintained at
follow-up, with Lee obtaining an average SE of 94.7%. Both the post-treatment and follow-up SEs
exceeded the conventional threshold for efficient sleep, which is typically set at >85%.
Sleep Onset Latency (SOL). The average SOL dropped 77%, from 71.6 minutes at baseline to
16.3 minutes at post-treatment, which then continued to drop another 30% to 11.4 minutes at follow-
up. Both the post-treatment and follow-up SOLs were well within the 30-minute cut-off commonly
used to distinguish normal from delayed sleep onset.
Wake After Sleep Onset (WASO). The number of WASO dropped 48%, from 2.5 at baseline to
1.3 at post-treatment, whilst the duration of WASO dropped 88%, from 132.5 minutes at baseline to
15.6 minutes at post-treatment. At follow-up, both the number and duration of WASO maintained their
improvements; the average number of WASO was 1 whilst the average duration of WASO was 11.4
minutes. Both the post-treatment and follow-up WASO durations were well within the 30-minute cut-
off commonly used to distinguish normal from prolonged mid-night awakenings.
Total Sleep Time (TST). The TST increased 32%, from 4.42 hours at baseline to 5.84 hours at
post-treatment. Such gain was maintained at follow-up, with Lee obtaining an average TST of 5.73
hours at ~9 months after treatment.

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 11
ISI. The ISI score dropped 68%, from 25 (indicating severe clinical insomnia) at baseline to 8
(indicating subthreshold insomnia) at post-treatment. The ISI score then continued to drop another
38% to 3 (indicating no clinically significant insomnia) at follow-up.
Insomnia-related Processes
APSQ. The APSQ score dropped 53%, from 53 at baseline to 25 at post-treatment, which then
continued to drop another 20% to 20 at follow-up.
DBAS-16. The DBAS-16 score dropped 40%, from 4.8 at baseline to 2.9 at post-treatment,
which then continued to drop another 57% to 1.3 at follow-up.
General Functioning
IIS. The IIS score dropped 30%, from 7 at baseline to 4.9 at post-treatment, which then
continued to drop another 32% to 3.3 at follow-up.
HAD. The HAD-anxiety score dropped 28%, from 18 at baseline to 13 at post-treatment, which
then continued to drop another 23% to 10 at follow-up. The pattern of change was slightly different for
the HAD-depression score, which only dropped by 1 point (8% reduction) from 13 at baseline to 12 at
post-treatment. A bigger improvement was, however, observed at ~9-month when the score dropped
67% to 4, below the clinical cut-off (8).
Discussion
The current report is the first study to demonstrate that insomnia symptoms associated with
social phobia, depression and alcohol misuse can be effectively treated using a brief 5-session CBT-I.
Overall, Lee’s response to the treatment was encouraging. Considerable reduction in insomnia
symptoms were observed after treatment; the ISI, SOL, WASO duration and SE demonstrated
improvements at a level that met dual criteria for clinical significance (criterion 1: a 50% reduction of
symptoms; criterion 2: conventional cut-offs; ISI<15; SOL or WASO<30 minutes; SE >85%). The
only exception was TST; the gain in this parameter did not reach clinical significance even though it
was extended by ~1.5 hours following treatment. This might be explained by the principle of the sleep

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 12
restriction therapy that aimed to consolidate rather than to lengthen sleep, and possibly by a ceiling
effect on how much sleep Lee’s body could actually obtain.
Sleep of chronic insomniacs is marked by extensive day-to-day variability (Vaillieres, Ivers,
Bastien, Beaulieu-Bonneau, & Morin, 2005). CBT-I involves the use of treatment strategies that aim to
help the patient establish a regular sleep-wake schedule (e.g., stimulus control and sleep restriction),
and these are typically associated with a reduction of such variability in sleep and thus improved the
quality of sleep (Edinger, Wohlgemuth, Radtke, Marsh, & Quillian, 2001). Consistently, a visual
inspection of Figure 1 indicates that Lee's sleep measures (SE, SOL, WASO and TST) were marked
with greater variability at baseline and beginning of treatment than at post-treatment and follow-up.
This shrinkage in variability can be interpreted as another indicator of treatment success.
Corresponding improvements were observed in the levels of sleep-related anxiety and
dysfunctional beliefs about sleep. These are cognitive processes hypothesised to be perpetuating Lee’s
insomnia and were actively targeted in the current treatment. Some improvements were noted in Lee’s
general anxiety, but only minimal change was observed in his depression rating. Moreover, a post-hoc
examination of Lee's notes indicated that the insomnia treatment did not change his score on the
Liebowitz Social Anxiety Scale (Liebowitz, 1987). It appears that improvements in sleep do not
necessarily bring about an immediate anxiolytic or mood-enhancing effect as one may hypothesise
based on the close link between sleep, anxiety and depression. Although these findings are consistent
with those of a previous study in which the success of CBT-I was not accompanied by similar mood
improvement in a mixed group of secondary insomnia patients (Lichstein, Wilson & Johnson, 2000),
they stand in contrast with those from another study in which the addition of CBT-I to an
antidepressant enhanced treatment outcomes for both conditions (Manber, Edinger, Gress, San Pedro-
Salcedo, Kuo, & Kalista, 2008). The lack of improvement in mood may be explained by the focus of
the treatment being on sleep (rather than anxiety or mood) and its relatively short duration. Further
investigation is required to delineate the often-assumed reciprocal interaction between insomnia and
anxiety and depression. More information about the interplay between social phobia and insomnia and

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 13
the shared vulnerability between the two conditions should inform the adaptation of CBT-I for use in
patients with comorbid anxiety disorders.
Maintenance of the improvements in sleep quality, insomnia-related psychological processes
and general level of daytime functioning was excellent at ~9-month follow-up. In fact, all of the sleep-
related variables further improved from immediately to ~9-month after treatment. These continual
improvements probably are a result of the combined effectiveness of the CBT-I and the subsequent
cognitive therapy for social phobia Lee received (Clark, 2001). It is interesting to note that there was a
sharp reduction in HAD depression scores from post-treatment to follow-up, but not anytime before.
This appears to suggest that a newly rectified sleep pattern may not be sufficient to bring about
immediate improvements in mood. The introduction of additional treatment that specifically targets
social anxiety and low mood may be necessary to alleviate these symptoms.
Case study has played an influential role in the development of clinical research and is a widely
endorsed approach to explore new phenomena and treatment strategies (Kazdin, 2003). Whilst it has
many advantages as a preliminary research methodology (e.g., being clinically relevant and time-
efficient), replications of the findings in larger samples of social phobics with comorbid insomnia are
required to establish the generalisability of the results and it would be important for future research to
evaluate the treatment effect against an active control treatment. It was a pragmatic decision to treat
Lee’s insomnia ahead of his social phobia treatment. Further research is needed to identify the most
effective treatment sequence for people with concomitant anxiety and sleep issues and to examine if
the gains in sleep can be maintained in the absence of the subsequent social phobia treatment. Within
the confines of the limitations discussed, the current case report highlights the potential to successfully
(and economically) treat insomnia comorbid with social anxiety. More systematic research is now
called for to investigate the clinical benefits of incorporating a brief CBT-I into existing treatments for
social phobia.

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 14
Author Note
Nicole Tang is funded by a Post Doctoral Award from the National Institute of Health
Research (Department of Health), United Kingdom. The author would like to thank
Drs. Jennifer Wild and Rachel Handley for facilitating the treatment and Dr. Claire Goodchild and
Professor David Clark for reading an earlier draft of the manuscript.

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 15
References
Bastien, C., Vallières, A., & Morin, C. M. (2001). Validation of the Insomnia Severity Index as a clinical outcome measure for insomnia research. Sleep Medicine, 2, 297-307.
Beck, A. T., Epstein, N., Brown, G., & Steer, R. A. (1988). An inventory for measuring clinical anxiety: psychometric properties. Journal of Consulting and Clinical Psychology, 56, 893-897.
Buckner, J.D., Bernert, R.A., Cromer, K.R., Joiner, T.E., & Schmidt, N.B. (2008). Social anxiety and insomnia: The mediating role of depressive symptoms. Depression and Anxiety, 25, 124-130.
Buysse, D. J., Reynolds III, C. F., Monk, T. H., Berman, S. R., & Kupfer, D. J. (1989). The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatric Research, 28, 193-213.
Clark, D. M. (2001). A cognitive perspective on social phobia. In W.R. Crozier, & L. E. Alden (Eds.), International Handbook of Social Anxiety: Concepts, Research and Interventions Relating to the Self and Shyness. pp. 405-430. Chichester, UK: John Wiley & Sons.
Clark, D. M., & Well, A. (1995). A cognitive model of social phobia. In R. Heimberg, M. Liebowitz, D.A. Hope, & F. R. Schneier (Eds.), New Oxford Textbook of Psychiatry. Oxford, UK: Oxford University Press.
Degonda, M., & Angst, J. (1993). The Zurich Study. XX. Social Phobia and Agoraphobia. European Archives of Psychiatry and Clinical Neuroscience, 243(2), 95-102.
Edinger, J. D. & Carney, C. (2008). Overcoming Insomnia: A Cognitive-Behavioral Therapy Approach. Therapist Guide. Oxford: Oxford University Press.
Edinger, J. D., Wohlgemuth, W. K., Radtke, R. A., Marsh, G. R., & Quillian, R.E. (2001) Cognitive behavioral therapy for treatment of chronic primary insomnia: A randomized controlled trial. Journal of the American Medical Association, 285, 1856-1864.
Gross, R. T. & Borkovec, T. D. (1982). Effects of a cognitive intrusion manipulation on the sleep-onset latency of good sleepers. Behaviour Therapy, 13, 112-116.
Harvey, A. G., Sharpley, A. L., Ree, M. J., Stinson, K., & Clark, D. M. (2007). An open trial of cognitive therapy for chronic insomnia. Behaviour Research and Therapy, 45, 2491-2501.
Kazdin, A. E. (2003). Drawing valid inferences from case studies. In A. E. Kazdin (Ed.). Methodological Issues and Strategies in Clinical Research (3rd ed.). Washington, DC: American Psychological Association.
Lichstein, K., Wilson, N., & Johnson C. T. (2000). Psychological treatment of secondary insomnia. Psychology and Aging, 15, 232-240.
Liebowitz, M.R. (1987). Social Phobia. Modern Problems of Pharmacopsychiatry, 22, 141-173.
Manber, R., Edinger, J., Gress, J., San Pedro-Salcedo, M., Kuo, T., & Kalista, T. (2008). Cognitive behavioral therapy for insomnia enhances depression outcome in patients with comorbid major depressive disorder and insomnia. Sleep, 31, 489-495.

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 16
Morin, C. M. & Espie, C. A. (2003). Insomnia: A Clinical Guide to Assessment and Treatment. New York: Springer.
Morin, C. M., Vallières, A., & Ivers, H. (2007). Dysfunctional beliefs and attitudes about sleep (DBAS): validation of a brief version (DBAS-16). Sleep, 30, 1547-1554.
Neckelmann, D., Mykletun, A., & Dahl, A. A. (2007). Chronic insomnia as a risk factor for developing anxiety and depression. Sleep, 30(7), 873-880.
Ohayon, M. M., & Roth, T. (2003). Place of chronic insomnia in the course of depressive and anxiety disorders. Journal of Psychiatric Research, 37(1), 9-15.
Smith, M., Huang, M., & Manber, R. (2005). Cognitive behavior therapy for chronic insomnia occurring within the context of medical and psychiatric disorders. Clinical Psychology Review, 25, 559-592.
Stein, M. B., Kroft, C. D. L., & Walker, J. R. (1993). Sleep impairment in patients with social phobia. Psychiatry Research, 49, 251-256.
Tang, N. K. Y. & Harvey, A. G. (2004a). Correcting distorted perception of sleep in insomnia: A novel behavioural experiment? Behaviour Research and Therapy, 42, 27-39.
Tang, N. K. Y. & Harvey, A. G. (2004b). Effects of cognitive arousal and physiological arousal on sleep perception. Sleep, 27, 69-78.
Vallieres, A.V., Ivers, H., Bastien, C. H., Beaulieu-Bonneau, S., & Morin, C.M. (2005). Variability and predictability in sleep patterns of chronic insomniacs. Journal of Sleep Research, 14, 447–453
Zigmond, A. S. & Snaith, R. P. (1983). The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica, 67, 361-370.

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 17
Table 1. Content and Procedure of the Treatment
Session Content HomeworkSession 1 Assessed insomnia using the Duke interview schedule
Reviewed sleep diary and pre-treatment questionnaires Provided psychoeducation on normal human sleep Discussed individual sleep needs and factors affecting sleep Explained treatment rationale and procedure Set treatment goals and expectations
To complete a daily sleep diary for a week To review the session tape
Session 2 Reviewed sleep hygiene practices Introduced the stimulus control rules Started sleep restriction therapy Discussed the lifestyle change involved (e.g., cutting down on alcohol)
To adhere to the agreed new sleep-wake schedule To practise all stimulus control rules To complete a daily sleep diary for a week To review the session tape
Session 3 Reviewed the sleep pattern over the past week, discussed and advised on problems encountered whilst implement-ing the new sleep-wake routine Offered motivation/encouragement to adhere to sleep restriction routine; adjusted the prescribed sleep window Discussed what caused sleepiness/tiredness during the day and whether taking a nap is the best way/only way to fight off these feelings. Explored other methods to combat daytime sleepiness/tiredness and set up a behavioural experiment to be com-pleted between sessions
To conduct a behavioural experiment as agreed To complete a daily sleep diary for a week To review the session tape
Session 4 Reviewed the sleep pattern over the past week, discussed and advised on problems encountered whilst implement-ing the new sleep-wake routine Offered motivation/encouragement to adhere to sleep restriction routine; adjusted the prescribed sleep window Reviewed the outcome of the behavioural experiment and discussed insights gained from the experience Drew a diagram charting the daily fluctuation of tiredness, sleepiness, mood and sense of achievement and high-lighted the lack of 1:1 correlation between these and sleep
To complete a daily sleep diary for a week, and monitor his mood, tiredness, sleepiness and sense of achievement To review the session tape
Session 5 Reviewed the sleep pattern over the past week, discussed and advised on problems encountered whilst implement-ing the new sleep-wake routine Offered motivation/encouragement to adhere to sleep restriction routine; adjusted the prescribed sleep window Reviewed the additional data on mood, tiredness, sleepiness and sense of achievement. Discussed ways to increase pleasurable activities during the day. Addressed concerns about losing the bout of art-related ideas/creativity during the pre-sleep period if insomnia was cured. Suggested to move work time forward and to create a wind-down routine.
To try and introduce a wind-down routine before bed To complete a daily sleep diary for a week, and monitor his mood, tiredness, sleepiness and sense of achievement alongside To review the session tape
Booster Session
Reviewed the sleep pattern over the past week and further adjusted the prescribed sleep window Reviewed learning from treatment and discussed relapse prevention
To review the session tape To complete and return a post-treatment questionnaire

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 18
Figure Caption
Figure 1. The daily changes in sleep diary outcomes variables over the course of the treatment.
Outcome variables presented here include: (1) sleep efficiency (SE; %, cut-off for normal sleep = 85%
or above, as indicated by the dotted horizontal line), (2) sleep onset latency (SOL; min, cut-off for
normal SOL = 30min or below, as indicated by the dotted horizontal line), (3) the total duration of
wake after sleep onset (WASO; min, cut-offs for normal WASO = 30min or below, as indicated by the
dotted horizontal line) and (4) total sleep time (TST; min)
Figure 2. The weekly changes in sleep questionnaire measures over the course of the treatment.
Measures presented here include: (1) Insomnia Severity Index (ISI; range: 0-28; cut-off for “no
clinically significant insomnia” = 7 or below, as indicated by the dotted horizontal line), (2) the
Anxiety and Preoccupation About Sleep Questionnaire score (APSQ; range: 10-100) and (3) the
Insomnia Interference Scale score (IIS; range: 0-10).

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 19
0
10
20
30
40
50
60
70
80
90
100
B-1 B-2 B-3 B-4 B-5 B-6 W1-1
W1-2
W1-3
W1-4
W1-5
W1-6
W1-7
W2-1
W2-2
W2-3
W2-4
W2-5
W2-6
W2-7
W3-1
W3-2
W3-3
W3-4
W3-5
W3-6
W3-7
W4-1
W4-2
W4-3
W4-4
W4-5
W4-6
W4-7
W5-1
W5-2
W5-3
W5-4
W5-5
W5-6
W5-7
P-1 P-2 P-3 P-4 P-5 P-6 P-7 P-8 FU-1
FU-2
FU-3
FU-4
FU-5
FU-6
FU-7
SE(%)
0
20
40
60
80
100
120
140
B-1 B-2 B-3 B-4 B-5 B-6 W1-1
W1-2
W1-3
W1-4
W1-5
W1-6
W1-7
W2-1
W2-2
W2-3
W2-4
W2-5
W2-6
W2-7
W3-1
W3-2
W3-3
W3-4
W3-5
W3-6
W3-7
W4-1
W4-2
W4-3
W4-4
W4-5
W4-6
W4-7
W5-1
W5-2
W5-3
W5-4
W5-5
W5-6
W5-7
P-1 P-2 P-3 P-4 P-5 P-6 P-7 P-8 FU-1
FU-2
FU-3
FU-4
FU-5
FU-6
FU-7
SOL(min)
(1)
(2)
(3)
(4)
Baseline Treatment Post-treatment Follow-up
WASO(min)
TST(min)

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 20
0
50
100
150
200
250
300
350
400
450
B-1 B-2 B-3 B-4 B-5 B-6 W1-1
W1-2
W1-3
W1-4
W1-5
W1-6
W1-7
W2-1
W2-2
W2-3
W2-4
W2-5
W2-6
W2-7
W3-1
W3-2
W3-3
W3-4
W3-5
W3-6
W3-7
W4-1
W4-2
W4-3
W4-4
W4-5
W4-6
W4-7
W5-1
W5-2
W5-3
W5-4
W5-5
W5-6
W5-7
P-1 P-2 P-3 P-4 P-5 P-6 P-7 P-8 FU-1
FU-2
FU-3
FU-4
FU-5
FU-6
FU-7
0
50
100
150
200
250
300
350
400
450
500
B-1 B-2 B-3 B-4 B-5 B-6 W1-1
W1-2
W1-3
W1-4
W1-5
W1-6
W1-7
W2-1
W2-2
W2-3
W2-4
W2-5
W2-6
W2-7
W3-1
W3-2
W3-3
W3-4
W3-5
W3-6
W3-7
W4-1
W4-2
W4-3
W4-4
W4-5
W4-6
W4-7
W5-1
W5-2
W5-3
W5-4
W5-5
W5-6
W5-7
P-1 P-2 P-3 P-4 P-5 P-6 P-7 P-8 FU-1
FU-2
FU-3
FU-4
FU-5
FU-6
FU-7
(1)

BRIEF CBT-I FOR INSOMNIA IN SOCIAL PHOBIA 21
0.0
7.0
14.0
21.0
28.0
Baseline Week 1 Week 2 Week 3 Week 4 Week 5 Post-treatment ~9-month F/U
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Baseline Week 1 Week 2 Week 3 Week 4 Week 5 Post-treatment ~9-month F/U
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
10.0
Baseline Week 1 Week 2 Week 3 Week 4 Week 5 Post-treatment ~9-month F/U
(2)
(3)
ISI
APSQ
IIS